

Hackerbiotic’sOpen Source E-book Series
HackerBiotic’s
Clinical Orders1st Edition
Code name : McBurneyCopyright © 2018 hackerbiotic
All written content licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Standard Format For Writing Admission
Orders
Admit:
Attending/Service/Unit/Resident/Inpatient/LOS in days
List Admitting Intern and Pager number
List Admitting Resident and pager number
List Admitting Attending
Diagnosis:
List the main diagnosis and any other that are pertinent to the care of the patient
Condition:
This indicates to the nursing staff and PR folks how sick the patient is
Serious, Guarded, Critical, Stable, good, fair etc.
DO NOT PUT CONDITION AS STABLE! Use "Fair". If they are stable, send them home
Vitals:
This is how frequently YOU want vital signs checked. This can be every 15 minutes, hourly,
every 4 hours, every 12 hours, daily or whatever you choose. If you put “per routine” you
better know what that Means.
q4h, q shift, routine, per ICU protocol.
Activity:
This refers to limitations on activity
Bed rest, bed rest with bathroom privileges, ad lib , amb TID, up to chair, No restrictions
Diet:
What you want the patient to eat
Regular, NPO, Diabetic 1800 Cal ADA, Cardiac prudent, Renal (60g prot, 40 meq K, 2 gm Na),
clears advance to soft, Advance as tolerated, no added salt ,ADA (diabetic), low sodium, clear
liquid, Heart Healthy Diet
ADC VAD NISMAL
ADC VAN DISMAL represents
an organized way to guide
your orders. The included
orders are just illustrative
examples
ADC VAN DISMAL
Admit
Diagnosis
Condition
Vitals
Activity
Diet
Nursing
IVF
Specials
Meds
Allergies
Labs
Ad lib :
at pleasure" and "at one's
pleasure, as much as one
desires, to the full extent of
one's wishes
Amb :
ambulate, walk

Nursing:
What you want the nurses to routinely do Accurate input and output values, daily weight,
calorie counts, CR (cardiorespiratory) monitor, pulse oximetry, Notify MD BP, HR, ICP, Temp
(list parameters) etc.
• Strict I/O’s, daily weights, Foley to gravity, O2 requirement; 1:1 Observation, Neuro
check q4h
• Wound care: Dressing changes, DVT stockings, etc;
• Respiratory care: updrafts, endotracheal suctioning, spirometry, incentive spirometer,
etc.
• Precautions: Aspiration precautions, fall precaution, seizure precautions
• Protocols: Hypoglycemia protocol, bedsore prevention, incentive spirometer.
IVF:
You should indicate the fluid and the rate that it is to run i.e.
2 lit NS + 20 mEq/L of KCl tra (to run at) 14 cc/hr
Specials :
Specialists or Consults
Meds:
These are the medications the patient will be receiving Include the name, dose, route and
frequency .Oxygen is a medication! Just because it comes out of the wall does not mean it is
routinely used. If you want the patient on oxygen list it here, how you want it delivered
(mask, nasal cannula etc.).
At your stage of training you should not get into the habit of writing prn (as needed) orders.
If a patient needs a medication YOU should evaluate that patient and determine for yourself
if the order is needed. Later on when you have developed clinical acumen, you may be able to
anticipate that certain medications will be needed based upon the natural history of the
disease.
• Norco 7.5 mg PO Q6H PRN Pain
• Clonidine 0.2 mg PO Q6H PRN SBP>180
• Metoprolol INJ 10 mg q6h PRN SBP >180
• Hydralazine INJ 10 mg IV q6h PRN SBP>180
• Acetaminophen 500 mg PO q4h PRN temp >101.4
• Diphenhydramine 25 mg IV q4h PRN itching or insomnia

Allergies:
specific medications, NKDA, etc
Labs:
These are the labs that need to be drawn now and those that need to be obtained routinely.
You should only order labs whose abnormal or normal results will change your treatment
plan. Ordering a lab just because you want to see the result is poor form AND you may get an
abnormal result and now YOU must explain why the result is abnormal. You can also order
other ancillary studies under this heading such as x-rays, ECG, EEG, etc. Whenever you order
one of these studies you need to write down in the order sheet the indication for the study.
Do not put “because I want it”.
studies, radiology or imaging: CBC, Chemistries, X-rays, MRI/CT, ECG, Pulse ox, Ca, Mg,
Phos, etc
NKDA:
Not Known Drug Allergy

STEMIAdmit : CCU Admission , Dr () services,
Dx : STEMI
cond : fair
Vitals : q1h
Act : CBR
Diet : NPO till stable then Heart Healthy Diet
Please :
1. ECG at arrival & 1h later
2. Cardiac Monitoring
3. IVF maintenance
4. Cardiologist Consult
5. IV Nitro 5 mg in 100 cc DW 5%, 10drop/min (10 Mcg/min) (if SBP>90 mmHg)
6. ASA Tab 325 mg PO stat & 80 mg po qd
7. Plavix or Osvix Tab 300 mg PO stat ( if age<70 yo) & 75 mg PO QD
8. Atorvastatin Tab 80 mg PO qhs
9. Morphine Inj 3 mg IV stat ( if HR>60, SBP>100, no Heart Block)
Or
Pethidine Inj 25 mg IV stat
10.Clemastine inj 1 Amp IV stat before SK
11.Streptokinase 1500000 unit in 100cc N/S during 30 min
12.Captopril Tab 12.5mg PO TID ( if SBP >100 mmHg & no Hx of Angioedema)
Or
Metoral Tab 25 mg PO BID (if SBP > 100 mmHg & PR > 60/min & no Wheeze)
Or
Inderal Tab 20 mg PO TID (if SBP > 100 mmHg & PR > 60/min & no Wheeze)
Or
Diltiazem Tab 30 mg PO TID (If BB contraindic. & if SBP > 100 mmHg & PR > 60/min)
13.Pantoprazole Tab 40 mg PO QD
14.MOM Syrup 30cc PO TID
15.Oxazepam Tab 10mg PO QHS (age<55 yo)
Or
Haloperidol Tab 0.5mg PO QHS (age>55 yo)
16.O2 Nasally 3lit/min if O2 sat<90%
17.Allergy to specific drug
18.CBC, BUN, Cr, Na, K, FBS
19.PT, INR, PTT, TG, Chol, LDL, HDL
20.CPK, LDH, Troponin

USA/NSTEMI
Admit : CCU Admission , Dr () services,
Dx : USA, NSTEMI
cond : fair
Vitals : q1h
Act : CBR
Diet : NPO till stable then Heart Healthy Diet
Please :
1. ECG at arrival & 1h later
2. Cardiac Monitoring
3. IVF maintenance
4. Cardiologist Consult
5. IV Nitro 5 mg in 100 cc DW 5%, 10drop/min (10 Mcg/min) (if SBP>90 mmHg)
6. ASA Tab 325 mg PO stat & 80 mg po qd
7. Heparin Inj 60 unit/kg IV stat & 12 unit/kg/h IV Infusion
Or
Enoxaparin Inj 60 mg SQ BID
8. Atorvastatin Tab 80 mg PO qhs
9. Morphine Inj 3 mg IV stat ( if HR>60, SBP>100, no Heart Block)
Or
Pethidine Inj 25 mg IV stat
10.Captopril Tab 12.5mg PO TID ( if SBP >100 mmHg & no Hx of Angioedema)
Or
Metoral Tab 25 mg PO BID (if SBP > 100 mmHg & PR > 60/min & no Wheeze)
Or
Inderal Tab 20 mg PO TID (if SBP > 100 mmHg & PR > 60/min & no Wheeze)
Or
Diltiazem Tab 30 mg PO TID (If BB contraindic. & if SBP > 100 mmHg & PR > 60/min)
11.Pantoprazole Tab 40 mg PO QD
12.MOM Syrup 30cc PO TID
13.Oxazepam Tab 10mg PO QHS (age<55 yo)
Or
Haloperidol Tab 0.5mg PO QHS (age>55 yo)
14.O2 Nasally 3lit/min if O2 sat<90%
15.Allergy to specific drug
16.CBC, BUN, Cr, Na, K, FBS
17.PT, INR, PTT, TG, Chol, LDL, HDL
18.CPK, LDH, Troponin
19.PTT qd

