A Global Perspective on Spinal Cord Injury Epidemiology
ALUN ACKERY,1 CHARLES TATOR,2 and ANDREI KRASSIOUKOV1,3
ABSTRACT
Spinal cord injury (SCI) is a devastating condition often affecting young and healthy individualsaround the world. This debilitating condition not only creates enormous physical and emotional costto individuals but also is a significant financial burden to society at large. This review was under-taken to understand the global impact of SCI on society. We also attempted to summarize the world-wide demographics and preventative strategies for SCI in varying economic and climatic environ-ments and to evaluate how cultural and economic differences affect the etiology of SCI. A PUBMEDdatabase search was performed in order to identify clinical epidemiological studies of SCI withinthe last decade. In addition, World Bank and World Health Organization websites were used to ob-tain demographics, economics, and health statistics of countries of interest. A total of 20 manuscriptswere selected from 17 countries. We found that SCI varies in etiology, male-to-female ratios, agedistributions, and complications in different countries. Nations with similar economies tend to havesimilar features and incidences in all the above categories. However, diverse methods of classifyingSCI were found, making comparisons difficult. Based upon these findings, it is clear that the cate-gorization and evaluation of SCI must be standardized. The authors suggest improved methods ofreporting in the areas of etiology, neurological classification, and incidence of SCI so that, in the fu-ture, more useful global comprehensive studies and comparisons can be undertaken. Unified injuryprevention programs should be implemented through methods involving the Internet and interna-tional organizations, targeting the different etiologies of SCI found in different countries.
1ICORD, University of British Columbia, Vancouver, Canada.2Department of Surgery, Division of Neurosurgery, Toronto Western Hospital and University of Toronto, Toronto, Canada.3Division of Physical Medicine and Rehabilitation, University of British Columbia, Vancouver, Canada.
INTRODUCTION
SPINAL CORD INJURY (SCI) is a devastating and debili-tating condition that affects all regions of the world
(Sekhon et al., 2001). A high incidence of SCI in youngerpopulations has resulted in enormous financial and phys-
ical costs for individuals and society (Fiefler et al., 1999;Ramer et al., 2000; Tator et al., 1993). A lack of inde-pendence and psychological well-being is associated withthese injuries. To date, there are only minimally effec-tive pharmacological and surgical procedures in place totreat SCI (Bracken et al., 1997, 2003; Fehlings et al.,
2001; Geisler et al., 1992; Hurlbert 2000; Sekhon et al.,2001). It is, therefore, imperative that the world etiologyof SCI is better understood so that global strategies fo-cusing on injury prevention can better formulated.
In the last 25 years, there has been enormous progressin certain areas of the world with regards to the devel-opment and standardization of injury assessment and pre-vention (Ditunno et al., 1994; Maynard, Jr. et al., 1997).However, there are many regions that do not have the re-sources to develop and implement assessment and pre-vention programs.
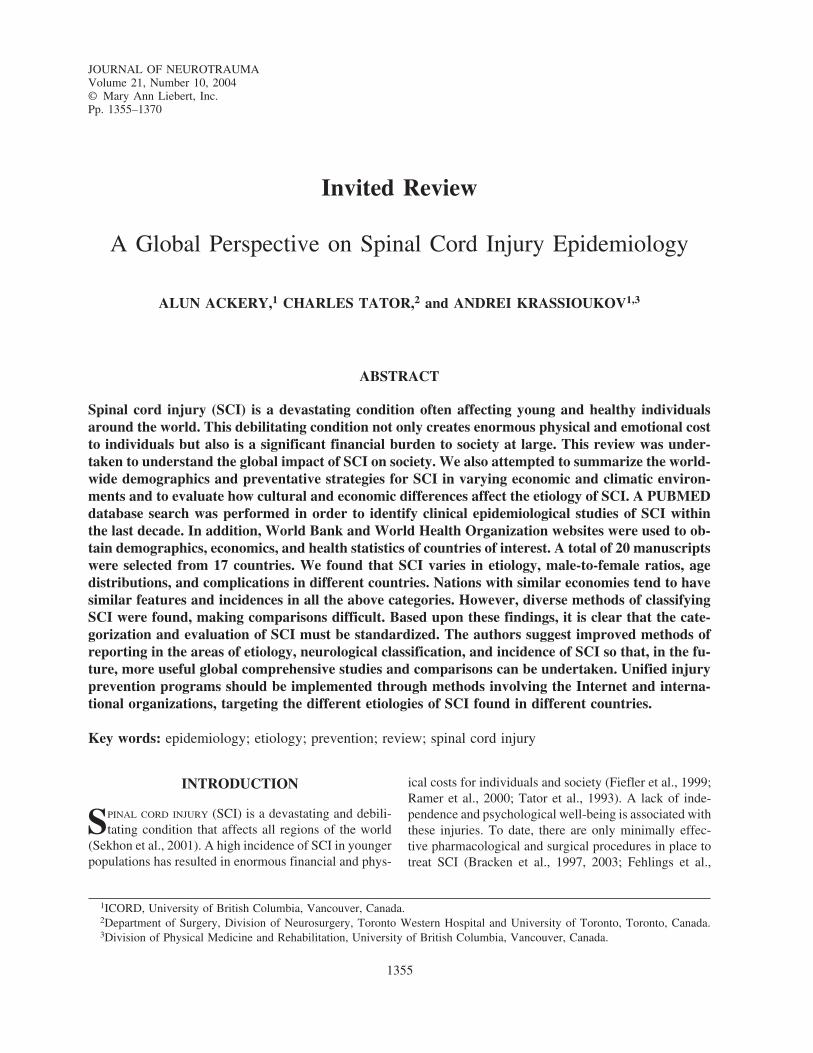
This comparative review focuses on 20 peer-reviewedmanuscripts (Table 1) that report the demographics andepidemiology of SCI in distinct regions of the world withvarying economy, climate, and geography (Aung et al.,1997; Bracken et al., 1997; Catz et al., 2002; da Paz etal., 1993; Dincer et al., 1992; Dryden et al., 2003; Exneret al., 1997; Fazlul Hoque et al., 1999; Geisler et al., 2002;Hart et al., 1994; Krassioukov et al., 2003; Levi et al.,1995; Levy et al., 1998; Martins et al., 1998; Nobunagaet al., 1999; O’Connor 2002; Pagliacci et al., 2003;Ravaud et al., 2000; Shingu et al., 1994; Silberstein etal., 1995). It summarizes the diverse causes of SCI foundin various regions of the world and discusses the differ-ences found within each socio-economic group. The lev-els of medical care and implementation of injury pre-vention programs in different regions are also discussed.Lastly, we give recommendations for future epidemio-logical studies on SCI in order to improve comparison ofdata on SCI between regions. We believe that these mea-sures will lead not only to better understanding of world-wide statistics on SCI, but also the ability to develop in-ternational injury prevention programs.
SEARCH
A thorough PUBMED database search (November2003) was undertaken to identify studies on epidemiol-ogy of SCI from different countries throughout the world.In an effort to concentrate on current data, we focusedon publications within the last decade. Selected publica-tions (Table 1) were analyzed, and an evaluation formwas utilized to extract relevant information reflecting asmuch international and cultural diversity as possible.Multiple manuscripts from North American countries(United States and Canada) were included because of theabundance of statistics and the depth of analysis foundin this region.
It should be noted that the authors performed additionalanalysis and recalculation of some parameters: to analyzedata in absolute values and to present them as a percent-age of the total SCI patients.
Data for 2002 from the World Bank Group (2003) web-site provided updated social and economic informationthat helped classify each country. Statistics pertinent tothe description of the social and economical status ofcountries were included (Table 2).
