

LEUCEMIA MIELOIDE ACUTA
REPORT del Gruppo di Lavoro
Giorgina Specchia

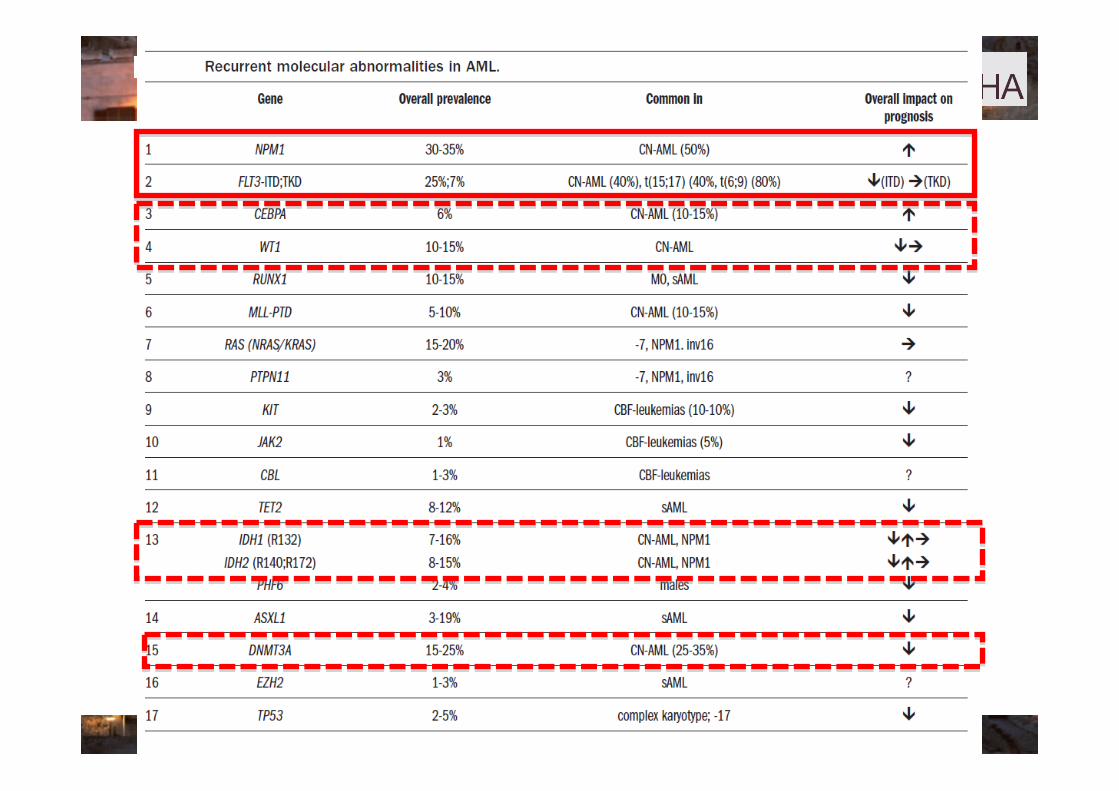
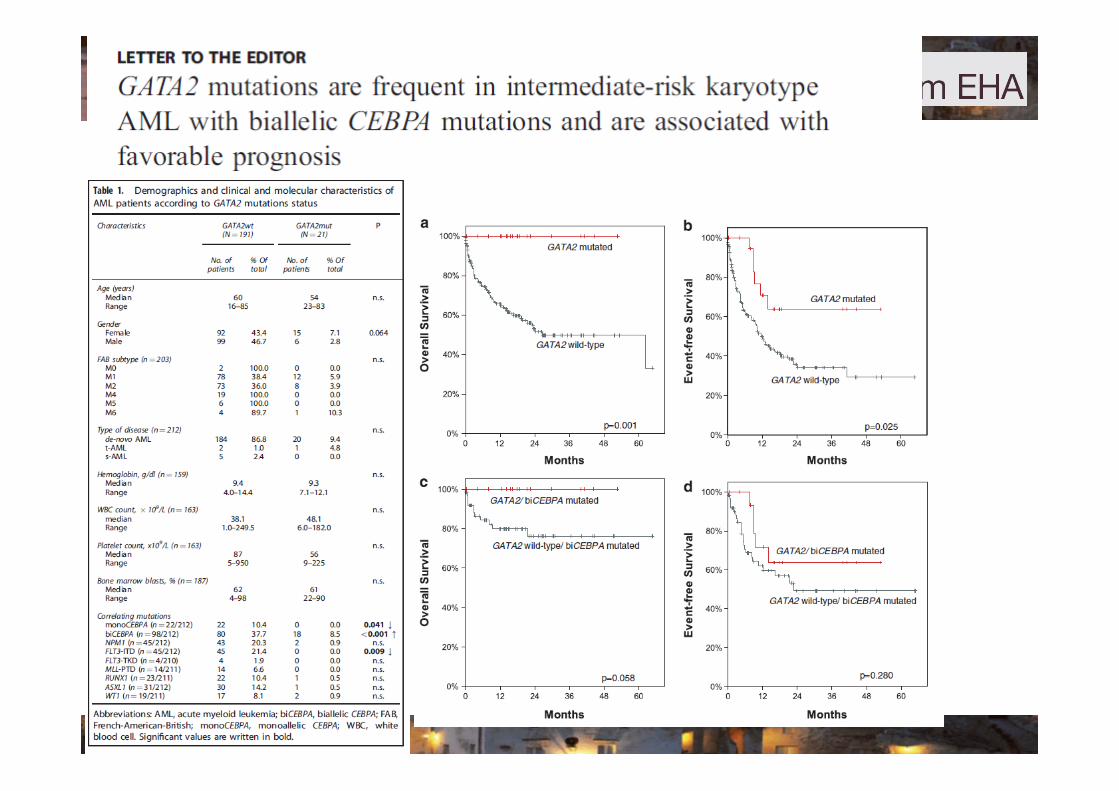
§ Rilevanza prognostica del profilo genetico integrato……..


