
Study sponsors
LASA: Low dose Atazanavir/r vs. Standard dose Atazanavir/r
The LASA studyAtazanavir/ritonavir 200/100 mg is Non-inferior to
300/100 mg in Virologic Suppressed HIV-infected Thai Adults
a multicentre, randomized, open-label trial
Torsak Bunupuradah, Sasisopin Kiertiburanakul, Anchalee Avihingsanon, Ploenchan Chetchotisakd, Malee Techapornroong, Niramon Leerattanapetch, Pacharee
Kantipong, Chureeratana Bowonwatanuwong, Sukit Banchongkit , Virat Klinbuayaem, Sripetcharat Mekviwattanawong, Sireethorn Nimitvilai, Supunnee
Jirajariyavej, Wisit Prasithsirikul, Warangkana Munsakul, Sorakij Bhakeecheep, Sushada Chaivooth, Praphan Phanuphak, David A Cooper, Tanakorn Apornpong,
Stephen J. Kerr, Sean Emery, Kiat Ruxrungtham on behalf of the LASA Study Group

Introduction • WHO recommends boosted protease inhibitors,
lopinavir/ritonavir (LPV/r) or atazanavir/ritonavir (ATV/r) as the preferred second-line therapy 1
• ATV/r-based regimen had lower pill burden, and less metabolic adverse effects compared to LPV/r-based regimen 2,3
1 WHO guideline 20132 Soriano et al. JAC 2008
3 Mallolas et al. JAIDS 2009
ATV/r0
1020304050607080
41
72
42
Caucasians ATV/r 300/100
Thais ATV/r 300/100
Thais ATV/r 200/100
Ritonavir-boosted Protease Inhibitor
Med
ian
AU
C (h
*mm
g/L)
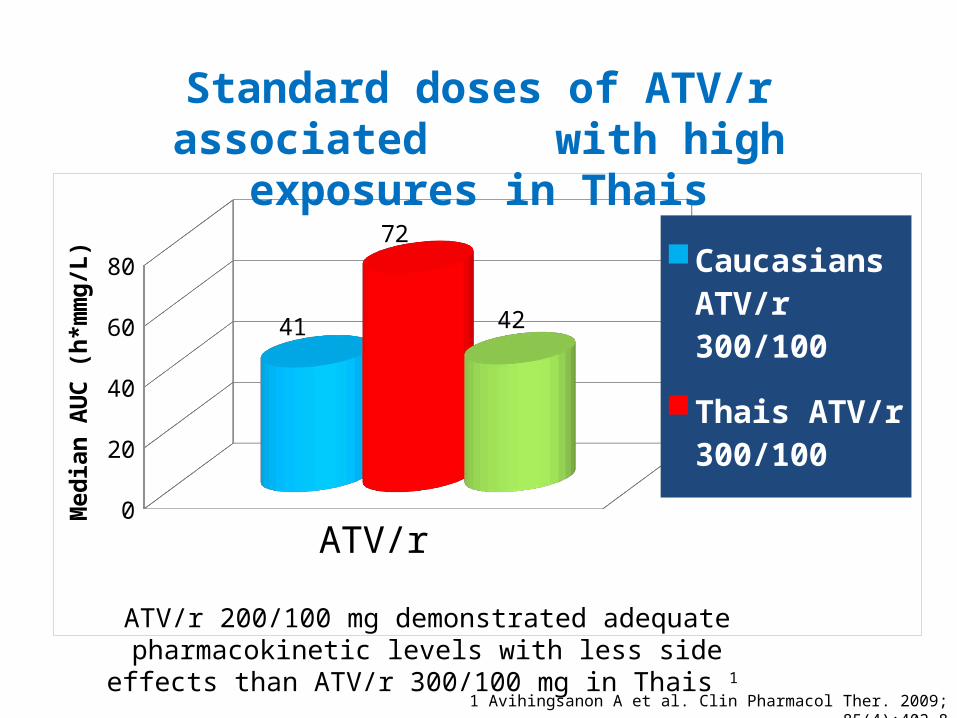
