39
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | abdul-waris |
| View: | 142 times |
| Download: | 0 times |

Seminar-Vasculitis
Abdul Waris Khan

Definition
• Vasculitis is a histological term describing inflammation of the vessel wall.
• Characterized by widespread vasculitis leading to systemic symptoms and signs, generally requiring treatment with corticosteroids and/ or immunosuppressive drugs.
• Two main features are helpful in classifying these vasculitides:-– The size of the blood vessels involved
– The presence or absence of anti-neutrophil cytoplasmic antibodies (ANCA) in the blood
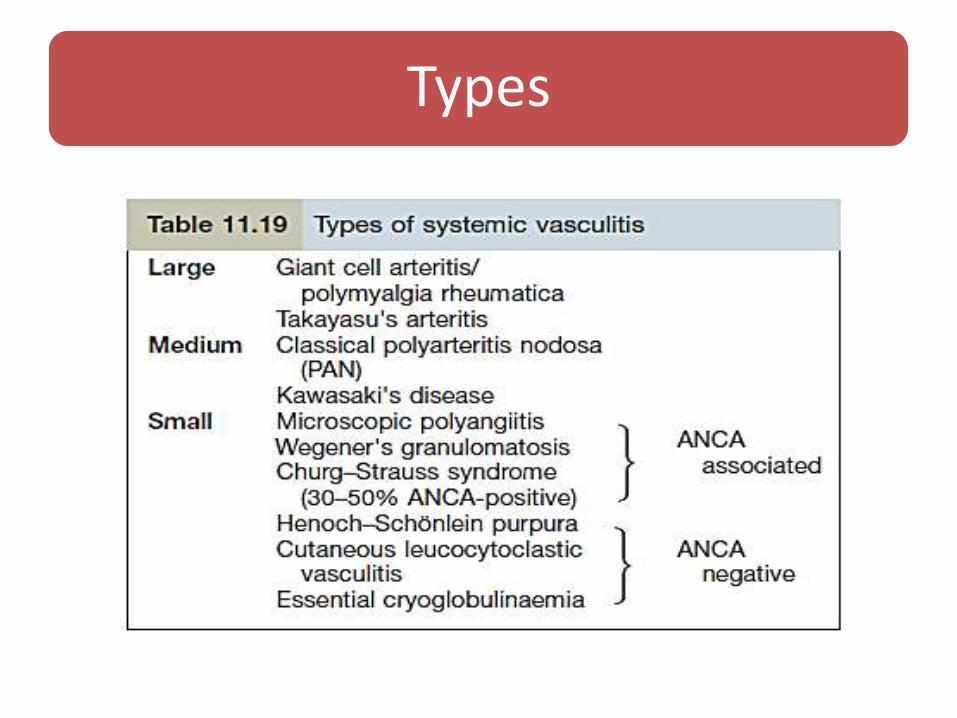
Types
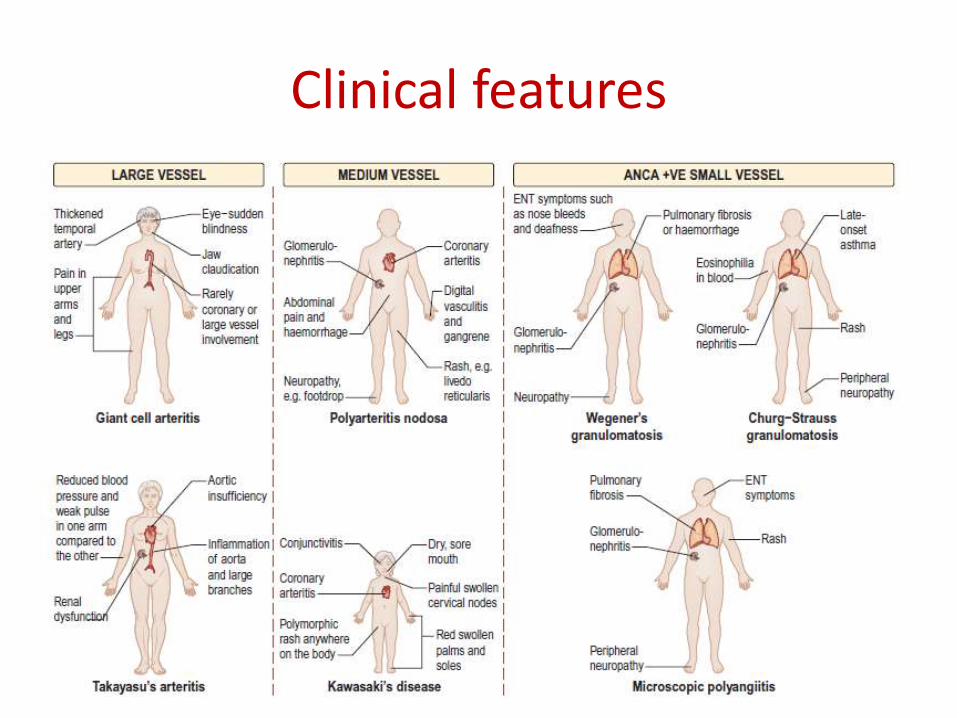
Clinical features