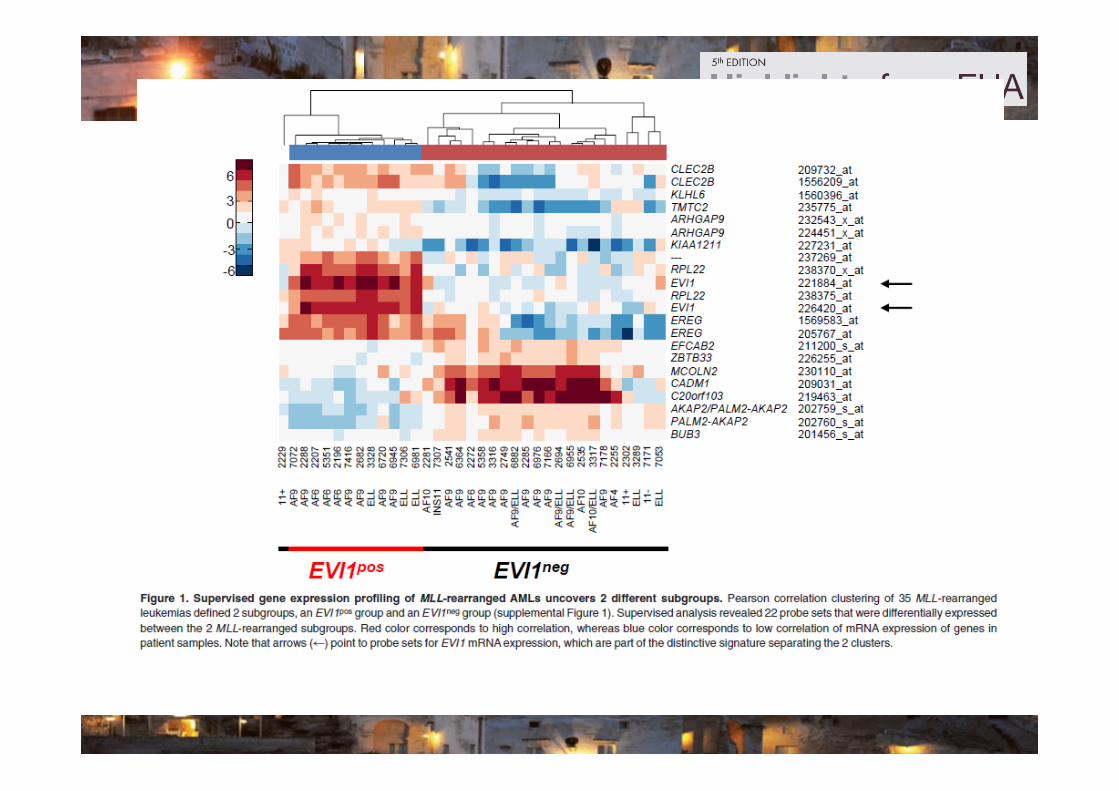
ü The proto-‐oncogene EVI1 (ecotropic viral integra;on site-‐1), located on chromosome band 3q26, is aberrantly expressed in human acute myeloid leukemia (AML) with 3q26 rearrangements.
ü Aberrant expression of EVI1 occurs in 8%-‐10% of human adult AML pa;ents and is associated with a poor outcome.
ü High expression of EVI1 was also found in leukemias with chromosomal abnormali;es, other than the ones affec;ng the EVI1 locus.
Aim: to inves;gate the frequency and the prevalence of EVI1 overexpression in a large cohort of MLLrearranged human AMLs.



