Usefulness of Losartan on the Size of the Ascending Aorta in an Unselected Cohort of Children, Adolescents, and Young Adults With Marfan Syndrome Christiane Pees, MD a, *, Franco Laccone, MD b , Marion Hagl b , Veerle DeBrauwer, MD c , Elisabeth Moser, MD d , and Ina Michel-Behnke, PhD a Since 2008, when angiotensin II type I receptor blockade with losartan was introduced in the prevention of cardiovascular manifestation of Marfan syndrome (MFS), a specific treatment to address the cardiovascular lesions became available. The present study aimed to compare the response of such in an unselected cohort of patients with genotyped MFS. At a tertiary university children’s hospital, 20 pediatric and adolescent patients aged 1.7 to 21.6 years with genetically proven MFS were enrolled in a prospective treatment study of losartan for evaluation of the aortic dimensions and elasticity indexes. The mean follow-up period was 33 – 11 months. A significant reduction in the normalized aortic dimensions with losartan was observed in the valve, root, sinotubular junction, and ascending aortic segments (p [ 0.008, p <0.001, p [ 0.012, and p [ 0.001, respectively). No correlation between elasticity behavior and the decrease in the aortic dimension with losartan therapy was detectable. A significant correlation between stronger improvement and younger age at onset (r [ 0.643, p [ 0.002) and a longer therapy duration (r [ L0.532, p [ 0.016) was verifiable. However, no correlation between improvement with therapy and the type of mutation or presentation of clinical forms was remarkable. Elasticity also seemed to improve but not significantly. In conclusion, in our cohort of young patients with MFS, a significant improvement with losartan monotherapy was proved in all affected proximal aortic segments, with a better response to therapy when started at an earlier age and with a longer therapy duration. Ó 2013 Elsevier Inc. All rights reserved. (Am J Cardiol 2013;112:1477e1483) Marfan syndrome (MFS) is an autosomal dominantly inherited connective tissue disorder caused by mutations of the fibrillin-1 gene (FBN1), located on chromosome 15q21. 1 Fibrillin-1 is a component of elastic fibers, leading to weaker connective tissue formation, predominantly in the muscu- loskeletal, ocular, and cardiovascular systems in the case of mutation. Furthermore, it sequesters the large latent complex of transforming growth factor-b binding protein (TGF-b) and regulates its bioavailability for activation. 2 In 2003, Neptune et al 3 demonstrated that dysregulation of TGF- b activation is an important pathogenetic factor contributing to the genesis of MFS, opening new avenues for potential therapeutic strategies. Angiotensin’s activity can influence TGF-b signaling by stimulating TGF-b mRNA and protein expression, probably through its induction of thrombo- spondin. 2 Angiotensin II and angiotensin II type I (AT1) receptor expression is increased in the MFS aortic tissue 2 and is associated with cystic media necrosis, 3 leading to aneurysm formation. 2 Therefore, AT1-receptor blockade, for example using losartan, induces a decrease in TGF- b signaling by a reduction in the free TGF-b levels. 4 In a mouse model, it was shown that losartan not only pre- vented, but also reversed, aortic root dilation and elastic fiber degeneration in FBN1-deficient mice. 4 Subsequent to these findings, losartan was tested in 18 pediatric patients with MFS and aggressive aortic disease, with a dramatic stabilization of the aortic root diameters. 5 This prompted us to adopt our current medical strategy in our pediatric population with MFS. We report the results of our prospective, nonrandomized losartan monotherapy study in 20 pediatric patients with MFS on their aortic root dimen- sions and tissue elasticity. Methods The patients were prospectively selected from the Pedi- atric and Young Adult Marfan Outpatient Clinic (Vienna, Austria). All had been classified according to the newly established Ghent criteria. 6 The inclusion criteria were a clinical diagnosis of MFS according to the current Ghent criteria, 6,7 the presence of an FBN1-mutation, age 1 to 22 years at the start of therapy, and a minimum of 12 months of follow-up with a minimum of 2 follow-up visits. The exclusion criteria were Marfan-like syndromes, intolerance to AT1-receptor blockers, renal insufficiency, an a Department of Pediatric Cardiology, Pediatric Heart Center Vienna, University Children’s Hospital, Vienna, Austria; b Institute for Medical Genetics, Medical University of Vienna, Vienna, Austria; c Department of Orthopedics, Hospital Mittersill, Mittersill, Austria; and d Department of Ophthalmology, Medical University of Vienna; together for the Pediatric and Young Adult Marfan Syndrome Outpatient Clinic Vienna, Vienna, Austria. Manuscript received May 9, 2013; revised manuscript received and accepted June 4, 2013. See page 1482 for disclosure information. *Corresponding author: Tel: (þ43) 1-40-400-3290; fax: (þ43) 1-40- 400-3417. E-mail address: [email protected](C. Pees). 0002-9149/13/$ - see front matter Ó 2013 Elsevier Inc. All rights reserved. www.ajconline.org http://dx.doi.org/10.1016/j.amjcard.2013.06.019
