50
Value Stream Mapping
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | jason-ryan |
| View: | 216 times |
| Download: | 1 times |
Value Stream Mapping
Aims for session
• Introduce the concept of Value Stream Mapping
• Consider identification of value and waste
Patient Flow Process
1. Understand the total process of care delivery – patient pathway
Diagnostic
tests

COMPASS WAITING LIST DIARY - CASE NOTES PULLED 3 WEEKS IN ADVANCE
THEATRE LIST PRINTED L4 HOURS BEFORE - ALLOCATE BEDS
THEATRE LIST SAME DAY FROM JANET. TRY 24 HOURS BEFORE
REPORTS ADMISSION AT FRONT RECEPTION.DETAILS CHECKED
PATIENT ARRIVES RECEPTION DAY SURGERY
TAKE PATIENT TO WARD AND TO BED AREA WITH NOTES. ADVICE TO UNDRESS/GOWN ON. TELL NURSING STAFF.
RECEPTIONIST FINDS OUT IF THEY TO GO TO RADIOLOGY AND WHAT TIME 1 WEEK IN ADVANCE
ADMIT PATIENT VIA CARE PLAN. 5-10 MIN.LOOK AT MOD
CHECK IF TO GO FOR ULTRASOUND - IF TO GO WALK THEM ROUND TO X-RAY WAITING ROOM.
1ST KUB - KID URETER BLADDER X-RAY. PATIENT FULL BLADDER.2ND ULTRASOUND 20-30 MINS IN RADIOLOGY.
PATIENT X-RAY AND ULTRASOUND REPORT BACK - BACK TO BED.
DOCTOR SPEAKS TO PATIENTS - CONSENT SIGNED
THEATRE STAFF ATTEND DAY SURGERY - DATA SHEET GIVEN TO DAY SURGERY STAFF.
THEATRE STAFF TAKE PATIENT STRAIGHT INTO MINOR OP THEATRE.
TEST 10-15 MIN ALLOCATION
DR CANNING 3 1/2 HOUR SESSION
VERBAL REPORT TO PATIENT AND INFORMATION.
TAKEN BACK TO DAY SURGERY
MAKE SURE PATIENT OK - ? DRINK OR EAT. DISCHARGE INSTRUCTIONS
IF DOCTOR NEEDS TO SEE- APPOINTMENT MADE STRAIGHT AWAY - GIVEN TO PATIENT
FOLLOW/REVIEW AT OUTPATIENTS VOL APPOINTMENT NEXT DAY. INDICATED ON CARE PATHWAY
IF RAH DR WILL INDICATE ON TAPE - SECRETARY WILL ARRANGE.
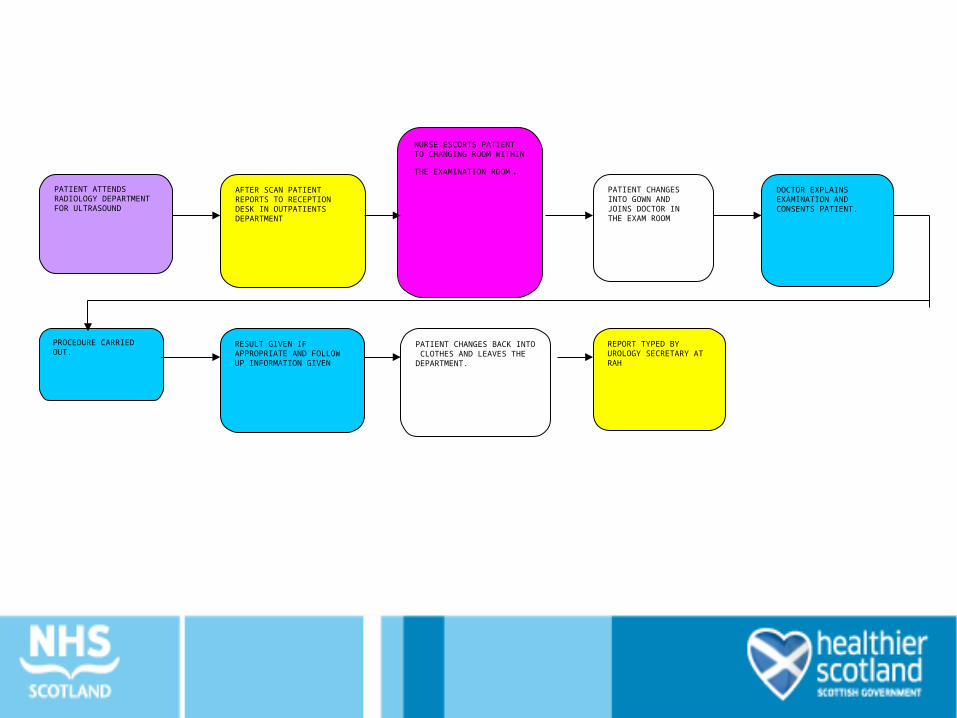
PATIENT ATTENDS RADIOLOGY DEPARTMENT FOR ULTRASOUND
AFTER SCAN PATIENT REPORTS TO RECEPTION DESK IN OUTPATIENTS DEPARTMENT
NURSE ESCORTS PATIENT TO CHANGING ROOM WITHIN THE EXAMINATION
ROOM.PATIENT CHANGES INTO GOWN AND JOINS DOCTOR IN THE EXAM ROOM
DOCTOR EXPLAINS EXAMINATION AND CONSENTS PATIENT.
PROCEDURE CARRIED OUT.
RESULT GIVEN IF APPROPRIATE AND FOLLOW UP INFORMATION GIVEN
PATIENT CHANGES BACK INTO CLOTHES AND LEAVES THE DEPARTMENT.
