

Are the new molecular markers useful for the management of MPNs?

Signaling abnormalities and Myeloproliferative Neoplasms
kinasepseudokinaseSH2FERM
kinasepseudokinaseSH2FERM
V617F
K539L
JAK2
WT MPL WT MPL+ TPO
TPO
Motif RWQFP
MPL W515A/L/K
W515L/K/A
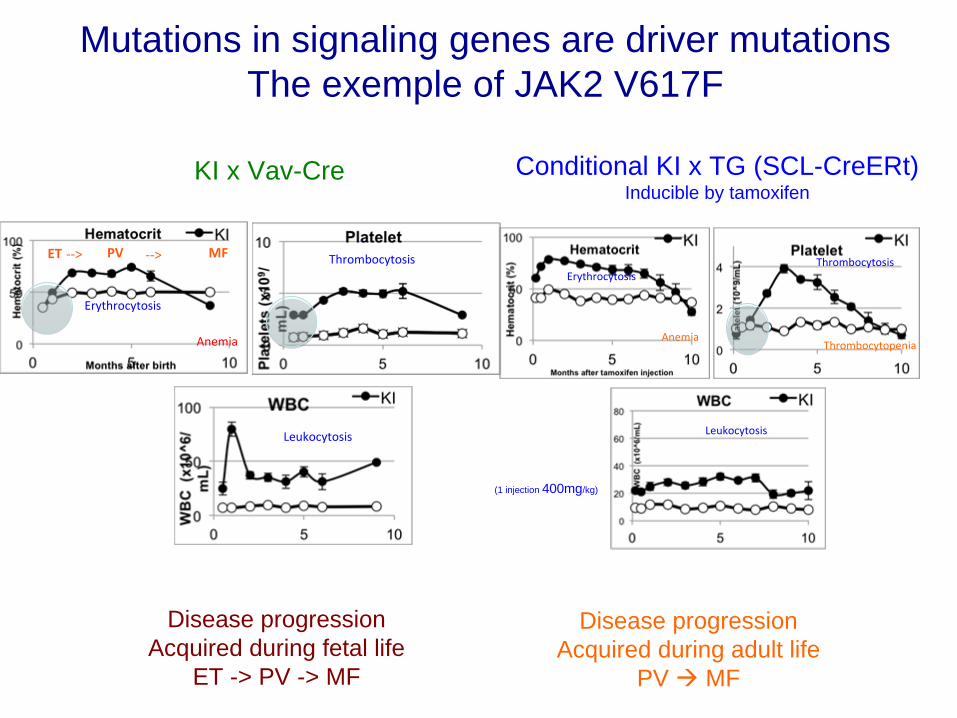
KI x Vav-Cre
ET PV‐‐> ‐‐> MF
Anemia
Erythrocytosis
Thrombocytosis
Leukocytosis
Disease progressionAcquired during fetal life
ET -> PV -> MF
(1 injection 400mg/kg)
Disease progressionAcquired during adult life
PV MF
Erythrocytosis
Anemia
Thrombocytosis
Thrombocytopenia
Leukocytosis
Conditional KI x TG (SCL-CreERt) Inducible by tamoxifen
