
INTRODUCTION
1. OVERVIEW BLOCK Emergency medicine block will be implemented in semester 7, the fourth year. This block runs for 6 weeks to 5 weeks on and one week for the exams. This block has the burden of six credits. In this block students will learn about the emergency sign, priority sign, the treatment of emergency cases and emergency drugs. Emergency medicine block consists of 5 modules, Traumatology, Respiration, Hemodynamic, Neurology, and Psychiatry with 5 scenario. Each scenario is given within 1 week. It is expected that each student is able to understand and master each learning objective.
The learning strategies that will be used in this block includes the seven jump tutorial discussion, , clinical skill laboratory, lectures , independent study and plenary.
The competency of block taken from the seven area of competency doctor by Indonesian Medical Council: 1. Communication e fektif 2. Basic clinical skills 3. Application of biomedical sciences in medical practice 4. Management of health problems in individuals, families and communities 5. Use of information technology 6. Introspective and life long study7. The application of ethics, morals and professionalism as well as patient safety.
2. LEARNING OBJECTIVES BLOCK a. GENERAL PURPOSE
At the end of this block, students are expected to: 1. Analyzed of Emergency Sign and mark the Priority Sign. 2. Assessment and management of early (initial assessment) in the case of trauma / multiple trauma / psychiatric emergencies in the order of priority (A-B-C) 3. Analyzed the normal organ function and organ failure caused by trauma /
multiple trauma 4. Explain and able to life saving procedures and maintain organ function 5. Analyzed and how to refer patients for definitive therapy
87
6. Explain the legal aspects of trauma and emergency situations b. SPECIAL PURPOSE
1. Explain the national policy in handling emergencies and disasters 2. Analyzing of Emergency Sign and mark the Priority Sign in cases of emergencies and traumatology. 3. Analyzing the failure of organ function due to trauma / multiple trauma 4. Assessment and management of early (initial assessment) in the case of trauma / multiple trauma / drowning in the order of priority (A-B-C) 5. Able to perform life saving procedures in cases of emergency caused by trauma 6. Explain and understand the use of drugs in treating patients with emergency 7. Capable of analyzing and management of vascular injuries 8. Initial examination and management of musculoskeletal trauma 9. Able to explain the symptoms of eye emergencies 10. Explain the legal aspects of trauma and emergency situations
a. Explain the informed consent in emergencies b. Explain how make a visum et repertum
11. Explain the symptoms in the field of pediatric emergency 12. Explain the symptoms of respiratory emergency 13. Explain the mechanisms of airway obstruction in adults 14. Understand and master the handling of emergencies in thoracic trauma 15. Explains emergency in maxillofacial trauma 16. Explaining the symptoms of emergency ENT (Ear Nose Throat) 17. Understand the purpose and indications RJPO action 18. Explain the results of radiological examination thorax and maxillofacial trauma 19. Explain the mechanisms of airway obstruction in adults and the management of
airway obstruction (respiratory resuscitation) 20. Explains emergency obstetrics and gynecology 21. Understanding the signs and symptoms of shock (hypoperfusion) 22. Able to calculate the fluid in the shock and bleeding 23. Explains emergency abdominal surgery and treatment 24. Explain the cardiac emergency 25. Understanding and assessing burns and principles of treatment of burns 26. Explain and capable of handling emergencies on the skin 27. Recognize emergencies at the injury head and the treatment 28. Explain the radiological examination to help establish the diagnosis of head injury 29. Explain a variety of emergencies in the field of neurology and handling 30. Explain the mechanism and management of disorders caused by impairment of consciousness intracerebral 31. Explain and perform how to stabilize the trauma patient transport 32. Describe the action or emergency patient referral management 33. Explains emergency psychiatry and handling 34. Explain the type and management of poisoning
87
35. Explain the gastroenterohepatologi emergency 36. Explain the emergency treatment of metabolic and endocrine 37. Explain the emergency treatment of hypertension and renal 38. Explain the forensic toxicology 39. Able to recognize the signs of death 40. Able to therapy and techniques as well as Cardiac Pulmonary Brain
Resuscitation (RJPO) correctly in adults and children 41. Able to perform an endotracheal tube 42. Able to take the corpus alienum ENT (Ear Nose Throat) 43. Able to make Visum Et Repertum
3. RELATED SCIENCES
1. Cardiology
2. Lung
3. Pediatrics
4. Surgery.
5. Neurology.
6. Ear Nose Throat (ENT).
7. Eye.
8. Skin and Genital
9. Anesthesia
10. Radiology
11. Psychiatry
12. Forensic
4. RELATIONS WITH THE OTHER BLOCKS In studying this block, there are connection with some of the previous block, ie: 1. Block 6 (NBSS) : Neurology, Pediatric, ENT, Eye, Surgery, Psychiatry,
Skin and Genital2. Block 9 (Reproductive System) : Obstetri 3. Block 10 (cardiovascular system) : Interna, Forensic 4. Block 11 (Hematoimunology) : Interna, Forensic 5. Block 12 (Respiratory System) : Interna, Pediatric 6. Block 14 (Gastroinstestinal System) : Interna
87
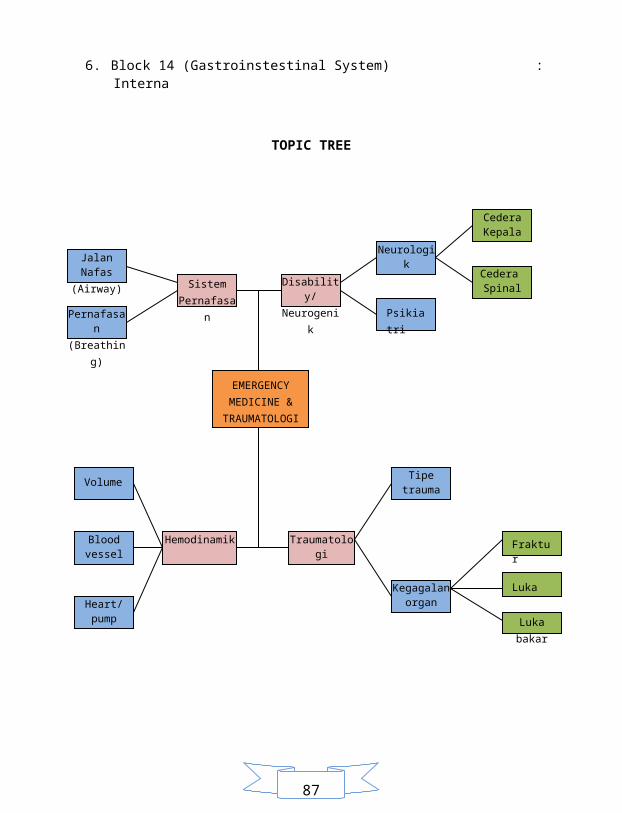
TOPIC TREE
Jalan Nafas(Airway)
Pernafasan(Breathing)
Sistem Pernafasan
Disability/Neurogenik
Neurologik
Psikiatri
Cedera Kepala
Cedera Spinal
EMERGENCY MEDICINE &
TRAUMATOLOGI
Volume
Blood vessel
Heart/pump
Hemodinamik Traumatologi
Tipe trauma
Kegagalan organ
Fraktur
Luka
Luka bakar
87
LEARNING ACTIVITY
A. Tutorial
Discussion tutorial on Emergency medicine there are 5 scenarios for 5 weeks. Each scenario consists of 2 meetings, step 1-5 and step 7. Step 6 independent learning to find answers the learning objectives in the scenarios. Scenario is that many cases occur in general practice or in hospital.
B. Lecture
During this block walk will be done several times face to face with the speakers in the form of lectures. Lectures are given will be tailored to each module each week. The function of college is to structuring the material, explanations are considered difficult subjects, discussion of material not covered in the tutorial, providing a multidisciplinary view of science and integrate knowledge.
C. Laboratory Skill
To train or equip psychomotor theory obtained should be given medical skills training (skills lab). Learning aims to train students to be more skilled in dealing with cases found in general practice.This event was held two sessions or two times with a 2 x 100 minutes for each topic skills. Prior to execution skills will be held pre test lab or home work. For students who pretest value of less than 70 then it will get the assignment from the CSL. The presence of skills lab must be 100%. Skills covered in this block-related emergencies cases (emergency medicine).
D. Plenary
Plenary will be held at 6 weeks. Each topic in the tutorials will be displayed in the plenary by 2-3 groups designated. Plenary aim to equalize students' perceptions about the Learning Objective in the scenario. Attended by pengampu each course / expert. Students can directly ask the experts about what is doubtful or who do not understand.
E. Self Guided Learning.
Students learn to be independent based on the goals and objectives of the scenario blocks, but can be developed based on the recommended references or sources - sources obtained from the internet. Independent learning is the core of competency-based curriculum. Students are required to report the results of their study to the group supervisor who has been appointed in writing. Reporting the results of study done for every module.
87
ASSESSMENT FRAMEWORK
Emergency total value of the end blocks 100%, between the one and the other does not
compensate each other, while the details are as follows : 1. Tutorial : 20% 2. Skills Laboratory : 20% 3. Final Exam : 60%
Tutorials
Assessment tutorial consists of verbal interactions of students during tutorials. Assessed
according to its activity (sharing, ideas, concentration, argumentation, domination, behavior /
manners / attitude, discipline. Students are required to follow tutorials 100%. Components of
the assessment tutorials also include an assessment of the written report guided independent
learning.
Clinical Skills Laboratory
