® ORTHOPAEDIC SPORTS MEDICINE Board Review Manual Volume 2, Part 3 December 2005 Osteochondral Injury of the Knee Endorsed by the Association for Hospital Medical Education www.turner-white.com
Transcript
®
ORTHOPAEDIC SPORTS MEDICINEBoard Review Manual
Volume 2, Part 3 December 2005
Osteochondral Injury of the Knee
Endorsed by theAssociation for HospitalMedical Educationwww.turner-white.com
The company long respected for advancing the science of cartilage repair has more to
offer than you ever anticipated. An established leader in the development of biomaterials
and cell therapies, Genzyme Biosurgery is excited to now be driving the marketing and
distribution of Synvisc® (hylan G-F 20). And our pioneering research into novel OA and
cartilage repair solutions is destined to redefine the field of orthobiologics. So take a
second look at Genzyme Biosurgery. What you see may surprise you.
Your vis ion is our new bottom l ine.
GENZYME and SYNVISC are registeredtrademarks of Genzyme Corporation.
Genzyme Biosurgery55 Cambridge ParkwayCambridge, MA 02142
1-800-901-7251www.genzymebiosurgery.com
Endorsed by the Association for HospitalMedical Education
®
ORTHOPAEDIC SPORTS MEDICINE BOARD REVIEW MANUAL
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 1
STATEMENT OF EDITORIAL PURPOSE
The Hospital Physician Orthopaedic Sports Medi-cine Board Review Manual is a peer-reviewedstudy guide for orthopaedic sports medicinefellows and practicing orthopaedic surgeons.Each manual reviews a topic essential to thecurrent practice of orthopaedic sports medi-cine.
PUBLISHING STAFFPRESIDENT, GROUP PUBLISHER
Bruce M. White
EDITORIAL DIRECTORDebra Dreger
ASSOCIATE EDITORTricia Faggioli
EDITORIAL ASSISTANTFarrawh Charles
EXECUTIVE VICE PRESIDENTBarbara T. White
EXECUTIVE DIRECTOR OF OPERATIONS
Jean M. Gaul
PRODUCTION DIRECTORSuzanne S. Banish
PRODUCTION ASSISTANTKathryn K. Johnson
ADVERTISING/PROJECT MANAGERPatricia Payne Castle
SALES & MARKETING MANAGERDeborah D. Chavis
Copyright 2005, Turner White Communications, Inc., Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. All rights reserved. No part of thispublication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or oth-erwise, without the prior written permission of Turner White Communications. The preparation and distribution of this publication are supported by sponsorshipsubject to written agreements that stipulate and ensure the editorial independence of Turner White Communications. Turner White Communications retains fullcontrol over the design and production of all published materials, including selection of appropriate topics and preparation of editorial content. The authors aresolely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner WhiteCommunications. Turner White Communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inac-curacies. Information contained within this publication should not be used as a substitute for clinical judgment.
NOTE FROM THE PUBLISHER:This publication has been developed withoutinvolvement of or review by the AmericanBoard of Orthopaedic Surgery.
Osteochondral Injuryof the KneeContributors:Jason M. Scopp, MDDirector, Cartilage Restoration Center, PeninsulaOrthopaedic Associates, PA, Salisbury, MD
Bert R. Mandelbaum, MDFellowship Director, Santa Monica Orthopaedicand Sports Medicine Group, Santa Monica, CA
Editor:Andrew J. Cosgarea, MDAssociate Professor, Department of Orthopaedic Surgery,Johns Hopkins University School of Medicine, Baltimore, MD
Chondral and osteochondral injuries are commonand typically affect a young, athletic population. In a ret-rospective review of more than 31,000 knee arthros-copies, Curl et al1 reported articular cartilage damagein 63% of patients, with more than 60% having a gradeIII or grade IV lesion. Failure to recognize these injuriescan result in long-term disability.
The stresses created during athletic activity place theknee at risk for a range of osteochondral injuries. Ifinjury occurs, it is imperative to recognize osteochon-dral status as being intimately linked with limb align-ment, meniscal status, and ligamentous status. A defi-ciency in one part of this functional unit can have animpact on the others and, in the short term, can lead toa loss of athletic performance. If articular cartilage losesthe ability to adapt to repetitive stresses, loss of athleticperformance may be followed by the development ofchondropenia and ultimately osteoarthritis (OA).
This manual reviews the functional anatomy of artic-ular cartilage, the pathophysiology of osteochondral in-jury, and the clinical evaluation and management ofathletes with osteochondral injuries of the knee. A clin-ical algorithm is presented as a clinical tool to organizethe treatment options for these patients.
ANATOMY AND BIOMECHANICS OF ARTICULARCARTILAGE
Articular (or hyaline) cartilage is a viscoelastic mate-rial that allows variable load bearing by the knee duringdaily functional and athletic activities. Stress reductionto the subchondral bone and minimization of frictionof the articular surface are essential in fulfilling thisrole. Articular cartilage provides joint surfaces with low-friction wear characteristics that are required for repet-itive motion, allowing the athlete to perform consis-tently at the highest levels of activity and performancewithout symptoms elicited from the knee joint.
The functional characteristics of articular cartilagedepend on its specific structural composition and orga-
nization.2 Normal articular cartilage is composed of anextracellular matrix and chondrocytes. The extracellu-lar matrix consists primarily of water, proteoglycans,and collagens. Type II collagen accounts for 90% to95% of the total collagen volume, while types V, VI, IX,X, and XI comprise the remaining 5% to 10%.3 Watercontent varies from 65% to 85%, depending on theload status and the presence or absence of degenerativechanges. During the early phases of OA, the water con-tent can increase to 90%.3
The functional organizational unit of articular carti-lage is composed of 4 layers: the superficial tangentialzone, the middle zone, the deep zone, and the calcifiedcartilage. The tidemark lies between the deep zone andthe calcified cartilage and represents the transitionfrom uncalcified to calcified cartilage. The subchondralbone and the calcified cartilage are continuous and arecrucial supportive structures involved in load transmis-sion. The resilience of the functional load-bearing unitis essential for durability and smooth joint motion.