Mutations in signaling genes are driver mutationsThe exemple of JAK2 V617F
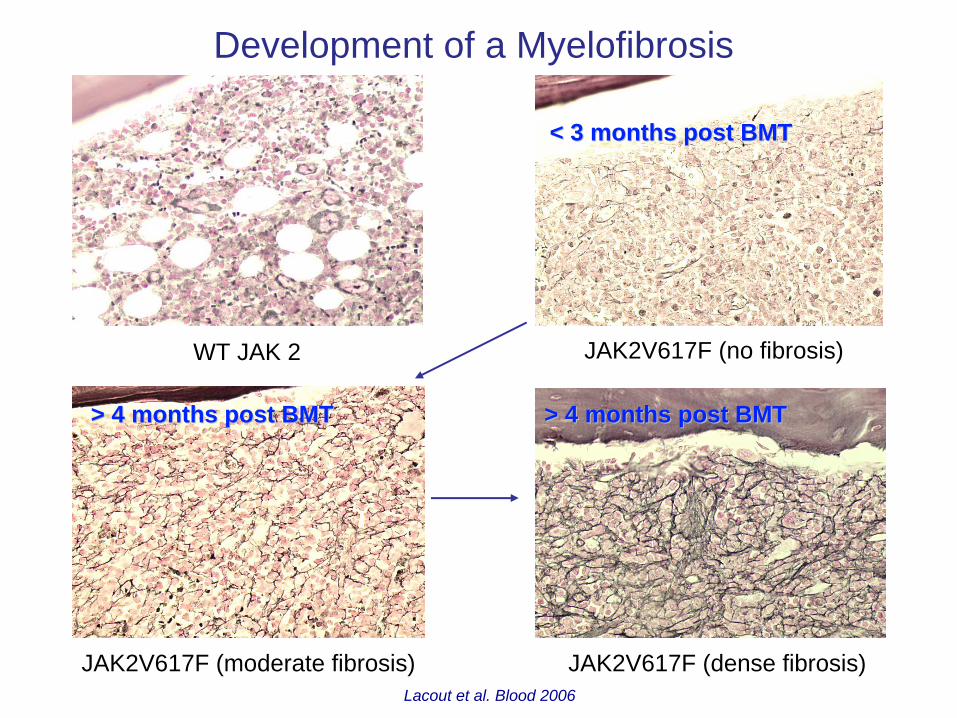
Development of a Myelofibrosis
JAK2V617F (no fibrosis)
JAK2V617F (moderate fibrosis) JAK2V617F (dense fibrosis)
WT JAK 2
< 3 months post BMT< 3 months post BMT
> 4 months post BMT> 4 months post BMT > 4 months post BMT> 4 months post BMT
Lacout et al. Blood 2006
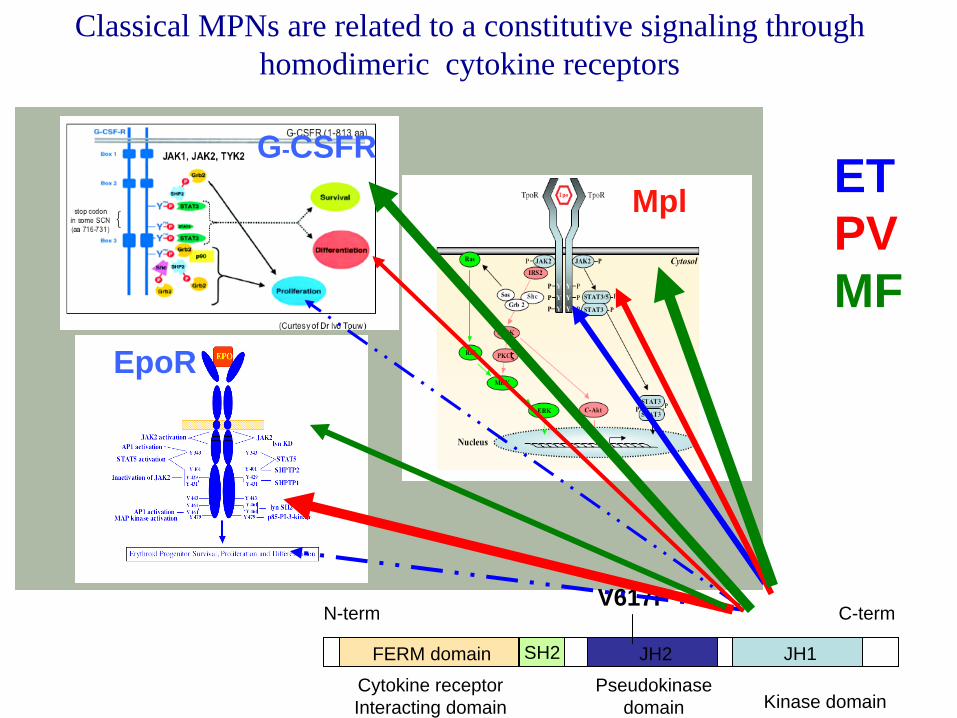
JH1JH2
Kinase domainPseudokinase
domain Cytokine receptorInteracting domain
V617FC-termN-term
FERM domain SH2
ETPVMF
Mpl
EpoR
G-CSFR
Classical MPNs are related to a constitutive signaling through homodimeric cytokine receptors

