
5/24/2017
1
Rich Rohaley, PharmD, RPh
Objectives� Describe the steroid hormone cascade
� Understand the pathophysiology of symptoms resulting
from hormone depletion
� Discuss menopausal treatment options including bio-
identical hormone replacement
� Apply laboratory results to guide hormone replacement
therapy dose adjustment
5/24/2017
2
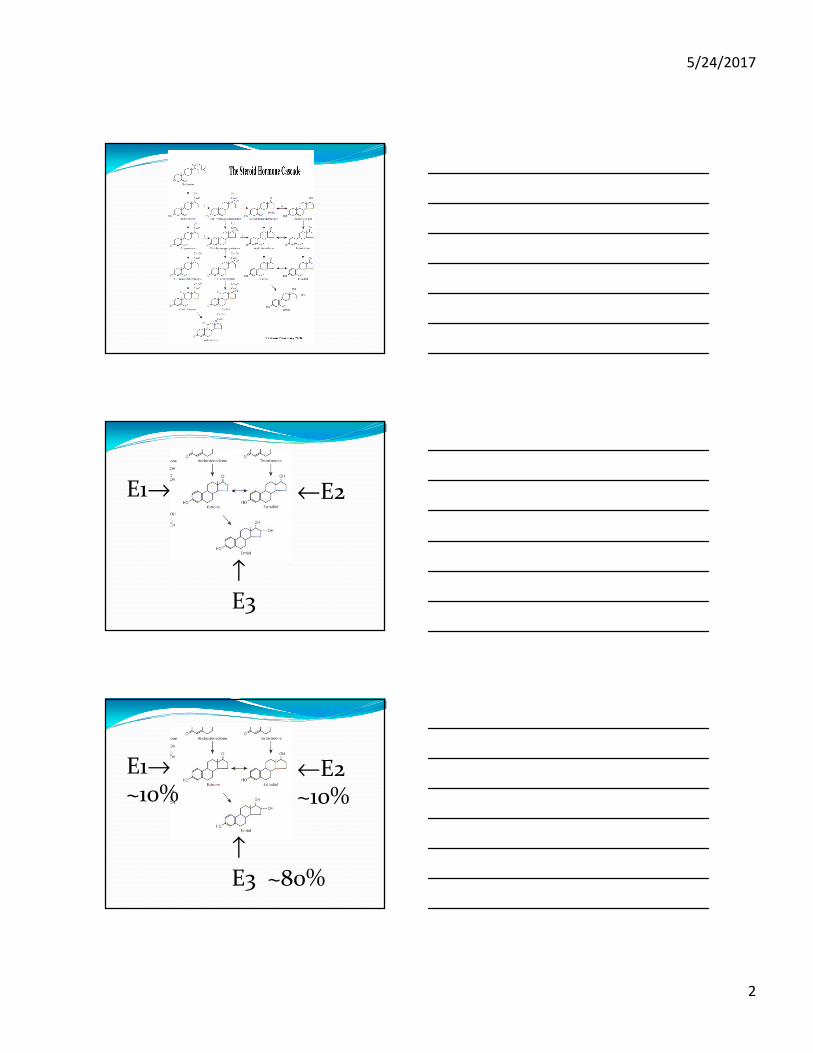
E1→ ←E2
↑
E3
E1→~10%
←E2~10%
↑
E3 ~80%
5/24/2017
3
5/24/2017
4
Lab ValuesFemale Male
� Estradiol
� Estrone
� FSH
� Progesterone
� LH
� Testosterone (total)
� DHEA-sulfate
� Cortisol
� Testosterone (free)
� Testosterone (total)
� Dehydrotestosterone
� DHEA-sulfate
� Estrogens (total)
� Progesterone
� Cortisol
Treatment Options
Treatment Options� Estrogens
� Premarin
� Cenestin & Enjuvia
� Estrace, Climara, Vivelle, Estring
� Femring
� Vagifem
� Estinyl
� Ortho-Est & Ogen
� Progesterone & Progestins
� Provera
� Prometrium
� Micronor & Aygestin
� Combinations
� Prempro
� Femhrt
� Activella & Combipatch
� Estratest
5/24/2017
5