PATHOPHYSIOLOGY OF ARTICULAR CARTILAGEINJURY
PROGRESSIVE LOSS OF CHONDRAL INTEGRITY
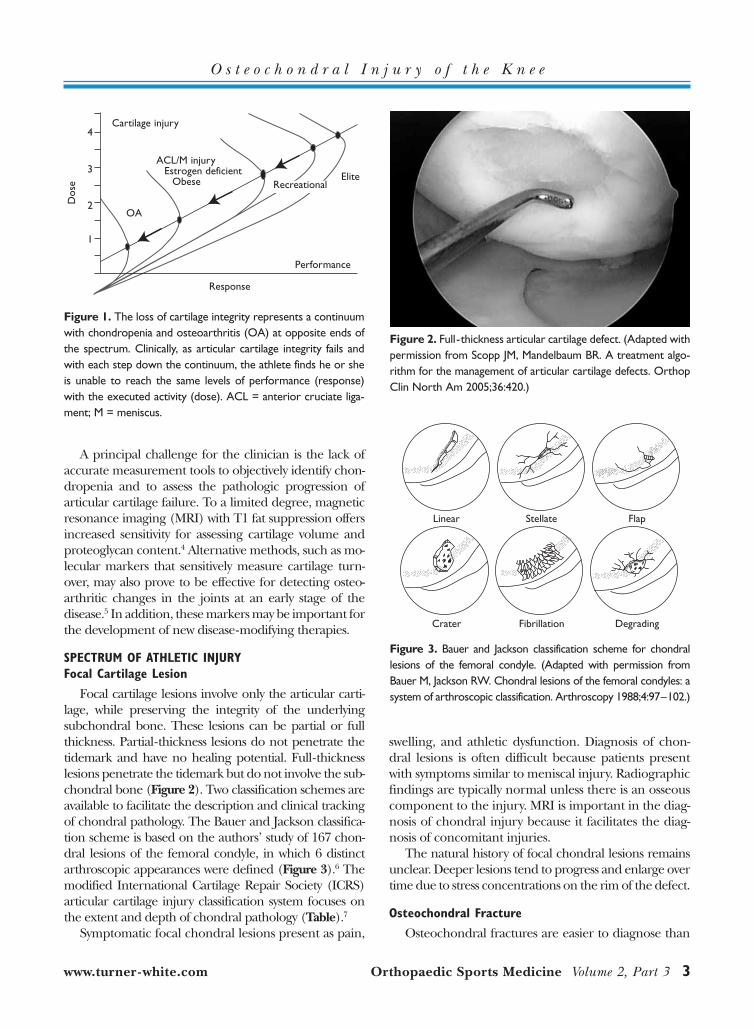
While the natural history of chondral injury of theknee is not well defined, it is apparent that a loss of artic-ular integrity through injury, pathologic loading, andaging can cause degenerative changes over time. Thesechanges begin as a loss of cartilage volume (chondrope-nia) and function, followed by development of articularcartilage defects that lead to elevated joint contact pres-sures and further joint degradation and, possibly, theeventual development of OA. The continuum of carti-lage injury can be clinically depicted in a dose-responsecurve (Figure 1). As the athlete competes, a force (dose)is presented to the articular cartilage. If the cartilage isnormal, a typical response occurs. However, as chon-dropenia and articular cartilage defects develop, the ultrastructural properties of articular cartilage can nolonger provide an adequate response, leading to symp-toms of pain, swelling, and a loss of athletic performance.
ORTHOPAEDIC SPORTS MEDICINE BOARD REVIEW MANUAL
Osteochondral Injury of the KneeJason M. Scopp, MD, and Bert R. Mandelbaum, MD
A principal challenge for the clinician is the lack ofaccurate measurement tools to objectively identify chon-dropenia and to assess the pathologic progression ofarticular cartilage failure. To a limited degree, magneticresonance imaging (MRI) with T1 fat suppression offersincreased sensitivity for assessing cartilage volume andproteoglycan content.4 Alternative methods, such as mo-lecular markers that sensitively measure cartilage turn-over, may also prove to be effective for detecting osteo-arthritic changes in the joints at an early stage of thedisease.5 In addition, these markers may be important forthe development of new disease-modifying therapies.
SPECTRUM OF ATHLETIC INJURY Focal Cartilage Lesion
Focal cartilage lesions involve only the articular carti-lage, while preserving the integrity of the underlying subchondral bone. These lesions can be partial or fullthickness. Partial-thickness lesions do not penetrate thetidemark and have no healing potential. Full-thicknesslesions penetrate the tidemark but do not involve the sub-chondral bone (Figure 2). Two classification schemes areavailable to facilitate the description and clinical trackingof chondral pathology. The Bauer and Jackson classifica-tion scheme is based on the authors’ study of 167 chon-dral lesions of the femoral condyle, in which 6 distinctarthroscopic appearances were defined (Figure 3).6 Themodified International Cartilage Repair Society (ICRS)articular cartilage injury classification system focuses onthe extent and depth of chondral pathology (Table).7
Symptomatic focal chondral lesions present as pain,
swelling, and athletic dysfunction. Diagnosis of chon-dral lesions is often difficult because patients presentwith symptoms similar to meniscal injury. Radiographicfindings are typically normal unless there is an osseouscomponent to the injury. MRI is important in the diag-nosis of chondral injury because it facilitates the diag-nosis of concomitant injuries.
The natural history of focal chondral lesions remainsunclear. Deeper lesions tend to progress and enlarge overtime due to stress concentrations on the rim of the defect.
Osteochondral Fracture
Osteochondral fractures are easier to diagnose than
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 3
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 1. The loss of cartilage integrity represents a continuumwith chondropenia and osteoarthritis (OA) at opposite ends ofthe spectrum. Clinically, as articular cartilage integrity fails andwith each step down the continuum, the athlete finds he or sheis unable to reach the same levels of performance (response)with the executed activity (dose). ACL = anterior cruciate liga-ment; M = meniscus.
4
3
2
1
Cartilage injury
Performance
Response
Dos
e
OA
ACL/M injury Estrogen deficient
Obese RecreationalElite
Figure 2. Full-thickness articular cartilage defect. (Adapted withpermission from Scopp JM, Mandelbaum BR. A treatment algo-rithm for the management of articular cartilage defects. OrthopClin North Am 2005;36:420.)
Figure 3. Bauer and Jackson classification scheme for chondrallesions of the femoral condyle. (Adapted with permission fromBauer M, Jackson RW. Chondral lesions of the femoral condyles: asystem of arthroscopic classification. Arthroscopy 1988;4:97–102.)