Transcript
Usefulness of Losartan on the Size of the Ascending Aorta in anUnselected Cohort of Children, Adolescents, and Young Adults
With Marfan Syndrome
Christiane Pees, MDa,*, Franco Laccone, MDb, Marion Haglb, Veerle DeBrauwer, MDc,Elisabeth Moser, MDd, and Ina Michel-Behnke, PhDa
Since 2008, when angiotensin II type I receptor blockade with losartan was introduced in
aDepartment oUniversity ChildrGenetics, MedicalOrthopedics, HosOphthalmology, Mand Young AdultAustria. Manuscripaccepted June 4, 2
See page 1482*Correspondin
400-3417.E-mail addres
0002-9149/13/$ -http://dx.doi.org/1
the prevention of cardiovascular manifestation of Marfan syndrome (MFS), a specifictreatment to address the cardiovascular lesions became available. The present study aimedto compare the response of such in an unselected cohort of patients with genotyped MFS. Ata tertiary university children’s hospital, 20 pediatric and adolescent patients aged 1.7 to21.6 years with genetically proven MFS were enrolled in a prospective treatment study oflosartan for evaluation of the aortic dimensions and elasticity indexes. The mean follow-upperiod was 33 – 11 months. A significant reduction in the normalized aortic dimensionswith losartan was observed in the valve, root, sinotubular junction, and ascending aorticsegments (p [ 0.008, p <0.001, p [ 0.012, and p [ 0.001, respectively). No correlationbetween elasticity behavior and the decrease in the aortic dimension with losartan therapywas detectable. A significant correlation between stronger improvement and younger age atonset (r [ 0.643, p [ 0.002) and a longer therapy duration (r [ L0.532, p [ 0.016) wasverifiable. However, no correlation between improvement with therapy and the type ofmutation or presentation of clinical forms was remarkable. Elasticity also seemed toimprove but not significantly. In conclusion, in our cohort of young patients with MFS,a significant improvement with losartan monotherapy was proved in all affected proximalaortic segments, with a better response to therapy when started at an earlier age and witha longer therapy duration. � 2013 Elsevier Inc. All rights reserved. (Am J Cardiol2013;112:1477e1483)
Marfan syndrome (MFS) is an autosomal dominantlyinherited connective tissue disorder caused by mutations ofthe fibrillin-1 gene (FBN1), located on chromosome 15q21.1
Fibrillin-1 is a component of elastic fibers, leading to weakerconnective tissue formation, predominantly in the muscu-loskeletal, ocular, and cardiovascular systems in the case ofmutation. Furthermore, it sequesters the large latent complexof transforming growth factor-b binding protein (TGF-b)and regulates its bioavailability for activation.2 In 2003,Neptune et al3 demonstrated that dysregulation of TGF-b activation is an important pathogenetic factor contributingto the genesis of MFS, opening new avenues for potentialtherapeutic strategies. Angiotensin’s activity can influenceTGF-b signaling by stimulating TGF-b mRNA and proteinexpression, probably through its induction of thrombo-spondin.2 Angiotensin II and angiotensin II type I (AT1)
f Pediatric Cardiology, Pediatric Heart Center Vienna,en’s Hospital, Vienna, Austria; bInstitute for MedicalUniversity of Vienna, Vienna, Austria; cDepartment ofpital Mittersill, Mittersill, Austria; and dDepartment ofedical University of Vienna; together for the PediatricMarfan Syndrome Outpatient Clinic Vienna, Vienna,t received May 9, 2013; revised manuscript received and013.for disclosure information.g author: Tel: (þ43) 1-40-400-3290; fax: (þ43) 1-40-
see front matter � 2013 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2013.06.019
receptor expression is increased in the MFS aortic tissue2
and is associated with cystic media necrosis,3 leading toaneurysm formation.2 Therefore, AT1-receptor blockade,for example using losartan, induces a decrease in TGF-b signaling by a reduction in the free TGF-b levels.4 Ina mouse model, it was shown that losartan not only pre-vented, but also reversed, aortic root dilation and elasticfiber degeneration in FBN1-deficient mice.4 Subsequent tothese findings, losartan was tested in 18 pediatric patientswith MFS and aggressive aortic disease, with a dramaticstabilization of the aortic root diameters.5 This prompted usto adopt our current medical strategy in our pediatricpopulation with MFS. We report the results of ourprospective, nonrandomized losartan monotherapy study in20 pediatric patients with MFS on their aortic root dimen-sions and tissue elasticity.
