33
1 West Penn Allegheny Health System Diane C Frndak, PhD, MBA, PA-C Center for Creating a Culture of Safety and Quality at WPAHS
| Date post: | 17-May-2015 |
| Category: |
Documents |
| Upload: | vijaybijaj |
| View: | 155 times |
| Download: | 4 times |
1
West Penn Allegheny Health System
Diane C Frndak, PhD, MBA, PA-CCenter for Creating a Culture of Safety
and Quality at WPAHS
• Admitted to the institution-registration process with a lot of personal information gathered-Given a unique number to identify you and an arm band
• Take all your clothes-Give you an uniform to wear which clearly identifies your role
• Declare all valuables-Put valuables in a bag
• Gather past records and document new issues through interviews to get facts; talk to others to understand what happened
• Examination—sometimes search body cavities
• Assigned a room which might be shared with a random individual also in the same uniform
• Shared bathroom/shower facilities
The Experience
• Some people are put in isolation
• A person with authority (and real clothes) reviews your case and makes a disposition
• Restricted family and visitor hours; certain areas that families cannot go with you
• Observations are recorded about you but you do not generally have access to them
• Long periods when you are waiting for time to pass
• Fairly bare, stark rooms with limited personal amenities given to you
• Limited privacy-strangers can enter your room at any time day or night
• Food—if you get any, may range from plain gelatin and broth to institutional food served on trays
• Your room can be changed which means you and your stuff are moved without your input or permission
• You are escorted everywhere you go within the facility
• Have many rules of what you are allowed to do and regulations about how you are to be treated to protect you

• “Things are done to you” --Determine what and when you can eat, drink, sleep, go for procedures
• Length of stay determined by others; If you leave before you are released, you are eloping
• Released at the end—have a discharge process that you go through and sometimes need to wait for it to happen
Patient or Prisoner?
Is this your life?
You are excited about having a great opportunity
to make a difference.