Linear Stellate Flap
Crater Fibrillation Degrading
chondral defects because the bony component can beseen radiographically (Figure 4). Osteochondral frac-tures are often the result of patellar dislocation. Nomuraet al8 evaluated chondral and osteochondral injuriesduring acute lateral patellar dislocation and found os-teochondral fractures in 19%. Of these, 95% involvedthe medial facet of the patella.
The natural history of osteochondral fractures is un-clear. Anatomic reduction and stable fixation allow theunderlying bone to heal, but the overlying articular car-tilage may degenerate over time as a response to the ini-tial traumatic event.
Osteochondritis Dissecans
In osteochondritis dissecans (OCD), a fragment ofsubchondral bone and articular cartilage separatesfrom the articular surface. The etiology of OCD is vari-able and may include a traumatic event, repetitive mi-crotrauma, or a loss of subchondral vascularity. Oftenno clear etiology exists, suggesting the cause may bemultifactorial.9 The knee is the most commonly affect-ed joint (75%–85% of cases); however, the capitellumof the elbow and the talar dome of the ankle can alsobe affected.9,10 Within the knee, the lateral aspect of themedial femoral condyle is involved in 80% to 85% ofpatients, the lateral femoral condyle in 10% to 15%,and the patella in up to 5%.11
Two distinct forms of OCD are recognized, based on
patient population affected. The juvenile form affectsindividuals whose physes remain open.12 The adultform is seen in adolescents with closed physes and inadults. Because treatment for the juvenile and adultforms often differs, it is important to think of each formas a separate clinical entity. However, the orthopaedicliterature often groups these 2 distinct forms together.
Clanton and DeLee13 described 4 grades of OCDlesions: grade 1 (depressed osteochondral fracture),grade 2 (osteochondral fragment attached by an os-seous bridge), grade 3 (detached, nondisplaced frag-ment), and grade 4 (displaced fragment [loose body]).Cahill and Berg14 described another classificationscheme based on the degree of radioisotopic uptake onscintigraphy: stage I (lesion visible on plain radio-graphs, but bone scan reveals normal findings), stage II(bone scan reveals increased uptake in the area of thelesion seen on plain radiographs), stage III (stage IIfindings plus increased isotopic uptake in the entirefemoral condyle), and stage IV (stage III findings plusuptake in the adjacent tibial plateau).
Plain radiographs (Figure 5) are often negative inthe early stages of OCD, which may prompt the clini-cian to consider other diagnostic modalities. The use ofMRI (Figure 6) allows for the evaluation of the under-lying subchondral bone as well as the presence or ab-sence of fluid behind the fragment. The presence offluid behind the fragment is suggestive of fragmentinstability.15 In 1990, Nelson et al15 used MRI to predictthe grade of OCD lesions and to correlate it with arthro-scopic findings; the authors were able to correctly pre-dict the grade of lesion in 11 of 12 patients.
The natural history of OCD in the knee depends onseveral variables. Physis status, lesion size, and degree offragment stability contribute to the progression or regres-sion of disease. While we know of no prospective, ran-domized controlled trial comparing various treatmentregimens for juvenile and adult OCD, certain facts as
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 4. Radiograph of an osteochondral fracture after dislo-cation of the patella.
Table. Modified International Cartilage Repair SocietyGrading System for Chondral Injury
Injury Grade Injury Description
0 Normal cartilage
1a Soft indentation
1b Superficial fissures and cracks
2 Defects extending down to < 50% of cartilage depth
3a Defects extending down to > 50% of cartilage depth
3b Defects extending down to calcified layer
3c Defects extending down to but not through subchondral bone
3d Delamination
4 Severely abnormal, with penetrationthrough subchondral plate
Data from International Cartilage Repair Society (ICRS) cartilage injuryevaluation package. Articular cartilage injury classification. Available atwww.cartilage.org/files/ICRS_evaluation.pdf. Accessed 29 Nov 2005.
well as conclusions drawn from the literature can helpguide the approach to treatment. For example, it isknown that defects of articular cartilage do not healwith normal articular cartilage. Mesenchymal tissue isconverted into fibrocartilage, and fibrocartilage has de-creased proteoglycan content compared with hyalinecartilage. Fibrocartilage is also less resilient and, there-fore, continued trauma to the joint can lead to furtherdegeneration.16,17 Further, studies show that articularcartilage lesions in the weight-bearing surface of thefemur progress.18 Finally, symptoms and radiographicevidence of gonarthrosis approached 100% in adultswith untreated OCD19; spontaneous healing typicallyoccurs if the physes are open.
EVALUATION
When evaluating a patient for chondral or osteo-chondral injury, it is important to appreciate that thefunctional unit of articular cartilage includes alignment(limb and patellofemoral), meniscal integrity, and liga-mentous stability. Malalignment, loss of meniscalintegrity, or ligamentous instability will increase theload on the chondral surface and may worsen existingdefects and/or prevent successful repair or restoration.
HISTORY
An accurate and thorough patient history is essential.The history should include a detailed description of thetraumatic episode as well as the type, location, timing, andduration of symptoms. Patients will often complain ofnonspecific symptoms including localized pain, swelling,and loss of motion. If the defect involves a detached orloose body, mechanical catching may be described.
PHYSICAL EXAMINATION
A comprehensive physical examination of the kneeprovides a functional assessment of articular cartilagestatus. Important elements to be assessed include rangeof motion, swelling (soft tissue, joint effusion), and jointline tenderness. Additionally, assessment for varus or val-gus malalignment and defects of the anterior and pos-terior cruciate ligaments provides insight regarding theknee macroenvironment and possible forces transferredthrough an articular cartilage defect. Each element ofthe examination should be compared with the asympto-matic side. Examination should also include an obser-vation of gait to evaluate for dynamic pathology as wellas adaptive mechanisms used to decrease weight bearingof the joint.
Wilson20 described a useful physical examination testfor OCD of the knee. The Wilson sign is elicited by flex-ing the knee to 90 degrees, internally rotating the tibia,and then slowly extending the knee. A positive sign ispain at approximately 30 degrees of flexion that is re-lieved by external rotation of the tibia.
