

N. Ferrara, MD Ordinario di Geriatria
Direttore della Scuola di Specializzazione in Geriatria
Università degli Studi di Napoli “Federico II”
Presidente della Società Italiana di Gerontologia e Geriatria
LETTURA1 Dicembre 2016
PERSONALIZED MEDICINE FOR OLDER PEOPLE:TIME FOR ONE PERSON TRIALS

ANTONIO CARDARELLI n. Civitanova del Sannio (IS) 29 marzo 1831
m. Napoli 8 Gennaio 1927

A. Cardarelli, lo scienziato
Observatio et ratio
OPINIONE DEGLI ESPERTI
- Il medico ricorre spesso al collega esperto,considerato una fonte d'informazione.
- Tuttavia nessun collega per quanto esperto puògarantire attualità, obiettività e completezza delleinformazioni fornite, perché i dati derivatidall'esperienza non possono essere generalizzati.
«Uso coscienzioso, esplicito e giudizioso della migliore
ed attuale evidenza scientifica per prendere decisioni
nell’ambito dell’assistenza del paziente»
Sackett D, et al, 1996
Successivamente “ridefinita” come:
«integrazione delle prove derivanti dalla migliore ricerca clinica con l’esperienza clinica e i valori dei
pazienti»
Sackett D, et al. 2000
CHE COS’È L’EVIDENCE BASED MEDICINE?

Quesito clinico
ricercabile
Ricercare e
raccogliere evidenze
Analizzare e
sinteteizzare
evidenze
Prendere una
decisione su
diagnosi e terapia
Competenze,
Esperienza
Fisiopatologia
Parere del paziente
Problema clinico
LE 5 TAPPE DELL’EBM

FORMULARE LA GIUSTA DOMANDA:
«PICO» PRINCIPLE
Qual è la durata del ricovero (O) per i pazienti che hanno subito la totale sostituzione dell’anca (P) che
hanno sviluppato un infezione postoperatoria (I) rispetto a coloro che non hanno sviluppato tale
infezione (C)?
TRIAL CLINICI
- Valutano l’efficacia e la sicurezza di terapiefarmacologiche e non su un vasto gruppo di persone.
- Solitamente i soggetti arruolati vengono suddivisi indue o più gruppi includendo un gruppo-controllo chenon riceve nessun trattamento o un placebo o untrattamento diverso a scopo comparativo

Studi originali commentati e analizzati da altri autori.
In questo gruppo rientrano:
- Review
- Systematic Review
- Metanalisi
- Linee Guida
PUBBLICAZIONI SECONDARIE