RVMI or inf MIAdmit : CCU Admission , Dr () services,
Dx : RVMI
cond : fair
Vitals : q1h
Act : CBR
Diet : NPO till stable then Heart Healthy Diet
Please :
1. ECG at arrival & 1h later
2. ECG c leads V6R & V2R
3. Cardiac Monitoring
4. IVF maintenance
5. If SBP < 90 mmHg only Hydration (N/S 1000cc free stat)
6. Cardiologist Consult
7. If SBP < 90 mmHg stat Dopamine 3-20 Mcg/kg/min
8. ASA Tab 325 mg PO stat & 80 mg po qd
9. Plavix or Osvix Tab 300 mg PO stat ( if age<70 yo) & 75 mg PO QD
10.Atorvastatin Tab 80 mg PO qhs
11.Clemastine inj 1 Amp IV stat before SK
12.Streptokinase 1500000 unit in 100cc N/S during 30 min
13.Pantoprazole Tab 40 mg PO QD
14.MOM Syrup 30cc PO TID
15.Oxazepam Tab 10mg PO QHS (age<55 yo)
Or
Haloperidol Tab 0.5mg PO QHS (age>55 yo)
16.O2 Nasally 3lit/min if O2 sat<90%
17.No IV Nitro, No Morphine, No Beta-Blocker
18.CBC, BUN, Cr, Na, K, FBS
19.PT, INR, PTT, TG, Chol, LDL, HDL
20.CPK, LDH, Troponin

Heart Failure/Pulmonary Edema
Admit : CCU Admission , Dr () services,
Dx : heart failure, pulmonary edema
cond : fair
Vitals : q1h
Act : CBR
Diet : NPO till stable then Heart Healthy Diet
Please :
1. ECG
2. Cardiac Monitoring
3. Put the pt in semi-sitting position
4. Internal folley if needed
5. Check I/O
6. IVF maintenance
7. Cardiologist Consult
If SBP > 100 mmHg :
8. IV Nitro 5 mg in 100 cc D5W, 10drop/min (10 Mcg/min)
[according to BP and pt situation increase dosage +10 mcg/min every 5 min]
9. Lasix Inj 80mg IV stat (Max: 100mg/6h & 240mg/24h) [if K > 3]
10.Morphine Inj 3 mg IV stat ( if HR>60, SBP>100, no Heart Block)
[according to BP and pt sutiotion repeat after 10 min]
11.Captopril Tab 12.5mg PO TID ( if SBP > 100 mmHg & no Hx of Angioedema)
If SBP < 100 mmHg :
12.Dopamine Inj 3-20 Mcg/kg/min
13.Lasix & IV Nitro & Morphine After SBP > 100 mmHg
14.Heparin Inj 60 unit/kg IV stat & 12 unit/kg/h IV Infusion [if ABNL Cr]
Or
Enoxaparin Inj 60 mg SQ BID [if NL Cr]
15.ASA Tab 80 mg po qd
16.Atorvastatin Tab 40 mg PO qhs
17.Pantoprazole Tab 40 mg PO qd
18.MOM Syrup 30cc PO TID
19.O2 Nasally 3-5 lit/min
20.No Beta-Blocker
21.CBC, BUN, Cr, Na, K, FBS
22.Check BUN, Cr, Na, K, FBS daily
23.PT, PTT, INR, TG, Chol, LDL, HDL
24.CPK, LDH, Troponin
25.LFT (SGOT, SGPT, ALP)
26.U/A
27.CXR after stable
28.ABG
29.D-Dimer , BNP

Depressed ST in ECG
D - Drooping valve (MV prolapse)
E - Enlargement of the left ventricle
P - Potassium low
R - Reciprocal ST Depression (eg. inf MI)
E - Encephalon (intracerebral Hemorrhage)
S - Subendocardial infarct
S - Subendocardial ischemia
E - Embolism (pulmonary)
D - Dilated cardiomyopathy
S - Shock
T - Toxicity (Digitalis/Quinidine)

Sinus Tachycardia
Consider PTE and Tamponade
Choice : Metoral 50 mg po stat
Wide QRS
If unstable : sock 200 j
If stable : amiodarone
1. Amiodarone 150 mg in 100 cc D5W in 30 min
2. Amiodarone 300 mg in 500 cc D5W in 6 hr
3. Amiodarone 450 mg in 500 cc D5W in 18 hr
Narrow QRS
If unstable : sock 200 j
If stable : amiodarone, adenosine, BB, CHB, Digoxin

AF
Choice :
Digoxin 0.5 mg (1 amp) IV stat slowly
Metoral 50 mg po stat
Next dose : 20 min later if not respond
2nd line :
Verapamil 5 mg (1 amp) IV slowly stat
3rd line :
Cardioversion
PSVT
Choice :
Adenosine 6 mg (1 amp) IV stat shoot + 20 cc n/s shoot
می تونیم از. و بعد دست مریض رو باال می گیریم n/sیک سه راهی وصل می کنیم اول آدنوزین می زنیم پشتش
تا آمپول ۳حداکثر . همون اول دو تا آمپول بزنیم
2nd : verapamil 5 mg IV stat
3rd : cardioversion 100-150 j

HTN Emergency
Admit :
Dx : HTN Emergency
Cond : fair to good
Vitals : q1h
Act : CBR
Diet : NPO till stable then Heart Healthy Diet
Please :
1. ECG
2. Cardiac Monitoring
3. IVF maintenance
4. Cardiologist Consult
5. Captopril 50 mg stat ch 30 min later
Or
IV nitro 5-10 mcg/min till SBP > 80% MAP (if ischemia)
Or
Lasix 80 mg Iv or IM stat (CHF)
Or
Labetalol 20 mg IV stat & 2 mg/min infusion (dissection)
Or
Nitroprusside 1-3 mcg/kg/min infusion (emergency)
6. Diazepam Amp 2.5 mg stat slowly [if there is indication]
.نیتروپروساید به نور حساس استدور سرم آلومینیوم بپیچین

HTN OPD
Pearl TNG + Captopril 25 mg stat
30 mins later check BP
If Bp is still elevated admit the pt and start Iv Nitro
Work up after Dx is made :
1. KUB Sono
2. Bun, Cr
3. Na, K
4. CXR
5. TSH, T4
6. Echo
Managing HTN
A : ACE + ARB
B : BB
C : CCB
D: Diuretic
Choice :
• ACEI : Captopril, Enalapril
• ARB : Losartan, Valsartan
: ساعت شروع کنید ۸کیپتوپریل هر low doseبا
• Capto 25 ½ q8h
Or
• Losartan 25 mg bid
:شروع می کنیم Diureticیک هفته بعد داروی دوم یک
• Tab Triamtren-H
Or
• Tab HCTZ 50 mg qd
ها باید صبح ها باشد نه شب Diureticمصرف
یا افزودن دوز داروهای قبل Beta Blockerیک هفته بعد اضافه کردن
• BB : tab metoral 50 mg , ½ tab BID
points :
CVA : Amlodipine
CHF : A+B
Diabetic : A
If there is tachycardia :
Beta blocker
If Renal problems :
ACE
If there is Edema:
HCTZ
Do not prescribe Thiazides for
young women
Do not prescribe Beta Blocker for
Elderly pts

DVT
Admit :
Dx : DVT
Cond :
Vitals : q1h
Act :
Diet :
Please :
1. ECG
2. Cardiac Monitoring
3. Leg elevation
4. IVF maintenance
5. Cardiologist Consult
6. Heparin 5000 unit IV stat then 1000 u/hr infusion
7. Warfarin 5 mg po stat
8. Amp Pethidine 25 mg IV PRN [if pain]
9. CBC, Bun, Cr, Na, K , Bs
10.PT, PTT, INR
11.Check PTT q6h
12.D-Dimer
13.Color Doppler Sono
Heparin in DVT : 80 unit/kg stat, 18 unit/kg/hr infusion

Warfarin Toxicity
Admit :
Dx : warfarin toxicity
Cond : fair to good
Vitals :
Act :
Diet :
Please :
1. ECG
2. Transfer 3 bag FFP
3. IVF maintenance
4. Cardiologist Consult
5. Amo Vit K #1 IV stat
6. CBC, Bun, Cr, Na,K, BS
7. Brain CT Scan
8. Pt, PTT, INR now & 6 hour later, then check qd
When you change warfarin dosage:
Check PT 3 days later
If OK
Check PT 1 wk Later
If OK
Check Pt 1 month later
زمانی هپارین قطع می شود که
روز گذشته باشد۵
INR > 1.8و
Tell the pt not to consume green
foods because there
Vit-K in them.