The assessment is conducted every end of the semester by assessing affective, cognitive, and
psychomotor skills. To assess students' ability in mastering medical skills will be held the
Objective Structured Clinical Examination (OSCE).
Final Exam
Block final exam held in week 6 at the end of the block. The number of exam is 150 points
with 1-day exam. Block test score of 50% of overall value. Terms of exam block is at least
80% college attendance.
87
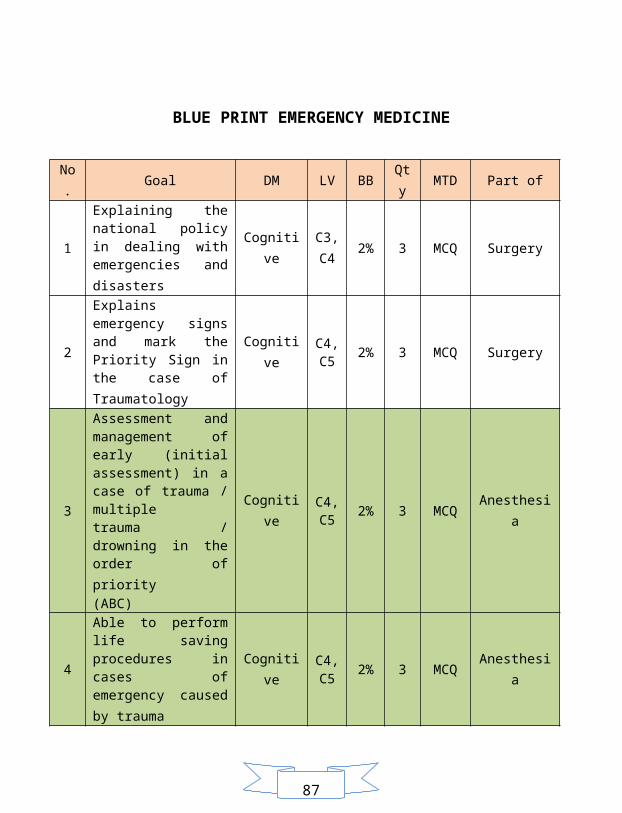
BLUE PRINT EMERGENCY MEDICINE
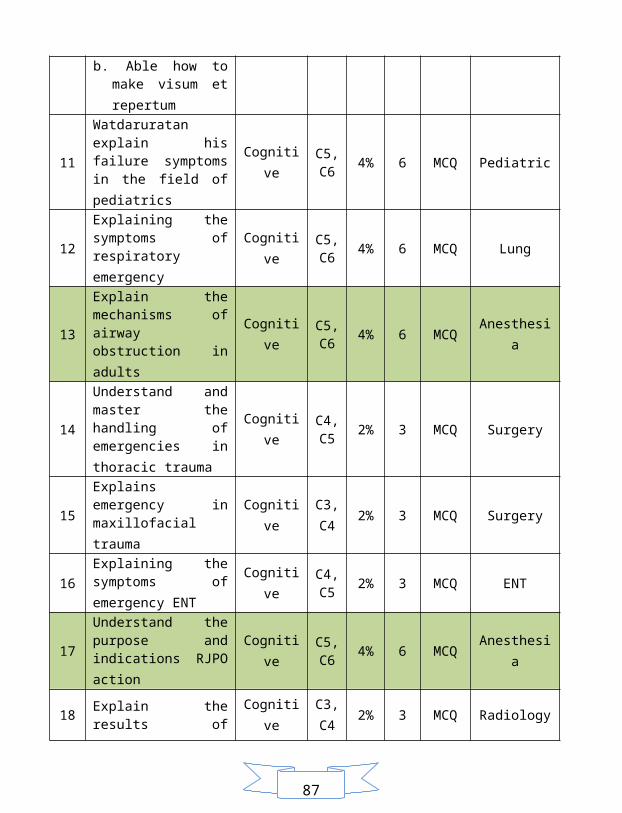
No. Goal DM LV BB Qty MTD Part of
1 Explaining the national policy in dealing with emergencies and disasters
Cognitive C3, C4 2% 3 MCQ Surgery
2 Explains emergency signs and mark the Priority Sign in the case of Traumatology
Cognitive C4, C5 2% 3 MCQ Surgery
3
Assessment and management of early (initial assessment) in a case of trauma / multiple trauma / drowning in the order of priority (ABC)
Cognitive C4, C5 2% 3 MCQ Anesthesia
4 Able to perform life saving procedures in cases of emergency caused by trauma
Cognitive C4, C5 2% 3 MCQ Anesthesia
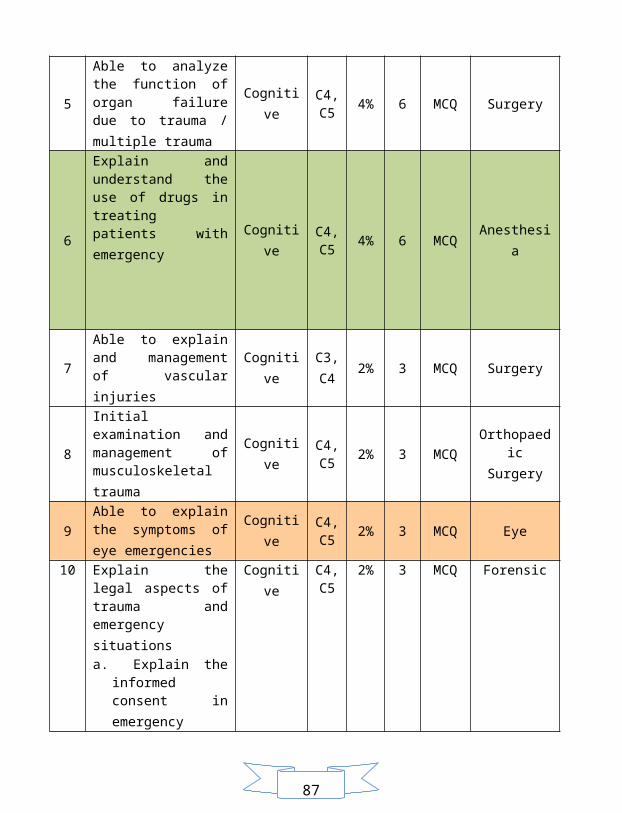
5 Able to analyze the function of organ failure due to trauma / multiple trauma
Cognitive C4, C5 4% 6 MCQ Surgery
6 Explain and understand the use of drugs in treating patients with emergency
Cognitive C4, C5
4% 6 MCQ Anesthesia
87
7 Able to explain and management of vascular injuries
Cognitive C3, C4 2% 3 MCQ Surgery
8 Initial examination and management of musculoskeletal trauma
Cognitive C4, C5 2% 3 MCQ Orthopaedic
Surgery
9 Able to explain the symptoms of eye emergencies
Cognitive C4, C5 2% 3 MCQ Eye
10
Explain the legal aspects of trauma and emergency situations a. Explain the informed
consent in emergency b. Able how to make
visum et repertum
Cognitive C4, C5 2% 3 MCQ Forensic
11 Watdaruratan explain his failure symptoms in the field of pediatrics
Cognitive C5, C6 4% 6 MCQ Pediatric
12 Explaining the symptoms of respiratory emergency
Cognitive C5, C6 4% 6 MCQ Lung
13 Explain the mechanisms of airway obstruction in adults
Cognitive C5, C6 4% 6 MCQ Anesthesia
14 Understand and master the handling of emergencies in thoracic trauma
Cognitive C4, C5 2% 3 MCQ Surgery
15 Explains emergency in maxillofacial trauma Cognitive C3,
C4 2% 3 MCQ Surgery
16 Explaining the symptoms of emergency ENT
Cognitive C4, C5 2% 3 MCQ ENT
17 Understand the purpose and indications RJPO action
Cognitive C5, C6 4% 6 MCQ Anesthesia
87
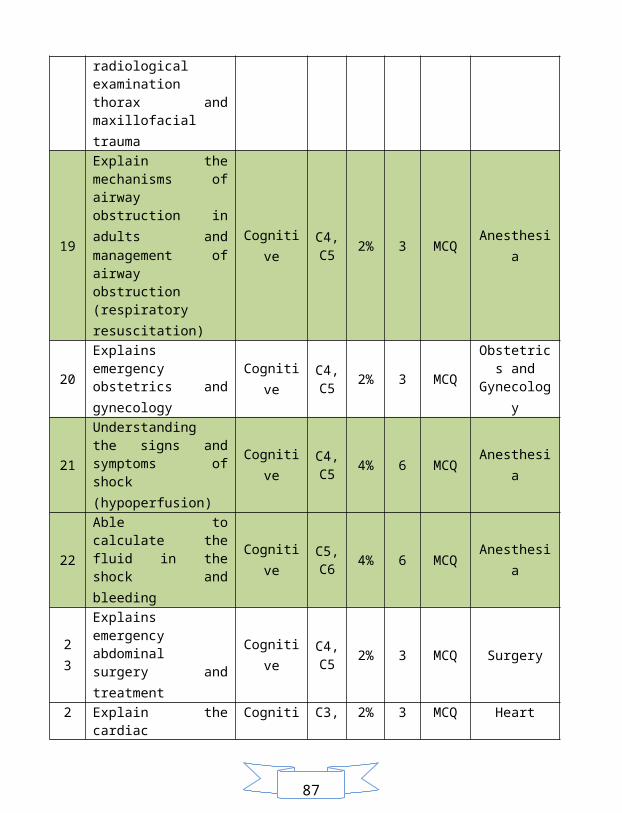
18 Explain the results of radiological examination thorax and maxillofacial trauma
Cognitive C3, C4 2% 3 MCQ Radiology
19
Explain the mechanisms of airway obstruction in adults and management of airway obstruction (respiratory resuscitation)
Cognitive C4, C5 2% 3 MCQ Anesthesia
20 Explains emergency obstetrics and gynecology
Cognitive C4, C5 2% 3 MCQ
Obstetrics and
Gynecology
21 Understanding the signs and symptoms of shock (hypoperfusion)
Cognitive C4, C5 4% 6 MCQ Anesthesia
22 Able to calculate the fluid in the shock and bleeding
Cognitive C5, C6 4% 6 MCQ Anesthesia
2 3 Explains emergency abdominal surgery and treatment
Cognitive C4, C5 2% 3 MCQ Surgery
2 4 Explain the cardiac emergency Cognitive C3,
C4 2% 3 MCQ Heart
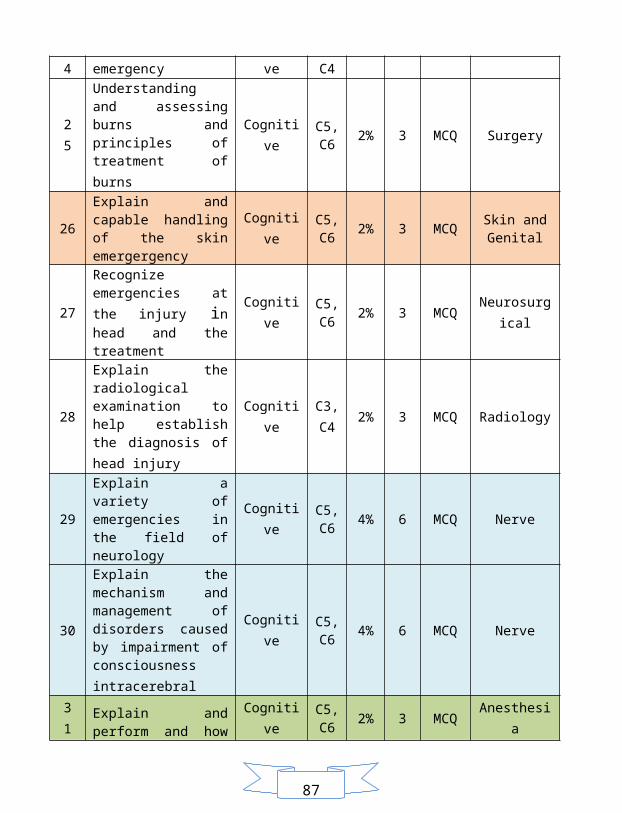
2 5 Understanding and assessing burns and principles of treatment of burns
Cognitive C5, C6 2% 3 MCQ Surgery
26 Explain and capable handling of the skin emergergency
Cognitive C5, C6 2% 3 MCQ Skin and
Genital
27 Recognize emergencies at the injury in head and the treatment
Cognitive C5, C6 2% 3 MCQ Neurosurgica
l
28 Explain the radiological examination to help establish the diagnosis of head injury
Cognitive C3, C4 2% 3 MCQ Radiology
29 Explain a variety of Cognitive C5, 4% 6 MCQ Nerve
87
emergencies in the field of neurology C6
30
Explain the mechanism and management of disorders caused by impairment of consciousness intracerebral
Cognitive C5, C6 4% 6 MCQ Nerve
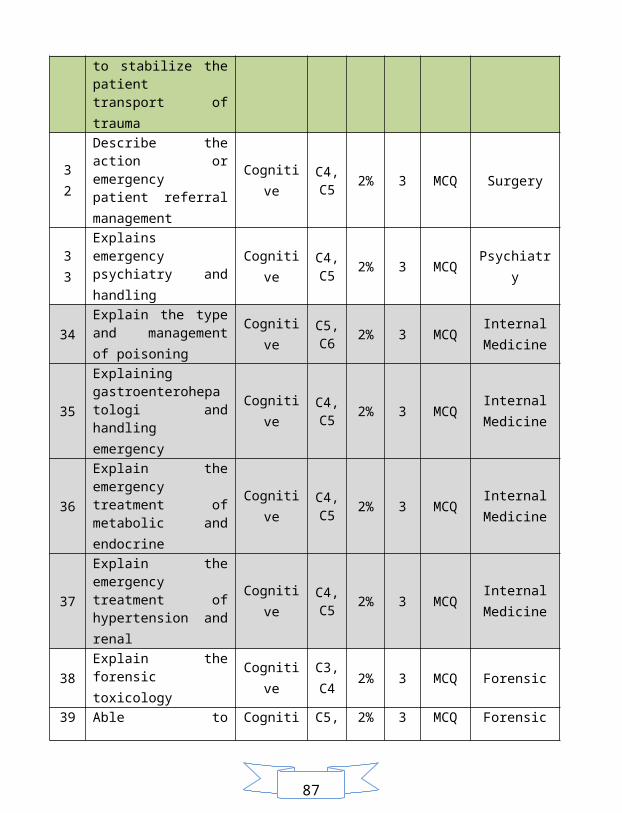
3 1 Explain and perform and how to stabilize the patient transport of trauma
Cognitive C5, C6 2% 3 MCQ Anesthesia
3 2 Describe the action or emergency patient referral management
Cognitive C4, C5 2% 3 MCQ Surgery
3 3 Explains emergency psychiatry and handling Cognitive C4,
C5 2% 3 MCQ Psychiatry
34 Explain the type and management of poisoning
Cognitive C5, C6 2% 3 MCQ Internal
Medicine
35 Explaining gastroenterohepatologi and handling emergency
Cognitive C4, C5 2% 3 MCQ Internal
Medicine
36 Explain the emergency treatment of metabolic and endocrine
Cognitive C4, C5 2% 3 MCQ Internal
Medicine
37 Explain the emergency treatment of hypertension and renal
Cognitive C4, C5 2% 3 MCQ Internal
Medicine
38 Explain the forensic toxicology Cognitive C3,
C4 2% 3 MCQ Forensic
39 Able to recognize the signs of death Cognitive C5,
C6 2% 3 MCQ Forensic
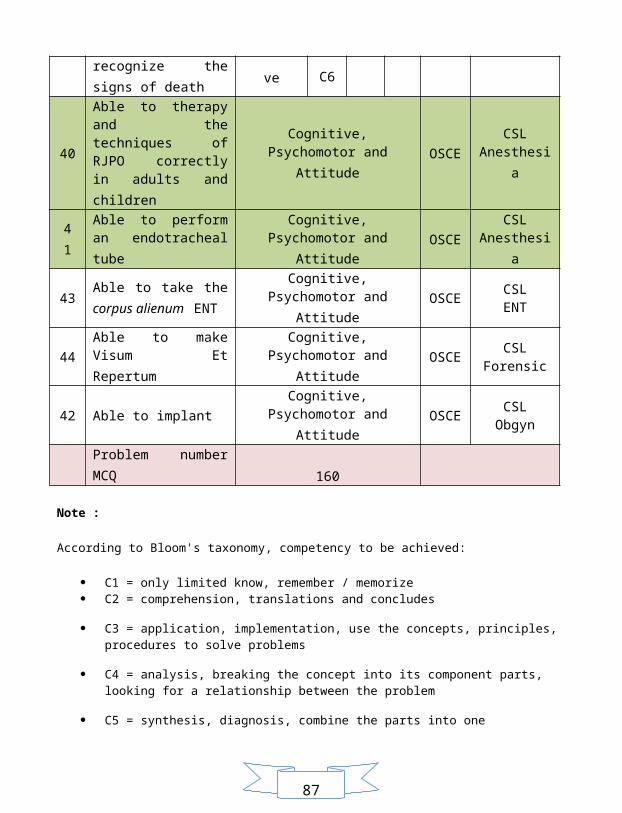
40 Able to therapy and the techniques of RJPO correctly in adults and children
Cognitive, Psychomotor and Attitude OSCE CSL
Anesthesia
4 1 Able to perform an endotracheal tube
Cognitive, Psychomotor and Attitude OSCE CSL
Anesthesia
87
43 Able to take the corpus alienum ENT
Cognitive, Psychomotor and Attitude OSCE CSL
ENT
44 Able to make Visum Et Repertum
Cognitive, Psychomotor and Attitude OSCE CSL
Forensic
42 Able to implantCognitive, Psychomotor and
Attitude OSCE CSL Obgyn
Problem number MCQ 160
Note :
According to Bloom's taxonomy, competency to be achieved:
C1 = only limited know, remember / memorize C2 = comprehension, translations and concludes
C3 = application, implementation, use the concepts, principles, procedures to solve problems
C4 = analysis, breaking the concept into its component parts, looking for a relationship between the problem
C5 = synthesis, diagnosis, combine the parts into one
C6 = evaluation, comparing the values, ideas, methods with a standard SOP
87
REFERENCES
Surgery:
Dr.dr. Iskandar Japardi, SpBS. 2004.Head Injury. Jakarta :EGC
Schwartz.2000. Digest Principles of Surgery. Edition 6th. Jakarta:EGC
A. Graham Apley, 1993.Apley's System of Orthopaedics and Fractures. Seven
Edition. UK.
Sabiston. 2004. Textbook of Surgery Teaching Science 1. Jakarta :EGC
Obstetri and Ginekologi :
Sastrawinata, Sulaiman. 1981.. Edition 1 Bandung : Ellstar Offset.Medicine faculty
of .Unpad
Sastrawinata , Sulaiman Prof,et.al. 2004. Obstetrics Patology. Edition 2.Jakarta :Publisher
EGC.
Sastrawinata, Sulaiman. 1981. Gynecology. Edition 1 Bandung : Ellstar Offset. Medicine
faculty of Unpad
Sarwono Prawirohardjo.1991. Obstetrics and Gynecology.Third Edition. Jakarta: Yayasan
Bina Pustaka
Cunningham, F.Gary [et.al].2006. Obstetri Williams. Volume 1.Edition 21. Jakarta :
EGC.
Supono, Obstetrics Physiology.2004.Department of Obstetri and Gynekology Palembang
Hospital Teaching. Medical Faculty of Sriwijaya University.
87
Interna :
Sudoyo AW, Setiyohadi B, Alwi I, et.al. 2006. Interna. Ed 4. Jakarta. Medical Faculty of
Indonesia University.
Anesthesia :
Anestesiologi.2004. Jakarta: Medical Faculty of Indonesia University.
Eye :
Prof Sidarta Ilyas.2004. Science of Eye. Third Edition.
Daniel G Vaughan.2000. General Ophthalmology. Edition 14. Jakarta: Widyamedika
dr. Nana Wijaya. 1993.Science of Eye. Jakarta ; Gaya Baru.
Prof Sidarta Ilyas . 2004.Atlas Science of Eye. Jakarta :
ENT :
Prof. Dr. Efiaty Arsyad Soepardi, SpTHT (K) et.al. 2003. Ear Nose Throat Head and
Neck. Edition 5th. Jakarta: Medical Faculty of Indonesia University.
Adams Boies Higler. 1997. BOEIS, ENT Disease Text Boks. Edition 6. Jakarta : EGC.
Skin and Genital :
Prof.Dr. R.S.Siregar,Sp.KK,. 2004. Illustrated Atlas of Skin. Edition 2. Jakarta; EGC.
87
Prof.Dr. dr. Adhi Djuanda , et al. 2002.Skin Disease. First Edition. Jakarta: Balai Medical
Faculty of Indonesia University.
Radiology :
Sjahriar Rasad.2002. Radiology Diagnostic. Edition Kedua. Jakarta: Medical Faculty of
Indonesia University
ATLAS Radiology.2000. Jakarta: Medical Faculty of Indonesia University.
Forensik :
Textbook of forensik dan medikolegal FK Unair, de Majo
Medical Faculty of Indonesia University .Forensic Science.2004. Jakarta : Medical
Faculty of Indonesia University
Pyshciatryc:
Dr. Rusdi Maslim.2002. Diagnostic of mental disorder. PPDGJ-III. Jakarta.
Neurology:
Adam Victor.2000.Principal of Neurology. Jakarta :EGC
Prof.Dr. Mahar Mardjono.2005. Basic of Clinical Neurology. Jakarta :EGC
Richard S. Snell.2006. Clinical Neuroanatomy. Jakarta :EGC
Pediatric:
87
Lecturer of Medical Faculty of Indonesia University. 1998.Pediatric..Jakarta ; Info
Medika Jakarta.
