Case Report & Case Series White matter tract recovery following medial temporal lobectomy and selective amygdalohippocampectomy for tumor resection via a ROVOT-m port-guided technique: A case report and review of literature Srikant S. Chakravarthi a , Anthony Zbacnik b , Jonathan Jennings b , Melanie B. Fukui a,b , Nathaniel Kojis a , Richard A. Rovin a , Amin B. Kassam a, ⁎ a Department of Neurosurgery, Aurora Neurosciences Innovation Institute, Aurora St. Luke's Medical Center, Milwaukee, WI, United States b Department of Radiology, Aurora St. Luke's Medical Center, Milwaukee, WI, United States abstract article info Article history: Received 10 April 2016 Accepted 31 July 2016 Background: Surgical approaches to the temporal region for resection of tumors is challenging due to the anatomic complexity and, in particular, understanding of the critical subcortical white matter. Knowledge of the location of white matter fiber tracts and delicate vessels is essential in preventing complications. As a result, accurate navigation, planning and trajectory are necessary in designing a safe corridor for resection. Case description: We describe here a 49-year-old male with a history of right mesial temporal lobe mass since 2012, with concomitant intractable seizures. MRI showed heterogeneous internal enhancement and multiple internal calcifications, resulting in local mass effect with uncal herniation. DTI showed lateral deviation of the Inferior Longitudinal Fasciculus (ILF) and focally diminished anisotropy of the uncinate. The findings were consistent with a WHO grade I pilocytic astrocytoma. BrightMatter Plan software (Synaptive Medical, Toronto, Canada) was then used to plan a trajectory for insertion of a port system (NICO BrainPath, Indianapolis, IN). Complete resection of the tumor, along with partial temporal lobectomy and amygdalohippocampectomy was performed to treat the seizure focus. Conclusions: To our knowledge, this is the first reported case of a temporal lobectomy and amygdalohippocampectomy using a port technique, in particular, one that demonstrates recovery of the critical (ILF and uncinate fasciculus) subcortical white matter tracts. The combination of real-time, rapid, geometrically accurate 3D-planning of white matter tracts is imperative, especially in conjunction with minimally invasive approaches, thereby offering a new, safer perspective into the approach of temporal lobe lesions. Published by Elsevier B.V. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Keywords: Diffusion Tensor Imaging (DTI) White matter tract recovery Port 1. Introduction Surgical treatment of temporal lobe epilepsy has been a well- established method for relief of intractable seizures, especially as a result of tumors. The epileptogenic focus includes the amygdala, hippocampus, and parahippocampal gyrus. Anterior temporal lo- bectomy (ATL) has been shown to be superior to medical manage- ment, and selective amygdalohippocampectomy (SA), including removal of the uncal portion, was developed to preserve the lateral temporal neocortex [1]. A narrow operative corridor, especially through the transsylvian approach, is required to access the medial temporal lobe structures. This approach, however, is technically complex and requires extensive knowledge in microsurgical anato- my as well as white matter fiber tract locations and can put these by- stander tracts at risk. To increase the efficacy and safety of this approach, we have incorporated intraoperative real-time use of DTI rendering with navigation and DTI; specifically, planning and trajectory software, have been recently utilized as an adjuvant to the standard surgical approach. To our knowledge, the application of a port Brain Path (BP) (NICO corporation, Indianapolis, Indiana) in entering the medial temporal lobe has not yet been reported. Here we present a case of the resection of a medial temporal lobe tumor with the use of a combination of technologies: 3D white matter rendering and planning software combined with portal access (BP) and guided by a Robotically Operated Video Optical Telescopic-microscopy system (ROVOT-m) (Synaptive Medical Corporation, Toronto, Canada). Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61 Abbreviations: DTI, Diffusion Tensor Imaging; FLAIR, Fluid-attenuated inversion recov- ery; MRI, Magnetic Resonance Imaging; T1WI, T1-weighted image; WHO, World Health Organization; ILF, Inferior Longitudinal Fasciculus; BP, Brain Path. ⁎ Corresponding author at: Aurora Neuroscience Innovation Institute, Aurora St. Luke's Medical Center, 2801 West Kinnickinnic River Parkway, Suite 630, Milwaukee, WI 53215, United States. E-mail address: [email protected](A.B. Kassam). Contents lists available at ScienceDirect Interdisciplinary Neurosurgery: Advanced Techniques and Case Management journal homepage: www.inat-journal.com http://dx.doi.org/10.1016/j.inat.2016.07.004 2214-7519/Published by Elsevier B.V. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Transcript
Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
White matter tract recovery following medial temporal lobectomy andselective amygdalohippocampectomy for tumor resection via a ROVOT-mport-guided technique: A case report and review of literature
Srikant S. Chakravarthi a, Anthony Zbacnik b, Jonathan Jennings b, Melanie B. Fukui a,b, Nathaniel Kojis a,Richard A. Rovin a, Amin B. Kassam a,⁎a Department of Neurosurgery, Aurora Neurosciences Innovation Institute, Aurora St. Luke's Medical Center, Milwaukee, WI, United Statesb Department of Radiology, Aurora St. Luke's Medical Center, Milwaukee, WI, United States
http://dx.doi.org/10.1016/j.inat.2016.07.0042214-7519/Published by Elsevier B.V. This is an open acce
a b s t r a c t
a r t i c l e i n f o
Article history:Received 10 April 2016Accepted 31 July 2016
Background: Surgical approaches to the temporal region for resection of tumors is challenging due to theanatomic complexity and, in particular, understanding of the critical subcortical white matter. Knowledge ofthe location of white matter fiber tracts and delicate vessels is essential in preventing complications. As a result,accurate navigation, planning and trajectory are necessary in designing a safe corridor for resection.Case description: We describe here a 49-year-old male with a history of right mesial temporal lobe mass since2012, with concomitant intractable seizures. MRI showed heterogeneous internal enhancement and multipleinternal calcifications, resulting in local mass effect with uncal herniation. DTI showed lateral deviation of theInferior Longitudinal Fasciculus (ILF) and focally diminished anisotropy of the uncinate. The findings wereconsistent with a WHO grade I pilocytic astrocytoma. BrightMatter Plan software (Synaptive Medical, Toronto,Canada) was then used to plan a trajectory for insertion of a port system (NICO BrainPath, Indianapolis, IN).Complete resection of the tumor, along with partial temporal lobectomy and amygdalohippocampectomy wasperformed to treat the seizure focus.Conclusions: Toourknowledge, this is thefirst reported case of a temporal lobectomyandamygdalohippocampectomyusing a port technique, in particular, one that demonstrates recovery of the critical (ILF and uncinate fasciculus)subcortical white matter tracts. The combination of real-time, rapid, geometrically accurate 3D-planning ofwhitematter tracts is imperative, especially in conjunctionwithminimally invasive approaches, thereby offeringa new, safer perspective into the approach of temporal lobe lesions.
Published by Elsevier B.V. This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Surgical treatment of temporal lobe epilepsy has been a well-established method for relief of intractable seizures, especially as aresult of tumors. The epileptogenic focus includes the amygdala,hippocampus, and parahippocampal gyrus. Anterior temporal lo-bectomy (ATL) has been shown to be superior to medical manage-ment, and selective amygdalohippocampectomy (SA), includingremoval of the uncal portion, was developed to preserve the lateral
uid-attenuated inversion recov-ted image; WHO, World Healthin Path.ation Institute, Aurora St. Luke'suite 630, Milwaukee, WI 53215,
).
ss article under the CC BY-NC-ND lic
temporal neocortex [1]. A narrow operative corridor, especiallythrough the transsylvian approach, is required to access the medialtemporal lobe structures. This approach, however, is technicallycomplex and requires extensive knowledge in microsurgical anato-my as well as white matter fiber tract locations and can put these by-stander tracts at risk. To increase the efficacy and safety of thisapproach, we have incorporated intraoperative real-time use ofDTI rendering with navigation and DTI; specifically, planning andtrajectory software, have been recently utilized as an adjuvant tothe standard surgical approach. To our knowledge, the applicationof a port Brain Path (BP) (NICO corporation, Indianapolis, Indiana)in entering the medial temporal lobe has not yet been reported.Here we present a case of the resection of a medial temporal lobetumor with the use of a combination of technologies: 3D whitematter rendering and planning software combined with portalaccess (BP) and guided by a Robotically Operated Video OpticalTelescopic-microscopy system (ROVOT-m) (Synaptive MedicalCorporation, Toronto, Canada).