Hairball-ology• New Hairballs Mean New Problems• Hairballs tend to oppose their own Proper Function• Hairballs grow and get uglier over time • It sometimes Hurts to Detangle Hairballs• Hairballs Grow to Fill the Known Universe• Navigating a Path within the hairball is hard and the outcome
uncertain• A Larger Hairball produced by adding smaller Hairballs does not
behave like the smaller Hairball• People within the Hairball do not do what the Hairball thinks they
are doing• The Hairball itself cannot understand itself • When you are within a Hairball you sometimes doesn't know you
are• The Bigger the Hairball the more it seems you can isolate the
more hair that seems to be availableAdapted from “the Systems Bible” by John Gall
Hairball-ology• Hairballs Attract Hairball People• Detangling people are generally hanging around hairballs • Sometimes when trying to Detangle the Hairball you get sucked
in• Hairballs Happen • If you get tangled into a hairball you may never get out• Smaller Hairballs are less complex than larger hairballs • Hairballs are disorganized but think they are organized• When you are truly in the hairball you can’t change the hairball
and may not even know you are in a hairball• Hairballs require dramatic attention when you look at them from
a far• When trying to help a hairball you don’t know where to start• You behave differently within the hairball• Detangling the hairball takes 1) cutting it out and throwing it
away; 2) A lot of patience and screams. Adapted from “the Systems Bible” by John Gall
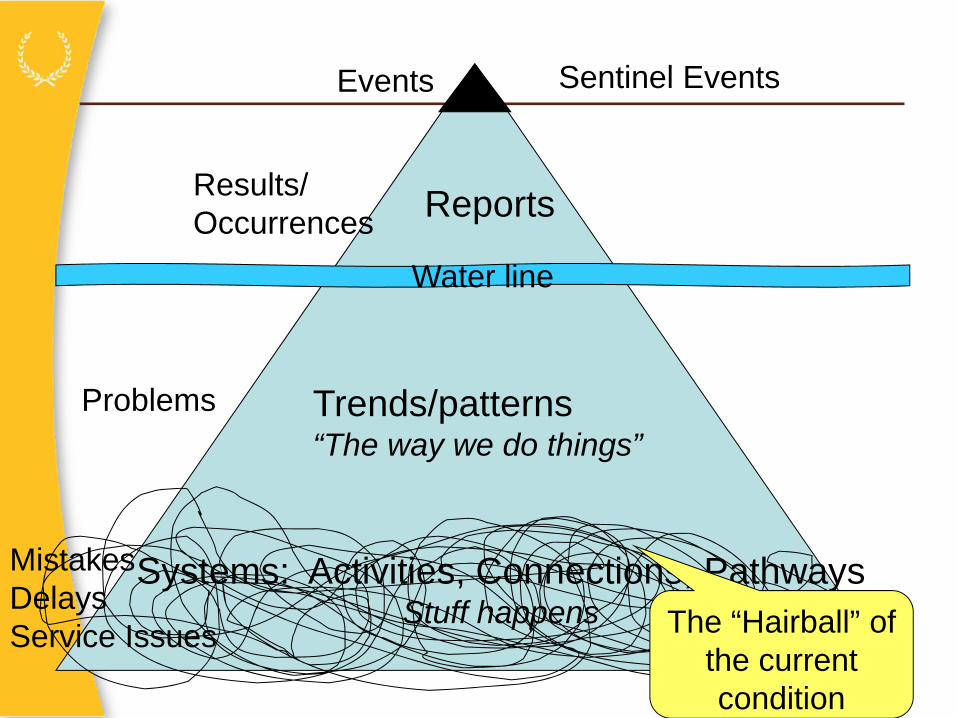
Water line
Trends/patterns“The way we do things”
Reports
Sentinel Events
MistakesDelaysService Issues
Problems
Results/Occurrences
Events
Systems: Activities, Connections, PathwaysStuff happens The “Hairball” of
the current condition
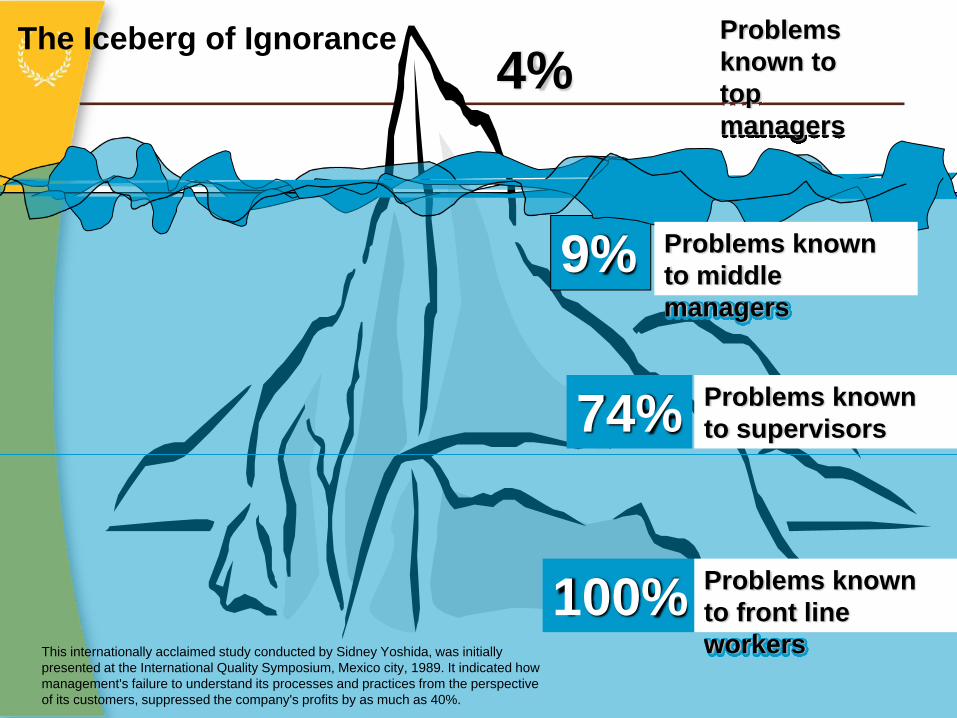
100%
4%
9%
74%
Problems known to top managers
Problems known to middle managers
Problems known to supervisors
Problems known to front line workers
The Iceberg of Ignorance
This internationally acclaimed study conducted by Sidney Yoshida, was initially presented at the International Quality Symposium, Mexico city, 1989. It indicated how management's failure to understand its processes and practices from the perspective of its customers, suppressed the company's profits by as much as 40%.
