

Page 1 of 6 CPF-020 04/13
Group Application (Delta Dental, VSP and Unum Life & LTD)
Group Information
Company Name: DBA:
Street Address:
City: State: Zip:
Billing Address (if different):
City: State: Zip:
Employer is: Partnership Corporation Sole Proprietorship Public Agency
Other (Please Explain):
Date Business Established:
SIC Code (required): Type of Business: Tax ID #:
Contact Name: Title:
E-mail: Phone: Fax:
What is your communication preference? Mail E-mail Fax
Coverage Applying For: (Check all that apply)
Dental Vision Life LTD
Requested Effective Date:
Group Eligibility Information
Total Number of Employees: Total Number of Eligible Employees: Total Number of Enrolling Employees:
Is the waiting period waived for initial enrollments? Yes No
Eligibility begins on the first of the month following:
Date of Hire 1 Mo. 2 Mo. 3 Mo. 6 Mo. Other:
Is this group a class carve-out? Yes No
If yes, state the class of employees to be covered:
(For Delta Dental, employees not covered by Delta PPO plans must enroll in DeltaCare USA plans or be left uninsured. Carve outs will be classified as level 2 regardless of true industry SIC)
Does company have a pre-tax Sec. 125 or POP plan? Yes No
Is your group currently subject to Cal-COBRA? Yes No
(Employed 2-19 eligible employees on at least 50%
of its working days in the previous calendar year)*
Is your group currently subject to COBRA? Yes No
(Employed 20+ eligible employees on at least 50%
of its working days in the previous calendar year)*
Domestic Partners allowed to enroll? Yes No
Children of Domestic Partners eligible to enroll? Yes No
*Visit www.dol.gov for more COBRA eligibility information.
Vision Service Plan
Prior Carrier: Cancel Date: Total Number of Enrolling Employees:
Vision Service Plan Selection (2+ Enrolling Employees)
Choice Plans Signature Plans
Plan A $20 Plan A $25/$25
Plan B $20/$20 Voluntary Plan B $25 $150/$150
Plan C $25 $150/$150 Plan C $25 Voluntary $150/$150
Plan A $25 Plan B $25
Vision Plan Employer Contribution
Employee: (100% for all plans except the voluntary plans)
Dependent: (minimum 0%)
A $15 administrative fee is charged each month to all VSP groups. New groups with 2 to 4 employees are charged a discounted administrative fee of $10 per month, guaranteed for one year.
Page 2 of 6 CPF-020 04/13
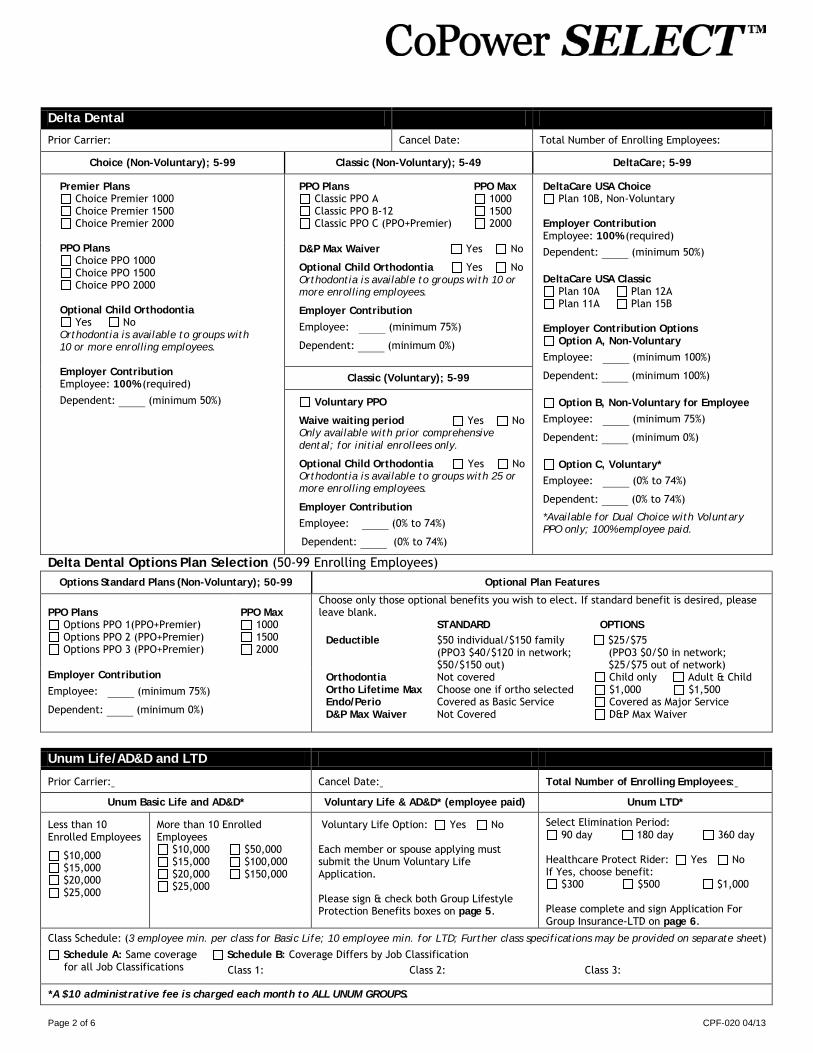
Delta Dental
Prior Carrier: Cancel Date: Total Number of Enrolling Employees:
Choice (Non-Voluntary); 5-99 Classic (Non-Voluntary); 5-49 DeltaCare; 5-99
Premier Plans Choice Premier 1000 Choice Premier 1500 Choice Premier 2000
PPO Plans
Choice PPO 1000 Choice PPO 1500 Choice PPO 2000
Optional Child Orthodontia
Yes No Orthodontia is available to groups with 10 or more enrolling employees. Employer Contribution Employee: 100% (required)
Dependent: (minimum 50%)
PPO Plans Classic PPO A Classic PPO B-12 Classic PPO C (PPO+Premier)
PPO Max 1000 1500 2000
DeltaCare USA Choice Plan 10B, Non-Voluntary
Employer Contribution Employee: 100% (required)
Dependent: (minimum 50%) DeltaCare USA Classic