LITERATURE REVIEW
The literature review reports on 20 manuscripts from17 countries and six continents. There were five manu-scripts from North America, one from South America,seven from Europe, two from Africa, four from Asia, andone from Australia/Oceania (Table 1). The majority ofthese studies entailed retrospective data collection, whilethree studies performed prospective data collection onSCI. Using World Bank Group (2003) classifications,countries were designated as a high-income country (n �11), lower-middle income country (n � 4), or low-in-come country (n � 2) (Table 2).
Canada
Canada is a developed country, having a high-incomeeconomy, a large gross domestic product (GDP), a largeurban population, and high life expectancy (Table 2).Two manuscripts were used to analyze the Canadian SCIepidemiology.
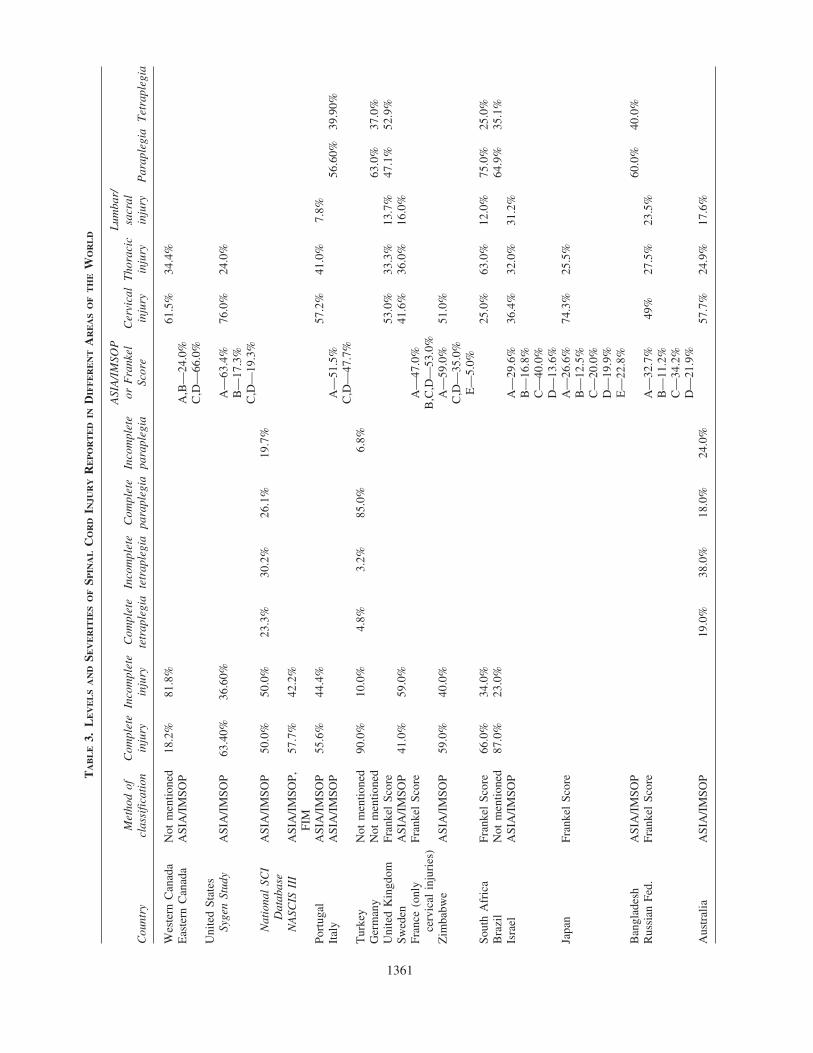
Dryden et al. (2003). This study reported the epi-demiology of SCI in Alberta, a province in WesternCanada on the border of the Rocky Mountains. Thisretrospective study used governmental agencies (Al-berta Ministry of Health and Wellness, the AlbertaTrauma Registry, and death reports from the office ofthe medical examiner) to formulate a database of 450participants with SCI occurring over a 3-year period(1997–2000). Individuals with SCI had a median ageof 35 years (no mean age provided), and a male-to-fe-male ratio of 2.5 to 1 (Table 1). The authors usedprovince-wide databases and death certificates to cal-culate an incidence of SCI of 52.5 cases per million(Table 1). Motor vehicle collisions (MVC) accountedfor the majority (56.4%) of injuries, with the highestoccurrence in individuals between the ages of 15 and29 (Fig. 1). Falls (19.1%) were the second most preva-lent cause of SCI, with high occurrence in the elderly(60 years and older; Fig. 1). The authors concluded thatprevention strategies should target males of all ages,and young and adolescent females, with special em-phasis on prevention of SCI in rural residents becausethey were 2.5 times more likely than urban residents tosustain SCI.
ACKERY ET AL.
1356
1357
TA
BL
E1.
CO
MP
AR
AT
IVE
AN
AL
YS
ISO
FSP
INA
LC
OR
DIN
JUR
YIN
DIF
FE
RE
NT
RE
GIO
NS
OF
TH
EW
OR
LD
Mea
n ag
eIn
cide
nce
per
Mal
e to
Cou
ntry
Ref
eren
ceY
ears
No.
of
pati
ents
(yea
rs)
mil
lion
peo
ple
fem
ale
rati
o
Nor
th A
mer
ica
Wes
tern
Can
ada
Dry
den
et a
l.—C
dn J
Neu
rol
Sci.
(200
3)19
97–2
000
450
35 (
med
ian)
52.5
2.5�
1E
aste
rn C
anad
aK
rass
iouk
ov e
t al
.—J
Neu
rotr
aum
a (2
003)
1998
–200
058
55.4
Not
men
tione
d2.
9�1
Uni
ted
Stat
esSy
gen
Stud
yG
eisl
er e
t al
.—Sp
ine
(200
1)19
92–1
998
760
32.6
Not
men
tione
d4.
0�1
Nat
iona
l SC
I D
atab
ase
Nob
unag
a et
al.—
Arc
h Ph
ys M
ed R
ehab
(19
99)
1973
–199
825
,054
32.3
Not
men
tione
d4.
4�1
NA
SCIS
III
Bra
cken
et
al.—
JAM
A (
1997
)19
91–1
995
499
Maj
ority
age
d 14
–34
Not
men
tione
d5.
6�1
Eur
ope
Port
ugal
Mar
tins
et a
l.—Sp
inal
Cor
d (1
998)
1989
–199
239
850
.557
.83.
4�1
Ital
yPa
glia
cci
et a
l.—A
rch
Phys
Med
(20
03)
1997
–199
968
433
.9—
road
col
lisio
ns18
–20
4.0�
143
.7—
rest
of
SCI’
sT
urke
yD
ince
r et
al.—
Para
pleg
ia (
1992
)19
74–1
985
1694
26.8
Not
men
tione
d3.
1�1
Ger
man
yE
xner
et
al.—
Spin
al C
ord
(199
7)19
76–1
996
22,2
12N
ot m
entio
ned
Not
men
tione
d2.
6�1
Uni
ted
Kin
gdom
Aun
g et
al.—
Spin
al C
ord
(199
7)19
85–1
988
219
Mal
e 35
.5,
fem
ale
44.2
Not
men
tione
d1.
6�1
Swed
enL
evi
et a
l.—Pa
rapl
egia
(19
95)
1995
353
31N
ot m
entio
ned
4.3�
1Fr
ance
Rav
aud
et a
l.—Sp
inal
Cor
d (2
002)
1995
–199
616
6830
.7N
ot m
entio
ned
4.0�
1(o
nly
cerv
ical
inj
urie
s)
Afr
ica
Zim
babw
eL
evy
et a
l.—Sp
inal
Cor
d (1
998)
1988
–199
413
6M
ajor
ity a
ged
20–4
0N
ot m
entio
ned
8.1�
1So
uth
Afr
ica
Har
t et
al.—
Para
pleg
ia (
1994
)19
88–1
993
616
Maj
ority
age
d 20
–29
Not
men
tione
d4.
