27
www.sage-growth.com What’s an IPA To Do? Prepared for IPN Sage Growth Partners October 22, 2014
| Date post: | 15-Jul-2015 |
| Category: |
Healthcare |
| Upload: | sage-growth-partners |
| View: | 109 times |
| Download: | 0 times |
www.sage-growth.com
What’s an IPA To Do? Prepared for IPN Sage Growth Partners October 22, 2014

www.sage-growth.com
About Us

www.sage-growth.com
A Growing Client Roster
www.sage-growth.com
Hypothesis: Health Care Will be Disrupted
There is an overwhelming confluence of
interests, incen6ves, and macro-‐environmental forces that will disrupt the industry and drive
real change – Payment model redesign will be a core catalyst for
change
4
www.sage-growth.com
A Step Further
• Even if no net-‐new, domes6c U.S. HC is a $1T arbitrage opportunity – and its largely in facili6es, specialists, transi6ons, and chronic care management
• Health care will experience its industrial revolu6on – Transparency – Standards – Focus on efficiency
• In an industrial model – community organizers/entrepreneurs (PCPs) are very well suited to assume the mantle of leadership
• The garage is coming to health care • Incen6ves are aligned between payers and enlightened providers beOer
then ever – economics and ACA are driving payers to shiQ risk
5
www.sage-growth.com
Lots of QuesOons
• The role of physicians – especially independents • The role of hospitals and health systems • The role of subs6tutes • The pace of migra6on to VBP • The pace of provider/payer convergence
• WHAT IS THE IPA TO DO?
6
www.sage-growth.com
Focus on Three Swim Lanes
Best Care
Dominant Delivery
Organiza6on(s)
Dominant Delivery Network
Dominant Enabling Business PlaZorm
Best Health Status Best Value