LINEE GUIDA
«Raccomandazioni di comportamento clinico, prodotteattraverso un processo sistematico, allo scopo diassistere medici e pazienti nel decidere le modalità diassistenza più appropriate in specifiche circostanzecliniche»
Institute of Medicine
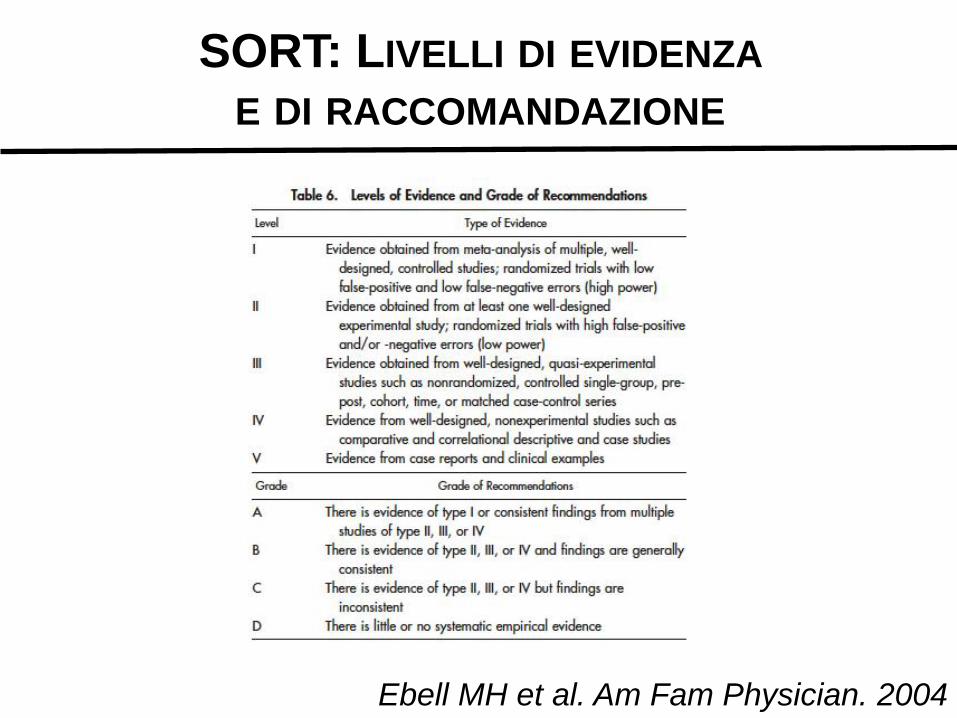
Ebell MH et al. Am Fam Physician. 2004
SORT: LIVELLI DI EVIDENZA
E DI RACCOMANDAZIONE
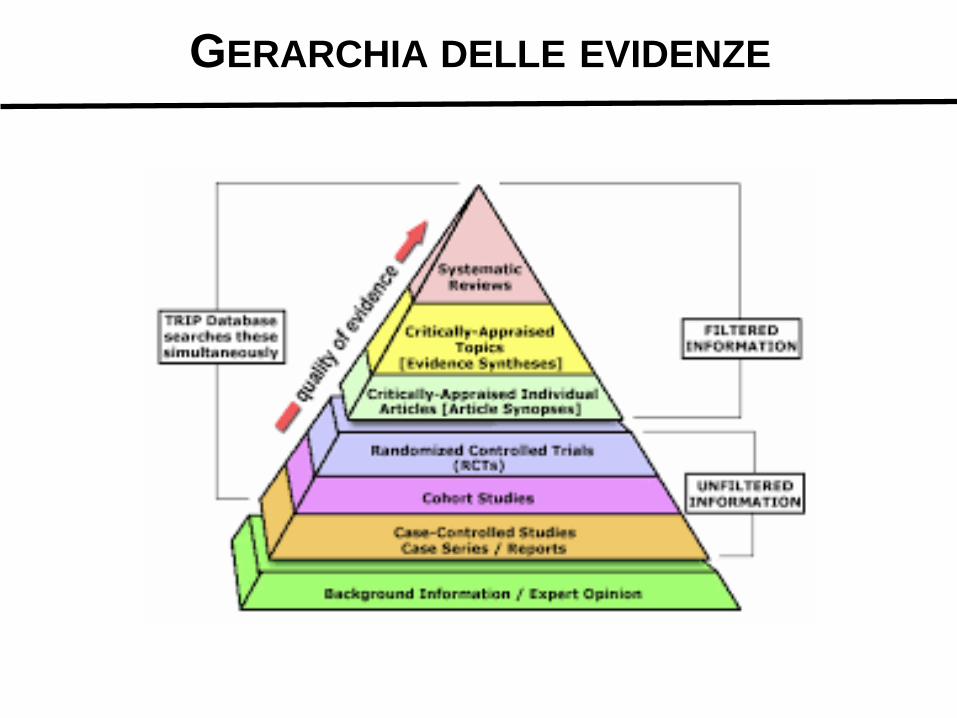
GERARCHIA DELLE EVIDENZE

L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione

L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione: durante l’arruolamento si genera una eccessiva eterogeneità dei gruppi in studio
Randomizzazione del campione
L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione
- Bias di misurazione

L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione
- Bias di misurazione: si verifica se i metodi dimisurazione non sono ben tarati o imprecisi o diversitra i pazienti studiati
Mascheramento

L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione
- Bias di misurazione
- Bias di pubblicazione

