

Storage lesionsG.D.A. SAMARANAYAKADIPLOMA TRAINEE IN TRANSFUSION MEDICINE

What are storage lesions?
Series of biochemical and biomechanical changes in red cells or platelets during ex vivo preservation that reduce their survival and function.

Storage lesions
Red cells Platelets

Red cell storage lesions - Introduction
Erythrocytes are prone to modifications due to High oxygen environment (prone to oxidative stress and hemoglobin
auto-oxidation) Absence of nucleus and other organelles – no repair mechanism
Ex vivo storage of blood Non-biological containers at non-
biological temperatures Changes in cellular biochemistry Change in normal ageing processes
that cells undergo in the body

The storage effects
Metabolic effects Biomechanical or membrane effects Oxidative effects

Metabolic effects Lack of mitochondria -> Energy
production only by glycolysis One molecule of glucose produce
two molecules of lactate two molecules of adenosine 50-
triphosphate (ATP) two protons -> increase the
acidity of the storage solution over time
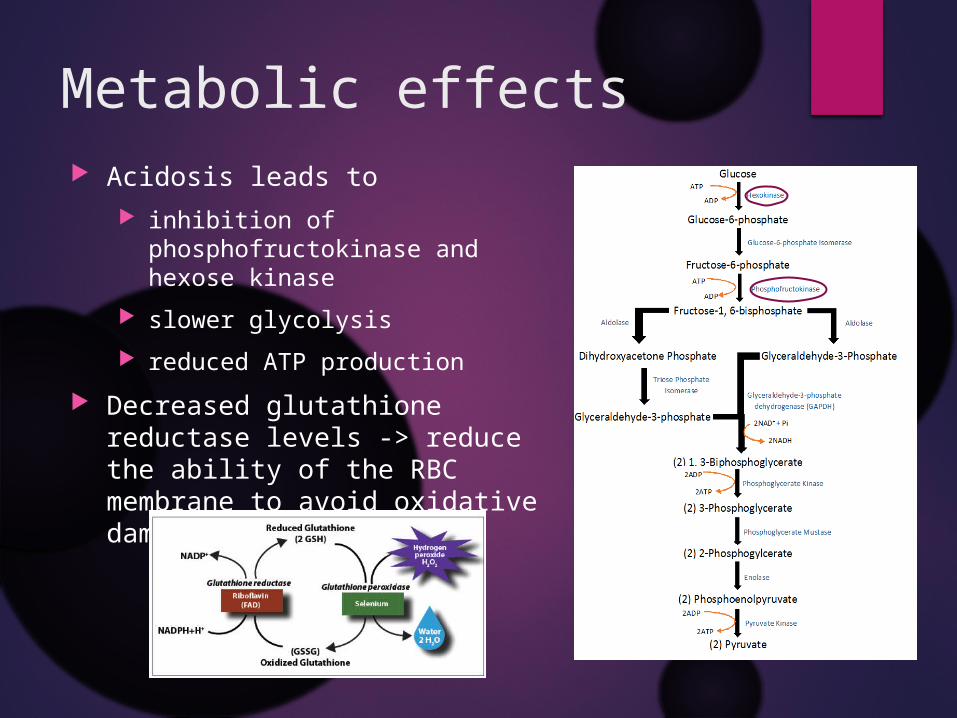
Metabolic effects Acidosis leads to
inhibition of phosphofructokinase and hexose kinase
slower glycolysis reduced ATP production
Decreased glutathione reductase levels -> reduce the ability of the RBC membrane to avoid oxidative damage

Metabolic effects The decrease in pH -> breakdown of 2,3-
diphosphoglycerate low level of 2,3-DPG leads to a left shifted oxygen
disassociation curve increase haemoglobin O2 saturation and affinity
2,3-DPG restored in vivo after transfusion one hour - 30% 24 hrs - 50% 3 days - full restoration

Metabolic effects Storage of red cells at 4 ± 2°C
helps maintain red cell functionality and viability by reducing the red cell metabolic rate.
For each one degree drop in storage temperature -> approximately a 10% decrease in red cell metabolic rate
At4°C, the metabolic rate is ten times lower than at 25°C
Metabolic activity does not completely cease when red cells are stored at cold temperature
glucose or dextrose are added to storage mediums to allow red cells to continue glycolysis.