Standard doses of ATV/r associated with high exposures in Thais
ATV/r 200/100 mg demonstrated adequate pharmacokinetic levels with less side effects than ATV/r 300/100 mg in Thais 1
1 Avihingsanon A et al. Clin Pharmacol Ther. 2009; 85(4):402-8
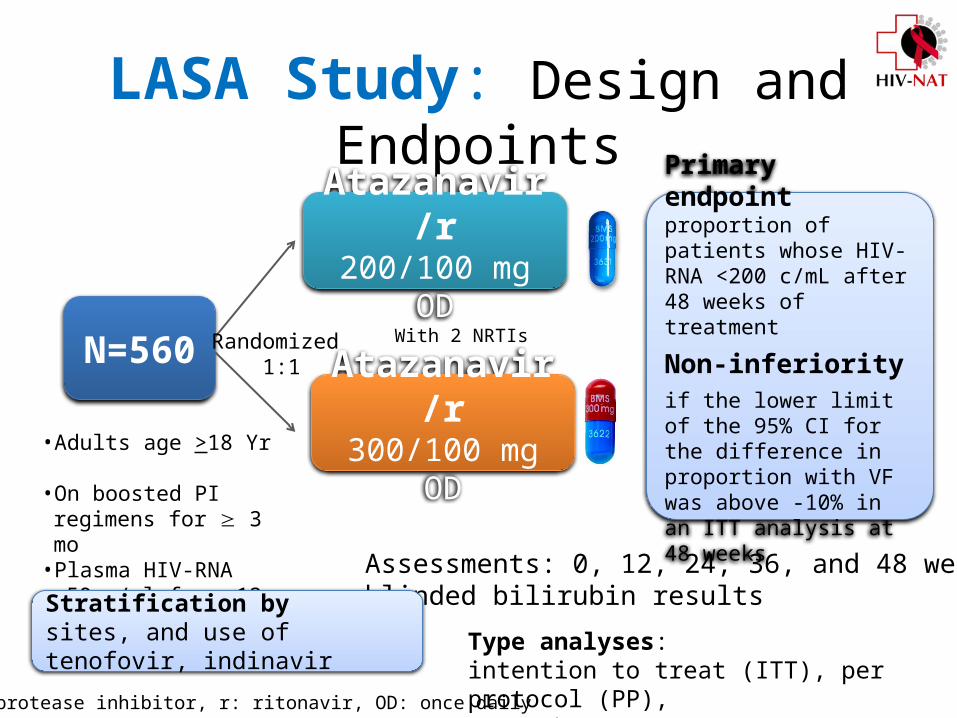
LASA Study: Design and Endpoints
N=560
• Adults age >18 Yr • On boosted PI regimens
for 3 mo• Plasma HIV-RNA <50 c/ml
for 12 mo
Atazanavir/r300/100 mg OD
Atazanavir/r200/100 mg OD
With 2 NRTIsRandomized 1:1
Primary endpoint proportion of patients whose HIV-RNA <200 c/mL after 48 weeks of treatment
Non-inferiorityif the lower limit of the 95% CI for the difference in proportion with VF was above -10% in an ITT analysis at 48 weeks
Assessments: 0, 12, 24, 36, and 48 weeksblinded bilirubin results
Stratification by sites, and use of tenofovir, indinavir
PI: protease inhibitor, r: ritonavir, OD: once daily
Type analyses: intention to treat (ITT), per protocol (PP), snap shot (non-completer=failure) analysis

14 study sites
Prapokklao HospitalChonburi HospitalRayong Hospital
Pranangklao HospitalNakorn Phatom Hospital Bamrasnaradura Institute
14 LASA study sites
HIV-NAT, TRCARCRamathibodi HospitalTaksin HospitalVajira Hospital
Sanpatong Hospital
Khon Kaen UniversityKhon Kaen Hospital