Vertigo

Vertigo
Admit :
Dx : choose according to above approach
cond : depends on condition
Vitals : depends on condition
Act : depend on condition
Diet : depends on condition
Please :
1. ECG
2. IVF 500cc N/S in 24h
3. Promethazine Inj ½ Amp (25 mg) IV stat
4. Ondansetron Inj 1 Amp IV PRN
5. Betahistine Tab 16 mg PO Q8h
6. Cinnarizine Tab 25 mg PO stat
7. Diazepam 5 mg slowly IV
8. lipid profile
9. CBC, BUN, Cr, Na, K, BS
• Tab Dimenhydrinate / diphenhydramine 50 mg QD
• Tab promethazine
• Tab plasil
• Tab betahistine
• Tab cartan (dexa)

Syncope/Faint

Syncope/Faint
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please :
1. TILT
2. Pulse oximetry
3. Cardiac monitoring
4. BS Glucometry
5. ECG
6. Serum N/S 50 cc iv stat
7. CXR
8. CBC, Bun, Cr, Na, K
9. R/O seizure
10.R/O aorta dissection
WOBBLER for ECG assessment in syncope
Abnormality ECG Section
W Wolff parkinson white P, PR
O Obstructed AV pathway PR
B Bifascicular block QRS
B Brugada ST
LLeft ventricular hypertrophy
(consider AS, HOCM)QRST
E Epsilon wave ST
RRepolarization abnormality
(long QT, short QT)QT

Agitation/Hysteric
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please :
1. ECG
2. Bs Glucometry
3. Amp diazepam 5 mg iv stat
4. Amp haloperidol 5 mg IM stat
5. R/O other disease

Headache

Headache
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please :
1. O2 nasally 6-8 lit/min
2. Iv line N/S 500cc
3. Amp Apotel 1 gr stat q20min in 150 cc N/S
4. If SAh : amp morphine 3-5 mg
5. Amp metoclopramide #1 in bottle
6. Amp dexamethasone #1 in bottle
7. Amp diazepam #1 in bottle
8. Imaging (Brain CT/MRI)
9. CBC, BUN,Cr, Na, K, BS
10.U/A
If migraine headache :
• Amp dexa #1 IM
• Amp promethazine #½ IM
Alarm sign:
Acute & severe
Associated with vomiting,fever,trauma
Awakening
Early morning
Neurologic deficit
Neck rigidity
Near 1st episode
Progressive
Positional
Always unilateral

Seizure

Seizure
Admit :
Dx : seizure
Cond :
Vitals :
Act :
Diet :
Please :
1. O2 nasally 6-8 lit/min
2. ECG
3. ABG
4. BS Glucometry
5. IVF N/S 500cc stat
6. Amp diazepam 5-10 mg IV stat if convulsion
7. CBC, BUN,Cr, Na, K, BS
8. Brain CT Scan if
1. First experience
2. Persistent headache
3. Long postictal period
4. Fever
5. Age > 45

CVAAdmit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please :
1. O2 nasally 6-8 lit/min
2. ECG
3. ABG
4. BS Glucometry
5. Pulse oximetry
6. Cardiac monitoring
7. NGT if unable to po feeding
8. IVF N/S maintenance
9. If not hemorrhage : Tab ASA 325 mg stat then 80 mg po qd
10.Atorvastatin Tab 80 mg qhs or 40 mg BID
11.Labetalol 10 mg IV stat if BP > 220/120
12.Apotel for headache
13.CBC, BUN,Cr, Na, K, BS
14.TG, Chol, LDL, HDL
15.CK-MB Troponin
16.CXR
17.Brain CT Scan
18.Brain MRI s gad c DWI
19.Echocardiography
20.Color doppler of Both carotid & vertebral Artery
21.Intubation if needed
22.CPR if needed
Hemorrhagic CVA :
Avoid ASA
Phenytoin 750 mg iv infusion
N/S consult
If BP > 180
Amlodipine 5 mg for blood
pressure control

WeaknessIf neurologic sign : approach to CVA
If not : approach to infection, cardiac, metabolic problems
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please :
1. O2 nasally 6-8 lit/min
2. ECG
3. ABG
4. BS Glucometry
5. Pulse oximetry
6. Cardiac monitoring
7. NGT if unable to po feeding
8. IVF N/S maintenance
9. Serum N/S 500-2000 cc if shock with check rales
10.Amp ceftriaxone 1 gr if sepsis
11.Amp apotel 1gr stat
12.CBC, BUN,Cr, Na, K, BS
13.PT, PTT, INR if SIRS+
14.Troponin if needed
15.U/A, U/C r/o sepsis
16.B/C R/o sepsis
17.CXR

Decreased LOC

Decreased LOC
Admit :
Dx : hypotension, hypothermia, hypoglycemia
Cond :
Vitals :
Act :
Diet :
Please :
1. BS Glucometry
2. ABG
3. ECG
4. Folley
5. O2 nasally 3-5 lit/min
6. Pulse Oximetry < 90 : intubate
7. Collar in trauma
8. Free hydration
9. Phenytoin 15-20 mg / kg c 25 /min
10.Antibiotic [if fever]
11.CBC, BUN, Cr, Na, K, BS
12.TSH, T4
13.Culture if Sepsis
14.CXR (aspiration pneumonia)
15.Brain CT Scan
Intubation if sign & symptoms of
herniation :
• semi-setting ,
• mannitol,
• hyperventilation
Dextrose naloxone may need (TNGO)

Multiple Sclerosis (Pulse Therapy)Admit :
Dx : Pulse therapy
Cond :
Vitals :
Act :
Diet :
Please :
1. Cardiac monitoring
2. ECG
3. Ranitidin 150 mg PO BID
4. Methylprednisolone 500 mg in 500 cc D5W during 4 hour BID x2day
5. LFT
6. U/A, U/C
7. ESR, CRP
8. Ck K & BS QD

Snake/Scorpion Bite
Admit :
Dx : snake bite / scorpion bite
Cond : fair to good
Vitals : q1h
Act : CBR
Diet :
Please :
1. Cardiac monitoring
2. ECG
3. Inform physician ASAP if INR > 2
4. Washing the wound
5. Apply ice pad locally
6. Td 0.5 cc IM
7. Vial anti venom #3 IV infusion (max: 8-10 vial)
[If manifestations consist for 6 hours add 2 vial more]
8. Keflin 1 gr IV stat
9. Amp dexamethasone #1 [½ if age < 10]
10.Amp chlorpheniramine #1 [½ if age < 10]
11.Amp metoclopramide #1 [½ if age < 10]
12.Tab acetaminophen 500
13.Cap cephalexin 50 mg q6h
14.CBC, BUN, Cr, Na, K, BS
15.LFT
16.PT, PTT, INR q8h
17.U/A BID
Alarm signs :
Hematuria
Convulsion
Decreased LOC
Bleeding
If INR > 2 :
Transfer 1 bag FFP
Anti venom indication :
Swelling
Coagulative problems
Progressive local symptoms
If U/A shows blood :
Hydrate the pt because of ATN
Do not order ibuprofen and
narcotics
Skin test before anti-venom :
Test venoum if allergy : 10x dilate in
n/s , 0.2 cc sq for 30 min

Insect Bite
1. Pull out the bite
2. tab / syrup hydroxyzine
3. Oint CALAMINE-D #1
4. Tab antihistamine #10
Domestic animal Human Bite
1/ washing the wound
2/ do not suture fast (wait)
Infection prophylaxis :
Dog bite :
• Co-amoxiclav x3 day
Cat bite :
• Cephalexin 500 qd for 3 days
Human bite :
• Cephalexin or Co-amoxiclav for 7-14 days
پیشگیری از کزاز و هاری در تمامی بیماران

Poisoning Admit :
Dx :
Cond : emergent
Vitals : q1h
Act : CBR
Diet :
Please :
1. BS Glucometry
2. ECG
3. Pulse oximetry
4. Cardiac monitoring
5. O2 supplement 6-8 lit/min
6. NG Washing
7. ABG (VBG)
8. Internist consult
9. IVF maintenance
10.Serum N/S 500cc IV stat
11.Charcoal 1 gr/kg + sorbitol 70% 1 gr/kg
12.Consider Antidote
13.CBC, BUN, Cr, Na, K, BS
14.PT, PTT, INR
ABC
If lithium ,alcohol, heavy metal and
non-halogen hydrocarbon :
[there is no need for NG washing
and charcoal sorbitol]
Do not release acetaminophen
poisoning rapidly.
Consider cardiac arrhythmia