Fixing the Hairball
• …few [hospitals] have well-defined paths for fixing broken systems. The whole idea of fixing systems is often seen as time-consuming, expensive and requiring special expertise. It is expected to involve late-night committees, capital budgets, and presentations to (and rejections from) senior leaders. It seems far easier to replace a person than to fix a system--even if it is the system that causes the problem. Hospitals need to make system fixes quick, easy and understandable. The proven approach is frequent, inexpensive, ongoing, short cycle-time experiments. These low stakes trials should be a part of every unit and department. Until they are implemented and well understood, it will remain easier to blame people than to fix system.
Breaking the Cycle of Fear
Physician Executive July/August 2007
Complex Adaptive System:
A collection of individual agents, who have the freedom to act in waysthat are not always totally predictable, and whose actions are interconnected
such that one agent’s actions changes the context for other agents.
The most frightening aspect of complexsystematic problems are that they areinherently uncontrollable.
This means that prediction and control are notpossible which can frustrate managersdesiring control of these organizations andprocesses.
Wheatley, Margaret J, “When Complex Systems Fail:” New Rolesfor Leaders” Leader to Leader, No 11, Winter 1999
The Alexandrian Solution
In 333 BC, Alexander the Great attempted to untie the knot, but he could not find an end to the knot, he lifted a sword and sliced right through it.
Can You Orbit Your Hospital’s a Giant Hairball?
“But hairballs can be effective. They provide necessary stability. It is not the job of the hairball to be vibrant, alive and creative. Orbiting is vibrancy…it is pushing the boundaries of ingrained corporate patterns.”
www.fastcompany.com “How is Your Company Like a Giant Hairball
What Does It Mean to Orbit the Hairball verb (past and past participle or·bit·ed, present participleor·bit·ing, 3rd person present singular or·bits)
Definition:
1. transitive and intransitive verb move around astronomical object: to move around an astronomical object in a path dictated by the force of gravity exerted by that body
2. transitive verb put something into astronomical orbit: to send something, especially a spacecraft or an artificial satellite, into orbit
http://encarta.msn.com/encnet/features/dictionary/DictionaryResults.aspx?refid=1861635322
What Does It Mean to Orbit the Hairball
3. intransitive verb follow regular path: to move regularly or repeatedly along the same path, especially a circular path
[Mid-16th century. < Latin orbita "wheel-track"]
go into orbit to become suddenly extremely angry and upset (slang)
http://encarta.msn.com/encnet/features/dictionary/DictionaryResults.aspx?refid=1861635322

http://www.baddesigns.com/path.html
The Path of Least Resistance
•Energy follows the path of least resistance and is looking for the next path of least resistance
•People always, always, always do what makes the most sense to them
Simple Approach to the Design of the Patient Experience
• Identify area of focus
• Observe and map process
• Understand customer requirements and what would “wow” the customer
• Do an “ideal” redesign (no defects, immediate, on demand, without waste, 1x1, safe)
• Can we change the entire process at once?
• Set up experiments to get closer to the ideal—progressive rapid experiments
• Compare results to past and world-class
• Never stop asking “How could we do this better?” and then do it.