Chiangrai Prachanukroh Hospital
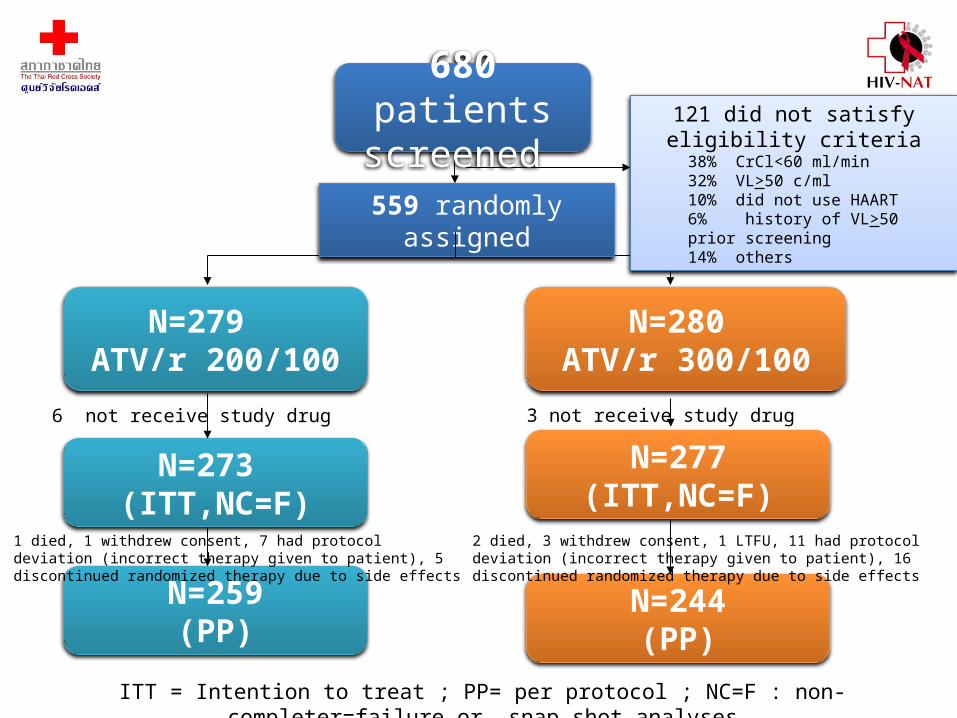
121 did not satisfy eligibility criteria38% CrCl<60 ml/min32% VL>50 c/ml10% did not use HAART6% history of VL>50 prior screening14% others 559 randomly assigned
ITT = Intention to treat ; PP= per protocol ; NC=F : non-completer=failure or snap shot analyses
680 patients screened
N=279 ATV/r 200/100
N=280 ATV/r 300/100
N=273 (ITT,NC=F)
N=259(PP)
6 not receive study drug
1 died, 1 withdrew consent, 7 had protocol deviation (incorrect therapy given to patient), 5 discontinued randomized therapy due to side effects
3 not receive study drug
N=277(ITT,NC=F)
N=244(PP)
2 died, 3 withdrew consent, 1 LTFU, 11 had protocol deviation (incorrect therapy given to patient), 16 discontinued randomized therapy due to side effects
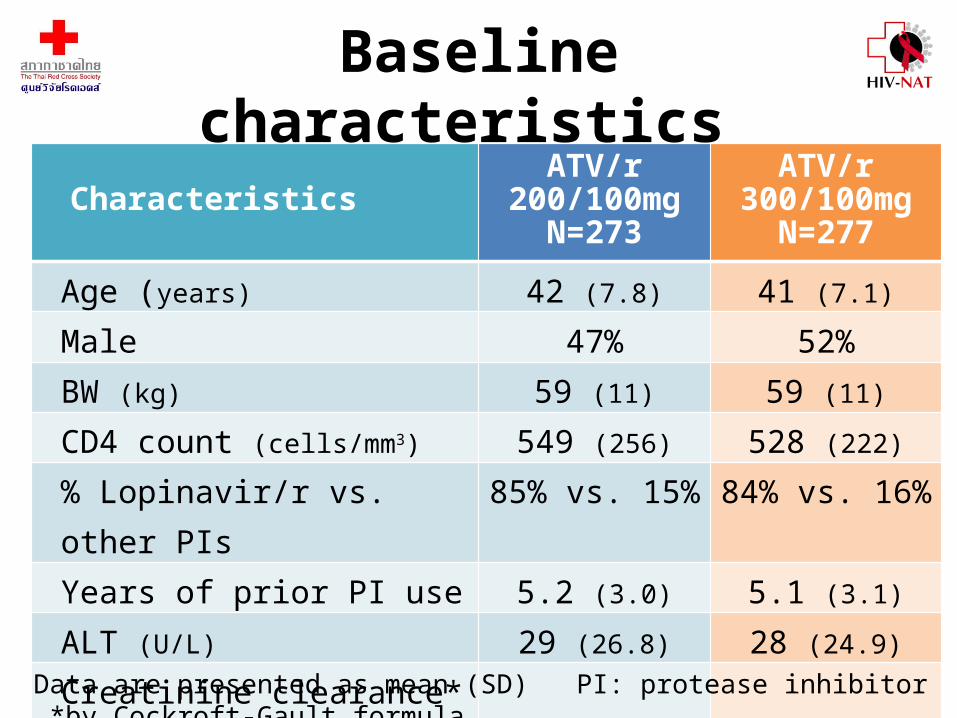
Baseline characteristics
CharacteristicsATV/r
200/100mgN=273
ATV/r 300/100mg
N=277Age (years) 42 (7.8) 41 (7.1)Male 47% 52%BW (kg) 59 (11) 59 (11)CD4 count (cells/mm3) 549 (256) 528 (222)% Lopinavir/r vs. other PIs 85% vs. 15% 84% vs. 16%Years of prior PI use 5.2 (3.0) 5.1 (3.1)ALT (U/L) 29 (26.8) 28 (24.9)Creatinine clearance* (mL/min) 94.6 (25.9) 95.7 (25.8)
Data are presented as mean (SD) PI: protease inhibitor *by Cockroft-Gault formula
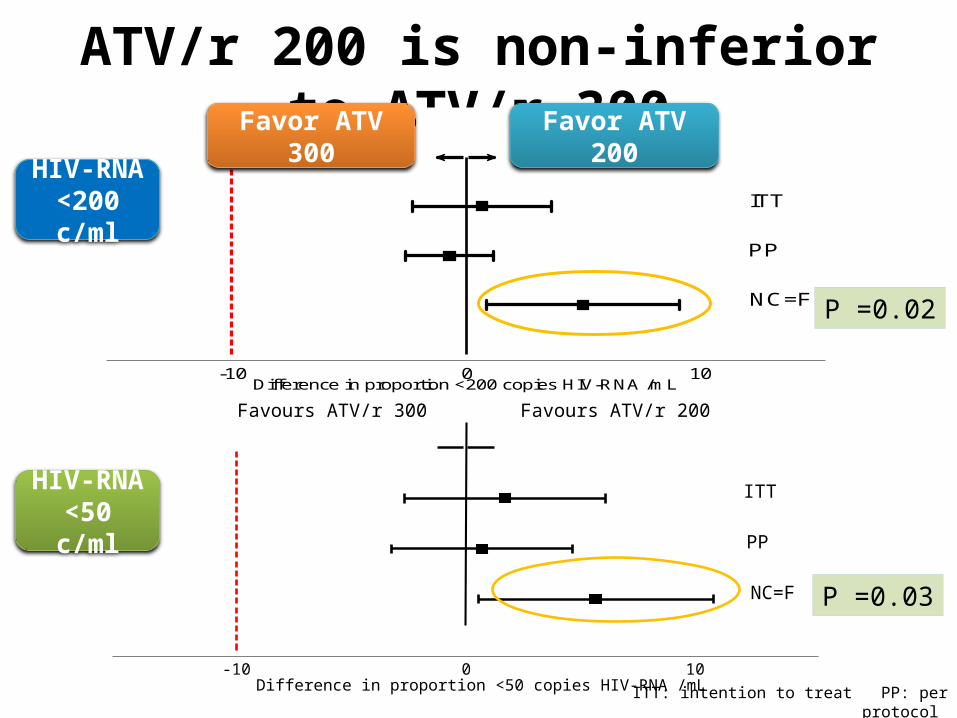
