61
Update from DDW 2015 for IAGH PROF REZA MALEKZADEH M.D DDRC/TUMS TIRMAH 1394
Update from DDW
2015 for IAGHPROF REZA MALEKZADEH M.D
DDRC/TUMS TIRMAH 1394

DDW 2015

Lecture at Department of Global health

Division of Cancer Epidemiology and Genetics, NCI9609 Medical Center Drive, Rockville, MD 20850.Tuesday May 19, 2015-Room 7E032/034 (7th floor)• Time Topic Speaker• 2:30 – 3:00 PM Arrival, checking into building• 3:00 – 3:15 PM Opening, overview of the meeting S. Chanock, S. Dawsey, C. Abnet• 3:15 – 3:30 Overview of the current GEMINI status R. Malekzadeh• What’s new in Golestan Cohort? Session chair: P. Boffetta • 3:30 – 3:45 The GCS Follow-up Progress & Repeated Measurements H. Poustchi/R. Malekzadeh• 3:45 – 4:00 Oral Hygiene Study And Challenges E. Vogtmann• 4:00 – 4:15 Updates on Database Management and GEMSHARE A. Etemadi• 4:25 – 4:30 Nutritional Studies R. Malekzadeh• 4:30 – 5:00 Discussion Group• 5:00 – 5:15 Break S. Merat• Novelties Session chair: C. Abnet• 5:15 – 5:30 Opium GWAS: a proposal J. Pollock• 5:30 – 5:45 Hepatitis B, opium use, and prevalent kidney disease in the GCS C. Wyatt• 5:45 – 6:00 Studying Microbiome-1 E. Vogtmann• 6:00 – 6:15 Studying Microbiome-2 R. Sinha• 6:15 – 6:30 Coffee Studies E. Loftfield• 6:30 – 6:45 Nail studies C. Abnet• 6:45 – 7:00 Discussion Group• Special Meetings• 7:00 – 7:45 Closed meeting of PIs PIs• TBD Working group for urine shipments• TBD Working group for NESP

Thursday May 21, 2015- Room 5E032/034 (5th floor)Time
Topic Speaker1:00 – 1:30 PM
Arrival, checking into building1:30 – 1:45 PI Meeting Report PIs
Focus: Esophageal Cancer Session chair: S. Dawsey1:45 – 2:00 GESP results and NESP report G.R. Roshandel/ S. Merat
2:00 – 2:15 Urinary biomarkers of Tobacco Exposure N. Freedman
2:15 – 2:30 PAH studies and early detection A. Etemadi
2:30 – 3:00 Discussion and Break Group
Focus: Gastric Cancer Session chair: C. Abnet3:00 – 3:15 Estrogen and gastric cancer C. Rabkin/C. Camargo
3:15 – 3:30 Aspirin for early prevention trial R. Malekzadeh
3:30 – 3:45 Discussion Group
3:45 – 4:00 Break S. Merat
Beyond Golestan Session chair: R. Malekzadeh4:00 – 4:15 Genome-wide Association Studies of GC & ESCC C. Abnet
4:15 – 4:30 Poly-Iran project G.R. Roshandel/ S. Merat
4:30 – 4:45 Poly-Iran Liver Study S. Merat
4:45 – 5:00 Hepatitis B and C Cohorts H. Poustchi/ R. Malekzadeh
5:00 – 5:15 Discussion and Break Group
Offspring Studies Session chair: F. Kamangar5:15 – 5:30 Pars Cohort R. Malekzadeh
5:30 – 5:45 CT angiography/CAC score in Pars Cohort J Lima/ MR Ostovaneh
5:45 – 6:00 PERSIAN Cohort H. Poustchi
6:00 – 6:15 Tehran CCS of pancreato-biliary Cancer A. Pourshams/ R. Malekzadeh
6:30 – 6:45 Discussion Group
Final Remarks, Closing
6:45 – 7:00 Overall summary, action list A. Etemadi
Closing & Ice cream Break S. Merat