PMR & GCA
• Polymyalgia rheumatica (PMR) and giant cell (temporal) arteritis are systemic illnesses of the elderly.
• Both are associated with the finding of a giant cell arteritis on temporal artery biopsy.
Polymyalgia rheumatica (PMR)
PMR causes a sudden onset of severe pain and stiffness of the shoulders and neck, and of the hips and lumbar spine.
These symptoms are worse in the morning, lasting from 30 minutes to several hours.
Clinical history is usually diagnostic and the patient is always over 50 years old.
Approximately one-third of patients develop systemic features of tiredness, fever, weight loss, depression and occasionally nocturnal sweats.

Investigation of PMR
A raised ESR and/or CRP is a hallmark of this condition.
Serum alkaline phosphatase and γ-glutamyltranspeptidasemay be raised as markers of the acute inflammation.
Anaemia often present.
Temporal artery biopsy shows giant cell arteritis in 10–30% of cases, but is rarely performed unless GCA is also suspected.
Giant cell arteritis
GCA is inflammatory granulomatous arteritis of large cerebral arteries which occurs in association with PMR.
The patient may have current PMR, a history of recent PMR, or be on treatment for PMR.
Clinical features of GCA
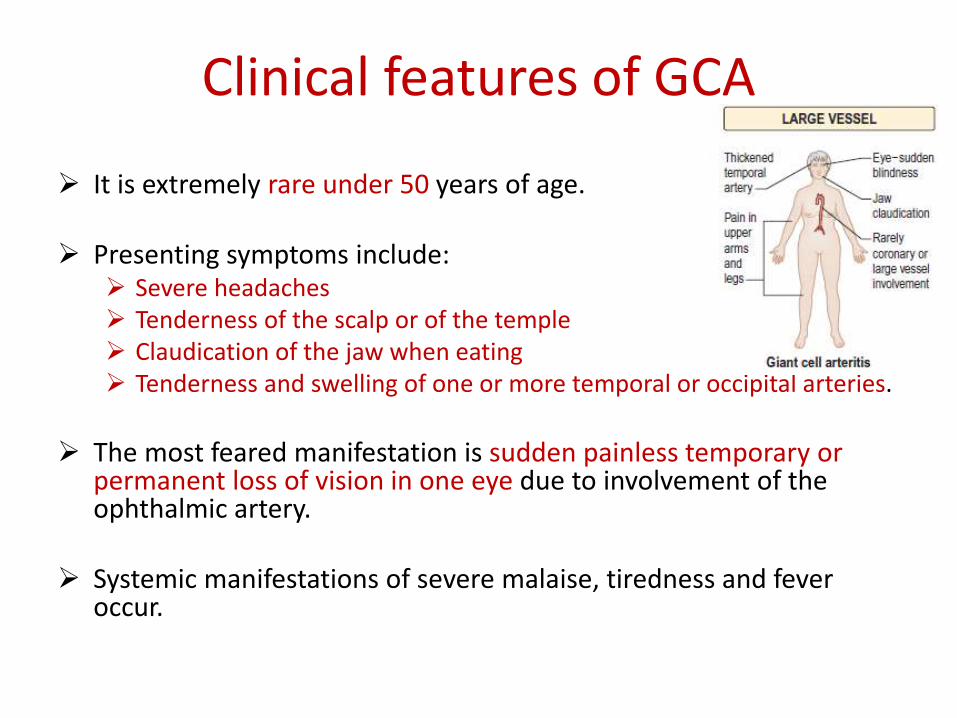
It is extremely rare under 50 years of age.
Presenting symptoms include: Severe headaches Tenderness of the scalp or of the temple Claudication of the jaw when eating Tenderness and swelling of one or more temporal or occipital arteries.
The most feared manifestation is sudden painless temporary or permanent loss of vision in one eye due to involvement of the ophthalmic artery.
Systemic manifestations of severe malaise, tiredness and fever occur.