Prof.Dr.Coory S. Matondang dkk, Physical Diagnosis in Children
87
MODUL 1 Traumatology
CHAPTER I. THE FIRST WEEK LEARNING OBJECTIVES
Students are able to : 1. Explaining the national policy in dealing with emergencies and disasters 2. Analyzed the Emergency Sign and mark the Priority Sign in case of emergencies and Traumatology. 3. Assessment and management of early (initial assessment) in the case of trauma / multiple trauma / drowning in the order of priority (A-B-C) 4. Analyzing the failure of organ function due to trauma / multiple trauma 5. Able to perform life saving procedures in cases of emergency caused by the trauma /multiple trauma 6. Explain and understand the use of drugs in treating patients with emergency 7. Capable of analyzing t Rauma handling and management of vascular injuries 8. Explain the hemodynamic emergency9. Initial examination and management of musculoskeletal trauma 10.Explain the legal aspects of trauma and emergency situations
a. Explain the informed consent in emergencies b. Explain how to make a visum et repertum
Expert lecture:
A. Surgery Lecture 1 by dr. Yuzar Harun, Sp. B a. Introduction of emergency block (20 minutes) b. Explaining the national policy in dealing with emergencies and disasters (40 minutes) c. Analyze the failure of organ function due to trauma / multiple trauma (40 minutes) Lecture 2 by dr. Pirma Hutauruk, Sp. B a. Capable of analyzing handling and management of vascular injury traumatology
(50 minutes) Lecture 3 by dr. Aswedi Putra, Sp. OT / dr. Eddy Marudut S, Sp.OT a. Initial examination and management of musculoskeletal trauma (100 minutes)
87
2. Anesthesia Lecture 1 by dr. Achmad Assegaf, Sp. An a. Analyze the Emergency Sign and mark the Priority Sign in case of emergencies
Traumatology. (50 minutes) b. Assessment and management of early (initial assessment) in the case of trauma /
multiple trauma / drowning in the order of priority (A-B-C) (50 minutes) Lecture 2 by dr. Achmad Assegaf, Sp. An a. Explain and understand the use of drugs in dealing with emergency patients (100
minutes) 3. Forensic
Lecture 1 by dr. Evi Diana, Sp. F a. Explain the legal aspects of trauma and emergency situations (informed consent in
emergencies) (50 minutes) b. Visum et repertum (50 minutes)
4. Eye Lecture 1 by dr. Helmi Muchtar, Sp. M Able to explain the symptoms of eye emergencies (100 minutes)
Tutorial Scenario 1
Skill Lab: Visum Et Repertum
87
CHAPTER II. SCENARIO 1
EARTHQUAKE VICTIMS
A boy of 16 years was brought to the Emergency Unit immediately after he had removed from
the rubble by an earthquake 6.7 Richter scale. The patient is awake, looking pale. He felt pain
in right thigh. On physical examination found deformity in the right thigh, visible bone
protruding through the skin which causes the wound in the right thigh 10 cm with a fair amount
of bleeding., Right leg look shorter, and the patient can not lift his right leg.
87
CHAPTER III. REVIEW REFERENCES
S CENARIO 1: EARTHQUAKE VICTIMS A. National policy in dealing with emergencies and disasters:
Set in integrated emergency response system, include: a. Ordinary people: the common people have to master the skills of basic life support b. Emergency communication system: 110 police, 113 fire, ambulance 118 c. Support systems (fire brigade, police, Red Cross): trained as a medical first responder d. Pre-hospital emergency ambulance, there are three types:
- Basic types : Able to perform the procedure ABCD - Paramedic Type: ABCD + invasive measures (intubation, lung puncture, infusion,
drugs) - Type of motorcycle is equipped with equipment and medicine, but without a
stretcher e. 24-hour emergency unitf. Disaster plan and training
2. Emergency and priority signs Symptoms and signs in medical emergencies : Symptoms and signs in medical emergencies is very diverse, distinctive and not typical. Abnormal changes of the patient's vital signs are lead to medical emergencies. Some things that can be observed suspicion in patients who directs us to a problem medical is: Symptoms: Fever Painful Nausea, vomiting Excessive urination, or not at all Dizziness, feeling faint, was coming to an end Shortness of breath or have difficulty Excessive thirst or hunger, a strange taste in mouth
Sign: Changes in mental status (unconscious, confused) Changes in heart rhythm; fast or very slow pulse, irregular, weak or very strong
87
Changes in respiratory, rhythm and quality of the mucous membrane color (pale, bluish, red too) Changes in skin condition: temperature, humidity, excessive sweating, extremely dry, including discoloration of the mucous membranes (pale, bluish, red too) Changes in blood pressure Bead eyes: very large or very small Typical odor of the mouth or nose Abnormal muscle activity such as seizures or paralysis Gastrointestinal disorders: nausea, vomiting or diarrhea Sign - Other signs that should not exist Think of all patient complaints are true. If the patient feel bad or uncomfortable it is
treated as a medical case
Triage: Triage is the process of sorting patients by severity of specific injuries or illnesses (based on the most likely to experience clinical deterioration soon) to determine the priority of the medical emergency treatment and transportation priorities (based on availability of the means for action).
Tagging and grouping based triage Priority Zero (Black): Patient death or fatal injury may be obvious and not resuscitated First Priority (Red): Patients severe injuries that require rapid assessment and medical actions and transport immediately to stay alive (eg, respiratory failure, torako-abdominal injury, head injury or facial maksilo-weight, shock or severe bleeding, severe burns) Priority Two (Yellow): The patient needs help, but with a less severe injury and certainly will not experience life threat in the near future. Patients may experience an injury in a broad range of species (eg, abdominal injuries without shock, chest injury without respiratory disorders, major fractures without shock, head injury or cervical spine is not weight, and minor burns) Third Priority (Green): Patients degan minor injuries that do not require immediate stabilization, requiring simple first aid but require periodic reassessment (soft tissue injuries, fractures and dislocations of the extremities, facial injuries, maksilo without airway disorders, and psychological emergency) Priority Four (Blue): the first group of victims with injuries or critical and potentially fatal penyaki which means do not require action and transport, and
87
Priority Five (White): the first group is definitely dead.
3. Initial management of trauma cases : The initial assessment is done on the case, of course, related to the patient's vital signs including blood pressure, pulse, respiration and body temperature, and status consciousness. Further assessment associated with trauma to the patient's condition. In this case the patient suffered an open fracture of the assessment is : A. Inspection (look)
The presence of deformity (deformity) such as swelling, shortening, rotation, angulation, bone fragments (open fracture).
2. Palpation (feel) Presence of tenderness (tenderness), crepitus, neurological and vascular status examination in the distal fracture. Palpation of the extremity the fracture, the injury involves the distal arterial pulsation, skin color, capillary refill test.
3. Movement (moving) The existence of limited motion in the fracture area.
Physical examination of the case? Obtaining a thorough history of the mechanism of injury may help identify orthopedic injuries. For example, past medical history, medications, and previous injury.
4. Life saving procedures in cases of emergency Basic life support INDICATIONS A. Stop breathing
Stop breathing characterized by the absence of chest movement and breathing the air flow from the victim / patient. Stop breathing is a case that should be taken Basic Life Support.
2. Stop cardiac
87
In the event of cardiac arrest, it will happen immediately stop the circulation. Stopping the circulation of these will quickly lead to brain and vital organs of oxygen deficiency. Troubled breathing (wheezing) is an early sign of impending cardiac arrest.
Cardiac pulmonary resuscitation consists of two stages, namely: Survey of Primary (Primary Survey), which can be done by everyone Secondary Survey (Secondary Survey), which can only be performed by trained
medical and paramedical personnel and is a continuation of the primary survey.
PRIMARY SURVEY In the primary survey focused on breathing assistance and help with circulation and defibrillation. To be able to remember easily the primary survey measures formulated by the alphabet A, B, C, and D, namely A = airway (airway) B = breathing (breathing assistance) C = circulation (circulatory assistance) D = defibrilation (electrical therapy)
A (Airway) Airway After completing the basic procedure, followed by action: 1. Examination of the airway. 2. Open the airway.
B (Breathing) Support of breath Consists of two stages: 1. Ensure victim / patient is not breathing.
By looking upward movement turunnva chest, listening for breath sounds and feel the breath of the victim / patient
2. Provide breathing assistance.
87
If the victim / patient is not breathing, breath support can dilakukkan through word of mouth, nose or mouth to mouth to a stoma (hole made in the throat)
C (Circulation) Help circulation Consists of two stages: 1. Ascertain whether the heart rate of victims / patients.
Whether or not heartbeat victim / patient can be determined by palpating the carotid artery in the neck area victim / patient.
2. Provide help circulation. If it has been confirmed no heartbeat, then they could be assisted circulation or the so-called external cardiac compression, performed with the following techniques:
D (DEFIBRILATION) Defibrilation or in the Indonesian language translated by the term defibrillation is to provide a therapeutic electrical energy. This is done if the causes of cardiac arrest (cardiac arrest) is an abnormal heart rhythm called ventricular fibrillation. In the present is already available tools to Defibrillation (defibrillator) which can be used by lay people, called Automatic External Defibrilation, where the tool can find victims of cardiac arrest defibrillation should be performed or not, if necessary defibrillation device can give the signal to rescuers to perform defibrillation or continuing help breathing and circulation assistance only.
5. Drugs in patients with emergency : Resuscitation drugs Vasopressin : Adrenaline, dobutamine, dopamine Anti-arrhythmia drugs Other : Atropine, calcium Route of administration : Peripheral veins, central veins, Intracardia, trachea, intraosseous
6. Types of fractures and wounds Fractures Definition:
87
Fractures (broken bones) is a breakdown of the continuity of the bone structure and is determined according to the type and extent. (Smeltzer SC & Bare BG, 2001)
Types of fractures: To be more systematic, the type of fracture can be divided by: Location
Bone fractures can occur in anywhere like on diafisis, metaphysical, epiphyseal, or intraartikuler. If the fracture is obtained in conjunction with dislocation of joints, it is called a fracture dislocation.
Wide Divided into a complete fracture (complete) and incomplete (incomplete). Example is an incomplete fracture of the crack.
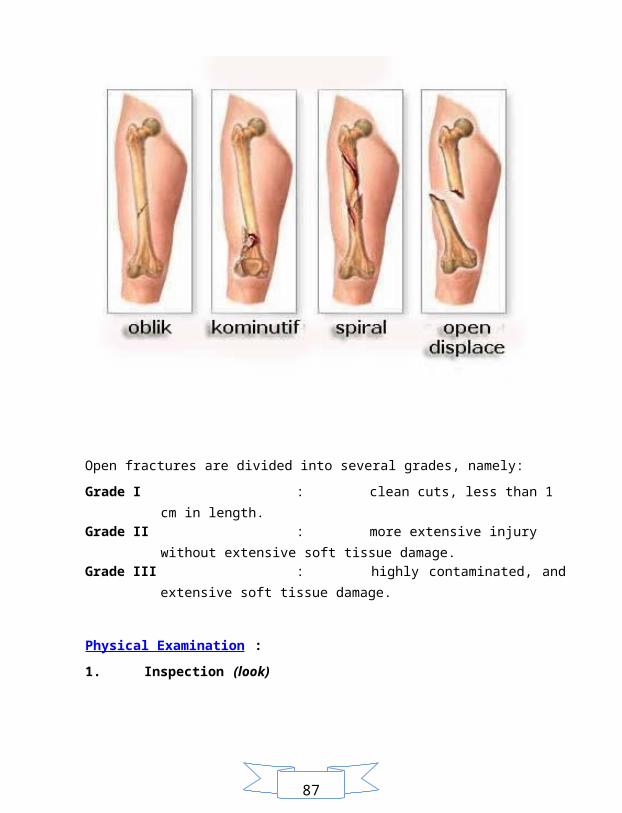
Configuration Judging from the line frakturnya, can be divided into transverse (horizontal), oblique (angled), or spiral (spiral / twist the stem around the bone). If more than one fracture line, then called kominutif, if one part broken while the other side of the bend is called greenstick. Fracture with fragments driven into the (often occurs in the skull and facial bones) is called depression, have a compression fracture where the bone (occurs in the spine) is called compression.
Relationship between the fracture Between the fracture can still relate (undisplaced) or far apart (displaced).
The relationship between fracture with surrounding tissue Fractures can be divided into an open fracture (if there is a relationship between bone and the outside world) or a closed fracture (if there is no relationship between the fracture and the outside world).
87
Open fractures are divided into several grades, namely: Grade I : clean cuts, less than 1 cm in length. Grade II : more extensive injury without extensive soft tissue damage. Grade III : highly contaminated, and extensive soft tissue damage.
Physical Examination : 1. Inspection (look)
The presence of deformity (deformity) such as swelling, shortening, rotation, angulation, bone fragments (open fracture).
2. Palpation (feel) Presence of tenderness (tenderness), crepitus, neurological and vascular status examination in the distal fracture. Palpation of the extremity the fracture, the injury involves the distal arterial pulsation, skin color, capillary refill test.
3. Movement (moving)
87
The existence of limited motion in the fracture area.
Examination Support: 1. Radiologic examination (x-rays), in areas suspected fracture, must follow the
rules of the role of two, consisting of: Includes two images are anteroposterior (AP) and lateral. Contains two fractures of the joints between the proximal and distal parts. Contains two extremity (especially in children), both the injured and those
not exposed to injury (to compare with normal) Performed twice, namely before and after the action action.
2. Laboratory examinations, including : Routine blood, Blood clotting factors, Blood type (especially if the surgery will be performed), Urinalysis, Creatinine (muscle trauma may increase the burden of creatinine for renal
clearance). Arteriography examination performed if suspicion of vascular damage caused by the fracture.
Complications: The cause of fracture complications in general can be divided into two, namely because of the trauma itself, could also be due to the handling of the fracture is called iatrogenic complications.
Definition of Injury Wound is a state of loss / breakdown of the continuity of the network (Mansjoer, 2000:396). According In ETNA, injury is an injury to the tissue that interferes with normal cellular processes, the wound can be described by the damage to the kuntinuitas / unity of body tissue that is usually accompanied by loss of tissue substance.
Classification of Wounds Wound distinguished by:
87
1) Based on the causes a) Excoriation or abrasion b) Vulnus scisum or cuts c) Vulnus laseratum or wound d) Vulnus punctum or stab wounds e) Vulnus morsum or animal bites f) Vulnus combotio or burns
2) Based on the presence / absence of tissue loss a) Excoriation b) Skin avulsion c) Skin loss
3) Based on the degree of contamination a) Clean cuts
a) The cut elective b) Sterile, potentially infected c) There is no k ontak the oropharynx, espiratorius tract, tract elimentarius,
genitourinarius tract. b) Clean cuts tercema r
a) The cut elective b) Potential infection: minimal spillage, normal flora c) Contact with the oropharynx, respiratory, and genitourinarius elimentarius d) Longer healing process
c) Contaminated wounds a) Potential infection: spillage of elimentarius tract, gall bladder, genito
urinary tract, urine b) The new trauma injuries: lacerations, open fractures, penetrating wounds.
d) Dirty wounds a) As a result of the surgery is highly contaminated b) Visceral perforation, abscess, old trauma.
Type of wound healing There are three types of wound healing, where the division is characterized by the number of the lost tissue.
87
1) Primary Intention Healing (primary wound healing) that is the healing that occurs immediately after the attempted bertautnya wound edges usually with stitches.
2) Secondary Intention Healing (Secondary wound healing) is a wound that does not have a primary healing. This type is characterized by the presence of extensive injury and loss of tissue in large numbers. The healing process occurs more complex and longer. Wounds of this type are usually kept open.