0�1
Sout
h A
mer
ica
Bra
zil
da P
az e
t al
.—Pa
rapl
egia
(19
92)
1988
108
30.3
Not
men
tione
d3.
9�1
Asi
a Isra
elC
atz
et a
l.—Sp
inal
Cor
d (2
002)
1959
–199
225
034
.5N
ot m
entio
ned
3.1�
1Ja
pan
Shin
gu e
t al
.—Pa
rapl
egia
(19
94)
1990
2665
48.5
39.4
4.3�
1B
angl
ades
hH
oque
et
al.—
Spin
al C
ord
(199
9)19
94–1
995
247
Maj
ority
age
d 10
–40
Not
men
tione
d7.
5�1
Rus
sian
Fed
.Si
lber
tste
in e
t al
.—Pa
rapl
egia
(19
95)
1989
–199
319
6N
ot m
entio
ned
29.7
3.5�
1
Aus
tral
ia/O
cean
iaA
ustr
alia
O’C
onno
r—A
cc A
nal
Prev
(20
02)
1998
–199
926
5M
ajor
ity a
ged
15–2
414
.53.
2�1
Krassioukov et al. (2003). This study was conductedin Toronto, Ontario, a major urban center in EasternCanada, with a retrospective chart review of all patientswith SCI (n � 58) admitted to the acute care unit of auniversity-based hospital between 1998 and 2000. Themean age of individuals with SCI was 53.6 years; how-ever, almost half the patients (48%) were 60 years orolder (mean age 73.3 years; Table 1). The authors foundthat falls were the leading cause of SCI (47%; Fig. 1).The authors suggested that the increased number of el-derly with SCI was due to the fact that this center pro-vides care to an urban population with a significant proportion of elderly individuals. The authors also ac-knowledged that, although there was an acute SCI unitin this hospital, the general acute trauma units were lo-cated elsewhere. The majority of individuals involved inMVC in this study were found in the younger age group(mean age 38.7 years). The American Spinal Injury As-sociation/International Medical Society of Paraplegia im-pairment scale (ASIA/IMSOP) was used in this study toevaluate the severity of SCI (Ditunno et al., 1994; May-nard, Jr. et al., 1997). The study focused on the evalua-tion of the secondary complications in the acute stage ofSCI and found that pneumonia (25.9%) and urinary tractinfections (UTI; 20.7%) were the most prevalent. The au-thors concluded that secondary complications occur morefrequently in the elderly and that “rigorous attention” tothe principles of acute management, especially avoidanceof complications, in this group is required.
United States
The United States is a developed nation, having a high-income economy, a large GDP, a large urban population,and high life expectancy (Table 2). Investigators in theUnited States have conducted a wide variety of studiesthat profile the epidemiology of SCI and three recentmanuscripts have been selected for this review.
Geisler et al. (2003). This is a report from the Sygen®
Group of the randomized, controlled clinical trial of GM-1 ganglioside for the treatment of SCI. It is the most re-cent epidemiological study conducted mainly in theUnited States from 1992 to 1998 with 760 SCI patientsenrolled in a study to determine the effectiveness of GM-1 ganglioside in acute SCI. There were 28 neurotraumacenters (26 in the United States, two in Canada) involvedin collecting patient information, and there was a male-to-female ratio of 4.0 to 1, and a mean age of 32.6 years(Table 1). MVCs comprised 54.1% of all causes of in-jury, while falls were second with 16.2% (Fig. 1). Thisstudy was extremely thorough in providing demographiccharacteristics such as race, height, weight, and numer-ous physiological parameters. All neurotrauma centersutilized ASIA/IMSOP score, functional independencemeasurements (FIM), and modified Benzel scores toidentify the severity of injury and functional outcomes(Table 3). The purpose of this manuscript was to assessthe epidemiology and broad management patterns in the
ACKERY ET AL.
1358
TABLE 2. 2002 WORLD BANK SOCIAL AND ECONOMICAL STATISTICSa
World status Population Gross domestic product Urban population Incidence perCountry (economy class) (millions) (billions in USD) (% of total) million people
FIG. 1. The causes of spinal cord injury (SCI) in each of the 20 manuscripts reviewed in the text. The causes are displayed as per-centages of the total sum. Etiologies of SCI were categorized into motor vehicle collisions, falls, violence, sports related and aquatic/div-ing, and self-inflicted/suicide attempts. Causes that did not fit under these criteria are shown as other/unrecognized etiologies.
Sygen trial, and injury prevention was outside the scopeof the study.
Nobunaga et al. (1999). The authors report findings fromthe National Spinal Cord Injury Database of the Model Sys-
tems Group, one of the oldest and most comprehensive sys-tems for the collection of information on SCI patients. Theyincluded data on 25,054 persons with SCI from 24 neuro-trauma centers collected between 1973 and 1998. The meanage at time of injury was 32.3 years, with a male-to-fe-
male ratio of 4.4 to 1 (Table 1). The manuscript is thor-ough in dividing the data collection into 5-year periods thatallowed understanding of the trends in etiology, race, age,time of year, and extent of injury. Prior to 1992, the studyused the Frankel Grade to evaluate the extent of injury;however, the study switched to ASIA/IMSOP scoring af-ter 1992 (modified version of Frankel Grade; Table 3). Thestudy showed that SCI predominantly occurs in the 16–30-year-old group, but that the average age was increasing, dueto the increased incidence of injury in the older age group(older than 50 years old). The authors also noted that sportsand MVC-related injuries were becoming less frequent,while violence-related SCIs were increasing, especially inyounger African-American men.
Bracken et al. (1997). This study includes epidemio-logical North American data on SCI and was generatedby the Third National Acute Spinal Cord Injury (NASCISIII) Randomized Controlled Trial comparing the neuro-protective efficacy of methylprednisolone and tirilizadmesylate in acute SCI. There were 14 neurotrauma hos-pitals (12 from the United States, two from Canada) in-volved in the trial conducted between 1991 and 1995.There were 499 patients in the study, with the majorityaged 14–34 (no mean age given) and a male-to-femaleratio of 5.6 to 1 (Table 1). MVCs comprised a large por-tion of the causation of SCI (44.6%), with falls havingthe second highest incidence (26.8%; Fig. 1). Demo-graphics on ethnicity and associated injuries were alsoprovided. All neurotrauma centers involved in the studyutilized ASIA/IMSOP scoring (not reported), NASCIS IIscoring, and FIM to classify the neurological impairmentsafter SCI (Table 3). The major secondary complicationreported was UTI (35.3%; Table 4). The major focus ofthis manuscript was on neuroprotection.
Portugal
Portugal is a developed country, having a high-incomeeconomy, a high GDP (relative to population size), a largeurban population, and high life expectancy (Table 2).
Martins et al. (1998). This study reported the epidemi-ology of SCI in the central region of Portugal based on 398cases of SCI collected between 1989 and 1992 and was un-dertaken at two Coimbra hospitals. The mean age of thepatients was 50.5 years (Table 1). However, the data pre-sented showed a bimodal curve, with higher incidences ofinjury in the 15–24 and 55–74 age groups. The male-to-fe-male ratio was 3.4 to 1, with MVC (57.3%) and falls(37.4%) being the predominant causes of SCI (Table 1; Fig.1). The incidence of SCI was 57.8 cases per million peo-ple, including both patients who survived the injury andthose that failed to reach the hospital alive (Table 1). Al-
though the authors indicated that ASIA/IMSOP scoring wasused, only crude data was presented with respect to com-plete versus incomplete injuries (Table 3). They concludedthat there was a need for improved rehabilitation and spe-cific care of SCI patients, especially due to the increase inincidence of MVC in the region.
Italy
Italy is a developed country, with a high-income econ-omy, a high GDP, a large urban population, and high lifeexpectancy (Table 2).