Why patients ask for Bio-Identical� ‘Cause Oprah said so
� ‘Cause Suzanne Somers wrote that book
� They want to avoid pharmaceuticals
� To be more “natural”
What does Bio-Identical mean?� Hormone chemically identical to what the organ (ovary)
releases
� Further defined to come from a natural source
� Further defined as varying in concentration/strength;
designed to be specific for any one individual
5/24/2017
6
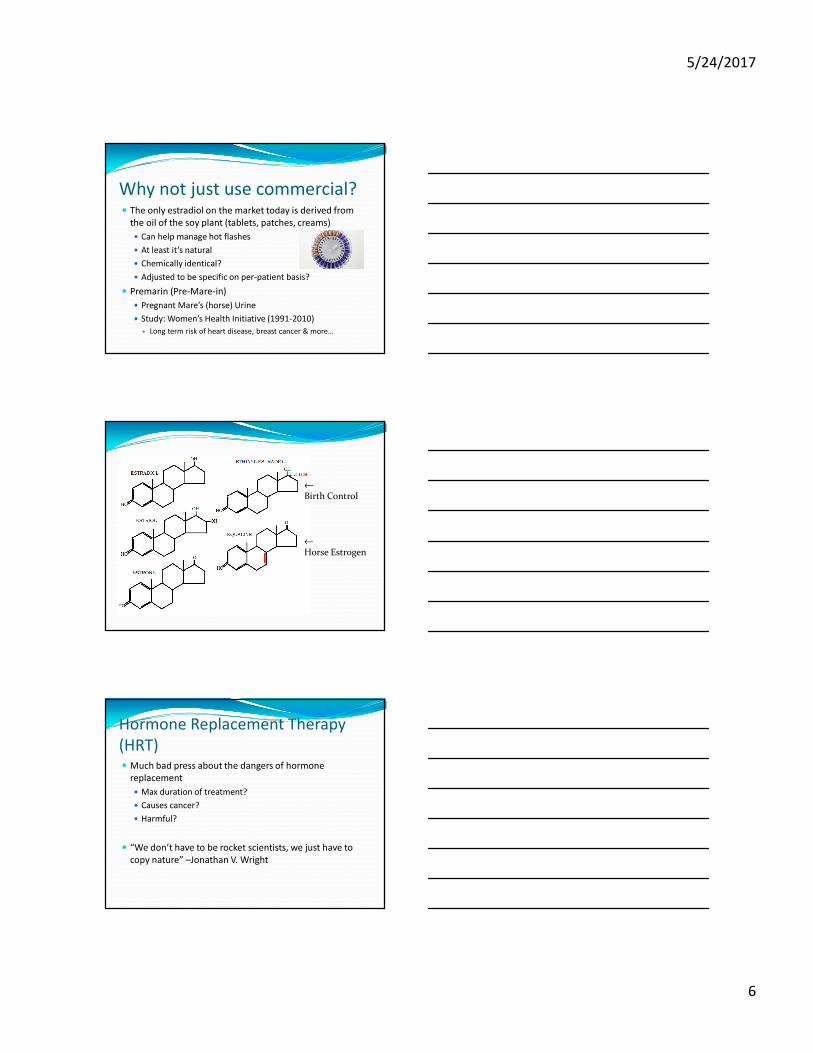
Why not just use commercial?� The only estradiol on the market today is derived from
the oil of the soy plant (tablets, patches, creams)
� Can help manage hot flashes
� At least it’s natural
� Chemically identical?
� Adjusted to be specific on per-patient basis?
� Premarin (Pre-Mare-in)
� Pregnant Mare’s (horse) Urine
� Study: Women’s Health Initiative (1991-2010)
� Long term risk of heart disease, breast cancer & more…
←
Birth Control
←
Horse Estrogen
Hormone Replacement Therapy
(HRT)� Much bad press about the dangers of hormone
replacement
� Max duration of treatment?