DIAGNOSTIC IMAGINGPlain Radiography
Since the physical findings of cartilage injury arenonspecific, plain radiographs should be used to ruleout fractures, evaluate for degenerative changes, andassess alignment. The standard radiographic series includes weight-bearing anteroposterior, 45-degree
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 5
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 5. Radiograph demonstrating an osteochondritis disse-cans lesion of the posterolateral medial femoral condyle.
Figure 6. Magnetic resonance image of the same lesion shownin Figure 5.
flexion posteroanterior, patellofemoral, and lateralviews. Additional views include “long-leg” hip-to-anklefilms taken to evaluate limb mechanical axis. Becausecartilage is not visible on plain radiography, joint spacewidth seen on weight-bearing radiographs has beenused as a proxy for cartilage integrity. Despite thesetechniques, radiographs are unable to detect subtlechanges in cartilage morphology associated with articu-lar cartilage defects, chondropenia, and early OA.21
Magnetic Resonance Imaging
MRI is becoming increasingly more important in theevaluation of chondral and osteochondral injury. Yulish
and colleagues22 were the first to report on the use of MRIto assess articular cartilage and claimed MRI could re-liably diagnose early and late stages of OA in the patella.However, this claim has not been reliably reproduced.Today, there remains a lack of consensus among investiga-tors on what constitutes the normal magnetic resonanceappearance of articular cartilage. Investigators have ap-plied a variety of magnetic resonance pulse sequencestoward the depiction of articular cartilage and havereached varied conclusions regarding its appearance.23,24
On high-resolution MRIs, articular cartilage demostratesa multilaminar appearance. However, there is disagree-ment about the number of layers in normal articular car-tilage and the histologic significance of each layer.
MRI has improved dramatically in recent years andnow has the potential to replace plain radiography inassessing articular cartilage structural integrity.21 Theuse of contrast enhancement through direct or indirectinjection increases the ability of MRI to detect focallesions. A recent preliminary study demonstrated goodcorrelation between an MRI-based quantification ofcartilage damage and arthroscopic findings.25 Other in-vestigators have explored MRI-based measurements ofcartilage thickness and volume26 and the assessment ofchondropenia and OA progression. Interobserveragreement, reproducibility, and accuracy remain signif-icant problems for MRI-based evaluation of the severityof knee OA.27 Moreover, optimal imaging protocolshave not been determined.28 Thus, the potential ofMRI as a primary outcome measurement tool for stud-ies of OA has not been realized.
Bone Scintigraphy
Bone scintigraphy can be used as a measure of osteo-blastic activity and blood flow. The degree of osseous up-take may correlate with the healing potential of an OCDfragment and serve as a useful prognostic indicator.14
MANAGEMENT
ASSESSMENT OF FACTORS INFLUENCING MANAGEMENT
Primary and secondary treatment options for isolateddefects of the femoral condyle and for patellar-trochleardefects are summarized in Figure 7 and Figure 8, respec-tively. The choice of treatment is influenced by severallocal, regional, and systemic factors that may affect theprogression or degeneration of the articular cartilagedefect. It is important to define and characterize thesefactors as the first step in managing a patient with afocal chondral lesion, osteochondral fracture, or OCD.
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 7. Treatment algorithm for articular cartilage defects ofthe femoral condyle, showing primary (1°) and secondary (2°)options. Secondary treatment choices should be considered ifprimary treatment fails or if other factors preclude the use of afirst-line option. *Appropriate treatment is staged to avoid com-promise of postoperative rehabilitation. ACI = autologous chon-drocyte implantation; OCG = osteochondral grafting; – indicatestreatment not recommended; + indicates acceptable treatment;++ indicates optimal treatment. (Adapted with permission fromScopp JM, Mandelbaum BR. A treatment algorithm for the man-agement of articular cartilage defects. Orthop Clin North Am2005;36:423.)
Femoral defects
Alignment *
Meniscus *
Ligaments *
Size
Small(0–1 cm2)
Medium(1–2 cm2)
Large(> 2 cm2)
1° Treatment options Small Medium LargeMicrofracture ++ ++ +OCG ++ ++ –Allograft – – ++ACI – – ++
2° Treatment options Small Medium LargeMicrofracture ++ + –OCG ++ ++ –ACI – ++ ++Allograft – – ++
In an effort to ensure uniform standards of manage-ment, the ICRS has developed a comprehensive methodfor classifying articular cartilage defects, which is basedon an assessment of 9 variables: etiology, defect thick-ness, lesion size, degree of containment, location, liga-mentous integrity, meniscal integrity, alignment, and rel-evant factors in the patient history (ie, general medical,systemic, and/or family history factors).7 Etiology is clas-sified as traumatic or chronic. Defect thickness is as-sessed according to the ICRS grading system shown inthe Table; partial-thickness defects that do not pene-trate the tidemark have no healing potential. Lesion sizedictates treatment approach; small (< 2 cm2) defectshave different treatment options than large (> 2 cm2)defects. A contained defect is surrounded by articular car-tilage on all sides; as the degree of containment decreas-es, consequent loss of joint space is seen on radiographs(Figure 9). In terms of location, defects in the weight-bearing surface of the knee may be isolated (unipolar) orcombined with a defect on the articulating surface (bipo-lar). As previously noted, ligamentous and meniscal in-
tegrity and varus/valgus alignment are critical compo-nents of the functional unit of articular cartilage. An unstable tibiofemoral or patellofemoral joint leads to in-creased articular cartilage lesions,29 loss of only 30% ofthe meniscus increases joint contact pressures by morethan 350%,3 and varus or valgus malalignment increasesmedial or lateral compartment forces, respectively.30
TREATMENT OPTIONS FOR SPECIFIC SITUATIONS
Scopp and Mandelbaum31 have introduced a clinicalalgorithm to organize management options for articu-lar cartilage defects. The algorithm includes 10 specific“situations” defined by lesion size and depth and asso-ciated factors (ie, alignment, ligament and meniscalintegrity). Each situation considers the injury category,the current surgical treatment options, and unresolvedquestions regarding management.
The surgical options presented should be consid-ered only after failure of conservative therapy. Non-operative modalities include rest (removal of athleticstress) and restoration of joint motion and strength.Limited weight bearing may be required after acuteinjury. Gait training should be incorporated into a phys-ical therapy regimen. Crutches should not be discon-tinued until the antalgic gait has been resolved. Painfuleffusions may be aspirated to facilitate the maintenanceof motion. Joint aspiration may also provide clinicaldata to confirm diagnosis. For example, cruciate liga-ment tears, traumatic patellar dislocations, and osteo-chondral fractures frequently present with a bloodyeffusion.