Pagliacci et al. (2003). The authors of this study de-scribe the etiology, clinical presentation, complications,outcome indicators, and links between acute interventionand rehabilitation of patients following SCI in Italy. Thisprospective study was conducted between 1997 and 1999in 32 Italian hospitals that were involved in SCI rehabil-itation. The study reported an incidence of SCI of 18–20per million people in Italy, with a male-to-female ratioof 4.0 to 1. The main etiologies of SCI were MVC(53.8%) followed by falls (22.6%). The mean age of in-dividuals with SCI resulted from MVC was 33.9 years,while all the other combined categories had a mean age of43.7 years (Table 1; Fig. 1). The study used ASIA/IMSOP scoring to assess the level and severity of SCI(Table 3). Authors also reported the length of hospital stayand rehabilitation for individuals with SCI. The most pre-dominant secondary complication reported was pressuresores (26.9%; Table 4). The authors concluded that therewas an increased need for improved planning based on pa-tients’ needs, a need for the implementation of injury pre-vention programs (i.e., reinforcing seat belt usage), andbetter overall organization in the management of patientswith SCI. This measure could optimize the treatment andreduce the costs of management of patients with SCI.
Turkey
The World Bank Group (2003) classified Turkey as acountry with a lower-middle income economy, with ahigh urban population, and a lower GDP and life ex-pectancy than most developed nations (Table 2).
Dincer et al. (1992). This study describes the epi-demiology of traumatic SCI in Turkey for the period of1974–1985, based on admissions to the Ankara Rehabil-itation Center. A total of 1694 patients were investigatedwith a mean age of 26.8 years, with predominance(72.23%) in the 15–39-year-old group (Table 1). Themale-to-female ratio was 3.1 to 1, with MVC (37.3%),falls (26.4%, where a large portion are falls from treesbecause of agricultural work), and violence (24.0%) be-
ACKERY ET AL.
1360
1361
TA
BL
E3.
LE
VE
LS
AN
DSE
VE
RIT
IES
OF
SPIN
AL
CO
RD
INJU
RY
RE
PO
RT
ED
IND
IFF
ER
EN
TA
RE
AS
OF
TH
EW
OR
LD
ASI
A/I
MSO
PL
umba
r/M
etho
d of
Com
plet
eIn
com
plet
eC
ompl
ete
Inco
mpl
ete
Com
plet
eIn
com
plet
eor
Fra
nkel
Cer
vica
lT
hora
cic
sacr
alC
ount
rycl
assi
fica
tion
inju
ryin
jury
tetr
aple
gia
tetr
aple
gia
para
pleg
iapa
rapl
egia
Scor
ein
jury
inju
ryin
jury
Par
aple
gia
Tet
rapl
egia
Wes
tern
Can
ada
Not
men
tione
d18
.2%
81.8
%61
.5%
34.4
%E
aste
rn C
anad
aA
SIA
/IM
SOP
A,B
—24
.0%
C,D
—66
.0%
Uni
ted
Stat
esSy
gen
Stud
yA
SIA
/IM
SOP
63.4
0%36
.60%
A—
63.4
%76
.0%
24.0
%B
—17
.3%
C,D
—19
.3%
Nat
iona
l SC
IA
SIA
/IM
SOP
50.0
%50
.0%
23.3
%30
.2%
26.1
%19
.7%
Dat
abas
eN
ASC
IS I
IIA
SIA
/IM
SOP,
57
.7%
42.2
%FI
MPo
rtug
alA
SIA
/IM
SOP
55.6
%44
.4%
57.2
%41
.0%
7.8%
Ital
yA
SIA
/IM
SOP
A—
51.5
%56
.60%
39.9
0%C
,D—
47.7
%T
urke
yN
ot m
entio
ned
90.0
%10
.0%
4.8%
3.2%
85.0
%6.
8%G
erm
any
Not
men
tione
d63
.0%
37.0
%U
nite
d K
ingd
omFr
anke
l Sc
ore
53.0
%33
.3%
13.7
%47
.1%
52.9
%Sw
eden
ASI
A/I
MSO
P41
.0%
59.0
%41
.6%
36.0
%16
.0%
Fran
ce (
only
Fr
anke
l Sc
ore
A—
47.0
%ce
rvic
al i
njur
ies)
B,C
,D—
53.0
%Z
imba
bwe
ASI
A/I
MSO
P59
.0%
40.0
%A
—59
.0%
51.0
%C
,D—
35.0
%E
—5.
0%So
uth
Afr
ica
Fran
kel
Scor
e66
.0%
34.0
%25
.0%
63.0
%12
.0%
75.0
%25
.0%
Bra
zil
Not
men
tione
d87
.0%
23.0
%64
.9%
35.1
%Is
rael
ASI
A/I
MSO
PA
—29
.6%
36.4
%32
.0%
31.2
%B
—16
.8%
C—
40.0
%D
—13
.6%
Japa
nFr
anke
l Sc
ore
A—
26.6
%74
.3%
25.5
%B
—12
.5%
C—
20.0
%D
—19
.9%
E—
22.8
%B
angl
ades
hA
SIA
/IM
SOP
60.0
%40
.0%
Rus
sian
Fed
.Fr
anke
l Sc
ore
A—
32.7
%49
%27
.5%
23.5
%B
—11
.2%
C—
34.2
%D
—21
.9%
Aus
tral
iaA
SIA
/IM
SOP
19.0
%38
.0%
18.0
%24
.0%
57.7
%24
.9%
17.6
%
ing the predominant etiologies of SCI (Table 1; Fig. 1).The authors did not report the methods of neurologicalevaluation of the severity of SCI (Table 3). They con-cluded that in less developed countries, such as Turkey,emergency first aid service and post-traumatic care werenot sufficient. Furthermore, socioeconomic measures thatfocus on mass education for injury prevention were con-sidered an essential component in the future managementof SCI in Turkey.
Germany
Germany is a developed European country, with ahigh-income economy, a high GDP, a large urban popu-lation, and high life expectancy (Table 2).
Exner and Meinecke (1997). The authors described 20years (1976–1996) of epidemiological data from 21 cen-ters providing care for individuals with SCI throughout
ACKERY ET AL.
1362
TABLE 4. MAJOR SECONDARY COMPLICATIONS OF SPINAL CORD INJURY
Major secondary Percentage of totalCountry complications SCI patients
North AmericaWestern Canada Not mentionedEastern Canada Pneumonia 25.9
Urinary tract infections 20.7United States
Sygen Study Not mentionedNational SCI Database Not mentionedNASCIS III Urinary tract infections 35.3
EuropePortugal Not mentionedItaly Pressure sores 26.9Turkey Not mentionedGermany Disorders of soft tissue 23.0
Pressure sores 33.3South Africa Pressure sores 11.0
Severe spasticity 7.0
South AmericaBrazil Pressure sores 54.1
Urinary tract infections 32.6
AsiaIsrael Not mentionedJapan Not mentionedBangladesh Urinary tract infections 62.0
Pressure sores 38.0Russian Fed. Not mentioned
Australia/OceaniaAustralia Not mentioned
Germany. The authors evaluated the epidemiology of newcases, as well as the readmissions of patients with SCI,examining the total SCI population in Germany. A totalof 22,212 new cases were reported, with a male-to-femaleratio of 2.6 to 1. The main etiologies of injury were MVC(38%), an accident at work (14%, presented in Fig. 1 as“Other”), sports and diving (4%), and attempted suicide(5%). They reported that the main secondary complica-tions that resulted in readmissions were “disorders of thesoft tissues” (23%) and UTI (21%; Table 4). In this study,no classification scale for neurological function was pro-vided, and no age information was reported. The authorsmentioned that injury prevention had been directed to-wards traffic-related injuries, and that rising velocity, in-creased traffic congestion, and a greater number of vehi-cles increased the risk of occurrence of SCI.
