

ANXIETY DISORDERS IN PRIMARY CARESHANNON HILLIER, DO, MPH
CLINICAL ASSISTANT PROFESSOR
DEPARTMENT OF PSYCHIATRY & BEHAVIORAL SCIENCES
OKLAHOMA STATE UNIVERSITY
OBJECTIVES
1. Understand the prevalence of anxiety disorders in the primary care setting
2. Understand diagnostic strategies for anxiety disorders in the primary care setting
3. Understand treatment strategies for common anxiety disorders

ANXIETY IN PRIMARY CARE
• Anxiety disorders frequently first present in primary care settings, often seeking help for seemingly unrelated general medical problems.
• Associated with impaired quality of life and compromised psychosocial functioning, and the disability they cause is comparable to that of chronic physical illnesses such as diabetes and hypertension.
• Greene, T., et al. (2016). "Prevalence, Detection and Correlates of PTSD in the Primary Care Setting: A Systematic Review." J Clin Psychol Med Settings 23(2): 160-180.
• Olariu, E., et al. (2015). "DETECTION OF ANXIETY DISORDERS IN PRIMARY CARE: A META-ANALYSIS OF ASSISTED AND UNASSISTED DIAGNOSES." Depress Anxiety 32(7): 471-484.

WHAT IS ANXIETY?
• Temporary sensation
• Medical sign/ symptom
• Medical comorbidity
• Psychiatric disorder
• Barrier to medical treatment compliance
• Increases number of physician visits and disability days
• Risk for Suicide
ANXIETY IS NOT?
• Not to be ignored
• Not to be managed with benzodiazepines

DIAGNOSTIC STRATEGY LADDER
• Clarify feeling
• Rule out medical causes
• Establish DSM5 criteria
• Treat accordingly
Clarify Rule Out Diagnose Treat

CLARIFY FEELING
• What does it feel like for the patient?
• Triggering event?
• Happened before?
• Severity?
• What makes it better?
• How long does it last?

RULE OUT MEDICAL CAUSES
• Medication Induced
• Hyperthyroidism
• Pulmonary Embolism
• Pheochromocytoma
• Drugs
• Pain

MEDICATION INDUCED
• Steroid
• Stimulants
• Psychotropics
• Asthma (ie. Albuterol)
• Sympathomimetics (ie. pseudoephedrine)
• Hormones (ie. BCP, thyroid)

HYPERTHYROIDISM
Bunevicius, R. et al. Mood and anxiety disorders in women with treated hyperthyroidism and opthalmopathy caused by Graves' disease. General Hospital Psychiatry. 2005 March-April.
Anxiety Disorder Euthyroidisim Hyperthyroidism All(n=30)
Controls(n=45)
Panic Disorder 12% 21% 17% 16%
Social Anxiety Disorder
25% 43% 33% 13%
Post traumatic Stress Disorder
0 7% 3% 2%
General Anxiety Disorder
56% 79% 67% 31%
Total anxiety disorder 69% 79% 73% 40%

PULMONARY EMBOLISM
Chun-ping, Liu et al. Depression, anxiety and influencing factors in patients with acute pulmonary embolism. Chinese Medical Journal 2011; 124(16): 2438-2442

COMORBIDITIES OF ANXIETY DISORDERS
Number of Disorders
1 65%
2 22%
3 7%
4 4%
Kroenke, K. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Annals of Internal Medicine. 2007;146(5):317-25

ILLICIT SUBSTANCES
• Methamphetamine
• Cocaine
• Crack
• Speed
• Bath salts

RULE OUT OTHER PSYCHIATRIC DISORDERS
• Depression
• Mania
• Psychosis

ALCOHOL WITHDRAWAL
CIWA scale

ESTABLISH DSM5 CRITERIA
• Symptoms
• Time
• Exclusions

DSM5 ANXIETY DISORDERS
• Generalized Anxiety Disorder
• Separation Anxiety Disorder
• Selective Mutism
• Specific Phobia
• Social Anxiety Disorder
• Panic Disorder
• Agoraphobia
• Other and Unspecified Anxiety Disorders

PRIMARY CARE ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

PREVALENCE OF DISORDERS IN PRIMARY CARE
Disorder Prevalence
Posttraumatic Stress Disorder 8.6%
Generalized Anxiety Disorder 7.6%
Panic Disorder 6.8%
Social Anxiety Disorder 6.2%
Kroenke, K. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Annals of Internal Medicine. 2007;146(5):317-25
DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

POST TRAUMATIC STRESS DISORDERSymptoms Timing Exclusions
A. Exposed to death, threatened death, actual/ threatened injury or sexual violence.
B. Intrusive symptoms (1/5)C. Persistent avoidance (1/2)D. Negative alterations in cognition
and mood associated (2/7)E. Alteration in arousal and
reactivity associated (2/6)
Persistence in symptoms for more than one month
Not due to medication, substance or illness
Acute Stress Disorder >2 days, < 1 mo
Adjustment Disorder w/in 3 mo, < 6 mo
Other Specified Trauma/Stressor Related Disorder