REPORT TYPED BY UROLOGY SECRETARY AT RAH
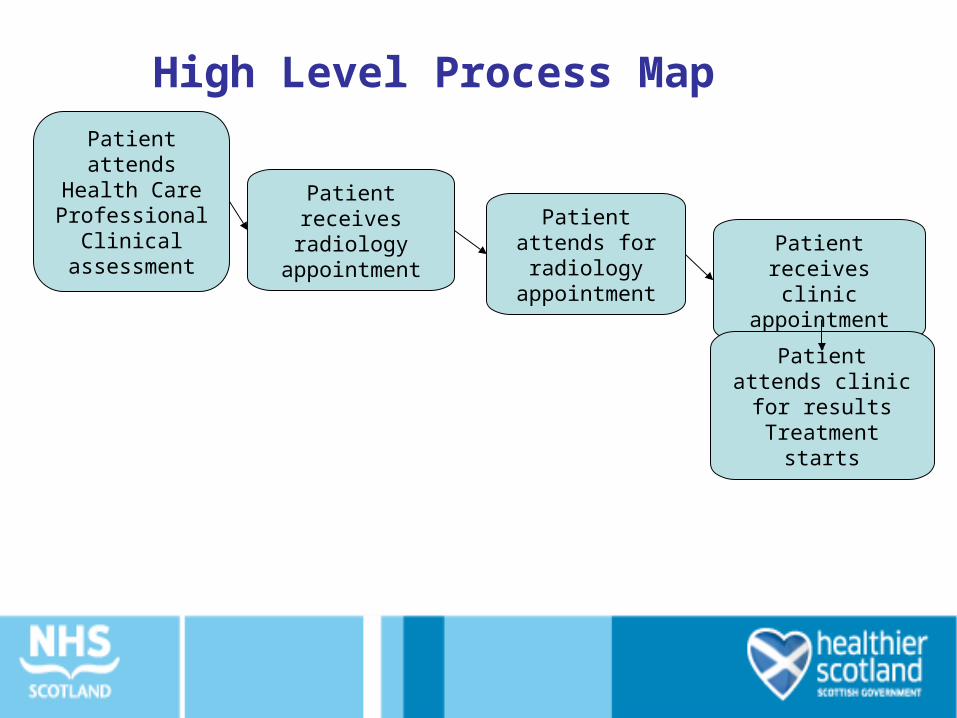
Patient attends Health
Care Professional
Clinical assessment
Patient receives radiology
appointmentPatient attends
for radiology appointment
Patient receives clinic
appointment
Patient attends clinic for results Treatment starts
High Level Process Map
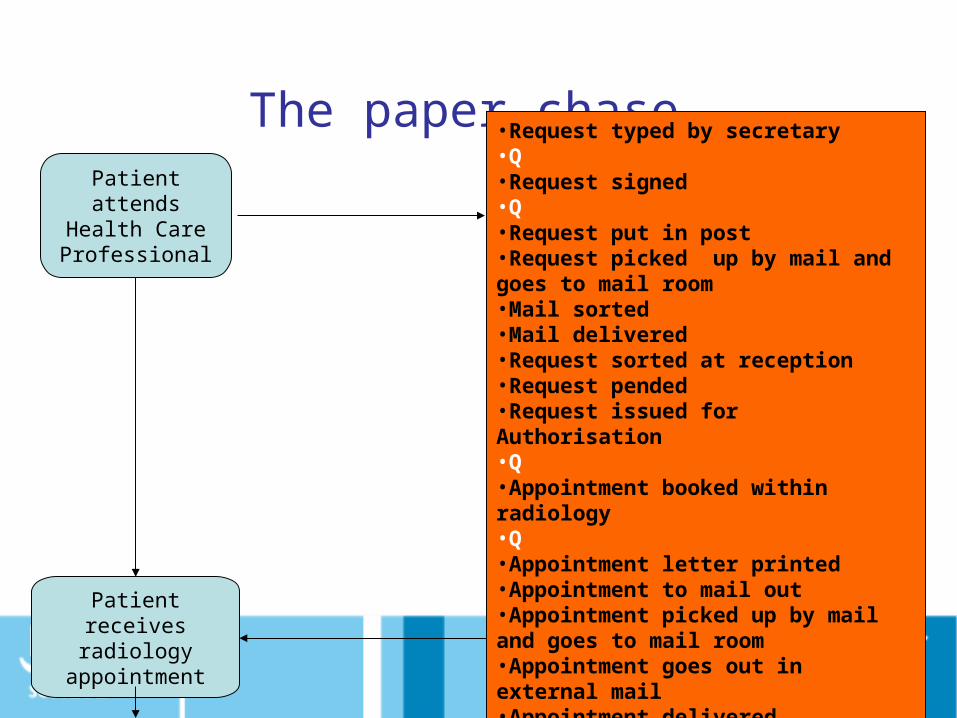
The paper chase
Patient attends Health Care Professional
Patient receives radiology
appointment
•Request typed by secretary•Q•Request signed•Q•Request put in post•Request picked up by mail and goes to mail room•Mail sorted•Mail delivered•Request sorted at reception•Request pended•Request issued for Authorisation•Q•Appointment booked within radiology•Q•Appointment letter printed•Appointment to mail out•Appointment picked up by mail and goes to mail room•Appointment goes out in external mail•Appointment delivered
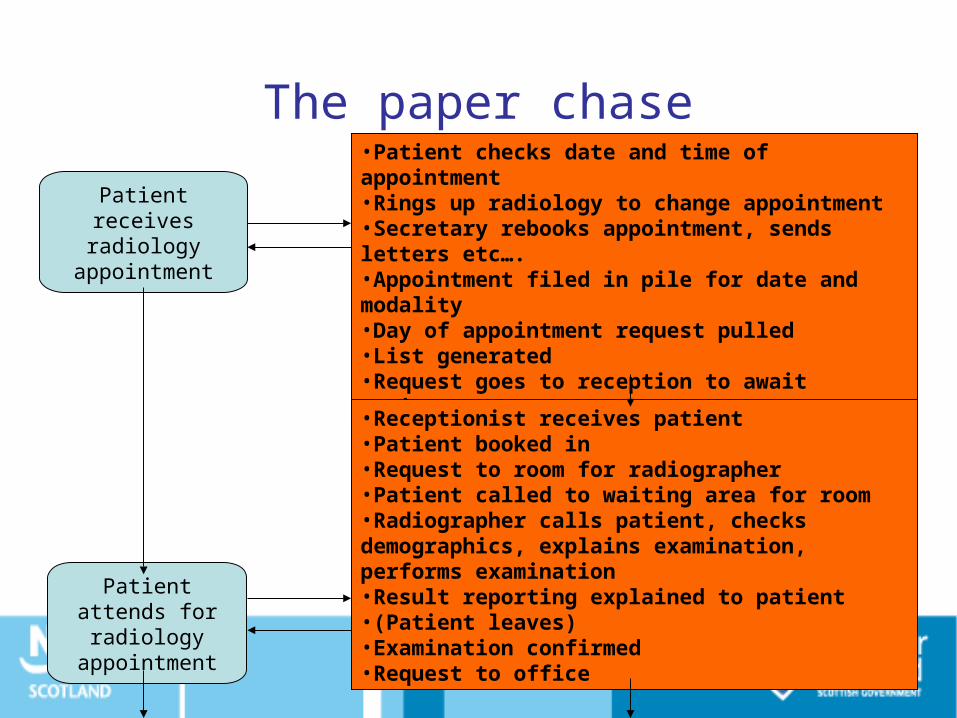
The paper chase
Patient attends for radiology appointment
Patient receives radiology
appointment
•Patient checks date and time of appointment•Rings up radiology to change appointment•Secretary rebooks appointment, sends letters etc….