30
H YPERTENSIVE E MERGENCIES C RITICAL C ARE OB STETRICS # T RIHEALTH C RITICAL C ARE OB Critical Care OBstetrics
HYPERTENSIVE
EMERGENCIES
CRITICAL CARE OBSTETRICS
#TRIHEALTHCRITICALCAREOB
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES
Learning Objectives
• Understand the scope of the problem
• Rationale
• Readiness
• Recognition
• Response
• Reporting
Critical Care OBstetrics
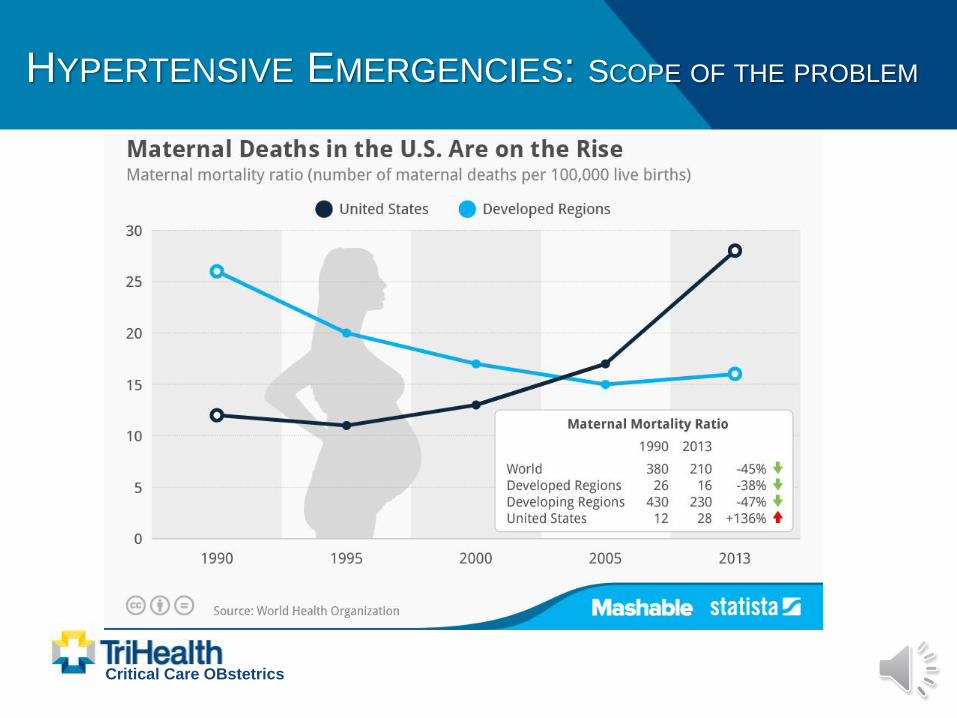
HYPERTENSIVE EMERGENCIES: SCOPE OF THE PROBLEM
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: SCOPE OF THE PROBLEM
Critical Care OBstetrics
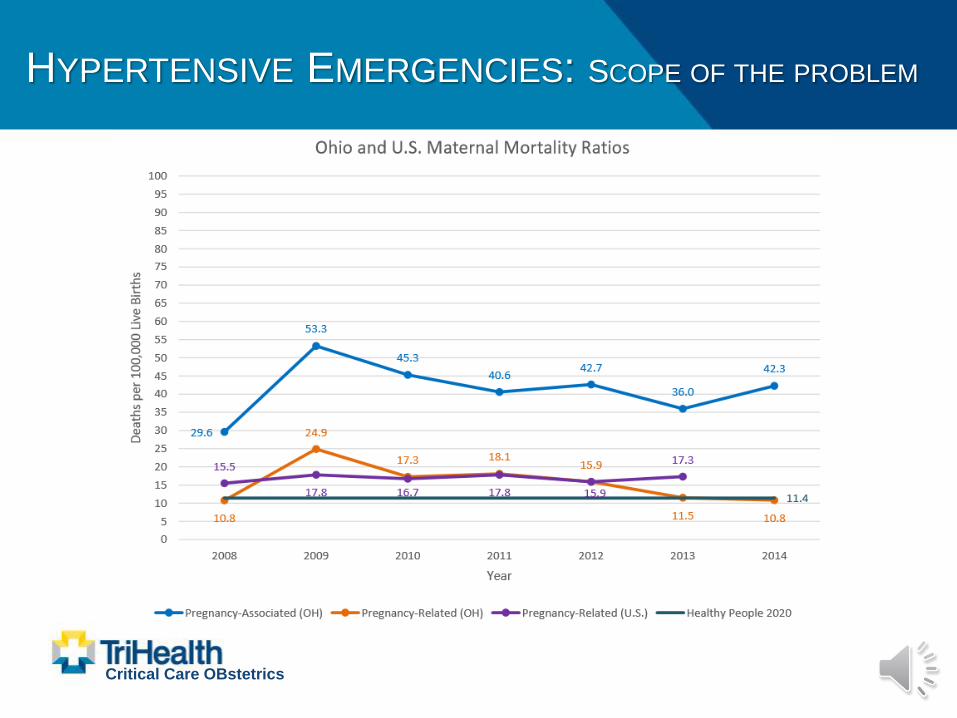
HYPERTENSIVE EMERGENCIES: SCOPE OF THE PROBLEM
MMR (Maternal Mortality Ratio) = # Maternal
Deaths / 100,000 live births (per year)
– Worldwide – MMR dropped 2.3% annually from 1990-
2015 (216/100,000 L.B’s.)
