Unilateral sudden hearing loss as a result anomalous carotid anatomy Stanley Owen Snyder, Jr., MD, Norfolk, Va. of The term sudden hearing loss refers to hearing losses of sensorineural origin that evolve over a short period of time and are often of unknown origin. Common causes include damage to the cochleovestibular nerve by viral infection, autoimmune disease, vascular insult, and labyrinthine membrane rupture. A 70-year-old man had a history of recent diplopia, dysarthria, syncopal episodes, dysequilibrium, and the sudden onset of deafness in his right ear. Angiography demonstrated severe ulcerative stenosis of the right internal carotid origin and an anomalous vessel (probable remnant of hypoglossal artery) origi- nating from the distal right internal carotid artery that perfnsed the entire distal vertebral and basilar artery ciroxlation. Arch angiograms confirmed the absence of a proximal right vertebral artery and revealed a small left vertebral artery that ended in the cervical region without reaching the poterior fossa. Standard right carotid endarterectomy with patch angioplasty resolved all neurologic symptoms except for persistent unilateral deafness at 9 months' follow-up. Presumed embolization through this anomalous vessel to the in- ternal auditory artery and subsequent cochlear and vestibular branches represents the first reported case of sudden hearing loss as a result of anterior circulatory ulcerative disease. (J VASC SURG 1990;12:341-4.) Sudden hearing loss (SHL) is an otologic term that generally refers to hearing losses of a sensori- neural origin. The following pathologic states have been linked with SHL: viral and bacterial, autoim- mune, vascular, labyrinthine membrane rupture, acoustic neuroma (10%), Meniere's disease (10%), multiple sclerosis (3%), ototoxic drugs, metastatic temporal bone lesions, idiopathic; but the most com- mon etiologic theories include viral agents, autoim- mtme mechanisms, labyrinth membrane rupture, and vascular insult. 1 Vascular occlusion by hypercoagulation syn- dromes, microembolism, or occlusive disease may cause necrosis of the membranous labyrinth followed by fibrosis and ossification of the inner ear. 2 Em- bolization to the basilar artery circulation from a proximal internal carotid artery (ICA) source via a rare anomalous persistent hypoglossal artery has been previously reported, 3 but this is believed to represent the first reported case of unilateral acute deafness caused by embolization from a carotid artery lesion. From the Norfolk Surgical Group, Ltd., Norfolk, Virginia. Presented at the Fourteenth Annual Meeting of the Southern Association for Vascular Surgery, Acapulco, Mexico, Jan 24- 27, 1990. Reprint requests: Stanley O. Snyder, Jr., MD, Norfolk Surgical Group, Ltd. 250 West Brambleton Ave., Suite 101, Norfolk, VA 23510. 24/6/22788 CASE REPORT A 70-year-old hypertensive, insulin-dependent diabetic white man came for treatment on Jan. 6, 1989, with a 3- week history of acute vertebrobasilar ischemia symptoms that included five syncopal episodes (with brief losses of consciousness), intermittent diplopia, dysequilibrium with falling to the right, and a sensation of his right ear being "blocked up". Significant past history began in January 1985 when he experienced problems with intermittent diz- ziness and was later hospkalized in August 1985 with an acute episode of dysarthria and left facial weakness. Pe- ripheral vascular laboratory studies in 1985 showed no evidence of hemodynamically significant carotid occlusive disease. Angiography on Aug. 8, 1985 (Fig. 1) revealed only "mild" right ICA occlusive disease but was notewor- thy in that a large persistent hypoglossal artery was dem- onstrated arising from the midportion of the extracranial right ICA. In addition, the right vertebral artery was absent and a tiny left vertebral artery was noted to be "rudimen- tary," ending in the posterior inferior cerebeUar artery with- out contributing to the large basilar artery that was per- fused by the persistent hypoglossal artery. Initial CT scan findings on Aug. 7, 1985, were negative, but a repeat scan 5 days later on Aug. 12, 1985, showed a low density infarct area in the right centrum ovale region. An electrocardio- gram was within normal limits, and echocardiography demonstrated no evidence of mural thrombus or valxallar abnormalities. Neurologic consultation was obtained and concluded that the symptoms were due to intracranial small vessel thrombosis caused by diabetes and hypertension and recommended anticoagulation rather than carotid endar- 341
Transcript
Unilateral sudden hearing loss as a result anomalous carotid anatomy Stanley Owen Snyder , Jr., MD, Norfolk, Va.
