84
Welcome! 10 th anniversary event Wednesday, January 31 st 2018 Mont-Saint-Guibert

Welcome!10th anniversary event
Wednesday, January 31st 2018 Mont-Saint-Guibert

Welcome
Serge GobletBoard Member

Introduction
Michel Lussier MS BME, MBAChairman of the Board

Agenda & Speakers
4
5:30 – 7:00pm Presentations• Welcome, by Serge Goblet, Member of the Board of Directors, Celyad• Introduction and agenda, by Michel Lussier MS BME, MBA, Chairman of the Board of Directors, Celyad• Cancer and Celyad’s technology, by Sophie Agaugue, PhD, R&D Manager, Celyad• 2017 Progress and Learnings , by Christian Homsy, MD, MBA, CEO, Celyad• AML and Celyad’s potential, by Xavier Poire, MD, Service Hématologique Adulte, Institut Roi Albert II,
Clinique universitaire de St-Luc• CYAD-01 rationale in colorectal cancer, by Alain Hendlisz, MD, PhD, Head of the Gastro-Enterology Unit,
Medical Oncology Clinic, Jules Bordet Institute• Celyad’s Clinical Development Plan, by Frédéric Lehmann, MD, PhD, VP of Clinical Development
&Medical Affairs, Celyad• Celyad’s R&D strategy, by Peggy Sotiropoulou, PhD,R&D Manager, Celyad• Celyad’s SNOWY project, by Valérie Steenwinckel, PhD, Industrialization Director, Celyad• 2017 – Progress and learnings, by Christian Homsy, MD, MBA, CEO, Celyad• Willy Borsus, Minister-President of Wallonia• Closing, by Christian Homsy, MD, MBA, CEO, Celyad• Q&A
7:00 – 9:00pm Cocktail & Networking

Forward looking statements
Forward-looking statements In addition to historical facts or statements of current condition, this presentation contains forward-looking statements, including statements about the potentialsafety and feasibility of CYAD-01 cell therapy, including current and planned preclinical and clinical trials for Celyad’s product candidates; the clinical and commercialpotential of these product candidates and the adequacy of Celyad’s financial resources; Celyad’s intellectual property portfolio, including plans related thereto;Celyad’s expectations regarding its strategic collaborations and license agreements with third parties, including Novartis, Celdara Medical, and Dartmouth College,and the potential impact of such collaborations on Celyad’s future financial condition; and Celyad’s expected cash burn, which reflect Celyad’s current expectationsand projections about future events, and involve certain known and unknown risks, uncertainties and assumptions that could cause actual results or events to differmaterially from those expressed or implied by the forward-looking statements. These forward-looking statements are further qualified by important factors andrisks, which could cause actual results to differ materially from those in the forward-looking statements, including risks associated with conducting clinical trials; therisk that safety, bioactivity, feasibility and/or efficacy demonstrated in earlier clinical trials or preclinical studies may not be replicated in subsequent trials or studies;risks associated with the timely submission and approval of anticipated regulatory filings; the successful initiation and completion of clinical trials, including its clinicaltrials for CYAD-01; risks associated with the satisfaction of regulatory and other requirements; risks associated with the actions of regulatory bodies and othergovernmental authorities; risks associated with obtaining, maintaining and protecting intellectual property, Celyad’s ability to enforce its patents against infringersand defend its patent portfolio against challenges from third parties; risks associated with competition from others developing products for similar uses; risksassociated with Celyad’s ability to manage operating expenses; and risks associated with Celyad’s ability to obtain additional funding to support its business activitiesand establish and maintain strategic business alliances and business initiatives. A further list and description of these risks, uncertainties and other risks can be foundin Celyad’s U.S. Securities and Exchange Commission (SEC) filings and reports, including in its Annual Report on Form 20-F filed with the SEC on April 4, 2017 andsubsequent filings and reports by Celyad. Given these uncertainties, the reader is advised not to place any undue reliance on such forward-looking statements. Theseforward-looking statements speak only as of the date of publication of this document. Celyad expressly disclaims any obligation to update any such forward-lookingstatements in this document to reflect any change in its expectations with regard thereto or any change in events, conditions or circumstances on which any suchstatement is based, unless required by law or regulation.
5
We kindly remind you that this presentation will be video recorded. The video will be posted on Celyad’s website shortly after the event.

Cancer and Celyad’s technology
Sophie Agaugue, PhDR&D Manager
6

What is cancer ?
02/02/2018 7
Normal cells grow, divideand die in an orderly fashion
02/02/2018 7
Cancer cells do not die, they just grow and divide in an uncontrolled way
Genetic, environmental factors
2 types of cancer: solid and liquid