� Causes cancer?
� Harmful?
� “We don’t have to be rocket scientists, we just have to
copy nature” –Jonathan V. Wright
5/24/2017
7
Women’s Health InitiativeCompared with the placebo, estrogen plus progestin resulted in:
Compared with the placebo, estrogen alone resulted in:
� Increased risk of heart attack
� Increased risk of stroke
� Increased risk of blood clots
� Increased risk of breast cancer
� Reduced risk of colorectal cancer
� Fewer fractures
(study included only women 65 and
older)
� No difference in risk for heart attack
� Increased risk of stroke
� Increased risk of blood clots
� Uncertain effect for breast cancer
� No difference in risk for colorectal cancer
� Reduced risk of fracture
(Findings about memory and cognitive function are not yet available)
Progesterone and Anticancer
Studies� Simon JA, Robinson DE, Andrews MC, et al. The
absorption of oral micronized progesterone: The effect of
food, dose proportionality, and comparison with
intramuscular progesterone. Fertil Steril 1993;60:26-33.
� Kim S, Korhonen M, Wilborn W, et al. Antiproliferative
effects of low-dose micronized progesterone. Fertil Steril
1996;65:323-331.
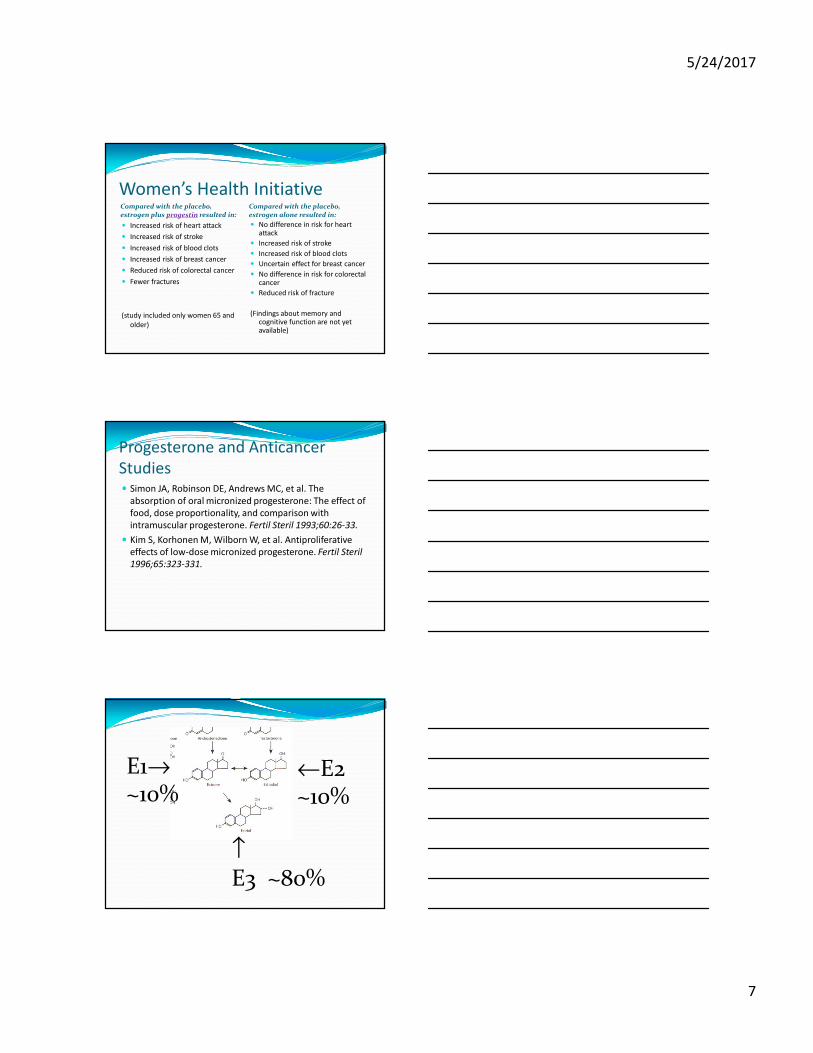
E1→~10%
←E2~10%
↑
E3 ~80%
5/24/2017
8
Estrogens� Estradiol (E2) ~ 10-20% of circulating estrogen
� High potency
� Estrone (E1) ~ 10-20% of circulating estrogen
� Medium potency
� Estriol (E3) ~ 60-80% of circulating estrogen
� Low potency (1/100th the strength of E2)
� If it’s so weak, why bother with it?