Metabolic effects The major membrane Na+/K+ ATPase is inhibited at low
temperature continuous leakage of intracellular potassium Na+ entry in to cells
K+ accumulation in storage solution Increase the risk of hyperkalemia-induced arrhythmia Specially in vulnerable patients Ex:- neonates, renal failure patients, massive transfusions
After transfusion Na+ content normalizes in 24 hours but K+ recovery takes at least 4 days
Washing or simply removal of the supernatant is an alternative to reduce K+ toxicity for high risk patients

Biomechanical effects
Normal shape of the RBC is a biconcave disc. Maximum surface area -> efficient gas
exchange and flexibility to travel through the capillaries

Biomechanical effects The red cell membrane consists of
lipid bilayer that is interspersed with proteins The lipid bilayer includes phospholipids, cholesterol and fatty acids -> asymmetrically
distributed between the inner and outer layers Phosphatidylserine is an important component
under normal circumstances is present entirely on the inner layer, but in senescent red cells, it is expressed on the outer layer of the membrane When expressed on the outer layer -> highly thrombogenic & leads to the removal of
red cells by reticuloendothelial macrophage. Auto-oxidation of haemoglobin within the red cell leads to precipitation of
structurally distorted forms of methaemoglobin a.k.a - haemichromes near the cell membrane causes disruption of AE1 and cytoskeletal membrane proteins

Biomechanical effects Membrane changes occur in parallel with metabolic
changes RBC shape maintenance -> dependent on [ATP] Shape changes due to ATP depletion
Echinocytes/burr cells Greek – sea urchin Disk shaped cells with projections on the membrane reversible
Sphero-echinocytes With further depletion of total ATP and ADP pool spherical red cells with thorny projections decreased surface to volume ratio and deformability ->
reduce RBC post-transfusion survival Irreversible change
Microvesiculation occurs from the tips of echinocytic spines


Biomechanical effects Microvesicle (MV) release is a controlled process
stimulated by pro-apoptotic signals, shear stress or oxidative damage mechanism to remove damaged cellular components.
RBC microvesiculation ->decreased surface to volume ratio and increased cell rigidity reduction in RBC deformability occlusion in capillary beds or intravascular rupture of RBCs.
Sialic acid content decreases with storage -> reduction of the electrostatic repulsive forces that protect RBCs from aggregation blood viscosity and potentially block flow in small vessels impairment of tissue perfusion.

Biomechanical effects Inceased number of Microvesicles causes
oversaturation of the body’s clearance systems for haemolysed red cells
Haemoglobin - scavenging of endothelial-derived nitric oxide
externalised phosphatidylserine - Thrombogenic

Oxidative effects For haemoglobin to be able to reversibly bind oxygen (oxyhaemoglobin ↔
deoxyhaemoglobin) within the red cell, its component haeme-irons must be maintained in their reduced, or ferrous (Fe 2+), form.
Under normal circumstances, a small amount of oxyhaemoglobin undergoes spontaneous oxidation, generating methaemoglobin (which has oxidised or ferric (Fe3+) iron and cannot bind oxygen) and reactive oxygen species
Methaemoglobin Inherently unstable haemin (also known as ferric or oxidized haeme)
Free haemin and iron, in conjunction with reactive oxygen species, can generate highly hazardous hydroxyl radicals that can cause oxidative injury to membrane lipids and proteins.
Under normal circumstances, red cells are protected against this oxidative injury the rate of spontaneous oxidation of haemoglobin is slow NADH-dependent cytochrome-b5 reductase (CYTb5) reduces methaemoglobin back into
oxyhaemoglobin cytosolic antioxidants (primarily reduced glutathione or GSH) and membrane anti-oxidants
(primarily ascorbic acid or vitamin C) neutralise the generated reactive oxygen species.