Investigation of GCA
• A temporal artery biopsy from the affected side is the definitive diagnostic test. This should be taken before, or within 7 days of starting, high doses of corticosteroids.
• Anemia may be present
• ESR is usually raised and the CRP very high.
• Liver biochemistry: Abnormalities occur, as in PMR
Histological features of GCA
The histological features of GCA are:
Cellular infiltrates of CD4+ T lymphocytes, macrophages and giant cells in the vessel wall.
Granulomatous inflammation of the intima and media
Breaking up of the internal elastic lamina
Giant cells, lymphocytes and plasma cells in the internal elastic lamina.

Treatment of PMR or GCA
Corticosteroids produce a dramatic reduction of symptoms of PMR within 24–48 hours of starting treatment, provided the dose is adequate.
This treatment should reduce the risk of patients who have PMR developing GCA.
In GCA, corticosteroids are obligatory because they significantly reduce the risk of irreversible visual loss and other focal ischaemic lesions, but much higher doses are needed than in PMR.

Sometimes biopsy is not obtainable, so the treatment should not be delayed, especially if there have already been episodes of visual loss or stroke.
PMR: 10–15 mg prednisolone as a single dose in the morning.
GCA: 60–100 mg prednisolone, usually in divided doses.
Most patients will eventually be able to stop corticosteroids after 12–18 months.
Calcium and vitamin D supplements and sometimes bisphosphonates are necessary to prevent osteoporosis while high-dose steroids are being used

Takayasu’s disease
This is rare, except in Japan.
It is of unknown aetiology and occurs in females.
There is a vasculitis involving the aortic arch as well as other major arteries.
There is also a systemic illness, with pain and tenderness over the affected arteries.
Absent peripheral pulses and hypertension are common.
Corticosteroids help relieve symptoms.
Treatment may require a surgical bypass to improve perfusion of the affected areas.
Eventually heart failure and strokes may occur but most patients survive for at least 5 years
Medium-sized vessel vasculitis

Polyarteritis nodosa (PAN)
Classical PAN is a rare condition which usually occurs in middle-aged men.
its occasional association with hepatitis B antigenaemiasuggests a vasculitis secondary to the deposition of immune complexes.
Pathologically, there is fibrinoid necrosis of vessel walls with microaneurysm formation, thrombosis and infarction.

Clinical features
These include fever, malaise, weight loss and myalgia. These initial symptoms are followed by dramatic acute features that are due to organ infarction.
Neurological: mononeuritis multiplex is due to arteritis of the vasa nervorum.
Abdominal: pain due to arterial involvement of the abdominal viscera, mimicking acute cholecystitis, pancreatitis or appendicitis. Gastrointestinal haemorrhage occurs because of mucosal ulceration.

Renal: presents with haematuria and proteinuria. Hypertension and acute/chronic kidney disease occur.
Cardiac: coronary arteritis causes myocardial infarction and heart failure. Pericarditis also occurs.
Skin: subcutaneous haemorrhage and gangrene occur. A persistent livedo reticularis is seen in chronic cases. Cutaneous and subcutaneous palpable nodules occur, but are uncommon.
Lung: involvement is rare.
Investigations
Blood count: Anaemia, leucocytosis and a raised ESR occur.
Angiography: Demonstration of microaneurysms in hepatic, intestinal or renal vessels if necessary.
Other investigations: as appropriate (e.g. ECG and abdominal ultrasound), depending on the clinical problem. ANCA is positive only rarely in classic PAN.