Methods
The patients were prospectively selected from the Pedi-atric and Young Adult Marfan Outpatient Clinic (Vienna,Austria). All had been classified according to the newlyestablished Ghent criteria.6 The inclusion criteria werea clinical diagnosis of MFS according to the current Ghentcriteria,6,7 the presence of an FBN1-mutation, age 1 to22 years at the start of therapy, and a minimum of12 months of follow-up with a minimum of 2 follow-upvisits. The exclusion criteria were Marfan-like syndromes,intolerance to AT1-receptor blockers, renal insufficiency, an
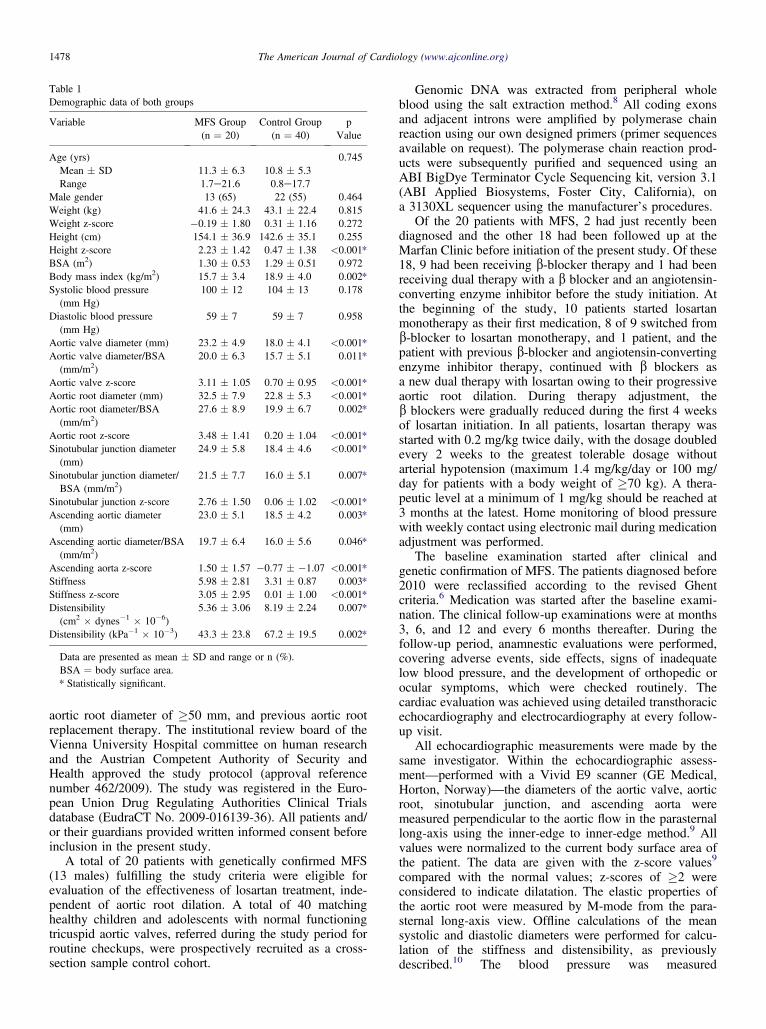
Data are presented as mean � SD and range or n (%).BSA ¼ body surface area.* Statistically significant.
1478 The American Journal of Cardiology (www.ajconline.org)
aortic root diameter of �50 mm, and previous aortic rootreplacement therapy. The institutional review board of theVienna University Hospital committee on human researchand the Austrian Competent Authority of Security andHealth approved the study protocol (approval referencenumber 462/2009). The study was registered in the Euro-pean Union Drug Regulating Authorities Clinical Trialsdatabase (EudraCT No. 2009-016139-36). All patients and/or their guardians provided written informed consent beforeinclusion in the present study.
A total of 20 patients with genetically confirmed MFS(13 males) fulfilling the study criteria were eligible forevaluation of the effectiveness of losartan treatment, inde-pendent of aortic root dilation. A total of 40 matchinghealthy children and adolescents with normal functioningtricuspid aortic valves, referred during the study period forroutine checkups, were prospectively recruited as a cross-section sample control cohort.
Genomic DNA was extracted from peripheral wholeblood using the salt extraction method.8 All coding exonsand adjacent introns were amplified by polymerase chainreaction using our own designed primers (primer sequencesavailable on request). The polymerase chain reaction prod-ucts were subsequently purified and sequenced using anABI BigDye Terminator Cycle Sequencing kit, version 3.1(ABI Applied Biosystems, Foster City, California), ona 3130XL sequencer using the manufacturer’s procedures.
Of the 20 patients with MFS, 2 had just recently beendiagnosed and the other 18 had been followed up at theMarfan Clinic before initiation of the present study. Of these18, 9 had been receiving b-blocker therapy and 1 had beenreceiving dual therapy with a b blocker and an angiotensin-converting enzyme inhibitor before the study initiation. Atthe beginning of the study, 10 patients started losartanmonotherapy as their first medication, 8 of 9 switched fromb-blocker to losartan monotherapy, and 1 patient, and thepatient with previous b-blocker and angiotensin-convertingenzyme inhibitor therapy, continued with b blockers asa new dual therapy with losartan owing to their progressiveaortic root dilation. During therapy adjustment, theb blockers were gradually reduced during the first 4 weeksof losartan initiation. In all patients, losartan therapy wasstarted with 0.2 mg/kg twice daily, with the dosage doubledevery 2 weeks to the greatest tolerable dosage withoutarterial hypotension (maximum 1.4 mg/kg/day or 100 mg/day for patients with a body weight of �70 kg). A thera-peutic level at a minimum of 1 mg/kg should be reached at3 months at the latest. Home monitoring of blood pressurewith weekly contact using electronic mail during medicationadjustment was performed.
The baseline examination started after clinical andgenetic confirmation of MFS. The patients diagnosed before2010 were reclassified according to the revised Ghentcriteria.6 Medication was started after the baseline exami-nation. The clinical follow-up examinations were at months3, 6, and 12 and every 6 months thereafter. During thefollow-up period, anamnestic evaluations were performed,covering adverse events, side effects, signs of inadequatelow blood pressure, and the development of orthopedic orocular symptoms, which were checked routinely. Thecardiac evaluation was achieved using detailed transthoracicechocardiography and electrocardiography at every follow-up visit.