•Appointment filed in pile for date and modality•Day of appointment request pulled •List generated•Request goes to reception to await patient•Receptionist receives patient•Patient booked in•Request to room for radiographer•Patient called to waiting area for room•Radiographer calls patient, checks demographics, explains examination, performs examination•Result reporting explained to patient•(Patient leaves)•Examination confirmed•Request to office
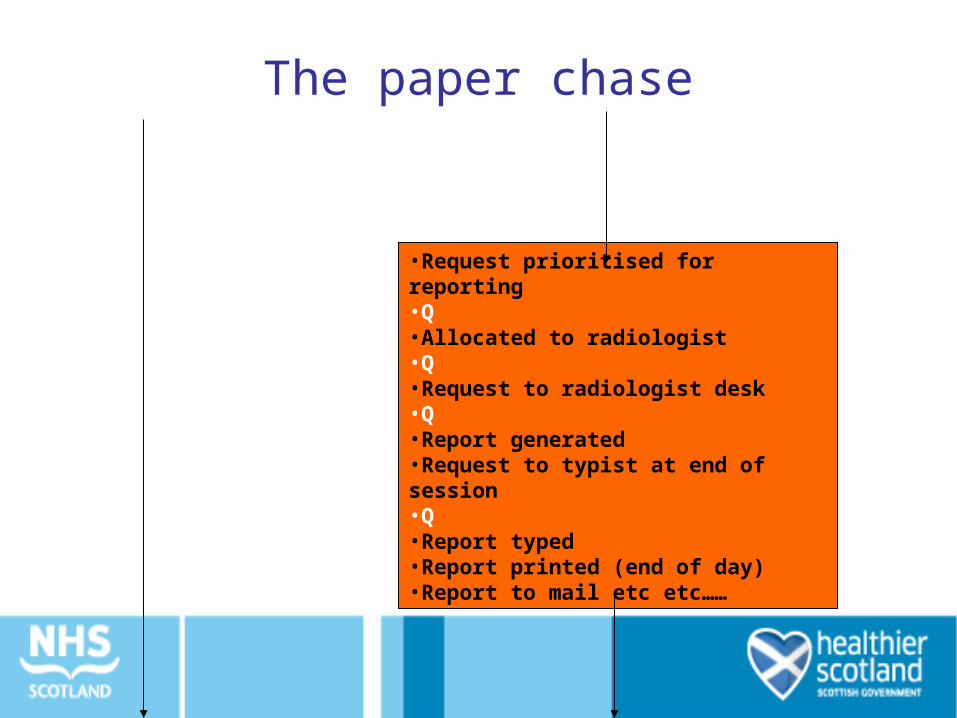
The paper chase
•Request prioritised for reporting•Q•Allocated to radiologist•Q•Request to radiologist desk•Q•Report generated•Request to typist at end of session•Q•Report typed•Report printed (end of day)•Report to mail etc etc……

The paper chase
•Report delivered to referrer•Matched with notes•Q•Read by referrer•To secretary for appointment•Q•OPD Appointment made, letters printed•Appointment sent out mail etc etc….•Q
Patient receives clinic
appointment
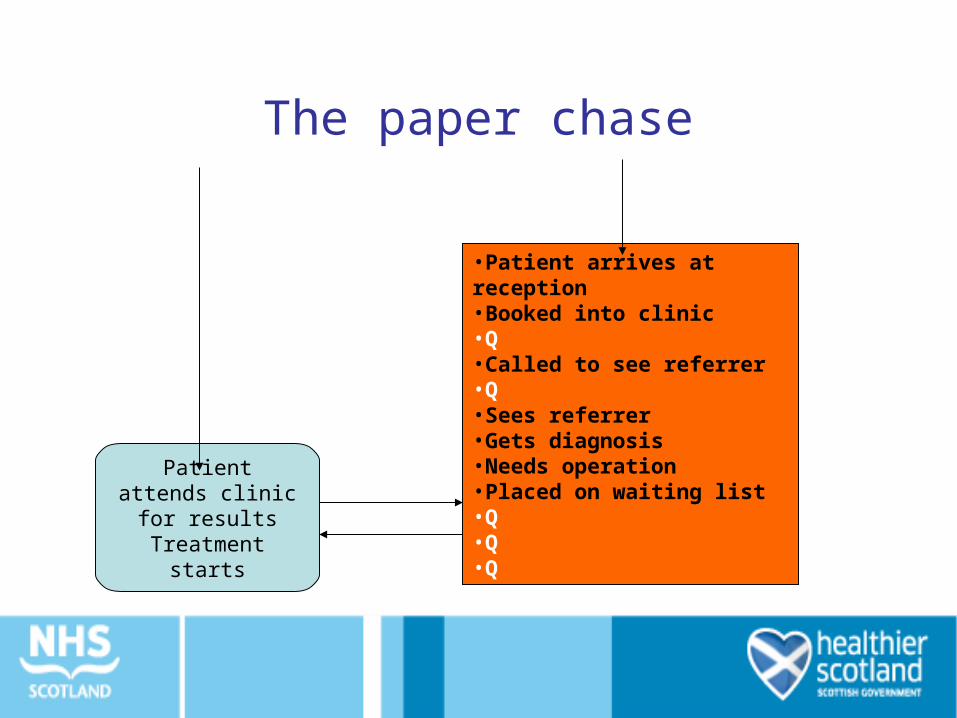
The paper chase
Patient attends clinic for results Treatment starts
•Patient arrives at reception•Booked into clinic•Q•Called to see referrer•Q•Sees referrer•Gets diagnosis•Needs operation•Placed on waiting list•Q•Q•Q

The patient journeyThe paper chase
The queues
5 steps in the patient journey
2 steps had clinical impact
35 process steps from referral to diagnosis
13 queues
•Referral to diagnosis
What is value?