CO Poisoning
Admit :
Dx : CO poisoning
Cond : emergent
Vitals : q1h
Act : CBR
Diet : NPO
Please :
1. Put the pt in supine position
2. BS Glucometry
3. ECG
4. ABG (VBG)
5. Pulse oximetry [it shows false data]
6. CO Oximetry
7. Cardiac monitoring
8. O2 supplement 10 lit/min (hyperbaric O2 if indicated)
9. amp apotel 1 gr over 20 min
10.amp ondansetron 4 mg IV stat
11.Observe for 4 hours
12.Internist consult
13.IVF maintenance
14.Serum N/S 500cc IV stat
15.CBC, BUN, Cr, Na, K, BS

Hypocalcemia
Admit :
Dx : severe hypocalcemia (ca : 5.5) e.g after post-parathyroidectomy
Cond :
Vitals : heart monitoring
Act :
Diet :
Please :
1. ECG (consider QT prolongation)
2. Nephrologist consult
3. Ca-gluconate 10% 2 vial in 100 cc D5W% infusion in 20 min with heart monitoring
(consider bradycardia)
4. Ca-gluconate 10% 6 vial in 500 cc D5W% infusion in 6 hour
5. Calcitriol cap | 2 cap | po stat & tid
6. Ca-carbonate 1 gr po tid (with meals)
7. CBC, BUN, Cr, Na, K, BS
8. Check K qd
9. Check Ca, P bid
10.PTH

Alcohol Poisoning
1. IVF | D5W 500 cc⅓ ⅔ | D5W 500 cc⅔ | D5W 500 cc
2. Amp metoclopramide #1
3. Amp diazepam #1
4. Amp ranitidine 50 mg
5. Amp vit B-complex

Methadone Poisoning
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. Heart monitoring
2. pulse oximetry
3. ECG
4. NGT
5. IVF 3000 c in 24 hour⅓ ⅔ | D5W 500 cc⅔ | D5W 500 cc
6. charcoal 1gr/kg + sorbitol
7. amp naloxone 2 amp stat
8. Infusion naloxone 10 amp in 100 cc ½ in 10 hr ⅔ | D5W 500 cc
9. CBC, BUN, Cr, Na, K, BS
10.U/A

Anaphylaxis
Admit : ICU admission
Dx : anaphylaxis
Cond : emergent
Vitals : q15min
Act : CBR
Diet : NPO
please
1. cardiac monitoring
2. pulse oximetry
3. VBG(serial)
4. ECG
5. Iv line 2 large bore
6. IVF 1000 cc N/s free
7. O2 Supply 6-8 lit/min
8. Epinephrine 1:1000 0.5 cc IM stat q5min
9. Amp Hydrocortisone 200 mg IV stat
10.Amp Ranitidine 50 mg IV Q8h
11.Amp Chlorpheniramine 10 mg IV stat
12.Diphenhydramine 50 mg q6h
13.Hydroxyzin 1 Tab po stat
14.spray salbutamol 6 puff q20min x3 if dyspnea
15.Salbutamol 8 puff q20min or ventolin 2.5 mg c nebulizer q20min
16.CBC, BUB, Cr, Na, K, Bs
17.Pt, PTT, INR
18.U/A
19.ESR
20.Troponin, CKMB
21.CXR

Hypoglycemia
Admit :
Dx :
Cond :
Vitals :
Act :
Diet : NPO
Please
1. ABG
2. BS Glucometry
3. Heart monitoring & pulse oximetry
4. Check BS q30 min x4 then q1hr x2, q2hr x2, q6hr
5. ECG stat and 1 hour later
6. Serum DW 10% 100 cc/hr infusion hold in bs>300
7. Vial DW 50% 1 gr/kg stat #3 if BS < 70
8. Vial DW 50 % stat if BS < 100
9. BS glucometry DW 50% بعد از اتمام
10.Internist consult
11.Amp glucagon
12.Ceftriaxone 1gr BID
13.Pantoprazol 40 mg BID
14.CBC, Bun, Cr, electr , BS
15.PTT, PTT INR
16.Troponin
ساعت بستری شود۲۴بیمار حداقل
BS > 150 x3
Can give po glucose instead of IV
glucose (but if the pt is full alert)

DKA
Admit : Endocrinologist or internist service
DDx : DKA, HHS
Cond : Emergent
Vitals :
Act :
Diet : NPO
Please
1. ECG
2. Check I/O
3. IVF 1000cc N/S stat (repeatable,max 2500cc)
Then
if BS>250 IVF 500cc HS/hr
if BS<250 IVF 125cc HS+125cc DW5% /hr
4. Regular Insulin
if BS>250 0.1 IU/kg stat & 0.1 IU/kg/h
if BS<250 0.05 IU/kg/
1. Optimal rate of glucose decline is 100mg/dL/h
2. Do not allow the blood glucose level to fall below 200 mg/dL during the first
4-5h of treatment
5. If 3.5<K<5.2 :
1. IV KCl inf. 15-30 meq/h
1. if K>5.2 then hold KCl inf.
2. if K<3.3 then hold insulin inf.
6. CBC, BUN, Cr, Na, K
7. Check BUN, Cr, Na, K Q4h
8. Check And Chart BS Q1h
9. U/A
10.ABG stat & Q4h
11.Endocrinologist Consult

Renal Colic
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please
1. IVF 500 cc n/s with :
2. amp ketorolac 30 mg IV stat
3. amp morphin 3-5 mg IV stat
4. Supp diclofenac (50-100 mg) rectally stat & q6h if needed
5. Amp apotel 1gr (100 cc N/S in 20-30 min)
6. Amp hyoscine 10 mg
7. Amp aminophylline 250 mg
8. CBC, bun, cr, Na, K, Ca,
9. U/A if not k/c of renal stone (first time)
10.KUB x-ray
11.KUB Sonography
12.bedside ultrasound ( r/o hydronephrosis)
Alarm sign :
Fever, anuric, pregnancy
When discharge :
Cap naproxen 500 mg #10
Tab tamsulosin 0.4 mg #20 QD
Supp diclofenac 100 mg #10
Consider :
25-50 mg pethidine , diclofenac amp ,
diazepam amp

Pneumonia
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. ECG
2. VBG
3. Sputum for gram stain & culture
4. IV line
5. Serum N/S 1 lit
6. IVF 1000 cc N/s in 1 hour if in shock
7. O2 supplement 6-8 lit/min
8. Spray salbutamol 4 puff stat (if COPD)
9. Cap azithromycin 500mg stat and daily (after po)
10.Amp ceftriaxone 1gr stat and q12h
11.CBC, Diff, BUN, Cr, Na, K
12.PT PTT INR if sepsis
13.CRP, ESR
14.CXR
15.B/C
16.U/A & U/C
vanco, cipro considered
Admission indication :
• Adult : CURB 65
• Age < 6 month :
• immune def,
• toxic,
• distress,
• dehydration,
• vomiting,
• low

Allergic Bronchitis [Severe Cough]
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. Amp aminophylline 500 mg in 200 cc D5W% in 30 min
Then
Aminophylline 250 mg in 100 cc D5W% in 30 min TID
2. Amp hydrocortisone 200 mg IV stat and 100 mg IV q6-8h
3. Tab airokast 10 mg po bid
4. Diphenhydramine syrup 5 cc po tid
5. Acetaminophen codeine 300/25 2 tab po bid
6. Pseudoephedrine syrup 5 cc po tid

Attack of Asthma
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. IV line
2. O2 6-8 lit/min so2>95
3. Spray salbutamol 6-12 puff q20 min x3
4. Spray atrovent 8-12 puff q20min x3
5. Tab prednisolone 50 mg [po stat]
6. amp methylprednisolone 40-60 mg stat if can nor be on po regimen or
amp hydrocortisone 200 mg IV stat
7. amp aminophylline 250 mg (1 amp) IV infusion
8. amp MGSO4 2 gr over 20 min (if not respond to previous order)
9. antibiotics if infection
10.CBC, BUN, Cr, Na, K, BS
11.CXR

UTI
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
• Cipro tab 500 mg bid x 3-5 days [choice]
• Tab cotrimoxazole 480 mg tid [معموال جواب نمیده]
• Tab nitrofurantoin 100 mg
• Syrup cefixime 100 mg wt/5 q6h [for ped]
: برای سوزش ادرار
• Syrup dicyclomine for ped
• Tab hyoscine 10 mg q6-8hr for adults
• Tab phenazopyridine 100 mg tid
Alarm sign:
• Fever
• Flank pain
• Chills
• Pediatric
• Male
• Pregnancy