GIMEMA ……… GIMEMA ,Pia.aforme macroregionali ?RETI …

AML Therapy in 2012 Younger AML

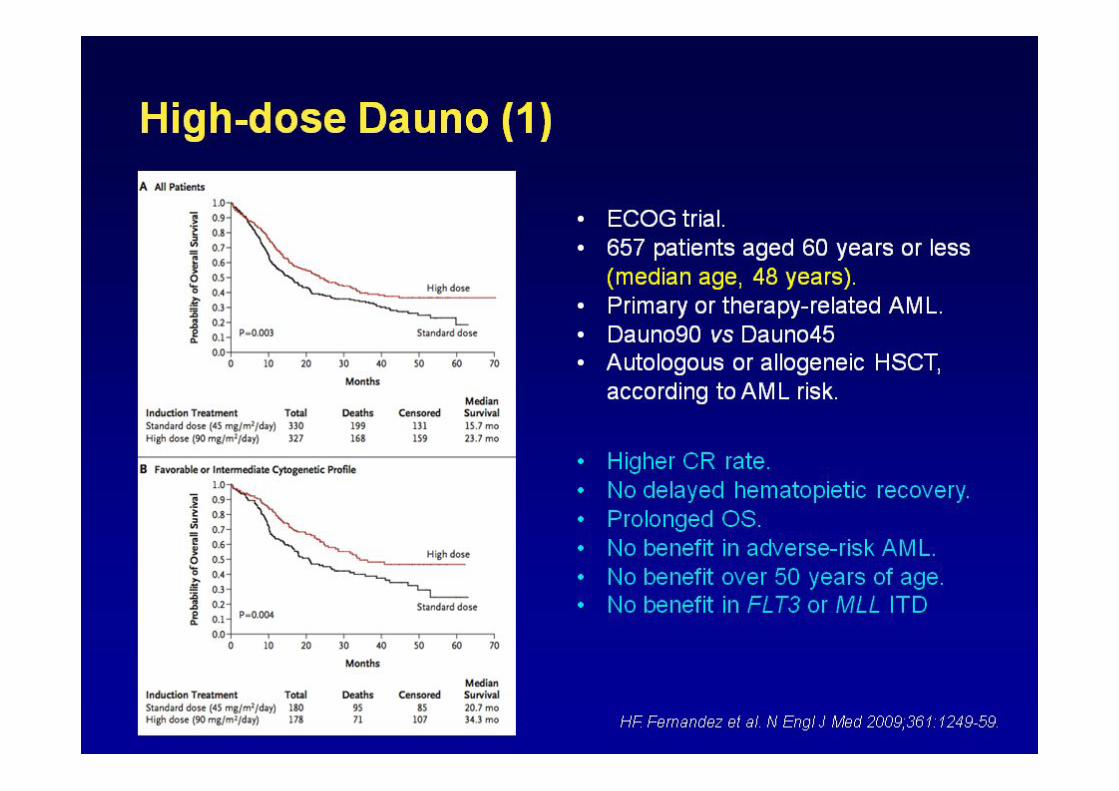
ELN Guidelines 2010 - Induction 18-60 years
ü Standard - 7 + 3
- AraC 100-200 + Dauno 60+, Ida 10-12, Mtx 10-12
- HiDAC too toxic - Phase 3 studies: SWOG 2 g x12, ALSG 3 g x 8 - Phase 2 studies: ECOG 3 g x 6, SWOG 7+3 fw by 2 g x 6 (7+3+3)
ü Promising options
- CSF priming - G-CSF: HOVON-SAKK study - GM-CSF: ALFA study
- Gemtuzumab ozogamicin (GO) - British AML15 study