United Kingdom
The United Kingdom is a developed country, with ahigh-income economy, a high GDP, a large urban popu-lation, and high life expectancy (Table 2).
Aung and El Masry (1997). The authors report a 4-yearretrospective study (1985–1988) on all new SCI admissionsto the Midlands Centre for Spinal Injuries in Oswestry. Re-porting on 219 patients with SCI, they found a male-to-fe-male ratio of 1.6 to 1, with an average age for males andfemales of 35.5 years and 44.2 years, respectively (Table1). They report that the MVC accounted for 50% of all SCI,followed by falls (42%) and sports injuries (7%; Fig. 1).The Frankel Grade was used to assess the level and sever-ity of injury (Table 3). Pneumonia (4.6%) was reported asthe main secondary complications in individuals with SCI,followed by pressure sores (6.8%; Table 4). The authorsalso assessed the risks of developing secondary complica-tions with respect to hospital admission time, but offeredno suggestions for injury prevention.
Sweden
Sweden is a developed European country, with a high-income economy, a high GDP, a large urban population,and high life expectancy (Table 2).
Levi et al. (1995). The authors report the results of asurvey from the Stockholm Regional SCI Center. Datacollection was performed between 1991 and 1994. Thesurvey included 374 patients, with a mean age of 31 yearsand a male-to-female ratio of 4.3 to 1 (Table 1). They re-ported that MVC (45.6%) was the most prevalent causeof SCI, followed by falls (37.1%), suicide attempts(4.0%), and violence (3.1%; Figure 1). The authors morespecifically classified the etiologies using the Interna-
tional Classification of Diseases (ICD) and classificationof external causes of injury. The ASIA/IMSOP score wasused to assess the severity and completeness of injury(Table 3), and the authors found that the most commonsecondary complications reported were UTI (67.4%) andpressure ulcers (38.8%; Table 4). No injury preventionmethods were discussed in this manuscript.
France
France is a developed country, with a high-incomeeconomy, a high GDP, a large urban population, and highlife expectancy (Table 2).
Ravaud et al. (2000). This manuscript reports results ofa multicenter (35 centers) epidemiological survey from theTETRAFIGAP group on the French tetraplegic spinal cordinjured population. It is important to note that no para-plegic patients were included in this study and that a fewcenters from Belgium and Switzerland were also included.The survey involved 1668 patients who fulfilled the in-clusion criteria. They reported a mean age of injury of 30.7years and a male-to-female ratio of 4 to 1 (Table 1). More-over, they reported that the MVC were the most prevalentcause of injury (57.9%), followed by sports and diving(22.3%) and falls (3.3%; Fig. 1). It is important to notethat falls in this study caused a much lower rate of SCIwhen compared to other high-income countries that re-ported both paraplegia and tetraplegia. For neurologicaland functional classification, the TETRAFIGAP groupused the Frankel Grade (Table 3). In a follow-up manu-script, the group reported the secondary complicationsfound in the survey, with urinary complications (32.1%)and pressure sores (27.7%) being the most prevalent (Table4). No injury prevention methods were discussed.
Zimbabwe
Zimbabwe is a developing African country, having alow-income economy, low GDP, a small urban popula-tion, and low life expectancy (Table 2).
Levy et al. (1998). The authors report a retrospectivestudy on the quality of life and epidemiology of SCI pa-tients in Zimbabwe at the National Rehabilitation Cen-ter. The manuscript reports a high incidence of MVC(56%, including bicycles and carts), falls from trees(11%), and violence (15%, including assault and gunshotwounds) as prevalent etiologies of SCI (Fig. 1). The male-to-female ratio was 8.1 to 1 based on 136 patients whohad SCI from 1988 to 1994 (Table 1). This study usedASIA/IMSOP scoring for assessment of individuals withSCI (Table 3). High rates of mortality in the hospital,high mental anguish, and shortage of post-injury follow-
SPINAL CORD INJURY EPIDEMIOLOGY
1363
up programs to treat SCI were discussed. This manuscriptdescribes the problems associated with SCI in a devel-oping country. The lack of wheelchairs, a high incidenceof secondary complications and minimal injury preven-tion programs are discussed in detail. The authors con-cluded that patients with SCI in Zimbabwe have an un-acceptably high rate of pressure sores (33.3%) and pain(77.0%; Table 4), and that adequate financial and familysupport is needed to deal with this devastating condition.The authors also indicated a lack of monetary resourcesto provide proper acute care for patients with SCI. Theauthors emphasized that, without establishing proper fi-nancial and family support systems, as well as providingproper motivation to individuals with SCI, patients arevirtually condemned to death after discharge.
South Africa
South Africa is an African nation that the World BankGroup (2003) has classified as lower-middle income,with a small GDP (relative to its population), a small ur-ban population, and a lower life expectancy as comparedto highly developed nations (Table 2).
Hart et al. (1994). The authors report the epidemiol-ogy of SCI at the Natalspruit Hospital Spinal Rehabili-tation program over a 6-year period (1988–1993). Thisstudy reported on 616 SCI, with a male-to-female ratioof 4 to 1, and a majority of the patients between the agesof 20 and 29 (Table 1). Violence (56%) was the mostpredominant cause of injury, followed by MVC (25%)and falls (2.5%; Fig. 1). The authors utilized the FrankelGrade to report the neurological and functional impair-ments after SCI. The most prevalent secondary compli-cations were pressure sores (11%) and severe spasticity(7%; Table 4). The authors report an increase of violencedue to the changing economic and political systems, butno injury prevention programs were discussed.
Brazil
Brazil is a South American nation that the World BankGroup (2003) classified as lower-middle income, with asmall GDP (relative to its population), and a lower lifeexpectancy as compared to highly developed nations(Table 1).
da Paz et al. (1992). This study reports the etiology, com-plications, and demographics of SCI in Brazil. Informationwas collected from a retrospective survey of 36 hospitalsthroughout all of Brazil in 1988. The authors reported amean age of 30.3 years, with a male-to-female ratio of 3.9to 1 (Table 1). The main causes of injury were MVC (42%),violence (27.9%), and falls from heights (15%; Fig. 1). The
main secondary complications were pressure ulcers(54.1%) and UTI (32.6%). No methods for neurologicalclassification of SCI were discussed (Table 3). The con-clusions stressed the need for better injury prevention pro-grams (e.g., seat belts) and increased number of hospitalbeds to provide care to patients with this type of injury.
Israel
Israel is a Middle East nation with a high-income econ-omy, a high urban population and GPD (relative to pop-ulation size), and high life expectancy similar to otherdeveloped nations (Table 2).
Catz et al. (2002). The authors presented a retrospec-tive study of SCI epidemiology of 250 consecutive pa-tients injured between 1959 and 1992 treated at theLoewenstein Rehabilitation Hospital in Israel. The au-thors reported that SCI patients had a mean age of 34.5years with a male-to-female ratio of 3.1 to 1 (Table 1).Motor vehicle collision (32.8%) was the most prevalentetiology of injury (Fig. 1). The study used ASIA/IMSOPscoring to evaluate the severity of SCI (Table 3). The au-thors concluded that their epidemiological data were sim-ilar to countries with similar socio-economic status.
Japan
Japan is an East Asian developed nation, having a high-income economy, a large GDP, a large urban population,and high life expectancy (Table 2).