Multiple Trauma

Multiple TraumaAdmit : ICU admission if very ill
Dx :
Cond :
Vitals : q 30 min then q3h if stable
Act : CBR
Diet : NPO
please
1. Cardiac monitoring
2. Pulse Oximetry
3. Foley catheter fixed
4. Chart I/O
5. ECG
6. ABG
7. NG tube fixed (contraindicated in skull base fx)
8. Reserve 6 units PC
9. IV line * 2 (large bore)
10.serum NS 1000cc IV free repeat another 1 liter if unstable
11.supplemental O2 4-5 lit/min
12.Amp Ranitidine 50 mg / IV / bd
13.Tetanus prophylaxis (if applicable)
14.CBC serial q6h
15.Check Na, K, BUN, Cr, BS,
16.PT, PTT, INR,
17.U/A
18.CXR
19.Pelvic X-ray (AP)
20.Neck view (AP & Lat) including C7-T1
21.FAST
22.Orthopedic X-rays (if applicable)
23.Brain CT scan (if GCS<15, head trauma, vomiting, amnesia)
24.Orthopedic consult (if applicable)
25.Neurosurgery consult (if applicable)
Primary survey
A: can speak normally , no cx midline tenderness
B: symmetrical NL BS without decrease s, o2 sat, emphysema
C: FAST, BP, External Bleeding, abdomen soft without tenderness, gross hematuria
D: GCS : decrease LOC, PTEA, FND, Seizure. N/V, Pupil
E: Expose (axilla/perineum/back) laceration. Laceration, pelvic fx, limb fx, pain and tenderness
F: int foley
G: NG-T
H: Hx of mechanism
I: imaging
Secondary :
Allergy
Medication
Past hx and pregnancy
Last mael
Environment

Penetrating wound with
pneumothorax
Admit :
Dx :
Cond :
Vitals : q 30 min then q3h if stable
Act : CBR
Diet : NPO
please
1. Reserve 2 bag p.c
2. Ext foley
3. BGRh cross match
4. G.S Consult
5. Pulse oximetry
6. Keflin 1 gr IV q6h
7. Gentamicin 80mg IV stat
8. Toxoid 0.5 cc
9. Fentanyl 50 mcg IV stat
10.Chest tube insertion
11.Chest tube dressing
12.CXR after stable & 6 hour later
13.Routine lab data
14.VBG

Head Injury

Head Injury [If Depressed FX]
Admit :
Dx : depressed skull Fx
Cond : emergent
Vitals : q1h
Act : CBR
Diet : NPO
please
1. Iv line
2. Head elevation 30
3. Check GCS q1h
4. BS Glucometry
5. Neurosurgeon consult
6. Amp ondansetron 0.15ng/kg PRN
7. Amp apotel 15 mg/kg for preventing fever
8. Dilantain 15-20 mg/kg stat and of loading dose for maintenance ⅓ ⅔ | D5W 500 cc
9. Brain CT scan without contrast

GI Bleeding

GI BleedingAdmit : Reserve ICU bed (if very ill)
Dx :
Cond : critical
Vitals : q30min
Act : CBR
Diet : NPO
please
1. Cardiac monitoring + Pulse Oximetry (if very ill)
2. NG tube + washing up to clearance
3. Foley cath fixed
4. Chart I/O
5. CV line + CVP control q1h
6. ECG
7. ABG
8. Supplemental O2 4 lit/min
9. Reserve 6 units of PC, 6 units of FFP
10.Transfuse PC if massive gross bleeding or not responsive to crystalloids
11.Transfuse FFP if INR > 1.5
12.Transfuse PLT if PLT < 100,000
13.Visit for Internal Medicine Resident (emergent endoscopy)
14.Serum NS 1000 cc / IV / stat free (repeatable)
15.GI consult
16.Amp Pantoprazole 80 mg IV stat then 8 mg/ hour infusion
17.Octreotide 50-100 mcg IV stat then 25-50 mcg infusion
18.CBC q6h
19.Na, K, BUN, Cr, BS,
20.PT, PTT, INR
21.LFT
22.CXR (portable)
23.Endoscopy
24.Abdominal sonography (R/O cirrhosis)

Bowel ObstructionAdmit :
Dx :
Cond :
Vitals :
Act :
Diet : NPO
Please
1. NG Tube
2. Internal folley
3. Chart I/O
4. ABG
5. ECG
6. Cardiac monitoring & Pulse oximetry (if very ill)
7. Serum NS 1000 cc / IV / stat free (more stat serum if needed)
8. Reserve 6 units of PC
9. Supplemental O2 (3-4 lit/min)
10.IVF
11.Cardiology consult
12.Amp Ranitidine 50 mg / IV / BID
13.Amp Ceftriaxone 1 gr / IV / BID
14.Vial Metronidazol 500 mg / IV / q8h
15.CBC, Na, K, BUN, Cr, BS,
16.PT, PTT, INR,
17.U/A
18.CXR (upright)
19.Abdominal X-ray (supine & upright)
20.Abdominopelvic sonography (CT scan may also be indicated)
Abd.X-ray (supine)>> not necessary (if
clinical Dx is highly suspected)
Gravindex :
The test detects the prevention of
agglutination of HCG-coated latex
particles by HCG present in the urine
of pregnant women (also known as
BHCG Test)

Acute Appendicitis
Admit :
Dx :
Cond :
Vitals : q6h
Act : CBR
Diet : NPO
Please
1. ECG
2. Serum NS 1000 cc / IV / stat free
3. Serum maintenance
4. Cardiology consult if age > 40 Y/O
5. OB/GYN consult if gynecologic problems may not be ruled out
6. Gravindex (for women)
7. CBC, diff, Na, K, BUN, Cr, BS
8. U/A
9. Abdominopelvic sonography (esp. for women)
10.CXR
After Diagnosis is made:
1. Ready for OR (shave, gown)
2. stat serum if dehydrated
3. analgesic (e.g. Morphine 5 mg / IM / stat)
4. stat dose of ABs for prophylaxis (Ceftriaxone & Metronidazole)
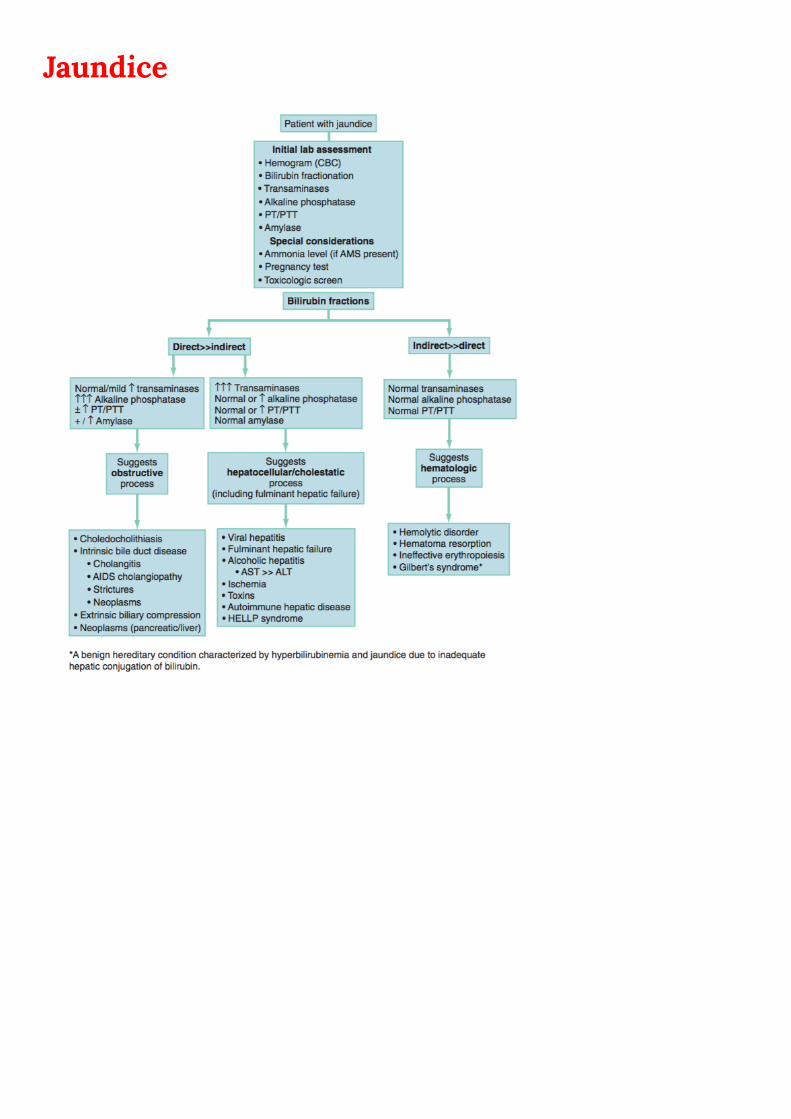
Jaundice