JHPU visit

JHPU visit & Lecture

• 9:50 a.m. Arrive at Bloomberg School of Public Health (615 North Wolfe Street Baltimore, MD 21205), welcome by Asieh Golozar and Mohammad Reza Ostovaneh
• Morning Meetings (Room E2133)
• 10:00 – 10:30 a.m. Hadi Kharrazi
• Assistant Professor, Department of Health Policy & Management; Assistant Director of the Center for Population Health Information Technology (CPHIT)
• 10:30 – 11:00 a.m. Judith Bass, PhD MPH
• Associate Professor, Department of Mental Health
•
• 11:00 – 11:45 a.m. Lunch/Seminar Prep
• E2133/Sheldon Hall (W1214)
• 12:00 – 1:15 p.m. Seminar • Sheldon Hall (W1214)
• Afternoon Meetings (Room E2527)• 1:30 – 4:00 p.m. Cardiology Presentations/Meeting • 1:45 – 2:00 p.m. Amir Pourmorteza, PhD• Stretch Quantifier for Endocardial Engraved Zones (SQUEEZ): A New CT Derived Tool to Assess Regional Cardiac Function• 2:00 – 2:15 p.m. Mohammad Ali Habibi, MD
Left Atrial Structure and Function: Role in Prognosis• 2:15 – 2:45 p.m. Mohammad Reza Ostovaneh, MD MPH
Utility of CT/CTA in Prevention of CVD in Middle East: Rationale and Design of the Study within Pars-Polypill Trial• 2:45 – 4:00 p.m. Group Discussion with Cardiology Faculties and Fellows
• 4:00 – 4:30 p.m. Azadeh Farzin, MD • Assistant Professor, Department of International Health; Department of Neonatology, School of Medicine• 4:30 – 5:00 p.m. Peter Zandi, MD PhD
Associate Professor, Department of Mental Health
• 5:30 p.m. Dnner
Achalasia• Dr Stavropoulos the only gastroenterologist with a world-
related population report of peroral endoscopy myotomy(POEM) for achalasia, presented 5-year data on his remarkable success in providing treatment to a high-risk population.
• He reported on 174 patients, of whom: Four were older than 90 years; 26% had severe comorbidities; 49% had previous treatments (eg, Botox®, failed Heller myotomies) that made POEM challenging; and 26% had advanced or end-stage achalasia with an esophageal diameter > 6 cm.


Eosinophilic Esophagitis
•The investigators compared the effectiveness of the six-food elimination diet vs topical corticosteroids, allowing either fluticasone or budesonide.
•The time horizon was 5 years.
•They allowed seven endoscopies to reassess the participants as foods were reintroduced.
Cotton CC, Hiller S, Green DJ, et al. Six-food elimination diet or topical steroids for first-line treatment of eosinophilicesophagitis: a cost-utility analysis. Program and abstracts of Digestive Disease Week; May 16-19, 2015; Washington,DC. Abstract 4.
Eosinophilic Esophagitis 2
• It was advantageous to go through the six-food elimination diet, even with all these endoscopies after each reintroduction.
• Going with the six-food elimination diet is shown to be more cost-effective.
• It is a whole lot less expensive from a food standpoint, but the endoscopies do still drive the cost
Celiac disease :most common small bowel disorders • Once considered a rare disorder, celiac disease is now one of the most
common small bowel disorders in the U.S. Every gastroenterologist deals with celiac disease, celiac patients and celiac misinformation.
• The prevalence of celiac disease has increased five times over the past 40 years.
• The drivers behind this increase are not clear, nor is it clear why some patients with celiac disease do not respond adequately to treatment.

Making a secure diagnosis remains a problem!• This is particularly true from patients who are already on a gluten-free diet
or have mild inflammation that may require specific application and interpretation of serology, biopsy and genetics, or possibly all three
• Meanwhile, many patients are trying to shortcut the diagnosis by using stool-based antibody tests that have not been validated for celiac disease, or genetic tests that are misinterpreted as positive for celiac disease.
• Other patients attempt to self-diagnose based on symptoms.
• Still others seek out practitioners who espouse alternative and untested theories such as “five cardinal signs of celiac” or “foods guaranteed to stop celiac.”