– U.S. – 1.7% annual increase (17.2/100,000 L.B’s.)
– TriHealth – equates to potentially 1-2 per year
Attributable Factors
– Increased: Maternal Age, BMI, Co-Morbidities
– Race (Non-Hispanic Black Women)
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: SCOPE OF THE PROBLEM
Critical Care OBstetrics
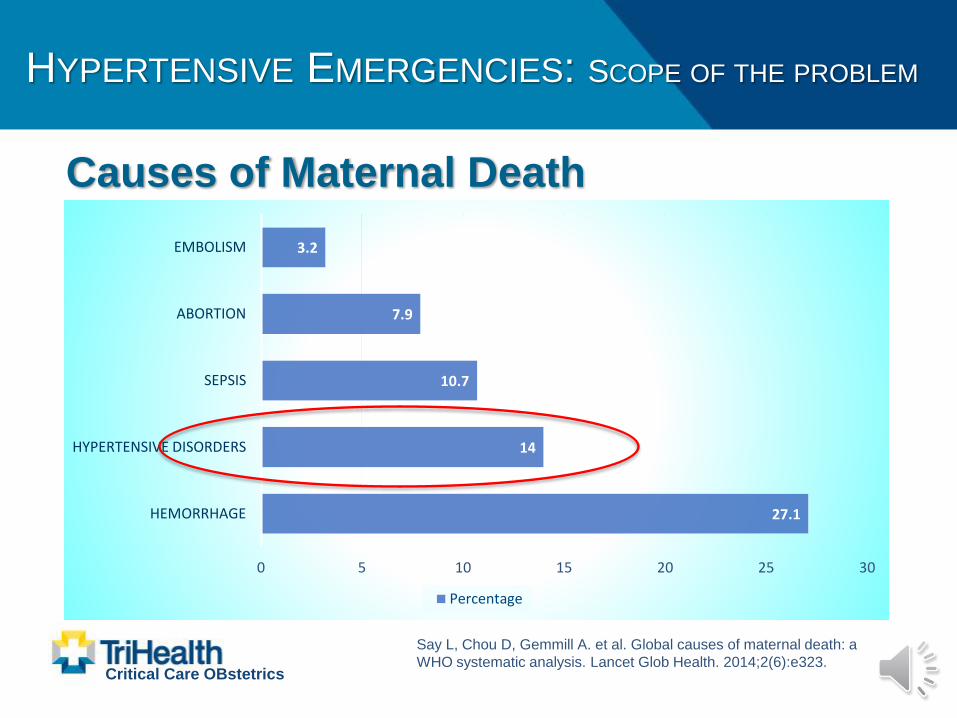
27.1
14
10.7
7.9
3.2
0 5 10 15 20 25 30
HEMORRHAGE
HYPERTENSIVE DISORDERS
SEPSIS
ABORTION
EMBOLISM
Percentage
Causes of Maternal Death
Say L, Chou D, Gemmill A. et al. Global causes of maternal death: a
WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323.

HYPERTENSIVE EMERGENCIES: SCOPE OF THE PROBLEM
Critical Care OBstetrics
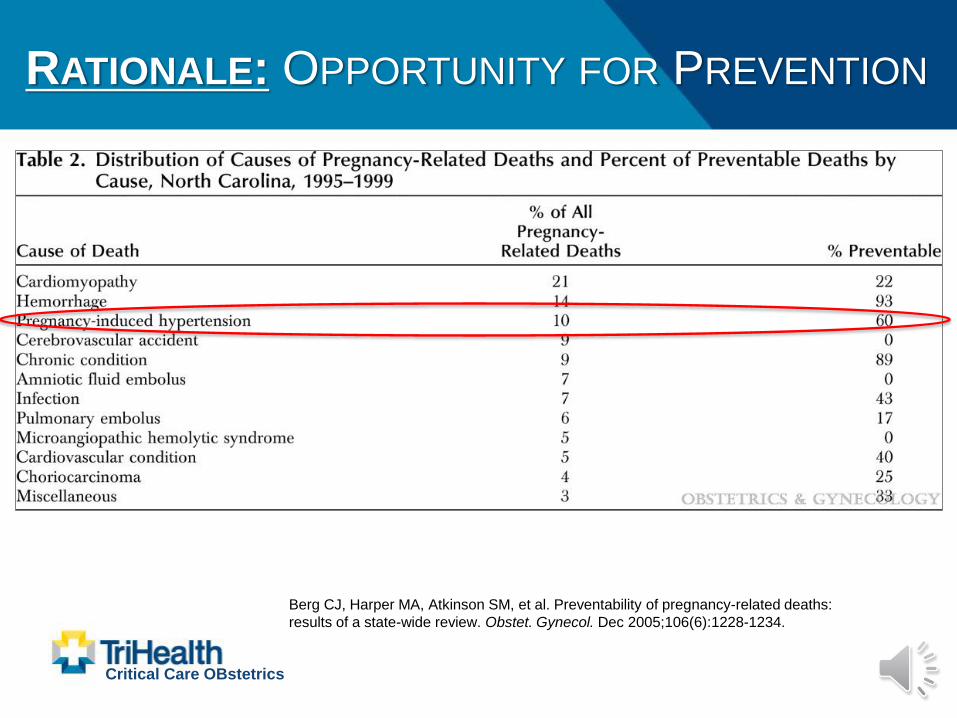
RATIONALE: OPPORTUNITY FOR PREVENTION
Critical Care OBstetrics
Berg CJ, Harper MA, Atkinson SM, et al. Preventability of pregnancy-related deaths:
results of a state-wide review. Obstet. Gynecol. Dec 2005;106(6):1228-1234.