Jaundice

Constipation
:داروهای گیاهی که بیمه نیستن ولی مفید هستن:
• Powder Bran 250 mg #3 TID
قاشق چای خوری : هر بار یک قاشق غذاخوری در یک لیوان آب حل می کند و میخوره و در اطفال
• Powder psyllium 3.5 mg #3
Branطرز مصرف مثل
• Powder sorbitol 5 gr #3 یک بسته پودر با یک لیوان آب هر روز صبح ناشتا مصرف می کند
➢ Tab C-lax
➢ Syrup mom #1 5-20 cc TID
➢ Syrup lactulose
➢ Supp bisacodyl 10 mg
➢ Tab bisacodyl 5 mg # 30 سال ممنوع۶زیر
alarm sign :
Decreased wt
age > 50
Anemia
Rectal bleeding
درصد موارد۱۰
هیپرتیروئید، کاسنر، افسردگی
:آموزش گالبی، انجیر، آلو، سبزیجات
مایعات زیاد
دقه پیاده روی۲۰تحرک روزانه

Diarrhea

Diarrhea OPD Management :
• Tab Loperamide 2 mg #20
تا قرص۸دو قرص بعد از هر بار دفع حداکثر
• Tab Diphenoxylate #30 q6h
ساعت۶یک قرص هر از
In pediatrics :
• Tab dicyclomine 10 mg #30
ماه ممنوعه۶زیر
If there is indication in adults :
• Tab ciprofloxacin 500 mg BID #30
سال ممنوع۱۸زیر
If there is indication in pediatrics :
• Tab cotrimoxazole 120, 480 mg #30
• Powder QRS
با قاشق چای خوری بدین
لیولن یک پاکت ۴آب جوشیده خنک شده
اگه تهوع داره متوکلوپرامید بهش بدین
تا میخوره بهش بدین
Giardiasis
Metro
15-20 mg/kg.day x3 day
250 mg TID
Amebiasis
Metro 30-50 /kg x7days
Tab Metronidazole 250 mg TID
یودوکینو ن نش نونیکودوی د خو نونیکودوی دشن ب اگ نونیکودوی دشن بوخ ه
Colitis
shigellosis
Cefixime 8 mg/kg/day
Cipro (adult)
Alarm sign :
• Age > 70 + abd pain
• Immune deficiency
• Recently AB-therapy
• T > 38.5
• Bloody Diarrhea
لوپراماید حس خوب و نعشگی دارد و بدون
.نسخه داده نمی شود
دیفنکوسیالت حاوی آتروپین است برای
تا آنجا که. جلوگیری از سواستفاده معتادان
.می توان از تجویز آن خودداری نمود
Vibrio
< 9 : cotri
>9 : tetra
اسهال خونی بدون تب رو درمان نکنین مگر
EHECآنتموبوا ببینید و گرنه s/eاینکه توی
داره HUSهس و شانس
اسهال غیر خونی درمان نمیشه به جز ویا و
ژیاردیا
ش نونیکودوی دشن بوخ هاسهال خونی با تب باال درمان می

Sore Throat

Biliary Disorders
1. NPO
2. CVS q4-6h
3. NG tube fixed (if N/V is significant)
4. Foley cath fixed (if ill or aged)
5. Chart I/O (if ill or aged)
6. Serum NS 1000 cc / IV / stat
7. Serum half Saline 1 lit / IV / tds
8. CBC, Na, K, BUN, Cr, BS, PT, PTT, INR, AST, ALT, ALP, Bil (T,D), Amylase
9. Amp Ranitidine 50 mg / IV / bd
10. Amp Pethidine 25 mg / IM / qid
11. Amp Ceftriaxone 1 gr / IV / bd
12. Vial Metronidazol 500 mg / IV / qid
13. Amp metoclopramide 10 mg / IV / stat (if vomits)
14. Abdominal X-rays (supine & upright)
15. Abdominopelvic sonography (liver, GB, biliary tracts)
16. ECG
17. CXR (upright)
If Cholangitis is your working diagnosis, add:
1. CVS q3h
2. Reserve ICU bed
3. Supplemental O2
4. Cardiac monitoring & Pulse Oximetry
5. ABG
6. Chart T
7. Visit for Infectious Disease Resident
8. Visit for Internal Medicine Resident for “GI consultation for emergent ERCP”
9. Check and Chart CVP q2h (stat serum according to CVP)
10. Reserve 6 units PC & 6 units FFP
11. Amp Vit K & FFP transfusion (if INR > 1.5)
12. Cardiology Consult
If Pancreatitis is your working diagnosis, add:
1. Reserve ICU bed (if severe)
2. Supplemental O2 (if severe)
3. Cardiac monitoring & Pulse Oximetry (if severe)
4. VBG, LDH, Amylase, Lipase, Ca (calculate Ranson’s Criteria)
5. CBC serial q8h (if severe)
6. Chart T
7. Abdominal X-ray (supine & upright)
8. Abdominopelvic CT scan with IV/oral contract (Pancreas Protocol)
9. stat serum according to output or CVP
10. Reserve 6 units PC
11. Visit for Internal Medicine Resident
پانکراتیت حاد یک بیماری طبی است، مگر
در صورت بروز عوارض در پانکراتیت شدید و
بنابراین الزم است بیمار در سرویس. نکروزان
مشترک داخلی ـ جراحی بستری گردد و
روزانه از جهت معاینه شکم و بررسی بروز
.عوارض، توسط یک جراح ویزیت شود

Back Pain

PE & DVT

Needle Stick Exposure

Anemia

Vaccination

Electrical shock injury
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please
1. Ecg now & 1 hour later
2. O2 nasally
3. Cardiac monitoring
4. Ophthalmologist consult
5. 1000 cc ringer in 2 hour
6. Td if burn
7. Routine lab data
8. CPK LDH
9. u/A

Intertrochanteric Femur FX
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please
1. skin traction 3 kg
2. internal folley
3. prep 2 bag p.c
4. cardiologist consult [if needed]
5. Enoxa 40 mg qd sq
6. Ranitidine 50mg UV BID
7. amp pethidine 25 mg PRN
Lower EXT FX (pelvic, femur, …) :
enoxa 40 SQ QD
Pt c shoulder joint dislocation :
1. 150 mg thiopental IV stat
2. Reduction

Generalized Peritonitis
Admit :
Dx :
Cond :
Vitals : q1h
Act :
Diet : NPO
Please
1. Cardiac monitoring & Pulse oximetry (if very ill)
2. Supplemental O2
3. ECG
4. ABG
5. Foley cath fixed, Chart I/O
6. Reserve 4 units PC
7. Cardiology consult (for males > 40 y/o and females > 45 y/o)
8. Serum NS 1000 cc / IV / stat (or more stat serum depending on hydration state)
9. Amp Ceftriaxone 1 gr / IV / bd
10. Vial Metronidazol 500 mg / IV / qid
11. Amp Ranitidine 50 mg / IV / bd
12. CBC, Na, K, BUN, Cr, BS,
13. PT, PTT, INR,
14. Amylase, LFT,
15. UA
16. CXR (upright)
17. Abdominal X-rays (upright & supine)
18. Abdominopelvic sonography

Hemoptysis
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please
1. IVF 500 cc N/S q8h
2. Ceftriaxone 1gr II q12h
3. Clindamycin 600 mg IV q8h
4. Dextromethorphan 10 cc po q6h
5. Salbutamol 2 puff q6h
6. Atrovent 2 puff q8h
7. Hydrocortisone 100 mg IV TID
8. Routine lab data
9. Pt, PTT, INR
10. VBG
11. CXR : look for cavity

Wound & Laceration
1. Irrigation & dressing
2. Suture the wound ( consider indication & contraindication )
3. X-ray may needed
4. Toxoid 0.5 cc stat
5. AB for extremity : cipro 500 #20 q12h, cephalexin 500 #30 q6h (OPD)
6. AB inpatient :
1. > 1cm : keflin 1gr ,
2. >5 cm : genta 80mg
7. Tetabulin 250 unit sq

Diabetic Foot
Admit :
Dx :
Cond :
Vitals :
Act :
Diet : Diabetic
please
1. Change dressing BID
2. Smear & culture of discharge
3. Ck BS q6h
4. Amp ceftriaxone 1gr q12h iv
5. Amp clindamycin 600 mg q8h IV
6. Foot x-ray (AP-LAt)