L’ERRORE DIETRO L’ANGOLO: I BIAS
La distorsione o bias è una modifica, intenzionale o non intenzionale, del disegno e/o della conduzione di uno studio clinico e dell’analisi e della valutazione dei dati, in grado di incidere sui risultati rendendoli inattendibili
Principali tipologie di bias:
- Bias di selezione
- Bias di misurazione
- Bias di pubblicazione: risultati positivi provenientidalla ricerca hanno una maggiore probabilità diessere pubblicati rispetto a quelli negativi.
LIMITI DELLA EBM: LA POPOLAZIONE ANZIANA
- Le evidenze ottenute dai numerosi studi scientificicondotti sono utili se applicabili a contesti reali.
- Se le conclusioni sono riferibili solo ad una partedella popolazione, queste diventano solo «parziali»evidenze.
- Gli anziani sono i maggiori consumatori delle risorsesanitarie eppure sono frequentemente esclusi dagliRCT, persino quelli condotti su condizioni croniche adelevata prevalenza nella popolazione anziana comel’insufficienza cardiaca.
Marchionni et al. G Ital Cardiol 2013;14

CHF: who’s who
Trials Real world
Age (years) Sex Diagnosis Treatment Compliance
50-65
M>F
CHF primary
only for CHF
optimum
75
F>M
Comorbidity
Concurrent meds
variable


EBM and Geriatrics
Elderly are almost systematically excluded from RCTs.
Even if included, RCTs show comparative efficacy of only some types of treatment, for an “average” randomized patient.
A new form of EBM is in place
EVIDENCE-BIASED MEDICINE
Evidence is derived from groups, yet decisions are made for individuals. This fundamental mismatch means that we can never fully escape the problems inherent in cross-level inference.
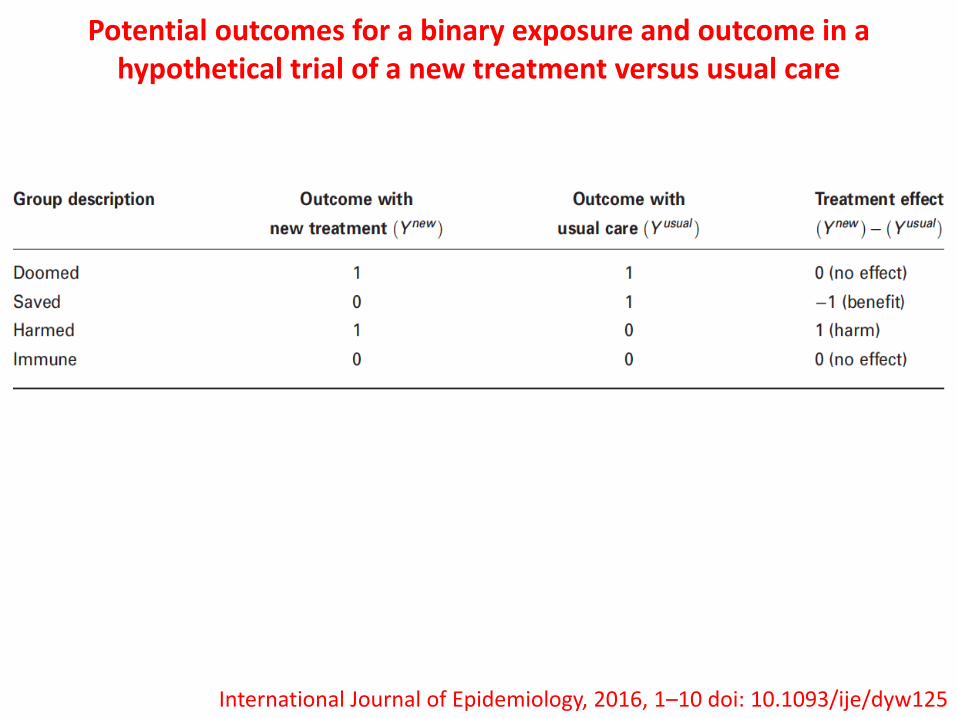
Potential outcomes for a binary exposure and outcome in a hypothetical trial of a new treatment versus usual care
International Journal of Epidemiology, 2016, 1–10 doi: 10.1093/ije/dyw125

Popular measures of treatment effect can be written in terms of the unidentifiable proportions of these patient types but can be estimated
using observable quantities.For example, the causal risk difference (RD) is simply the difference of
the proportion of harmed and saved types:
Similarly, the causal relative risk (RR) and the odds ratio (OR) can be estimated as
International Journal of Epidemiology, 2016, 1–10 doi: 10.1093/ije/dyw125