Plan 10A Plan 12A Plan 11A Plan 15B
Employer Contribution Options
Option A, Non-Voluntary
Employee: (minimum 100%)
Dependent: (minimum 100%)
Option B, Non-Voluntary for Employee
Employee: (minimum 75%)
Dependent: (minimum 0%)
Option C, Voluntary* Employee: (0% to 74%)
Dependent: (0% to 74%)
*Available for Dual Choice with Voluntary PPO only; 100% employee paid.
D&P Max Waiver Yes No
Optional Child Orthodontia Yes No Orthodontia is available to groups with 10 or more enrolling employees.
Employer Contribution
Employee: (minimum 75%)
Dependent: (minimum 0%)
Classic (Voluntary); 5-99
Voluntary PPO
Waive waiting period Yes No Only available with prior comprehensive dental; for initial enrollees only.
Optional Child Orthodontia Yes No Orthodontia is available to groups with 25 or more enrolling employees.
Employer Contribution
Employee: (0% to 74%)
Dependent: (0% to 74%)
Unum Life/AD&D and LTD
Prior Carrier: Cancel Date: Total Number of Enrolling Employees:
Unum Basic Life and AD&D* Voluntary Life & AD&D* (employee paid) Unum LTD*
Less than 10 Enrolled Employees
$10,000 $15,000 $20,000 $25,000
More than 10 Enrolled Employees
$10,000 $50,000 $15,000 $100,000 $20,000 $150,000 $25,000
Voluntary Life Option: Yes No Each member or spouse applying must submit the Unum Voluntary Life Application. Please sign & check both Group Lifestyle Protection Benefits boxes on page 5.
Select Elimination Period: 90 day 180 day 360 day
Healthcare Protect Rider: Yes No If Yes, choose benefit:
$300 $500 $1,000 Please complete and sign Application For Group Insurance-LTD on page 6.
Class Schedule: (3 employee min. per class for Basic Life; 10 employee min. for LTD; Further class specifications may be provided on separate sheet)
Schedule A: Same coverage for all Job Classifications
Schedule B: Coverage Differs by Job Classification Class 1: Class 2: Class 3:
*A $10 administrative fee is charged each month to ALL UNUM GROUPS.
Delta Dental Options Plan Selection (50-99 Enrolling Employees) Options Standard Plans (Non-Voluntary); 50-99 Optional Plan Features
PPO Plans
Options PPO 1(PPO+Premier) Options PPO 2 (PPO+Premier) Options PPO 3 (PPO+Premier)
PPO Max
1000 1500 2000
Choose only those optional benefits you wish to elect. If standard benefit is desired, please leave blank. STANDARD OPTIONS Deductible $50 individual/$150 family
(PPO3 $40/$120 in network; $50/$150 out)
$25/$75 (PPO3 $0/$0 in network; $25/$75 out of network)
Orthodontia Not covered Child only Adult & Child Ortho Lifetime Max Choose one if ortho selected $1,000 $1,500 Endo/Perio Covered as Basic Service Covered as Major Service D&P Max Waiver Not Covered D&P Max Waiver
Employer Contribution
Employee: (minimum 75%)
Dependent: (minimum 0%)

Page 3 of 6 CPF-020 04/13
Payment
Invoices Would you like to receive invoices electronically? Yes No If Yes, complete the following:
Contact Name Title Email The above information will be used to authenticate access to the invoice. You must notify CoPower if this contact or e-mail address changes.