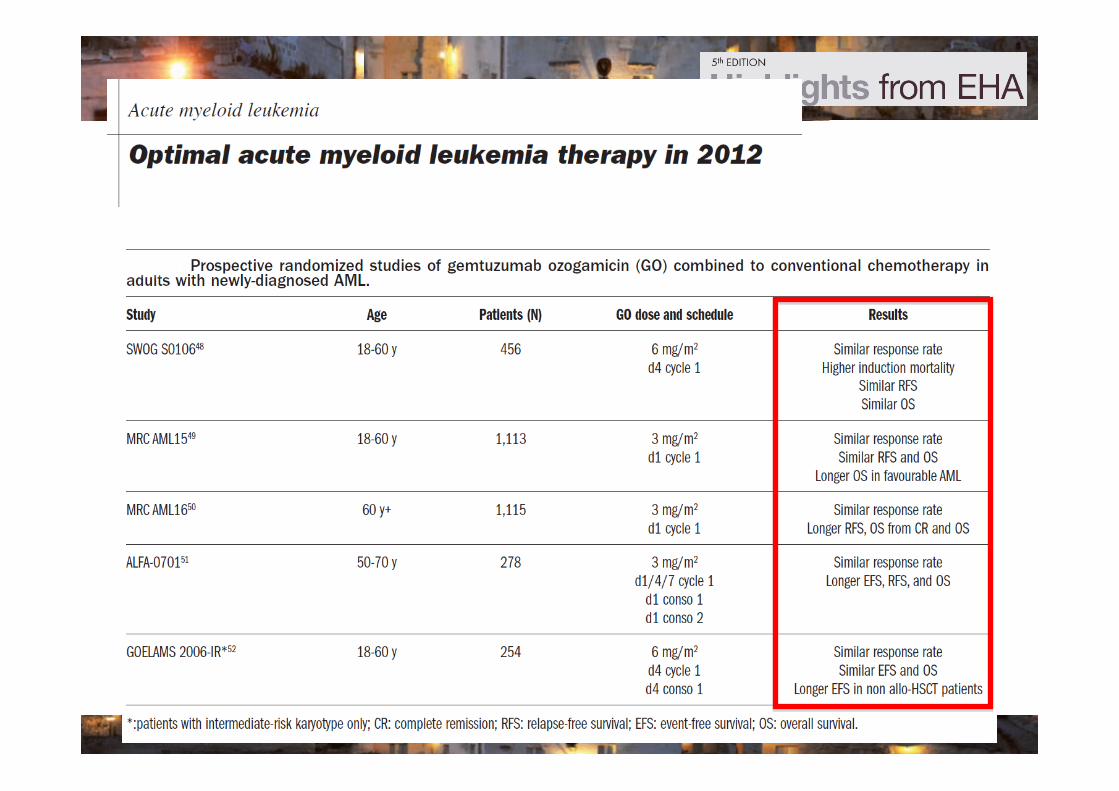

3 RCT
ALFA 0701
NCRI AML 16
E/G AML 17
AddiEon of gemtuzumab (GO)
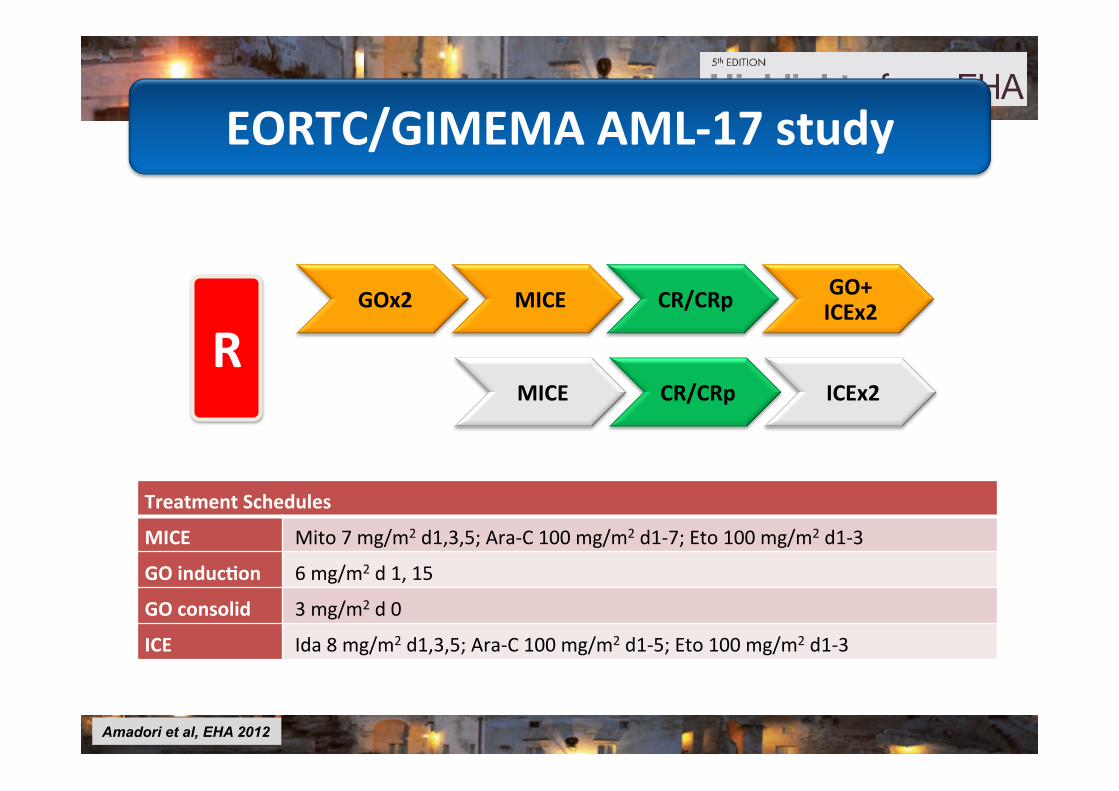
Treatment Schedules
MICE Mito 7 mg/m2 d1,3,5; Ara-‐C 100 mg/m2 d1-‐7; Eto 100 mg/m2 d1-‐3
GO inducEon 6 mg/m2 d 1, 15
GO consolid 3 mg/m2 d 0
ICE Ida 8 mg/m2 d1,3,5; Ara-‐C 100 mg/m2 d1-‐5; Eto 100 mg/m2 d1-‐3
GOx2 MICE CR/CRp GO+ ICEx2
MICE CR/CRp ICEx2 R
Amadori et al, EHA 2012
EORTC/GIMEMA AML-‐17 study

No GO GO No GO GO CR+CRp (%) 47,4 52,3 52,4 32,5 No resp (%) 40,8 29,4 29,8 31,3 Ind death (%) 9,9 11,8 15,5 26,5 Inev/unkn (%) 2 6,6 2,4 9,6
0
10
20
30
40
50
60
PaEe
nts %
Age 61-‐69 Age 70-‐75
P=0.01
Induction results by age