3) Tertiary Intention Healing (Tertiary wound healing) that is wound was left open for a few days after debridement action. Once believed to be clean, the wound edges (4-7 days). This wound is the last type of wound healing (Mansjoer,2000:397 ; In ETNA, 2004:4).
Wound Healing Phase
The wound healing process has three phases, namely the inflammatory phase, proliferation and maturation. From one phase to another phase with a continuity that can not be separated.
1) Phase InflammationThis phase appears soon after injury and can continue for 5 days. Inflammation serves to control bleeding, prevent the invasion of bacteria, removing debris from the wound tissue and prepare for continued healing process.
2) Phase ProliferationThis stage lasts from day 6 up to 3 weeks. Fibroblasts (connective tissue cells) have a major role in the proliferative phase.
3) Phase of maturationThis stage lasts from the day 21 and can last for months and ended when the signs of inflammation had disappeared. In this phase there is a wound remodeling is the result of an increase in tissue collagen, collagen breakdown and regression of excess wound vascularity (Mansjoer, 2000:397; InETNA, 2004:1).
Some of the steps that must be considered in cleaning the wound that is:1) Irrigation by as much as possible in order to remove dead tissue and foreign bodies.2) Remove all foreign objects and excision of all dead tissue.3) Give an antiseptic4) If the required actions can be performed by administering a local anesthetic5) If you need to do the closure of the wound (Mansjoer, 2000: 398; 400)
Suturing wounds
87
Clean wounds and are believed not to have an infection and was less than 8 hours may be sewn primer, while the wound is heavily contaminated or not demarcated and should be allowed to recover per sekundam or per tertiam.
Wound closureWound closure is to strive for better environmental conditions in the wound healing process takes place so that optimal.
Consideration dressingConsiderations in the closed dressing and bandage the wound is very dependent on the assessment of the condition of the wound. Serves as a protective dressing to the evaporation, an infection, seek a good environment for wound healing, as fixation and suppression effects that prevent the gathering of blood seepage causing hematoma.
Giving AntibioticsGiving antibiotics to the wound clean principle need not be given antibiotics and the wound is contaminated or dirty it needs to be given antibiotics.
Removal of the stitchesStitches removed when the function is no longer needed. Time of suture removal depends on various factors such as, location, type of appointment of injury, age, health, attitudes of patients and the presence of infection
REFERENCES
Atkinson R S, Hamblin J J, Wright J E C. Shock. In the book: Hand book of Intensive Care. London: Chapman and Hall, 1981; 18-29.Bartholomeusz L, Shock, in the book: Safe Anaesthesia, 1996; 408-413Buckley R, Panaro CDA. General principles of fracture care. Available at http://www.emedicine.com/orthoped/byname/General-Principles-of-Fracture-Care.htm. Last Update: July 19, 2007Femur Fractures. Available at: http://medisdankomputer.co.cc/?p=380. Last Update: March 15, 2009
87
Open fracture. Available at http://bedahugm.net/Bedah-Orthopedi/Fraktur-Terbuka.html. Last update: January 8, 2009Fracture. Available at http://bedahugm.net/Bedah-Orthopedi/Fracture.html. Last Update: August 3, 2008.Fracture. Available at http://www.klinikindonesia.com/bedah/fraktur.php. Last update: January 7, 2009Mangunsudirejo RS. Fracture healing, treatment, and complications, book 1. Issue 1. London: 1989Rasjad, C. Introductory book Orthopaedic Surgery ed. III. Yarsif Watampone. Makassar: 2007. pp. 352-489Sjamsuhidajat R, Wim De Jong, Textbook of Surgery, revised ed, EGC. New York: 1998. pp. 1138-96Thijs L G. The Heart in Shock (With Emphasis on Septic Shock). In a collection of papers: Indonesian Symposium On Shock & Critical Care. Jakarta, Indonesia, August 30 - September 1, 1996; 1-4.Wilson R F, ed. Shock. In the book: Manual of Critical Care. 1981; c :1-42.Zimmerman JL, Taylor RW, Dellinger RP, Farmer JC, Diagnosis and Management of Shock, in the book: Fundamental Critical Support. Society of Critical Care Medicine, 1997.
MODULE 2 Emergency of Respiration
CHAPTER I. THE SECOND WEEK LEARNING OBJECTIVES
Students are able to :
87
1. Explain the symptoms in the field of pediatric emergency 2. Explaining the symptoms of respiratory emergency 3. Explain the mechanisms of airway obstruction in adults 4. Understand and master the handling of emergencies in thoracic trauma 5. Explains emergency in maxillofacial trauma 6. Explaining the symptoms of emergency ENT 7. Understand the purpose and indications RJPO action 8. Explain the results of radiological investigations thorax and maxillofacial trauma 9. Explain the mechanisms of airway obstruction in adults and the management of airway obstruction (respiratory resuscitation)
Expert lecture: A. Pediatric
Lecture 1 by dr. Ferdi, Sp. An Emergencies in pediatrics (100 minutes)
2. Surgery Lecture 4 by dr. Yuzar Harun, Sp. B a.Emergencies in thoracic trauma (5 0 minutes) Lecture 5 by dr. Yuzar Harun, Sp. B a.Traumatology maxillofacial (50 minutes)
3. Anesthesia Lecture 3 by dr. Indra Faisal, Sp. An a. Explain the symptoms of respiratory emergency (100 minutes) Lecture 4 by dr. Dendy Maulana, Sp. An b. Explain the mechanisms of airway obstruction in adults and drowning (drowning)
(50 minutes) c. Explain the management of airway obstruction (respiratory resuscitation) (50 minutes)
Lecture 5 by dr. Undang Komarudin, Sp. An Understand the objectives and actions Cardiac Pulmonary Brain Resuscitation (RJPO) (100 minutes)
4. ENT (Ear, Nose, Throat)
Lecture 1 by dr. Fatah Satya W, Sp. ENT
87
a. Emergencies in ENT (100 minutes)
5. Radiology Lecture 1 by dr. Karyanto, Sp. Rad a. Explain the results of radiological examination and maxillofacial trauma of the thorax
(100 minutes)
Tutorial Scenario 2
Skill lab Cardiac Pulmonary Brain Resuscitation (RJPO) in children and adults / Traumatology Advanced Life Support (ATLS)
87
CHAPTER II. SCENARIO 2
FACES TRAUMA
A boy aged 8 years was brought to the Emergency Unit after an accident. He bounced from the
host and his bike hit the pavement and the bottle containing the liquid battery rupture and the
liquid is brought about him. Conscious patient, suffering from facial and jaw injuries are very
severe, the patient also look crowded. On physical examination the doctor found the patient's
difficulty answering the question being asked by a doctor because of the deformity on the right
cheek and out of the mouth and nose bleeding.
87
CHAPTER III. REVIEW REFERENCES
S CENARIO 2: FACES TRAUMA A. Initial assessment on facial trauma
Assessment on Face Trauma A history of trauma to the face Ample use of acronyms in the evaluation of facial trauma patient (allergies, medications, past history, last meal, events surrounding the accident) can facilitate a history of trauma with lengkap.3 Acronyms can also be used if the trauma of threatened jiwa.4 Ask specific questions about trauma: Mechanism of trauma Whether the patient had lost consciousness Does the patient have vision problems such as double or blurred vision Is dental patients can normally closed (normal occlusion) Whether the patient can bite without pain Does the patient possess an area that feels numbness or tingling in the face In women, ask if the trauma is derived from a partner or a person being under threat In children, ask the same thing as the woman to menenetukan whether there is violence on children. Deformities of the face looks Swelling, asymmetry, oblique, with skin abrasions to the soft tissue injury Hematoma or bleeding in the wound or the mouth of the hole gidung and as a way out bleeding from the maxillary sinus / fracture Physical examination Examination of systematic head and face can be the starting point and is done in a consistent treatment to prevent checks being let loose. In patients with acute facial trauma, physical examination can be disrupted by the swelling of the face. Secondary asymmetrical facial appearance of the fracture can usually be hidden. 3 Check for tenderness, crepitus (without a strong emphasis for flat bones), "step in" or discontinuity edge orbital bone and bone madibula rhyme. Check as well as the right and the left side and compare. 2 Examiner carefully assessed for neurological deficits, including facial trigeminal nerve and facial. Sensory disturbances in the forehead, cheeks, and lower lip. Lacerations,
87
contusions, and abrasions of the skin can focus the examiner to indicate parts that have a risk of nerve injury. 3 Complete eye examination includes evaluation of a history of eye disease, visual acuity, perception of light and red light, ocular motility, pupil assessment, and examination of the conjunctiva and eyelids. Long-term morbidity in facial fractures are the most associated with ocular and orbital damage. 3 Hipestesia the second nostril Cheeks bulge disappeared 2 Examination of the oral cavity particularly important in patients who mehilangan teeth, bone fragments, or foreign body when there is trauma. Identification and removal of prosthetic oral cavity needs to be done. Occlusion and interkuspasi carefully done because both mandibular and maxillary fractures can result in malocclusion. 3 In the oral cavity appears occlusion disorders (malocclusion) that bulge premolars are not met with the hollow tooth opponent / partner, can also appear gingival laceration fracture area, maxilla are sometimes found floating in the hematoma (floating maxilla)
Maxillofacial Trauma and classification Maxillofacial trauma can be classified into two parts, the hard tissue facial trauma and facial soft tissue trauma. Maxillofacial trauma to the tissue can include soft tissue and hard tissue. The meaning of facial soft tissue is soft tissue that covers the face of hard tissue. While the definition of hard tissue facial bones of the head is composed of 1. Nasal bone 2. Bone arch zigomatikus 3. Mandibular bone 4. Bone / maxillary 5. Eye socket bone 6. Tooth 7. Alveolar bone Le Fort classification used to help diagnose and p treatment : Le Fort I : Limited to the alveolar trauma left, right, or bilateral. Le Fort II : Trauma pyramid os maxillary, nasal, zigoma; occur separation of the center of the face with cranial bone. Le Fort ILI :Trauma of the maxillary bone, nose, zigoma, orbita; place separations
around the bones of the face with a base kranii
87
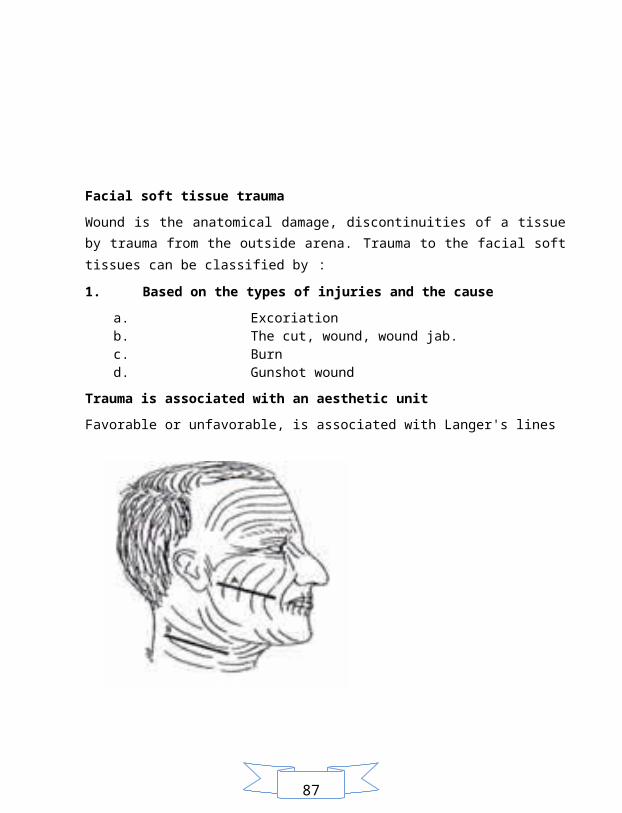
Facial soft tissue trauma Wound is the anatomical damage, discontinuities of a tissue by trauma from the outside arena. Trauma to the facial soft tissues can be classified by : 1. Based on the types of injuries and the cause
a. Excoriation b. The cut, wound, wound jab. c. Burn d. Gunshot wound
Trauma is associated with an aesthetic unit Favorable or unfavorable, is associated with Langer's lines
Figure 1.
A. Laceration that crosses the line of Langer unfavorable cosmetic result in poor healing.
87
B. Facial incision is placed parallel to Langer's lines (Pedersen GW. Practical textbook oral surgery (oral surgery). Rather Purwanto language, Basoeseno. Jakarta: EGC, 1987:226).
2. Maxillofacial trauma Management of facial trauma Primary survey: airway: airway disorders result from direct trauma to the larynx, foreign bodies (including an aspirated tooth and bone fragments), or massive bleeding from the upper airways. Treatment of airway disorders is quite difficult with the trend that 10% of patients had facial trauma and cervical spine trauma. 3 b reathing : It consists of two stages: 1. Ensure the patient / victim is not breathing
By seeing the movement of the chest rise and fall, hear and feel the breath of breath, a technique helper hold the ears and nose above the mouth of the patient / victim while still maintaining the airway remains open. Do no more than 10 seconds
2. Provide breathing assistance Help the breath can be done through word of mouth, mouth to nose, mouth to stoma (a hole made in the throat). Respiratory assistance given by 2 times, each time blowing time from 1.5 to 2 seconds and the volume of 700 ml - 1000 ml (10 ml / kg or until visible chest patients / victims given oxygen mengembang.Konsentrasi 16-17%. Note the patient's response
c irculation : The most important action is to help the circulation of Foreign heart massage. External Cardiac Massage can be done because most of the heart is located between the breastbone and the backbone so that the pressure from the outside can cause effects on the heart pump which was considered sufficient to regulate the blood circulation at least on the state of clinical death .
Secondary survey
87
neck examination, neurological, scalp, orbit, ear, nose, face, middle, mandibular oral cavity, and occlusion. Head injury (brain injury) may delay the timing of the operation of open reduction internal fixation (ORIF) in bone ftraktur face. If there are wounds, covered with moist gauze while awaiting definitive therapy Mandibuka bilateral fracture should be stabilized so as not to interfere with the airway If there is a septal hematoma or hematoma auricula rice, drainage should be performed and followed by a swathe of press / nose tamponade. 2
Advanced Handling Handling information that is in the first week post-trauma. Mandibular fracture: reduction and fixation of the maxillary arch with a wire or bar produced union and the occlusion is achieved within ± 5 weeks. Reduction and screw fixation with mini plates do not require locking teeth as in the wire and arch bar. Fracture of the maxilla: the reduction of the sulcus approach ginggivobucalis and infra cilliar palpebra inferior; can also be fixed with wire or mini screw plate. Rima important orbital fracture repositioning and fixation surgery to restore form and restore the function of orbital motion of the affected eye. Nasal fracture repair should not be too long since the trauma, given the nasal bones are flat and often broken-shaped impression, deviation or crushed.
3. Emergency in thorax trauma Cause of: Airway obstruction, major hemothoraks, cardiac tamponade, pneumothorax persisted. Management of emergency : Determination of injury (penetrating thoracic wall or not) Determination of vital functions (if necessary resuscitation) Cleanup and closure of wounds
Airway obstruction From outside the airway: Foreign
87
From within: The tongue that closes the airway How to deal with obstruction: If the blockage seen taken with a finger or tool to pinch and pull If looks do not blow back or back slaps If the base of the tongue falls backwards doing headt tilt or chin lift.