ATV/r 200 is non-inferior to ATV/r 300Favours ATV/r 300 Favours ATV/r 200
NC=F
PP
ITT
-10 0 10 Difference in proportion <200 copies HIV-RNA /mL
P =0.02
HIV-RNA <200 c/ml
Favor ATV 300 Favor ATV 200
Favours ATV/r 300 Favours ATV/r 200
NC=F
PP
ITT
-10 0 10 Difference in proportion <50 copies HIV-RNA /mL
ITT: intention to treat PP: per protocol NC=F: non-completer equal to failure/snap shot
P =0.03
HIV-RNA <50 c/ml

% Patients with suppressed HIV-RNA at week 48
ITT PP NC=F0
20
40
60
80
100 97 99 9696 9991
ATV/r200
ATV/r300
ITT PP NC=F0
20
40
60
80
100 93 95 9292 9486
ATV/r200ATV/r300
HIV-RNA <200 c/ml
HIV-RNA <50 c/ml
P =0.03
P =0.02P =NS
P = NS
P = NS
P = NS
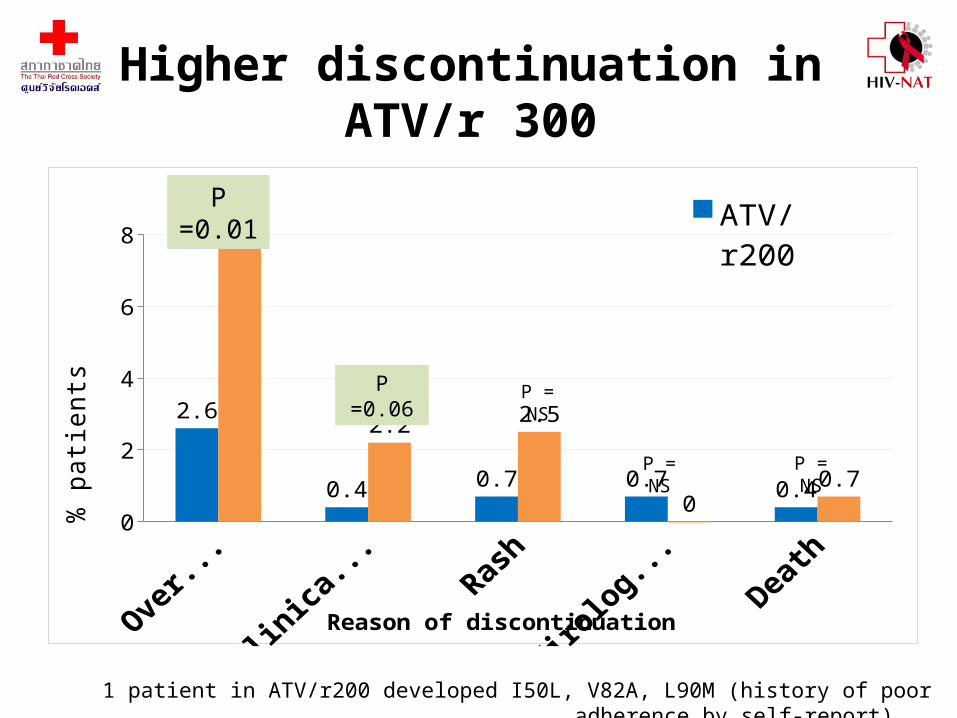
Higher discontinuation in ATV/r 300
Overall Clinical Jaundice
Rash Virologic Failure
Death0
2
4
6
8
2.6
0.4 0.7 0.7 0.4
7.6
2.2 2.5
00.7
ATV/r200ATV/r300
Reason of discontinuation
% p
atien
ts
P =0.01
P =0.06 P = NS
P = NS P = NS
1 patient in ATV/r200 developed I50L, V82A, L90M (history of poor adherence by self-report).
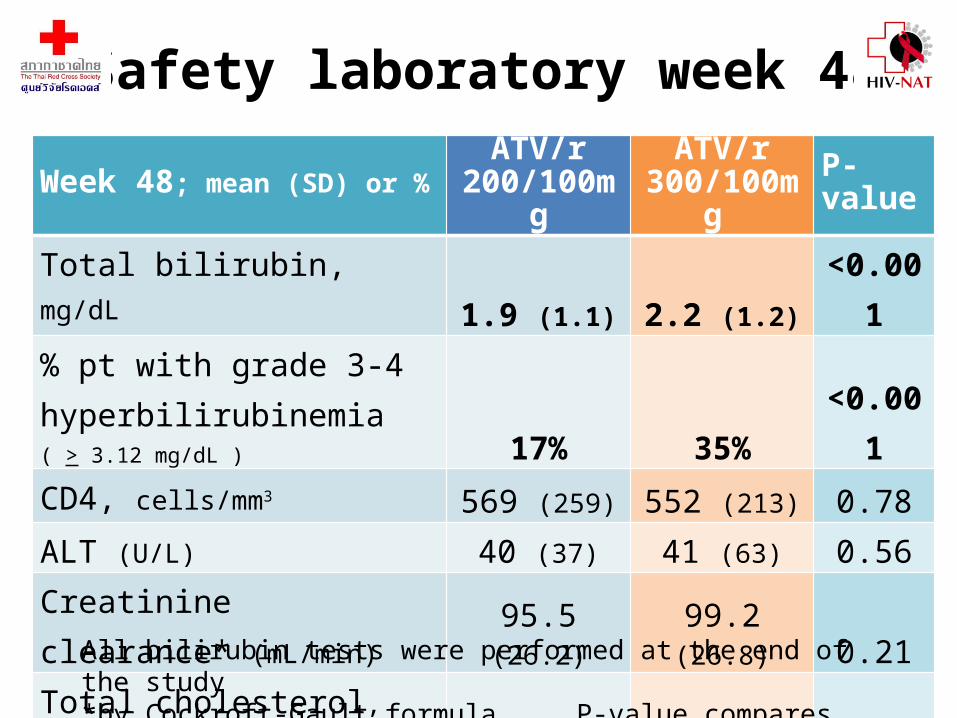
Safety laboratory week 48
Week 48; mean (SD) or %ATV/r
200/100mgATV/r
300/100mg P-value
Total bilirubin, mg/dL 1.9 (1.1) 2.2 (1.2) <0.001% pt with grade 3-4 hyperbilirubinemia ( > 3.12 mg/dL ) 17% 35% <0.001CD4, cells/mm3