WHO classification of MPNs
Essential Thrombocythemia
(ET)
CML Classical MPNs Rare and unclassified MPNs
Polycythemia vera (PV)
Myelofibrosis(PMF)
Bcr-abl PDGFRaFGFR1Kit
Classification of MPN

Spectrum of chronic myeloid hemopathies
Myeloproliferation
Myelodysplasia
CMML RACML PMFETPV
BCR-ABLJAK2V617FMPLW515L
SF3B1TET2ASXL1SRSF2

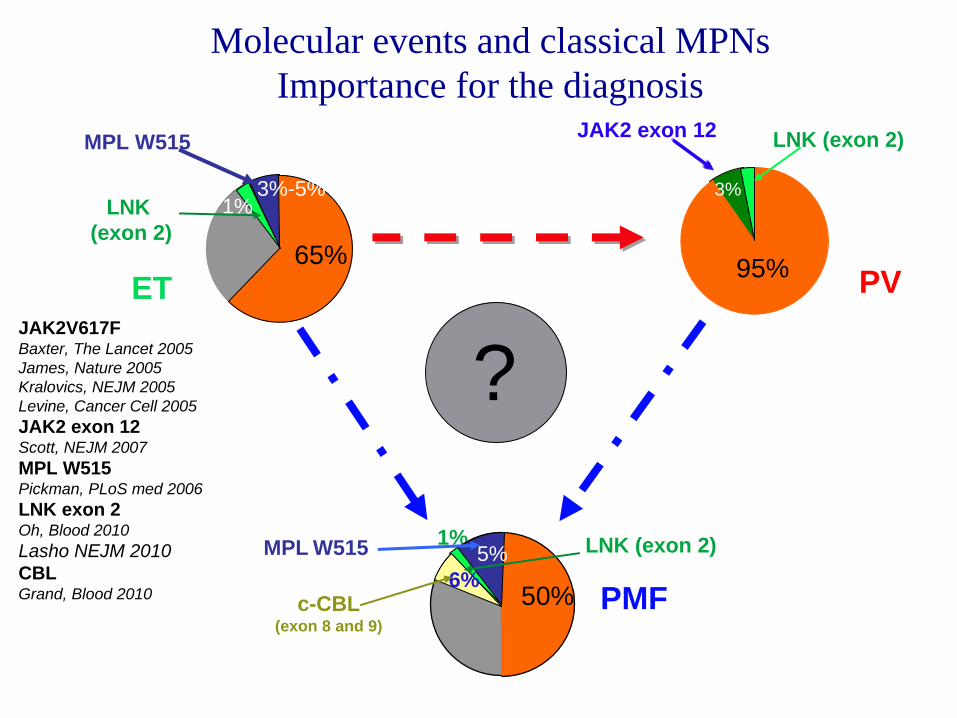
Molecular events and classical MPNs Importance for the diagnosis
JAK2V617FBaxter, The Lancet 2005 James, Nature 2005Kralovics, NEJM 2005Levine, Cancer Cell 2005JAK2 exon 12Scott, NEJM 2007MPL W515Pickman, PLoS med 2006LNK exon 2Oh, Blood 2010Lasho NEJM 2010CBLGrand, Blood 2010
?PV
JAK2 exon 12 LNK (exon 2)
95%95%
3%LNK
(exon 2)
ET
MPL W515
30% 65%
3%-5%1%
PMFc-CBL(exon 8 and 9)
MPL W515 LNK (exon 2)1%
45%50%5%
6%