(years)0 1 2 3 4 5 6
0102030405060708090
100
O N Number of patients at risk : Treatment 204 236 102 61 42 30 13210 236 78 41 32 27 17
No GOGO
Logrank test: p=0.07
(years)0 1 2 3 4 5 6
0102030405060708090
100
O N Number of patients at risk : Treatment 76 84 35 21 15 9 277 83 16 5 5 4 2
No GOGO
Logrank test: p=0.002
(years)0 1 2 3 4 5 6
0102030405060708090
100
O N Number of patients at risk : Treatment 33 34 12 4 1 1 036 44 21 14 10 8 7
No GOGO
Logrank test: p=0.02
OS (all pts) OS (age 70-‐75y)
OS
sAML 61-‐69y
Survival
• Phase III randomized study of midostaurin restricted to FLT3 mutated pts younger than 60 yrs is ongoing.
• Phase II study of Quizartinib or AC220, the most selective FLT3 inhibitor available, in relapsed AML have confirmed that clonal responses could be observed with monotherapy.
Midostaurin /Quizartinib
Plerixafor, a CXCR4 antagonist blocking the
CXCR4/SDF-1 interaction has been
developed as an agent capable to mobilize
hematopoietic progenitors from the
hematopoietic niche to the peripheral blood.
Trials ongoing…………………………
Purine analogues
FLUDARABINE………… CLADRIBINE……….. CLOFARABINE…………

ü The value of allogeneic HSCT needs to be reassessed based on:
- the identification of AML genetic heterogeneity.
- the availability of different transplant sources and donor types. - The use of reduced-intensity conditioning (RIC).

AML Therapy in 2012 Older AML

• Older age per se, however, should not be a reason to withhold intensive therapy.
• Remission induction chemotherapy provides better quality of life and longer survival than supportive care only.
• Intensive chemotherapy should thus remain the standard in pts capable to tolerate it.
• The 3+7 remains the most frequently used chemotherapy induction regimen.
Standard therapy in older AML pts
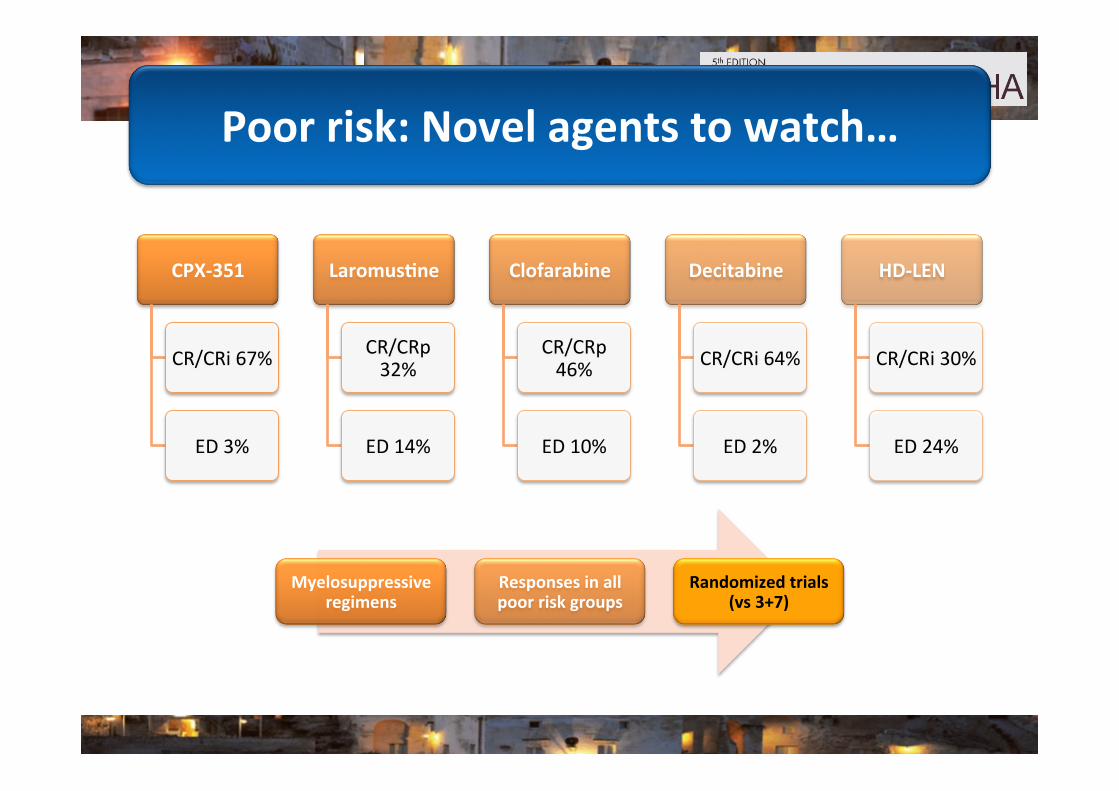
Poor risk: Novel agents to watch…
CPX-‐351
CR/CRi 67%
ED 3%
LaromusEne
CR/CRp 32%
ED 14%
Clofarabine
CR/CRp 46%
ED 10%
Decitabine
CR/CRi 64%
ED 2%
HD-‐LEN
CR/CRi 30%
ED 24%
Myelosuppressive regimens
Responses in all poor risk groups
Randomized trials (vs 3+7)