Treatment
Is with corticosteroids, usually in combination with immunosuppressive drugs such as azathioprine.
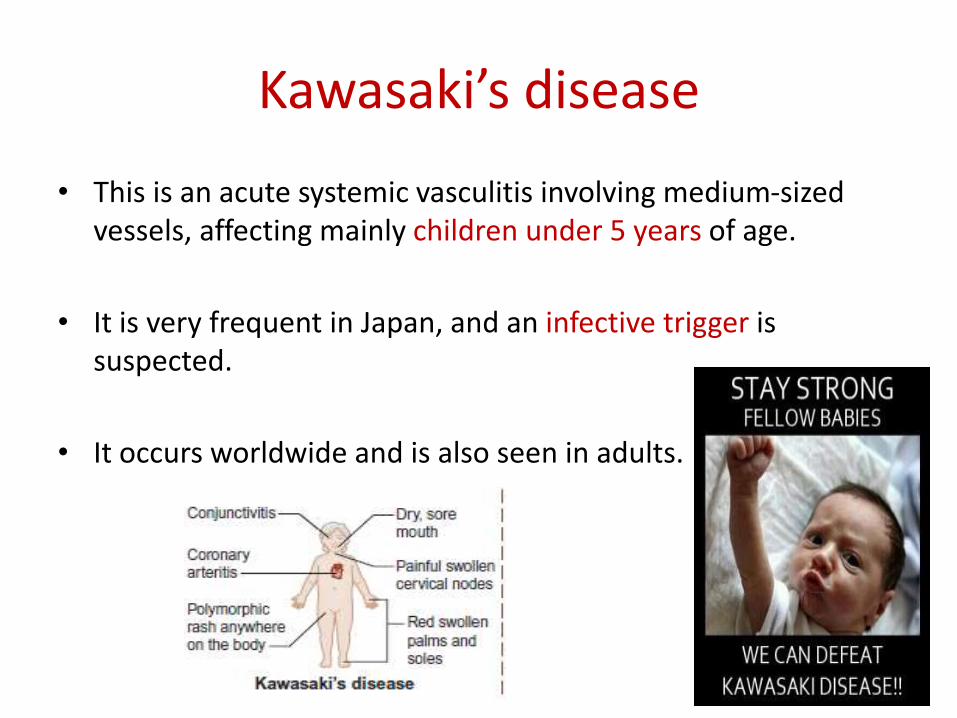
Kawasaki’s disease
• This is an acute systemic vasculitis involving medium-sized vessels, affecting mainly children under 5 years of age.
• It is very frequent in Japan, and an infective trigger is suspected.
• It occurs worldwide and is also seen in adults.

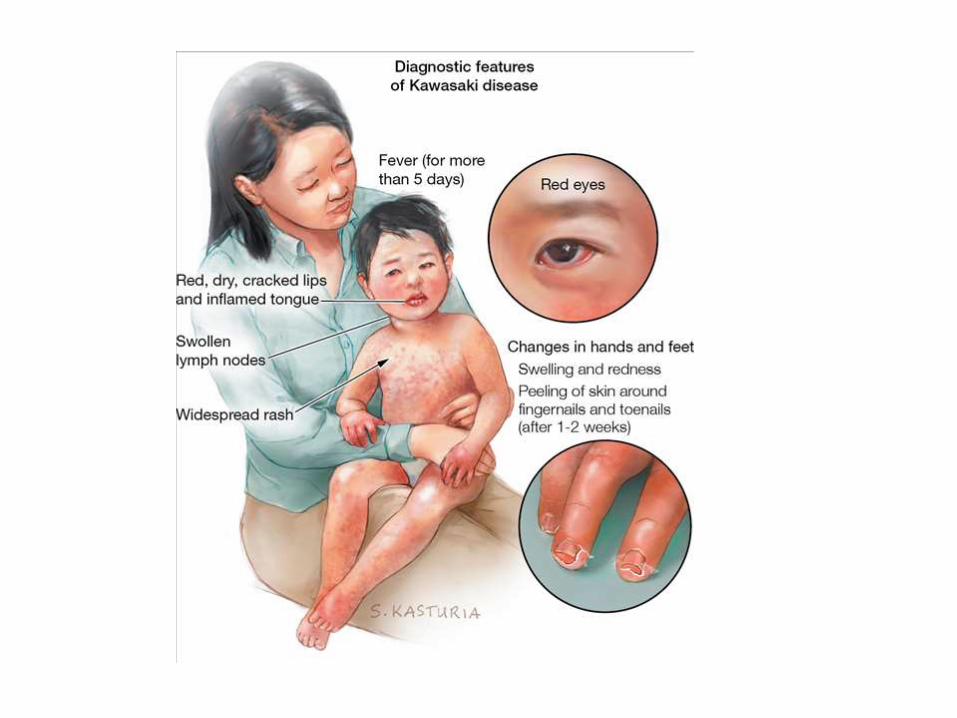
Clinical features
Fever lasting 5 days or more
Bilateral conjunctival congestion 2–4 days after onset
Dryness and redness of the lips and oral cavity 3 days after onset
Acute cervical lymphadenopathy accompanying the fever
Polymorphic rash involving any part of the body
Redness and oedema of the palms and soles 2–5 days after onset
Diagnosis
The persistent fever plus at least 4/5 features should be present to make the diagnosis, or < 4 if coronary aneurysms can be seen on two dimensional echocardiography, MRI or angiography.
Cardiovascular changes in the acute stage include pancarditis and coronary arteritis leading to aneurysms or dilatation.
Anti-endothelial cell autoantibodies are often detectable.
Other features include diarrhoea, albuminuria, aseptic meningitis and arthralgia and, in most, there is a leucocytosis, thrombocytosis and a raised CRP.