HYPERTENSIVE EMERGENCIES: RATIONALE
Implementation of “Common Guideline” UK
• 1,087 / 210,631 women with severe
preeclampsia or eclampsia (5.2/1000)
• 151 with serious complications (13.9%)
– 82 with eclampsia (39/10,000)
– 49 required ICU admission (23/10,000)
– 0 maternal deaths
– 25 developed pulmonary edema (12/10,000)
Tuffnell DJ, Jankowicz D, Lindow SW, et al. Outcomes of severe pre-eclampsia/eclampsia in Yorkshire
1999/2003. BJOG May 2005; 112(7):875-80.
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: READINESS
Steps
1. Develop Awareness among all providers
2. Ensure Access to medications &
consultants
3. Develop Evidence-Based Protocol
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: READINESS
Ancillary Services:
• Laboratory: ability to draw & run stat labs
(CBC, CMP, LDH, Coags, UPCR)
• Pharmacy: available in Pyxis or “HTN Med
Kit”: Labetalol, Hydralazine, Magnesium
Sulfate, Calcium Gluconate, Nitric Oxide, oral
Nifedipine (short acting)
• Radiology: stat chest X ray availability
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: READINESS
Equipment:
• Maternal pulse oximetry
• Supplemental O2
• Bag-mask ventilation + suction
• Padding for bed
• Continuous electronic fetal monitoring (if
viable fetus)
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: READINESS
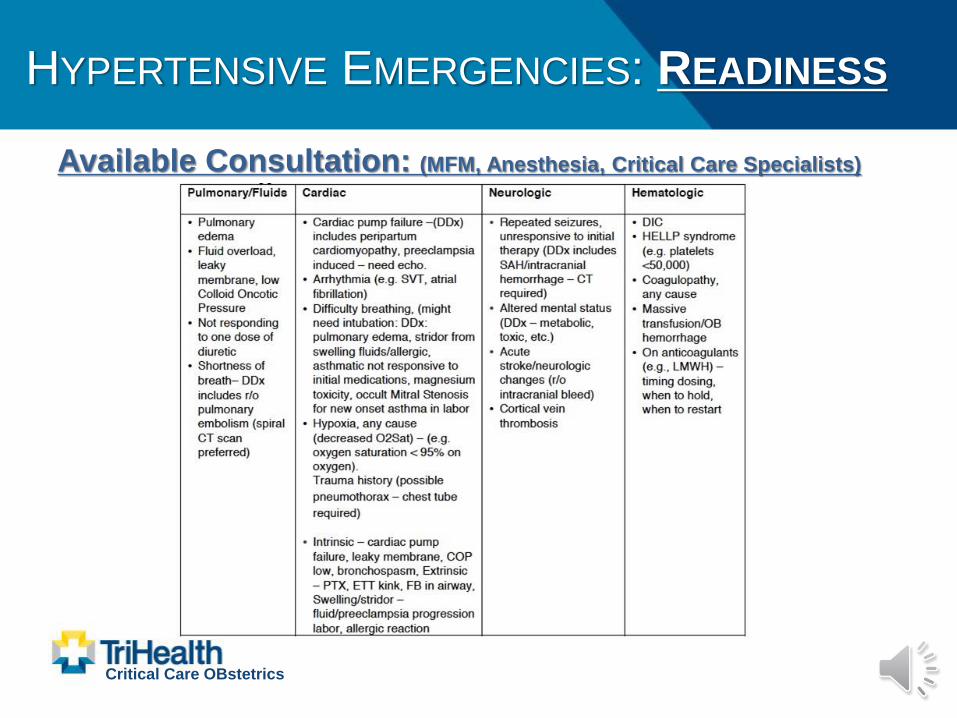
Available Consultation: (MFM, Anesthesia, Critical Care Specialists)
Critical Care OBstetrics

HYPERTENSIVE EMERGENCIES: RECOGNITION
Type of Hypertension Criteria / Characteristics
Hypertensive Emergency 2 NEW ONSET BPs > 160 mmHg systolic or 110 mmHg diastolic measured ≥ 15 min apart (does not have to be consecutive but within 1 hr of each other)
Gestational Hypertension SBP ≥ 140 or DBP ≥ 90 mmHg on 2 occasions ≥ 4 hrs apart after 20 weeks’ GA in a woman with previously normal BPs & absence of criteria for preeclampsia or CHTN
Preeclampsia GHTN definition above but in presence of proteinuria (UPCR ≥ 0.3 or 24 hr≥ 300 mg)
Preeclampsia with Severe Features 2 or more BPs > 160 mmHg systolic or 110 mmHg diastolic measured ≥ 4 hrs apart while at rest and / or GHTN definition above but in presence of proteinuria and/or thrombocytopenia (<100k), impaired liver functions (2 x upper limit), severe RUQ pain, progressive renal insufficiency (creat > 1.1 mg/dL or doubling), pulmonary edema, new onset visual or cerebral disturbance
Chronic Hypertension SBP ≥ 140 or DBP ≥ 90 mmHg on 2 occasions ≥ 4 hrs apart PRIOR TO 20 weeks’ GA