Azacitidine and Decitabine:
significant benefit in HR-MDS (and pts
with 20-30% marrow blasts), compared
with conventional care including LDAC.
Hypomethylating Agents
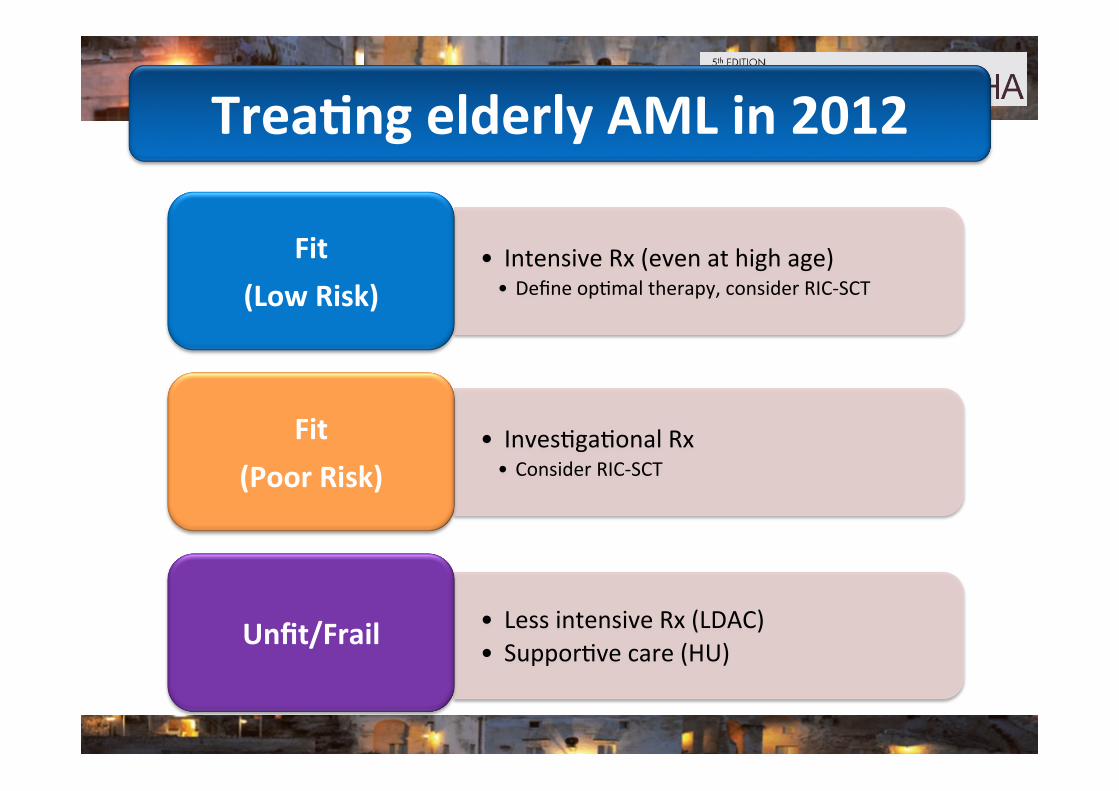
• Intensive Rx (even at high age) • Define op;mal therapy, consider RIC-‐SCT
Fit (Low Risk)
TreaEng elderly AML in 2012
• Inves;ga;onal Rx • Consider RIC-‐SCT
Fit (Poor Risk)
• Less intensive Rx (LDAC) • Suppor;ve care (HU) Unfit/Frail
Novel Agents which may have role in treaEng AML
• Hedgehog inhibitors.
• PARP inhibitors.
• Aminopep;dase inhibitors: Tosedostat
• Rigoser;b: ON 01910
• HDM2 inhibitors
• .........................