4. Traumatology in the eyes and treatment
A. Definition Eye trauma is whether or not intentional acts that cause eye injury.
B. The types of eye trauma 1. ACID TRAUMA
Traumatic acid is one type of chemical eye trauma and emergencies including the eyes caused by chemical substances are acidic with a pH <7. Some acids are often the eye is sulfuric acid, acetic acid, hidroflorida, and hydrochloric acid. Proper management of the trauma chemical is irrigated with sterile isotonic saline and check the pH of the ocular surface by putting the indicator in the fornix of a sheaf of papers. Repeat the irrigation if the pH is not located between 7.3 to 7.7. (Vaughan, 2000).
2. BASE TRAUMA
The trauma of alkaline chemicals will give a mild irritation to the eyes when viewed from the outside. However, when seen on the inside of the eye, this trauma resulted in an emergency base. Base will penetrate the cornea, camera oculi anterior, and to the retina quickly, so it ended in blindness. At the base trauma will occur corneal collagen tissue destruction. Coagulation chemicals are alkaline and cell happening persabunan process, accompanied by dehydration. According to the classification Thoft, basa trauma can be divided into :
87
Degree 1 :Conjunctival hyperemia T erjadi accompanied by keratitis pungtata
Degree 2 :Conjunctival hyperemia T erjadi with loss of corneal epithelium
Grade 3 :Occuri conjunctival hyperemia accompanied by necrosis and loss of corneal epithelium
Grade 4 : perilimal conjunctival necrosis by 50% Action if there is trauma to quickly perform basic irrigation with normal saline as long as possible. When irrigation may be done at least 60 minutes after trauma. Patients were given sikloplegia, antibiotics, EDTA to bind bases. EDTA is given after 1 week of trauma base, necessary to neutralize the collagenase which is formed on the seventh day. Complications that can occur is simblefaron, corneal opacification, edema, and neovascularization of the cornea, cataracts, accompanied by ptisis eyeball.
3. Penetrating trauma Is a trauma in which some or all layers of the cornea and sclera have damage. Etiology Occurs due to the entry of foreign objects into the bulbus oculi : Ø Metal : Magnet, the magnet is not Ø Non-metallic Clinical Manifestations - Decreased visual acuity - Low intra-ocular pressure - Iridocornealis shallow angle - Shape and location of the pupil changes - No sightings of the cornea or sclera rupture - Tissue prolapse (off), such as iris, lens, retina - Conjunctival chemosis Management Topical antibiotics, eyes closed, and immediately sent to the eye doctor to do surgery. Systemic antibiotics administered orally or intravenously, anti-tetanus prophylactic, analgesics, and sedatives if necessary. should not be given local steroids and splint should not be pressing the eyeball. Expenditures of foreign objects should be done in a hospital with adequate facilities.
87
4. Blunt trauma 1. Blunt trauma palpebra
A blunt impact could push the eye back to the possibility of damaging the structure on the surface (eyelids, conjunctiva, sclera, cornea and lens) and the structure of the back of the eye (retina and neural). Because palpebra a protective ball when there is trauma to the eye it will do reefleks close. This will cause the occurrence of hematoma palpebra. Hematoma is due discharge of blood from damaged blood vessels in the trauma
2. Blunt trauma to the lens a. Lens dislocation. Lens dislocation occurred in zonula Zinn
which breakup will lead to impaired lens position. b. Lens subluxation. Partly due to rupture so that the lens Zinn
zonula move. c. Luxation Anterior lens. If all the zonula Zinn around the
equator dropped out due to trauma to the lens into the anterior chamber.
d. Luxation Posterior lens. In blunt trauma is hard on the eyes may occur due to rupture the posterior lens luksasi Zinn zonula around the equator of the lens ring so that the lens falls into the glass body and sinking on the plain below the Polus posterior ocular fundus.
e. Traumatic cataract. In the blunt trauma of the anterior subcapsular cataracts will be seen or posterior. Contusion cataract lenses pose like a star, and can also be printed in the form of cataract is called a Vossius ring
3. Blunt trauma to the cornea Corneal abrasion is a state in which the corneal epithelium regardless of which can be caused by blunt trauma, sharp trauma and chemical trauma and foreign bodies subtarsal. And recurrent corneal abrasion can cause extreme pain, which is an emergency corneal abrasion to the eye that can lead to ulceration and edema of the cornea which would disturb the visual acuity
4. Trauma fundus oculi
87
Blunt trauma to the eye can lead to abnormalities in the retina, choroid, and optic nerve. Changes that occur may include retinal edema, retinal hemorrhage, retinal detachment, and optic nerve atrophy. If found patients with blunt trauma and sharp vision that can not be corrected with the glasses, while the clear eyes of the state media, it can be estimated by abnormalities in the fundus or in the back of the eyeball (Ophthalmologist Association of Indonesia, 2002
REFERENCES
Apley and Solomon, Fracture and Joint Injuries in Apley's System of Orthopaedics and Fractures, Seventh Edition, Butterwordh-Heinemann, London, 1993, pp. 499-515. Armis, Principles of Fracture Age Sistema in Musculoskeletal Trauma, FKUGM, London, p: 1-32. Berend ME, Harrelson JM, Feagin JA, Fractures and Dislocation in Sabiston Jr DC, Texbook of Surgery The Biological Basis of Modern Surgical Practice, Fifteenth Edition, WB Saunders Company, Philadelphia, 1997, pp. 1398 to 1400. Carter MA, Anatomy and Physiology of Bone and Joints in Price SA, Wilson LM, Clinical Pathophysiology Concepts of Disease Processes, Book II, issue 4, EGC, Jakarta, 1994, p 1175-80. Dorland, Medical Dictionary, 26th edition, EGC Medical Book Publishers, London, 1996, p 523,638,1119. Rasjad C, in Introduction to Trauma Surgery MDs, Ujung Pandang Lamumpatue Stars, 1998, p: 343-525 Reksoprodjo, S, the set of MDs examination of Surgery Faculty of Medicine Lecture, Publisher Binarupa script, Jakarta, 1995, p: 453-471.
87
Sjamsuhidajat R, Musculoskeletal System in Syamsuhidajat R, de Jong W, Textbook of Surgery, EGC, Jakarta, 1997, p: 1124-128
MODULE 3 Emergency hemodynamic
CHAPTER I. THE THIRD WEEK LEARNING OBJECTIVES
1. Explains emergency obstetrics and gynecology 2. Understanding the signs and symptoms of shock (hypoperfusion) 3. Able to calculate the fluid in the shock and bleeding 4. Explains emergency abdominal surgery and treatment 5. Explain the cardiac emergency 6. Understanding and assessing burns and principles of treatment of burns 7. Know and be able to perform stabilization actions with strict monitoring on burns 8. Explain and capable of handling emergencies on the skin
Expert lecture:
87
1. Obstetrics and Gynecology Lecture 1 by dr. Taufiqurrahman R, Sp. OG a. Emergency Obstetrics and Gynecology (100 minutes)
2. Heart Lecture 1 dr. Asrizal T, Sp. JP a. Emergency heart (100 minutes)
3. Surgery Lecture 5 by dr. Yuzar Harun, Sp. B a. burns, treatment principles, and criteria for inpatient stabilization
and reference (10 0 minutes) Lecture 6 by dr. Pirma Hutauruk, Sp. B a. aspect of emergency abdominal surgery and treatment (100 minutes)
4. Anesthesia lecture 6 by dr. Undang Komarudin, Sp. An
a. Understanding the signs and symptoms of shock (hypoperfusion) (50 minutes) b. Being able to calculate the infusion of fluids in shock and bleeding (50 minutes)
5. Skin and Genital
Lecture 1 by dr. M. Syafei Hamzah, Sp. K K emergency Skin (100 minutes)
Tutorial Scenario 3
Skill lab ETT (Endo tracheal tube)
87
CHAPTER II. SCENARIO 3
STOVE EXPLODES
A woman of 35 years, 8 months pregnant during the antenatal care (ANC) has done regular to a
gynecologist. During the ANC obtained blood pressure 180/100 mmHg, the second leg
swelling.
One day he was taken to the Emergency Unit with burns along his chest and abdomen caused
by the explosion of a stove when she was cooking. Patients are aware of pain in the chest and
abdomen which caught fire. Slightly hoarse voice, his eyebrows on fire. The patient
87
complained of breathlessness and coughing, black sputum. Blisters were found in the chest and
abdomen, but the patient still feels pain.
At the time of the patient's sudden seizure and tension obtained 200/110 mmHg and a weak but
rapid pulse. On examination DJJ 160 x per minute ..
Laboratory results obtained: proteinuri +3.
CHAPTER III. REVIEW REFERENCES
S CENARIO 3: STOVE EXPLODES
1. The principle of treatment of burns and their classification Burn patients should be evaluated systematically. The main priority is to maintain the airway remains patent, effective ventilation and support the systemic circulation. Endotracheal intubation performed in patients suffering from severe burns or suspicion of inhalation injury or burns to the upper airway. Intubation can not be done if there has been a burn edema or fluid resuscitation is too much. In burn patients, intubation and nasotrakea orotrakea preferred over tracheostomy. Treatment of burns resuscitation
87
a. Management of airway resuscitation : 1. Intubation
Intubation action done before the manifestation of mucosal edema causing obstruction. Purpose of intubation to maintain airway and the airway pemelliharaan facilities.
2. Cricothyroidotomy Aiming with intubation only be considered too aggressive and lead to greater morbidity than intubation. Cricothyroidotomy minimize dead space, tidal volume increase, it is easier to do bronchoalveolar rinses and the patient can talk, if compared with intubation.
3. Oxygen administration 100%
Aims to provide the oxygen requirements when there is blocking the airway pathology of oxygen supply. Be careful in giving large doses of oxygen as it can cause oxidative stress, so it will form free radicals that are vasodilator and modulator of sepsis.
4. Airway care 5. Suction secretions (periodic) 6. Inhalation therapy
Aims to seek a better air atmosphere in the airway lumen and liquefy thick secretions so easily removed. Inhalation therapy generally uses liquid sodium chloride 0.9% base plus bronchodilator when necessary. Additionally bias added substances with specific properties such as atropine sulfate (lowering the production of secretions), sodium bicarbonate (to overcome cellular acidosis) and steroids (still controversial)
7. Rinse bronchoalveolar 8. Rehabilitative care for respiration 9. Escharotomy on the wall of the piston which aims to improve lung compliance
b. Management of fluid resuscitation Fluid resuscitation is done by giving replacement fluids. There are several ways to calculate the fluid requirements of this : The way Evans 1. Extensive burns (%) x weight (kg) into mL NaCl per 24 hours 2. Extensive burns (%) x weight (kg) to 24 mL plasma per hour 3. 2,000 cc glucose 5% per 24 hours
87
Half of 1 +2 +3 is given in the first 8 hours. The rest are given in the next 16 hours. On the second day given half the amount of fluid the first day. On the third day be half the amount of fluid the second day.
Baxter Formula
Extensive burns (%) x weight (kg) x 4 mL Half of the amount of fluid given in the first 8 hours. The rest are given in the next 16 hours. On the second day given half the amount of fluid the first day. On the third day be half the amount of fluid the second day.
c. Nutritional resuscitation In burn patients, the enteral feeding should be done early and the patient does not need to be fasted. If the patient is unconscious, then feeding through naso-gastric can tube (NGT). Nutrition provided should contain 10-15% protein, 50-60% carbohydrates and 25-30% fat. Early nutrition can enhance immune function and prevent the atrophy of intestinal villi. It is expected early nutrition can help prevent the occurrence of SIRS and MODS. Treatment of burns Generally to relieve pain from burns used a small dose of morphine intravenously (initial adult dose: 0.1 to 0.2 mg / kg and the 'maintenance' 5-20 mg/70 kg every 4 hours, whereas a dose of children 0.05 to 0.2 mg / kg every 4 hours). But there is also a provision stating methadone (5-10 mg adult dose) every 8 hours is the treatment of chronic pain is good for all adult burn patients. If the patient still feels pain despite the administration of morphine or methadone, benzodiazepines may also be given in addition.
2. Inhalation trauma Trauma can be defined as the inhalation of acute damage to the respiratory system caused by the inhalation of combustion products or vapor where the patient is in a closed room. Region are usually exposed to inhalation trauma is oropharings, tracheobronchial tree or lung parenchyma. Some literature mentions inhalation trauma was found in 3-15% of patients who present with severe burns. The incidence of burns increases with age. With the highest incidence
87
is found in over 59 years and the lowest incidence below the age group 5-14 years. The prevalence of men and women are equal, namely 1: 1. TRAUMA MECHANISM There are two mechanisms of occurrence of inhalation injury, namely carbon monoxide and smoke inhalation. Smoke is divided into two, namely the direct trauma and smoke poisoning. Direct trauma to the respiratory system the most rare cases, some experts conclude that carbon monoxide poisoning is a major cause of inhalation trauma. Carbon monoxide Carbon monoxide gas is a gas that is odorless, colorless and does not cause irritation resulting from incomplete combustion of carbon. Effect of this gas in the tissues causing hypoxia due to carbon monoxide binds to hemoglobin and oxygen and compete with binding to hemoglobin. Affinity for carbon monoxide binds to hemoglobin 200 times more than the oxygen concentration karboksihemoglobin high enough so that even if the concentration of carbon monoxide in the air only 5%. Toxicity of carbon monoxide depends on the concentration in the air and how much exposure to carbon monoxide.
Direct trauma Inhalation of hot, dry air (300 o F or more) caused damage to the tissue in the upper respiratory tract and laryngs. In the edema can arise laryngs laryng, spasm laryngs, and shortness of breath. If there is hot steam vapor will cause damage to the distal part of the respiratory tract.
Toxicity of smoke In addition there are also noxious carbon monoxide gas that is the result of degradation of man-made material, while the nature of the material produced oxidation of sulfur and nitrogen, and aldehydes. One of the aldehyde, acrolein showed irritation of the respiratory tract of the upper and pulmonary edema.
Pathophysiology Direct effects of smoke inhalation on the loss of cilia function and severe mucosal edema. Within a few seconds then it will decrease surfakatan work which will be seen as micro and macro atelectasis. If inhalation trauma severe enough, it will cause damage to the
87
alveoli and the bronchial epithelium which will also spread to the capillary. Which in minutes will be detected as bronchial edema and perivasculer, which will lead to the onset of wheezing due to bronchial obstruction. Ekspetorasi black sputum usually occurs at this time. After several hours, the mucosa of trakeobronkial will begin to form membrane peeling and mucopurulent. At this time the patient will spend sputum and bronchial mucosa contain. Once established it will be followed by pseudomembranous necrotizing bronchiolitis, hyaline membrane formation, intraalveolar perdarhan, fibrin-thrombus formation, and the latter no pulmonary edema.
DIAGNOSIS Diagnosis of inhalation injury on the basis that: 1) Anamnesis
Obtained from the anamnesis causes burns and whether the patient is stuck in the house that tebakar or not. If the patient is stuck in the house then it will increase the likelihood of inhalation trauma. Meanwhile, when the cause of burns due to flames in the room that opens the possibility for the occurrence of inhalation injury is reduced.
2) Examination Examination reveals a black-colored sputum, colored laryngs hita (by examination laryngoskop) is a significant sign of inhalation trauma. As for some additional symptoms, among others, eyebrows and nose hair on fire, a hoarse voice, cough and difficulty breathing.
3) Investigations Several investigations can be done to establish the diagnosis of inhalation injury : a) Chest x-rays b) Blood Gas Analysis c) Bronchoscopy Bronchoscopy is the gold standard examination to confirm the presence of inhalation trauma. At bronchoscopy examination found : Black Hyperemia, bronkorhea Petechial Pink-gray areas of necrosis à White area is flat but sometimes concave
87
MANAGEMENT Treatment for patients with inhalation trauma, namely; 1) Make sure the airway remains free to make endotracheal intubation. If there is a
deep burn on the neck and the body then quickly made incisions to relieve the neck and body.