Oxidative effects Under aerobic storage conditions ->
RBCs are constantly exposed to a pro-oxidative environment.
Superoxide dismutase and methaemoglobin reductase repair any oxidative damage via the hexose-monophosphate shunt.
Glutathione stores decline during storage likelihood of hydroxyl radical formation via
the Fenton reaction increases
Fenton’s reaction – ferrous and ferric ions react with peroxide to form hydroxyl radicles
Fe2+ + H2O2 ----> Fe3+ + .OH + OH-
Fe3+ + H2O2 ----> Fe2+ + .OOH + H+

Oxidative effects Oxidative insult to proteins and lipids
protein oxidation and lipid peroxidation formation of lysophospholipid, may contribute to
transfusion-related acute lung injury RBC function and viability deteriorate as the oxidative
injury persists over storage.


The impact of storage-induced changes
Reduction in RBC quality over time poor in vivo efficacy of stored RCC Lead to adverse post-transfusion events
Accumulation of bioactive substances in stored blood actively modify the immune function may lead to TRIM
Metabolic modulation, shape changes, altered rheological properties and oxidative injury Profressive RBC lysis release of cytosolic content and large amounts of haemoglobin ultimate manifestation of the storage lesion -> RBC is no longer
viable and can provide no therapeutic effect

The impact of storage-induced changes
• S-Nitrosothiol-Hb (SNO-Hb) release NO -> vasodilatation• SNO-Hb decays almost instantaneous following blood withdrawal• Old red cells -> insufficient NO bioavailability (INOBA )• Impaired NO production and increased NO scavenging by stored RBCs• Reduced NO levels below a critical threshold in vascular beds• vasoconstriction occurs, leading to reduced blood flow and insufficient O2
delivery to end organs.

The impact of storage-induced changes
Free haemoglobin potent inducer of oxidative stress augment the storage
lesion development Increase rate of nitric oxide (NO) scavenging by endothelial
cells leads to vasoconstriction, platelet activation and
inflammation -> clinically significant outcomes in critically ill transfusion recipients

The impact of storage-induced changes
Non-transferrin-bound iron/free iron Generates reactive oxygen species, which may in
turn cause the production of cytokines and altered immunity.
promote the growth of bacteria.

However Even if a significant storage lesion is observed during
prolonged storage, the reversible character of some of the changes and the remaining quality of RBC after prolonged storage may still be adequate for the transfused RBC to perform all of the clinically required functions
Requirements of stored RBC• 24 hours after transfusion >75% of transfused
RBC should be present in the circulationand
• At expiration the plasma Hb may not exceed 0.8% - 1%

Platelets Platelets are cellular fragments derived from the cytoplasm
of megakaryocytes Do not contain a nucleus Have mitochondria and various cytoplasmic granules. Do not possess either a golgi body or rough endoplasmic
reticulum Platelets are released and circulate approximately 9 to 12
days as small, disk-shaped cells

Biochemical changes In the resting state
15% ATP - by glycolysis 85% by TCA cycle – with O2 consumption
In the activated state 50% ATP by glycolysis - increase lactate production.
Decreased pO2 in the plastic platelet container Increasing the rate of glycolysis to compensate for the decrease in ATP
regeneration from the oxidative (TCA) metabolism This increases glucose consumption and causes an increase in lactic acid This results in a fall in pH - <6.4 after 5-7 days of storage at 22°C.
Lactic acid is buffered by bicarbonate - When the bicarbonate buffers are depleted during PC storage pH rapidly falls to less than 6.2

Activation Platelets get activated following exposure to
foreign surfaces – plastic bag low pH – metabolic alteration shear stress - during component separation
Upon activation, the platelets lose their discoid morphology and become more spherical with multiple pseudopods.
Conformational changes in GPIIb/IIIa complex exposes binding sites for adhesive proteins (fibrinogen, vWF) resulting in platelet aggregates.