Chronic Hypertension with Super-Imposed Preeclampsia
CHTN definition now with new-onset proteinuria, sudden exacerbation of HTN when previously well-controlled, or any severe features
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RECOGNITION
Ensure Proper BP Measurement:
• Sitting or semi-recumbent position with back supported
and arm measured at heart level
• Patient resting quietly for 5 min
• Appropriate cuff size (bladder width encircles 80% arm)
• No dangling legs or legs crossed
• No consumption of caffeine or nicotine within 30 min
• Do not reposition patient to the other side in an attempt
to lower BP
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RECOGNITION
Triage / Admission Risk Assessment:Assess whether low, medium, or high risk for a Hypertensive Emergency
• Medium risk for a Hypertensive Emergency
– Two appropriately measured BPs 140-149 / 90-99 mmHg at least 15 minutes apart within
one hour (does not need to be consecutive readings) OR
– Any history of CHTN, GHTN, morbid obesity (BMI > 40), pre-gestational diabetes, or recent
ingestion of a stimulant such as cocaine, methamphetamine, or PCP
• High risk for a Hypertensive Emergency
– Two appropriately measured BP 150-159 / 100-109 mmHg at least 15 minutes apart within
one hour (does not need to be consecutive readings) AND
– Any history of above
• If “High Risk” criteria are met:
– Notification of chief resident, attending OB, charge nurse
– Labs: coags, PE1 with UPCR or PE2
– Consider Foley cath (urometer), continuous pulse ox, CEFM
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RESPONSE
BP = CO + SVRCardiac Output: Systemic Vascular Resistance
CO = HR x SV SVR = Mean Arterial Pressure (MAP) x CO
“The Pump” “The Pipes”
Wide pulse pressure Narrow pulse pressure
Factors Influencing: Factors Influencing:
- Volume (high) - Stress
- Anxiety - Volume (low)
- Pain - Caffeine, nicotine
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: SYSTOLIC VS DIASTOLIC
Systolic hypertension = most important
predictor of cerebral injury & infarction
• Series 28 women with severe preeclampsia & stroke
– 27/28 women had severe systolic hypertension prior to stroke
– 54% died
– Only 13% had severe diastolic HTN prior
– Similar findings among non-pregnant adults
Tuffnell DJ, Jankowicz D, Lindow SW, et al. Outcomes of severe pre-eclampsia/eclampsia in Yorkshire
1999/2003. BJOG May 2005; 112(7):875-80.