Challenges…Dangers
• “There is a danger that we are losing celiac disease — a real disease — in this morass of non-science,”
• “The field has almost been hijacked by non-scientists.
• The practicing gastroenterologist is getting swamped by misinformation.”
More Confusion!
• Another emerging area of confusion is the patient with celiac disease who is nonresponsive or has incomplete symptom or biopsy improvement on a gluten-free diet.
• Recent data confirm that not all patients with celiac disease respond to a gluten-free diet, Dr. Murray explained.
• But questions about nonresponse or inadequate response to a gluten-free diet are particularly difficult for patients who removed gluten from their diet before appropriate testing to confirm that they have celiac disease.
Controversy….cont.!!
• Different approaches to patients who do not respond to gluten-free diets can be even more confusing than making the original diagnosis of celiac disease.
• Some patients appear to be true non-responders. Others may not adhere to the gluten-free diet
• and some may be suffering the consequences of unrecognized gluten.
Potential Answers to Dilemmas
• There are no clear answers to questions about how we manage patients with celiac disease and partial histologic recovery,” Dr. Semradsaid.
• “But this symposium is going to address the latest evidence on these dilemmas to facilitate decision-making and management of celiac disease. Regardless of where you practice, you are going to see these patients and these dilemmas. This symposium is your one opportunity to get some answers.”
Something to question your Celiac patients about when they may not be responding to treatment.• Dr Green and his colleagues at Columbia Univ looked at the
gluten component using liquid chromatography.
• They looked at a composite of 22 probiotics, and a little more than two thirds of these were listed as gluten-free.
• When they actually studied them, they found that 55% contained gluten and two of them contained an incredibly high amount of gluten—amounts that they would view as a very alarming amount suggesting that gluten is in a lot of these probiotics, even when they say it isn't.
POEM is a real deal that should be considered
• Remarkably, all these patients did better.
• There were no major adverse events, suggesting that POEM is a real deal that should be considered, even for elderly, end-stage patients with comorbidities, before you consider esophagectomy.
• But it really comes down to the expertise of the locals, and although I don't know what we can extrapolate from this world renowned experience, look at your institution referral rates for where these patients are best served.
POEM for type III achalasia
• It is my bias that for type III achalasia, and particularly for chest pain, POEM is the way to go.
• And it may become one of the first interventions, as we look at these patients in the long term.

Crohn Disease and Therapy Withdrawal• One study[4] looked at withdrawal therapy in patients (from a single
institution) who had significant, deep remission.
• In 61 patients who were in deep remission, investigators withdrew the anti–TNF-alpha antagonist, be it infliximab or adalimumab.
• They found that the relapse rate was approximately one half at 2 years.
• The highest relapse rate was in the first year.
• Ileal disease somewhat increased the risk for disease flare-up, but they found no other identifiable factors.

Crohn’s …UK study• Another fascinating build on that study comes from the United Kingdom.[5]
In the United Kingdom, regulators require a reassessment of disease after 12 months of therapy, and if the patient is in clinical remission, it is recommended that you withdraw therapy.
• The investigators looked at 160 cases: 130 with infliximab and 30 with adalimumab.
• When they withdrew the therapy, the relapse rate was quite striking—44% at 1 year and 50% at 2 years

Crohn’s …UK study cont
• Younger age at diagnosis and an elevated white blood cell count were predictive of relapse.
• No other predictors were found, including such factors as smoking.
• Again, there was a very high relapse rate, even in the deep remission population.
• We clearly need better indicators of whom these agents can be withdrawn from.
Postsurgical patient with Crohn disease• Regueiro and colleagues did a postoperative intervention with an anti–
TNF-alpha antagonist in the postsurgical patient with Crohn disease.
• This was a 5-year, randomized, placebo-controlled, multicenter study comparing the withdrawal of all therapy with infliximab (5 mg/kg). Dose escalation was allowed, the time horizon was 5 years, and 297 patients were followed.
• The primary endpoint was a composite of clinical symptoms combined with endoscopic findings.

Results• At the end of the evaluation at 76 weeks, no statistical difference was
found between the placebo and control populations,
• Although there was a numerical difference: 13% recurrence in the active treatment group vs 20% in the placebo group.
• If you look at endoscopic recurrence, there was nearly a twofold difference (30% with infliximab vs 60% with placebo).
• Because the primary endpoint was not met, however, it was not statistically significant, so the sponsor decided to close the study.

Conclusions
• The mucosal relapse rate is strikingly in favor of continued therapy. I'm
not sure that we have grounds to say that we should withdraw therapy
in patients who had enough complications to warrant surgery.
LINX for Treatment of GastroesophagealReflux Disease• Ongoing evaluation of the LINX® Reflux Management System (Torax Medical,
Inc.; Shoreview, Minnesota).
• LINX is a magnetic device used for the enhancement of the lower esophageal sphincter.
• Ganz et al and has now presented the 5-year data from 100 patients.
•
• All patients were on proton pump inhibitors (PPIs) at study entry, and the use of PPIs at 5 years was 15%.