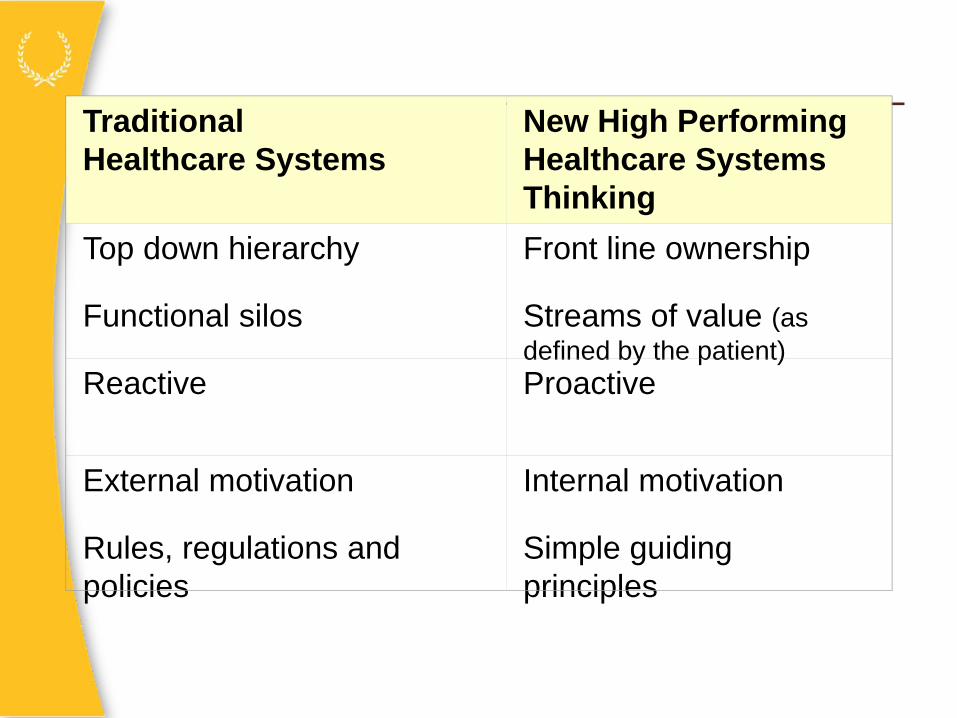
TraditionalHealthcare Systems
New High Performing Healthcare Systems Thinking
Top down hierarchy Front line ownership
Functional silos Streams of value (as defined by the patient)
Reactive Proactive
External motivation Internal motivation
Rules, regulations and policies
Simple guiding principles

TraditionalHealthcare Systems
New High Performing Healthcare Systems Thinking
Healthcare is unique We can learn from others
Patients are passive Patients design their care
Maximize unit efficiency Eliminate patient delays and waste of time
“Doctors will be doctors” Everyone has a role
Long planning cycles—taskforces, committees, input…
Rapid cycle improvements

TraditionalHealthcare Systems
New High Performance Healthcare Systems Thinking
Retrospective data Real-time data
Is the performance acceptable?
No defects impacting patients are okay
Take the problem to the meeting (3 weeks to get it scheduled)
Take the meeting to the problem
Sentinel events create an organizational response
Identify G-L-I-T-C-H-E-S
Workarounds/heroes required