2) Make sure the ventilation and adequate oxygenation to peripheral regions 3) Fluid resuscitation 4) Pulmonary toilet and bronchodilators 5) Analgosedasi 6) Specific Antidotum
3. Management of shock (hemodynamic) Shock Response Reduction of shock begins with general measures aimed at improving tissue perfusion; improve oxygenation of the body; and maintain body temperature. This action does not depend on the cause of shock. Diagnosis should be established so that it can be a causal treatment. Immediately provide first aid in accordance with the principles of resuscitation ABC. Airway (A = water way) should be free if necessary with the installation of an endotracheal tube. Respiration (B = breathing) should be ensured, if necessary, to provide artificial ventilation and administration of oxygen 100% . Circulatory volume deficit (C = circulation) in true hypovolemic shock or relative hypovolemia (septic shock, neurogenic shock, and anaphylactic shock) should be treated with intravenous fluids and if necessary the provision of inotropic drugs to maintain cardiac function or vasoconstrictor drugs to cope peripheral vasodilatation. Maintain Respiration 1. Clear the airway. Perform exploitation, if any secretions or vomit. 2. Tilted-head prop his chin, if necessary, attach a walker breath (Gudel / oropharingeal
airway). 3. Give oxygen 6 liters / minute 4. If breathing / ventilation is inadequate, give oxygen to the pump lid (Ambu bag) or
ETT.
87
Maintain Circulation Immediately attach an intravenous infusion. Can more than one infusion. Monitor pulse, blood pressure, skin color, the contents of the vein, urine production, and (CVP).
Find and Overcome Cause Bleeding is a common cause of shock in trauma patients, either because of bleeding or bleeding that looks invisible. Visible bleeding, bleeding from wounds, or hematemesis from gastric ulcer. Bleeding is not visible, such as bleeding from the gastrointestinal tract, such as duodenal ulcers, splenic injury, pregnancy outside the uterus, pelvic fractures, and large or multiple fractures.
4. Emergency obstetric A. Abortion
Abortion is spending the products of conception are age less than 20 weeks of pregnancy. The diagnosis is based on the presence of amenorrhea, signs of pregnancy, vaginal bleeding, placental tissue and the possibility of spending fetal death. On septic abortion, vaginal bleeding a lot or moderate fever (chills), possible symptoms of peritoneal irritation, and possible shock.
2. Ekstrauteri pregnancy (ectopic) The cause of this disorder is the ovum transport delays due to mechanical obstruction of the road that passes through the uterine tubes. Especially in the ampulla of tubal pregnancy, ovarian pregnancy is rare. The diagnosis is confirmed by the presence of amenorrhea 3-10 weeks, rarely longer, irregular vaginal bleeding (not always).
3. Placenta previa Placenta previa is the implantation of the placenta into the lower uterine segment. The cause of this disorder is the phase shift occurs / over the placenta overlaps internum cervix which causes the release of the placenta.
4. Solusio (abruption) Placenta Placental abruption is a normal placenta detaching embedded in the wall of the uterus either partial mauppun complete, at the age of 20 weeks or more. The cause is retroplasenta hematoma due to bleeding from the uterus (changes in blood vessel walls), increased pressure in the room intervillus enhanced by hypertension or toxemia. The diagnosis is confirmed through the findings of pain (due to contraction
87
peralinan often exist as a continuous pain, tetanik uterus), bleeding per vagina (rare and in severe cases, external bleeding varies), to weigh fluctuating heart sounds (almost always exceeds the limits of the norm, it is generally not there are in severe cases), shock (weak pulse, rapid, low blood pressure, pallor, cold sweats, cold extremities, blue nails). is dead or can not live.
5. Retained placenta (Placenta Incompletus) The cause of this disorder is retained (born less powerful pain or pathology equipment) and incarceration (spasm in the isthmus region of the cervix, often caused by an overdose of painkillers). Diagnosis is made by the placenta is not born spontaneously and was not sure if the placenta is complete.
6. Ruptured uteri The cause of uterine rupture include obstetric measures (version), fetopelvik imbalance, where the latitude is negligible for a drug overdose or labor induction of labor pain, scarring of the uterus (the state after cesarean section, meomenukleasi, Strassman operation, wedge excision suetu tuba), accidents ( traffic accidents), are very rare.
7. Septic shock (Bacteria, Endotoxin) The cause of this disorder is the inclusion of gram negative bacterial endotoxin (coli, proteus, pseudomonas, aerobakter, enterococcus). Gram-positive bacterial toxin (streptococci, Clostridium welchii) is less common.
8. Weight preeclampsia The term eclampsia comes from the Greek word for "thunder". The word is used because it seems eclampsia symptoms occur suddenly without any prior signs of another. Eclampsia in women who suffer from seizures occur, followed by a comma. Dependent on the onset, divided into eclampsia eclampsia gravidarum, eclampsia parturientum, and puerperal eclampsia. If either one of the following signs or symptoms are found in pregnant women, mothers predictably suffered severe preeclampsia. 1. Blood pressure was 160/110 mmHg. 2. Oliguria, the urine is less than 400 cc / 24 hours. 3. Proteinuria, more than 3g / liter. 4. Subjective complaints (epigastric pain, visual disturbances, headache, pulmonary
edema, cyanosis, impaired consciousness). 5. On examination, found increased levels of liver enzymes with jaundice, bleeding
in the retina, and platelets less than 100,000 / mm.
87
Diagnosis of eclampsia should be distinguished from epilepsy, seizures due to drug anesthesia, or coma due to other causes such as diabetes. The hardest complication is maternal and fetal mortality.
2. Treatment of hypertension of pregnancy a. Control of Hypertension
Methyldopa Clonidine [α-adrenergic agonist] Calcium channel blockers Hydralazine Beta blockers
b. Provision of the antihypertensive effect of breast feeding o Knowledge about the pharmacokinetics of anti-HT drugs in breast milk is
minimal. o Giving a thiazide diuretic should be sad indarkan therefore can cause a decrease
in milk production. o Methyldopa estimated safe for nursing mothers. o Except for propranolol, another beta blocker type found in breast milk with
high levels. o Captopril Clonidine and levels in breast milk is minimal.
c. Obstetric Management of Public On my first visit to ask: o Old hypertensive and type of drug used o And a history of kidney disease or heart o Outcome of last delivery Physical examination: o Fundus examination occuli o Renal artery auscultation o Dorsalis pedis artery pulse examination (coarctatio aorta) o Examination of TD in a sitting position Laboratory tests at the first antenatal visit:
87
o Complete blood and urine examination o Renal physiology o Hepatic physiology o Serum electrolyte o ECG o 24-hour urine creatinine clearance to see o Thorax X-ray o Ultrasound examination: to determine the gestational age Diet advice : Retriksi regular food without salt The frequency
of antenatal antenatal care more often than REFERENCES
Ahmadsyah I, Prasetyono anyway. Luka. In: Sjamsuhidajat R, de Jong W, editor. Textbook of surgery. Issue 2. New York: Medical Books EGC; 2005. h. 73-5. Moenadjat Y. B root injuries. Issue 2. New York: Publishing Center School of Medicine; 2003. Heimbach DM, Holmes JH. Burns. In: Brunicardi FC, Andersen DK, billiar TR, Dunn DL, Hunter JG, Pollock RE, editors. Schwartz's principal surgery. 8 th ed. USA: The McGraw-Hill Companies; 2007. Naradzay JFX, Alson R. Thermal burns. In: Slapper D, Talavera F, Hirshon JM, Halamka J, Adler J, editors. Downloaded from: http://www.emedicine health. com . Agusuts 28, 2009. Split Thickness Skin Grafting and Full. Downloaded from http://www.burnsurvivorsttw.org/burns/grafts.html. 30 August 2009 . Cuningham FG, Mac Donald PC, Gant NF, et al. Hypertensive Disorders in Pregnancy. In: Williams Obstetrics. 22th ed. Connecticut: Appleton and Lange, 2007: 443-452. Dekker GA, Sibai BM. Ethiology and pathogenesis of Preeclampsia: Current Concept. AMJ Obstet Gynecol 1998; 179: 1359-75. Lockwood CJ and MJ Paidas. Preeclampsia and hypertensive disorders In Wayne R. Cohen Complications of Pregnancy. 5th ed. Philadelphia: Williams and Wilkins Lippicott, 2000: 207 -26. Sibai BM. Hypertension in pregnancy. In: Obstetrics normal and problem pregnancies. 4 th
edition, Churchill Livingstone, USA, 2002: 573-96. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. AMJ. Obstet Gynecol, 2000; 183: S1 - S22. Angsar MD et al. Guidelines for Management of Hypertension In Pregnancy In Indonesia. Fetomaternal Medicine Association POGI
87
M ODUL 4 Emergency neurogenic
CHAPTER I. FOURTH WEEK LEARNING OBJECTIVES
1. Recognize emergencies at the injury head and penatalaksaannya 2. Explain the radiological examination to help establish the diagnosis of head injury 3. Explain a variety of emergencies in the field of neurology and handling 4. Explain the mechanism and management of disorders caused by impairment of consciousness intracerebral 5. Explain and perform and how to stabilize the trauma patient transport 6. Describe the action or emergency patient referral management
Expert lecture: 1. Surgery
lecture 7 by dr. Sullyaman, Sp. BS Recognize emergencies at the injury head and penatalaksaannya (100 minutes) lecture 8 by dr. Yuzar Harun, Sp. B a. Explain and perform and how to stabilize the trauma patient transport (5 0 minutes) b. Describe the action or the management of emergency patient referrals (50 minutes)
2. Nerve Lecture 1 by dr. Roezwir Azhary, Sp. S
87
Explain a variety of emergencies in the field of neurology and handling (100 minutes) Lecture 2 by dr. Roezwir Azhary, Sp. S Explain the mechanism and management of disorders caused by impairment of consciousness intracerebral (100 minutes)
3. Radiology Lecture 2 by dr. Karyanto, Sp. Rad Explain the radiological examination to help establish the diagnosis of head injury (100 minutes)
Tutorial Scenario 4
Skill lab Assessment of Glasgow Coma Scale (GCS)
87
CHAPTER II. SCENARIO 4
Racing
A young man of 18 years in the conscious state was brought to the emergency unit after a
motorcycle accident. The patient can not walk alone, confused speech. Obtained vital sign
obtained TD 150/90 mmHg, pulse 60x / min, RR 2 8 x / min. Results found history anamnesis
loss of consciousness for 10 minutes, and on physical examination found he matom in the
region of the right orbit and right temporal region. After 30 minutes, the patient experienced a
rapid decline in consciousness and response to pain is the lower, right pupil fixed and dilated,
while the left pupil small and reactive.
87
CHAPTER III. REVIEW REFERENCES
SCENARIO 4: racing
A. Ways to stabilize and transport trauma patients The focus of treatment of victims with head injuries at area hospitals are pre save lives and prevent disability. In the pre-hospital phase of the emphasis given to maintain the smooth airway, control bleeding and syock, patient stabilization and transport to the nearest hospital. Airway (airway) Oxygenation of brain disorders and other vital tissues are the fastest killer in the case of trauma. To avoid the interference problem handling airway is a priority over all other issues. In patients with impairment of consciousness have a high risk for the occurrence of airway disorders., In addition to checking the existence of a foreign body, airway obstruction may occur because the base of the tongue falling backwards so that it covers the flow of air into the lungs. In addition aspiration of gastric contents is also a danger that threatens the airway. Breathing (helps breathing) Second act of believing that there are no barriers to airway breathing is helpful. Make sure the patient's breathing is still there. Circulations (control bleeding) Efforts to mempertahnakan cirkulasi that can be done pre hospital is to prevent loss of blood in cases of trauma with bleeding. If you find any bleeding, apply first attempt to control bleeding by bandaging press on the injured area.
Stabilization (maintain position) Often changes in patient position that is not true it will add to the injury suffered. Not uncommon in cases of spinal cord injuries are not properly handling the stabilization of secondary injury that would cause interference resulting in a more severe and recovery is not perfect. Installation of the traumatized limb splint, long spine board in case of injury
87
to the spine and neck in neck injuries can colar and stabilization of simple tools that others can reduce the risk of secondary damage due to an unstable position.
Transportation (transportation to Hospital) Wherever possible the patient was brought immediately to the nearest hospital for treatment can be done completely with the proper equipment.
2. Trauma capitis and classification Trauma capitis is a mechanical trauma that directly or indirectly on the head and cause neurological dysfunction. A. Simple Head Injury
Simple diagnosis can be confirmed by head injury: There is a history of trauma capitis Not pass Symptoms of headache and dizziness Generally do not require special treatment, just given symptomatic medication and get enough rest.
2. Commotio Cerebri Commotio cerebri (apoplexy) is a stupor that lasted no more than 10 minutes due to head trauma, which is not accompanied by damage to brain tissue. Patients may complain of headache, vertigo, and vomiting may appear pale. Vertigo and vomiting may be due to a concussion in a maze or terangsangnya centers in the brain stem. Commotio cerebri on may also have retrograde amnesia, the memory loss during a limited period before the accident. Amnesia is due to elimination of recorded events in the temporal lobes. Additional checks are always made is a photo of the skull, EEG, memory checks. Symptomatic therapy, treatment for 3-5 days for observation of possible complications and gradual mobilization.
3. Contusio Cerebri At contusio cerebri (brain contusion) hemorrhage-bleeding within the brain tissue without tearing jaringanyang invisible, even though the neurons were damaged or lost.
87
What is important for the occurrence of lesions is the acceleration of the head contusion that instantly cause a shift in the brain and the development of destructive compression forces. Strong acceleration also means the head hyperextended. Therefore, the brain is too strong stretching of the brain stem, causing a reversible blockade of the trajectory of the ascending reticular diffuse. Due to blockade it, the brain does not receive afferent input and, therefore, lost consciousness during reversible blockade lasts. Incidence of lesions in the region contusio "coup", "contrecoup", and "intermediate" cause symptoms of neurologic deficit that may be a reflex babinsky positive and UMN paralysis. After pulleys consciousness returned, the patient usually indicates "organic brain syndrome". Due to the force developed by the mechanisms that operate in the aforementioned trauma capitis, impaired autoregulation of cerebral blood vessels, resulting in vasoparalitis. Low blood pressure and pulse become slow, or become rapid and weak. As well as vegetative centers are involved, it nausea, vomiting and respiratory problems can arise. Investigations such as CT-scan is useful to see the location of the lesion and the possibility of short-term complications. Therapy with antiserebral edema, anti-bleeding, symptomatic, and treatment of neurotrophic 7-10 days.
4. Laceratio Cerebri Laceratio cerebri is said if the damage is accompanied by a tear piamater. Laceratio usually associated with a subarachnoid hemorrhage traumatika, acute subdural and intercerebral. Laceratio Laceratio can be divided into direct and indirect. Laceratio directly caused by penetrating head injury caused by a penetrating foreign body or fracture fragment, especially in an open depressed fracture. Laceratio while not directly caused by a severe deformity due to tissue mechanical strength.
5. Fracture Database Cranii Fractur be the basis cranii anterior fossa, fossa posterior fossa and the media. The symptoms depend on the location or where the affected fossa. Fracture of the anterior fossa symptoms : Subkonjungtival glasses hematoma without bleeding Epistaxis Rhinorrhoe
The distribution of other head injuries :
87
Mild Head Injury → includes Laseratio and Commotio Cerebri o GCS score of 13-15 o There is no loss of consciousness, or if there is no more than 10 minutes o The patient complained of dizziness, headache o There is vomiting, there is retrograde amnesia and no abnormalities found on
neurologic examination.