International Journal of Epidemiology, 2016, 1–10 doi: 10.1093/ije/dyw125

Impact of statistical power and the proportion of ‘true’ modifiersamong the variables examined on the credibility of statistically
significant results in HTE analyses
International Journal of Epidemiology, 2016, 1–10 doi: 10.1093/ije/dyw125
• Person-level treatment effects cannot be identified in randomized clinical trials and population average treatment effects may not apply to all patients.
TAKE HOME MESSAGES

• Person-level treatment effects cannot be identified in randomized clinical trials and population average treatment effects may not apply to all patients.
• One-variable-at-a-time subgroup analyses are highly prone to false-positive resultsdue to multiple comparisons and false-negative results due to inadequate power, and have limited ability to inform decisions for individuals, becauseindividuals vary from one another in multiple ways simultaneously.
TAKE HOME MESSAGES
• Person-level treatment effects cannot be identified in randomized clinical trials and population average treatment effects may not apply to all patients.
• One-variable-at-a-time subgroup analyses are highly prone to false-positive resultsdue to multiple comparisons and false-negative results due to inadequate power, and have limited ability to inform decisions for individuals, becauseindividuals vary from one another in multiple ways simultaneously.
• Subgroup analyses that incorporate information on multiple variables, such as those based on predicted outcome risk, may yield more patient-centred results.
TAKE HOME MESSAGES


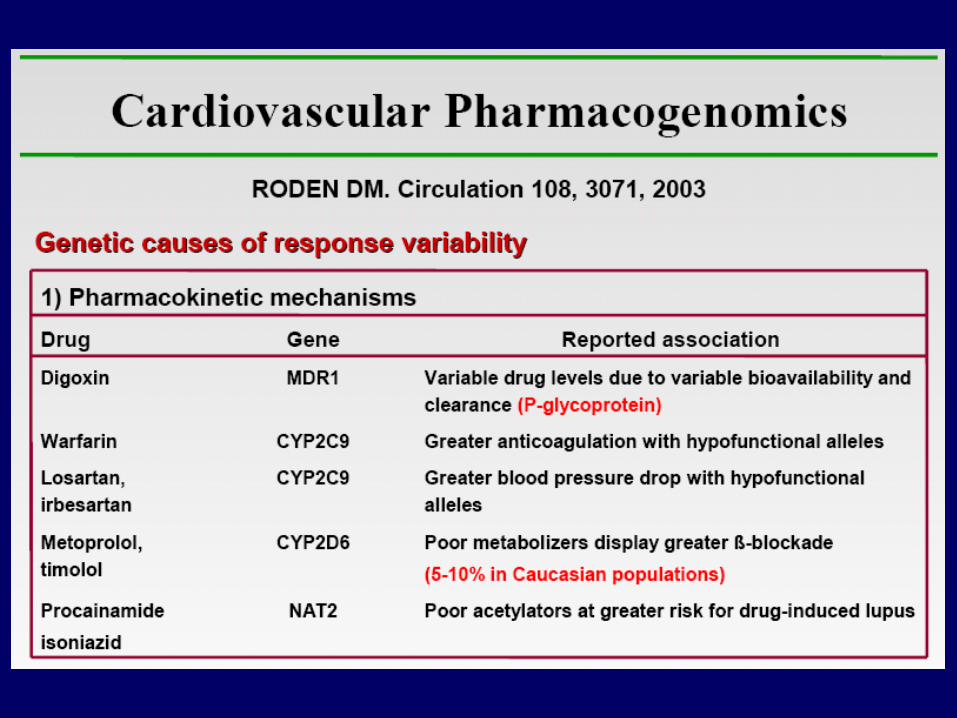
Factors of variability in drug response
PHARMACOCYNETIC
PHARMACODYNAMIC
Physiological- age- gender
Pharmacological response
Genetic - metabolic enzymes- transporters- receptors
Pathological- Liver diseases- Kidney diseases
Enviromental- concomitant therapy- diet- smoking - alcool
DRUG

Variability in drug response
The individual variability in drug response is a
clinical problem of overriding importance
The study of this variability covers an area of research
known as pharmacogenetics
The genetic variations at specific sites of the genome
are called polymorphisms.