of
The term sudden hearing loss refers to hearing losses of sensorineural origin that evolve over a short period of time and are often of unknown origin. Common causes include damage to the cochleovestibular nerve by viral infection, autoimmune disease, vascular insult, and labyrinthine membrane rupture. A 70-year-old man had a history of recent diplopia, dysarthria, syncopal episodes, dysequilibrium, and the sudden onset of deafness in his right ear. Angiography demonstrated severe ulcerative stenosis of the right internal carotid origin and an anomalous vessel (probable remnant of hypoglossal artery) origi- nating from the distal right internal carotid artery that perfnsed the entire distal vertebral and basilar artery ciroxlation. Arch angiograms confirmed the absence of a proximal right vertebral artery and revealed a small left vertebral artery that ended in the cervical region without reaching the poterior fossa. Standard right carotid endarterectomy with patch angioplasty resolved all neurologic symptoms except for persistent unilateral deafness at 9 months' follow-up. Presumed embolization through this anomalous vessel to the in- ternal auditory artery and subsequent cochlear and vestibular branches represents the first reported case of sudden hearing loss as a result of anterior circulatory ulcerative disease. (J VASC SURG 1990;12:341-4.)
Sudden hearing loss (SHL) is an otologic term that generally refers to hearing losses o f a sensori- neural origin. The following pathologic states have been linked with SHL: viral and bacterial, autoim- mune, vascular, labyrinthine membrane rupture, acoustic neuroma (10%), Meniere's disease (10%), multiple sclerosis (3%), ototoxic drugs, metastatic temporal bone lesions, idiopathic; but the most com- mon etiologic theories include viral agents, autoim- mtme mechanisms, labyrinth membrane rupture, and vascular insult. 1
Vascular occlusion by hypercoagulation syn- dromes, microembolism, or occlusive disease may cause necrosis o f the membranous labyrinth followed by fibrosis and ossification of the inner ear. 2 Em- bolization to the basilar artery circulation from a proximal internal carotid artery (ICA) source via a rare anomalous persistent hypoglossal artery has been previously reported, 3 but this is believed to represent the first reported case o f unilateral acute deafness caused by embolization from a carotid artery lesion.
From the Norfolk Surgical Group, Ltd., Norfolk, Virginia. Presented at the Fourteenth Annual Meeting of the Southern
Association for Vascular Surgery, Acapulco, Mexico, Jan 24- 27, 1990.
Reprint requests: Stanley O. Snyder, Jr., MD, Norfolk Surgical Group, Ltd. 250 West Brambleton Ave., Suite 101, Norfolk, VA 23510.
24/6/22788
CASE REPORT A 70-year-old hypertensive, insulin-dependent diabetic
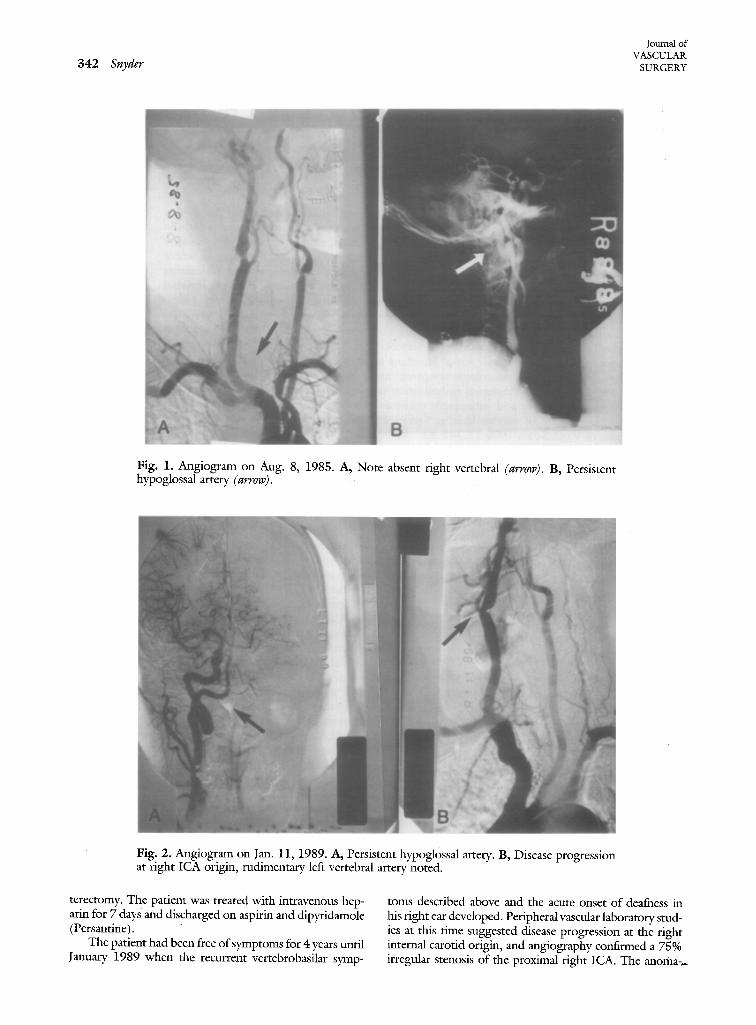