Moderate head injury
o GCS score of 9-12 o There are faint more than 10 minutes o There are headaches, vomiting, seizures and retrograde amnesia o Neurological examination found lelumpuhan nerves and limbs. Serious Head Injuries
o GCS score <8 o Gejalnya similar to CKS, just in a more severe o The occurrence of a progressive impairment of consciousness o The presence of skull fractures and brain tissue apart.
3. Glasgow Coma Scale (GCS) examination The degree of injury can be assessed according to the level of consciousness through the GCS system, the method of EMV (Eyes, Verbal, Movement) 1. The ability of the eyelid (E)
Spontaneously 4 On orders 3 Pain stimuli 2 Not react 1
2. Communication capability (V) Good orientation 5 Answer chaotic 4 The words do not mean 3 Groan 2 No sound 1
87
3. Motor skills (M) Ability according to the command 6 Local reaction 5 Avoidance 4 Abnormal flexion 3 Extension 2 Not react 1
4. Management of trauma capitis P rioritas prevention of head trauma a. Improve cardiovascular (shock tackle) b. Fix the balance of respiration, ventilation or good airway c. Evaluate the level of awareness d. Observe the lesion in the head, whether there are impressions of fracture, signs -
sign fracture of the cranial base, likuorhoe, be careful of the fracture cervical (neck stabilization)
e. Lesion observed in other body parts f. Complete neurologic examination and X fot the head, neck, CT-Scan g. P erhatikan pupil h. Overcome cerebral edema i. Fix the balance of fluids, electrolytes and calories j. Intra-cranial pressure monitor k. Symptomatic treatment or conservative l. If there is deterioration of consciousness accompanied by intra-cranial bleeding
more than 75 cc, open kranioserebral penetrating injury, fracture impressions of more than 1 cm immediately made operative
5. Management of patients with impairment of consciousness Management of Patients with decreased / kahilangan awareness 1. Handling emergency decompression of the lesion persisted space (space occupying
lesions / SOL) can save patients' lives. 2. If there is an increase in ICT, the following is the first treatment:
a. Elevation of the head b. Intubation and hyperventilation c. Sedation in the event of severe agitation (midazolam 1-2 mg iv) d. Osmotic diuresis with mannitol 20% 1 g / kg iv
87
e. Dexametason 10 mg iv every 6 hours in case of cerebral edema by a tumor or abscess after this therapy ICP monitor should be installed.
3. Cases of suspected encephalitis by herpes virus infection can be administered acyclovir 10 mg / kg iv every 8 hours
4. Cases of meningitis do therapy empirically. Protect patients by ceftriaxon 2x1 4x1 g ampicillin iv and pending culture results
General Therapy 1. Airway protection: adequate oxygenation and ventilation 2. Intravenous hydration: using normal saline in patients with cerebral edema or
increased ICP 3. Nutrition: do administration via enteral nutrition by tube nasoduodenal, avoid the use
of naso gastric tube because of the threat of aspiration and reflux 4. Skin: avoid pressure sores by tilting right and left every 1 to 2 hours, and use a
mattress that can be developed with wind and heel protector 5. Eyes: avoid abrasion of the cornea with the use of lubricants or close your eyes with
plaster 6. Bowel care: avoid constipation with stool softeners (docusate sodium 100 mg 3x1)
and the provision of ranitidine 50 mg iv every 8 hours to avoid stress ulcer caused by steroids and intubation
7. Bladder treatments: indwelling and intermittent catheters cateter urine every 6 hours 8. Joint mobility: passive ROM exercises to prevent contractures 9. Prophylaxis of deep vein thrombosis (DVT): 5000 iu sc administration every 12
hours, the use of pneumatic compression stockings, or both.
6. Reference to case management In accordance with the circumstances of each region vary widely, depending on the selection of transportation facilities, security, geographical situation, and quickly achieve the specified referral hospital. The principle is "To get 0a definitive care in the shortest time '. Thus, whenever possible should any patients with head trauma admitted to hospital with a CT scan of existing facilities and neurological surgery. But, look at the situation and conditions in our country, where only in provincial hospitals have facilities (especially outside of Java), then the referral system as it is difficult to implement. Therefore, there are three things to do : 1. When it is within easy reach and without aggravate the condition of the patient,
should be directly referred to the existing hospital neurosurgical facilities (provincial hospital).
2. If not possible, should be referred to the nearest hospital surgical facilities.
87
3. If the status of the ABC has not stabilized, could be referred to the nearest hospital to get better handling. During the trip, there could be a variety of circumstances such as shock, seizures, apnea, airway obstruction, and anxiety. Thus, while on the move, the state of ABC patients must remain strictly monitored and supervised. With the risk during transport, it is necessary in the preparation and transport requirements, which is accompanied by medical personnel, nurses are able to handle a minimum of ABC, as well as emergency equipment and medicine (among ambubag, oropharyngeal and nasopharyngeal tube, suction, oxygen, intravenous fluids or RL NaCl 0.9%, infusion sets, syringes 5 cc, 25 cc aquabidest, diazepam ampoules and vials khlorpromazine). In addition, a complete referral letter and jela s. But, often considered the social, geographical, and cost make it difficult to refer patients, so it is necessary to handle for us to determine the best decisions for the patient. There are several criteria for head injury patients are still being treated at home but with close observation, namely:
1. Orientation of time and place is still good 2. No neurological focal symptoms. 3. No headache or vomiting - vomiting. 4. There was no skull fracture. 5. Can anyone watching at home. 6. Residence not far from health centers / sub-clinics.
In addition, an explanation should be given to the family to actively supervise (and ask the patient to wake) every two hours. Where the headache gets worse, more frequent vomiting, seizures, decreased consciousness, and the paralysis then immediately report to the clinic or medical officer nearest.
87
REFERENCES
Chusid, Correlative neuroanatomy and Functional Neurology, part two. Gajah Mada University Press, 1991 Harsono, Capita Selekta Neurology, second edition. Gajah Mada University Press, 2003 Alexander J, Head Injuries, PT Dhiana Popular. Scholastic Group, Jakarta, 1981 Sidharta P, Mardjono M, Basis of Clinical Neurology, Dian Rakyat, Jakarta, 1981 Hasan Sjahrir, Neurology Specialty Neurology, Dian Rakyat, Jakarta, 2004 Mahar Mardjono, Priguna Sidharta, Basis of Clinical Neurology, dian people, Jakarta, 2004 Arif et al Mansjoer Editor, Structure of Nerve Trauma in Selekta Capita Medicine Third edition vol 2, Media Aesculapius, Jakarta, 2000 Robert L. Martuza, Telmo M. Aquino, Trauma in the Manual of Neurologic Therapeutics With Essentials of Diagnosis, 3th ed, litle Brown & Co, 2000 Chusid, Correlative neuroanatomy and Functional Neurology, part two. Gajah Mada University Press, 1991 Harsono, Capita Selekta Neurology, second edition. Gajah Mada University Press, 2003 Alexander J, Head Injuries, PT Dhiana Popular. Scholastic Group, Jakarta, 1981 Sidharta P, Mardjono M, Basis of Clinical Neurology, Dian Rakyat, Jakarta, 1981 Hasan Sjahrir, Neurology Specialty Neurology, Dian Rakyat, Jakarta, 2004 Mahar Mardjono, Priguna Sidharta, Basis of Clinical Neurology, dian people, Jakarta, 2004 Arif et al Mansjoer Editor, Structure of Nerve Trauma in Selekta Capita Medicine Third edition vol 2, Media Aesculapius, Jakarta, 2000
87
Robert L. Martuza, Telmo M. Aquino, Trauma in the Manual of Neurologic Therapeutics With Essentials of Diagnosis, 3th ed, litle Brown & Co, 2000
87
MODULE 5 Emergency Psychiatry
CHAPTER I. THE FIFTH WEEK LEARNING OBJECTIVES
1. Explains emergency psychiatry and handling 2. Explain the type and management of poisoning 3. Explaining gastroenterohepatologi and handling emergency 4. Explain the emergency treatment of metabolic and endocrine 5. Explain the emergency treatment of hypertension and renal 6. Explain the forensic toxicology 7. Able to recognize the signs of death
Expert lecture: 1. Psychiatry
Lecture 1 by dr. Woro Pramesti, Sp. KJ Explains emergency psychiatry and handling (100 minutes)
2. Internal Medicine Lecture 1 by dr. Ali Imron, Sp. PD, KGEH Explain the type and management of poisoning (10 0menit) Lecture 2 by dr. Ali Imron, Sp. PD, KGEH Explain gastroenterohepatologi and handling emergencies (10 0 minutes) Lecture 3 by dr. Tehar Karo - K aro, Sp. PD Explain metabolic and endocrine emergency treatment (10 0 minutes) Lecture 4 by dr. Ahmad Taruna, Sp. PD Explain emergency treatment of hypertension and kidney (10 0 minutes)
3. Forensic Lecture 2 by dr. Evi Dian a-Fitr, Sp. F Explain the forensic toxicology (10 0 minutes) Lecture 3 by dr. Evi Dian a-Fitr, Sp. F Able to recognize the signs of death (50 minutes)
87
Tutorial Scenario 5
Skill lab Intake of Foreign Objects (Corpus Alienum)
87
CHAPTER II. SCENARIO 5
FEEL PURSUED
A 20-year-old woman, left her boyfriend about a month ago. He felt frustrated, often locked
himself in his room, and feel there is talk about him, and something to tease him that he felt his
girlfriend decided to use him because there guna.Akhir-ultimately-his behavior is getting worse
and finally he found his room with his mouth foaming , as well as his body was found a bottle
of Baygon. The family immediately took him to the hospital.
87
CHAPTER III. REVIEW REFERENCES
SCENARIO 5: Feel pursued 1. Emergency psychiatry
a. Restless noisy conditions Signs and symptoms: Restlessness, pacing, Yelling, Skip, skip, Angry, angry, Suspicious + + +, aggressive, violent, agitation, Happy + + +, + + + Singing, Speaking chaotic, Disturbing other people, did not sleep for days, It's hard to communicate. Management: Klormetiazol 1-2 g per os, repeated every 2 hours If it is difficult, give haloperidol 5 mg valium 20 mg IM + in a separate
syringe Alcoholic delirium, give chlorpromazine 200 mg 100 mg IM repeated every 2
hours, plus high-dose multivitamin b. Acts of violence (violence)
Violence is a person of physical aggression against others. The violence may arise due to psychiatric disorders, but can also occur in ordinary people who can not handle the pressure of everyday life with a better way. Clinical features and diagnosis Psychiatric disorders are often related to: Psychotic disorders such as schizophrenia and manic, especially when people
are paranoid and have hallucinations telling (commanding hallucinations) Alcohol intoxication or other substance Withdrawal symptoms from alcohol or sedative-hypnotic drugs Catatonic furor Depression agitatif Personality disorder is characterized by anger and impulse control disorders Organic mental disorders, particularly those of frontal and temporal lobes of
the brain Evaluation and management of Protect yourself Alert to the signs of the emergence of violence Make sure there is adequate staffing for patient safety tie
87
Binding of patients only performed by trained staff. Usually after the binding of benzodiazepines or antipsychotics given
Perform appropriate diagnostic evaluation, the vital signs, physical examination and psychiatric interview. Evaluation of suicide risk
Exploration of the possibility of psychosocial interventions to reduce the risk of violence
Need to be treated to prevent violence. Continuous observation Therapy psikofarmaka Antipsychotic drugs are usually given
c. Suicide (suicide) Suicide is the death of the intended and carried out by a person against himself. Clinical features and diagnosis High risk of suicide: The man, the older the age, social isolation / living alone, history of suicide / attempted suicide in the family, history of illness / chronic pain, Just finished the operation, does not have a job. Evaluation and management of Do not leave the patient alone in the room Remove objects that could harm Therapy psikofarmaka Transquilizer given lightly, especially if sleep disturbed. The drug of choice is lorazepam 3x1 mg daily, for 2 weeks. Do not give the drug in large quantities at once to the patient and the patient should control within a few days.
d. Delirium Clinical features and diagnosis Prodromal
Typically patients complain of fatigue, anxiety, iritabel, sleep disorders Disturbance of consciousness
Decrease in the clarity of the level of awareness on the environment Vigilance
Consists of hyperactivity (associated with withdrawal syndrome) and hipoaktivitas (all decreased activity)
Concentration problems Marked difficulties in maintaining presence, focus, and divert attention
Orientation In the mild delirium orientation disruption time, an interruption in severe delirium places and people orientation
87
Language and cognitive Language abnormalities occur and incoherence. Memory and cognitive functions commonly disturbed
Perception Visual and auditory hallucinations occurred
Mood Symptoms are often: anger, rage, fear is groundless
Sleep-wake disorders Often exhibit agitation at night and trouble sleeping = sundowning
Neurological symptoms Include: dysphasia, tremor, asterixis, incoordination, and urinary incontinence.
Interview guide and psychotherapy Be supportive and not threatening Reassure the patient Offer drug Evaluation and management of The main thing is to treat the cause. When the cause anticholinergic toxicity, use pisostigmin salicylate 1-2 mg IV / IM, can be repeated 15-30 minutes if necessary.
e. Depression Symptoms and signs: Sudden changes in life Early morning insomnia Agitation Loss of appetite and a willingness Feeling very desperate Social relations rewind Sinful delusion Not able to express thoughts and feelings
Treatment: ECT (electro-convulsive therapy) Tricyclic antidepressants 150-200 mg / day + 4x10 mg valium or 10-20 mg
IM
87
2. Management of poisoning victims 1. Stabilization
Form of cardiopulmonary resuscitation promptly and precisely as follows: Liberation of the airway Improvement of respiratory function Improvement of blood circulation system
2. Decontamination Decontamination is a therapeutic intervention aimed to reduce exposure to toxins, reduce absorption, and prevent damage. Decontamination of pulmonary Decontamination of the eyes Skin decontamination Gastrointestinal decontamination In general the Baygon intoxication if swallowed dose subtoksik, decontamination is not necessary, except when swallowing> 100 mg / kg, then do: a. Induction of vomiting b. Gastric aspiration and kumbah Effective when carried out for 2-4 hours first,
and with good technique. c. Activated charcoal
- A single dose: 1 g / kg or 30-100 g of adult and children 15-30 grams (specific drugs and antidotum)
3. Elimination Action is the action to accelerate the elimination of toxins expenditures are circulating in the blood, or in the gastrointestinal tract after more than 4 hours. When still in the GI tract given repeated doses of activated charcoal 30-50 g every 4 hours PO / enteral. Another act of elimination: Forced diuresis, alkalinization of urine, urine acidification, hemodialysis / peritoneal dialysis.
4. Antidotum provision (if available) In most cases of poisoning are very few types of toxins antidotumnya drugs and drug preparations that are commercially available antidotes are very few in number.
87
3. Types of poisoning a. Chemicals
1. Cyanide 2. Methanol / ethylene glycol 3. Reciprocal 4. Mercury 5. Arsenic 6. Na hypochlorite 7. Thallium 8. Organophosphate 9. Fe
b. Drug 1. Amphetamines 2. Digoxin 3. Isoniazid 4. Opioid 5. Paracetamol 6. Warfarin 7. Propranolol
c. Natural toxins 1. Datura / amethyst 2. Amanita phaloides 3. Oleander
d. Animal toxins
1. Scorpion 2. Snake 3. Spiders 4. Jellyfish - Jellyfish
e. Food 1. Jengkol 2. Cassava
f. Microbial toxin: Botulinum
Based on where toxins are:
87
In the wild o Toxins in natural gas
In households o Detergent o Disinfectant o Insecticide o Cleaner
In agriculture o Insecticide o Herbicide o Pesticide
In industrial and laboratory o Strong acid o Strong base
In food o CN in cassava o Botulinus toxin o Preservative o Additives
In medicine o Hypnotic o Sedatives
Based on the organ of the body: Are hepatotoxic Nephrotoxic Based on the effects of: Local
o Corrosive poison o Halogen groups
Systemic o Barbiturates, alcohol, morphine -> to the SSP o Digitalis and oxalate -> towards heart o CO to the blood Hb
Combination
87
o Carbolic acid, causing erosion of the stomach and depression SS
Several types of toxins that have the specific odor.