A tumor is a micro-environment by itself
Primary tumor
Metastases
02/02/2018 8

How does the immune system fight against cancer ?
02/02/2018 9
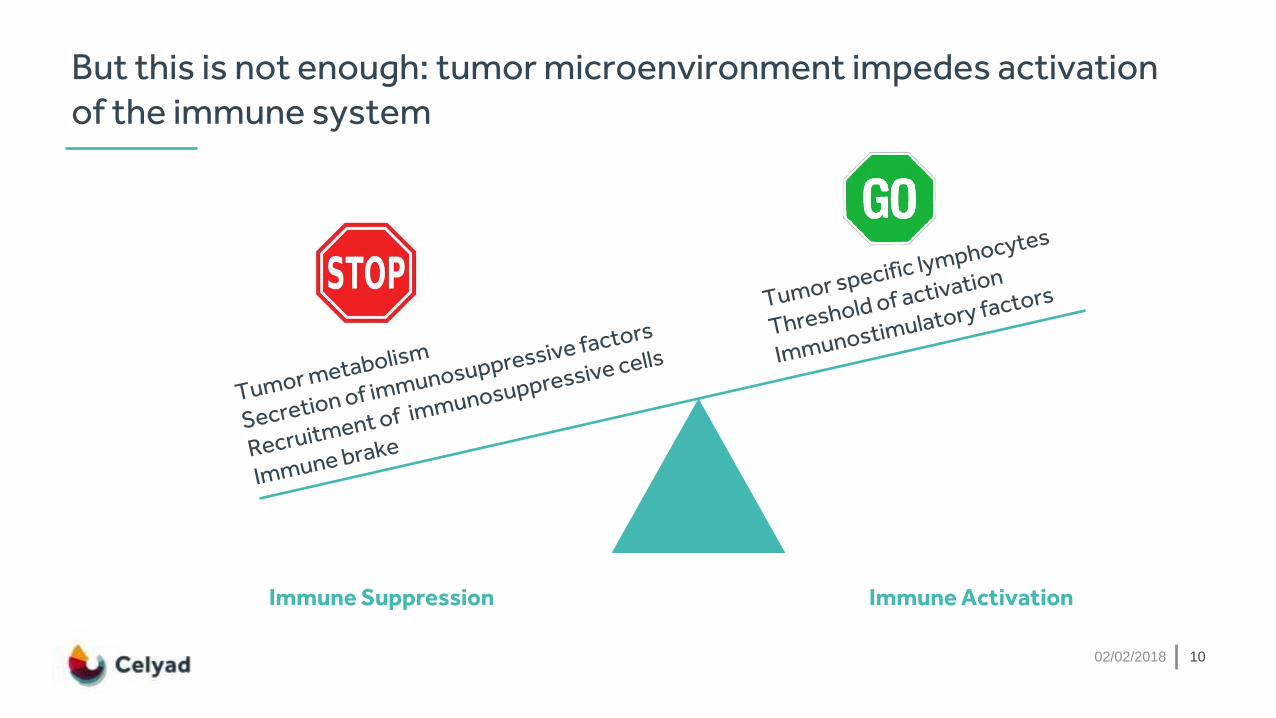
But this is not enough: tumor microenvironment impedes activation of the immune system
Immune Suppression Immune Activation
02/02/2018 10

How to make our own immune cells fight cancer ? The explosion of immunotherapy
Antibody approach: Breaks the tumor inhibitoryeffect on immune system
Cellular approach: Accelerates the immune effect against the tumor
02/02/2018 11
Tumorantigen

T-cells need to be “armed” to fight Cancer
CAR-T cells =tumor specific –
gene modified T-cells
Issues: low frequency of tumorspecific T-cells in patientsNo good tumor specific antigen to select T-cells
02/02/2018 12

How to « arm » a T-cell: standard CAR-T construct
ChimericAntigenreceptor
scFV (single chain variable
fragment)
Signalling domain
Chimeric Antigen Receptor (CAR) T-cell
02/02/2018 13

CD19 CAR-T: an extraordinary technology that has now come to the market
02/02/2018 14

CYAD-01 a unique CAR-T combining properties of NK and T cells
CYAD-01: a unique construct only developed at Celyad in clinical development
+
02/02/2018 15

A Single NK Cell Receptor Binding 8 Different Ligands expressed in the majority of tumors
02/02/2018 16
Cancer type Expression of at least one NKG2D ligand
Bladder carcinoma 96% (mets 100%)
TNBC 100%
Colorectal cancer 100%
Ovarian carcinoma 84%
Pancreatic cancer 90%
Lung cancer (NSCLC) 100%
AML 100%Dulphy et al unpublished data
Celyad’s unpublished data

CYAD-01 cells destroy diverse types of tumors and prolong survival of mice
PANCREATIC CANCER
Demoulin et al. Future Oncology 2017
02/02/2018 17
Barber et al. 2009, J Immunol
OVARIAN CARCINOMA
Zhang et al. 2007, Cancer Res
LYMPHOMA

Beyond direct killing, inducing multifaceted attack on the tumor
02/02/2018 18
Lonez et al., BMJ Open, 2017

2017 – Progress and learnings
Christian Homsy, MD, MBACEO
19

THINK Trial
20
▪ First patients in January 2017▪ First experience in oncology
▪ 3 administrations▪ Primary Endpoint: Safety &Tolerability▪ Secondary Endpoint: Efficacy as
Monotherapy (w/o preconditioning)▪ Hematological & solid tumors
THINK Study (THerapeutic Immunotherapy w/ NKG2D-based therapy)
▪ Seven advanced refractory tumor indications
▪ Global development: EU and USA
o 3 dose levels (3x108,1x109 and 3x109)
Apheresis
1st CYAD-01 (D1)2nd CYAD-01 (D2)
3rd CYAD-01 (D3)
End safety
D1 D15 D29
Tumor assessment
D43 D57D-21
Washout period
13 weeks w/o any other non-investigational cancer therapy
D-35