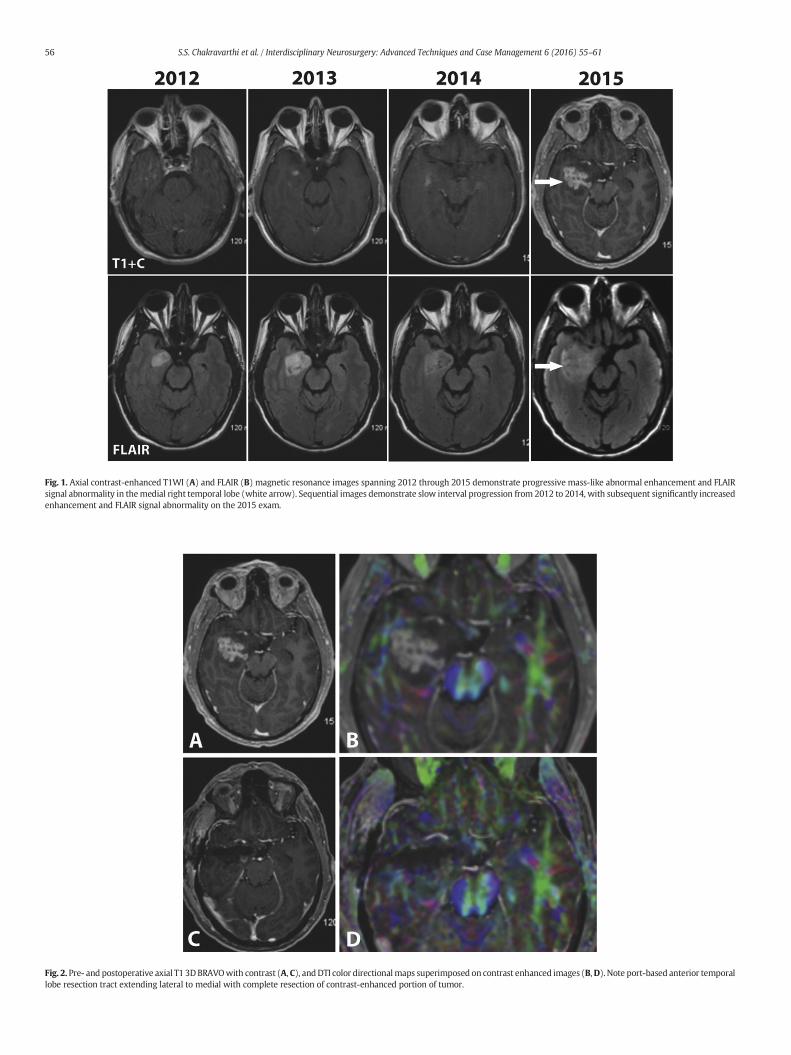
Fig. 1. Axial contrast-enhanced T1WI (A) and FLAIR (B) magnetic resonance images spanning 2012 through 2015 demonstrate progressive mass-like abnormal enhancement and FLAIRsignal abnormality in themedial right temporal lobe (white arrow). Sequential images demonstrate slow interval progression from 2012 to 2014, with subsequent significantly increasedenhancement and FLAIR signal abnormality on the 2015 exam.
Fig. 2. Pre- and postoperative axial T1 3DBRAVOwith contrast (A, C), andDTI color directionalmaps superimposed on contrast enhanced images (B,D). Note port-based anterior temporallobe resection tract extending lateral to medial with complete resection of contrast-enhanced portion of tumor.
56 S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
57S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
1.1. Case report
We present a 49-year old male who presented to the neurosurgeryclinic with a history of intractable seizures, hypertension and a recur-rent incisional hernia requiringmultiple repairs. He has had a right tem-poral lobemass since 2012. His only complaint on admissionwas amildright-sided headache, but otherwise denied dizziness, nausea, or visualabnormalities.
MR imaging demonstrated a T2 FLAIR signal hyperintensity in themesial right temporal lobe that showed a slow-interval increase insize and enhancement over a period of several years (Fig. 1). Therewas also extensive heterogeneous enhancementwithin themid and lat-eral portion of this ovoid lesion. There was uncal herniation with masseffect of the right cerebral peduncle and effacement of the rightparamesencephalic cistern. Multiple small calcifications were seen aswell on CT. Diffusion-weighted imaging demonstrated no signs ofacute infarct. DTI revealed lateral deviation of the Inferior LongitudinalFasciculus with focally diminished fractional anisotropy (FA), as wellas, decreased FA of the uncinate fasciculus (Fig. 2). These imaging fea-tures were most consistent with an oligodendroglioma.
1.2. Operative technique
The patient was brought into the operating room for the purposes ofdiagnosis and molecular profiling, cytoreduction, and seizure control.Planning and 3D trajectory rendering using BrightMatter Plan software(Synaptive Medical, Toronto, Canada) was utilized. There were two key
Fig. 3. Trajectory planningwas performedusing BrightMatter Plan (BMP) software. Real-time potrajectory and target; B. Oblique view of trajectory and insertion of port displaying trajectory inan automated BMP software algorithm shows Inferior Longitudinal Fasciculus (ILF; lateral to poin blue, and corpus callosum in red.D. Port trajectory and insertion are displayed, aswell as bordplanned craniotomy as displayed on skin; F. Postoperative coronal CT showing resection cavity
features in planning the trajectory: a) a transulcal corridor was used topreserve the overlying neocortex and b) trajectorywas planned parallelto the ILF and uncinate fasciculus to promote recovery. This trajectorywas used to guide the insertion of the BP (Fig. 3).