Post Tonsillectomy Bleeding
Admit :
Dx :
Cond :
Vitals : q1h
Act :
Diet : NPO
please
1. head elevation
2. Cold neck compression patch طرف گردن۲در هر
3. Cold liquid Gargle
4. Pack c gauze soaked c amp Tranexamic acid
5. Prep 2 bag P.C
6. Hydrate c 1000 cc N/S stat
7. IVF maintenance
8. Amp Keflin 1gr q6h
9. Amp Tranexamic acid 1 amp IM stat
10.CBC, BUN, Cr, Na, K, BS
11.Ck HB q6h
12.PT, PTT, INR

Dacryocystitis
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. Smear & culture of eye discharge
2. IVF 100 cc in 24 hour
3. Cefepime 1gr iv q8h
4. Clindamycin 600 mg IV q8h
5. Cloxacillin 1 gr IV q6h
6. Ranitidine 50 mg iv q8h
7. CBC, BUN, Cr, Na, K, BS
8. PNS CT s contrast

Optic Neuritis/AION
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. ECG
2. ASA 80 & Atorvastatin 80
3. Methylprednisolone 500 mg in 500 cc DW5% in 4 hour BID x3day
[check BP and HR q1h]
4. CBC, BUN, Cr, Na, K, BS
5. Dsdna, lupus anticoagulant
6. C3, C4, ANA, C-ANCA, P-ANCA
7. ESR, CRP
8. Check BS & K QD
9. Brain MRI c & s GAD
10. Cervical MRI c & s GAD
11. CDS of carotid and vertebral
12. Echo
Pt K/C of HTN & HLP came with LT
eye blindness R/O lt optic neuritis
R/O AION :
(Anterior ischemic optic neuropathy)

Pt with FND symptoms and Brain CT
Shows ICH
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
please
1. Check GCS & pupil q1h
2. Head elevation
3. Phenytoin 125 mg q8h
4. Manitol 20% 400 cc in 45 min then 40 cc q6h
5. Transfer to ICU

Thermal Trauma (Burn)
Admit :
Dx :
Cond : Emergency
Vitals :
Act : CBR
Diet : NPO
Please
1. Washing c silver sulfadiazine
2. Debriding with mild soap and water
3. Sterile dressing
4. ECG
5. IV line large gauge
6. Ringer 1 lit free
7. Ringer lactate 4 cc / kg / % BSA (½ in 8 hour and ½ in next 16hr)
8. Keflin 1 gr iv stat
9. Pethidine 50 mg iv stat
10. Midazolam 2 mg iv stat
11. Toxoid 0.5 cc IM stat
12. CBC, elect
13. echarotomy
14. ABG
15. CXR
16. U/A
17. Stablish airway : inhalation injury
Oint silver-sulfadiazine #1
• Cephalexin 500 mg po q6h
• Ibuprofen

Varicella (Chicken Pox)
Admit :
Dx :
Cond :
Vitals :
Act :
Diet :
Please
1. Isolate room c negative pressure
2. Serum 500 cc q8h⅓ ⅔ | D5W 500 cc⅔ | D5W 500 cc
3. Syrup diphenhydramine 7.5 cc q6h
4. Tab loratadine 1 tab q12h
5. Amp ranitidine 50 mg IV q8h
6. Amp acyclovir 500mg in 500 cc N/S in 4 hour IV q8h
7. Tab acyclovir if age > 13
8. Amp Apotel
9. Oint calamine-D روزانه بعد از حمام
10. Tab cephalexin (250-500) q6h if ofoonat poosti
11. CBC, BUN, Cr, Na, K, BS
12. BUN Cr QD
13. OB Sono if pregnant
مصرف مایعات- گواهی یک هفته - حمام روزانه

Dental Abscess
• IVF 2000 cc N/S in 24 hours⅓ ⅔ | D5W 500 cc⅔ | D5W 500 cc
• Ceftriaxone 1 gr IV q12h
• Metronidazole 500 mg IV q8h
Bell's palsy
1. Amp acyclovir 500 mg q8h in 500 cc n/s
2. Tab prednisolone 50 mg QD
3. Brain CT & PNS CT Scan
Angioedema
1. Amp hydrocortisone 100 mg IV tid
2. Amp clemastin 2 mg IV tid
Or
Amp chlorpheniramine 10mg tid iv

Birth Control
• Tab ocp (LD/HD) #21 یک بسته یا
)موثرتره( روز و بعد یک هفته استراحت ۲۱از روز شروع خونریزی تا قاعدگی تا اتمام و بعد یک هفته استراحت۵از روز
در ماه اول یک روش جایگزین حتما استفاده شود
• Tab OCP Triphasic BWY
Emergency contraception
• Tab OCP HD #4
ساعت ۷۲اثر تا / ساعت بعد۱۲دو قرص / دو تا قرص در اسرع وقت
• Tab OCP LD #8 قرص در اسرع وقت۴
ساعت بعد۱۲ قرص ۴
تهوع زیاد میده
• Tab OCP triphasic #یک بسته
قرص سفید یکی۴
ساعت بعد۱۲ قرص سفید دیگر ۴
• Tab levonorgestrel 750 mcg #2
)بیشترین موفقیت( قرص یک جا بدون تکرار ۲
Tab ondansetron
Tab metoclopramide واسه تهوع در کنارش میدیم

Premature Ejaculation
Tab sertraline 25, 50, 100
شش ساعت قبل یک دونه میخوره sex هفته روی یکی میخوره بعد از آن قبل از ۳
Tab tramadol 25mg یک ساعت قبل از سکس
on & off: مفید ترین روش روش های غیر دارویی را برای مریض ارائه دهید
Vit D deficiency
Check 25(OH)
< 20 ng/ml : def
20-30 : insufficiency
Vitamin D3 (cholecalciferol) pearl 50,000 IU #10 هفته سپس ماهی یک عدد۸هفته ای یک عدد به مدت
Ck 25 (OH) D after treatment if < 20 ng/ml : repeat Txاگه بازم باال نیومد مشاوره گوارش جهت سو جذب
ماه بعد چک کرد۴-۳ می توان از ابتداا با ماهی یک عدد شروع کرد و ۳۰-۲۰در گروه
.نیاز به ویتامین دی دارند IU 800افراد بالغ روزانه
. احمال توکسیسیته وجود دارد۱۰۰در صورت افزایش بیشتر از

Epistaxis
• Oint tetracycline #1 طرفه برای دو روز ۲انجام تامپون •
• Cephalexin q6h
• Drop phenylephrine #1 اگر مسن نیست و فشار خون ندارد
Enterobiasis
• Tab mebendazole 100 mg # 2xFM
Or
• Tab albendazole 400 mg # 4
• Syrup hydroxyzine 10 mg/ 5 cc (wt/4) #1
Or
• Tab hydroxyzine 10 q6h #10
Generalized pain in elderly patients
• Tab naproxen 250, 500 #30 TID
• Amp vit-D #3 monthly
• Tab Ca-D #100 qd
• Gel piroxicam #1
• Tab prednisolone 5 mg #30 qd
• Tab Amitriptyline 25mg #100 qhs
Alarm signs :
HTN
Head trauma
Bilateral
On coagulate drug

Opium quitting
• Tab amitriptyline 10,25 mg bid
Or
• Imipramine
• Tab clonazepam 1 or 2 mg qhs
• Serum therapy B-complex, vit-b, vit-c
• Tab folic acid 1 mg
• Tab ibuprofen 400 mg q4-6h
PMS
• Cap fluoxetine 10, 20 #100 qd روز دوم سیکل ۱۴در
• Tab alprazolam 0.5, 1 mg #30 روز۱۴فقط همون
• Tab ca-carbonate #100 bid روز۱۴همان (یکی صبح یکی شب (
• Tab aldactone 25 mg #14 روز۱۴همون
برا اونایی که ورم می کنن
Hiccups
Choice :
• Amp chlorpromazine 25mg in 100 cc N/S
2nd:
• Amp Haloperidol 5 mg IM
3rd :
• Amp metoclopramide IM
بای پریدین: در صورت ایحاد بی قراری های هالوپریدول و متلکلوپرامید