www.sage-growth.com
THE EVIDENCE
8
www.sage-growth.com
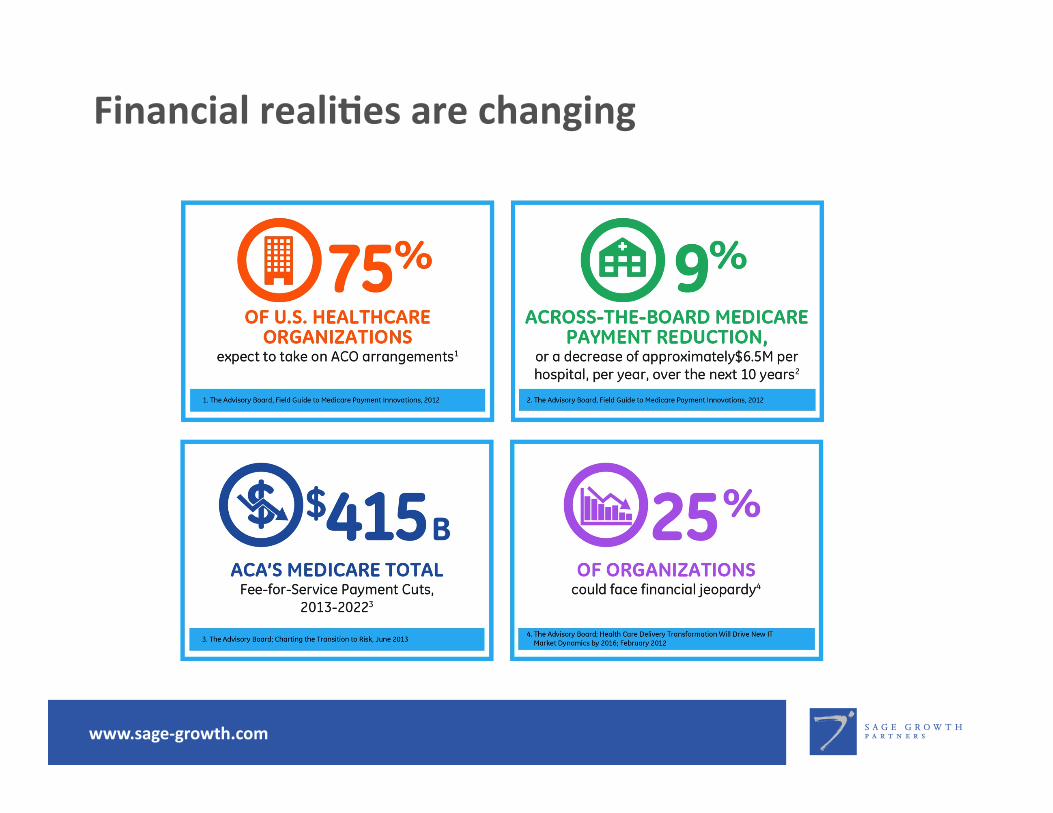
Financial realiOes are changing
www.sage-growth.com
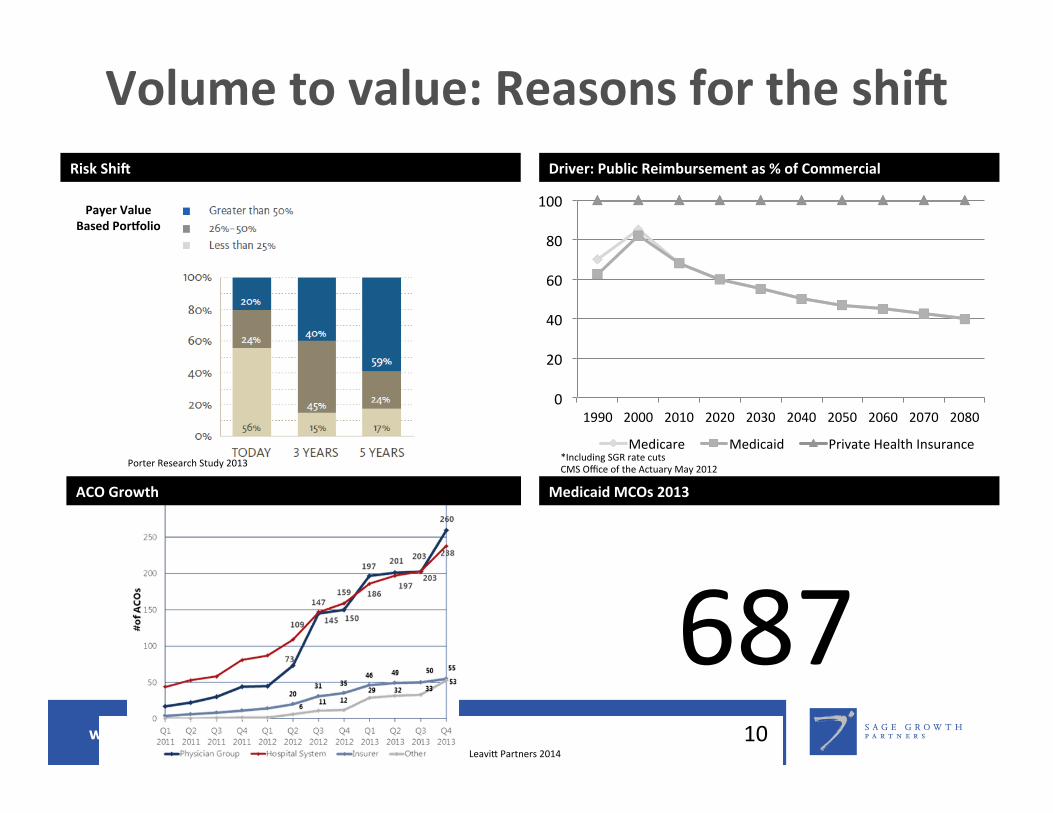
Volume to value: Reasons for the shiT
10
Risk ShiT
Payer Value Based PorVolio
0
20
40
60
80
100
1990 2000 2010 2020 2030 2040 2050 2060 2070 2080
Medicare Medicaid Private Health Insurance
Driver: Public Reimbursement as % of Commercial
ACO Growth
687 Medicaid MCOs 2013
Porter Research Study 2013 *Including SGR rate cuts CMS Office of the Actuary May 2012
LeaviO Partners 2014
www.sage-growth.com