Total: 15 patients (10 at pre-defined dose)
- All adverse events are unrelated to CYAD-01- No critical toxicity events related to date
> THINK confirms the safety profile of CYAD-01
THINK study: Status Report
21
THINK Trial
Safety

Total: 15 patients (10 at pre-defined dose)
- Further improvement of manufacturing process achieved- First dose of dose-level 3 produced & administered> Celyad’s manufacturing process optimized
THINK study: Status Report
22
THINK Trial
Feasibility

Total: 15 patients (10 at pre-defined dose)
- Hematological arm: CYAD-01 active in 3/3 AML patients (w/o pre-conditioning): - 1 MLFS – World Premiere- All blast reduction during treatment- All hematological improvements
- Solid arm: CYAD-01 resulted in 2 out of 4 Stable Diseases for CRC patients and 1 ovarian cancer
- 6 patients out of 10 treated at the per-protocol dose reached Stable Disease (SD) till Complete Response (CR)
> THINK validates the activity of NKG2D
THINK study: Status Report
23
THINK Trial
Clinical activity

Complete dose escalation
Plan expansion phase with second cycle of treatmentpotentially improving response durability
Going forward
24
THINK Trialin 2018
Hematological Solid
3 new studies 3 new studies

Acute Myeloid Leukemia(AML)
Xavier Poiré, MDUnité de greffe médullaire
Service d’Hématologie Adulte
Institut Roi Albert II
Cliniques Universitaires St-Luc (Bruxelles)
25

Acute Myeloid LeukemiaWhere are we and where are we going to?
Xavier Poiré, MDUnité de greffe médullaire
Service d’Hématologie AdulteInstitut Roi Albert II
Cliniques Universitaires St-LucBruxelles
31/01/2018

Normal hematopoiesis
X. Poiré, 31/01/2018 27

Cellular division and leukemogenesis
X. Poiré, 31/01/2018 28
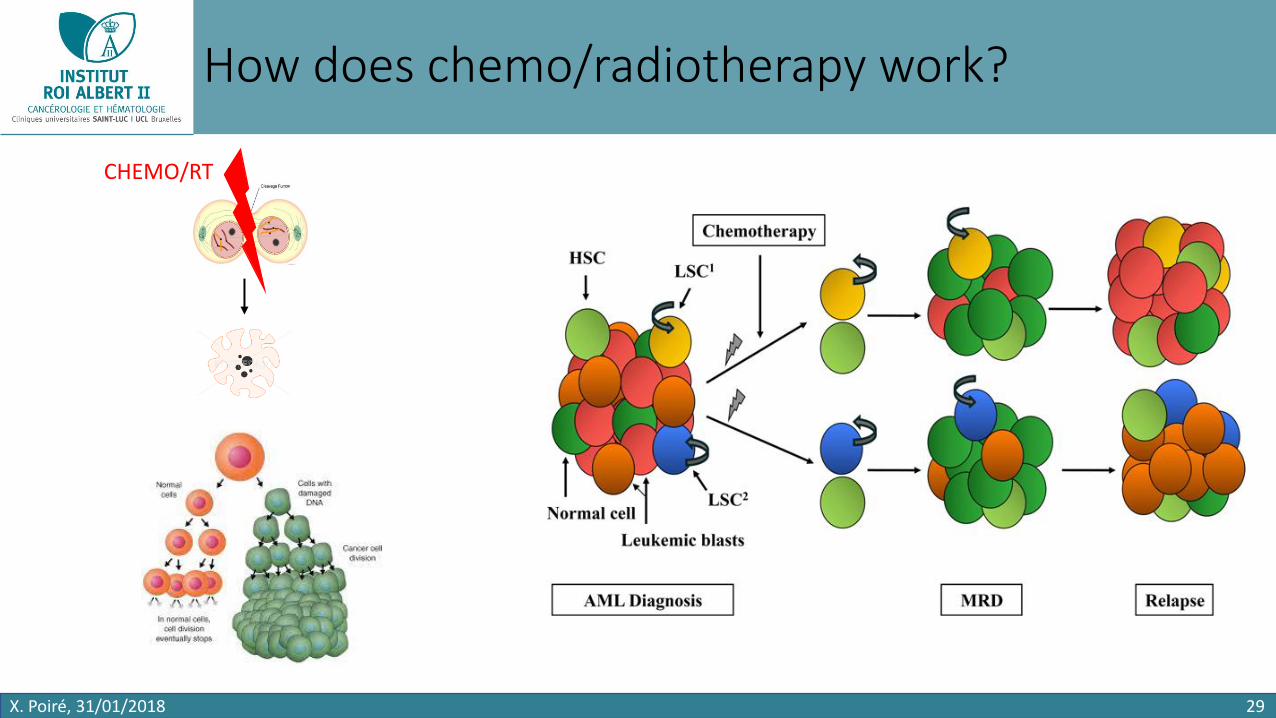
How does chemo/radiotherapy work?
X. Poiré, 31/01/2018 29
CHEMO/RT