Diagnostic algorithm for MPN diagnosis
Tefferi A , Vainchenker W JCO 2011;29:573-582
Molecular events and classical MPNs Importance for the diagnosis
JAK2V617FBaxter, The Lancet 2005 James, Nature 2005Kralovics, NEJM 2005Levine, Cancer Cell 2005JAK2 exon 12Scott, NEJM 2007MPL W515Pickman, PLoS med 2006LNK exon 2Oh, Blood 2010Lasho NEJM 2010CBLGrand, Blood 2010
?PV
JAK2 exon 12 LNK (exon 2)
95%95%
3%LNK
(exon 2)
ET
MPL W515
30% 65%
3%-5%1%
PMFc-CBL(exon 8 and 9)
MPL W515 LNK (exon 2)1%
45%50%5%
6%
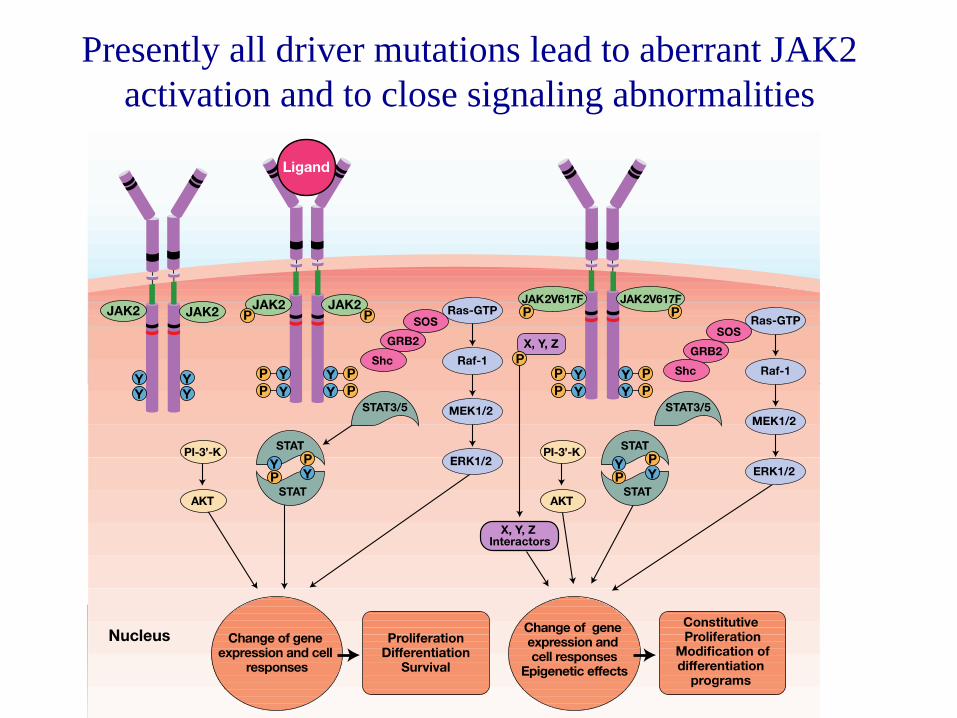
Presently all driver mutations lead to aberrant JAK2 activation and to close signaling abnormalities

Most new therapies target JAK2 ATP binding pocket and have no specificity for JAK2 mutants
ser523 Tyr 570
Reddy et al. Expert Opin. Ther Targets 2012
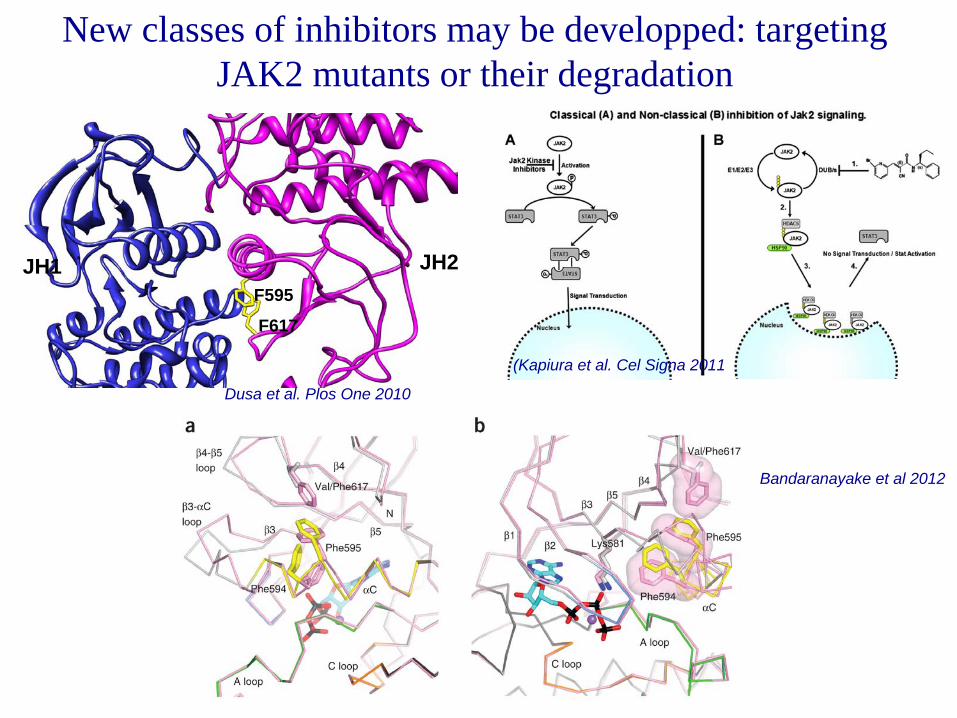
New classes of inhibitors may be developped: targeting JAK2 mutants or their degradation
JH1 JH2F595
F617
Dusa et al. Plos One 2010
(Kapiura et al. Cel Signa 2011
Bandaranayake et al 2012