Estriol (E3)� Originally (~90 years ago) thought to be just a metabolite
of estradiol
� “It would be unusual if nature produced three estrogens of which only one was utilized” –J.Wright
� E1 and E2 are competitively inhibited by E3
� This reduces estrogenicity/estrogen dominance
� Risk of cancer virtually vanishes
� Even in high doses does not promote endometrial proliferation
� Great treatment for vaginal atrophy (vaginal thinning or painful intercourse), recurrent UTI’s, incontinence
Estrogen in Bio-HRT� “TriEst”
� 10% : 10% : 80% (E1:E2:E3)
� 3 : 7 : 90
� Bi-Est
� Comprised of E2 and E3
� E1 removed due to potential side effects
� 10 : 90
� 20 : 80
� 50 : 50
5/24/2017
9
Estrogens� Estrogens increase HDL
� May be why premenopausal women are protected from
heart disease
� Maintain bone density
� Bisphosphonates maintain and may increase bone density
by 2-3%
� Combination HRT may increase bone density by >15%
Serum E2� Menopause = E2 <50pg/ml
� Associated with anxiousness & depression
� Postmenopausal women are found to feel the best when
E2 levels are between 50-150pg/ml
Progestins vs. Progesterone� Progestins:
� Synthetic “estrogens”
� Patentable receptor substitutes
� Ex: Provera®, Micronor®
� Progesterone
� Chemically identical
� Does not interfere with estrogen’s cardio-protection
� Virtually no unwanted effects
5/24/2017
10
Progesterone Intro� Important component of HRT
� Menopausal women with an intact uterus continue to
produce estrogen, and unopposed estrogen can further
stimulate the endometrial tissue
� Abnormal bleeding
� Endometrial cancer proliferation
� Must be added to estrogen therapy to reduce this
overstimulation
� Proven to reduce risk of endometrial cancer
Progesterone in HRT� Progesterone deficiency (w/relation to estrogen) may lead to:
� Swollen breasts / breast tenderness
� Headaches
� Low libido
� Depression / anxiety
� Mood swings / irritability
� Insomnia
� Lack of focus
� Acne
� Weight gain / bloating
� Joint pain
� Early menstruation
� Cramps
PMS & Pre or Peri-Menopause� Associated with declining estrogen, testosterone, and
progesterone
� Often the symptoms are misdiagnosed and treated as
individual symptoms
� Ex: Depression → SSRI’s (Prozac)
5/24/2017
11
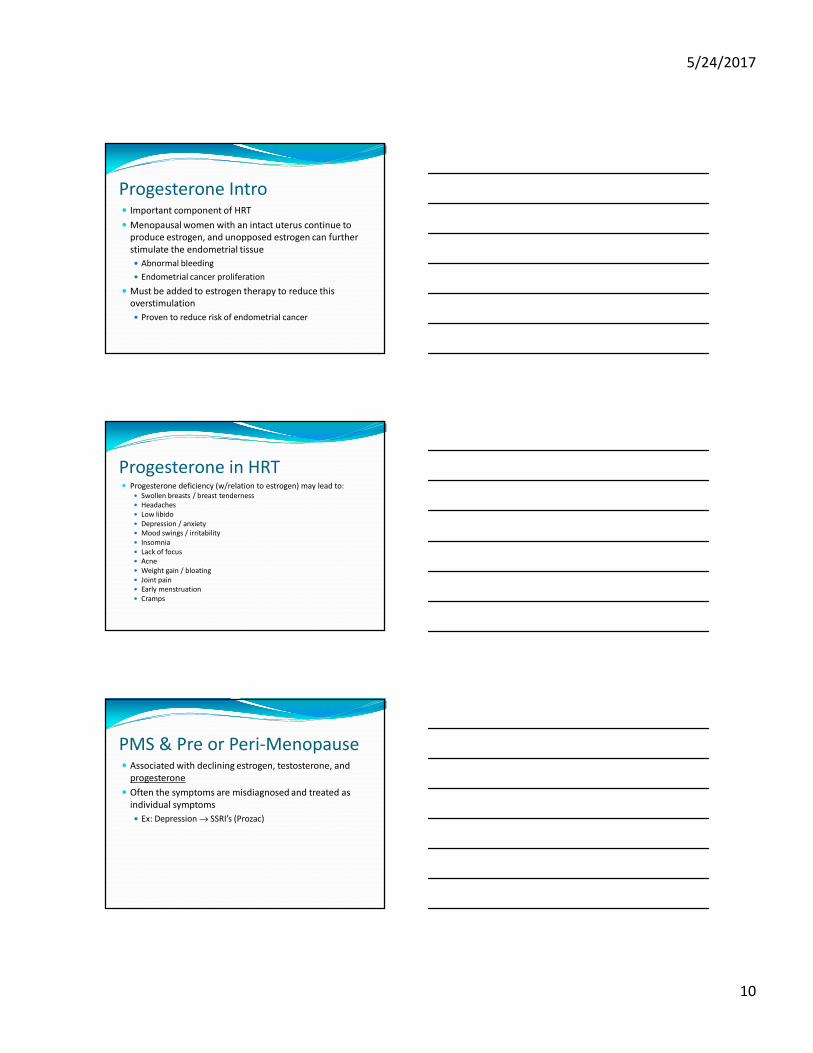