Induction and consolidation therapies
X. Poiré, 31/01/2018 30
INDUCTION CONSOLIDATION
Normal hematopoiesis
Leukemic cells
4-6 weeks
GOOD LEUKEMIA
BAD LEUKEMIA
60-70% SURVIVAL
10-20% SURVIVAL

Allogeneic stem cell transplantation
X. Poiré, 31/01/2018 31
BAD LEUKEMIA
NORMAL STEM CELLS
IMMUNE CELLS

Allogeneic stem cell transplantation
X. Poiré, 31/01/2018 32
Conditionnement Greffe Prévention GvHD
ChimioRadiothérapie
ImmunosuppressionGlobules blancs
Aplasie
Diarrhée
MuciteFièvre
Transfusion
4-6 weeks
Relapse?
50% SURVIVAL
DLI
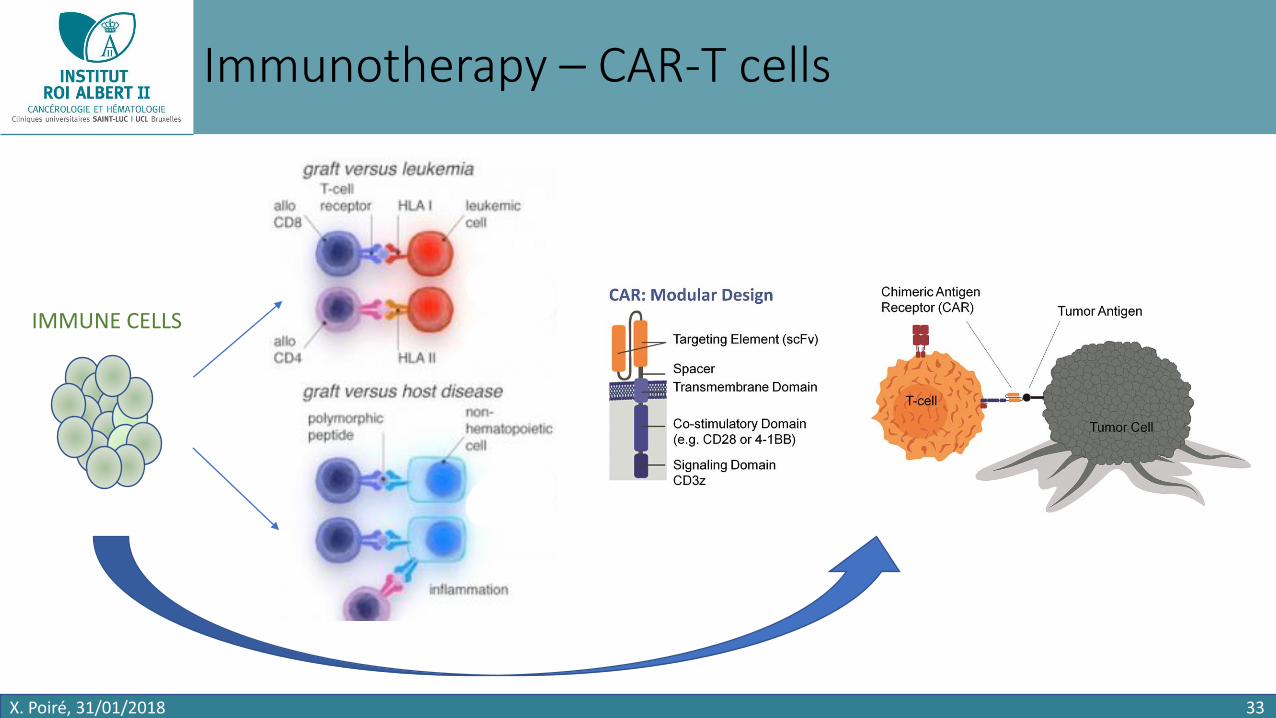
Immunotherapy – CAR-T cells
X. Poiré, 31/01/2018 33
IMMUNE CELLS