white man came for treatment on Jan. 6, 1989, with a 3- week history of acute vertebrobasilar ischemia symptoms that included five syncopal episodes (with brief losses of consciousness), intermittent diplopia, dysequilibrium with falling to the right, and a sensation of his right ear being "blocked up". Significant past history began in January 1985 when he experienced problems with intermittent diz- ziness and was later hospkalized in August 1985 with an acute episode of dysarthria and left facial weakness. Pe- ripheral vascular laboratory studies in 1985 showed no evidence of hemodynamically significant carotid occlusive disease. Angiography on Aug. 8, 1985 (Fig. 1) revealed only "mild" right ICA occlusive disease but was notewor- thy in that a large persistent hypoglossal artery was dem- onstrated arising from the midportion of the extracranial right ICA. In addition, the right vertebral artery was absent and a tiny left vertebral artery was noted to be "rudimen- tary," ending in the posterior inferior cerebeUar artery with- out contributing to the large basilar artery that was per- fused by the persistent hypoglossal artery. Initial CT scan findings on Aug. 7, 1985, were negative, but a repeat scan 5 days later on Aug. 12, 1985, showed a low density infarct area in the right centrum ovale region. An electrocardio- gram was within normal limits, and echocardiography demonstrated no evidence of mural thrombus or valxallar abnormalities. Neurologic consultation was obtained and concluded that the symptoms were due to intracranial small vessel thrombosis caused by diabetes and hypertension and recommended anticoagulation rather than carotid endar-
341
342 Snyder Journal of
VASCULAR SURGERY
Fig. 1. Angiogram on Aug. 8, 1985. A, Note absent right vertebral (arrow). B, Persistent hypoglossal artery (arrow).
Fig. 2. Angiogram on Jan. 11, 1989. A, Persistent hypoglossal artery. B, Disease progression at l'ight ICA origin, rudimentary left vertebral artery noted.
terectomy. The patient was treated with intravenous hcp- arin for 7 days and discharged on aspirin and dipyridamole (Persantine).
The patient had been free of symptoms for 4 years until January 1989 when the recurrent vertebrobasilar syrup-
toms described above and the acute onset of deafness in his right ear developed. Peripheral vascular laboratory stud- ies at this time suggested disease progression at the right internal carotid origin, and angiography confirmed a 75% irregular stenosis of the proximal right ICA. The anoma-~
Volume 12 Number 3 September i990 Unilateral sudden hearing loss 343
Fig. 3, Magnetic resonance imaging on Jan. 10, I989, shows multiple infarcts, old right centrum ovale (small arrow), right pontine (large arrow).
Endotyml~ati¢,
o.4m~ar
¢ J
Anterior Artery
~mmml
AO~mry
~mmm!
Fig. 4. Internal auditory (labyrinthine) artery anatomy. (From Belal A, jr. Laryngoscope 1980;90:1831-93
344 Snyder
j UU[llal Ol
VASCULAR. SURGERY
lous persistent hypoglossal artery was again demonstrated, and additional disease was noted at the left ICA origin (Fig. 2, A and B). CT scanning confirmed the previous tight parietal infarct from 1985, but a magnetic resonance image study (Fig. 3) showed evidence of multiple small infarcts including the right pontine area. On physical ex- amination the patient's Weber test lateralized to the left ear, and Rinne tests were abnormal with air conduction greater than bone conduction on the left, but no perception present on the right side. Ear, nose, and throat consultation confirmed complete hearing loss of the right ear with an audiogram and suggested embolization as the pathologic event.