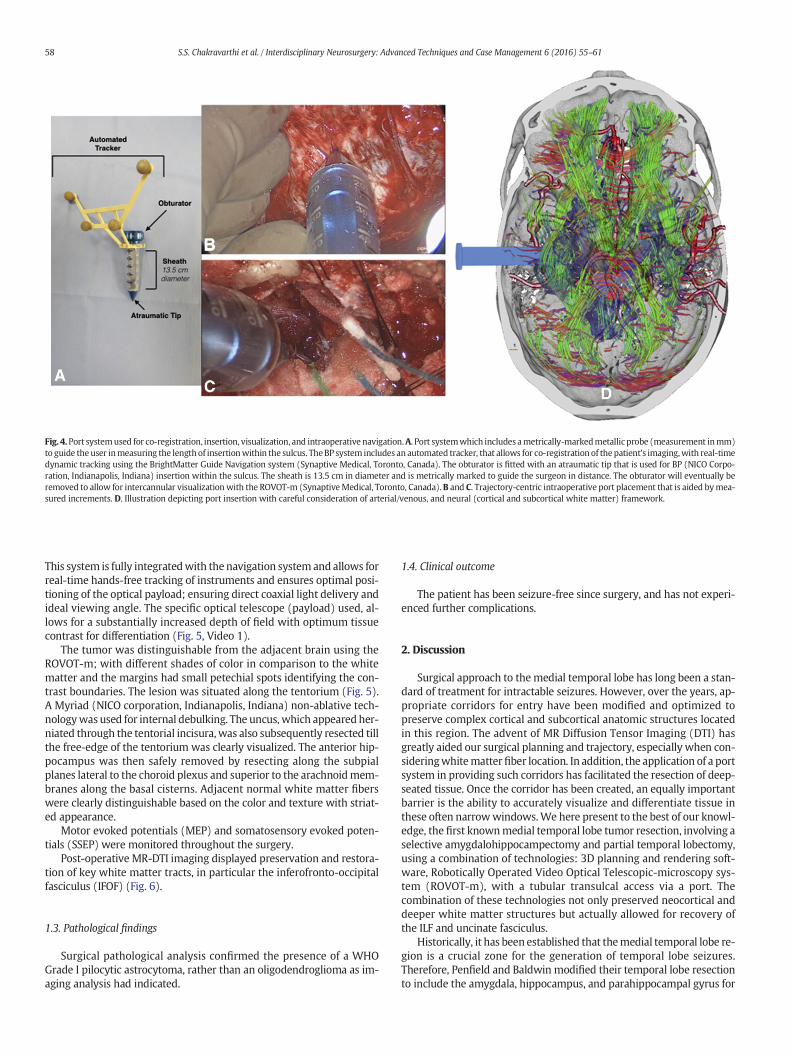
The procedure was carried out with the patient awake. An appropri-ate pterional craniotomy was then cut. A corridor along the sulcus be-tween the middle temporal and superior temporal gyrus was used forthe approach. Under direct ROVOT-m guidance, an entry pathway wasprepared for cannulation, by first dissecting the arachnoid membrane,mobilizing a surface vein (that was preserved), and then slightlyseparating the entry sulcus. With the aid of neuronavigation, usingreal-time 3D DTI, and neurophysiological monitoring, cannulation wasundertaken. The BP port systemwas used to provide a corridor for visu-alization andbimanual resection. The BP system consists of a specificallydesigned obturator with an atraumatic tip to traverse the sulcus. Thisthen allows the placement of the overlying 13.5 mm cylindrical sheathto allow for visualization and dissection. The BP is integrated via a spe-cifically designed tracking mechanism to allow for real-time navigationreferred to as BrightMatter Guide (Synaptive Medical, Toronto, Canada)which allows for co-registration of the port and intraoperativeneuronavigation (Fig. 4). Ultrasoundwas then used to confirm the posi-tion of the tumor.
The robotic guidance system was then placed into position for sub-sequentmicrodissection. The ROVOT-m is an optical positioning systemwith a computer-machine interface (robotically-controlled) that allowsfor a specific video telescopic system to provide optimum light andmagnification maximizing visualization especially in small corridors.
rt insertionwas simulated preoperatively based on our planned trajectory.A. Axial viewofferior to the bulk of ILF fibers; C. Diffusion tensor imaging tractography, generated throughrt) and inferofronto-occipital fasciculus (IFOF; medial to port) in green, corticospinal tractsers of craniotomy allowing for resection andmaneuverability of the port; E. Lateral viewof.
Fig. 4.Port systemused for co-registration, insertion, visualization, and intraoperative navigation.A. Port systemwhich includes ametrically-markedmetallic probe (measurement inmm)to guide theuser inmeasuring the lengthof insertionwithin the sulcus. TheBP system includes an automated tracker, that allows for co-registration of thepatient's imaging,with real-timedynamic tracking using the BrightMatter Guide Navigation system (Synaptive Medical, Toronto, Canada). The obturator is fitted with an atraumatic tip that is used for BP (NICO Corpo-ration, Indianapolis, Indiana) insertion within the sulcus. The sheath is 13.5 cm in diameter and is metrically marked to guide the surgeon in distance. The obturator will eventually beremoved to allow for intercannular visualizationwith the ROVOT-m (SynaptiveMedical, Toronto, Canada).B and C. Trajectory-centric intraoperative port placement that is aided bymea-sured increments. D. Illustration depicting port insertion with careful consideration of arterial/venous, and neural (cortical and subcortical white matter) framework.
58 S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
This system is fully integratedwith the navigation system and allows forreal-time hands-free tracking of instruments and ensures optimal posi-tioning of the optical payload; ensuring direct coaxial light delivery andideal viewing angle. The specific optical telescope (payload) used, al-lows for a substantially increased depth of field with optimum tissuecontrast for differentiation (Fig. 5, Video 1).