Shingu et al. (1994). The investigators of this studyperformed a nationwide SCI epidemiological survey inJapan. The Prevention Committee of the Japanese Med-ical Society of Paraplegia conducted the survey in 1990and included 2665 patients (Table 1). The annual SCI in-cidence was 39.4 per million people, but this only in-cludes people who survived the SCI and reached the hos-pital alive (Table 1). The investigators found that themale-to-female ratio was 4.3 to 1, and the mean age was48.5 years (Table 1). The study used the Frankel Gradeto evaluate the neurologic function following injury(Table 3). Motor vehicle collisions (44.6%) were the mostprevalent cause of injury, with falls following closely be-hind (41.0%; Fig. 1). The authors suggested the organi-zation of a campaign to encourage SCI prevention.
Bangladesh
Bangladesh is a developing Asian country, with a low-income economy, low GDP, a small urban population,and low life expectancy (Table 2).
Hoque et al. (1999). This group reported the epidemi-ology of SCI in Bangladesh in 1994 and 1995, and
ACKERY ET AL.
1364
recorded 247 patients with SCI admitted to the Center forthe Rehabilitation of the Paralysed in Savar, Dhaka. Amajority of these patients were between 20 and 40 yearsold (no mean age reported), and the male-to-female ra-tio was 7.5 to 1 (Table 1). Falls (63.0%), primarily fromtrees or while carrying a heavy load on the head, werethe primary cause of injury followed by MVC (18%; Fig.1). The authors indicated that there is a high mortalityrate of people with SCI and that it is underreported be-cause of the lack of follow-up and reporting resources. Itwas interesting that the MVC usually involved rickshawsand other small transport vehicles. The predominant sec-ondary complications reported were UTI (62.0%) andpressure sores (38.0%; Table 4). Moreover, the study re-ported that developing countries, such as Bangladesh, areinadequately resourced to deal with SCI patients. Furtherresearch is needed to study the diverse causes of SCI inthese lower socio-economic regions (e.g., falls while car-rying a heavy load on the head).
Russian Federation
Although Russia is located on two continents, the studywas conducted in Novosibirsk, which is located in Asia.The World Bank Group (2003) classified it as a lower-middle income country, with a small GDP (relative to itspopulation), and a lower life expectancy as compared tohighly developed nations (Table 2).
Silberstein et al. (1995). The authors report the SCIepidemiology of Novosibirsk during 5 consecutive years(1989–1993) collected by the Department of Spinal CordInjuries, Research Institute of Traumatology. They re-ported a total of 196 SCI patients, an SCI incidence of29.7 cases per million people, a male-to-female ratio of3.5 to 1, and a mean age for males and females of 34.7and 32.3 years, respectively (Table 1). Falls (37.3%) werethe most prevalent cause of injury, followed by sportsand diving (32.9%), MVC (25.1%), and suicide (3.1%)(Fig. 1). The authors used the Frankel Grade to classifyneurological function after SCI (Table 3). Injury preven-tion was not discussed in this study.
Australia
Australia is a developed nation, having a high-incomeeconomy, a large GDP, a large urban population, and highlife expectancy (Table 2).
O’Connor (2002). The author reports the incidence andpatterns of SCI in Australia. Information on 265 SCI pa-tients was collected using the Australian SCI register dur-ing the year’s 1998 and 1999. The authors found that theSCI incidence were 14.5 per million people, and the ma-
jority of these injuries occurred in the 15–24-year-old group(no mean age given). The male-to-female ratio was 3.2 to1 (Table 1). Motor vehicle collisions accounted for 43% ofSCI, while falls had the second highest prevalence (31%;Fig. 1). The Australian SCI registry used ASIA/IMSOPscoring to classify neurological function after SCI (Table3). This study showed that national population-based sur-veillance is fundamental in understanding the epidemiologyof SCI in Australia. The authors suggested a need for or-ganization of injury prevention programs that will help re-duce overall health costs and benefit the society as a whole.
DISCUSSION
Twenty manuscripts were evaluated during the prepa-ration of this review in order to create a global perspec-tive on the epidemiology of SCI. Although we selectedmanuscripts that contained data on the epidemiology ofSCI, the majority of the studies also addressed other as-pects of SCI such as therapeutic approaches, manage-ment, and secondary complications.
Incidence of SCI
It has been reported that the annual incidence of SCIvaries between 11.5 and 57.8 cases per million people indifferent countries (Martins et al., 1998; Tator 1995, 2000).Of the 20 studies reviewed for this manuscript, only six re-ported the SCI incidence (Table 1), and these were all fromdeveloped countries (Western Canada, Portugal, Italy,Japan, the Russian Federation, and Australia). Portugal andWestern Canada had the highest reported annual incidencerate of SCI per million people (57.8 and 52.5, respectively),but were the only studies to include those who died beforebeing admitted to hospital, collecting data from death cer-tificates and coroner’s reports. In contrast, Australia had thelowest reported incidence of SCI (14.5); however, deathsat the scene of trauma were not included. Unfortunately, itis not possible to estimate the worldwide incidence of SCIbecause of the lack of consistency of data reporting. Thesix studies that reported SCI incidence all had large num-ber of patients (265–4665 patients) and used multiple sitesor nationwide governmental databases to generate the in-cidences per million, but not all of them included cases ofSCI that failed to survive long enough to be admitted tohospital. Therefore, in order to appreciate the full extent ofthe incidence of SCI, the goal should be to collect multi-centered data and to include cases that failed to survive longenough to be admitted.
Etiology of SCI
Identifying the causes of SCI throughout the world isimportant in order to understand global trends and ulti-
SPINAL CORD INJURY EPIDEMIOLOGY
1365
mately to improve strategies for SCI prevention. In com-paring data from selected studies, we found a lack of uni-formity with respect to classification of the etiologies ofSCI, and thus, it is difficult to compare the individual eti-ologies. The same etiology was often grouped into vary-ing and more specified categories. For example, the studyfrom Zimbabwe had six identified causes of injury: (1)traffic accidents, (2) assaults, (3) falling out of trees, (4)falling out of carts, (5) falling off of bicycles, and (6)gunshot wounds (Levy et al., 1998). In contrast, the Aus-tralian study identified the predominant causes of SCI,but also broke down the etiology of very specific causes,such as intentional/unintentional SCI, specific types offalls, the environment setting, including whether theywere work-related or not, as well as others (O’Connor,2002). In general, most studies identified the followingleading causes of SCI: MVCs, falls, sports/aquatics-re-lated injuries, violence-related injuries, and self-inducedinjuries (Fig. 1). In addition to the above frequent causesof injury, there were also unusual causes of SCI identi-fied throughout the world: falling from trees, bull attacks,and carrying heavy loads on the head (Fazlul Hoque etal., 1999; Levy et al., 1998). These indicate the culturalspecificity of SCI, but nevertheless there is a need foruniform methods of classification. The “falls” categoryis especially problematic, and can include industrial andsports categories in some countries.
Several trends in the etiology of SCI were identified.For example, MVCs were the leading cause of SCI in de-veloped nations, comprising up to 58% (Martins et al.,1998) and found predominantly in younger age groups(Krassioukov et al., 2003; O’Connor, 2002). Falls werethe second leading cause of SCI among these countries,with a prevalence of up to 46.6% and found predominantlyin the elderly (Krassioukov et al., 2003; O’Connor, 2002).However, there is a large discrepancy between developedand undeveloped nations. For example, falls were the lead-ing cause of SCI in Bangladesh, and there was a signifi-cant increase in the incidence of SCI due to violence inmost of the lower-middle income countries (Brazil, SouthAfrica, and Turkey) (da Paz et al., 1993; Dincer et al.,1992; Fazlul Hoque et al., 1999; Hart et al., 1994).
Adoption of uniform methods of reporting SCI in epi-demiological studies would benefit global comparisonsbetween different countries and help to improve the un-derstanding of global etiologies. Moreover, more specificdescription of terms would help countries compare theiretiologies. For example, falls can arise from a variety ofcauses (i.e., low falls, high falls, diving, falling from atree). We suggest that the use of the current InternationalStatistical Classification of Diseases (ICD) and RelatedHealth Problems (1992) would enable authors to use thesame terminology for comparing etiologies. However,
even this system requires improvements to classify somecauses of SCI.