All echocardiographic measurements were made by thesame investigator. Within the echocardiographic assess-ment—performed with a Vivid E9 scanner (GE Medical,Horton, Norway)—the diameters of the aortic valve, aorticroot, sinotubular junction, and ascending aorta weremeasured perpendicular to the aortic flow in the parasternallong-axis using the inner-edge to inner-edge method.9 Allvalues were normalized to the current body surface area ofthe patient. The data are given with the z-score values9
compared with the normal values; z-scores of �2 wereconsidered to indicate dilatation. The elastic properties ofthe aortic root were measured by M-mode from the para-sternal long-axis view. Offline calculations of the meansystolic and diastolic diameters were performed for calcu-lation of the stiffness and distensibility, as previouslydescribed.10 The blood pressure was measured
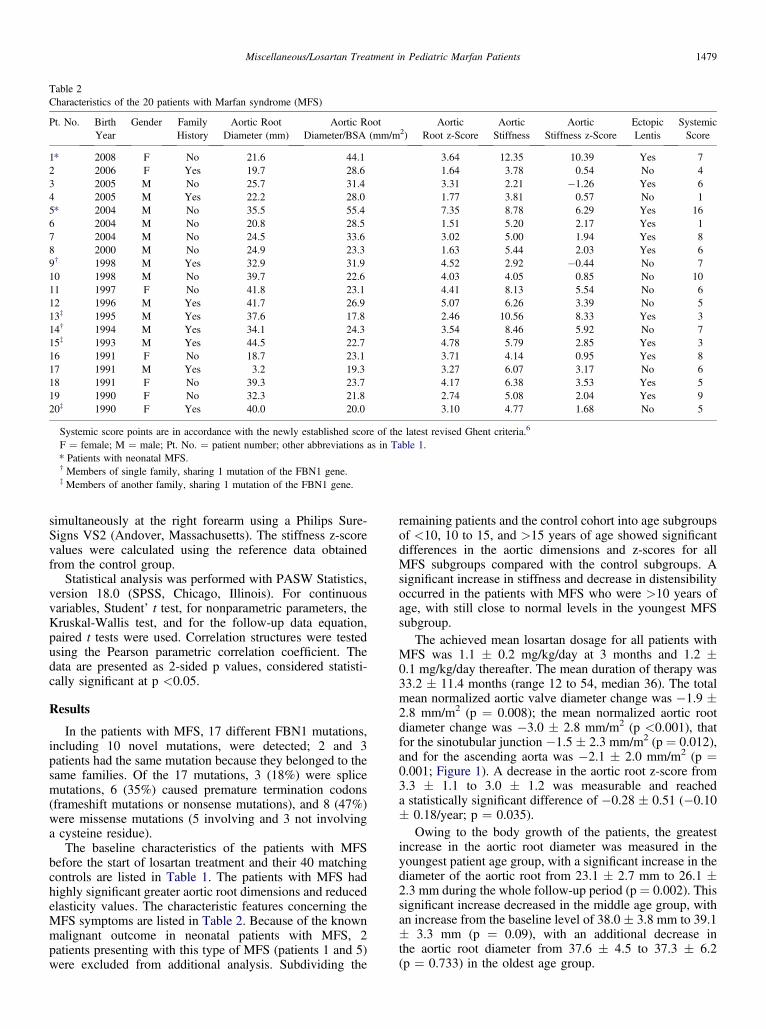
Table 2Characteristics of the 20 patients with Marfan syndrome (MFS)
Pt. No. BirthYear
Gender FamilyHistory
Aortic RootDiameter (mm)
Aortic RootDiameter/BSA (mm/m2)
AorticRoot z-Score
AorticStiffness
AorticStiffness z-Score
EctopicLentis
SystemicScore
1* 2008 F No 21.6 44.1 3.64 12.35 10.39 Yes 72 2006 F Yes 19.7 28.6 1.64 3.78 0.54 No 43 2005 M No 25.7 31.4 3.31 2.21 �1.26 Yes 64 2005 M Yes 22.2 28.0 1.77 3.81 0.57 No 15* 2004 M No 35.5 55.4 7.35 8.78 6.29 Yes 166 2004 M No 20.8 28.5 1.51 5.20 2.17 Yes 17 2004 M No 24.5 33.6 3.02 5.00 1.94 Yes 88 2000 M No 24.9 23.3 1.63 5.44 2.03 Yes 69† 1998 M Yes 32.9 31.9 4.52 2.92 �0.44 No 710 1998 M No 39.7 22.6 4.03 4.05 0.85 No 1011 1997 F No 41.8 23.1 4.41 8.13 5.54 No 612 1996 M Yes 41.7 26.9 5.07 6.26 3.39 No 513z 1995 M Yes 37.6 17.8 2.46 10.56 8.33 Yes 314† 1994 M Yes 34.1 24.3 3.54 8.46 5.92 No 715z 1993 M Yes 44.5 22.7 4.78 5.79 2.85 Yes 316 1991 F No 18.7 23.1 3.71 4.14 0.95 Yes 817 1991 M Yes 3.2 19.3 3.27 6.07 3.17 No 618 1991 F No 39.3 23.7 4.17 6.38 3.53 Yes 519 1990 F No 32.3 21.8 2.74 5.08 2.04 Yes 920z 1990 F Yes 40.0 20.0 3.10 4.77 1.68 No 5
Systemic score points are in accordance with the newly established score of the latest revised Ghent criteria.6
F ¼ female; M ¼ male; Pt. No. ¼ patient number; other abbreviations as in Table 1.* Patients with neonatal MFS.† Members of single family, sharing 1 mutation of the FBN1 gene.z Members of another family, sharing 1 mutation of the FBN1 gene.