• The activity is done right first time
• The activity transforms the patient and moves them towards the next defined outcome
• The activity is something that the patient cares about
•Have a look at the process map•Which steps add value for the patient?•How many are there?•Which steps are necessary but don’t add value?•How many are there?•How long does the whole process take?•How much time adds value for the patient?
Activity: Identifying Value
Who to Involve
• Small team 8-12 people, mixed disciplines
• Represent people at all the steps you will look at
• ‘Fresh eyes’
• Patients/ carers
• Nominate a team and clinical lead
What to Measure
Agree beforehand improvements in - Journey time for patients - Time spent on non value adding work - Throughput (productivity) - Morale / staff satisfaction
Observe and Gather Data
• Walk the patient journey - see the actual work place
• Follow and make notes about each component – What happens to the patient– What staff are doing– What the information / communication flow is
• Take photos of wastes

Measure the distance patients / staff have to travel
Track both the patient and information flows

Take the cameras on the walkabout, you’ll never convey this verbally!
What do patients actually experience and say about the process?

Ask staff at each step for their views on ‘show stoppers’, frustrations and positives
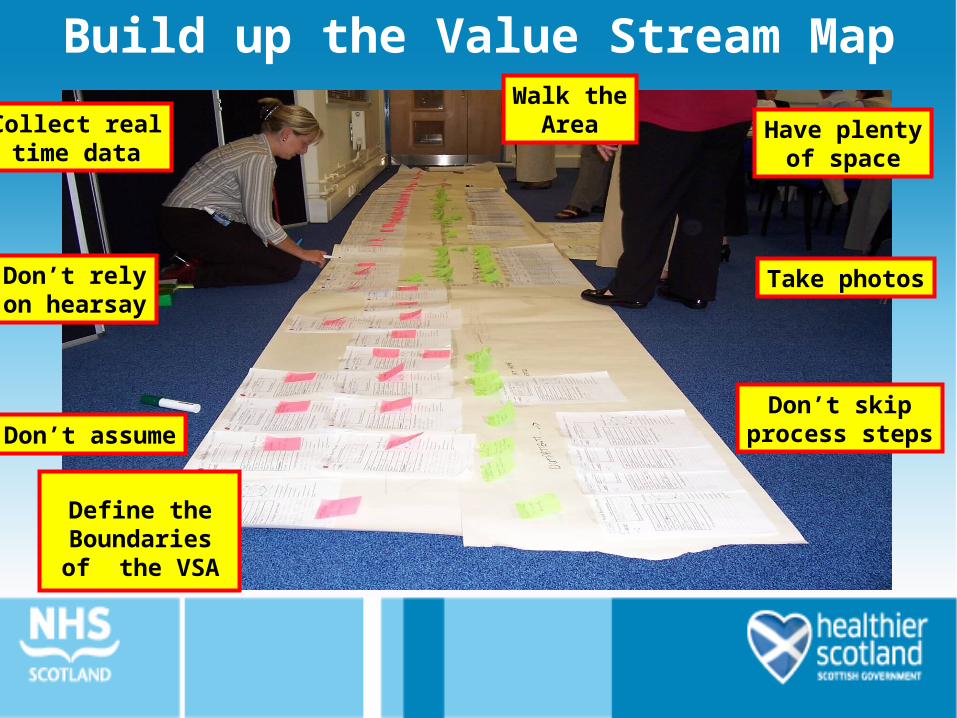
Take photos
Have plentyof space
Don’t skipprocess steps
Walk theArea
Define the Boundaries of the VSA
Don’t assume
Don’t relyon hearsay
Collect realtime data
Build up the Value Stream Map
Understanding your Current State Map:
• Add value
• Remove waste

Coffee
Lean Tools Overview
• PDSA
• Glenday Sieve
• Workplace Organisation
• Rapid Improvement Events

PDSA Cycle
The improvement guideLangley et al 1996

What change can we make that will result in an improvement ?
Act
• What changes are to be made?
• Next cycle?
Plan• Objective• Questions and predictions (why)• Plan to carry out the cycle (who, what, where, when)• Plan for data collection
Study• Complete the analysis of the data
•Compare data to predictions
•Summarize what was learned
Do• Carry out the plan• Document problems and unexpected observations• Begin analysis of the data
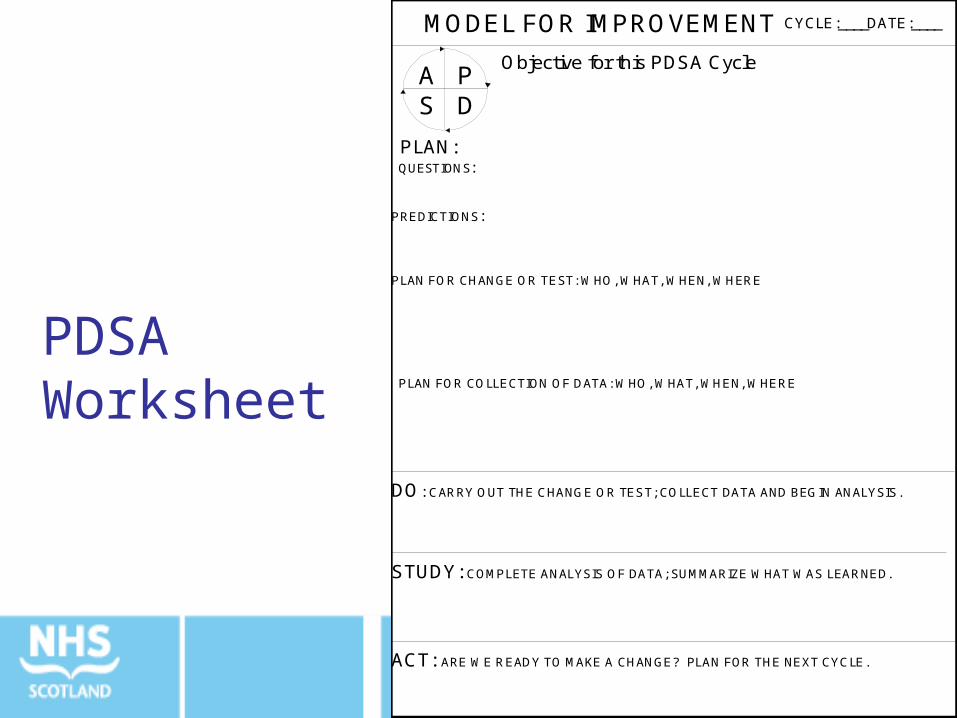
MODEL FOR IMPROVEMENT
Objective for this PDSA Cycle
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
DATE:____CYCLE:____
PLAN:QUESTIONS:
PREDICTIONS:
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE
PDS
A
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED.