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 7
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 8. Treatment algorithm for patellofemoral articular carti-lage defects, showing primary (1°) and secondary (2°) options.Secondary treatment choices should be considered if primarytreatment fails or if other factors preclude the use of a first-lineoption. ACI = autologous chondrocyte implantation; PF = patel-lofemoral; – indicates treatment not recommended; + indicatesacceptable treatment; ++ indicates optimal treatment (Adaptedwith permission from Scopp JM, Mandelbaum BR. A treatmentalgorithm for the management of articular cartilage defects.Orthop Clin North Am 2005;36:424.)
Figure 9. Uncontained full-thickness defect of the lateral fem-oral condyle after traumatic dislocation of the patella. (Adaptedwith permission from Scopp JM, Mandelbaum BR. A treatmentalgorithm for the management of articular cartilage defects.Orthop Clin North Am 2005;36:422.)
Situation 1: Meniscal Tears with Partial-ThicknessArticular Cartilage Defects
Meniscal tears with partial-thickness articular cartilagedefects are the most common type of articular cartilageinjury encountered in orthopaedic surgical practice. Theprimary treatment option for this combined injury is arth-roscopic chondroplasty with partial meniscectomy. Whilethere is no easy way to determine the extent of chon-droplasty required, it is important to remove any looseflaps of cartilage and edges that appear friable.
Mechanical and thermal chondroplasty may lead toprogression of partial-thickness defects. Caffey et al32
studied the effects of radiofrequency probes on humanarticular cartilage using 5 different systems. They con-cluded that when probes were held 1 mm from thechondral surface, no cellular death was seen. However,when the chondral surface was contacted, treated de-fects demonstrated energy penetration to the subchon-dral bone and cellular death of adjacent chondrocytes.No statistical differences between monopolar and bipo-lar devices were noted.32
Osteogenic protein 1 (OP-1) has been shown tostimulate synthesis of matrix by normal articular chon-drocytes33 and to possibly up-regulate matrix produc-tion in osteoarthritic chondrocytes.34 The use of OP-1 iscurrently being investigated for the treatment of partial-thickness chondral defects.
Glucosamine sulfate and chondroitin sulfate are usedto minimize the symptoms of OA, although their mech-anism of action remains unclear. Chan et al35 studied bo-vine articular cartilage explants after physiologic concen-trations of chondroitin sulfate and glucosamine sulfatewere administered and concluded that the substancescan regulate gene expression and synthesis of nitric ox-ide and prostaglandin E2, providing a plausible explana-tion for their purported anti-inflammatory properties.
The role of physical therapy after arthroscopic chon-droplasty and partial meniscectomy for every patient isunclear, but it is helpful when strength deficits exist pre-operatively. Physical therapy has also been shown to has-ten the return to sport in athletes.36,37
Situation 2: Small (< 1 cm2) Full-Thickness FemoralArticular Cartilage Defects without OCD
Unstable chondral fragments should be removed toprevent the development of loose bodies. To fill the de-fect, however, several techniques have been advocated.
The use of microfracture for small chondral defectshas been well studied. With this technique, a small pick isused to penetrate the subchondral bone. This releasesmesenchymal stem cells, which can form a fibrocartilagecover over the defect. Steadman et al38 followed a case
series of 72 patients (75 knees) for an average of 11 yearsfollowing microfracture. The authors found that over thefollow-up period, 80% of patients who were younger thanage 45 years and had no ligamentous or meniscal injurydemonstrated good or excellent results. Results seen withthe microfracture technique have led to a question of thedurability of fibrocartilage repair in active individuals.Gobbi et al39 prospectively followed 53 athletes after mi-crofracture (mean follow-up, 72 months) and found that80% noted a decline in sports activity at final follow-up.
Osteochondral grafting is another technique used tofill a small articular cartilage defect. During autogenousosteochondral grafting, a core of bone and cartilage isimmediately transferred to the defect. Because hyalinecartilage is transferred, no fibrocartilage forms, unlessmultiple plugs are transferred (the spaces betweenplugs fill in with fibrocartilage).40
Situation 3: Medium (1–2 cm2) Full-ThicknessFemoral Articular Cartilage Defects without OCD
Débridement, microfracture, and osteochondralgrafting offer technically simple primary treatment op-tions. As the defects get larger, autologous chondrocyteimplantation becomes a viable treatment option. Thisapproach is cellular-based. Chondrocytes are harvestedat an index operation (knee arthroscopy) and cultured.During a second operation, the cultured chondrocytesare implanted into the articular cartilage defect, be-neath a periosteal patch. Peterson et al41 studied thebiomechanics and long-term durability of this repairtechnique; 51 of 61 patients followed for up to 11 yearswere found to have good to excellent results on follow-up examinations. Second-look arthroscopies were per-formed in several of these patients, and indentationprobe measurements found the repaired cartilage tohave 90% of the stiffness characteristics of the sur-rounding normal articular cartilage. Biopsy samplesobtained from these patients showed hyaline-like char-acteristics and stained positive for type II collagen.
Situation 4: Large (> 2 cm2) Full-Thickness FemoralArticular Cartilage Defects with OCD or AvascularNecrosis
Osteochondral grafting, autologous chondrocyteimplantation, and osteochondral allografts can be usedto manage these large articular cartilage defects. Osteo-chondral allografts have 2 components (cartilage andbone). The transplanted cartilage is aneural, avascular,and immunoprivileged. The allograft bone is used as ascaffold and vehicle for the transfer of chondrocytes. Ina study used to evaluate the viability of chondrocytes attime of implantation, Allen et al42 found a significant
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
decrease in chondrocyte viability after 14 days of stor-age, but 60% to 90% chondrocyte viability has beenseen on retrieval studies.