Initial Payment Please make check payable to CoPower and submit with your Employer Application and any other enrollment paperwork. This is a pre-paid plan. Monthly payments are due no later than the first day of the coverage month.
Ongoing Payment Do you wish to have your monthly invoice amount automatically debited from your company account? Yes No If yes, please complete the following. Allow up to one billing cycle to process your request. You must continue to submit your payment until your invoice indicates that the amount due will be debited from your account.
Bank Account Information (must be a Checking Account) Account Holder’s Name (if different from above): Name of Bank: Bank Address: Bank Routing Number: Account Number:
I hereby authorize CoPower to initiate debits from the account identified above. I understand it remains in effect until I give written notice to CoPower, which I must do by the 25th of the month. If I want to change the banking information that CoPower debits, I will submit a new Direct Debit Authorization form by the 25th of the month. In the event a debit is made to my account in error, I authorize CoPower to make a correcting entry to my account. CoPower will notify me of payments returned for insufficient funds or closed accounts, and repayment instructions. Please attach a copy of a voided check.
Signatures Employer Signature My signature on this document certifies that all of the information contained in this application is true and correct to the best of my knowledge. I confirm that all enrollees are eligible employees, COBRA participants, and/or their dependents. In addition, my group complies with all the rules and regulations as set forth by the applicable carrier(s).
Signature of Company Officer:
Date:
Name (print): Title (print):
Producer Statement (must be completed for commissions)
Producer Statement (must be completed for commissions)
Date: Date:
Producer’s Signature: Producer’s Signature:
Producer’s Name (print): Producer’s Name (print):
Federal Tax ID or SSN: Federal Tax ID or SSN:
Company Name: Company Name:
Address: Address:
City: City:
State: Zip: State: Zip:
Telephone: Fax: Telephone: Fax:
E-mail: E-mail:
Make commissions payable to: Producer Agency Make commissions payable to: Producer Agency
Multiple producer split: : Yes No Multiple producer split: : Yes No
Percentage of split: % Percentage of split: %

Page 4 of 6 CPF-020 04/13
GROUP MASTER APPLICATION COMPENSATION DISCLOSURE INSERT
Your insurance or benefits advisor can offer you advice and guidance as you select the policy and provider most appropriate for your needs. At Unum we recognize the important role these professionals play in the sale of our products and services and offer them a variety of compensation programs. Your advisor can provide you with information about these programs as well as those available from other providers. We support disclosure of broker compensation so that customers can make an informed buying decision. Unless you have agreed in writing to compensate the broker differently, Unum provides Base Commissions to all brokers in connection with the sale of an insurance policy. Base commissions are a fixed percentage of the policy premium, and include and one time, first year flat amount for each policy sold. Base Commissions are paid by Unum to your broker as long as they remain the broker of record on your policy; however, in some circumstances your broker or record may continue to receive commissions on eligible business for a fixed period of time, even after a broker of record change has occurred. A broker may also qualify for Supplemental Commissions paid by Unum. For group insurance products, Supplemental Commissions may be paid in an amount equal to a fixed percentage of total eligible insurance premiums. The Supplemental Commission percentage may range from:
• For group life and disability products: 0% to 1.25% of total eligible inforce premiums paid. • For the group critical illness product: 0% to 1.25% of total eligible inforce premiums, 0% to 11% of total eligible
new sales premiums paid and $1 per application for using our laptop enrollment system. The exact Supplemental Commission percentage payable to any broker is based upon the total dollar amount of all group insurance or number of policies that the broker had in force with Unum in the prior calendar year. Supplemental Commissions may be calculated differently for other insurance products. The premium you pay is not impacted whether or not your broker receives Supplemental Commissions. If you would like additional information about the range of compensation programs our company offers for your group insurance policy or any other Unum insurance product, you can find more details at www.unum.com. Should you have other questions not addressed by the website, including the Supplemental Commission percentage applicable to your broker, or if you want to speak to us directly about broker compensation, please call 1-800-633-7491, option 3. Policyholder Representative Signature: ________________________________________________________ (must be an officer of the company) Print Policyholder Representative Name: _________________________________________________________ Date: ________________________
Unum Use Only Policy No:
Policyholder Name:
Field Office Contact Name:
Field Office Contact Number:
Fax or email to BCS: 423-763-6255 or [email protected] Unum is providing this notice on behalf of the following insuring companies: Unum Life Insurance Company of America, First Unum Life Insurance Company (NY), Provident Life and Accident Insurance Company and provident Life and Casualty Insurance Company (NY). Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries. 1052-05-CA (09/08)
Page 5 of 6 CPF-020 04/13

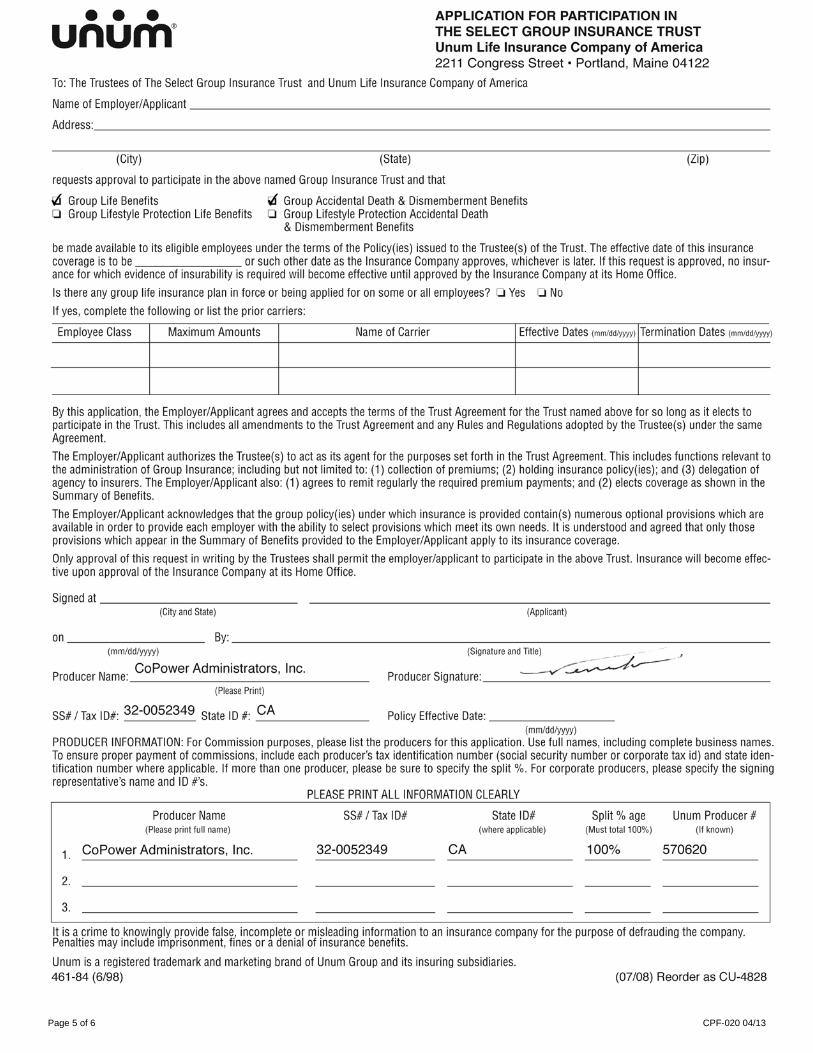
••• unum® APPLICATION FOR GROUP INSURANCE Unum Life Insurance Company of America 2211 Congress Street • Portland, Maine 04122
Name of Applicant - ---------------------------------------
Address:----------- -------------,---------------------(Street)
(City) (State) (Zip)
applies to the Unum Life Insurance Company of America, for:
o Group Life Benefits 0 Group Cancer Benefits o Group Long Term Care Benefits 0 Group Accidental Death
and Dismemberment Benefits o Group Short Term Disabili ty Benefits 0 Group Worksite Short Term Disabili ty Benefits o Group Long Term Disability Benefits
o Tax Qualified* o Non-Tax Qualified** 0 Nursing Home Insurance
o Group Critical Illness Benefits 0 Comprehensive Insurance o Group Accident Benefits
Is there any group life insurance plan in force or being applied for on some or all employees? o Yes o No If yes, complete the following or list the prior carriers:
Employee Class Maximum Amounts Name of Carrier Effective Dates (mmtddtyyyy) Termination Dates (mmtddfWYYJ
If the Insurance Company approves this application, a policy will be issued. The applicant agrees that acceptance of the policy will be an approval of the policy terms. The policy specifications will be made a part of the policy along with a copy of this form.
Signed at---------- --(City and State) {Applicant)
on, _____________ ___ By: ----------------- -------
(mm/ddlyyyy) (Signature and Title)
Broker Name: _______________ _ Broker Signature: ___ __________ _ _ ___ _ (Please Print)
SS# I Tax ID# (last 4 digits): ______ _ Policy Effective Date: _ _ ______ _ (mm/dd/yyyy)
*The contract for Long-Term Care Insurance is intended to be a federally qualified Long-Term Care Insurance contract and may qualify for Federal and State tax benefits .
.. The contract for Long-Term Care Insurance is not intended to be a federally qualified Long-Term Care Insurance contract.
Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries.
AE-1080-CA
Page 6 of 6 CPF-020 04-13
– LTD
CoPower Administrators
2349