569 (259) 552 (213) 0.78ALT (U/L) 40 (37) 41 (63) 0.56Creatinine clearance* (mL/min) 95.5 (26.2) 99.2 (26.8) 0.21Total cholesterol, mg/dL 196 (43.4) 187 (38.8) 0.07Triglyceride, mg/dL 176 (107.4) 182 (120.1) 0.27
All bilirubin tests were performed at the end of the study*by Cockroft-Gault formula P-value compares mean change from baseline
2015 2016 2017 2018 20190
2
4
6
8
10
12
14
16
910
1113
14
Cost
Sav
ing
(mill
ion
USD
)
300 mg 200 mg
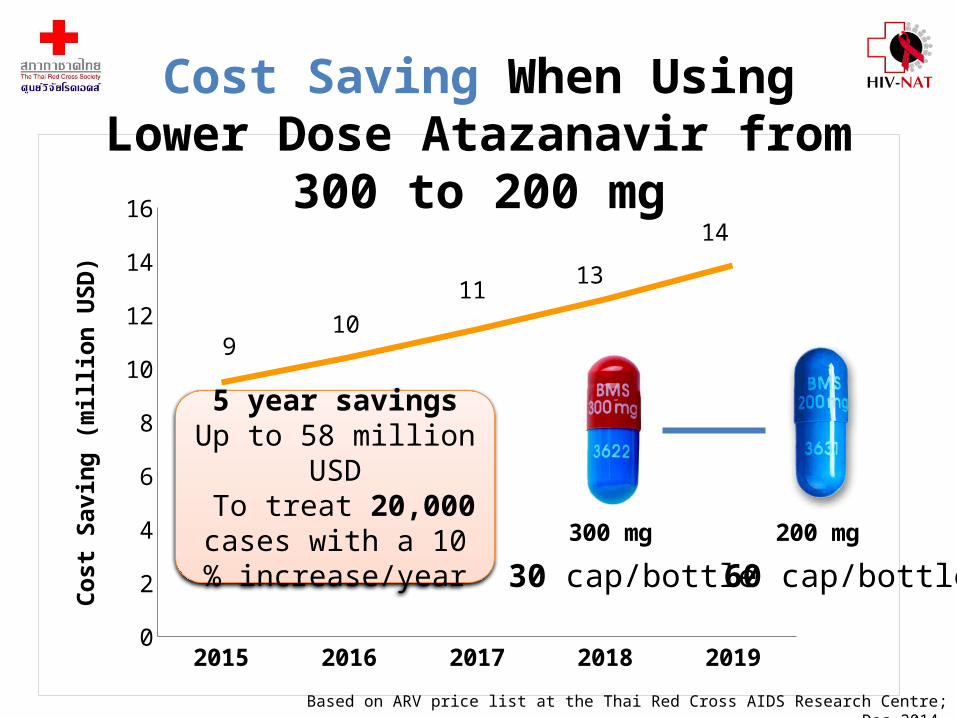
Cost Saving When Using Lower Dose Atazanavir from 300 to 200 mg
30 cap/bottle 60 cap/bottle
5 year savingsUp to 58 million USD To treat 20,000 cases
with a 10 % increase/year
Based on ARV price list at the Thai Red Cross AIDS Research Centre; Dec 2014
Conclusions • ATV/r 200 mg is non-inferior in terms of virologic
efficacy to ATV/r 300 mg by ITT, PP and SNAPSHOT analyses
• By SNAPSHOT, ATV/r 200 is superior to ATV/r 300-Higher discontinuation rate due to intolerance in ATV/r300 versus ATV/r200
Study limitations
• The applicability to other ethnicities, larger body weights is not known
• The results are not generalizable to patients with treatment naïve or failing first-line therapy