Treatment of OCD. Juvenile forms (open growthplates) that do not heal with conservative treatment andsymptomatic adult forms require operative interven-tion. The basic tenets of surgical treatment includerestoration of the congruity of the joint surfaces, en-hancement of the local blood supply to the fragment orthe crater, rigid fixation of unstable fragments, and pro-tected weight-bearing with motion of the joint as soonas possible postoperatively.18
In situ drilling. Subchondral drilling can be used forstable OCD lesions with intact articular cartilage. In thistechnique, the subchondral bone is channeled in ananterograde or retrograde fashion. Image intensifica-tion can be used to facilitate the technique so that theintact cartilage surface is not violated. The goal of sub-chondral drilling is to promote revascularization.18
In situ fixation. Fixation can be accomplished withmetallic pins, compression screws, bioabsorbable pins,or osteochondral grafts. If an OCD lesion is intact orpartially detached, it can be fixed in situ and stabilized.If a metallic screw is used, it should be countersunk toavoid abrasion on the articulating surface. Several head-less screw options exist that allow for compressionacross the defect. If a metallic implant is used, reopera-tion is required for removal. The use of autogenousosteochondral grafts to stabilize the lesion eliminatesthe need for metallic intra-articular fixation and pro-motes revascularization of the subchondral bone, whileaddressing any bone loss.43
Open reduction internal fixation of displaced fragments.When an OCD lesion is completely detached and thereis an adequate bony component to the fragment, openreduction internal fixation can be attempted. The sub-chondral bed must be meticulously prepared to removeall fibrous tissue. The subchondral bone should then bedrilled to enhance revascularization. It is vital to ensureanatomic reduction to decrease abrasive wear on theadjacent chondral surfaces.
Osteochondral autograft and allograft. As discussed,these options allow for immediate transfer of bone andhyaline cartilage to fill a defect devoid of both. The useof allograft allows management of larger bony defectswithout the morbidity associated with harvesting multi-ple grafts.18,42
Autologous chondrocyte implantation. This techniquecan be used to manage OCD defects up to 8 mm deepwithout bone grafting. In a study of 58 patients withOCD treated with autologous chondrocyte implanta-tion, Peterson et al44 observed 91% good to excellent
results at a mean follow-up of 5.6 years. Average defectdepth was 7.8 mm, and no bone graft was used.
Fragment excision. Excision of the OCD fragmentwithout other treatment has been reported to be unsuc-cessful.14,45 Lesions progress in size and continue to besymptomatic.
Treatment of avascular necrosis. Management ofavascular necrosis parallels that of OCD. The defect leftafter débridement is managed depending upon lesionsize and bone loss.
Situation 5: Femoral Articular Cartilage Defects with Malalignment and/or Ligamentous or MeniscalInstability
Again, it is imperative to consider articular cartilage,limb alignment, the meniscus, and the ligaments asfunctionally interconnected: a defect in one affects theothers. Osteotomy, meniscal repair or allograft replace-ment, cruciate reconstruction(s), autologous chondro-cyte implantation, fresh allograft, or osteochondralautograft may be needed to reestablish alignment,chondral integrity, meniscal integrity, and ligamentousintegrity.46
Situation 6: Patellar and/or Trochlear ArticularCartilage Defects without Malalignment or Instability
Nonoperative treatment of patellofemoral pain cansuccessfully eliminate dynamic malalignment and coreweakness.47 Weakness of hip external rotators and ab-ductors can affect lower extremity control. These fac-tors are known to increase tension in the anterior cru-ciate ligament and to contribute to patellofemoral painand instability.48 Rehabilitation that includes a combina-tion of muscle strengthening, stretching, and patello-femoral taping is beneficial in creating an internal bio-mechanical environment that encourages maximaltissue healing.49 Operative intervention for pain with-out instability or tilt has a low level of success. In a studyof 22 knees, Schonholtz et al50 found improvement inonly 1 patient whose only symptom was pain.
Despite malalignment and patellofemoral instability,first-line treatment for patellar and/or trochlear articu-lar cartilage defects is rehabilitation, including taping,bracing, and pelvic stabilization. There is no single bestoption for management of anterior knee instability.The goal is to find the most accurate and least invasivemethod of treatment.49
Instability is caused by many structural and functional
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 9
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
factors that contribute to the malalignment and dysfunc-tion. Surgical treatment is aimed at addressing specificpathophysiology identified by careful preoperative exam-ination. Lateral retinacular release will provide goodresults when there is clinical and radiologic evidence ofpatellar tilt but will not consistently correct subluxation.51
Proximal medial imbrication may be helpful followinglateral release when there is injury to the medial patello-femoral ligament. Distal realignment is reserved formore profound levels of malalignment as well as articu-lar cartilage lesions. When there is anteromedializationof the tibial tubercle, decreased contact pressures areseen in the lateral facet of the patella. There is also a shiftin the contact pressures of the patella, both proximallyand medially.52 Therefore, prior to treatment it is criticalto understand the location of the articular cartilage de-fect to avoid increasing the load upon repair.
Cartilage repair options for the patellofemoral jointparallel those for the tibiofemoral joint, with some modi-fications in technique as well as postoperative regimens(Figure 8). A “demand-match” approach has been de-scribed, by which patient-specific factors are matchedwith cartilage restoration techniques.53 Patient-specificfactors include activity level, physiologic age, and gen-eralized laxity. Knee-specific factors include functionalstatus of the meniscus, alignment, and ligament status.Cartilage-specific factors include procedure cost, pri-mary repair versus salvage, lesion dimensions, lesiondepth, and degree of containment. The use of marrow-stimulation techniques, cell-based techniques, or osteo-chondral transfer must be considered and applied
according to treatment recommendations outlined inFigures 8 and 9 and discussed above.
Situation 8: Tibial Articular Cartilage Defects withoutMalalignment or Instability
Isolated articular cartilage defects of the tibial plateauare uncommon. Treatment is based on lesion size(Figure 8). However, access may require release of themedial collateral ligament as well as detachment ofmeniscal insertions.
Complex posttraumatic osteochondral defects of thetibial plateau secondary to trauma or avascular necrosisrequire osteochondral substitution. In 1 study, 89% ofpatients treated with osteochondral autografts for post-traumatic osteochondral defects of the tibial plateaudemonstrated good to excellent results at 2- to 5-yearfollow-up.54 Allograft tibial plateau substitution may beused in massive defects. The use of tibial plateau allo-graft allows for meniscal transplantation at the sametime. Concomitant osteotomy must be considered whenmalalignment is present but should not conflict withpostoperative protocols and may need to be staged.