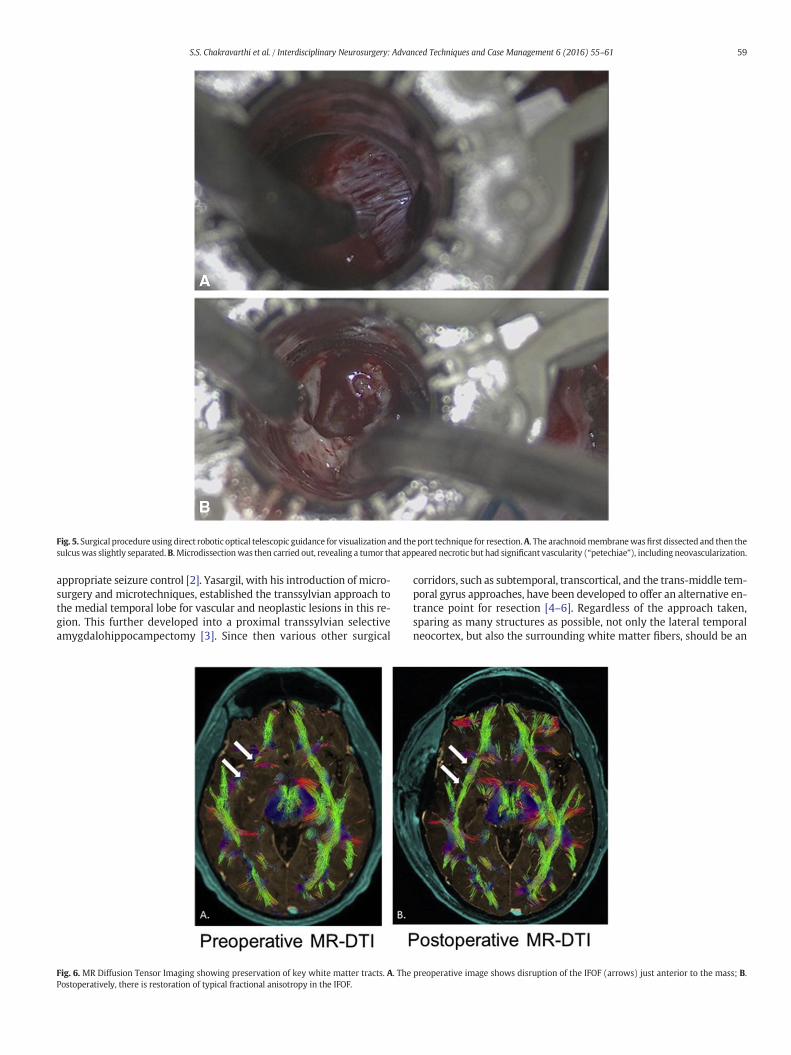
The tumor was distinguishable from the adjacent brain using theROVOT-m; with different shades of color in comparison to the whitematter and the margins had small petechial spots identifying the con-trast boundaries. The lesion was situated along the tentorium (Fig. 5).A Myriad (NICO corporation, Indianapolis, Indiana) non-ablative tech-nologywas used for internal debulking. The uncus, which appeared her-niated through the tentorial incisura,was also subsequently resected tillthe free-edge of the tentorium was clearly visualized. The anterior hip-pocampus was then safely removed by resecting along the subpialplanes lateral to the choroid plexus and superior to the arachnoidmem-branes along the basal cisterns. Adjacent normal white matter fiberswere clearly distinguishable based on the color and texture with striat-ed appearance.
Motor evoked potentials (MEP) and somatosensory evoked poten-tials (SSEP) were monitored throughout the surgery.
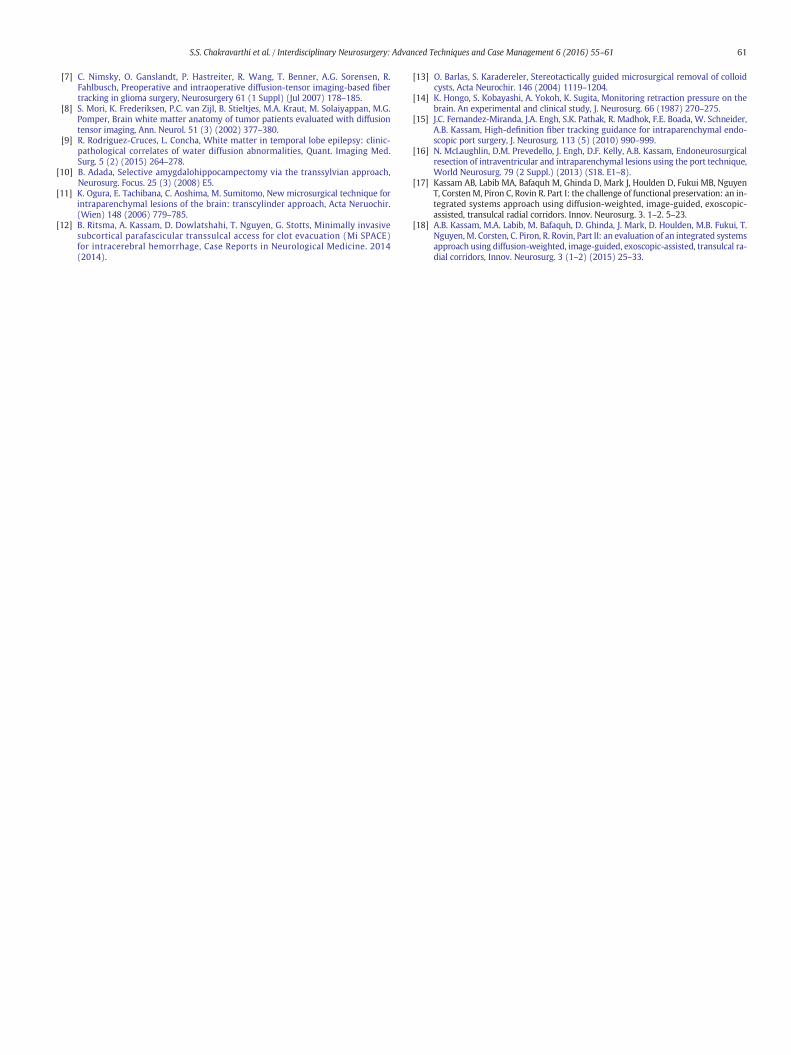
Post-operative MR-DTI imaging displayed preservation and restora-tion of key white matter tracts, in particular the inferofronto-occipitalfasciculus (IFOF) (Fig. 6).