P-D-C-A everythingMini experiments
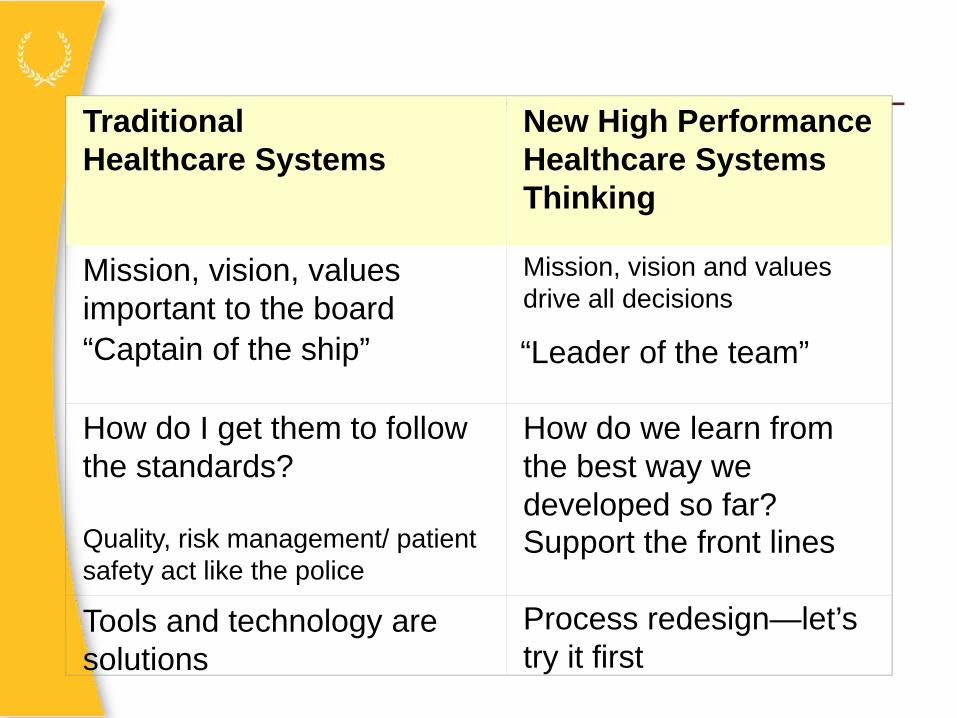
TraditionalHealthcare Systems
New High Performance Healthcare Systems Thinking
Mission, vision, values important to the board
Mission, vision and values drive all decisions
“Captain of the ship” “Leader of the team”
How do I get them to follow the standards?
How do we learn from the best way we developed so far?
Quality, risk management/ patient safety act like the police
Support the front lines
Process redesign—let’s try it first
Tools and technology are solutions
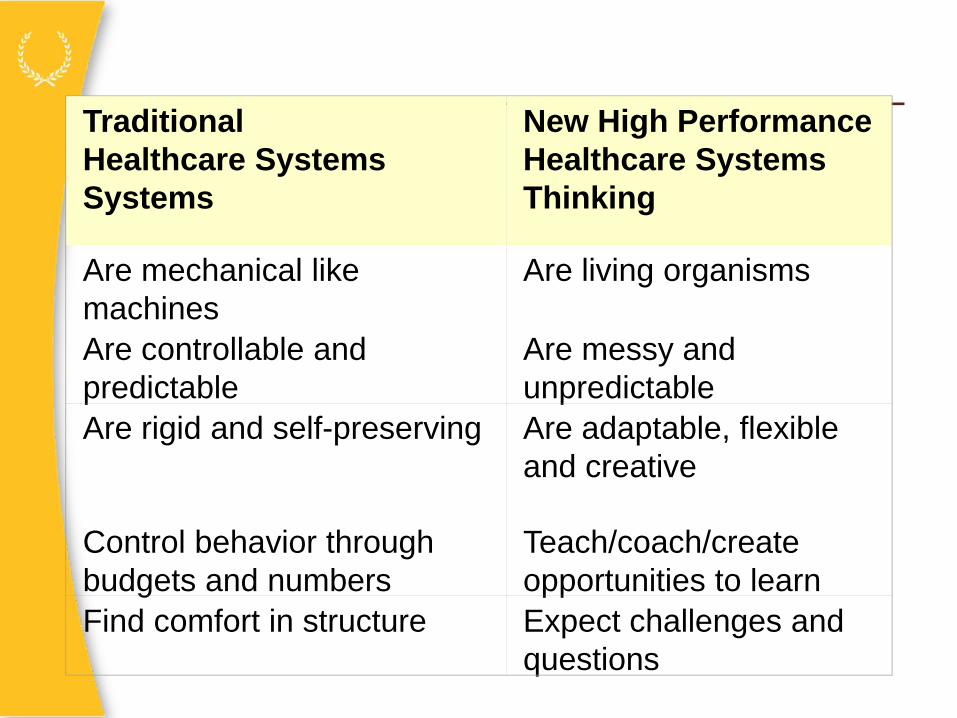
TraditionalHealthcare SystemsSystems
New High Performance Healthcare Systems Thinking
Are mechanical like machines
Are living organisms
Are controllable and predictable
Are messy and unpredictable
Are rigid and self-preserving Are adaptable, flexible and creative
Control behavior through budgets and numbers
Teach/coach/create opportunities to learn
Find comfort in structure Expect challenges and questions
The traditional thinking
• The organization as a top-down hierarchy.