Situation 9: Significant Chondropenia and Early OA(Figure 11)
Nonoperative management of early OA is multifactor-ial. Nonsteroidal anti-inflammatory medications are effec-tive for managing minor pain and inflammation presentin the early degenerative knee. Viscosupplementation,oral chondroprotective agents (glucosamine sulfate,chondroitin sulfate), physical therapy, and unloading
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
Figure 11. Bipolar lesions with full-thickness defects of themedial femoral condyle and medial tibial plateau. The diminishedcartilage volume seen in the surrounding areas is demonstrativeof chondropenia. (Adapted with permission from Scopp JM,Mandelbaum BR. A treatment algorithm for the management ofarticular cartilage defects. Orthop Clin North Am 2005;36:425.)
Figure 10. Arthroscopic image showing patellofemoral malalign-ment. This is demonstrated by contact of the patella with theridge of the lateral femoral condyle. (Adapted with permissionfrom Scopp JM, Mandelbaum BR. A treatment algorithm for themanagement of articular cartilage defects. Orthop Clin NorthAm 2005;36:425.)
braces provide effective nonoperative management in thechondropenic knee.55
Operative options include arthroscopy and osteot-omy. The use of arthroscopy in the chondropenic kneeis controversial but is most effective when mechanicalsymptoms exist for less than 6 months and there is neu-tral alignment with minimal radiographic evidence ofjoint degeneration.56 Tibial or femoral osteotomy maymaintain the patient’s active lifestyle and delay the needfor arthroplasty. Unicompartmental and total kneearthroplasty each can provide reliable relief of symp-toms but may not permit a return to the activities thatthe patient values.55
Situation 10: Degenerative Meniscal Tears with Late OA
Primary treatment should follow the regimen out-lined in situation 9. If the nonoperative measures fail,operative interventions should be considered. Theresults of arthroscopy for late OA (global grade IVchanges) are variable and unpredictable.55 Indicationsfor the use of arthroscopy, osteotomy, and arthroplastyare variable among practitioners, but each of theseoptions should be part of the therapeutic armamentar-ium for OA in the aging athlete.
REFERENCES
1. Curl WW, Krome J, Gordon ES, et al. Cartilage injuries: areview of 31,516 knee arthroscopies. Arthroscopy 1997;13:456–60.
2. Burks RT. Arthroscopy and degenerative arthritis of theknee: a review of the literature. Arthroscopy 1990;6:43–7.
3. Buckwalter JA, Einhorn TA, Simon SR. Orthopaedicbasic science: biology and biomechanics of the musculo-skeletal system. 2nd ed. Rosemont (IL): American Acad-emy of Orthopaedic Surgeons; 2000.
4. Potter HG, Linklater JM, Allen AA, et al. Magnetic reso-nance imaging of articular cartilage in the knee: An eval-uation with use of fast-spin-echo imaging. J Bone JointSurg Am 1998;80:1276–84.
5. Verzijl N, DeGroot J, Bank RA, et al. Age-related accu-mulation of the advanced glycation endproduct pentosi-dine in human articular cartilage aggrecan: the use ofpentosidine levels as a quantitative measure of proteinturnover. Matrix Biol 2001;20:409–17.
6. Bauer M, Jackson RW. Chondral lesions of the femoralcondyles: a system of arthroscopic classification. Arthros-copy 1988;4:97–102.
7. International Cartilage Repair Society. Cartilage injuryevaluation package. Available at www.cartilage.org/files/ICRS_evaluation.pdf. Accessed 29 Nov 2005.
8. Nomura E, Inoue M, Kurimura M. Chondral and osteo-chondral injuries associated with acute patellar disloca-
tion. Arthroscopy 2003;19:717–21.9. Clanton TO, DeLee JC. Osteochondritis dissecans. His-
tory, pathophysiology and current treatment concepts.Clin Orthop Relat Res 1982;(167):50–64.
10. Aichroth P. Osteochondritis dissecans of the knee. A clin-ical survey. J Bone Joint Surg Br 1971;53:440–7.
11. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecansof the knee: a historical review of etiology and treatment.Arthroscopy 1990;6(3):190-197
12. Green WT, Banks HH. Osteochondritis dissecans in chil-dren. J Bone Joint Surg Am 1953;35-A:26–47.
13. Clanton TO, DeLee JC. Osteochondritis dissecans. His-tory, pathophysiology and current treatment concepts.Clin Orthop Relat Res 1982;(167):50–64.
14. Cahill BR, Berg BC. 99m-Technetium phosphate com-pound joint scintigraphy in the management of juvenileosteochondritis dissecans of the femoral condyles. Am JSports Med 1983;11:329–35.
15. Nelson DW, DiPaola J, Colville M, Schmidgall J. Osteo-chondritis dissecans of the talus and knee: prospectivecomparison of MR and arthroscopic classification. J Comput Assist Tomogr 1990;14:804–8.
16. DePalma, AF, McKeever CD, Subin DK. Process of repairof articular cartilage demonstrated by histology and auto-radiography with tritiated thymidine. Clin Orthop RelatRes 1966;48:229–42.
17. Mitchell N, Shepard N. The resurfacing of adult rabbitarticular cartilage by multiple perforations through thesubchondral bone. J Bone Joint Surg Am 1976;58:230–3.
18. Schenck RC Jr, Goodnight JM. Osteochondritis disse-cans. J Bone Joint Surg Am 1996;78:439–56.
19. Linden B. Osteochondritis dissecans of the femoral con-dyles: a long-term follow-up study. J Bone Joint Surg Am1977;59:769–76.
20. Wilson JN. A diagnostic sign in osteochondritis dissecansof the knee. J Bone Joint Surg Am 1967;49:477–80.
21. Loeuille D, Olivier P, Mainard D, et al. Review: Magneticresonance imaging of normal and osteoarthritic carti-lage. Arthritis Rheum 1998;41:963–75.
22. Yulish BS, Montanez J, Goodfellow DB, et al. Chondro-malacia patellae: assessment with MR imaging. Radiology1987;164:763–6.
23. Lequesne MG, Mery C, Samson M, Gerard P. Indexes ofseverity for osteoarthritis of the hip and knee. Validation—value in comparison with other assessment tests [publishederrata appear in Scand J Rhematol 1988;17:following 241and 1988;73:1]. Scand J Rheum Suppl 1987;65:85–9.