Miscellaneous/Losartan Treatment in Pediatric Marfan Patients 1479
simultaneously at the right forearm using a Philips Sure-Signs VS2 (Andover, Massachusetts). The stiffness z-scorevalues were calculated using the reference data obtainedfrom the control group.
Statistical analysis was performed with PASW Statistics,version 18.0 (SPSS, Chicago, Illinois). For continuousvariables, Student’ t test, for nonparametric parameters, theKruskal-Wallis test, and for the follow-up data equation,paired t tests were used. Correlation structures were testedusing the Pearson parametric correlation coefficient. Thedata are presented as 2-sided p values, considered statisti-cally significant at p <0.05.
Results
In the patients with MFS, 17 different FBN1 mutations,including 10 novel mutations, were detected; 2 and 3patients had the same mutation because they belonged to thesame families. Of the 17 mutations, 3 (18%) were splicemutations, 6 (35%) caused premature termination codons(frameshift mutations or nonsense mutations), and 8 (47%)were missense mutations (5 involving and 3 not involvinga cysteine residue).
The baseline characteristics of the patients with MFSbefore the start of losartan treatment and their 40 matchingcontrols are listed in Table 1. The patients with MFS hadhighly significant greater aortic root dimensions and reducedelasticity values. The characteristic features concerning theMFS symptoms are listed in Table 2. Because of the knownmalignant outcome in neonatal patients with MFS, 2patients presenting with this type of MFS (patients 1 and 5)were excluded from additional analysis. Subdividing the
remaining patients and the control cohort into age subgroupsof <10, 10 to 15, and >15 years of age showed significantdifferences in the aortic dimensions and z-scores for allMFS subgroups compared with the control subgroups. Asignificant increase in stiffness and decrease in distensibilityoccurred in the patients with MFS who were >10 years ofage, with still close to normal levels in the youngest MFSsubgroup.
The achieved mean losartan dosage for all patients withMFS was 1.1 � 0.2 mg/kg/day at 3 months and 1.2 �0.1 mg/kg/day thereafter. The mean duration of therapy was33.2 � 11.4 months (range 12 to 54, median 36). The totalmean normalized aortic valve diameter change was �1.9 �2.8 mm/m2 (p ¼ 0.008); the mean normalized aortic rootdiameter change was �3.0 � 2.8 mm/m2 (p <0.001), thatfor the sinotubular junction �1.5 � 2.3 mm/m2 (p ¼ 0.012),and for the ascending aorta was �2.1 � 2.0 mm/m2 (p ¼0.001; Figure 1). A decrease in the aortic root z-score from3.3 � 1.1 to 3.0 � 1.2 was measurable and reacheda statistically significant difference of �0.28 � 0.51 (�0.10� 0.18/year; p ¼ 0.035).
Owing to the body growth of the patients, the greatestincrease in the aortic root diameter was measured in theyoungest patient age group, with a significant increase in thediameter of the aortic root from 23.1 � 2.7 mm to 26.1 �2.3 mm during the whole follow-up period (p ¼ 0.002). Thissignificant increase decreased in the middle age group, withan increase from the baseline level of 38.0 � 3.8 mm to 39.1� 3.3 mm (p ¼ 0.09), with an additional decrease inthe aortic root diameter from 37.6 � 4.5 to 37.3 � 6.2(p ¼ 0.733) in the oldest age group.
Figure 1. Decrease in the normalized 4 proximal aortic dimensions withlosartan therapy. Gray bar indicates before therapy; black bar, duringtherapy, with measurement at the latest follow-up visit.