AcknowledgementsWe thank all LASA participantsLASA Study team KhonKaen University :Ploenchan Chetchotisakd, Piroon Mootsikapun, Siriluck Anunnatsiri, Ratthanant Kaewmart, Viraphong Lulitanond, Parichat Seawsirikul, Anchalee Tiyabut, Sunattana PanilChonburi Hospital: Chureeratana Bowonwatanuwong, Hutsaya Tantipong, Prakit Yothipitak, Uangarun Ampunpong, Suluck Soontaros Chiangrai Prachanukroh Hospital: Pacharee Kantipong, Suwimon Saejung, Sawat Petcharat, Worarat Imsanguan, Pottjavitt Ussawawuthipong, Ruengrit Jinasen, Phakamas Kumbua, Nussara Khampachua, Supawadee Pongprapass, Juthamas LimlertjareonwanitSanpatong Hospital, ChiangMai: Virat Klinbuayaem, Utoomporn Kumpeerapanya, Pranee Leechanachai, Phennapha Klangsinsirikul, Yaowaluk Siriwarothai, Chokannikar Tunkham, Prathum Tachorn, Channat PrompingBamrasnaradura Infectious Disease Institute, Nonthaburi: Wisit Prasithsirikul, Patama Sutha, Unchana Thawornwan, Supeda Thongyen, Anongnuch NarkkhoksungRamathibodi Hospital, Mahidol University: Sasisopin Kiertiburanakul, Somnuek Sungkanuparph, Laor Chumla, Nutaporn SanmeemaTaksin Hospital: Supunnee Jirajariyavej, Kittipong Kongchan, Plernta Sirimanuwat, Ratchada Wattanasopon, Jaratsri Itsariyathanakorn, Jittikarn SuthisiriVajira Hospital: Warangkana Munsakul, Wisanee Phesajcha, Orranuch Teansuwan, Nawaporn Sae-kao, Wipawan KarakateKhon Kaen Hospital: Niramon Leerattanapetch, Pornrith Pisuttimarn, Duangkamon Aeksomtaramet, Wilasinee