PTSD
• Research suggests that posttraumatic stress disorder (PTSD) is common, debilitating and frequently associated with comorbid health conditions, including poor functioning, and increased health care utilization.
• People with PTSD may be twice as likely to have a non-psychiatric health condition compared to those without PTSD, even when controlling for age, socioeconomic status and major depression.
• Greene, T., et al. (2016). "Prevalence, Detection and Correlates of PTSD in the Primary Care Setting: A Systematic Review." J Clin Psychol Med Settings 23(2): 160-180.

POST TRAUMATIC CHECK-LIST
• PTSD Checklist-Civilian - The PCL is a 17-item measure designed to assess PTSD symptom severity.
• The PCL has been shown to have excellent internal consistency, convergent validity with alternative measures of PTSD, and test-retest reliability.
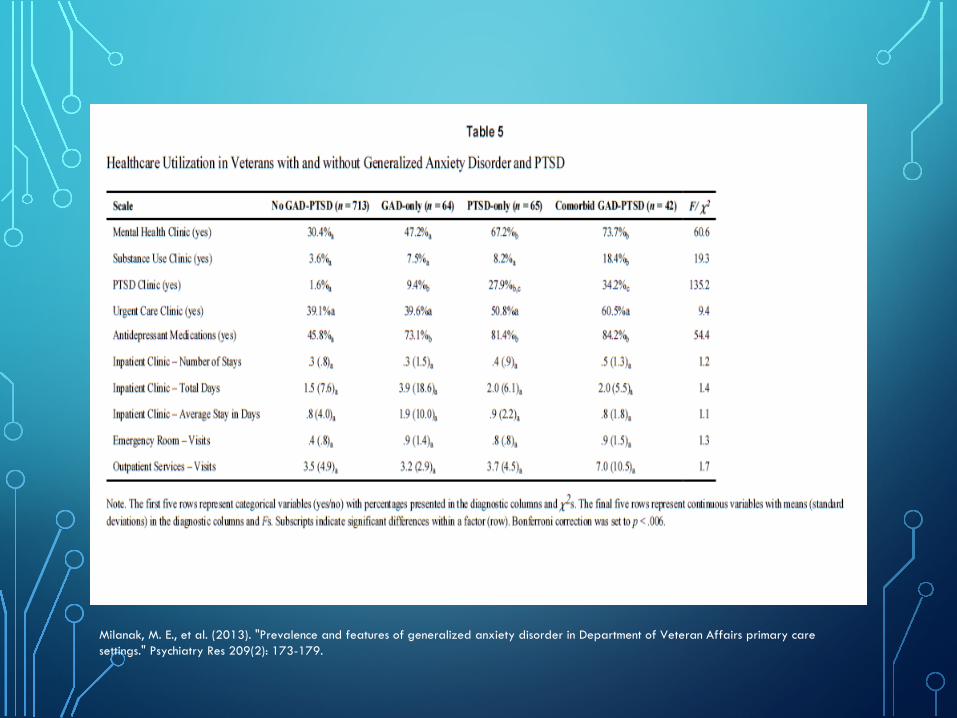
Milanak, M. E., et al. (2013). "Prevalence and features of generalized anxiety disorder in Department of Veteran Affairs primary care settings." Psychiatry Res 209(2): 173-179.

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

GENERALIZED ANXIETY DISORDER
Symptoms Timing Exclusions
• Excessive anxiety and worry with 3 or more of:
• Restlessness or feeling keyed up or on edge
• Easily fatigued• Difficulty Concentrating
or mind going blank• Irritability• Muscle tension• Sleep disturbance• Impairs functioning
6 months • Not attributable to physiological effects of a substance or medical condition
• Not better explained by another mental condition

GAD-7
Plummer, F., et al. (2016). "Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic meta-analysis." Gen Hosp Psychiatry 39: 24-31.

GAD-7 SCORING
Plummer, F., et al. (2016). "Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis." Gen Hosp Psychiatry 39: 24-31.

GAD-2
Plummer, F., et al. (2016). "Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic meta-analysis." Gen Hosp Psychiatry 39: 24-31.