CAR-T cells – does it work?
X. Poiré, 31/01/2018 34
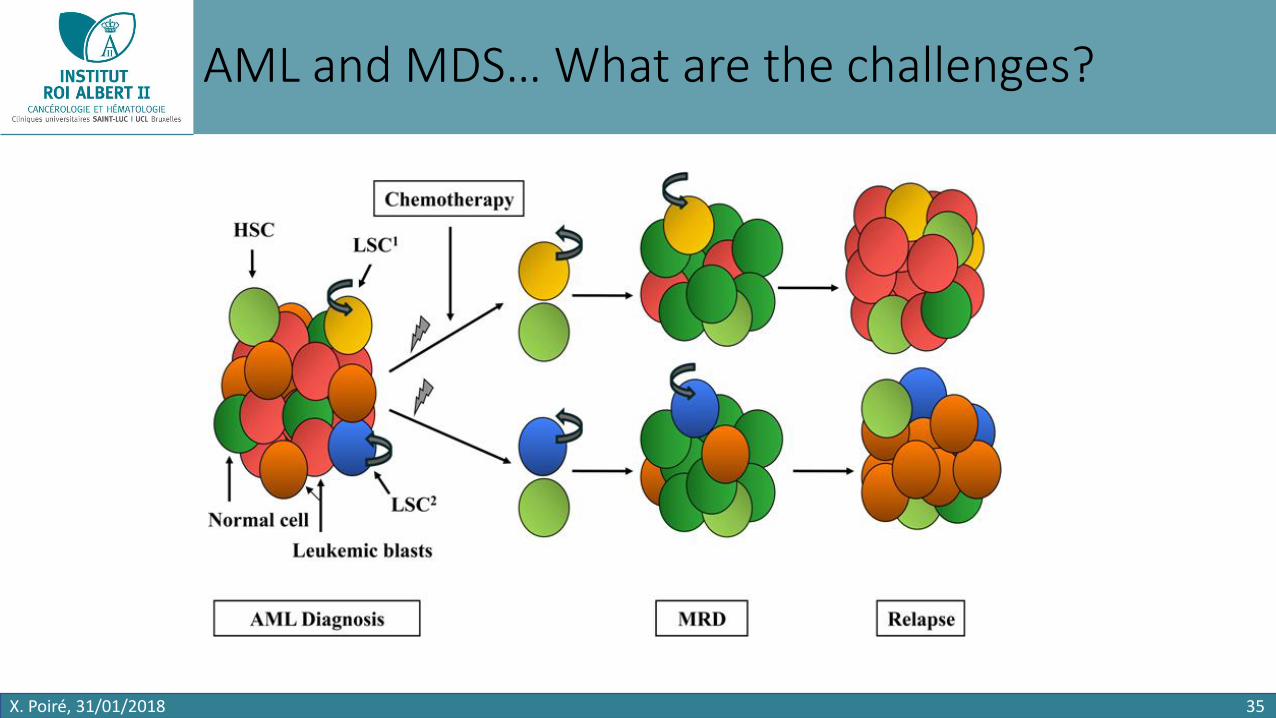
AML and MDS… What are the challenges?
X. Poiré, 31/01/2018 35

NKG2D CAR-T cells
X. Poiré, 31/01/2018 36

NKG2D CAR-T cells – Does it work in AML/MDS?
X. Poiré, 31/01/2018 37
+8/del(7)(q22q36), FLT3/NPM1 wild-type DNMT3A mutation
Normal cytogenetics46,XY,i(7)(p10)[2]/46,XY[18]DNMT3A/IDH2 mutations
46,XY,i(7)(p10)[3]/46,XY[17]
Negative NGS pannel

Advanced ColoRectal Cancer: the path towards
Immunotherapies
Alain HENDLISZ MD, PhD
Head of the Gastro-Enterology Unit, Medical Oncology Clinic
Jules Bordet Institute

+
Alain Hendlisz
Institut Jules Bordet, Université Libre de BruxellesNovembre 2017
Advanced ColoRectal Cancer: the path towards Immunotherapies

Colorectal Cancer: Belgian Overview
4607 men
3597 women
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
Incidence
CRC incidence in men and women
Total: 8204
CRC is 3rd most common cancer in men &
2nd most common cancer in women
* Belgian Cancer Registry, Cancer Incidence in Belgium 2011, available at http://www.kankerregister.org
Belgian Registry 2012

CRC STAGE TREATMENT5-YEAR SURVIVAL
RATE (%)
Stage I • Surgery 74
Stage II• Surgery• Chemotherapy
37-67
Stage III• Surgery• Chemotherapy
28-73
Stage IV• Cryo- or radiofrequency ablation• Chemotherapy• Targeted therapy
6
5%
39%
36%
20%
Localized
Regional
Distant
Unknown
CRC Stage at Diagnosis
Colorectal Cancer: stages & survival
Schmoll Ann Oncol 2012ASCO www.cancer.org 2012

+ ESMO Guidelines
Van Cutsem et al. Ann Oncol. 2014
L1
L2
L3
L3

mCRC: Treatments over Time
0 10 20 25
SURVIE GLOBALE (MOIS)
155 30 35 40 45
Saltz1
Goldberg3
Saltz5
Bokemeyer7
Saltz1
Douillard2
Hurwitz4
Falcone6
Douillard2
Douillard9
Van Cutsem8
Passardi10
5-FU/LV bolus 12.6
FOLFOX 19.5
XELOX/FOLFOX + bevacizumab NO16966 21.3
FOLFOX + cetuximab OPUS (KRAS) 22.8
IFL 14.8
5-FU/LV infusion 14.1
IFL + bevacizumab AVF2107g 20.3
FOLFOXIRI Italian GONO Trial 22.6
FOLFIRI 17.4
FOLFOX + panitumumab PRIME (KRAS) 23.9
FOLFIRI + cetuximab CRYSTAL (KRAS) 23.5
FOLFOX or FOLFIRI ITACA 20.6
FOLFOX or FOLFIRI + bevacizumab ITACA 20.6
Stintzing14
Schwartzberg13mFOLFOX6 + bevacizumab PEAK (RAS) 28.9
mFOLFOX6 + panitumumab PEAK (RAS) 41.3
FOLFIRI + bevacizumab FIRE-3 (RAS) 25.0
FOLFIRI + cetuximab FIRE-3 (RAS) 33.1
Lenz15FOLFOX or FOLFIRI + bevacizumab CALGB 80405 (RAS) 31.2
FOLFOX or FOLFIRI + cetuximab CALGB 80405 (RAS) 32.0
Bokemeyer12
Ciardiello11
FOLFOX + cetuximab OPUS (RAS) 19.8
FOLFIRI + cetuximab CRYSTAL (RAS) 28.2
2014
2014
2014
2000
2004
2008
2011
2000
2000
2004
2007
2000
2011
2011
2014
2013
2014
1. Saltz. NEJM 2000. 2. Douillard. Lancet 2000. 3. Goldberg. J Clin Oncol 2004 4. Hurwitz. NEJM 2004 5. Saltz. J Clin Oncol. 2008 6. Falcone J Clin Oncol 2007
7. Bokemeyer. Ann Oncol 2011 8. Van Cutsem. J Clin Oncol 2011. 9. Douillard. J Clin Oncol 2011 10. Passardi. J Clin Oncol 31, 2013 11. Ciardiello. J Clin Oncol 2014 12. Bokemeyer. J Clin Oncol 2014 13. Schwartzberg. J Clin Oncol. 2014 14. Stintzing. Ann Oncol 2014 15. Lenz. Ann Oncol. 2014