1.3. Pathological findings
Surgical pathological analysis confirmed the presence of a WHOGrade I pilocytic astrocytoma, rather than an oligodendroglioma as im-aging analysis had indicated.
1.4. Clinical outcome
The patient has been seizure-free since surgery, and has not experi-enced further complications.
2. Discussion
Surgical approach to themedial temporal lobe has long been a stan-dard of treatment for intractable seizures. However, over the years, ap-propriate corridors for entry have been modified and optimized topreserve complex cortical and subcortical anatomic structures locatedin this region. The advent of MR Diffusion Tensor Imaging (DTI) hasgreatly aided our surgical planning and trajectory, especially when con-sideringwhitematterfiber location. In addition, the application of a portsystem in providing such corridors has facilitated the resection of deep-seated tissue. Once the corridor has been created, an equally importantbarrier is the ability to accurately visualize and differentiate tissue inthese often narrowwindows.We here present to the best of our knowl-edge, the first knownmedial temporal lobe tumor resection, involving aselective amygdalohippocampectomy and partial temporal lobectomy,using a combination of technologies: 3D planning and rendering soft-ware, Robotically Operated Video Optical Telescopic-microscopy sys-tem (ROVOT-m), with a tubular transulcal access via a port. Thecombination of these technologies not only preserved neocortical anddeeper white matter structures but actually allowed for recovery ofthe ILF and uncinate fasciculus.
Historically, it has been established that themedial temporal lobe re-gion is a crucial zone for the generation of temporal lobe seizures.Therefore, Penfield and Baldwin modified their temporal lobe resectionto include the amygdala, hippocampus, and parahippocampal gyrus for
Fig. 5. Surgical procedure using direct robotic optical telescopic guidance for visualization and the port technique for resection.A. The arachnoidmembranewasfirst dissected and then thesulcuswas slightly separated.B. Microdissectionwas then carried out, revealing a tumor that appeared necrotic but had significant vascularity (“petechiae”), including neovascularization.
59S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
appropriate seizure control [2]. Yasargil, with his introduction of micro-surgery and microtechniques, established the transsylvian approach tothe medial temporal lobe for vascular and neoplastic lesions in this re-gion. This further developed into a proximal transsylvian selectiveamygdalohippocampectomy [3]. Since then various other surgical
Fig. 6. MR Diffusion Tensor Imaging showing preservation of key white matter tracts. A. ThePostoperatively, there is restoration of typical fractional anisotropy in the IFOF.
corridors, such as subtemporal, transcortical, and the trans-middle tem-poral gyrus approaches, have been developed to offer an alternative en-trance point for resection [4–6]. Regardless of the approach taken,sparing as many structures as possible, not only the lateral temporalneocortex, but also the surrounding white matter fibers, should be an
preoperative image shows disruption of the IFOF (arrows) just anterior to the mass; B.
60 S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
important factor. The subtemporal and transsylvian approaches pene-trate the cortex either inferiorly ormedially at the limen insulae, respec-tively. They effective spare the lateral temporal neocortex, which isconsidered a non-epileptogenic zone; but can cause neuropsychologicaldeficits if removed [3]. However, this comes at the expense of thesubtemporal approach requiring significant brain retraction, very littleworking space, and as a result, a risk of injury to the vein of Labbé.The transsylvian approach on the other hand, may cause injury tothe vessels of the middle cerebral arteries and perforators (laterallenticulostriate arteries) and possibly to the uncinate fasciculus itself[6,10].