Other mutations are important for disease diversity (thus for the prognosis)

Three mutations have a clear impact on survival and leukemic transformation
Guglielmelli P et al. Blood 2011
Tefferi et al et al. Leukemia 2012
IDH1/IDH2
EZH2

Mutations and PrognosisSRSF2 (Zhang et al Blood 2012, Lasho and Tefferi 2012)
Zhang et al. Blood 2012
The role of ASXL1 mutations in prognosis are more controversial and TET2 mutations do not seem to have a prognosis impact
PVPMF
Tefferi A et al. Leukemia 2009
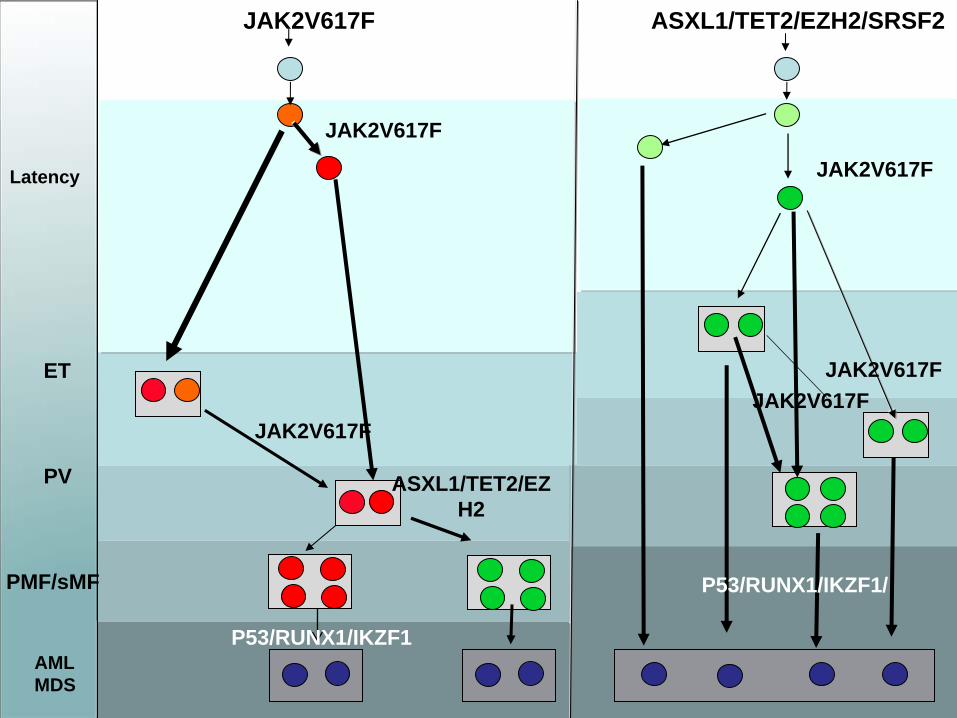
JAK2V617F
AMLMDS
ASXL1/TET2/EZH2/SRSF2
ET
PV
PMF/sMF
Latency JAK2V617F
ASXL1/TET2/EZ H2
P53/RUNX1/IKZF1
P53/RUNX1/IKZF1/
JAK2V617F
JAK2V617F
JAK2V617FJAK2V617F