• Work designed in functional silos
• Decision-making is separated from work – decision-making being management’s job
• In making decisions, managers use measures of budget, activity, productivity, and standards
• Managers believe their job is to manage budgets and manage people
Most organizations are designed and managed this way. The news is this doesn’t work very well.
www.lean-service.com/systems
Who do you work for?
• If the patient is the focus of everything we do-everyone of us works for the patient.
– If managers think vertically to optimize their area, department or function, the horizontal flow of value to the customer can easily get lost
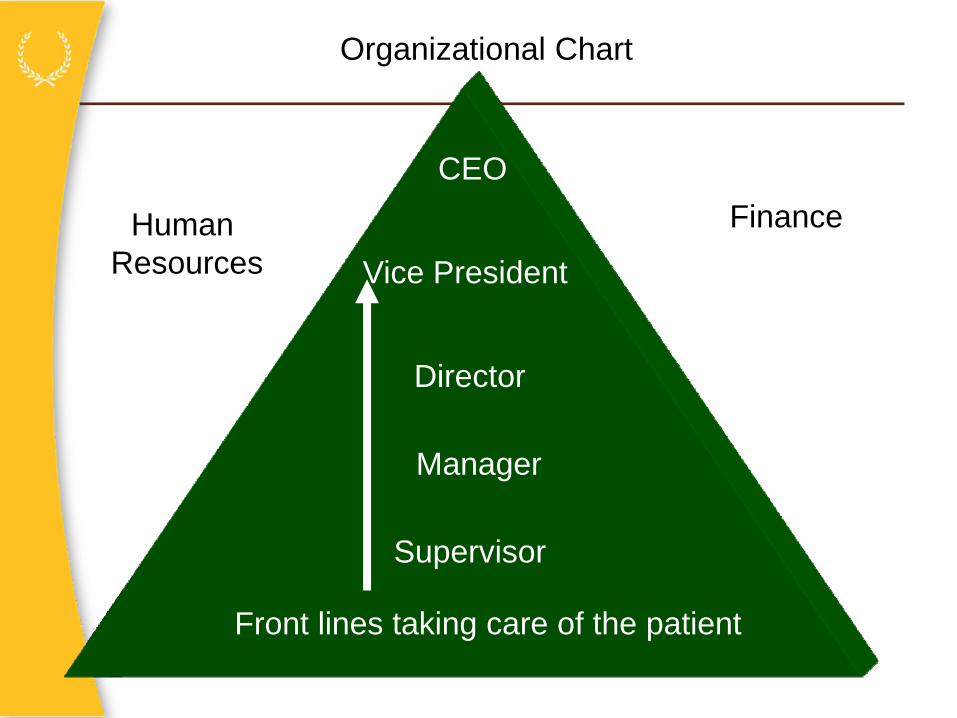
Front lines taking care of the patient
CEO
Vice President
Director
Manager
Supervisor
Human Resources
Finance
Organizational Chart

Front lines taking care of the patient where thevalue exchange occurs
CEO
VP
Director
Manager
Supervisor Human Resources
Finance
The Patient is the Focus of Everything We Do
Blister analogy• Organizational problems are
like poorly fitting shoes on a foot
• First a red spot occurs with pain—if no response– A blister—sterile inflammatory
response
– If no response (numbness to the pain)
• Ulcer– Amputation
“Real-time is the best time”
- immediate problem identification
- real-time data
- real-time response
• We accept preventable, needless events, by creating workarounds.
• Workarounds are symptoms of a system or process problem
• Many acts of modern day heroism are immediate preceded by acts of utter insanity requiring the very acts of heroism that we are bragging about in the first place
• Instead of workarounds, why not respond, “since we can’t ____, let’s find out why and do something about it”
Workaround Waste