ACT: ARE WE READY TO MAKE A CHANGE? PLAN FOR THE NEXT CYCLE.
PDSA Worksheet
Scottish Primary Care CollaborativeAyrshire GP Practice
0
2
4
6
8
10
12
14
16
Nu
mb
er
of
Da
ys
GP 3rd Available Appointment
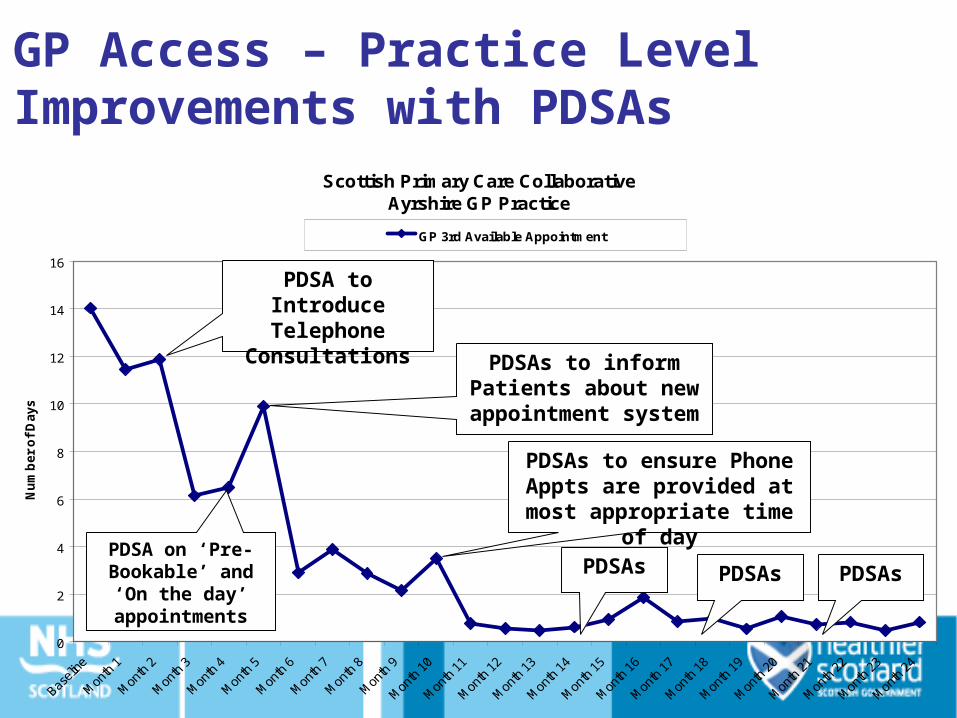
GP Access – Practice Level Improvements with PDSAs
PDSAs to inform Patients about new
appointment system
PDSA on ‘Pre-Bookable’ and ‘On
the day’ appointments
PDSA to Introduce Telephone
Consultations
PDSAs PDSAs PDSAs
PDSAs to ensure Phone Appts are provided at most
appropriate time of day
Scottish Primary Care CollaborativeBorders GP Practice
0
10
20
30
40
50
60
70
80
90
Baseli
ne
Mon
th 1
Mon
th 2
Mon
th 3
Mon
th 4
Mon
th 5
Mon
th 6
Mon
th 7
Mon
th 8
Mon
th 9
Mon
th 1
0
Mon
th 1
1
Mon
th 1
2
Mon
th 1
3
Mon
th 1
4
Mon
th 1
5
Mon
th 1
6
Mon
th 1
7
Mon
th 1
8
Mon
th 1
9
Mon
th 2
0
Mon
th 2
1
Mon
th 2
2
Mon
th 2
3
Mon
th 2
4
% o
f P
eop
le w
ith
Dia
bet
es
% of Diabetes Patients with a BP<140/80
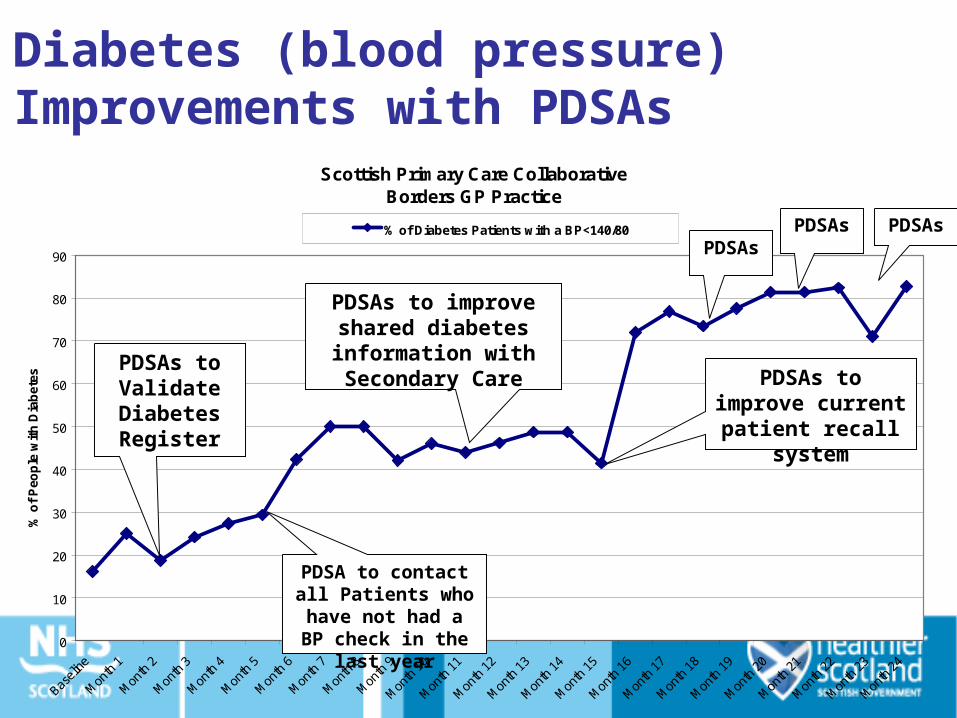
Diabetes (blood pressure) Improvements with PDSAs
PDSAs to improve shared diabetes information with Secondary Care
PDSA to contact all Patients who have not had a BP check
in the last year
PDSAsPDSAs PDSAs
PDSAs to improve current patient recall system
PDSAs to Validate Diabetes Register

Glenday Sieve
• Heard of the Pareto (80/20 principle)?