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

PANIC DISORDER
Symptoms Timing Exclusions
Recurrent unexpected panic attacks which peaks within minutes and has 4 or more symptoms of a panic attack
1 month of the following:
Persistent concern or worry about having attacks
Maladaptive change in behavior related to the attacks
• Not attributable to physiological effects of a substance or medical condition
• Not better explained by another mental condition

PANIC ATTACK
• Palpitations, pounding heart, or accelerated heart rate
• Sweating
• Trembling or shaking
• Sensations of shortness of breath or smothering
• Feelings of choking
• Chest pain or discomfort
• Nausea or abdominal distress
• Feeling dizzy, unsteady, light-headed, or faint
• Chills or heat sensations
• Paresthesias
• Derealization or depersonalization
• Fear of losing control
• Fear of dying

PANIC DISORDER
• A panic attack is the end result of any of the anxiety disorders
• Panic disorder is when the attack occurs “Out of the Blue”

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

SOCIAL ANXIETY DISORDERSymptoms Timing Exclusions
• Marked fear or anxiety about social situations in which they may be exposed to possible scrutiny
• Fears that they will act in a way that will be negatively evaluated
• The social situations almost always provoke anxiety
• The situations are avoided or endured with great anxiety
• The anxiety is out of proportion to the situation
6 months • Not attributable to physiological effects of a substance or medical condition
• Not better explained by another mental condition

SOCIAL ANXIETY DISORDER
• Can have a performance only subtype:
• The fear is restricted to speaking or performing in public

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

SPECIFIC PHOBIASymptoms Timing Exclusions
1. Marked fear or anxiety about a specific object or situation
2. The phobic object or situation almost always provokes immediate fear or anxiety
3. The phobic object or situation is actively avoided or endured with intense anxiety
4. The fear is out of proportion to the actual danger
5. Causes impairment
6 months Not better explained by another mental condition

SPECIFIC PHOBIA-SPECIFIERS
• Animal
• Natural environment
• Blood-injection Injury
• Situational
• Other

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

AGORAPHOBIASymptoms Timing Exclusions
• Marked fear or anxiety about two or more of:
1. Using Public transportation2. Being in open spaces3. Being in enclosed places4. Standing in line or being in a
crowd5. Being outside of the home alone
• The individual fears or avoids these situations
• The situations almost always provoke fear or anxiety
• The agoraphobic situations are actively avoided, require the presences of a companion or endured with great anxiety
• The fear is out of proportion• Causes impairment
6 months • Not attributable to physiological effects of a substance or medical condition
• If it is caused by a medical condition, it is clearly excessive
• Not better explained by another mental condition

DSM5 ANXIETY DISORDERS
• Post Traumatic Stress Disorder
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Specific Phobia
• Agoraphobia
• Obsessive Compulsive Disorder

OBSESSIVE COMPULSIVE DISORDER
Symptoms Timing Exclusions
• Presence of Obsessions, Compulsions or both
• The Obsessions or compulsions are time consuming or cause impairment
NO TIME LISTED IN DSM5
• Not attributable to physiological effects of a substance or medical condition
• Not better explained by another mental condition

OBSESSIONS
1. Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress
2. The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize with some other thought or action
*Must have both

FREQUENCY OF OBSESSIONS(IN A SAMPLE OF 560 PTS WITH OCD)
Obsession Frequency
Contamination 50%
Pathological Doubt 42%
Somatic 33%
Need for Symmetry 32%
Aggressive 31%
Sexual 24%
Multiple Obsessions 72%
Adapted from Rasmussen SA, Eisen JL: “Clinical and Epidemiologic Findings of Significance to NeuropharmacologicTrials of OCD.” Psychopharmacology Bulletin 24:466–470, 1988.

COMPULSIONS
1. Repetitive behaviors or mental accts that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly
2. The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situations; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive
• *must have both

FREQUENCY OF COMPULSIONS(IN A SAMPLE OF 560 PTS WITH OCD)
Compulsion Frequency
Checking 61%
Washing 50%
Counting 36%
Need to ask or confess 34%
Symmetry and Precision 28%
Hoarding 18%
Multiple Compulsions 58%
Adapted from Rasmussen SA, Eisen JL: “Clinical and Epidemiologic Findings of Significance to NeuropharmacologicTrials of OCD.” Psychopharmacology Bulletin 24:466–470, 1988.
OCD VS. OCPD
• OCD causes distress to the patient
• OCPD causes distress to everyone else

TREATMENT LADDER
• Establish diagnosis
• Choose appropriate long term treatment
• Choose short term relief
• Reassess and de-escalate

LONG TERM TREATMENTS
• Selective Serotonin Reuptake Inhibitors (SSRI)
• Selective Serotonin/Norepinephrine Inhibitors (SNRI)
• Cognitive Behavior Therapy

SSRI
• Essentially, are equally effective for the anxiety disorders
• An individual SSRI is likely to be more effective if it was effective in a family member

SNRI
• Norepinephrine can be activating and possibly exacerbate the symptoms

USING SSRI/SNRI
• Start at lowest recommended dose
• Reassess in 4-6 weeks and increase if necessary
*To diagnose an anxiety disorder and write months worth of prescriptions is ineffective, wasteful and below standard of care