Median Survival29,8 months
(95% CI 26·0–34·3)
Median Survival25,8 months(22·5–29·1)
Cremolini et al, Lancet Oncol 2015
Metastatic ColoRectal Cancerdifferent valid strategies

+
Koopman, Lancet 2007
CAIRO 1 trial
Metastatic ColoRectal Cancerdifferent strategies-same results
Median survival17.4 mo
(95% CI15.2–19.2)
Median survival16.3 mo
(95% CI 14.3–18.1)
HR 0.92 (95% CI 0.79–1.08)
p=0.3281

mCRC
Non Resectable
65%
Resectable
15%
AggressiveTreatment
Response
ConservativeTreatment
Control
Therapeutic Strategies
Maybe Resectable
20%
Palliative Treatment
75 + 20 %5%
Cure

Strategy influences Treatment: ‘Why’ comes before ‘How’
Metastatic ColoRectal Cancer:
Defining Principles of Chemotherapy
Principle nr 1
Principle nr 2 Use all drugs available
Principle nr 3 Efficacy and Toxicity with number of drugs combined
Primum non nocere

+
Koopman, Lancet 2007
CAIRO 1 trial
Metastatic ColoRectal CancerLong-Term Results Disappointing
Median survival17.4 mo
(95% CI15.2–19.2)
Median survival16.3 mo
(95% CI 14.3–18.1)
HR 0.92 (95% CI 0.79–1.08)
p=0.3281

Active immunotherapy
Adoptive cell transferimmunotherapy
IL-2IFNIL-15IL-21
Peptide vaccineDC vaccineGenetic vaccine
OX40
CD137
CD40
PD-1
CTLA-4
T cell cloningTCR or CAR
genetic engineering
General Approaches for Cancer Immunotherapy

Pembrozilumab in metastatic CRC
Le DT NEJM 2015

Checkmate 142: Nivolumab & Ipilimumab MSI-H mCRC
Overman et al J Clin Oncol 2018
MSI = 5-10 % of the mCRC patients

140 2 4 6 8 10 12
Weber et al. J Clin Oncol 2012 & 2015
Toxicity Immune Checkpoint Inhibitors
Rash, pruritusLiver toxicityDiarrhea, colitisHypophysitis
Wks
Toxi
city
Gra
de
+ CONCLUSIONS
mCRC remains major Health Issue in Industrialized World
Huge Progresses in Therapeuties allow Treatment Personnalization
Hope in Immunotherapies but currently only for MSI-H patients
Promising new immunotherapies are currently being explored

What is next?

CYAD-01Clinical Development
Frédéric Lehmann, MD, PhDVP of Clinical Development & Medical Affairs

56
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Hematological indications Solid cancer indications
CYAD-01: Clinical Development Plan Overview
• r/r AML patient has reached a MLFS with CYAD-01 withoutpre-conditioning lymphodepletion
• Reinforces confidence and the validity of NKG2D ligands as a target
THINK Study Stand alone THINK Study
1st objective clinical responsein the Phase I dose escalation
(1st dose-level)

57
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Hematological indications
CYAD-01: Clinical Development Plan Overview
Solid cancer indicationsOverall Safety Overview
CYAD-01 (aka NKR-2 CAR-T)

58
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Hematological indications
CYAD-01: Clinical Development Plan Overview
THINK Study
Hematological indications
• Safety: No DLT at dose-level 1
• 2nd dose-level (1.109/dose) ongoing
Data as of December 31, 2017
• Clinical status

59
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Solid cancer indications
THINK Study
Solid cancer indications
• Safety: No DLT at dose-level 1&2
• 3rd dose-level (3.109/dose) activated
CYAD-01: Clinical Development Plan Overview
• Clinical status
Two out of four metastatic colorectal cancer patients treated at per-protocol dose reported as“stable disease” up to 3-months follow-up*+
* Median progression free survival in these patients under standard of care is between 1.9 and 3.2 months(e.g. regorafinib or trifluridine/tipiracil).
+ Fifth CRC patient treated at a dose lower then per-protocol dose did not show signs of clinical activity