Age Distributions and Male-to-Female Ratios
The highest incidences of SCI in all countries were re-ported in persons between 20 and 40 years of age. Theless developed countries displayed lower mean age av-erages than the more developed countries. It appears thatdeveloped countries have higher mean ages at the timeof SCI, probably due to a more aged population (Table1). The higher life expectancies found in more developedcountries (Table 2), as well as the advanced medical care,make it possible for elderly people to survive a SCI. Forexample, the study by Krassioukov et al. (2003) in East-ern Canada indicated that the mean age at the time of SCIwas 55.4 years, and nearly half the subjects were overthe age of 60 (Table 1). It is interesting to note that thestudy by Tator et al. (1993) published a decade earlierwith analysis of data from 1947 to 1981 in the same re-gion reported a mean age of 34.5 years. The ageing pop-ulation (i.e., baby boomers) is a new demographic trendfor developed countries (Dryden et al., 2003; Kras-sioukov et al., 2003; McColl et al., 2002; Nobunaga etal., 1999; Shingu et al., 1994; Tator et al., 1993). How-ever, SCI still predominantly affects a young population,resulting in significant functional impairment and ac-companying long-term social and financial costs.
It has been well documented previously that SCI inmales is more prevalent than in females (Bracken et al.,1981; Sekhon et al., 2001; Tator et al., 1993). This re-view confirms this global trend, despite major economic,geographic, and cultural differences. A majority of thestudies showed a male-to-female ratio of approximately3–4 to 1). However, low-income countries, such as Zim-babwe and Bangladesh, displayed even higher male-to-female ratios of 8.1 and 7.5 to 1, respectively (FazlulHoque et al., 1999; Levy et al., 1998). Reports from thesecountries did not address the specific reasons for thesehigher ratios, but it is likely that the majority of womenremained home as housewives, while men performedrisk-taking activities outside the home—at work or insports—and were exposed to more violence (FazlulHoque et al., 1999).
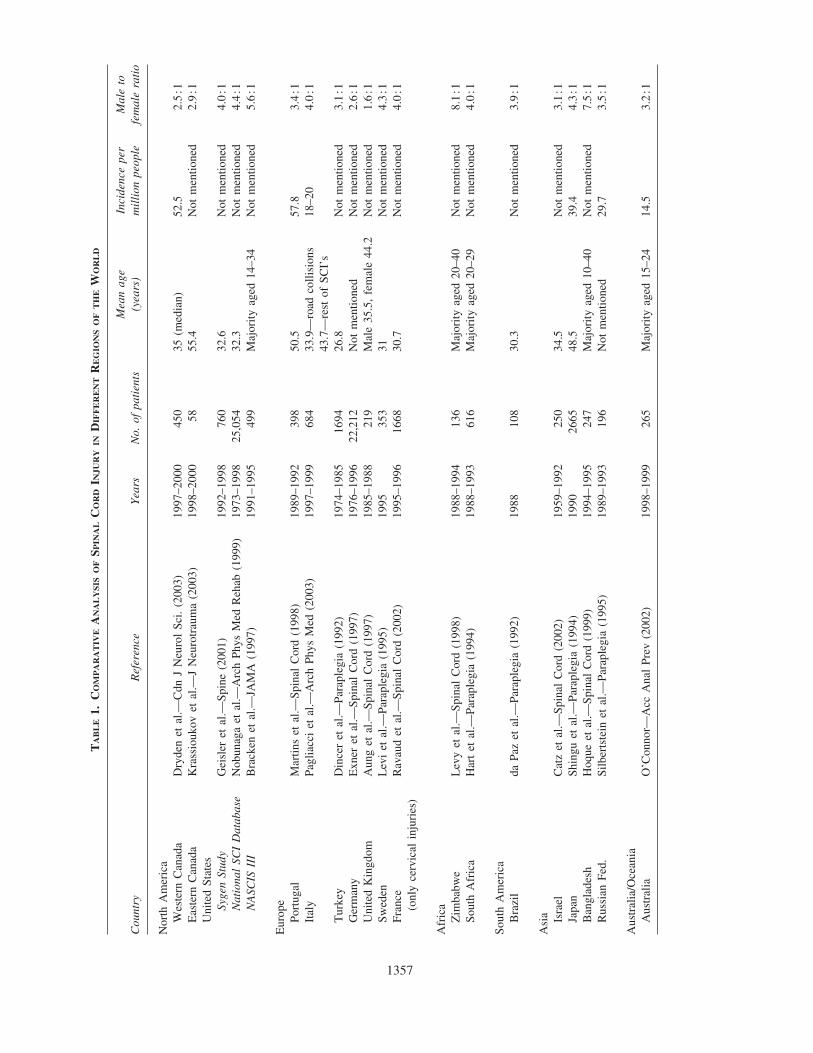
Level and Severity of Spinal Cord Injury
A majority of the analyzed studies utilized theASIA/IMSOP score for the assessment of the severity ofSCI (Ditunno et al., 1994; Maynard, Jr. et al., 1997). TheASIA/IMSOP score has become a standard tool in theevaluation of patients with SCI in North America and Eu-rope and is a modification of the previously introducedFrankel Grade (Frankel et al., 1969). It appears that the
ACKERY ET AL.
1366
ASIA/IMSOP system is used in both developed and de-veloping countries. Eleven manuscripts in the review uti-lized the ASIA/IMSOP score, and six countries reportedusing the Frankel Grade of neurological classification,and all of the latter were from epidemiological studiesconducted prior to 1995. The Turkish and Brazilian man-uscripts did not mention a method for neurological clas-sification, but both studies were published in 1992 be-fore the ASIA/IMSOP score was introduced. However,two studies published after 1992 (Western Canada andGerman) also did not identify their method of neurolog-ical assessment for SCI. Additional outcome measuresincluded in some studies were the FIM, bladder auton-omy, Benzel scores, and feelings of dependency (Brackenet al., 1997; Pagliacci et al., 2003).
Data on levels and severity of SCI are summarized inTable 3. Although there were significant differences inthe reporting of levels and severity of injuries betweenthe studies, few clear trends could be identified. The ma-jority of studies, with the exception of South Africa, re-ported a high incidence of SCI at the cervical level (Table3), ranging from 41.6% to 76.0%. Cervical injuries werefrequent in both high- and low-income countries. A mi-nority of studies provided more detailed information onthe levels of SCI, such as the evaluation of upper andlower cervical injuries (Russia and Israel). The Frenchstudy focused only on the cervical SCI (Ravaud et al.,2000). There were some differences between the studieswith respect to the completeness of SCI. For example,the studies from Brazil and Turkey reported significantlyhigher rates of complete SCI (87.0% and 90.0%, respec-tively) (da Paz et al., 1993; Dincer et al., 1992). It is likelythat there was underreporting of incomplete cases in thesestudies. In both studies, the authors did not indicate thetools that were utilized for the assessment of the SCI. Incontrast, the majority of studies that utilized theASIA/IMSOP score for the assessment of SCI showed asignificant incidence of incomplete SCI, ranging from34.0% to 59.0% (Table 3). The authors of the present re-view suggest that the use of ASIA/IMSOP scale in as-sessment and reporting of the severity of SCI could pro-vide not only valuable clinical information for readers,but also would allow comparison of clinical data betweenstudies. However, we also would like to indicate that, inorder to decrease inter-observer variability of ASIA/IMSOP assessment, a thorough training is recommendedto personnel who are involved in neurological assessmentof individuals with SCI (Priebe et al., 1991).