• Ladies – think of your wardrobe…..
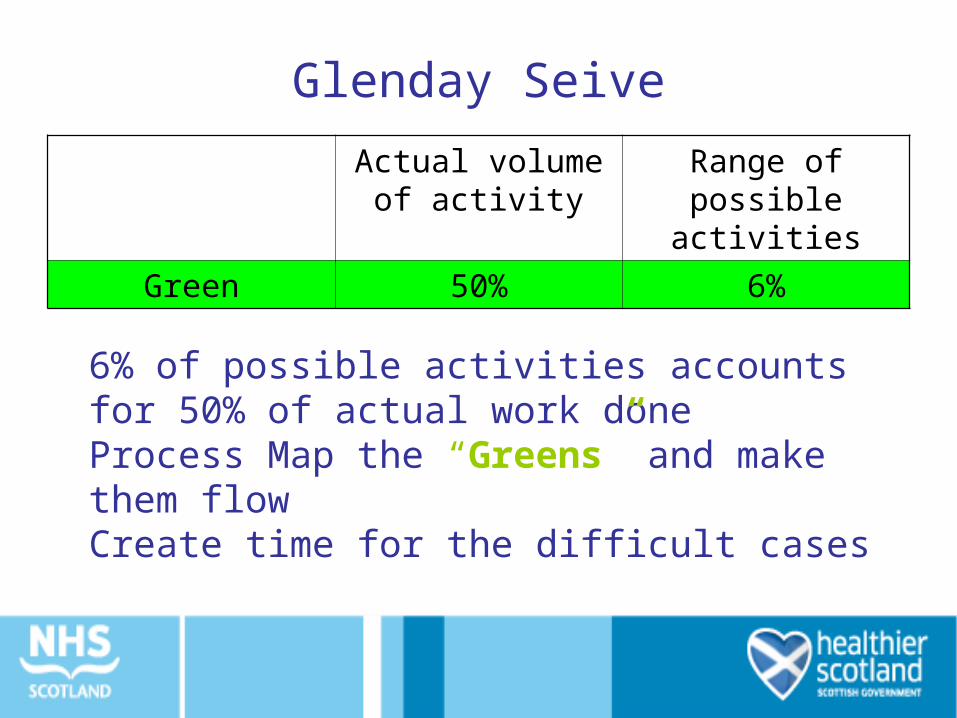
Glenday Seive
Actual volume of activity
Range of possible activities
Green 50% 6%
6% of possible activities accounts for 50% of actual work doneProcess Map the “Greens” and make them flowCreate time for the difficult cases
Glenday Sieve
• Orthopaedics – Hips and knees
• General Surgery – hernias and lap cholecystectomy
• District Nurse – wound care, medication
MRI Team, NHS Tayside
•220 codes for appointments MRI RIE - 63% of MRI throughput from 2.7% of - 63% of MRI throughput from 2.7% of procedure codesprocedure codes (i.e. 6 codes)
•Group patients by the process they go through (rather than clinical condition)
Surgery example
• 213 cases over 8 months at Clatterbridge.– 52% of theatre throughput from 4.2% of procedures
• Group patients by the process they go through (rather than clinical condition)
• Focus initially on smart process for the critical few [4.2%]

Workplace organisation
6S – A Technique to
• Promote workplace organisation
• Set and ensure adherence to standards
• Embed the spirit of continuous improvement
• Improve Quality, Cost Delivery, Safety and Morale
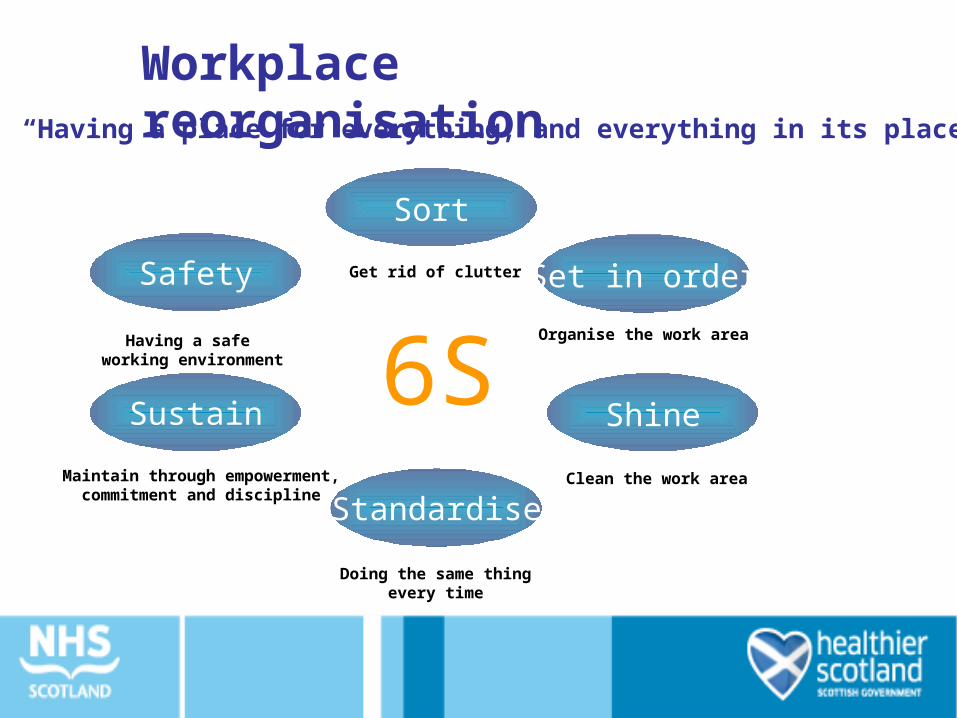
Sort
Get rid of clutter Set in order
Organise the work area
Shine
Clean the work area
Standardise
Doing the same thingevery time
Sustain
Maintain through empowerment,commitment and discipline
6SSafety
Having a safe working environment
“Having a place for everything, and everything in its place”
Workplace reorganisation

Characteristics of a 6S Workplace• Only have what is needed• Clean enough to “eat off the floor”• Everything is organised for the team• Obvious to everyone when something is out of order• Anything that is required can be retrieved within 30 seconds