60
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Solid cancer indications
THINK Study
Hematological indications
THINK Study Stand alone
CYAD-01: Clinical Development Plan Overview
Protocol Amendment
Increase the durability of the early signs of clinical activity
by increasing the number of CYAD-01 injections (>3)

61
CYAD-01 (aka NKR-2 CAR-T)
Multiple cancer indications
Solid cancer indications
THINK Study
Hematological indications
THINK Study Stand alone
AML-SHRINK Study
DEPLETHINK StudySIBLINK Study
SHRINK Study
DEPLETHINK Study
LINK Study
Concurrent with SoC
Preconditioning (CY-Flu)
Loco-regional
2018
CYAD-01: Clinical Development Plan Overview

CYAD-01 (aka NKR-2 CAR-T)
CYAD-01: Clinical Development Plan Overview
AML-SHRINK Study SHRINK StudyConcurrent with SoC
1. Immediate tumor debulking by the standard of care
2. Synergism effect by combination standard treatment and CYAD-01
• Increase the NKG2D ligand expression on tumor tissues
• Better proliferation & expansion of CYAD-01 due to the lymphopenia status
• Better CYAD-01 infiltration into the tumor environment
• Induce an antigen spreading boosting the adaptive memory immune response
Open-label dose escalation Phase I study
Multiple IV administrations of CYAD-01, concurrently with standard therapy for a specific disease
62

CYAD-01 (aka NKR-2 CAR-T)
CYAD-01: Clinical Development Plan Overview
DEPLETHINK StudySIBLINK Study
DEPLETHINK StudyPreconditioning (CY-Flu)
1. Evaluate the “standard” lymphodepletion preconditioning (CAR-T paradigm )
2. Increase the CYAD-01 expansion and persistence
3. Improve anti-tumor activity/synergism effect
Open-label dose escalation Phase I study
CYAD-01 + Preconditioning lymphodepletion chemotherapy
Phase I refractory cancer pts
63

CYAD-01 (aka NKR-2 CAR-T)
CYAD-01: Clinical Development Plan Overview
LINK StudyLoco-regional
Open-label dose escalation Phase I study
Multiple hepatic transarterial administrations
Unresectable liver metastases from colorectal cancer pts
1. Lower systemic toxicity
2. Higher and persistent concentration of
the CYAD-01 infused cells into the tumor
64

Multiple cancer indications
CYAD-01 (aka NKR-2 CAR-T)CYAD-01 (aka NKR-2 CAR-T)
CYAD-01: Integrated Clinical Development with data end 2018
65

What lies ahead
Peggy Sotiropoulou, PhDR&D Manager

02/02/2018 67
1st Challenge: Fratricide in vitro and in vivo
CYAD-01
NKG2D
CYAD-01
NKG2D
NKG2DLNKG2DL
Self-fratricide
(suicide)
Fratricide
(canibalism)

CYAD-01
NKG2D
NKG2DL CYAD-01
NKG2D
NKG2DL
CD314
68
Self-fratricide
(suicide)
Fratricide
(canibalism)
• No in vitro fratricide
• Production of required amount of cells made possible
CYAD-01
NKG2D
NKG2DL
CYAD-02: Elimination of ligands
CYAD-01
NKG2D
NKG2DLs
CYAD-01
NKG2D

Autologous
CAR-T cellproduction
Infusion
2nd Challenge: Time-consuming process in the autologous setting
Allogeneic
CAR-T cellproduction
Off the shelfCAR T CAR TCAR T CAR T CAR T CAR T

02/02/2018 70
Alloreactivity controlled through co-expression of an inhibitory peptide (termed a T-cell
receptor inhibitory molecule – TIM) to reduce TCR-signaling and thereby reduce GvHD.
CYAD-101: Allogeneic approach of CYAD-01

71
3rd ChallengeTo increase efficacy of CAR T therapy in solid tumors
Hartman et al,
EMBO Mol Med 2017He
ma
top
oie
tic
So
lid

02/02/2018
Homing InfiltrationFace
immunosuppressive microenvironment
Targeting tumour heterogeneity
CYAD-03NKG2D CAR-T cells in solid and recalcitrant tumors
Mig
ratio
n to
ward
s th
e tu
mo
ur
Tumor-
tropic
factors

What is next?Automation,
towards a new paradigm
Valerie Steenwinckel, PhDIndustrialization Director

Intensely Focused on Manufacturing Improvements in Anticipation of Commercial Ready Product
74
• Evolution from drug product manufactured in academic setting (DFCI) towards a commercial-ready process that is reproducible and scalable, with attractive COGs
• Legacy method (LY process) failed to consistently yield drug product with target T cell numbers
• Of 15 patients treated at December 31, 2017, 10 were dosed at per-protocol intended dose and 5 were treated at lower doses
• New manufacturing process is currently being used in the clinic
• mAb manufacturing process inhibits NKG2D expression on the T cell surface during production• Enables significantly higher cell numbers than the legacy process• Validated in both in vivo and ex vivo models• CMC amendments to THINK protocol are in effect with applicable regulators• First patient treated January 2018
• Continued focus on next-generation process improvements, including automated and closed system approach
Celyad would like to develop an automated machine that will allow to bring CAR-T cell therapies to all patients in the most cost effective and efficient manner.
02/02/2018 75
Automation Program Mission