1480 The American Journal of Cardiology (www.ajconline.org)
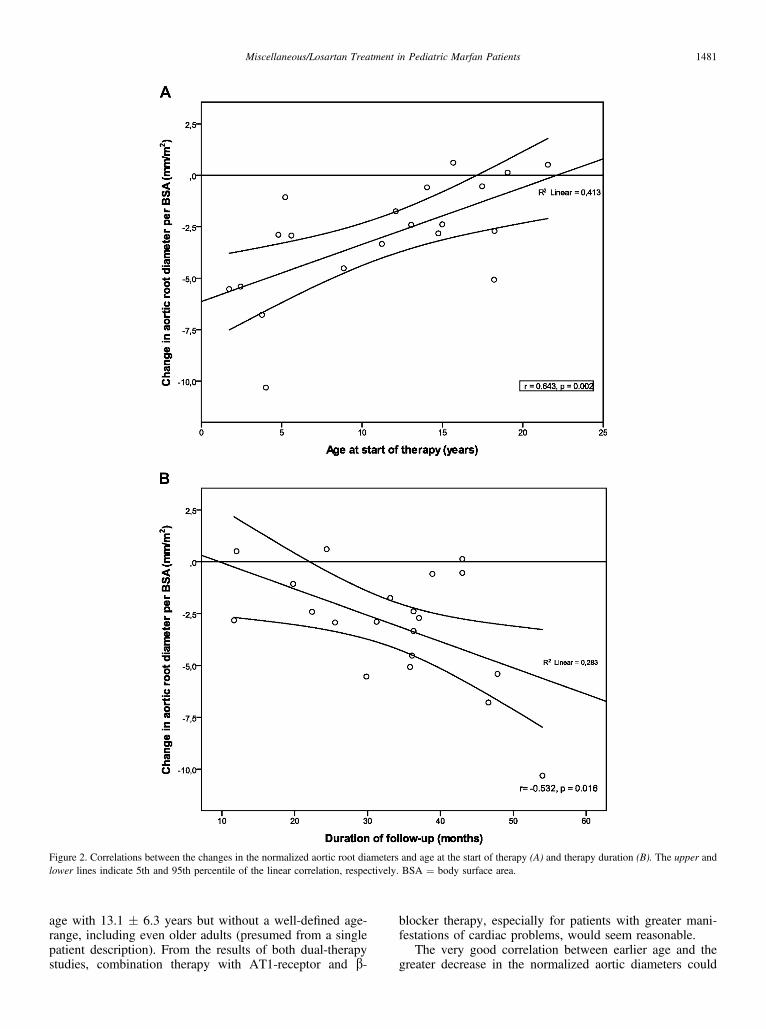
Comparing the different age subgroups with each other,the youngest age subgroup showed the greatest decrease inthe normalized aortic root values during follow-up. There-fore, a significant correlation between a younger age at thestart of therapy and a decrease in the normalized aortic rootdiameter was achieved (r ¼ 0.643, p ¼ 0.002; Figure 2). Asignificant correlation between the decrease in normalizedaortic root diameters and the length of follow-up was alsoverifiable (r ¼ �0.532, p ¼ 0.016; Figure 2).
No correlation was found between the presentation typesof MFS or the type or exon location of the mutation and thedecrease in the normalized aortic root diameter or z-score.
Regarding the elasticity investigation, the mean stiffnessz-score before the start of therapy for the patients with MFSwas 5.53 � 2.27 (z-score 2.46 � 2.35) vs 4.54 � 1.27 (z-score 1.55 � 1.76) at the latest follow-up visit. However, nostatistically significance was found (p ¼ 0.162 and p ¼0.193, respectively). We therefore subanalyzed the patientdata for the predefined different age groups of the patientswith MFS. These analyses revealed a stiffness value of 4.33� 1.34 (z-score 1.07 � 2.00) in the youngest age subgroupat baseline, showing elasticity levels still close to normal inthe youngest patients with MFS, with no statisticallysignificant differences to the matching cohort subgroup. Inthe older age subgroups, significant deterioration of theelasticity indexes was found in the patients with MFScompared with the matching healthy cohort. Because of thesmall subgroup size (n ¼ 6 in each group), no statisticallysignificant differences between the beginning and end of
therapy were noted; however, a tendency was seen towardimproved elasticity through medical therapy for mostpatients, with decreased stiffness in 73%.
No correlation between a decrease in the aortic root z-score and a decrease in stiffness was detectable (r ¼ 0.165,p ¼ 0.574). Also, no correlation was found between stiff-ness and mutation location, type of mutation, patient age atthe start of therapy, or therapy duration.
The body mass index increased from a mean value of16.0 kg/m2 to 17.4 kg/m2, with better weight gain regardinga lower height velocity increase. However, a significantreduction in the height percentiles or z-scores was notfound.
No patient presented with adverse events, and nosignificant changes in the blood pressure levels occurred.Two withdrawals from losartan treatment occurred duringthe first 6 months because of noncompliance, and thesepatients were not listed in the present study populationbecause they did not fulfill the inclusion criteria. Nodissection of the aorta occurred; in 2 patients, preventivevalve-sparing root replacement (David procedure) was per-formed after 20 and 24 months of losartan therapy,respectively. Of these 2 patients, 1 had neonatal MFS.