ActivationPlatelet activation causes1. Release of granular contents
Function -> recruitment of leucocytes and platelets promote, immunity against infection contribute to wound healing presence of these contents in storage medium -> various
transfusion reactions2. Expression of sequestered membrane proteins (CD62, CD63)
& phospholipids Negatively charged phospholipids providing a surface for the
prothrombinase complex (X-Va) thereby contributing to procoagulant activity

Activation Agitation while storage cause platelet lysis and calpain
(protease) activation Platelet lysis
discharge cytosolic lactate dehydrogenase (LDH) and granular contents
accumulation in the storage solution Activation of calpain
degradation of cytoskeletal proteins like actin generate platelet microvesicles.
Microvesicle formation leads to decrease in mean platelet volume (MPV) and also contributes to procoagulant activity

Assessment of platelet storage lesions
Biochemical tests - assess platelet viability pH, pO2, LDH accumulation, glucose consumption, and ATP
depletion Assess alterations in the discoid morphology
Swirling phenomenon decrease in MPV
Platelet activation markers – various assays can be used release of specific granular contents (β thromboglobulin,
platelet factor 4) changes in GP expression on platelet surface (GPIb, GPIIb,
and GPIIIa)


RCC and Platelets Stored PRBC and platelet transfusions seem to upregulate pro-
inflammatory gene expression in the leukocytes of the transfusion recipient.
Cytokines and chemokines that have been shown to increase during storage of RBCs and platelets are Interleukin (IL)-1β, IL-6, IL-8, Tumor necrosis factor-α Myeloperoxidase (MPO) neutrophil-activating peptide-2 (NAP-2) Monocyte Chemoattractant Protein-1 (MCP-1)
RANTES (regulated on activation, normal T cell expressed and secreted; CCL5) - associated with allergic reactions
IL-6, IL-8, and MCP-1 - may be associated with TRALI Fas ligand and TGF-β - may contribute to transfusion-related immune
modulation.

How to extend the storage duration

Additive solutions Greater plasma recovery from whole blood donations for
transfusion or fractionation Minimization of the adverse effects mediated by plasma
allergic and FNHTRs transfusion-related acute lung injury Use of photochemical pathogen reduction technologies,
because the presence of plasma may interfere with the technology system
Potential improvements in platelet & RBC storage through manipulation of the storage medium.
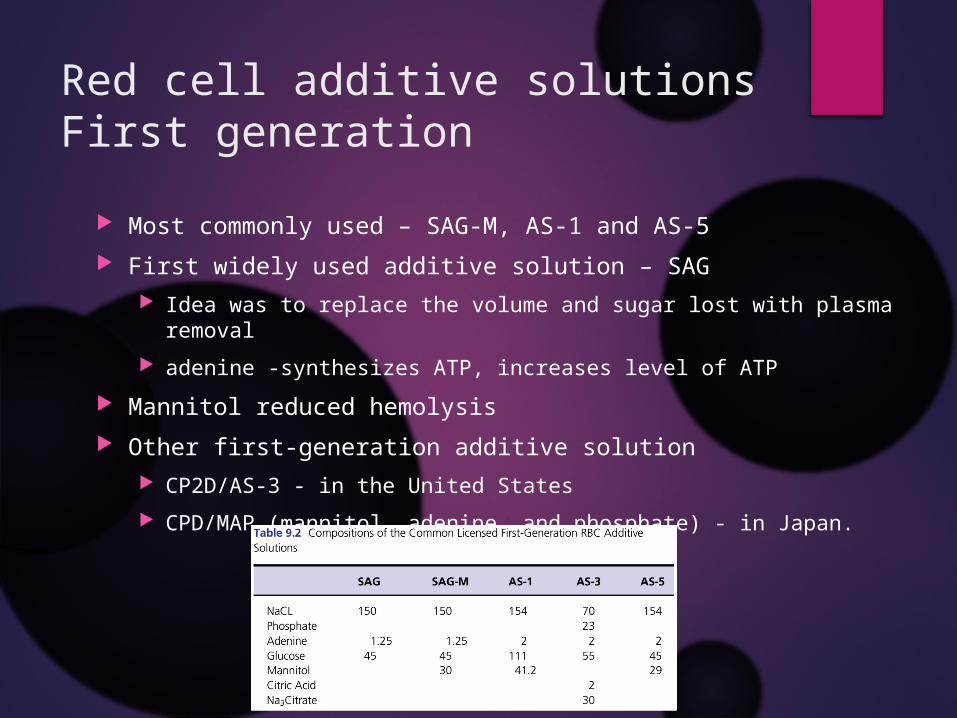
Red cell additive solutionsFirst generation
Most commonly used – SAG-M, AS-1 and AS-5 First widely used additive solution – SAG
Idea was to replace the volume and sugar lost with plasma removal adenine -synthesizes ATP, increases level of ATP
Mannitol reduced hemolysis Other first-generation additive solution
CP2D/AS-3 - in the United States CPD/MAP (mannitol, adenine, and phosphate) - in Japan.