EFFICACY OF THE PHARMACOLOGICAL TREATMENT: FAILURE OF THERAPY AND ADVERSE REACTIONS
EFFICACY
CAUSES:-Inadequate dosage
Individual genetic variability- Drug interactions
ADVERSE DRUG REACTIONS
OPERATIVE TOOLS- Pharmacological monitoring- Pharmacogenetic analysis- Pharmacovigilance
PHARMACOLOGICAL TREATMENT
Patients
FAILURE OF THERAPY

PHARMACOGENETICS: refers to “the role of geneticvariation affecting drug response or adverse reactionsto drugs” (Weinshilboum, 2003)
The likely role of genetics in potentially causingadverse drug reactions was set out in a 1957 paperwith the programmatic title “Drug Reactions, Enzymesand Biochemical Genetics” (Motulsky, 1957)
The term pharmacogenetics was coined by FriedrichVogel of Heidelberg, Germany in 1959 (Vogel, 1959)
Motulsky et al. J Zhejiang University SCIENCE 2006 7:169-170

PHARMACOGENOMICS:
The sequencing of the human genome and theintroduction of new technologies have made it possibleto analyze multiple genes simultaneously.
The newer term "pharmacogenomics" describes suchlarge-scale, often genomewide approaches.
The term was introduced in the 1990s with emergenceof the Human Genome Project and the development ofthe genome sciences.
Motulsky et al. J Zhejiang University SCIENCE 2006 7:169-170

All subjects differ in the drug response
PHARMACOGENETICS

Objectives
• To check subgroups of patients withhigh probability to response or not toa therapy
• To check subgroups of patients withhigh probability of adverse drugreactions
• To optimize the dosage
Personalized Therapy
MAX EFFICACY
+
MINOR TOXICITY

At this time pharmacogenetic label informations arereported for more than 120 drugs, and this number isincreasing more and more.
Pharmacotherapy. 2008 Aug;28(8):992-8.
Pharmacogenomic biomarker information in drug labels approved by theUnited States food and drug administration: prevalence of related drug use.
Frueh FW, Amur S, Mummaneni P, Epstein RS, Aubert RE, DeLuca TM, Verbrugge
RR, Burckart GJ, Lesko LJ.
Office of Clinical Pharmacology, Office of Translational Science, Center for Drug Evaluation and Research, U.S. Food and Drug Administration (FDA), Silver Spring, MD 20993, USA.







Tra il 10 e il 30 % dei soggetti depressi sono parzialmente o
totalmente resistenti alla terapia con antidepressivi
CAUSE GENETICHE?
DEPRESSIONE


INCLUDING ELDERLY POPULATION

Clinical, drugs interactions and pharmacogeneticsevaluation of Warfarin treatment in an elderly patient:
a case report
G. Corbi , V. Simeon , V. Conti, N. Ferrara , F. Cacciatore , A. Filippelli
Journal of Gerontology and Geriatrics 2016;64:70-72

Terapia

Esito Non sanguinamento
Allungamento tempi ospedalizzazione
Genotipizzazione Citocromo P4502C9 (CYP2C9)
Complesso Vitamina K epossido reduttasi
(VKORC1)
Risultato Metabolizzatore intermedio
(CYP2C9*1/*2)
Omozigote per VKORC1*2/*2 (richieste
ridotte dosi di Warfarin required).
Dose richiesta 1.8 mg/die (algoritmo del IWPC)
MENO DELLA METÀ DELLA DOSE PRESCRITTA




Schork. Nature 2015;520:609

In January, US President Barack Obama announced a US$215-million national Precision Medicine Initiative.
This includes, among other things, the establishmentof a national database of the genetic and other data ofone million people in the United States.
Researchers need to probe the myriad factors— genetic and environmental, among others —that shape a person’s response to a particular treatment.

It’ s time for one-person trials

It’ s time for one-person trials
A key component will be transforming everyday clinical care into solid N-of-1 trials.