25. Drape JL, Pessis E, Auleley GR, et al. Quantitative MR imag-ing evaluation of chondropathy in osteoarthritic knees.Radiology 1998;208:49–55.
26. Eckstein F, Westhoff J, Sittek H, et al. In vivo reproducibilityof three-dimensional cartilage volume and thickness mea-surements with MR imaging. AJR Am J Roentgenol 1998;
www.turner -white.com Orthopaedic Sports Medicine Volume 2, Part 3 11
O s t e o c h o n d r a l I n j u r y o f t h e K n e e
170:593–7.27. McNicholas MJ, Brooksbank AJ, Walker CM. Observer
agreement analysis of MRI grading of knee osteoarthri-tis. J R Coll Surg Edinb 1999;44:31–3.
28. Waldschmidt JG, Braunstein EM, Buckwalter KA. Mag-netic resonance imaging of osteoarthritis. Rheum Dis ClinNorth Am 1999;25:451–65.
29. Dunn WR, Lyman S, Lincoln AE, et al. The effect of ante-rior cruciate ligament reconstruction on the risk of kneereinjury. Am J Sports Med 2004;32:1906–14.
30. Cerejo R, Dunlop DD, Cahue S, et al. The influence ofalignment on risk of knee osteoarthritis progressionaccording to baseline stage of disease. Arthritis Rheum2002;46:2632–6.
31. Scopp JM, Mandelbaum BR. A treatment algorithm forthe management of articular cartilage defects. OrthopClin North Am 2005;36:419–26.
32. Caffey S, McPherson E, Moore B, et al. Effects of radiofre-quency energy on human articular cartilage: an analysisof 5 systems. Am J Sports Med 2005;33:1035–9.
33. Nishida Y, Knudson CB, Eger W, et al. Osteogenic protein1 stimulates cells-associated matrix assembly by normalhuman articular chondrocytes: up-regulation of hyalur-onan synthase, CD44, and aggrecan. Arthritis Rheum2000;43:206–14.
34. Loeser RF, Pacione CA, Chubinskaya S. The combinationof insulin-like growth factor 1 and osteogenic protein 1promotes increased survival of and matrix synthesis bynormal and osteoarthritic human articular chondrocytes.Arthritis Rheum 2003;48:2188–96.
35. Chan PS, Caron JP, Rosa GJ, Orth MW. Glucosamine andchondroitin sulfate regulate gene expression and synthe-sis of nitric oxide and prostaglandin E(2) in articular car-tilage explants. Osteoarthritis Cartilage 2005;13:387–94.
36. St-Pierre DM. Rehabilitation following arthroscopicmeniscectomy. Sports Med 1995;20:338–47.
37. Vervest AM, Maurer CA, Schambergen TG, et al. Effec-tiveness of physiotherapy after meniscectomy. Knee SurgSports Traumatol Arthrosc 1999;7:360–4.
38. Steadman JR, Briggs KK, Rodrigo JJ, et al. Outcomes ofmicrofracture for traumatic chondral defects of theknee: average 11-year follow-up. Arthroscopy 2003;19:477–84.
39. Gobbi A, Nunag P, Malinowski K. Treatment of full thick-ness chondral lesions of the knee with microfracture in agroup of athletes. Knee Surg Sports Traumatol Arthrosc2005;13:213–21.
40. Hangody L, Fules P. Autologous osteochondral mosaic-plasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and clinical ex-perience. J Bone Joint Surg Am 2003;85-A Suppl 2:25–32.
41. Peterson L, Brittberg M, Kiviranta I, et al. Autologous chon-drocyte transplantation. Biomechanics and long-termdurability. Am J Sports Med 2002;30:2–12.
42. Allen RT, Robertson CM, Pennock AT, et al. Analysis ofstored osteochondral allografts at the time of surgical im-plantation. Am J Sports Med 2005;33:1479–84.
43. Berlet GC, Mascia A, Miniaci A. Treatment of unstableosteochondritis dissecans lesions of the knee using auto-genous osteochondral grafts (mosaicplasty). Arthroscopy1999;15:312–6.
44. Peterson L, Minas T, Brittberg M, Lindahl A. Treatmentof osteochondritis dissecans of the knee with autologouschondrocyte transplantation: results at two to ten years. J Bone Joint Surg Am 2003;85-A Suppl 2:17–24.
45. Cahill B. Treatment of juvenile osteochondritis dissecansand osteochondritis dissecans of the knee. Clin SportsMed 1985;4:367–84.
46. Gillogly SD, Myers TH. Treatment of full-thickness chon-dral defects with autologous chondrocyte implantation.Orthop Clin North Am 2005;36:433–46.
47. Post WR. Patellofemoral pain: results of nonoperativetreatment. Clin Orthop Relat Res 2005;(436):55–9.
48. Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effec-tiveness of a neuromuscular and proprioceptive trainingprogram in preventing anterior cruciate ligament in-juries in female athletes: 2-year follow-up. Am J SportsMed 2005;33:1003–10.
49. Dye SF, Staubli HU, Biedert RM, et al. The mosaic ofpathophysiology causing patellofemoral pain: therapeu-tic implications. Oper Tech Sports Med 1999;7:46–54.
50. Schonholtz GJ, Zahn MG, Magee CM. Lateral retinacu-lar release of the patella. Arthroscopy 1987;3:269–72.
51. Fulkerson JP, Schutzer SF, Ramsby GR, Bernstein RA.Computerized tomography of the patellofemoral jointbefore and after lateral release or realignment. Arthros-copy 1987;3:19–24.
52. Fulkerson JP, Becker GJ, Meaney JA, et al. Anteromedialtibial tubercle transfer without bone graft. Am J SportsMed 1990;18:490–7.
54. Ma HL, Hung SC, Wang ST, et al. Osteochondral auto-grafts transfer for post-traumatic osteochondral defect ofthe knee—2 to 5 years follow-up. Injury 2004;35:1286–92.
55. Cole BJ, Harner CD. Degenerative arthritis of the kneein active patients: evaluation and management. J AmAcad Orthop Surg 1999;7:389–402.
56. Hunt SA, Jazrawi LM, Sherman OH. Arthroscopic man-agement of osteoarthritis of the knee. J Am Acad OrthopSurg 2002;10:356–63.