– No surprise shortages of supplies – visual management of stock levels• Responsibilities defined and everyone taking their
responsibilities• Performance visible to all• Improvement ideas being routinely generated and implemented
Adapted from Ross International, RIE Training material
6S VisionTaken from Ross International, RIE Training
material
Adapted from Ross International, RIE Training material
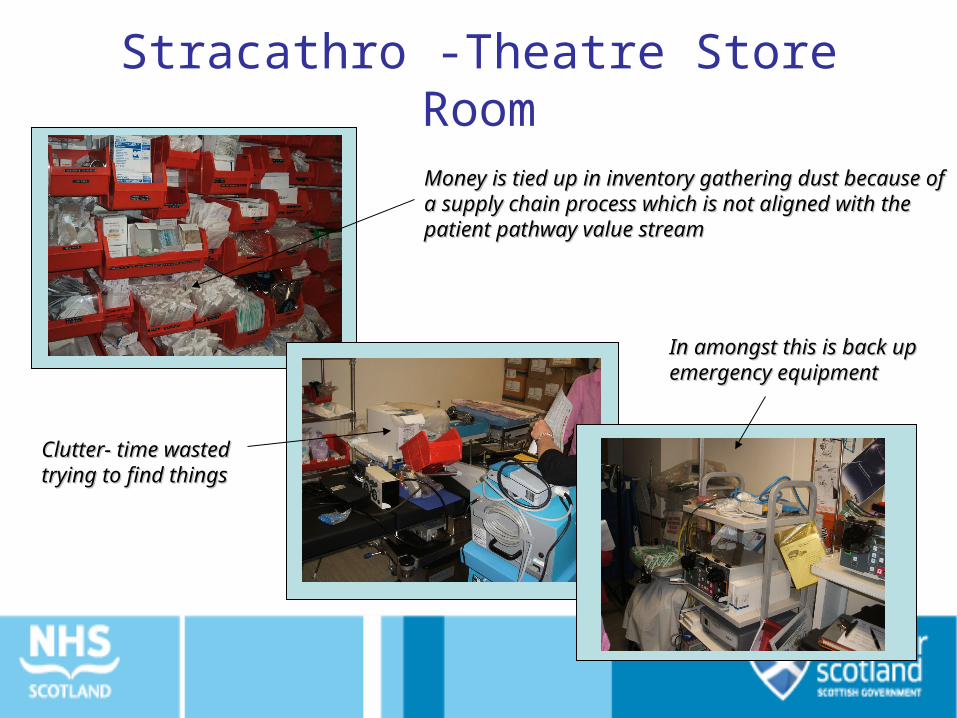
Money is tied up in inventory gathering dust because of Money is tied up in inventory gathering dust because of a supply chain process which is not aligned with the a supply chain process which is not aligned with the patient pathway value streampatient pathway value stream
In amongst this is back up In amongst this is back up emergency equipmentemergency equipment
Clutter- time wasted Clutter- time wasted trying to find thingstrying to find things
Stracathro -Theatre Store Room
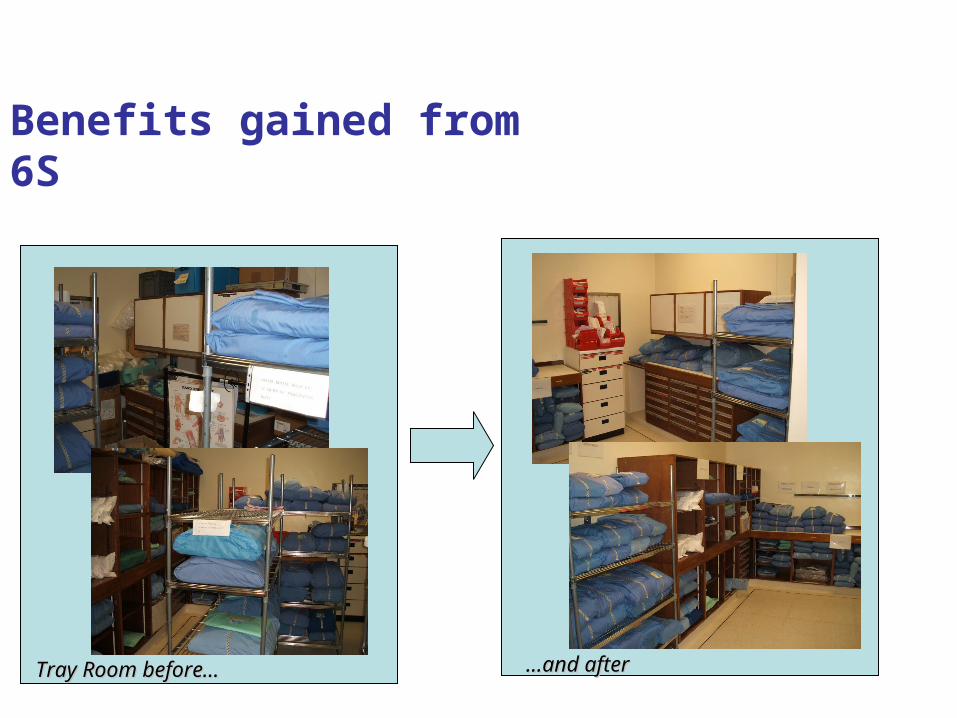
Benefits gained from 6S
Tray Room before…Tray Room before… ……and afterand after

6S Check Sheet Area
1 2 3 4 5Just beginning Focus on basics Make it visual Focus on consistency Focus on prevention
SORTSeparate the essential from
the non-essential
Necessary and unnecessary items are mixed throughout
the workplace
Necessary and unnecessary items
are separated
Unnecessary items have been removed from the
workplace.
A dependable, documented method (e.g.
red tagging) has been established to keep the
work area free of unnecessary items
Employees are continually seeking
improvement opportunities
SETA place for everything and
everything in its placeItems are randomly located throughout the workplace.
A designated location has been
established
Designated locations are marked to make
organisation more visible.
A dependable, documented method has
been established to recognise if items are out
of place or exceed quantity limits.