HRT & Osteoporosis
HRT & Osteoporosis� Progesterone
� Can rebuild bone, even after it’s been lost
� Osteoblast activation
� DHEA
� Testosterone
5/24/2017
12
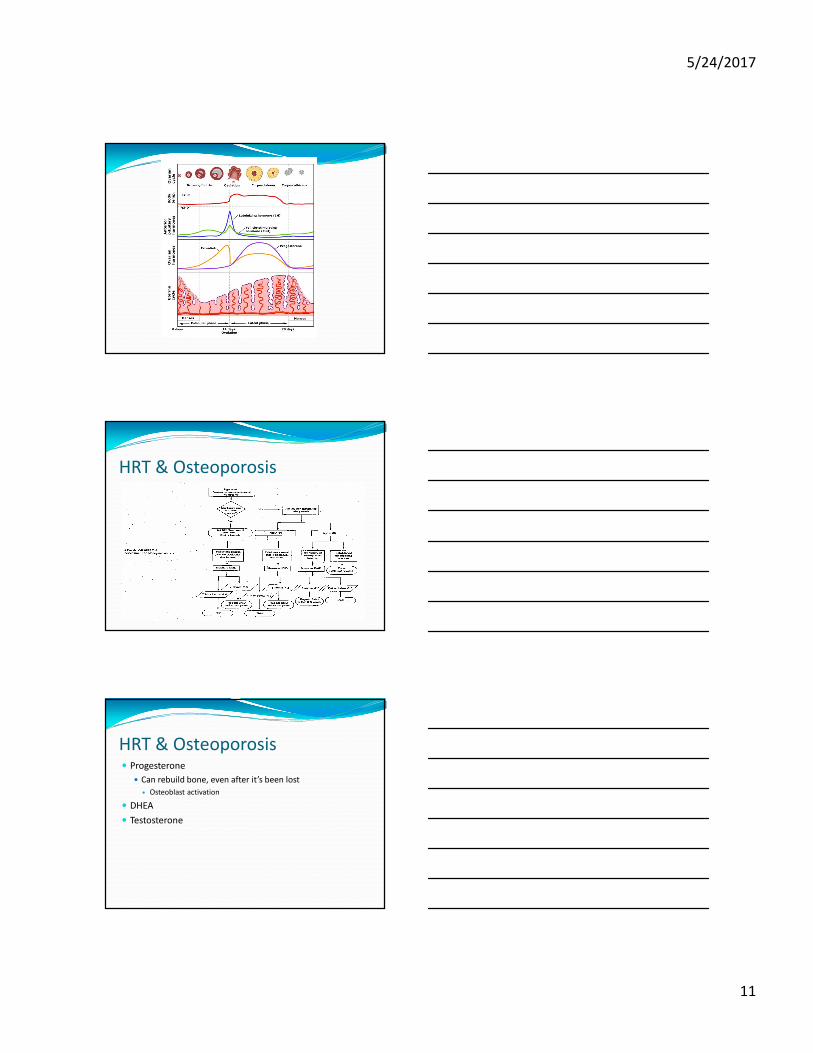
HRT & Menopause
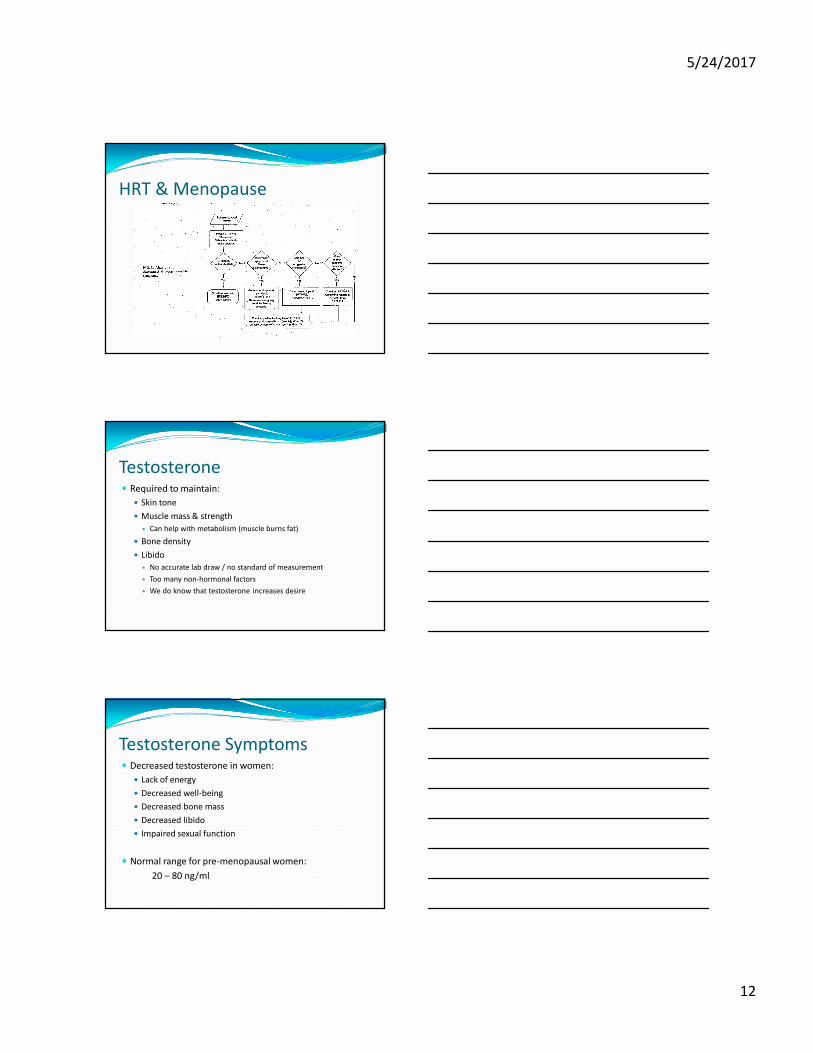
Testosterone� Required to maintain:
� Skin tone
� Muscle mass & strength
� Can help with metabolism (muscle burns fat)
� Bone density
� Libido
� No accurate lab draw / no standard of measurement
� Too many non-hormonal factors
� We do know that testosterone increases desire
Testosterone Symptoms� Decreased testosterone in women:
� Lack of energy
� Decreased well-being
� Decreased bone mass
� Decreased libido
� Impaired sexual function
� Normal range for pre-menopausal women:
20 – 80 ng/ml
5/24/2017
13
Dosage Forms for HRT� Oral
� Capsules
� Buccal
� Troche
� Transdermal
� Creams
� Gels
� Vaginal
� Suppositories
� Creams
Patient Cases� LG is a 52 YOF with complaints of hot flashes and night
sweats that are waking her every two hours. She also
complains of fatigue and a mental “fog” affecting her
productivity at work
� What lab values could be useful?