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RESPONSE
Whom to Activate the Protocol:
• Two NEW ONSET blood pressure values
greater than 160 mmHg (systolic) or 110 mmHg
(diastolic) appropriately measured at least 15
minutes apart (does not have to be consecutive
but do occur within 1 hour of each other)
• “New Onset” denotes blood pressure elevations
into the severe range for the first time in at least
72 hours
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RESPONSE
Goal: initiation of treatment within 30-60 min
• Target BP: 2 consecutive BP readings measured appropriately <
160 mm Hg (systolic) or < 110 mm Hg (diastolic) no sooner than 15
minutes apart
• Adequate reduction is a witnessed drop in systolic BP > 20 mmHg
and/or drop in diastolic BP > 10 mmHg – if this is witnessed,
withhold additional treatment doses for 10 minutes and repeat BP
measurements
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RESPONSE
Steps:1. Initiate Magnesium Sulfate protocol if suspicion for
preeclampsia
2. Base determination of initial anti-HTN med by patient’s
PMHx, allergies, whether the HTN is predominantly
systolic or diastolic, and pulse pressure– If underlying heart failure, asthma, cocaine or methamphetamine abuse,
bradycardia (HR < 60 bpm) – avoid Labetalol
– If predominantly systolic HTN and pulse pressure is > 70, consider
Labetalol
– If predominantly diastolic HTN and pulse pressure is < 50, consider
Hydralazine
– If mixed picture or no IV access, initiate oral Nifedipine
Critical Care OBstetrics
HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
Stage:
Definition
Nurse
to
Patient
Ratio:
Monitoring:
Notify:
At
Bedside:
Meds & Frequency:
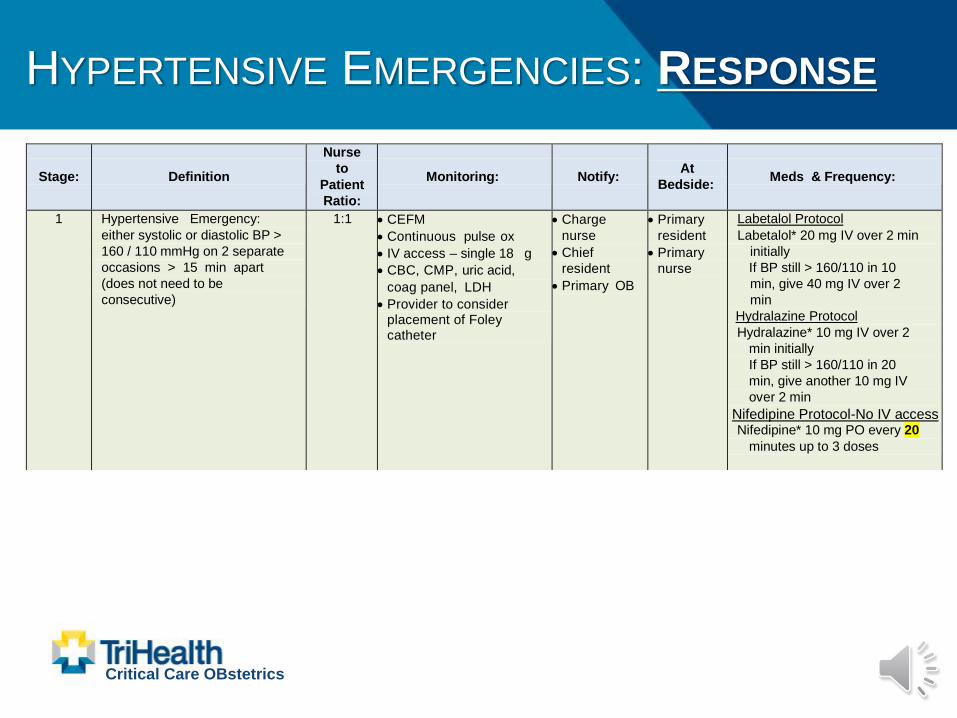
1 Hypertensive Emergency:
either systolic or diastolic BP >
160 / 110 mmHg on 2 separate
occasions > 15 min apart
(does not need to be
consecutive)
1:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• CBC, CMP, uric acid,