Treatment
• Is with a single dose of high-dose intravenous immunoglobulin (2 g/kg), which prevents the coronary artery disease, followed after the acute phase by aspirin 200–300 mg daily.
• There is no evidence that steroid treatment improves the outcome.
Small vessel vasculitis
This can be separated into those that are positive or negative for anti-neutrophil cytoplasmic antibody (ANCA)

ANCA-positive small vessel vasculitis
Wegener’s granulomatosis
Churg–Strauss granulomatosis
Microscopic polyangiitis
ANCA-negative small vessel vasculitis
Henoch–Schönlein purpura
Cryoglobulinaemicvasculitis
Cutaneous leucocytoclasticvasculitis
ANCA-positive small vessel vasculitis
Wegener’s granulomatosis It is characterized by lesions involving the upper respiratory tract, lungs and kidneys.
It often starts with severe rhinorrhoea, with subsequent nasal mucosal ulceration followed by cough, haemoptysis and pleuritic pain.
Etiology is unknown
Single or multiple nodular masses or pneumonic infiltrates with cavitation are seen on chest X-ray.
The typical histological changes are usually best seen on renal biopsy, which shows necrotizing microvascular glomerulonephritis.
This disease responds well to treatment with cyclophosphamide 150–200 mg daily.
Rituximab is also being used.
A variant of Wegener’s granulomatosis called ‘midline granuloma’ affects the nose and paranasal sinuses and is particularly mutilating; it has a poor prognosis.
Churg–Strauss syndrome
This condition classically occurs in males in their 4th decade, who present with rhinitis and asthma, eosinophilia and systemic vasculitis.
The aetiology is uncertain.
Typically, it involves the lungs, peripheral nerves and skin, but renal involvement is uncommon.
Transient patchy pneumonia-like shadows may occur.
Skin lesions include tender subcutaneous nodules as well as petechial or purpuric lesions.
ANCA is usually positive.
The disease responds well to corticosteroids.

Microscopic vasculitis (polyangiitis)
This involves the kidneys and the lungs where it results in recurrent haemoptysis.
ANCA is usually positive.

ANCA-negative small vessel vasculitis

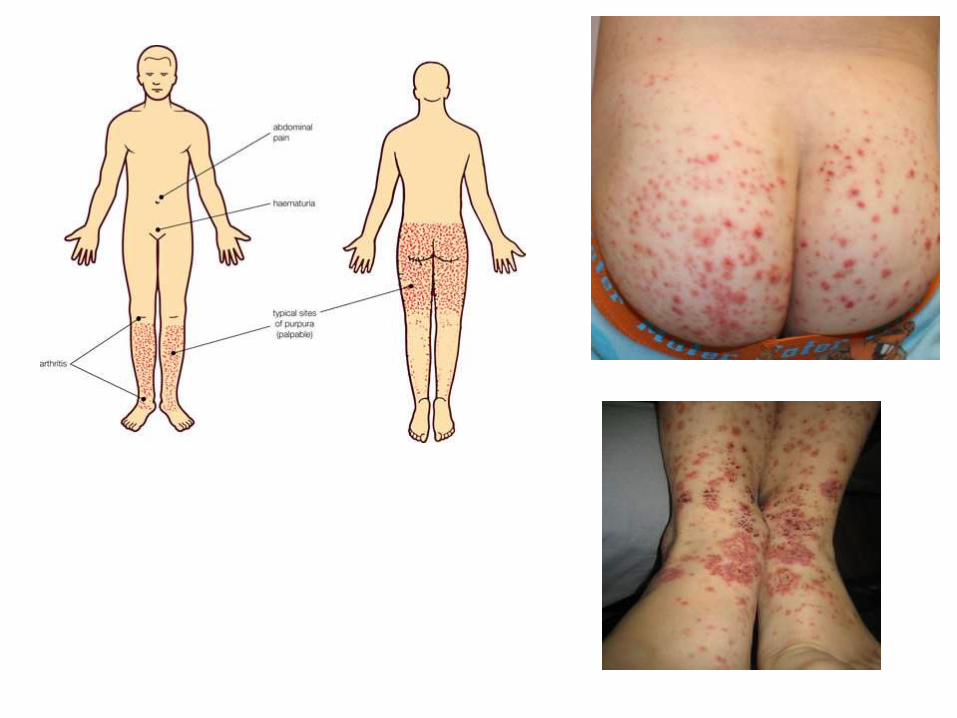
Henoch–Schönlein Purpura
• This clinical syndrome comprises a characteristic skin rash, abdominal colic, joint pain and glomerulonephritis.
• Approximately 30–70% have clinical evidence of renal disease with haematuria and/or proteinuria
• The renal lesion is a focal segmental proliferative glomerulonephritis, sometimes with mesangial hypercellularity.
• In more severe cases, epithelial crescents may be present.
• Immunoglobulin deposition is mainly IgA in the glomerular mesangiumdistribution, similar to IgA nephropathy.
• There is no treatment of proven benefit; steroid therapy is ineffective.
• Treatment is usually supportive but with crescentic GN aggressive immunosuppression has been tried with variable outcome.