USING SSRI/SNRI
• Slow taper and discontinue 6-12 months AFTER the remission of symptoms
• Some patients require long term treatment

SHORT TERM TREATMENT
• Benzodiazepines
• Propranolol
• Hydroxyzine

BENZODIAZEPINES
• Alprazolam is not recommended for chronic use
• Best for situations in which an individual knows that will face anxiety
• Flight, court, funeral
* To use alprazolam on a daily basis is irresponsible, dangerous and below the standard of care
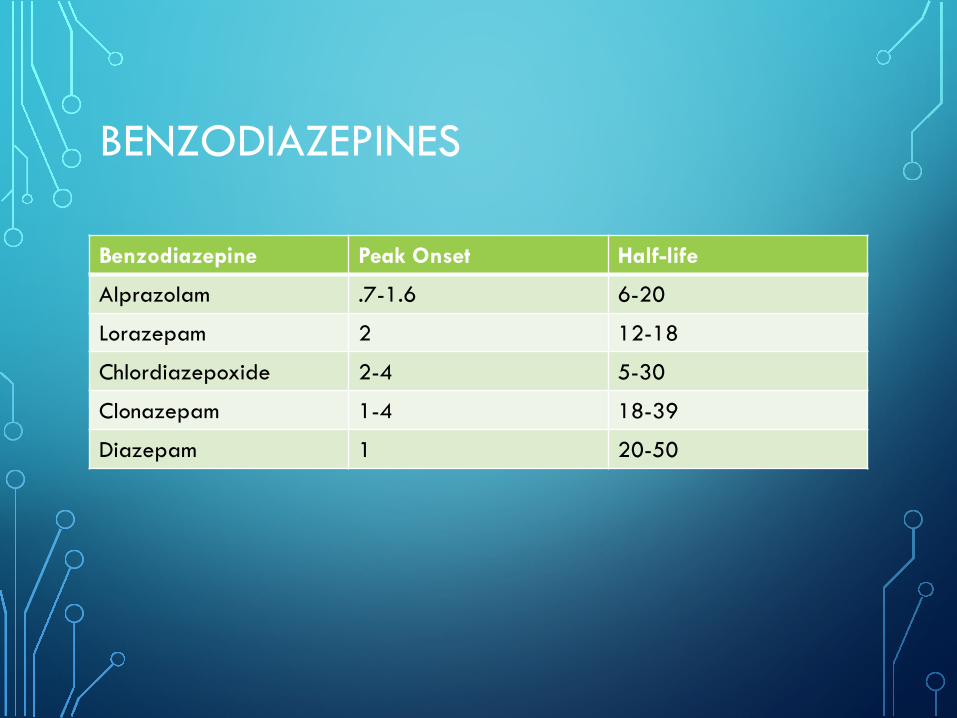
BENZODIAZEPINES
Benzodiazepine Peak Onset Half-life
Alprazolam .7-1.6 6-20
Lorazepam 2 12-18
Chlordiazepoxide 2-4 5-30
Clonazepam 1-4 18-39
Diazepam 1 20-50
PSYCHOTHERAPY
• Cognitive Behavioral Therapy is effective, rapid acting and portable
• Engages patient into getting better
• Short term (12 weeks) and protocol driven

EXPERT CONSULTATION
• Anxiety disorders can be effectively treated in the primary care setting
• While a referral is not necessary, sometimes consultation and advice can
• OSU PSYCHIATRY ECHO

PROJECT ECHO: “CHANGING THE WORLD FAST”

HOW IT WORKS• Primary care physicians (PCPs) and other clinicians can learn to provide
excellent psychiatric care directly to patients in their own practices.
• In the Project ECHO model, clinicians attend teleECHO™ clinic sessions, where they connect with a subspecialty team of experts
• This approach saves time, adds convenience and improves treatment adherence for patients. It also increases the knowledge, mastery and joy of medical practice for clinicians.

BENEFITS TO PRIMARY CARE PROVIDERS
• Gain up-to-date specialty knowledge
• Learn from evidence-based case studies
• Engage in a vibrant learning community where knowledge is shared
• Receive free CME credit for participation

WHAT DOES A PSYCHIATRIC TELE-ECHO CLINIC LOOK LIKE?
Noon –12:10 p.m. Introductions
12:10 –12:30 p.m. Didactic Presentations
12:30 –2 p.m. Case Presentations
EVERY THURSDAY

HOW DO I GET STARTED?
1. Sign interest sheet with contact information
2. Contact Courtney Busse-Jones1. [email protected]
3. Develop Case Presentation & send to ECHO Coordinator
4. Register for teleECHO Clinic via Zoom – receive your ID #
5. Attend weekly teleECHO Clinics
6. Complete Pre/Post Test for each teleECHO Clinic to receive 1A CME
7. Complete Attestation Form & Outcome Measures for extra 1A Credit