In order to avoid, as much as possible, the eloquent areas of thebrain, and reduce postoperative deficits, interest has recently shiftedto intraoperative MR imaging. Integrating functional data with naviga-tional tools has allowed accurate identification of functional cortices.However, real-time knowledge of white matter fiber tracts within thesurgical corridor can only be accessed using diffusion-tensor imaging(DTI). Nimsky et al. [7] reported that shifting of white matter tracts isoften caused by surgical intervention, and can be effectively visualizedusing intraoperative DTI. Tumors can not only displace, but infiltratenearby white matter tracts [8]. Rodriguez-Cruces and Concha [9] haveindicated that reduction in fractional anisotropy and increases inmeandiffusivity aremost prominent inwhitematter tracts closely asso-ciated with the epileptogenic temporal lobe, such as the uncinate andarcuate fasciculi, cingulum and external capsule. Nearby contralateralstructures, such as the corpus callosum can also be affected, especiallywith an infiltrating neoplastic lesion, as in this case.
Knowledge of the anatomical intricacy of our approaches and theheterogeneity of the temporal lobe itself necessitated the display ofreal-time DTI imaging in conjunction with trajectory planning using atranscylindrical approach with the BP port system. Ogura et al. [11]have introduced a transcylindrical approach for intraparenchymal le-sions. They commented on trying to avoid the need for unnecessary re-traction during surgery, which in effect decreases the risk of injury tobrain matter. Kassam's group applied the use of a transulcal port accessfor evacuation of intracerebral hemorrhage (ICH) [12]. With the aid ofMRI tractography, dominant, eloquent cortical and subcortical regionswere safely accessed, with limited collateral tissue injury. With regardto the pressure exerted on the brain itself during port insertion, it hasbeen shown that forces are more widely distributed and are minimal(10–15 mm Hg), as compared to conventional microsurgical retractorsystems [13,14]. In contrast to the risk of vascular injury and vasospasmin a traditional transsylvian or transcortical approach, no such injury hasbeen noted in a transcylindrical approach using a port [15,16].
The combination of DTI with 3D rendering that can be precisely reg-istered to standard MRI sequences, as well as detailed vascular imagingwith CT angiography, provides a comprehensive dataset for preopera-tive trajectory planning. In this case, the trajectory was designed tospare the surrounding eloquent tracts, including uncinate fasciculus,Meyer's loop, IFOF, and ILF. The technical nuances of using the combina-tion of all of these technologies has been detailed in a recent report byour group describing an integrated systems approach to access the sub-cortical space [17,18].
In this particular case the preoperative planning required a relativelyanterior, inferior, and lateral engagement point to maximize tract pres-ervation, which can be re-evaluated intra-operatively with real-timedisplay of the 3D tractography. In addition, the relatively inferior trajec-tory avoids the Sylvian vessels and preserves the uncinate fasciculus.This report is novel in that it demonstrates actual recovery of the criticalwhite matter tracts that are simply bystanders in the epileptogenicfocus but are critical in neurocognitive functional preservation.
3. Conclusion
The eloquence of the temporal lobe certainlywarrants every effort tomaximize functional preservation by leaving the smallest anatomical
and physiological foot-print, thus achieving the objectives of surgery:resection of the pathology while preserving the anatomy. The work ofGazi Yasargil and Patrick Kelly ushered an era of truly minimally inva-sive subcortical surgery with the advent of transulcal corridor micro-surgery. Over the ensuing half century there has been a significantevolution in technology. However, the underlying principle of accuratepreoperative visualization and targeting, intraoperative atraumatic ac-cess and optimum visualization and tissue differentiation, remainunchanged.
The approach described in this report stands on the shoulder ofthese giants, further paving the way towards the pursuit of “zero-footprint” surgery from a functional perspective. The systematic combina-tion of the technologies described herein provides a method for selec-tive amygdalohippocampectomy and partial temporal lobectomy forthe treatment of intractable temporal lobe seizures in the presence ofa tumor.
The advent of MRI tractography, in conjunction with robotic tele-scopic visualization technology, has greatly aided the eyes of a neuro-surgeon, letting us see previously “invisible” anatomy. In this case, thisultimately allowed the objectives of surgery to be met. Not only wasthe anatomy preserved but we documented actual anatomic recoveryof critical white matter pathways. Ultimately, it is of great importanceto realize that every detail of the cortical and subcortical frameworkmatters, and therefore, should be considered eloquent and preserved.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.inat.2016.07.004.
Consent
Thepatient described has given their informed consent for collectionand potential publication of the case report.
Disclosure
Amin Kassam reports involvement in Synaptive Medical (consultant),KLS Martin (consultant), and Medtronic (Advisory board).
Conflict of interest
Authors Srikant Chakravarthi, Anthony Zbacnik, Jonathan Jennings,Melanie Fukui, Nathaniel Kojis and Richard Rovin declare that thereare no conflicts of interest regarding the publication of this paper.
Acknowledgements
We would like to thank Nico Corporation (Indianapolis, IN) andSynaptive Medical Corporation (Toronto, ON) for their support andadvisement during the implementation and manuscript preparation oftheir technologies.