coag panel, LDH
• Provider to consider placement of Foley catheter
• Charge
nurse
• Chief
resident
• Primary OB
• Primary
resident
• Primary
nurse
Labetalol Protocol
Labetalol* 20 mg IV over 2 min
initially
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
Hydralazine Protocol
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Nifedipine Protocol-No IV access Nifedipine* 10 mg PO every 20
minutes up to 3 doses
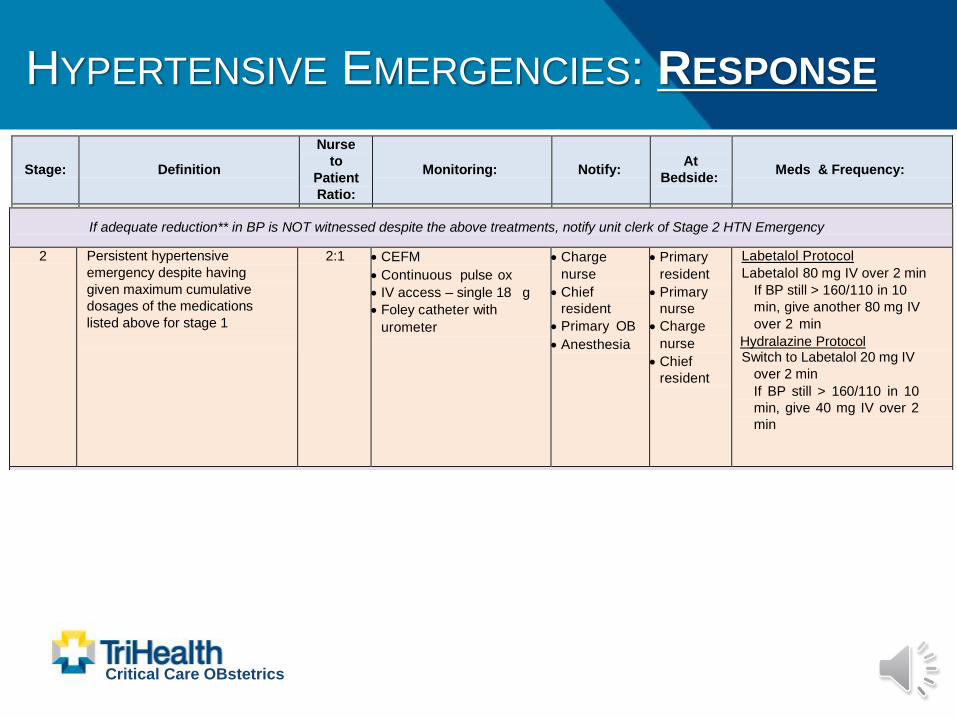
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 2 HTN Emergency
2 Persistent hypertensive
emergency despite having
given maximum cumulative
dosages of the medications
listed above for stage 1
2:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• Foley catheter with
urometer
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
Labetalol Protocol
Labetalol 80 mg IV over 2 min
If BP still > 160/110 in 10
min, give another 80 mg IV
over 2 min
Hydralazine Protocol Switch to Labetalol 20 mg IV
over 2 min
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
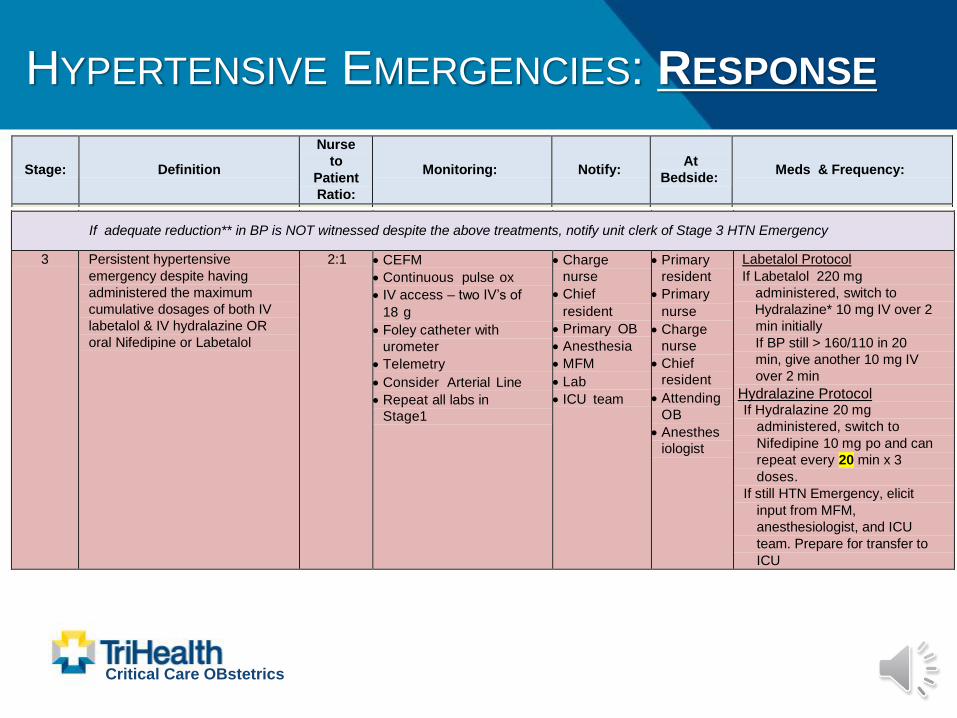
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 3 HTN Emergency
3 Persistent hypertensive
emergency despite having
administered the maximum
cumulative dosages of both IV
labetalol & IV hydralazine OR
oral Nifedipine or Labetalol
2:1 • CEFM
• Continuous pulse ox
• IV access – two IV’s of
18 g
• Foley catheter with
urometer
• Telemetry
• Consider Arterial Line
• Repeat all labs in
Stage1
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• MFM
• Lab
• ICU team
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
• Attending
OB
• Anesthes
iologist
Labetalol Protocol
If Labetalol 220 mg
administered, switch to
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Hydralazine Protocol If Hydralazine 20 mg
administered, switch to
Nifedipine 10 mg po and can
repeat every 20 min x 3
doses.