Discussion
The present prospective study is the first to showa significant improvement in aortic dilatation by a decreaseof all 4 examined proximal adjusted aortic diameters withlosartan monotherapy in an unselected cohort of pediatricpatients with MFS. The decrease in the normalized aorticroot diameters by adjustment to the body surface area withlosartan therapy was much more pronounced, just aspostulated in an earlier study by Baumgartner et al11 with b-blocker therapy. However, compared with the previousstudy by Brooke et al,5 which published the first studyresults of AT1-antagonism therapy combined with b-blocker therapy in young patients highly affected by MFS,the decrease in the z-score values in our study was not asprominent. Thus, a significant reduction in the aortic z-scorewas seen in 14 of 18 of our patients. The most importantdifferences between these 2 studies, in addition to thetherapy strategies, were the greater manifestation of cardiacproblems in the cohort of Brooke et al,5 with a mean aorticz-score nearly twice as great as that in our children (7.21 �2.69 vs 3.48 � 1.41), and a significantly lower mean age oftheir patients at therapy initiation (mean 6.5 years, range14 months to 16 years; vs 11.3 years, range 20 months to22 years). Therefore, younger age and early preventivetherapeutic medical intervention in patients with MFSshould be considered relevant factors of influence, becausewe could verify a significant correlation between an earlierage at the start of therapy and a greater decrease in thenormalized aortic root diameter. Recently, another therapystudy of pediatric patients with MFS was published by Chiuet al.12 Again, combined therapy with losartan andb blockers was compared with b-blocker monotherapy.They found a significant reduction in the annual dilation ratewith the dual-therapy strategy, but with b-blocker mono-therapy, an increase in the aortic root occurred.12 Theirpatient cohort included affected patients of a similar mean
Figure 2. Correlations between the changes in the normalized aortic root diameters and age at the start of therapy (A) and therapy duration (B). The upper andlower lines indicate 5th and 95th percentile of the linear correlation, respectively. BSA ¼ body surface area.
Miscellaneous/Losartan Treatment in Pediatric Marfan Patients 1481
age with 13.1 � 6.3 years but without a well-defined age-range, including even older adults (presumed from a singlepatient description). From the results of both dual-therapystudies, combination therapy with AT1-receptor and b-
blocker therapy, especially for patients with greater mani-festations of cardiac problems, would seem reasonable.
The very good correlation between earlier age and thegreater decrease in the normalized aortic diameters could
1482 The American Journal of Cardiology (www.ajconline.org)
have been an expression of somatic growth, by which thedecrease in the excessive aortic root dilatation with therapyhad a stronger effect on the normalized diameter by thesimultaneous increase in the body surface area. However,we also demonstrated persistent normal aortic wall elasticityduring the first 10 years of life, despite already minor tosignificant dilatation of the aortic root. These normal elas-ticity levels were retained with therapy. Likewise, Baum-gartner et al11 reported only mild alterations in aorticelasticity in their youngest patients, with a mean age of9.7 years. However, their youngest patients also hadsignificant aortic root dilation.11 An explanation could bethat TGF-b elevation owing to fibrillin-1 mutation primarilyleads to excessive aortic growth13 but that aortic walldegeneration through upregulation of collagen synthesiscausing aortic wall fibrosis,14 measurable by the elasticityindexes, occurs later in life. The interdependence of bothparameters could not be proved by our data, neither from thebaseline measurements, showing a dilated, but still normal,elastic aortic wall in the youngest age group, nor from theimprovement in the normalized aortic diameters with los-artan therapy but insignificant changes in the elasticitylevels. These results are in line with the data fromChiu et al.12
The stiffness measurement of the aortic wall is anupcoming tool for the evaluation of the aortic wall texture.Hirata et al15 stated that the stiffness and distensibilityindicate the intrinsic elastic properties of the aorta, ratherthan its diameter. Also, deteriorated elasticity values are notspecific findings for MFS. We recently reported similarlevels of aortic stiffness in children with bicuspid aorticvalves with a similar increase after 10 years of age, even inthose with noncompromised aortic valve function.10 Stiff-ness is known to be an independent risk factor for cardiacproblems, including aortic dilatation in adults.16 However,aortic dissection has also been seen in nondilated aortas.17
Therefore, the decrease in aortic root dimensions with los-artan therapy is a promising and important finding in theyoung patients with MFS, but restitution of the deterioratedelasticity indexes would be a better indication of therecovery of the aortic wall with therapy than the diameterdecrease alone.
Our results were biased by the small patient number,a wide age range, a wide range of clinical symptoms atpresentation, and the noncontrolled and nonrandomizedcharacter of the study. An extended follow-up period forthese patients should allow us to determine whether thebeneficial effect on the aortic diameter decrease is consistentwith additional growth and to determine whether an age-dependent AT1-antagonism effect is present on aortic wallelasticity. Despite the prospective nature of our study,additional, double-blind, multicenter trials have beenannounced and will add to the knowledge of AT1-receptorblocker effects on aortic root dilatation and elasticity inpatients with MFS.18,19
Our study is the first to demonstrate the positive outcomeof losartan monotherapy in a nonselected pediatric groupwith MFS. The normalized aortic dimensions weredecreased with therapy, with significantly better resultsachieved with an earlier start to therapy. However,remarkably, no statistically significant improvement in the
aortic wall elasticity was verifiable, although the normalelasticity levels in the youngest patients were maintainedduring therapy. Therefore, the results of the present studyhave added insight regarding the beneficial effect of losartanas monotherapy, even in mild to moderate cases, in additionto the reported results in severely affected children andadolescents.
Acknowledgment: We are grateful for the editorial assis-tance by Lisa Lennkh.
Disclosures
The authors have no conflicts of interest to disclose.
1. Dietz HC, Cutting GR, Pyeritz RE, Maslen CL, Sakai LY, Corson CM,Puffenberger EG, Hamosh A, Nanthakumar EJ, Curristin SM, StettenG, Meyers DA, Francamano CA. Marfan syndrome caused by recurrentde novo missense mutation in the fibrillin gene. Nature 1991;352:337e339.