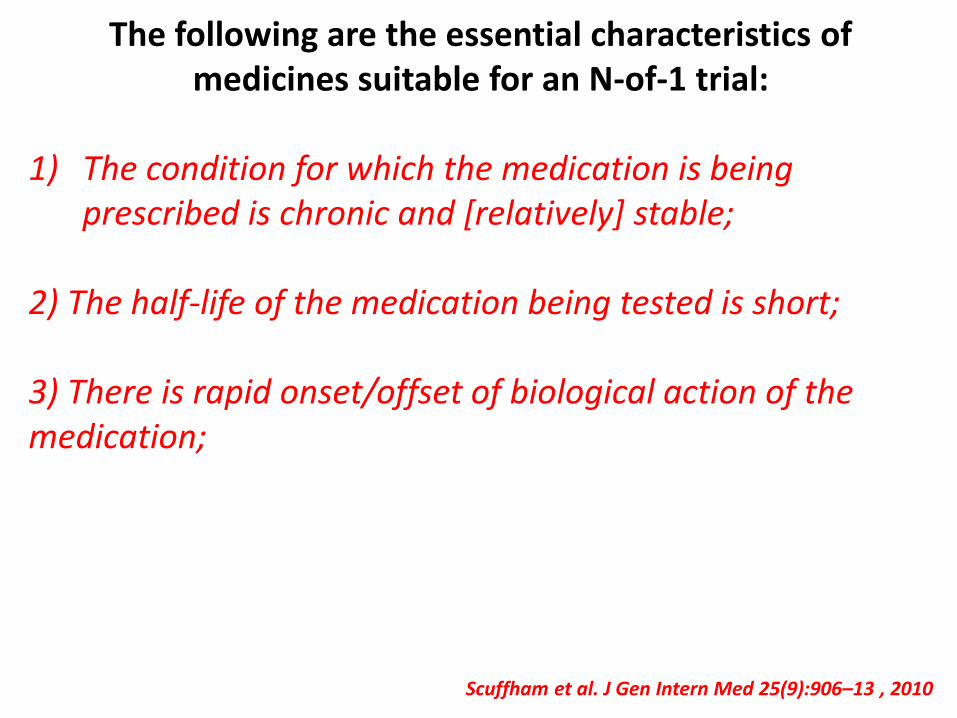
The following are the essential characteristics of medicines suitable for an N-of-1 trial:
1) The condition for which the medication is being prescribed is chronic and [relatively] stable;
Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010

The following are the essential characteristics of medicines suitable for an N-of-1 trial:
1) The condition for which the medication is being prescribed is chronic and [relatively] stable;
2) The half-life of the medication being tested is short;
Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010
The following are the essential characteristics of medicines suitable for an N-of-1 trial:
1) The condition for which the medication is being prescribed is chronic and [relatively] stable;
2) The half-life of the medication being tested is short;
3) There is rapid onset/offset of biological action of the medication;
Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010

The following are the essential characteristics of medicines suitable for an N-of-1 trial:
1) The condition for which the medication is being prescribed is chronic and [relatively] stable;
2) The half-life of the medication being tested is short;
3) There is rapid onset/offset of biological action of the medication;
4) The effect of the medication can be measured using a validated outcome measure;
Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010

The following are the essential characteristics of medicines suitable for an N-of-1 trial:
1) The condition for which the medication is being prescribed is chronic and [relatively] stable;
2) The half-life of the medication being tested is short;
3) There is rapid onset/offset of biological action of the medication;
4) The effect of the medication can be measured using a validated outcome measure;
5) The medication does not alter the underlying condition.Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010
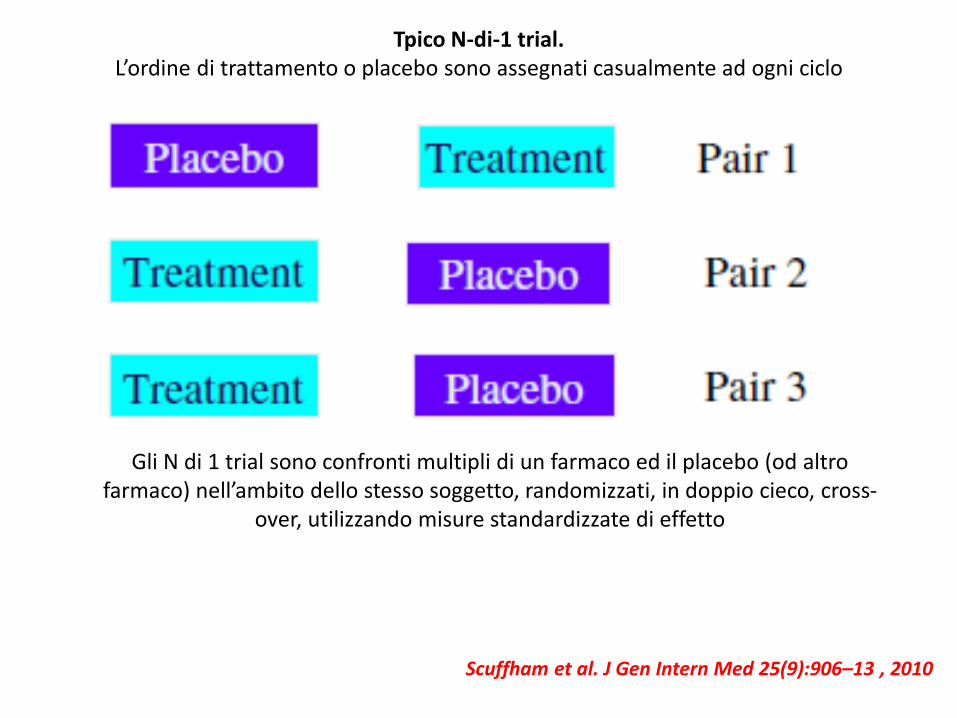
Tpico N-di-1 trial. L’ordine di trattamento o placebo sono assegnati casualmente ad ogni ciclo
Gli N di 1 trial sono confronti multipli di un farmaco ed il placebo (od altro farmaco) nell’ambito dello stesso soggetto, randomizzati, in doppio cieco, cross-
over, utilizzando misure standardizzate di effetto
Scuffham et al. J Gen Intern Med 25(9):906–13 , 2010