� Is she a Bio-HRT candidate?
� Which hormones should be included?
Useful Lab ValuesFemale
� Estradiol
� Estrone
� FSH
� Progesterone
� LH
� Testosterone (total)
� DHEA-sulfate
� Cortisol
5/24/2017
14
Potential Starting Dose� Oral Capsule:
� TriEst (10/10/80%) 1mg
Progesterone 100mg
DHEA 5mg SR Capsule
� Take one capsule once daily for 10 days, then increase to
one capsule twice daily
Patient Cases� After initiating a sustained release capsule of TriEst 1mg
/Progesterone 100mg / DHEA 5mg four weeks ago, the
patient calls back complaining of mastalgia. Her hot
flashes are gone and she’s sleeping great. For this reason,
she’s willing to tolerate the tenderness. What should we
do?
Adjusted Dose
5/24/2017
15
Patient Cases� NH is a 42 YOF presenting with
weight gain and difficulty sleeping. She is a yoga instructor and exercises very regularly claiming nothing in her diet has significantly changed. She asks if there’s anything she can do for her weight that isn’t a “pharmaceutically engineered monster”.
� Labs
� E2 = 122 pg/ml
� E1 = 55 pg/ml
� FSH = 45 mIU/ml
� Progesterone = 0.2 ng/ml
� LH = 27 mIU/ml
� Cortisol = 4.7ug/dl
Potential Starting Dose� Transdermal Cream:
� Progesterone 100mg/ml Cream
� Apply 0.5ml to an area of thin skin every evening, rub in well and
rotate sites
Patient Cases� NH saw weight loss of 3 lbs
over 6 weeks. She decided that
if a little helped a little, a lot
may help a lot. She self
adjusted her dose to 2ml of the
cream. She now notes
regaining the lost weight with
10 extra lbs from baseline,
noting water retention and
bloating.
� Labs
� E2 = 116 pg/ml
� E1 = 56 pg/ml
� FSH = 43 mIU/ml
� Progersterone =
12 ng/ml
� LH = 2 mIU/ml
� Cortisol = 34 ug/dl
5/24/2017
16
Patient Cases� SP is a 49 YOF 6 years post hysterectomy. She has been on
0.05mg/24h Vivelle patch since the surgery. She’s
complaining of vaginal irritation and dryness leading to
uncomfortable intercourse and difficulty reaching climax.
She also notes that the mood never strikes like it used to.
� What labs would we look at?
� Options for dryness?
� Options for libido?
Options for SP� Dryness & Atrophy
� Estradiol 0.01%
Estriol 1% Vaginal Cream
� Apply a pea sized amount once daily for a week, then reduce to two days per week as needed for irritation.
� Libido
� Testosterone 1% Cream
� Apply 0.25ml to area of thin skin once each morning
� “Cuddle Cream”
� Testosterone 5% Ointment
� Apply a small amount to the clitoral area upon initiation of sexual activity
5/24/2017
17
Where to Get More Information� Pam W. Smith, MD
� Jonathan V. Wright, MD
Where to Get More Information
Conclusion� Hormones are highly interdependent and converted by
the aromatase enzyme family
� Pituitary hormones signal recruitment of hormones from
various body tissues when primary source is depleted,
leading to a variety of symptoms
� Bio-identical hormones are one of the many options for
treating menopause
� Laboratory results when combined with subjective
information, can help tailor medications to a safe and
efficacious dose
5/24/2017
18
Questions?