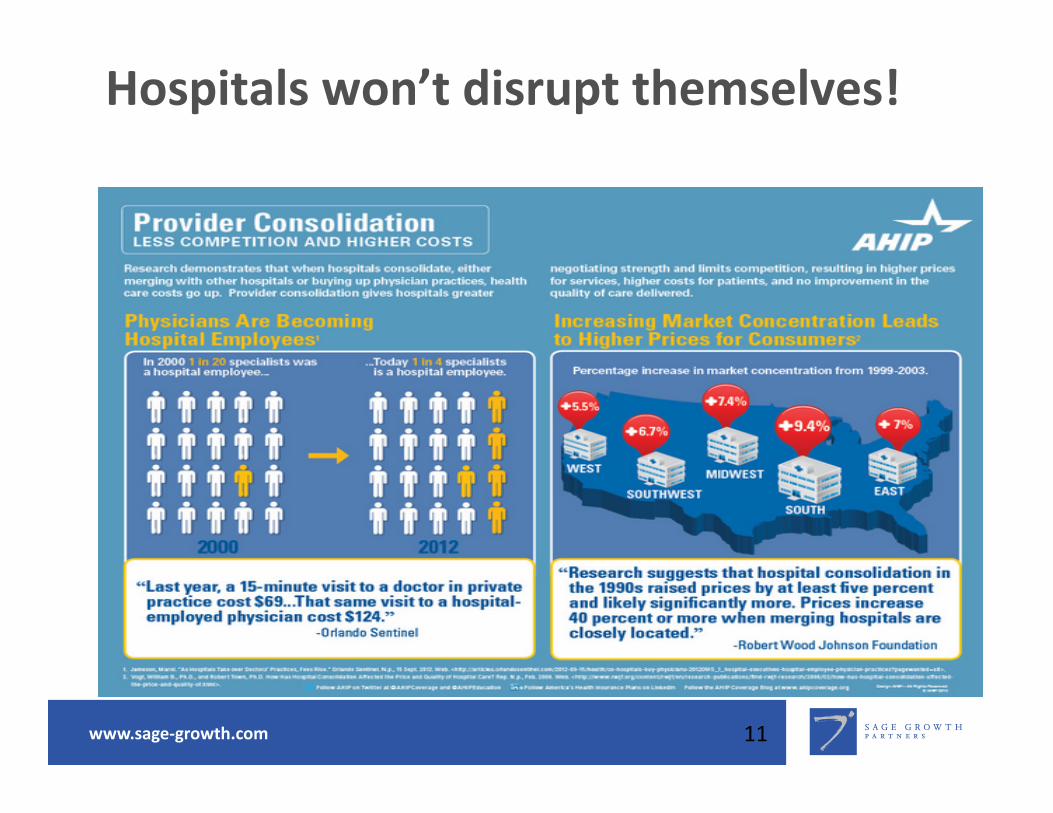
Hospitals won’t disrupt themselves!
11
www.sage-growth.com
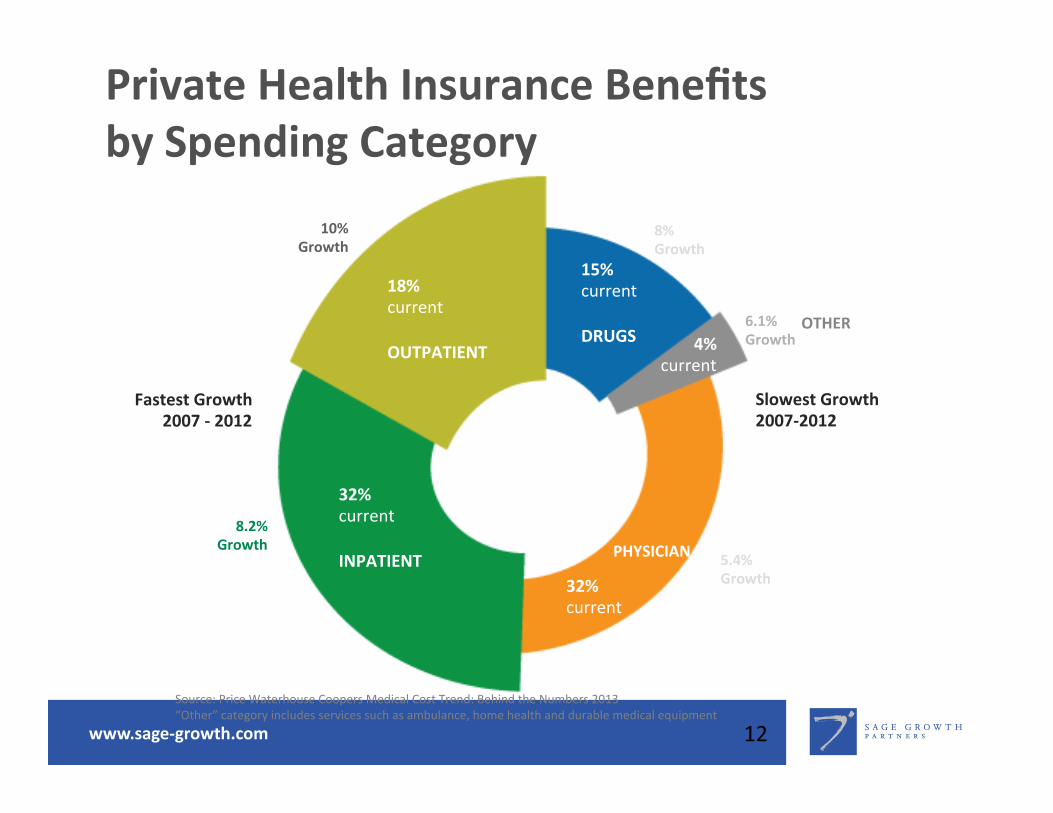
Private Health Insurance Benefits by Spending Category
12
18% current OUTPATIENT
32% current INPATIENT
32% current
PHYSICIAN
4% current
OTHER
15% current DRUGS
Fastest Growth 2007 -‐ 2012
Slowest Growth 2007-‐2012
8.2% Growth
10% Growth
8% Growth
6.1% Growth
5.4% Growth
Source: Price Waterhouse Coopers Medical Cost Trend: Behind the Numbers 2013 “Other” category includes services such as ambulance, home health and durable medical equipment