Scuffham et al. J Gen Intern Med 25(9):906–13, 2010

"Here's my sequence...”

AbstractIn the last century, medicine has undergone an unprecedented wave of radical changes. From the implementation of surgery up to thedevelopment of single gene-targeted therapies, clinical decision making has become increasingly complex to handle. Today, thiscomplexity needs to be rethought in the light of two emerging paradigms: evidence-based medicine (EBM) and personalizedmedicine (P-Med). The new availability of diverse sources of scientific evidence raises significant issues concerning how clinicians willcompare, evaluate and orient their decisions in front of a rapidly growing plethora of therapies, procedures, medical technologies anddrugs. In this paper, we compare the background visions behind these two paradigms, evaluating their respective relevance for presentand future clinical decision making. In particular, we argue that EBM and P-Med are driven by two diverse modes of reasoning about'evidence making' in medicine. EBM is grounded on statistical notions and epidemiological data, generally gathered through systematicmeta-reviews of randomized controlled trials; P-Med, instead, is grounded on mechanistic explanations of molecular interactions,metabolic pathways and biomarkers. While both paradigms are epistemically sound, we argue that they cannot, and should not, behybridized into a unique model. Rather, they ought to represent two compatible, but alternative ways of informing the clinicalpractice. Hence, we conclude that clinicians may expect to see their responsibility increasing as they will deal with diverse, but equallycompelling, ways of reasoning and deciding about which intervention will qualify as the 'best one' in each individual case.
AbstractIn the last century, medicine has undergone an unprecedented wave of radical changes. From the implementation of surgery up to thedevelopment of single gene-targeted therapies, clinical decision making has become increasingly complex to handle. Today, thiscomplexity needs to be rethought in the light of two emerging paradigms: evidence-based medicine (EBM) and personalizedmedicine (P-Med). The new availability of diverse sources of scientific evidence raises significant issues concerning how clinicians willcompare, evaluate and orient their decisions in front of a rapidly growing plethora of therapies, procedures, medical technologies anddrugs. In this paper, we compare the background visions behind these two paradigms, evaluating their respective relevance for presentand future clinical decision making. In particular, we argue that EBM and P-Med are driven by two diverse modes of reasoning about'evidence making' in medicine. EBM is grounded on statistical notions and epidemiological data, generally gathered through systematicmeta-reviews of randomized controlled trials; P-Med, instead, is grounded on mechanistic explanations of molecular interactions,metabolic pathways and biomarkers. While both paradigms are epistemically sound, we argue that they cannot, and should not, behybridized into a unique model. Rather, they ought to represent two compatible, but alternative ways of informing the clinicalpractice. Hence, we conclude that clinicians may expect to see their responsibility increasing as they will deal with diverse, but equallycompelling, ways of reasoning and deciding about which intervention will qualify as the 'best one' in each individual case.
THANK YOU FOR YOUR ATTENTION