Why it is important to automate?
• Ease of manufacturing
• Increase reproducibility
• Reduce time of manipulation
• Ease of Tech transfer to potential other sites
• Decrease batch failure (human error)
• Cost of good reduction
• Less operator time per batch
• Less environmental needs/control
02/02/2018 76
• Scalability
• Increased capacity of centralized manufacturing approach
• Footprint
• Parallel processing
• Possibility adapt to market demand
• De-centralized model
• Point of Care approach (machine in hospital)

To treat large number of patients Celyad needs to automate and close the production process
02/02/201877
Ideal features of the machine:
• Automated with closed system from start to end
• Minimal Operator interactions
• Ultra Low batch failure
• Parallel batch production
• Ultra-low cost of Goods of disposable
• Able to evolve towards point of care when market will growth
...Like GMP in a box

Celyad has already evaluated the close system manufacturing options
• Evaluated and selected the core technologies that could be used to automate our CAR-T process (ex: washing, concentration,…)
• Tested the complete concept with a prototype (in house)
• Mature the concept to be compatible with PoC: cartridge based approach with parallel processing
02/02/2018 78
Example of cartridge and machine

Conclusion
Christian Homsy, MD, MBA
CEO
79
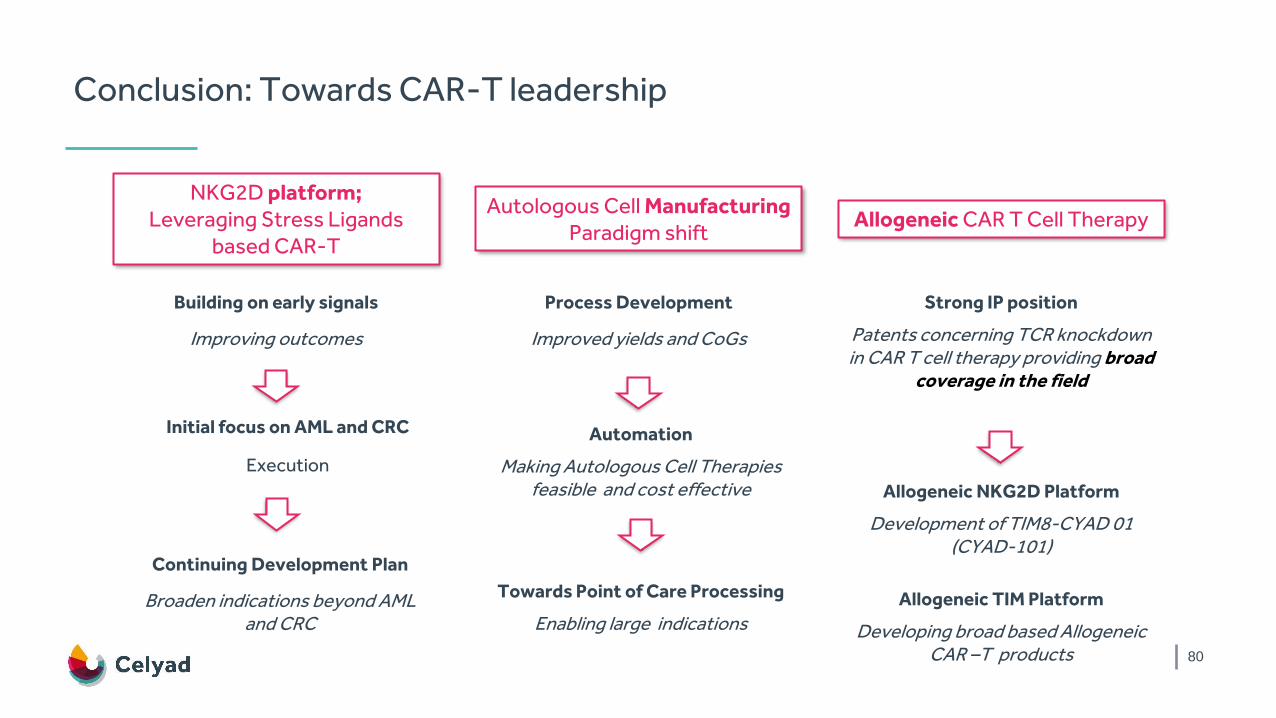
Conclusion: Towards CAR-T leadership
80
NKG2D platform;Leveraging Stress Ligands
based CAR-T
Autologous Cell ManufacturingParadigm shift
Allogeneic CAR T Cell Therapy
Building on early signals
Improving outcomes
Process Development
Improved yields and CoGs
Strong IP position
Patents concerning TCR knockdown in CAR T cell therapy providing broad
coverage in the field
Initial focus on AML and CRC
Execution
Continuing Development Plan
Broaden indications beyond AML and CRC
Automation
Making Autologous Cell Therapies feasible and cost effective Allogeneic NKG2D Platform
Development of TIM8-CYAD 01 (CYAD-101)
Towards Point of Care Processing
Enabling large indicationsAllogeneic TIM Platform
Developing broad based Allogeneic CAR –T products

Willy Borsus
Minister-President of Wallonia
81

Closing
Christian Homsy, MD, MBA
CEO
82

Q&A
83

Merci!Dank u!
Thank you!
84

