Kamonmitr, Janyarat Tamangklang, Mathana Mitchai, Netchanok Moolmanee, Sookpanee Wimonklang, Supranee Naprasert, Thawarat KhotphuwiangPrapokklao Hospital: Malee Techapornroong, Supavadee Tongsakulrungraeng, Somwadee Sriatcha, Monthip Ratchatawijin, Pathanee TearsonsernNakhon Pathom Hospital: Sireethorn Nimitvilai, Panita Kapol, Sutas Bounyong, Tussanee Theerakul, Rapeepun SirithaemkhuntiRayong Hospital: Sukit Banchongkit, Nopadol Yueannuwong, Waraporn KaewvilaiPranangklao Hospital: Sripetcharat Mekviwattanawong, Oomporn Changsuphan, Nareerat Yungyuen, Jhanya Kirtma, Jariya Padungpattanodom, Kingtong WongsirikulChulalongkorn University: Kiat RuxrungthamHIV-NAT, the Thai Red Cross AIDS Research Centre: Kiat Ruxrungtham, Anchalee Avihingsanon, Torsak Bunupuradah, Vorapot Sapsirisavat , Jintanat Ananworanich, Nadia Kancheva Landolt, Wasana Prasitsuebsai, Anuntaya Uanithirat, Sasiwimol Ubolyam, Apicha Mahanontharit, Naphassanant Laopraynak, Peeraporn Kaew-on, Duangsamorn Taechamahapun, Chalandakorn Ruengprasertkit, Jintana Intasan, Walairat Charoenporn, Jaravee Jamthong, Bencharat Thongpunchang, Tanakorn Apornpong, Stephen J KerrKirby Institute for Infection and Immunity in Society, UNSW, Sydney, Australia: Wendy Lee, Alli Humphries, Jessica Taylor, Stephen J Kerr, David Cooper, Sean Emery