2. Gelb BD. Marfan’s syndrome and related disorders—moretightly connected than we thought. N Engl J Med 2006;355:841e844.
3. Neptune ER, Frischmeyer PA, Arking DE, Myers L, Bunton TE,Gayraud B, Ramirez F, Sakai LY, Dietz HC. Dysregulation of TGF-beta activation contributes to pathogenesis in Marfan syndrome. NatGenet 2003;33:407e411.
4. Habashi JP, Judge DP, Holm TM, Cohn RD, Loeys BL, Cooper TK,Myers L, Klein EC, Liu G, Calvi C, Podowski M, Neptune ER,Halushka MK, Bedja D, Gabrielson K, Rifkin DB, Carta L, Ramirez F,Huso DL, Dietz HC. Losartan, an AT1 antagonist, prevents aorticaneurysm in a mouse model of Marfan syndrome. Science 2006;312:117e121.
5. Brooke BS, Habashi JP, Judge DP, Patel N, Loeys B, Dietz HC III.Angiotensin II blockade and aortic-root dilation in Marfan’s syndrome.N Engl J Med 2008;358:2787e2795.
6. Loeys BL, Dietz HC, Braverman AC, Callewaert BL, De Backer J,Devereux RB, Hilhorst-Hofstee Y, Jondeau G, Faivre L, Milewicz DM,Pyeritz RE, Sponseller PD, Wordsworth P, De Paepe AM. The revisedGhent nosology for the Marfan syndrome. J Med Genet 2010;47:476e485.
7. De Paepe AM, Devereux BB, Dietz HC, Hennekam RC, Pyeritz RE.Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet1996;62:417e426.
8. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure forextracting DNA from human nucleated cells. Nucl Acids Res 1988;16:1215.
9. Warren AE, Boyd ML, O’Connell C, Dodds L. Dilation of theascending aorta in paediatric patients with bicuspid aortic valve:frequency, rate of progression and risk factors. Heart 2006;92:1496e1500.
10. Pees C, Michel-Behnke I. Morphology of the bicuspid aortic valve andelasticity of the adjacent aorta in children. Am J Cardiol 2012;110:1354e1360.
11. Baumgartner D, Baumgartner C, Schermer E, Engl G, Schweigmann U,Mátyás G, Steinmann B, Stein JI. Different patterns of aortic wall elas-ticity in patients with Marfan syndrome: a noninvasive follow-up study.J Thorac Cardiovasc Surg 2006;132:811e819.
12. Chiu HH, Wu MH, Wang JK, Lu CW, Chiu SN, Chen CA, Lin MT,Hu FC. Losartan added to b-blockade therapy for aortic root dilation inMarfan syndrome: a randomized, open-label pilot study. Mayo ClinProc 2013;88:271e276.
13. Faivre L, Collod-Beroud G, Callewaert B, Child A, Binquet C, GautierE, Loeys BL, Arbustini E, Mayer K, Arslan-Kirchner M, Stheneur C,Kiotsekoglou A, Comeglio P, Marziliano N, Wolf JE, Bouchot O,Khau-Van-Kien P, Adès L, De Backer J, Coucke P, Francke U,De Paepe A, Jondeau G, Boileau C. Clinical and mutation-type anal-ysis from an international series of 198 probands with a pathogenicFBN1 exons 24-32 mutation. Eur J Hum Genet 2009;17:491e501.
Miscellaneous/Losartan Treatment in Pediatric Marfan Patients 1483
14. Williams A, Davies S, Stuart AG, Wilson DG, Fraser AG. Medicaltreatment of Marfan syndrome: a time for change. Heart 2008;94:414e421.
15. Hirata K, Triposkiadis F, Sparks E, Bowen J, Wooley CF, BoudoulasH. The Marfan syndrome: abnormal aortic elastic properties. J Am CollCardiol 1991;18:57e63.
16. Nollen GJ, Groenink M, Tijssen JG, Van Der Wall EE, Mulder BJ.Aortic stiffness and diameter predict progressive aortic dilatation inpatients with Marfan syndrome. Eur Heart J 2004;25:1146e1152.
17. Gott VL, Greene PS, Alejo DE, Cameron DE, Naftel DC, Miller DC,Gillinov AM, Laschinger JC, Pyeritz RE. Replacement of the aortic rootin patients with Marfan syndrome.N Engl J Med 1999;340:1307e1313.
18. Detaint D, Aegerter P, Tubach F, Hoffman I, Plauchu H, DulacY, Faivre LO, Delrue MA, Collignon P, Odent S, TchitchinadzeM, Bouffard C, Arnoult F, Gautier M, Boileau C, Jondeau G.Rationale and design of a randomized clinical trial (Marfan Sar-tan) of angiotensin II receptor blocker therapy versus placebo inindividuals with Marfan syndrome. Arch Cardiovasc Dis2010;103:317e325.
19. Möberg K, De Nobele S, Devos D, Goetghebeur E, Segers P, TrachetB, Vervaet C, Renard M, Coucke P, Loeys B, De Paepe A, De BackerJ. The Ghent Marfan Trial—a randomized, double-blind placebocontrolled trial with losartan in Marfan patients treated with b-blockers.Int J Cardiol 2012;157:354e358.