If still HTN Emergency, elicit
input from MFM,
anesthesiologist, and ICU
team. Prepare for transfer to
ICU
HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
Stage:
Definition
Nurse
to
Patient
Ratio:
Monitoring:
Notify:
At
Bedside:
Meds & Frequency:
1 Hypertensive Emergency:
either systolic or diastolic BP >
160 / 110 mmHg on 2 separate
occasions > 15 min apart
(does not need to be
consecutive)
1:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• CBC, CMP, uric acid,
coag panel, LDH
• Provider to consider placement of Foley catheter
• Charge
nurse
• Chief
resident
• Primary OB
• Primary
resident
• Primary
nurse
Labetalol Protocol
Labetalol* 20 mg IV over 2 min
initially
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
Hydralazine Protocol
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Nifedipine Protocol-No IV access Nifedipine* 10 mg PO every 20
minutes up to 3 doses
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 2 HTN Emergency
2 Persistent hypertensive
emergency despite having
given maximum cumulative
dosages of the medications
listed above for stage 1
2:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• Foley catheter with
urometer
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
Labetalol Protocol
Labetalol 80 mg IV over 2 min
If BP still > 160/110 in 10
min, give another 80 mg IV
over 2 min
Hydralazine Protocol Switch to Labetalol 20 mg IV
over 2 min
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 3 HTN Emergency
3 Persistent hypertensive
emergency despite having
administered the maximum
cumulative dosages of both IV
labetalol & IV hydralazine OR
oral Nifedipine or Labetalol
2:1 • CEFM
• Continuous pulse ox
• IV access – two IV’s of
18 g
• Foley catheter with
urometer
• Telemetry
• Consider Arterial Line
• Repeat all labs in
Stage1
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• MFM
• Lab
• ICU team
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
• Attending
OB
• Anesthes
iologist
Labetalol Protocol
If Labetalol 220 mg
administered, switch to
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Hydralazine Protocol If Hydralazine 20 mg
administered, switch to
Nifedipine 10 mg po and can
repeat every 20 min x 3
doses.
If still HTN Emergency, elicit
input from MFM,
anesthesiologist, and ICU
team. Prepare for transfer to
ICU
Stage:
Definition
Nurse
to
Patient
Ratio:
Monitoring:
Notify:
At
Bedside:
Meds & Frequency:
1 Hypertensive Emergency:
either systolic or diastolic BP >
160 / 110 mmHg on 2 separate
occasions > 15 min apart
(does not need to be
consecutive)
1:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• CBC, CMP, uric acid,
coag panel, LDH
• Provider to consider placement of Foley catheter
• Charge
nurse
• Chief
resident
• Primary OB
• Primary
resident
• Primary
nurse
Labetalol Protocol
Labetalol* 20 mg IV over 2 min
initially
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
Hydralazine Protocol
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Nifedipine Protocol-No IV access Nifedipine* 10 mg PO every 20
minutes up to 3 doses
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 2 HTN Emergency
2 Persistent hypertensive
emergency despite having
given maximum cumulative
dosages of the medications
listed above for stage 1
2:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• Foley catheter with
urometer
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
Labetalol Protocol
Labetalol 80 mg IV over 2 min
If BP still > 160/110 in 10
min, give another 80 mg IV
over 2 min
Hydralazine Protocol Switch to Labetalol 20 mg IV
over 2 min
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 3 HTN Emergency
3 Persistent hypertensive
emergency despite having
administered the maximum
cumulative dosages of both IV
labetalol & IV hydralazine OR
oral Nifedipine or Labetalol
2:1 • CEFM
• Continuous pulse ox
• IV access – two IV’s of
18 g
• Foley catheter with
urometer
• Telemetry
• Consider Arterial Line
• Repeat all labs in
Stage1
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• MFM
• Lab
• ICU team
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
• Attending
OB
• Anesthes
iologist
Labetalol Protocol
If Labetalol 220 mg
administered, switch to
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Hydralazine Protocol If Hydralazine 20 mg
administered, switch to
Nifedipine 10 mg po and can
repeat every 20 min x 3
doses.
If still HTN Emergency, elicit
input from MFM,
anesthesiologist, and ICU
team. Prepare for transfer to
ICU
HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
Stage:
Definition
Nurse
to
Patient
Ratio:
Monitoring:
Notify:
At
Bedside:
Meds & Frequency:
1 Hypertensive Emergency:
either systolic or diastolic BP >
160 / 110 mmHg on 2 separate
occasions > 15 min apart
(does not need to be
consecutive)
1:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• CBC, CMP, uric acid,
coag panel, LDH
• Provider to consider placement of Foley catheter
• Charge
nurse
• Chief
resident
• Primary OB
• Primary
resident
• Primary
nurse
Labetalol Protocol
Labetalol* 20 mg IV over 2 min
initially
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
Hydralazine Protocol
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Nifedipine Protocol-No IV access Nifedipine* 10 mg PO every 20
minutes up to 3 doses
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 2 HTN Emergency
2 Persistent hypertensive
emergency despite having
given maximum cumulative
dosages of the medications
listed above for stage 1
2:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• Foley catheter with
urometer
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
Labetalol Protocol
Labetalol 80 mg IV over 2 min
If BP still > 160/110 in 10
min, give another 80 mg IV
over 2 min
Hydralazine Protocol Switch to Labetalol 20 mg IV
over 2 min
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 3 HTN Emergency
3 Persistent hypertensive
emergency despite having
administered the maximum
cumulative dosages of both IV
labetalol & IV hydralazine OR
oral Nifedipine or Labetalol
2:1 • CEFM
• Continuous pulse ox
• IV access – two IV’s of
18 g
• Foley catheter with
urometer
• Telemetry
• Consider Arterial Line
• Repeat all labs in
Stage1
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• MFM
• Lab
• ICU team
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
• Attending
OB
• Anesthes
iologist
Labetalol Protocol
If Labetalol 220 mg
administered, switch to
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Hydralazine Protocol If Hydralazine 20 mg
administered, switch to
Nifedipine 10 mg po and can
repeat every 20 min x 3
doses.