Table 1. Characteristic smell of the poison
Odor Cause Acetone Isopropyl alcohol, acetone Almond Cyanide Garlic Arsenic, selenium, thallium Rotten eggs Hydrogen sulfide, mercaptan
No The clinical Possible causes
A. Pin-point pupils, RR decreased
Opioids, Clonidine, phenothiazines, inhibitor cholinesterase: organophosphates, carbamat
2. Dilated pupils, RR decreased
Benzodiazepines
3. Dilated pupils, tachycardia
Tricyclic antidepressants, amphetamines, ecstasy, cocaine, antihistamines, anticholinergics: benzeksol, benztropin
4. Cyanosis CNS depressant drugs
5. Hypersalivation organophosphate / carbamate, insecticide
6. Nystagmus, ataxia, cerebellar signs
Alcohol, anticonvulsants: phenytoin, carbamazepine
7. Extrapyramidal symptoms
Phenothiazines, haloperidol, metoclopramide
87
8. Seizures Tricyclic antidepressants, anticonvulsants, theophylline, antihistamines, NSAIDs, phenothiazines, isoniazid
9. Hyperthermia Lithium, tricyclic antidepressants, antihistamines
10. Bradycardia B - blockers, digoxin, opioids, Clonidine, organophosphates, calcium antagonists
11. Abdominal Cramp, diarrhea, takikardi, halusinasi
Withdrawal alkohol, opiat, benzodiazepin
Clinical simptom may indicate the cause of poisoning
4. Sign - signs of death (tanatologi) Two stages of death: 1. Somatic death / systemic death / clinical death 2. Cellular death / molecular death
Somatic signs of death: 1. Loss of movement and sensibility 2. Cessation of breathing 3. Cessation of heart beat and blood circulation
Sign - signs of cellular death: 1. Decrease in body temperature (argor mortis) 2. Bruised corpse (livor mortis) 3. Rigid bodies (rigor mortis) 4. Changes in skin 5. Changes in eye 6. Decay and sometimes the process of mummification and adipocere
According to the language, tanatologi derived from Thanatos (death-related) and logos (science). Meanwhile, according to the terms, tanatologi is the study of death and the changes
87
that occur after death and the factors influencing those changes. While tanatologi itself is part of the forensic medical science that studies about the things that has to do with death and the changes that occur after a person dies and the factors that influence it.
Stadium Death In essence there are two stages of death stages, namely stage somatic death / mortality clinical / systemic death, and death of cellular / molecular death, but the stage of death is also divided into five stages as follows: 1. Somatic death / clinical death / death is the cessation of the systemic function of the
nervous system, cardiovascular system, respiratory system and thus lead to irreversible tissue anoxia is complete and thorough.
2. The death of cellular / molecular death is the cessation of activity of the network system, cell and molecular body, resulting in the death of an organ or tissue that occur some time after somatic death.
3. Near-death (suspended animation, apparent death) is the third interruption of life support systems are determined by simple medical devices. With advanced medical equipment can still be proved that the three systems are still functioning. NDE is often found in cases of poisoning a sleeping pill, electric shock and drowning.
4. Cerebral death was damage to both hemispheres of the brain that is irreversible, except the brain stem and cerebellum, while the other two systems, namely the respiratory and cardiovascular systems are still functioning with the aid of tools.
5. Brain death (brain stem) is when the entire contents of the neuronal damage is irreversible intracranial, including the brain stem and cerebellum. With known brain death (brain stem death), it can be said as a whole person can not otherwise live longer, ARF sehin a tool can be stopped.
How to Detect Mortality Changes may occur early in the time of death or a few minutes later, for example, the heart and blood circulation stops, breathing stops, and corneal light reflex missing eye, pale skin, muscle relaxation occurs. But after some time off after the changes occur is clear, thus allowing a more definitive diagnosis of death. The signs of a bruised corpse (livor mortis / hipostatis / lividitas post-death), a rigid body (rigor mortis), decreased body temperature, decomposition (Putrefection / decomposition), mummifikasi, and adiposera, and or biochemical changes.
87
REFERENCES
Elvira, SD and H. Gitayanti Of 2010. Textbook of Psychiatry. London: Faculty of medicine. Faculty of Medicine, UI. Of 1997. Science Forensic Medicine. London: School of Medicine. K edokteran UI faculty., 2006. Medicine IV Edition. New York: Publishing Center for Medicine in the Faculty of Medicine, University of Indonesia. Faculty of Medicine, UI. Capita Selekta Medicine. Issue 3. New York: Media Aesculapius. Hariadi, A. Of 2010. Textbook of Forensic Medicine and Science Medikolegal. New York: FK Unair. Purwadianto, A. and Budi S. Of 2000. Emergency Medical Care. New York: Binarupa script.
87
SUMMARY OF BLOCK ACTIVITY
I. Lectures
Module TopicsNumber
of Hours
Science Informant
I Lecture 1 Surgery
a. Introduction of block
emergencies and Policy
national in dealing with
emergencies and disasters (50
minutes)
b. The failure organ function
due to trauma / multiple
trauma (50 minutes)
2 x 50 ' Surgery dr. Yuzar Harun, Sp.B
Lecture 2 Surgery
Management of vascular injury
(10 0 minutes)
2 x 50 ' Surgery dr. Pirma Hutauruk, Sp.B
Lecture 3 Surgery
Initial inspection and management
of musculoskeletal trauma (100
minutes)
2 x 50 ' Surgery dr. Aswedi Putra, Sp.OT
Lecture 1 Anesthesia
a. Emergency Sign) and mark
the priority sign in case of
emergencies Traumatology.
2 x 50 ' Anesthesia dr. Achmad Assegaf,
Span
87
(50 minutes)
b. Assessment and management
of early (initial assessment) in
the case of trauma / multiple
trauma / drowning in the
order of priority (ABC) (50
minutes)
Lecture 2 Anesthesia
The use of drugs in treating
patients with emergency
2 x 50 ' Anesthesia dr. Achmad Assegaf,
Span
Lecture 1 Forensic
a. A legal specification of trauma
and emergency situations
(informed consent in
emergencies)
b. Visum et repertum (50 minutes)
2 x 50 ' Forensic dr. Evi Diana, Sp.F
Lecture 1 Eye
Emergency Eye (100 minutes)
2 x 50 ' Eye dr. Helmi Muchtar, Sp.M
II Lecture 1 Child
Emergencies in pediatrics
2 x 50 ' Pediatric dr. Ferdi, Sp.A
Lecture 4 Surgery
a. Emergencies in thoracic trauma
(50 minutes)
b.Trauma maxillofacial (50
minutes)
2 x 50 ' Surgery dr. Yuzar Harun, Sp.B
Anesthesia Lecture 3 2 x 50 ' Anesthesia dr. Indra Faisal, Sp.An
87
Respiratory emergencies
Anesthesia Lecture 4
a. Mechanism occurrence of
airway obstruction in adults
and drowning (drowning) (50
minutes)
b.Management airway
obstruction (respiratory
resuscitation) (50 minutes)
2 x 50 ' Anesthesia dr. Dendy Maulana, Sp.An
Anesthesia Lecture 5
Understand the objectives and
actions of RJPO
2 x 50 ' Anesthesia dr. Undang Komaruddin, Sp.An
ENT Lecture 1
Emergency in ENT
2 x 50 ' ENT dr. Fatah Satya W, Sp.THT
Radiology Lecture 1
The examination support thorax
trauma and maxillofacial
radiologists
2 x 50 ' Radiology dr. Haryadi, Sp.Rad
III Obstetrics and Gynecology lecture
Emergency Obstetrics and Gynecology (100 minutes)
2 x 50 ' OBGYN dr. Taufiqurrahman, Sp.OG
Heart Lecture
Cardiac emergency
2 x 50 ' Heart dr. Asrizal T, Sp.JP
Surgery Lecture 5
Burns, treatment principles, and
criteria for inpatient stabilization
2 x 50 ' Surgery dr. Yuzar Aaron, Sp.B
87
and referral (100 minutes)
Surgery Lecture 6
Aspects of emergency abdominal surgery and treatment
2 x 50 ' Surgery dr. Pirma Hutauruk, Sp.B
Anesthesia Lecture 6
a. Signs and symptoms of
shock (hypoperfusion) (50
minutes)
b. Fluid administration in shock and bleeding (50 minutes)
2 x 50 ' Anesthesia dr. Undang Komaruddin, Sp.An
Lecture Dermatology
Emergency on the Skin
2 x 50 ' Skin and Genital
dr. M.Syafei Hamzah, Sp.KK
IV Surgery Lecture 7
Emergency on injury head and the treatment
2 x 50 ' Neurosurgery dr. Sullyaman, Sp.BS
Surgery Lecture 8
a. Stabilitation and transport of
trauma patients (50 minutes)
b.Management emergency patient
referral (50 minutes)
2 x 50 ' Surgery dr. Yuzar Aaron, Sp.B
Nerves Lecture 1
Emergency in the field of
neurology and treatment
2 x 50 ' Nerve dr. Roezwir Azhary, Sp.S
Nerves Lecture 2
Mechanisms and management of disorders caused by impairment of
2 x 50 ' Nerve dr. Roezwir Azhary, Sp.S
87
consciousness intracerebral
Radiology Lecture 2
Radiologist examination to help
establish the diagnosis of head
injury (100 minutes)
2 x 50 ' Radiology dr. Haryadi, Sp.Rad
V Psychiatry lecture
Emergency psychiatry and
treatment(100 minutes)
2 x 50 ' Psychiatry dr. Woro Pramesti, Sp.Kj
Lecture 1 interna
The type and management of poisoning
2 x 50 ' IPD dr. Ali Imron, Sp.PD., KGEH
Lecture 2 Interna
Emergency in gastroentero hepatology and the treatment
2 x 50 ' IPD dr. Ali Imron, Sp.PD., KGEH
Lecture 3 Interna
The treatment of metabolic and
endocrine emergency cases
2 x 50 ' IPD dr. Tehar Karo-karo, Sp.PD
Lecture 4 Interna
The treatment of hypertension and kidney emergency (100 minutes)
2 x 50 ' IPD dr. A.Taruna, Sp.PD
Lecture 2 Forensic
ForensicToxicology (100 minutes)
2 x 50 ' Forensic dr. Evi Diana, Sp.F
Lecture 3 Forensic
Signs of death
2x50 ' Forensic dr. Evi Diana, Sp.F
87
SCHEDULE OF LEARNING
Time WEEK 1. Traumatology MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 22 / 10 / 2012 23 / 10 / 2012 24 / 10 / 2012 25 / 10 / 2012 26 / 10 / 2012
07:00 to 07:50
7:50 to 8:40
Block Contract Lecture 3
Surgery8:40 to 09:30 TUTORIAL
Scenario 1 Lecture 1 Eye Lecture 1 Surgery TUTORIAL Scenario
109:30 to 10:20 Lecture 1
Forensic 10:20 to 11:10 CSL 1 Lecture 2 Surgery
11:10 to 12:00
12:00 to 13:00 Break
13:00 to 13:50 Lecture 1
Anesthesia Lectura 2 Anesthesia CSL 2
13:50 to 14:40
14:40 to 15:30
15:30 to 16:20
Note: The schedule is not filled is used for guided independent study.

87
TIME WEEK 2. Emergency respiration MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 29 / 10 / 2012 30 / 10 / 2012 31 / 10 / 2012 1 / 11 / 2012 2 / 11 / 2012
07:00 to
07:50
7:50 to 8:40
Lecture1 Pediatric
Lecture 4 Anaesthesia
8:40 to 09:30 Scenario 2
TUTORIAL Scenario 2 TUTORIAL09:30
to 10:20
Lecture 3 Anesthesia
10:20 to
11:10 Lecture 4 Surgery CSL 211:10
to 12:00
12:00 to
13:00 Break
13:00 to
13:50 Lecture 1 ENT
Lecture 1 Radiology
Lecture 5 Anaesthesia CSL 2 13:50
to 14:40 14:40
to 15:30
15:30 to
16:20
Note: The schedule is not filled is used for guided self-study
87
TIME WEEK 3. Emergency hemodynamic MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 5 / 11 / 2012 6 / 11 / 2012 7 / 11 / 2012 8 / 11/ 2012 9 / 11 / 2012
07:00 to
07:50
7:50 to 8:40 Lecture 6
ANAESTHESIA Lecture 1 SKIN and
Genital
TUTORIALScenario 3
8:40 to 09:30 TUTORIAL
Scenario 309:30 to
10:20 Lecture 1 Obstetrics
10:20 to
11:10 Lecture 5 SURGERY CSL 3 11:10
to 12:00
12:00 to
13:00 Break
13:00 to
13:50 Lecture 1 HEART
Lecture 6 SURGERY CSL 3 13:50
to 14:40 14:40
to 15:30
15:30 to
16:20
Note: The schedule is not filled is used for guided independent study.
87
TIME WEEK 4. Emergency neurogenic MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 12 / 11 / 2012 13 / 11 / 2012 14 / 11 / 2012 15 / 11/ 2012 16 / 11 / 2012
07:00 to
07:50
7:50 to 8:40
Lecture 7
SURGERY
8:40 to 09:30 TUTORIAL
Scenario 4TUTORIAL Scenario 4 09:30
to 10:20
10:20 to
11:10 Lecture 1 NERVE
Lecture 8 SURGERY CSL 4 11:10
to 12:00
12:00 to
13:00 Break
13:00 to
13:50 Lecture 2 Radiology
Lecture 2 NERVE CSL 4 13:50
to 14:40 14:40
to 15:30 15:30
to 16:20
Note: The schedule is not filled is used for guided independent study.
87
TIME WEEK 5. Emergency Psychiatry MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 19 / 11 / 2012 20 / 11 / 2012 21 / 11 / 2012 22 / 11/ 2012 23 / 11 / 2012
07:00 to
07:50
7:50 to 8:40
Lecture 2 Interna
Lecture 3 Interna
8:40 to 09:30 Scenario 5
TUTORIALScenario 5
TUTORIAL09:30 to
10:20
Lecture 2 FORENSIC
Lecture 1 Psychiatry Lecture 4
Interna10:20
to 11:10 Lecture 1
Interna Lecture 3 FORENSIC CSL
11:10 to
12:00 12:00
to 13:00
Break
13:00 to
13:50 CSL 13:50 to
14:40 14:40
to 15:30
15:30 to
16:20
Note: The schedule is not filled is used for guided independent study.
87
TIME WEEK 6. FINAL EXAM BLOCK
MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY
26 / 11 / 2012 27 / 11 / 2012 28 / 11 / 2012 29 / 11/ 2012 30 / 11 / 201207:00 to
07:50
7:50 to 8:40
OSCE
8:40 to 09:30
09:30 to 10:20
10:20 to 11:10
11:10 to 12:00
12:00 to 13:00 Break
13:00 to 13:50
OSCE
Final Exam13:50 to
14:40
14:40 to 15:30
15:30 to 16:20
87