On Jan. 12, 1989 the patient tmderwent tight carotid endarterectomy with special care taken to keep the distal tip of the No. 12 USCI (Bard Cardiosurgery, Billetica, Mass.) shunt proximal to the takeoff of the persistent hy- poglossal artery. At surgery, the right ICA lesion was noted to be extremely necrotic, irregular, and ulcerative with ev- idence of recent hemorrhage within the plaque. The pro- cedure was uneventful, and after surgery the patient has remained essentially free of symptoms except for persistent right ear deafness.
D I S C U S S I O N
Sudden hearing loss from a sensorineural origin evolves over a period of hours to days. Vascular oc- clusion is an attractive SHL etiologic thcory, as ex- perimental microembotization o f the cochlear vessels has shown damaged cochlear function within 60 sec- onds, and this toss is permanent after 30 minutes with resultant fibrosis and calcification of the co- chlea. 1
Embryologically the hypoglossal artery is patent between the carotid and vertebrobasilar system for approximately 1 week in utero and is obliterated in the 7 to 12 mm embryonic stage as the two longi- tudinal neural arteries formed along the basal surface of the hindbrain fuse to form the basilar artery, and join the vertebral arteries that represent the fusion of the transverse anastomoses between the six cervical segmental arteries. At this stage there is regression of the primitive trigeminal, otic, hypoglossal, and proatlantal carotid-basilar anastomoses as the pos- terior communicating arteries develop to provide perfusion to the hindbrain.
The internal auditory artery (or labyrinth artery) (Fig. 4) branches from the anterior inferior cerebeltar
artery and is the primary blood supply to the cochlea as it divides into the common cochlear artery and anterior vestibular artery. The anomalous vessel vi- sualized in this case (Fig. 2, A) provides embolic access to the basilar artery and anterior inferior cer-: ebellar artery. It meets all the following anatomic diagnostic criteria for persistent hypoglossal artery as described by Lie: ~ (1) It arises as a robust branch of the cervical internal carotid artery at the C-1 to C-3 level. (2) It proceeds in a tortuous fashion through the anterior condyloid foramen (the hypoglossal ca -~ nal) to the posterior cranial fossa. (3) The basilar artery is seen only beyond the point of anastomosis with the hypoglossal artery. (4) The posterior com- municating arteries are not visible arteriographically. In addition, the ipsilateral proxinaal vertebral artery is absent as described by McCarmey ct al.6 PreoB; erative recognition of this anomaly can be critical because the brain stem, cerebellum, and ipsilateral cerebral hemisphere are perfused by a single carotid artery possibly mandating the use of a shunt for in- traoperative protection during endarterectomy.
The acute onset of symptoms including tmilateral SHL in this patient with demonstrated disease pro- gression of a markedly ulcerative plaque and multiple anterior and posterior cerebral infarcts seen by mag- netic resonance imaging supports the hypothesis of unilateral SHL caused by embolization from a prox- imal ICA source to the vestibular cochlear region via a persistent hypoglossal artery.
The author thanks Martha Wimett for assistance in the preparation of this manuscript.
REBERENCES
1. Cole RR, Jahrsdoerfer RA. Sudden hearing loss: an updat. Am J Otol 1988;9:211-5.
2. Belal A Jr. The effect of vascular occlusion in the human inner ear. J Laryngol Otol 1979;193:955-68.
3. Ouriel K, Green RM, DeWeese JA. Anomalous carotid-basilar anastomoses in cerebrovascular surgery. J Vasc SURG 1988; 7:774-7. Belal A Jr. Pathology of vascular sensoineural hearing impair- ment. Laryngoscope 1980;90:1831-9. Lie TA. Congenital abnormalities of the carotid arteries. Am- sterdam: Excerpta Medica 1968:52-93. McCarmey SF, Ricci MA, Labreque P, Symes JF. Persistent hypoglossal artery encountered during carotid endarterectomy. Ann Vase Surg 1989;3:257-60.