Red cell additive solutionsSecond generation
Addition of phosphate and bicarbonate Buffers protons and reduce acidity
Guanosine guanosine triphosphate was detected in red cells and known to
decrease during storage. However, guanosine nucleotides - minimal role in critical events
in RBC storage, inhibiting the primitive coagulation enzyme transglutaminase.

Platelet additive solutions Acetate
efficiently substitute in the citric acid cycle decreasing both the glycolytic rate and lactic acid generation. Acetate must also be transformed to acetic acid to enter the cycle, removing hydrogen ions
produced by the anaerobic metabolism of glucose This bicarbonate-sparing buffering effect also helps preserve pH
Most commercially available PASs do not contain additional glucose glucose carmelizes upon heat sterilization at the neutral or slightly basic PAS pHs
Citrate important in maintaining anticoagulation However upregulates glycolysis and make platelets more susceptible to activating stimuli.
use of the lowest possible concentrations of citrate in the medium Phosphate serves as a buffer Magnesium and potassium - decrease platelet activation and may downregulate glycolysis

Storage containers Plays a major role in storage lesions Allows gas exchange – depends on the thickness of the bag & gas
transport capacity of the material. Polyvinyl chloride (PVC) bags plasticized with Di(2-ethylhexyl)
phthalate (DEHP) - standard RBC and platelet storage containers. The presence of DEHP reduces hemolysis by fourfold during storage by
intercalating into the red cell membrane. Used in most of the countries.
PVC bags plasticized with butyryl-n-trihexyl citrate more expensive Sweden, Spain, and Norway have an unusual smell when initially unwrapped.
Newer plastic bags have higher gas permeability polyolefin with no plasticizer (Baxter's PL 732) thin walled PVC with tri-(2-ethylhexyl)trimellate plasticizer (TOTM)

Storage under anaerobic conditions - RCC
Researchers have demonstrated that anaerobic storage can slower the decreases in 2,3-DPG and ATP levels decrease production of free radicles and membrane
damage Vox Sang. 2007 Jan;92(1):22-31. Extended storage of red blood cells under
anaerobic conditions. Yoshida T1, AuBuchon JP, Tryzelaar L, Foster KY, Bitensky MW.
Transfusion. 2009 Mar;49(3):458-64. doi: 10.1111/j.1537-2995.2008.02038.x. Epub 2009 Jan 2. Anaerobic storage of red blood cells in a novel additive solution improves in vivo recovery. Dumont LJ1, Yoshida T, AuBuchon JP.

Rejuvenation Red cells at the end of storage time - low pH, ATP and 2,3-DPG
concentrations. Rejuvenation - metabolic recharging of red cells at the end of their
storage period. By incubation in a high-pH solution of phosphate, inosine, pyruvate, and
adenine for 2 hours. Increases red cell ATP and 2,3-DPG concentrations and increases their in
vivo recovery Restored normal distribution of phospholipids - prevents red cells from
participating in plasma coagulation reactions. Rejuvenation does not reverse the oxidative damage to cell membrane Ex - Rejuvesol - Cytosol Labs

Pre transfusion washing Reduce inflammation markers. Association with fewer transfused blood units, and
decreased mortality. Remove accumulated storage-related compounds
(potassium and lactate). Older erythrocytes are lysed during the washing process.
induce higher hemolysis and MV release reduced transfusion-induced impaired vascular function

Frozen storage of red cells and platelets
Freezing significantly reduces the metabolic rate Cryopreservative agents helps to reduce intracellular
dehydration and mechanical damage due to water crystal forming during freezing process
platelets at -80°C with DMSO - shelf life up to 2 years. Red cells at -80°C with glycerol – up to 10 years
Cryopreservation and Freeze-Drying Protocols - Volume 368 of the series Methods in Molecular Biology™ pp 283-301
Referances

Thank you