www.sage-growth.com
The (really) lean health plan
13
www.sage-growth.com
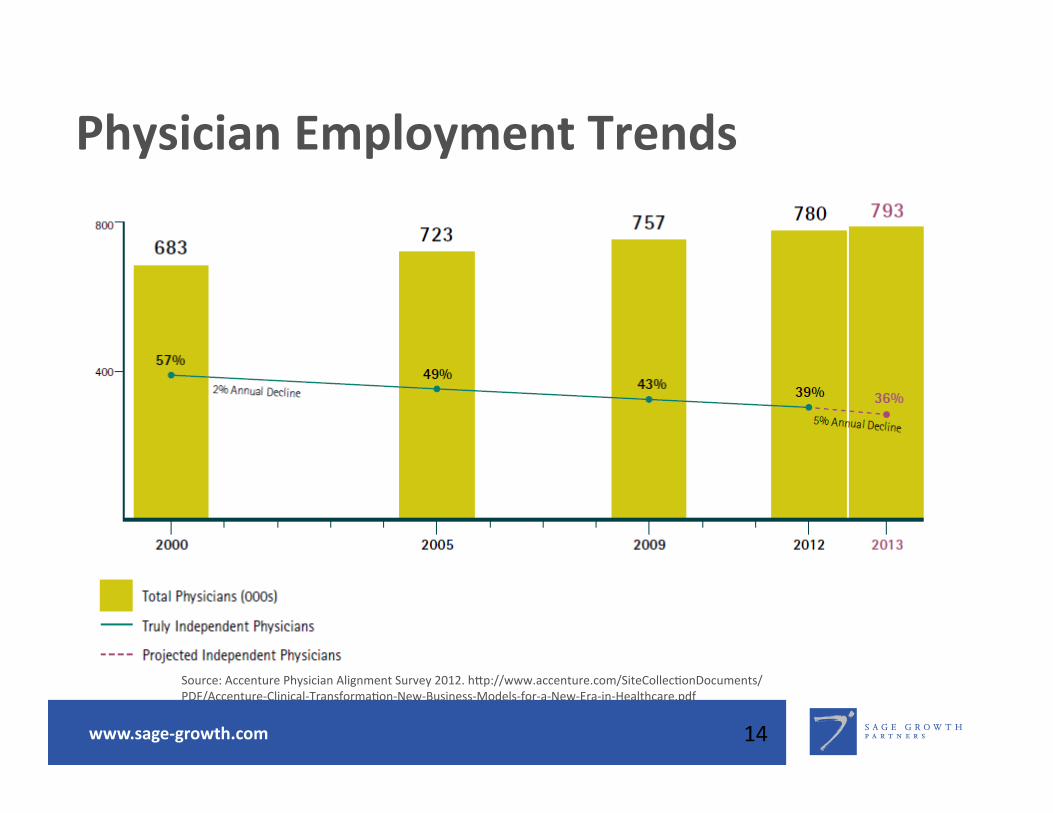
Physician Employment Trends
14
Source: Accenture Physician Alignment Survey 2012. hOp://www.accenture.com/SiteCollec6onDocuments/PDF/Accenture-‐Clinical-‐Transforma6on-‐New-‐Business-‐Models-‐for-‐a-‐New-‐Era-‐in-‐Healthcare.pdf