References
[1] T.J. Kovanda, R.S. Tubbs, A.A. Cohen-Gadol, Transsylvian selectiveamygdalohippocampectomy for treatment of medical temporal lobe epilepsy:surgical technique and operative nuances to avoid complications, Surg. Neurol.Int. 5 (2014) 133.
[2] W. Penfield, M. Baldwin, Temporal lobe seizures and the technique of subtotaltemporal lobectomy, Ann. Surg. 136 (1952) 625–634.
[3] H.G. Weiser, N.G. Yasargil, Selective amygdalohippocampectomy as a surgicaltreatment of mesiobasal limbic epilepsy, Surg. Neurol. 17 (1982) 445–447.
[4] P. Yang, H. Zhang, J. Pei, Q. Lin, Z. Mei, Z. Chen, Y. Jia, Z. Zhong, Z. Zheng, Keyholeepilepsy surgery: corticoamygdalohippocampectomy for mesial temporal sclerosis,Neurosurg. Rev. 39 (1) (2016) 99–108.
[5] T. Hori, S. Tabuchi, M. Kurosaki, S. Kondo, A. Takenobu, T. Watanabe, Subtemporalamygdalohippocampectomy for treating medically intractable temporal lobeepilepsy, Neurosurgery 33 (1993) 50–57.
[6] P. Niemeyer, The transventricular amygdalohippocampectomy in temporal lobeepilepsy, in: M. Baldwin, P. Bailey (Eds.), Temporal Lobe Epilepsy, Charles C Thomas,Springfield, IL 1958, pp. 461–482.
61S.S. Chakravarthi et al. / Interdisciplinary Neurosurgery: Advanced Techniques and Case Management 6 (2016) 55–61
[7] C. Nimsky, O. Ganslandt, P. Hastreiter, R. Wang, T. Benner, A.G. Sorensen, R.Fahlbusch, Preoperative and intraoperative diffusion-tensor imaging-based fibertracking in glioma surgery, Neurosurgery 61 (1 Suppl) (Jul 2007) 178–185.
[8] S. Mori, K. Frederiksen, P.C. van Zijl, B. Stieltjes, M.A. Kraut, M. Solaiyappan, M.G.Pomper, Brain white matter anatomy of tumor patients evaluated with diffusiontensor imaging, Ann. Neurol. 51 (3) (2002) 377–380.
[9] R. Rodriguez-Cruces, L. Concha, White matter in temporal lobe epilepsy: clinic-pathological correlates of water diffusion abnormalities, Quant. Imaging Med.Surg. 5 (2) (2015) 264–278.
[10] B. Adada, Selective amygdalohippocampectomy via the transsylvian approach,Neurosurg. Focus. 25 (3) (2008) E5.
[11] K. Ogura, E. Tachibana, C. Aoshima, M. Sumitomo, New microsurgical technique forintraparenchymal lesions of the brain: transcylinder approach, Acta Neruochir.(Wien) 148 (2006) 779–785.
[12] B. Ritsma, A. Kassam, D. Dowlatshahi, T. Nguyen, G. Stotts, Minimally invasivesubcortical parafascicular transsulcal access for clot evacuation (Mi SPACE)for intracerebral hemorrhage, Case Reports in Neurological Medicine. 2014(2014).
[13] O. Barlas, S. Karadereler, Stereotactically guided microsurgical removal of colloidcysts, Acta Neurochir. 146 (2004) 1119–1204.
[14] K. Hongo, S. Kobayashi, A. Yokoh, K. Sugita, Monitoring retraction pressure on thebrain. An experimental and clinical study, J. Neurosurg. 66 (1987) 270–275.
[15] J.C. Fernandez-Miranda, J.A. Engh, S.K. Pathak, R. Madhok, F.E. Boada, W. Schneider,A.B. Kassam, High-definition fiber tracking guidance for intraparenchymal endo-scopic port surgery, J. Neurosurg. 113 (5) (2010) 990–999.
[16] N. McLaughlin, D.M. Prevedello, J. Engh, D.F. Kelly, A.B. Kassam, Endoneurosurgicalresection of intraventricular and intraparenchymal lesions using the port technique,World Neurosurg. 79 (2 Suppl.) (2013) (S18. E1–8).
[17] Kassam AB, Labib MA, Bafaquh M, Ghinda D, Mark J, Houlden D, Fukui MB, NguyenT, CorstenM, Piron C, Rovin R. Part I: the challenge of functional preservation: an in-tegrated systems approach using diffusion-weighted, image-guided, exoscopic-assisted, transulcal radial corridors. Innov. Neurosurg. 3. 1–2. 5–23.
[18] A.B. Kassam, M.A. Labib, M. Bafaquh, D. Ghinda, J. Mark, D. Houlden, M.B. Fukui, T.Nguyen,M. Corsten, C. Piron, R. Rovin, Part II: an evaluation of an integrated systemsapproach using diffusion-weighted, image-guided, exoscopic-assisted, transulcal ra-dial corridors, Innov. Neurosurg. 3 (1–2) (2015) 25–33.