A dependable documented method has
been developed to provide continual evaluation, and a
process is in place to implement
improvements
1 2 3 4 5 Comments

Theatre Tray Room - 6S Score
0
1
2
3
4
5Sort
Set
Shine
Standardise
Sustain
Safety Score After 6S
Current Score
Rapid Improvement Events (RIEs) – an overview
What are RIEs?
•Common Lean tool to introduce Lean principles and thinking in organisations•RIEs select critical business areas and make real improvements for patients and staff•Process-focussed and brings together the team in a highly structured way•Results-focussed – establishing the root cause of problems, and achieving measurable improvements•Process which is action-orientated and data driven
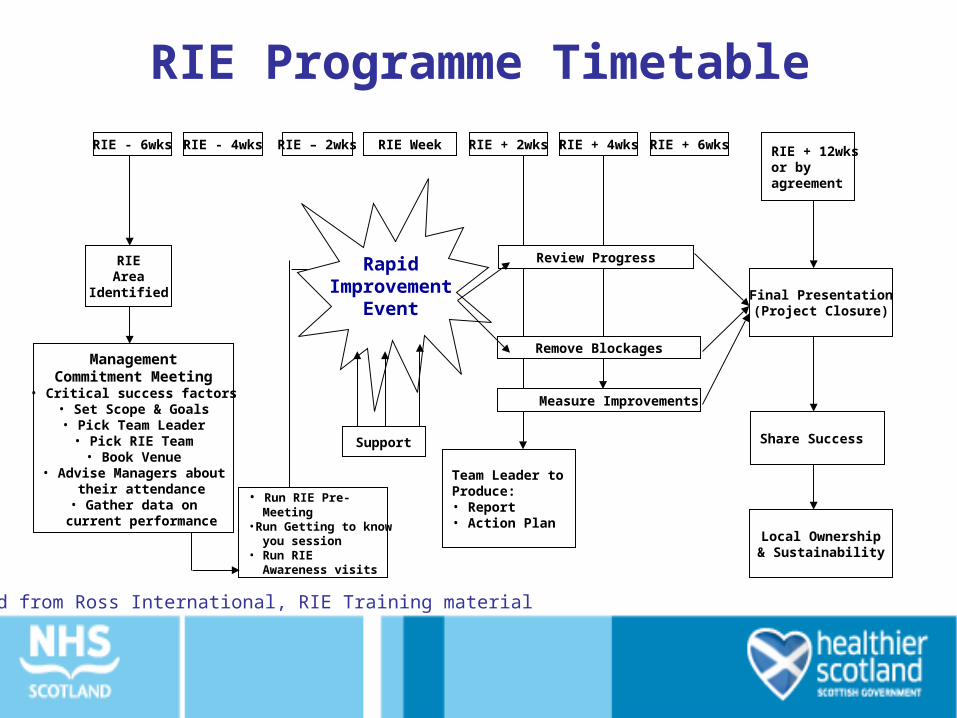
RIE Programme Timetable
RIE - 6wks RIE - 4wks RIE – 2wks RIE Week RIE + 2wks RIE + 4wks
Review Progress
RIE + 6wks RIE + 12wksor byagreement
Remove Blockages
Measure Improvements
Final Presentation(Project Closure)
Share Success
Local Ownership& Sustainability
Team Leader toProduce:• Report• Action Plan
Support
• Run RIE Pre- Meeting•Run Getting to know you session• Run RIE Awareness visits
ManagementCommitment Meeting• Critical success factors
• Set Scope & Goals• Pick Team Leader
• Pick RIE Team• Book Venue
• Advise Managers about their attendance• Gather data on
current performance
RIEArea
Identified
RapidImprovement
Event
Adapted from Ross International, RIE Training material
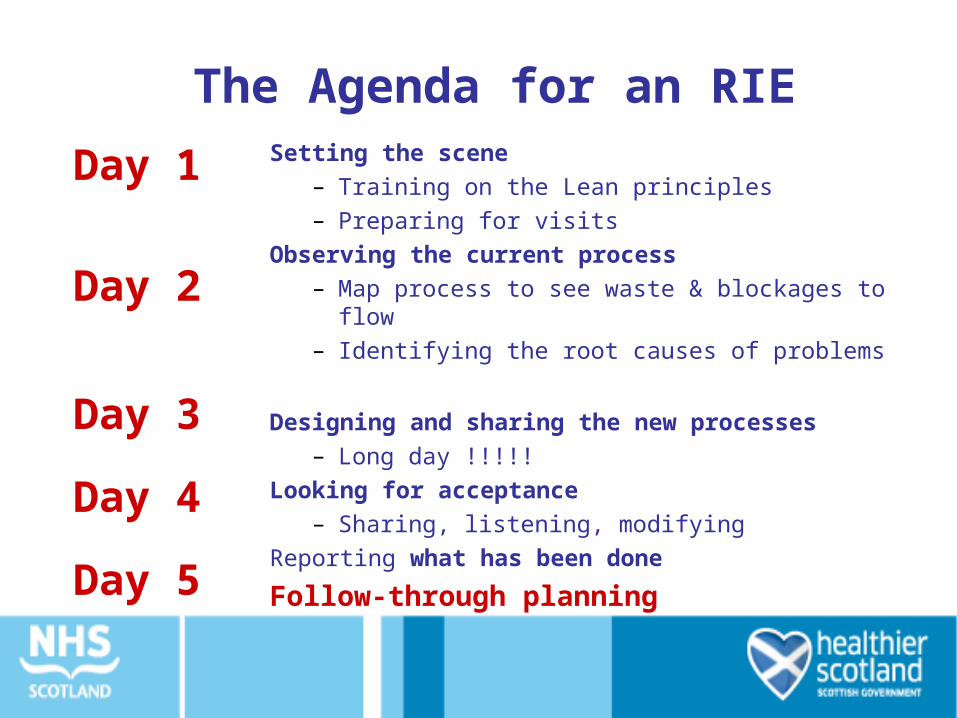
The Agenda for an RIESetting the scene
– Training on the Lean principles– Preparing for visits
Observing the current process– Map process to see waste & blockages to flow– Identifying the root causes of problems
Designing and sharing the new processes– Long day !!!!!
Looking for acceptance– Sharing, listening, modifying
Reporting what has been done
Follow-through planning
Day 1
Day 2
Day 3
Day 4
Day 5
One Team’s experience
NHS Tayside Urology RIE