www.sage-growth.com
Sustainable?
• Hospitals lose on average $176,463 per physician on owned physician prac6ces
• The longer a hospital owns physician groups, the higher the likelihood it is losing money on them.
• The more physicians a hospital employs, the more likely they incur losses
• 78% of hospitals are paying physicians non-‐produc6vity incen6ves (pa6ent sa6sfac6on, clinical quality, and ci6zenship), expected to rise to 94% in 3 years
15
Sources: MGMA 2013 Cost Survey All mul6-‐specialty groups, hospital-‐owned and Report: Hospital-‐owned prac6ces lose up to $100K per doc each year – FiercePrac6ceManagement

www.sage-growth.com
New reality High performing provider organizaOons must manage risk
• Market forces driving a heightened need for financial accountability
• Insurers seeking to transfer the financial risk of clinical service
• The risk-‐transference taking the form of payment-‐for-‐value arrangements
• Entrepreneurial provider-‐sponsored organiza6ons are well posi6oned
• Organiza6ons may lack technology and solu6ons infrastructure to transform their business models

www.sage-growth.com
Where are you? Are you ready?
www.sage-growth.com
NEW (?) PAYMENT MODELS

www.sage-growth.com
IncenOves Drive (bad) Behavior
19

www.sage-growth.com
Why VBP?
• Purchasers are demanding more accountability around quality and cost
• Medicare and Medicaid need the “stop loss” • Its a way to take and grow share • It allows a focus on “industrial improvement”
• Its working in key markets • Its driving quality outcomes
20

www.sage-growth.com
The Impact of Truly Independent PCPs
21

www.sage-growth.com
BUILDING CAPABILITIES TO ADDRESS MARKET NEEDS

www.sage-growth.com
CITI research1 Framework for managing populaOon health
1Source: Popula6on Health Management-‐Hill’s Handbook to the Next Decade in Healthcare Technology, 14 May 2013

www.sage-growth.com
What’s an IPA to Do? NOT MUTUALLY EXCLUSIVE
24
Dominant Delivery
Organiza6on(s)
Dominant Delivery Network
Dominant Enabling Business PlaZorm

www.sage-growth.com
If It Were My IPA, I’d be thinking about…
• PopulaOon Health – let’s define – needs to be CORE – AOribu6on/iden6fica6on – Surveillance – Risk assessment – Risk stra6fica6on – what’s our triangle look like? – Gap assessment – Coordinate/drive interven6ons
• On-‐ramps for providers – especially PCPs – Running through walls to enhance/aggregate primary care
– Build a new economic model – “the era of 3x” – Employment op6ons – Find the entrepreneurs
25
www.sage-growth.com
If It Were My IPA, I’d be thinking about…
• Aggressively courOng Payers/Purchasers (Insurers, TPA/ASO, Employers, Unions, Purchasing Groups) – Make something different happen – Get out and talk early and oQen – Don’t make assump6ons and don’t ignore purchasers
• Embracing transparency wholeheartedly – Prices, Costs, Quality
• Don’t forget the infrastructure – And plan the Ecosystem – IT, Rev Cycle, Messaging, CDS, PH, PI, Retail, remote monitoring, etc. etc. etc.
• Capital Partners – be creaOve
26
www.sage-growth.com
Contact: Sage Growth Partners 3500 Boston Street, Suite 435 Bal3more, Maryland 21224 410.534.1161

