Guglielmelli P et al. Blood 2009;114:1477-1483
©2009 by American Society of Hematology
JAK2V617F and Prognosis Inverse correlation between JAK2V617F and prognosis in PMF
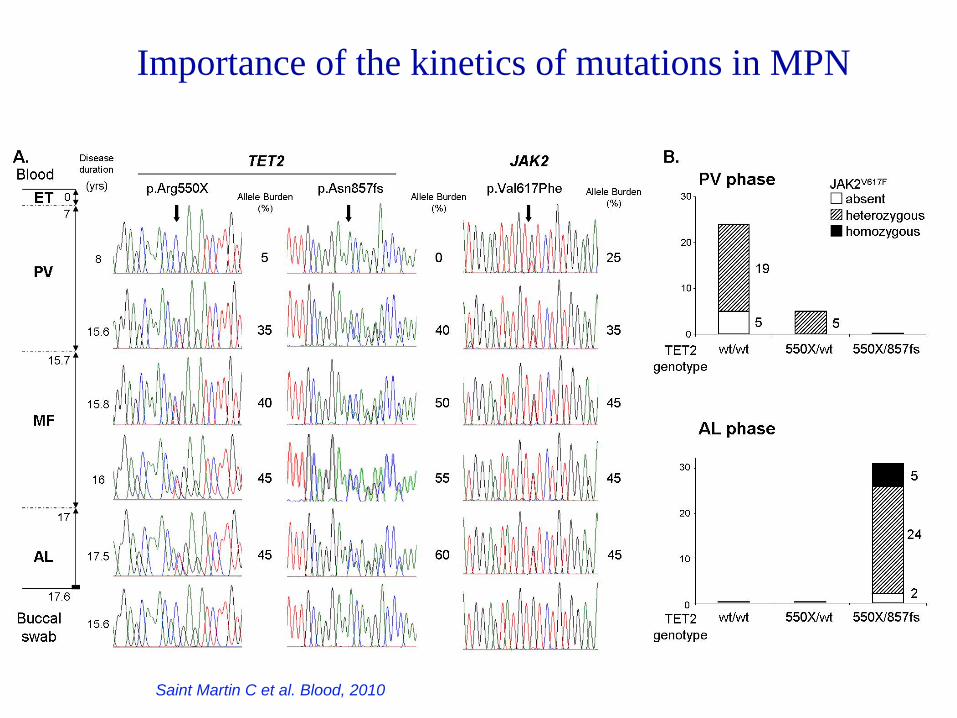
Importance of the kinetics of mutations in MPN
Saint Martin C et al. Blood, 2010

Peg‐Interferon
(IFN) molecular response <1%
JAK2V617F 7/29 patients
0 5 10 15 20
020
4060
801 0
Months
% V
617F
0 6 12 18
020
4060
801 0
Months
% V
617F P<.001
%V6
17F
%V6
17F
Kiladjian JJ et al, Blood, 2006
Patients with <1% JAK2 VFin peripheral granulocytes
One patient with a frameshift in exon 11 of TET2
25% of mutant TET2 at diagnosis
del C4575, 1525fs
114 63 141 174 82
0 1 2 10 7
0%10%20%30%40%50%60%70%80%90%
100%
1 2 3 4 5
% o
f c
olo
nie
s
JAK2 WTJAK2 V617F
82
61
JAK2 WT/VF
JAK2 VF/VF
JAK2 wt
Implications for therapy The exemple of Peg-Interferon
Kiladjian JJ, Delhommeau F Leukemia 2010

c.4577delC, p.Gln1526Serfsc.1849G>T, p.Val617Phe
Peg-Interferon
inhibits the TET2m-JAK2V617F subclone, but not the initial TET2m-JAK2WT clone
22
TET2 exon 11JAK2 Allelic
discrimination
Prior IFNa treatment
24 months
36 months
20%
<1%
<1%
JAK2V617F
JAK
2wild
-type
JAK2 exon 14
Wild type JAK2Wild type TET2
Kiladjian JJ, Delhommeau F Leukemia 2010

Conclusion• Mutations in signaling molecules are important for diagnosis • Mutations in signaling molecules are not important for the
present therapies as there is no true targeted therapy of the mutant molecules
• Mutations in the epigenetic regulators or splicing machinery or others are important for understanding the disease heterogeneity and thus for the prognosis
• Following mutation burden and acquisition of new mutations is important for:– Prognosis– Understanding the efficacy of therapy on the clonal disorder

INSERM U985Villejuif, France
Olivier Bernard
Thomas Mercher
Véronique Della Valle
Cyril Quivoron
Lucie Couronné
INSERM U1009Villejuif, France
Eric SolaryFrançois Delhommeau
Sabrina DupontChloe James
Nicole CasadevallValérie Ugo
Stéphane GiraudierRodolphe BesancenotJean Pierre LeCouédic
Isabelle PloElodie Pronier
Jean Luc VillevalCatherine LacoutCaroline Marty
De Duve InstituteLudwig Institute
Brussels, Belgium
Stefan ConstantinescuChristian PecquetMichael GirardotAlexandra Dusa
Jean-Philippe Defour
Acknowledgments