How Does the LINX System Work?
The LINX System is designed to help the LES resist opening to gastric pressures.
The LINX System is designed to expand to allow for normal swallowing
Magnetic attraction of the device is designed to close the LES immediately after swallowing.
How is the LINX System Implanted?
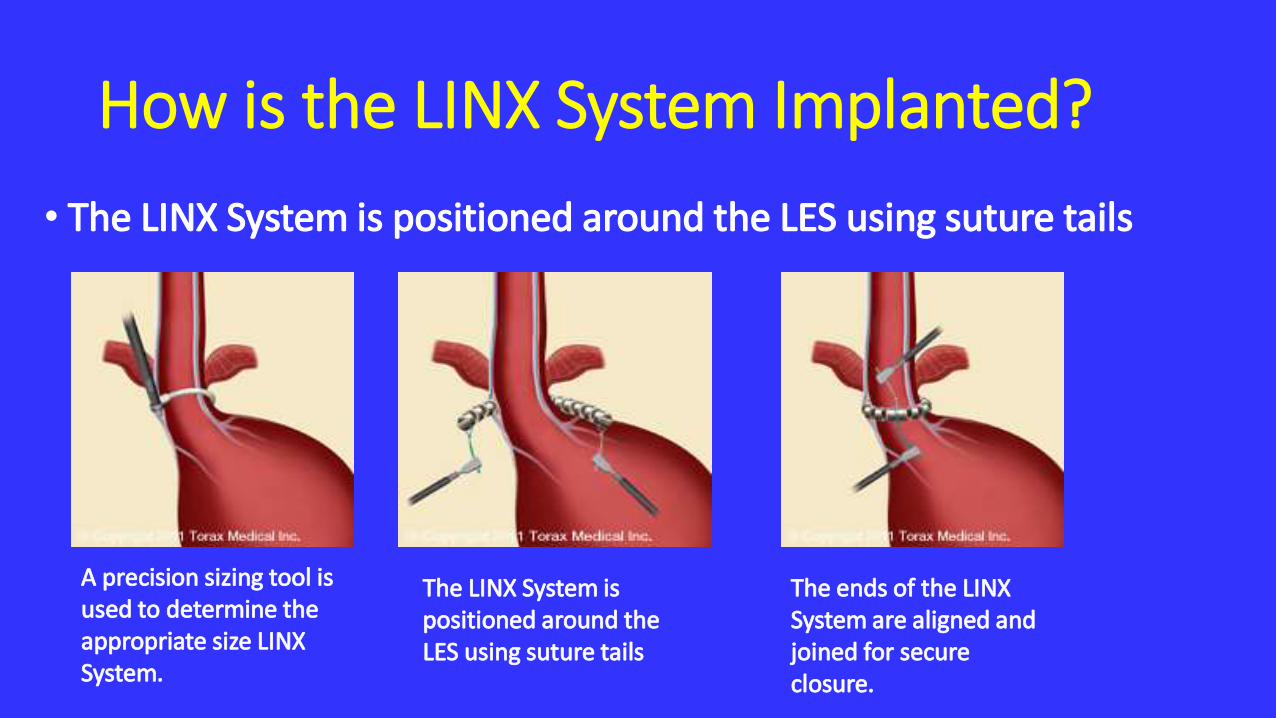
• The LINX System is positioned around the LES using suture tails
A precision sizing tool is used to determine the appropriate size LINX System.
The LINX System is positioned around the LES using suture tails
The ends of the LINX System are aligned and joined for secure closure.
Reduction in regurgitation• Regurgitation was reduced from 57% at baseline to 1.2% at 5 years.
• It's a very powerful indication that this is a durable operation, with no significant gas or bloating effect.
• Retching and the inability to vomit seem to be very much overcome with this device.
• Patients are placed under general anesthesia during the this laparoscopic procedure
• The LINX System does not require any anatomic alteration of the stomach. Most patients go home the day after surgery and resume a normal diet.
Safety is overwhelmingly in favor of the device• Again, I think this is something that you should be looking at
with your local surgeons.
• I would deal with your thoracic and foregut surgeons, particularly those who have an interest in this area.
• Many of these operations with LINX seem to require some crural diaphragm repair, especially if there is a hiatal hernia, so it may be something that you want to deal with an expert for.
• I think the safety is overwhelmingly in favor of the device, and the efficacy is quite striking.