Cornمیخچه: اگر فشار عمودی درد
زگیل: اگر از بغل درد
شست و شو با آب گرم و خشک
Zinc oxide دور زخم
:محلول ضد میخچه را با گوش پاک کن روی محل
Lactic Acid 16.7% + Salicylic Acid 16.7% + Flexible Collodion base Up to 100%بانداژ
Hair loss
• Cap zinc 50 mg #100
• Susp minoxidil (2% for F)(5% for M) #1 بار روی اسکالپ۲روزی یک یا
ماه بعد۴شروع اثر
ساعت بعد موها شسته نشه۴تا
• Or foam minoxidil
• For male : tab finasteride 1 mg #100 QDبرای فردی که زنش قصد بارداری داره ممنوعه
Anorexia
• Tab cyproheptadine 4 mg #30 QD
• Cap Zinc 50 mg #100 QD
• Syrup Multivitamin

H.pylori Infection
• Cap tetracycline 250 mg #100 ساعت۶ قرص هر ۲
• Tab bismuth 120 mg #56 ساعت۶ قرص هر ۲
• Tab clarithromycin 500 mg BID
• Tab amoxicillin 250 mg ساعت۶یک گرم هر
• Cap omeprazole 20 mg #28 به همه بدید، صبحانه ناشتا یه دونه
• Tab metronidazole 250 mg #56
Choice : MBTO منو ببر تهران االغ
هفته ای است۲درمان
امپروزال+ دارویی است ۴درمان
دارویی است۳دنباله درمان

Cough
• Syrup dextromethorphan for dry cough سرفه ی تک تک
ساعت ۶ سی سی هر ۵
• Dextromethorphan-p همراه با سودوافدرین هست
اثر ضد احتقانی
در صورتی که مریض التهاب داره، آبریزش داره
در مریض فشار خون ممنوعه
روز ممنوع۲بیش از
دکسترومتورفان چون آثار اپوعید داره برای معتادنی خوبه
• Syrup/tab Bromhexine q6h
• For pediatric cough به شدت خلط آور است
برونشیت، آسم، نومونی
• Syrup expectorant برای سرفه هایی که هم خلط دارن و هم عالئم آلرژیک
اثر خلط آوری: گایفنازین
اثر ضد احتقان: سودوافدرین
اثر آنتی هیستامین : کلروفنیرآمین
• Syrup guaifenesin برای سرفه های سرماخوردگی
سال ممنوع۴زیر
• Syrup diphenhydramine
برای سرفه های فارنژیت
به شدت خواب آور
Alarm sign : duration > 3 wk

Pharyngitis
• Vial penicilline
< 27 kg 600.000 benzatin
> 27 kg 1.200.000 benzatin
<27 : #1 6.3.3
>27 : #2 6.3.3
• Tab penicillin V 500 TID x10 #30
• Tab erythromycin 400 mg TID x10 days #30
در صورت حساسیت
• Tab syrup acetaminophen
Common Cold
Adult :
• Tab coldstop #30 ساعت ۶ قرص هر ۲
• Coldstop :
500 mg acetaminophen
30 mg pseudoephedrine
25 mg diphenhydramine
:گرفتگی بینی مخصوصا اطفال
• Drop Nacl
: ماه ۶بچه های باالی
• Pediatric grip syrup
:برای همه
• Eff -tab Vit-c آب میوه طبیعی
پرهیز از آب میوه بازاری و نوشابه و اینا
سوپ و ایاها
مصرف مایعات فراوان
باکتریال
تب/ گلودرد شدید / شروع سریع و حاد
تهوع و درد شکم/ سردرد / متوسط تا شدید
/اریتم واضح گلو/ پتشی روی کام / لنفادنوپاتی
وایرال
همراهی با سرفه،/ تب کمتر/ شروع آهسته
اسهال/ کانژکتیویت، کورایزا
Alarm sign :
Epiglottitis, distress, drooling,
extra tonsil inflammation &
exuda

Erectile Dysfunction
• Tab sildenafil 25, 50 , 100تک دوز یک ساعت قبل از نزدیکی
یا نیتروکانتین بخوره TNGمریض نباید داروهایی مثه
• Tab viagra 50 این خارجیه گرون تر و بهتره
یک ساعت قبل از نزدیکی
Sinusitis1st choice:
• Cap co-amoxiclav 625mg #42 TID x2wk
2nd choice :
• Tab cefixime 400 mg BID #28
• Tab ibuprofen 400 mg #30
• Drop phenylephrine 0.5% #1
روز ۳حداکثر
ساعت یک قطره در هر سوراخ بینی ۱۲هر
• Serum physiology
• Tavanex 750 mg po QD
Choice :
• Amoxicillin (80-90mg/kg) سینوزیبت بدون عارضه
روز پس از رفع عالئم۷تا
:موارد نیاز به کوآموکسی سال۲زیر
نگهداری در مهدکودک
ماه گذشته۳مصرف آنتی بیوتیک در
) ساعت باید تب و کم و ترشحات بینی کاهش یابد ۴۸در عرض ( ساعت اول ۷۲عدم پاسخ به داروهای قبلی در
روز ۱۰سرماخوردگی بیش از
سرفه شبانه طول کشیده : بچه ها
Cefepime 1 gr IV q8h
Metronidazole 500 mg IV q8h
Nasal spray fluticasone 2 puff q8h
Nasal spray nacl 2 puff q6h
Pantoprazol 40 mg qd po
PNS CT

Otitis Media (AOM)
• Syrup amoxicillin 125-50 mg 80-90 mg/kg
• Syrup ibuprofen
• Drop dexamethasone
• Syrup co-amoxiclav
• Amp ceftriaxone 50 mg/kg درمان تک دوز سفتریاکسون معادل چند روز شربت است
Brucellosis
• Cap doxy 300 mg q12h
• Cap rifampin 300 mg q12h
• Amp panto 40 mg qd

Pediatric Dosage syrup
cefixime 100 mg wt/5 q12h
hydroxyzine wt/4
cephalexin
125 wt/4
q6h250 wt/8
ondansetron wt/4 q8h
salbutamol wt/2 q6h
azithromycin
100 wt/4
qd200 wt/8
erythromycin 200 Wt /4 q6h
cotrimoxazole Wt /2 Q12h
Amoxicilline
125 wt
q8h250 wt/2
400 wt/3
co-amoxiclav
156 wt
q8h312 wt/2
Diphenhydramine wt/3 q6h
Acetaminophen 125 wt/2 q6h
Brufen wt/2
pencllin-v 250 wt/2 q6-8h
Expectorant 0.5 cc/kg/24hr q8h
Promethazine 0.4 cc/kg/24hr q6h
Drop
Drop Acetaminophen 8 drop/kg/24hr Wt x 2
Drop Dextromethorphan 8 drop/kg/24hr q6h
Drop plasil 2 drop/kg/24hr wt/2 q8h
Drop Rifampin 2 drop/kg/24hr
Drop Dimethicone 3 drop/kg/24hr q8h
Drop ferrous sulfate 1-2 drop/kg/24hr Max : 15 drop
Drop Nistatin 20-40 drop q6h

Syrups with dosage of 1 cc/ kg
[consider dividing]
• Syrup amoxicillin 250 q8h
• Syrup ampicillin 250 q6h
• Syrup cephalexin 250 q6h
• Syrup erythro 200 q6h
• Syrup penicillin-v 250 mg q6h
• Syrup pediatric grip q6h
• Syrup dicyclomine q6h [above 6 m/o]
• Syrup hydroxyzine q6h
• Syrup brufen q6-8h
Medication : Take with Food
• Clindamycin
• Co Amoxiclav
• Baclofen
• Statins (nights)
• Danazol
• Sulfonamides
• NSAIDs

Medication : Take with plenty of water
• Alendronate
• Laxative
• Almgs
• Doxycycline
• Vitamins and supplements
• Ca (night)
• L-Carnitine
• Glucosamine
Medication : Before Breakfast
• PPIs
• Alendorante
• levothyroxine

Medication : Before Meals
• Bisacodyl
• Penicillin
• Bismuth
• Cardiac drugs
• Levodopa
• Methotrexate
• Loratadine
• Clidinium-C
• Digoxine
• Warfarin
• Captopril
• Rifampin
• Tetracycline
• Sucralfate
Antihistamines
• Tab loratadine 10 mg qd/bid
• Tab cetirizine 10 mg qd/bid
• Tab fexofenadine (Telfast) 60,120,180 qd/bid
اثری ندارد QTروی . تنها دارویی که می توان با ماکرولید ها داد•
• Tab cyproheptadine 4 mg
• Anorexia nervosa
• Carcinoid syndrome
• Cold hives
• Tab Hydroxyzine 10 mg
تنها آنتی هیستامین که می توان زیر یک سال داد•
• Amp chlorpheniramine
• Amp clemastin