If still HTN Emergency, elicit
input from MFM,
anesthesiologist, and ICU
team. Prepare for transfer to
ICU
Stage:
Definition
Nurse
to
Patient
Ratio:
Monitoring:
Notify:
At
Bedside:
Meds & Frequency:
1 Hypertensive Emergency:
either systolic or diastolic BP >
160 / 110 mmHg on 2 separate
occasions > 15 min apart
(does not need to be
consecutive)
1:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• CBC, CMP, uric acid,
coag panel, LDH
• Provider to consider placement of Foley catheter
• Charge
nurse
• Chief
resident
• Primary OB
• Primary
resident
• Primary
nurse
Labetalol Protocol
Labetalol* 20 mg IV over 2 min
initially
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
Hydralazine Protocol
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Nifedipine Protocol-No IV access Nifedipine* 10 mg PO every 20
minutes up to 3 doses
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 2 HTN Emergency
2 Persistent hypertensive
emergency despite having
given maximum cumulative
dosages of the medications
listed above for stage 1
2:1 • CEFM
• Continuous pulse ox
• IV access – single 18 g
• Foley catheter with
urometer
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
Labetalol Protocol
Labetalol 80 mg IV over 2 min
If BP still > 160/110 in 10
min, give another 80 mg IV
over 2 min
Hydralazine Protocol Switch to Labetalol 20 mg IV
over 2 min
If BP still > 160/110 in 10
min, give 40 mg IV over 2
min
If adequate reduction** in BP is NOT witnessed despite the above treatments, notify unit clerk of Stage 3 HTN Emergency
3 Persistent hypertensive
emergency despite having
administered the maximum
cumulative dosages of both IV
labetalol & IV hydralazine OR
oral Nifedipine or Labetalol
2:1 • CEFM
• Continuous pulse ox
• IV access – two IV’s of
18 g
• Foley catheter with
urometer
• Telemetry
• Consider Arterial Line
• Repeat all labs in
Stage1
• Charge
nurse
• Chief
resident
• Primary OB
• Anesthesia
• MFM
• Lab
• ICU team
• Primary
resident
• Primary
nurse
• Charge
nurse
• Chief
resident
• Attending
OB
• Anesthes
iologist
Labetalol Protocol
If Labetalol 220 mg
administered, switch to
Hydralazine* 10 mg IV over 2
min initially
If BP still > 160/110 in 20
min, give another 10 mg IV
over 2 min
Hydralazine Protocol If Hydralazine 20 mg
administered, switch to
Nifedipine 10 mg po and can
repeat every 20 min x 3
doses.
If still HTN Emergency, elicit
input from MFM,
anesthesiologist, and ICU
team. Prepare for transfer to
ICU
HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
Key Points:
• Notify unit clerk and “rally the troops”
• Perform a “huddle” & appoint a leader
• Reassess every 10-15 minutes and follow
protocol
• Ensure the patient’s family is supported
• Continue until 2 consecutive BP readings no
sooner than 15 minutes apart are obtained at or
below goal
HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
Upon Resolution:
• Repeat BPs q 15 min x 1 hr
– Then every 30 min x 1 hr
– Then every 60 min x 4 hrs
• Initiate an ORAL agent aligned with what worked
best in protocol

HYPERTENSIVE EMERGENCIES: RESPONSE
Critical Care OBstetrics
If NO Resolution with Protocol:
• Consider consultation by MFM, Anesthesia, or
Intensivist
• Patient may need to be transported to a higher
acuity bed like ICU for
initiation of “drip” agent
• Additional triggers for
consultation
REPORTING / SYSTEMS LEARNING
• Establish a culture of huddles for high-risk
patients and post-event debriefs
• Conduct a multidisciplinary review of
serious Hypertensive Emergencies for
systems issues
• Monitor outcomes and processes metrics
Critical Care OBstetrics
TAKE-AWAY POINTS
• Most maternal major morbidity & mortality
from Hypertensive Emergencies are
preventable
• Preparation and awareness are
ESSENTIAL
• Requires reliance not on individuals but on
team approach
Critical Care OBstetrics
Thank You
Critical Care OBstetrics
CRITICAL CARE OBSTETRICS
#TRIHEALTHCRITICALCAREOB

