Barrett Esophagus Mayoclinic study
• In looking at 337 patients at Mayoclinic .
• Progression of disease was strikingly low. The incidence of progression from low-grade dysplasia to either high-grade dysplasia or esophageal cancer was approximately 0.8% per year.
• This is very low and very different from what we have seen from a lot of European studies.

Barrett Esophagus Pen.study• Dr Falk's group at the University of Pennsylvania looked at 354 patients with
indefinite dysplasia.
• Reactive atypia is sometimes the mirror of confusion, at least in a lot of institutions.
• They found that indefinite dysplasia was strikingly low.
• An incidence of any dysplasia was about 1.4 cases per 100 person-years of high-grade dysplasia or esophageal adenocarcinoma.
• This suggests that indefinite dysplasia shouldn't be dismissed.

Two recent publications
• One is in the American Journal of Gastroenterology and is the BOB CAT guidelines which is a Delphi consensus guideline that registers recommendations for no dysplasia, low-grade dysplasia, and indefinite for dysplasia, as well as surveillance recommendations.
• This is something that I think is worth looking at.
• The other is a study[16] from the University of Washington in Seattle that looked at indefinite dysplasia, and is published in Clinical and Translational Gastroenterology.
PPI Safety and Bone Density:Targownick's study from Canada.
•This is a 5-year study that looked at it in an interesting way: Rather than standard bone density, they looked at three-dimensional CT.
•It is a very significant, highly advanced way to evaluate patients.

PPI and fracture •They looked at 104 participants: 52 PPI users and 52 controls.
•The bottom line is that there was no difference.
• If patients need a PPI, they should take it. If they need calcium and vitamin D, they should take them, but not because they are on a PPI.
IBS and peppermint oil• L-menthol, which is the main component of peppermint oil,
has antispasmodic and antinausea or anticarminative effects, as well as topical analgesic effects and a 5-HT3 receptor antagonist property.
• This was a prospective randomized study in IBS-D (diarrhea) and IBS-M (mixed).
• Seventy-two participants were enrolled, and the endpoint was 4 weeks.

Result of IBS trial
• There was nearly a twofold incremental gain in the active therapy arm with peppermint oil.
• IBgard is an over-the-counter, commercially available product, and it seems to have a remarkable effect.
• Virtually all patients who had moderate to severe symptoms improved, particularly related to abdominal pain or discomfort, bloating, or distention.
Irritable Bowel Syndrome therapy with peppermint oil
• For the passage of gas, sensation of incomplete evacuation, or obstipation, all seemingly improved in a very statistically significant fashion.
• There was no improvement in the constipation.
• There is a very low threshold to use this medication as it relates to a favorable benefit.
Big Data Provides a Powerful Tool, Not a Magic Wand, for GI Research• Datasets that make traditional data processing impossible or
inadequate or datasets that are large, varied or stream in rapidly.
• Analysis of the data must undergo the same scientific skepticism and attention to detail that researchers normally apply to their work.
• whether a certain disease responds to a medication, can now be refined to see which therapies work against certain subsets of the disease.

Personalized Medicine Coming to the Upper GI Tract
• Two decades of genomic research are about to transform the diagnosis and treatment of cancer, bacterial infection and other maladies in the upper GI tract.
• Emerging genomic data have revealed unrecognized and clinically important heterogeneity in esophageal disease, while gastric cancer has recently been categorized in four distinct genomic subtypes.
Personalized medicine is the promise
• “Personalized medicine is the promise of the future in the upper GI tract,” The Genomic Revolution – Personalizing the Upper GI Tract.
• The Cancer Genome Atlas (TCGA), a comprehensive and coordinated effort to accelerate understanding of the molecular basis of cancer.
• The TCGA project, supported by the National Institutes of Health, is mapping the genetic variation found in 31 common cancers, including gastric and esophageal disease.

Cancer included in the TCGA
• “Cancers were selected for inclusion in the TCGA based on their generally poor prognosis and overall public health impact.
• In addition to esophageal and gastric cancers, TCGA is characterizing cholangiocarcinoma, colorectal adenocarcinoma, hepatocellular carcinoma and pancreatic ductal adenocarcinoma.
Gastric cancers occur in four major subtypes based on their genomic makeup.
•Tumors that are positive for Epstein-Barr virus.
• Microsatellite unstable tumors.
•Genomically stable tumors.
•Tumors with chromosomal instability.