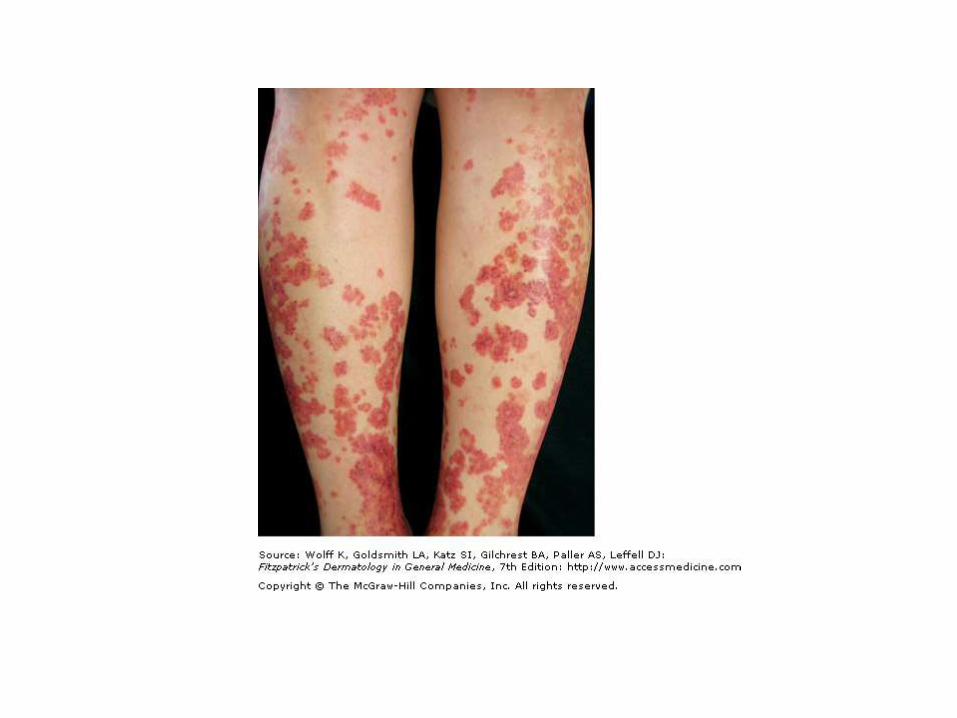
Leucocytoclastic vasculitis
• (LCV) is the most common cutaneous vasculitis affecting small vessels.
• This usually appears on the lower legs as a symmetrical palpable purpura.
• It can be caused by drugs (15%), infection (15%), inflammatory disease (10%) or malignant disease (<5%) but often no cause is found (55–60%).
• Investigations are only necessary with persistent lesions or associated signs and symptoms.
• LCV often settles spontaneously, treatment with analgesia, support stockings, dapsone or prednisolone may be needed to control the pain and to heal up any ulceration.

References
• Kumar & Clark's clinical medicine 8th edition

