Precession medicine
•Researchers are already shifting their focus to target each of the subtypes based on specific pathways and potential clinical vulnerabilities for both prevention and treatment.
oesophageal cancer with more greater degree of heterogeneity • Has confirmed a greater degree of heterogeneity between tumors than
is seen in other tumor types, as well as a greater prevalence of mutations and unusual amplification patterns,
• This heterogeneity is likely a result of inflammation that precedes many esophageal cancers
• And while the wide degree of variation in esophageal tumors makes targeted treatment a more difficult goal to achieve, evidence supporting a link with inflammation may suggest other clinical pathways.

Target therapy
• This developing ability to target therapy based on an individual’s unique disease brings a lot of promise and excitement also brings a significant degree of challenge.
• We gastroenterologists have to understand both the promise of these technologies in developing more personalized medicine and also what the challenges are.”
Role of Gut Microbiota in Gastric cancer
• In Helicobacter predominant patients, the microbial compositions of gastric mucosa from gastric cancer patients are significantly different to chronic gastritis and intestinal metaplasia patients.
• These alterations of gastric microbial composition may play an important, as-yet-undetermined role in gastric carcinogenesis of Helicobacter predominant patients
The gastric microbiota consists of bacteria from seven to eleven phyla
• Proteobacteria,
• Firmicutes,
• Bacteroidetes.
• Actinobacteria
• Fusobacteria.
• Interference by Helicobacter pylori (H. pylori) does not remarkably interrupt the composition and structure of the gastric microbiota.

Increase the production of N-nitrosocompounds by gastric microbiota
• Absence of bacterial commensal from the stomach delays the onset of H. pylori-induced gastric cancer,
• Presence of artificial microbiota accelerates the carcinogenesis.
• Altered gastric microbiota may increase the production of N-nitrosocompounds, promoting the development of gastric cancer.
Role of microbiota in the development of gastric cancer
• Lowered acid secretion due to gastric atrophy favorsovergrowth of bacteria in the gastric fluid, enhancing the production of carcinogenic N-nitrosamine compounds.
• Recent studies on animal models strongly support the fundamental role of microbiota in the development of gastric cancer.
Animal Studies• Transgenic INS-GAS mice over-expressing human gastrin may spontaneously develop intramucosal
carcinoma[33].
• Gastric intraepithelial neoplasia developed in all specific pathogen-free male INS-GAS mice with a complex microbiota 7 mo after H. pylori infection[34].
• For germ free male INS-GAS mice which were absent of microbiota, however, the incidence of gastric intraepithelial neoplasia was only 10.0%.
• The incidence merely increased to 44.4% 11 mo after H. pylori infection[34].
• These results suggest a role of microbiota in the carcinogenesis of the stomach.
• Furthermore, colonization of the stomach by an artificial intestinal microbiota (Altered Schaedler’s Flora, including ASF356 Clostridium species, ASF361 Lactobacillus murinus and ASF519 Bacteroids species) increased the incidence of gastric intraepithelial neoplasia to 69.0% in male INS-GAS mice 7 mo after H. pylori infection[35]. Antibiotic treatments significantly delayed onset of gastric neoplasia in helicobacter-free and specific pathogen-free INS-GAS mice[36].
• These findings indicate the involvement of microbiota in the development of gastric cancer.
Widespread misinformation adds more complications.
• The most common presentation has changed from diarrhea to predominately extraintestinal manifestations or silent disease,”
• “Some individuals don’t even know they have celiac disease and others are convinced they have the disease when they do not.

Systematic review of Intragastric Balloon for Weight Loss
• In a systematic review of one newer balloon, the Orberaballoon, investigators summarized the results of 7 studies reporting Complications
• Two cases of intestinal obstruction occurred.
• Balloon leakage was the most common adverse event.
• Leakage was more common when the balloon was left in place longer than the recommended 6 months

Weight loss at 3 and 6 months and after balloon removal.
• The average weight loss was 12.9 kg after 3 months and 16 kg after 6 months.
• 80% of the 6-month weight loss was achieved in the first 3 months.
• An average of 52% of weight loss was sustained 1 year after balloon removal.

Thanks for your attention

