Secondary Complications following SCI
The secondary complications that follow SCI are of-ten debilitating and can be life-threatening. However, by
properly educating patients and care-givers, a majority ofthem could be prevented. UTIs, pressure sores, cardiacand vascular/hemorrhagic complications, psychiatriccomplications, and autonomic dysreflexia are the mostfrequent post-injury conditions found in SC patients(Krassioukov et al., 2003). Of the 20 manuscripts re-viewed, 10 of them reported numerous secondary com-plications. The developed high-income countries that re-ported secondary complications showed that UTI,pressures sores, and, in two studies (Eastern Canada andthe United Kingdom), pneumonia were the prominentpost-injury conditions that occur in patients with SCI,with incidences at 20–35% (Table 4). Brazil and SouthAfrica were the only middle-income countries to reportsecondary complications. Brazil reported higher inci-dences of pressure ulcers (54.1%) than the high-incomenations; however, South Africa reported an occurrenceof pressure ulcers at much lower rate (11.0%).Bangladesh and Zimbabwe, both low-income undevel-oped nations, reported their secondary complications(Table 4). Bangladesh reported a high incidence of UTIs(62%) and pressure sores (38%), while Zimbabwe re-ported a majority of individuals experienced a general“pain” (77%), while also reporting a high incidence ofpressure sores (33%; Table 4).
The pressure ulcers and UTIs are preventable post-in-jury complications. Proper patient education and nursingavailability can provide vast improvements for the pa-tient and help reduce hospital costs (Barber et al., 1999;Kennedy et al., 2003).
Financial Burdens of Spinal Cord Injury
Although the majority of manuscripts in this reviewdid not focus on the medical costs of SCI, we felt it wasnecessary to address this issue when countries with vary-ing economies are found throughout the world. The Cen-ters for Disease Control estimated that the United Statesspends $9.7 billion ($US) on the treatment of SCI eachyear and that management of pressure ulcers alone, acommon secondary complication of SCI, costs approxi-mately $1.2 billion (2003). It has been estimated thatcosts per SCI patient often exceed $1 million (Mckinleyet al., 1999). Harvey et al. (1992) estimated that the av-erage initial hospital expenditures in the United Stateswere $95,203, home modifications cost $8,203, medicalservices and supplies cost $7,866, and personal assistance(i.e., nurse and homecare) cost $6,269 per year. It hasalso been reported that SCI is the second most expensivecondition to treat in the United States, exceeded only bythe respiratory distress syndrome of infants (Winslow etal., 2002). Moreover, SCI contributes to high hospital ex-penses, ranking third among conditions requiring the
SPINAL CORD INJURY EPIDEMIOLOGY
1367
longest length of stay in hospitals (Winslow et al., 2002).Reports of costs of SCI in Australia predict that, basedon an incidence rate of 25 new cases of injury per mil-lion people per year, by 2006, annual Australian costswould exceed $250 million (Walsh, 1988). Fiedler et al.(1999) describe that quality clinical care for SCI patientsrequires a value-driven approach and that managed careand other cost-preventative measures can shorten thelength of stay in hospitals and reduce overall costs.
There is limited information on the cost of SCI in lessdeveloped countries. Less developed countries do not havesufficient resources to implement programs to effectivelysupport individuals with SCI and their families, often con-demning patients to death after their discharge from the re-habilitation or acute hospital (Levy et al., 1998). In orderto achieve global success in diminishing the financial bur-dens of SCI, especially in less developed countries, researchperformed on injury prevention and medical managementmust be supported and the results disseminated throughglobal organizations like the World Health Organization.The Internet makes this dissemination of information pos-sible, at minimal cost (Edwards et al., 2002).
Injury Prevention and Education
Basic science research has made tremendous progressin the areas of repair and regeneration following SCI(Kwon et al., 2001; Ramer et al., 2000). However, to date,treatments are not available that ensure full recovery, andtherefore, development of injury prevention programs isessential.
Education about methods of injury prevention could de-crease the incidence of SCI, especially with certain causes.MVCs are a highly prevalent cause of SCI, and reinforc-ing the use of seat belts and airbags could have a benefi-cial effect (da Paz et al., 1993). In elderly populations, ed-ucation about the risk of falls could also have beneficialresults. Examples would include educating elderly in thesafe way to move (i.e., handrails, moving with caution onslippery surfaces, and using bathtub rails). In less devel-oped countries, falls result predominantly from carryingheavy objects and falling from heights (Fazlul Hoque et al.,1999; Levy et al., 1998). For example, education on safetree climbing in the Bangladesh population could be ben-eficial for decreasing the high incidence (43%) of falls fromtrees (Fazlul Hoque et al., 1999). It is important to ac-knowledge that the mission statement of the World HealthOrganization (2003) clearly focuses on injury preventionrelated to falls in adolescents and the elderly.
Sports and recreational activities as a cause of SCI areprevalent throughout the world, and specific sports havehigher incidences of SCI (Tator et al., 1993). Many coun-tries must recognize that these trends in sports-relatedSCI emanate especially from contact sports and high-ve-
locity movement sports such as hockey, skiing, and div-ing (O’Connor, 2002; Tator et al., 1993). Preventativeprograms are well implemented in developed countries,but must be translated to less developed countries as well.The World Health Organization (2003) has developed anInternet site that communicates some of this information.
Reporting Data on Spinal Cord Injury in the Future
It is imperative that injury prevention SCI programs andregistries collect similar criteria to allow proper compar-isons between regions. To date, the current World HealthOrganization’s ICD (1992) provides the most thorough andreadily available codes for reporting the etiology of SCI.ICD E codes classify the external cause of injury, while Ncodes classify the nature of injury. It is important to includethe date, location, gender, and age of patients with SCI. Inorder to calculate the most accurate incidence of SCI, stud-ies should also include acute deaths from SCI. Level of in-jury and ASIA/IMSOP scoring should be reported in orderto provide precise and consistent information about sever-ity of injury. If possible, FIM or other functional outcomessuch as walking index for spinal cord injury (WISCI)should be utilized (Ditunno et al., 2000). Follow-up infor-mation should be collected and should include all secondarycomplications—both the total number of SCI patients withcomplications and the types of complications. It is ac-knowledged that lower socio-economic regions of the worldcannot afford to be as thorough as others. However, it isimportant that all data be collected consistently for accu-rate comparisons.
CONCLUSION
SCI is a devastating condition with enormous financial,social, and personal costs. Etiologies of injury vary through-out the world, while countries with similar economic sta-tus display similar trends in SCI etiology. Moreover, coun-tries of similar socio-economic status display similar agedistributions and male-to-female ratios for SCI. Developedcountries display greater age of individuals at the time ofSCI, possibly because of longer life expectancies. Less de-veloped countries have an increased male-to-female ratio,possibly because of the predominant manual labor and risk-taking behavior that males perform in these countries.While conducting this review, we realized the lack of uni-formity in data collection and comparative information ondifferent aspects of SCI throughout the world. In spite ofthese difficulties, this review provides some comparativeinformation among nations, on the causes, incidences, andseverity of SCI. It is recommended that all countries adopta unified method of evaluating and reporting the severity
ACKERY ET AL.
1368
of SCI in order to develop international comparative stud-ies (O’Connor, 2002). Education on injury prevention is anessential tool that is a cost-effective measure, and morecomprehensive programs must be implemented in less de-veloped countries. International effort is required to helpdecrease SCI incidence, a devastating and highly pre-ventable condition. Special initiatives are warranted in or-der to decrease or prevent possible secondary complica-tions of SCI in regions with low socio-economic status.
ACKNOWLEDGMENTS
The authors wish to acknowledge the support and inputof Dr. Theo van Rijn (Vancouver) during the preparationof this manuscript. Research of Dr. C. Tator is supportedby the grants from Ontario Neurotrauma Foundation and the Canadian Institutes of Health Research. Researchof Dr. A. Krassioukov is supported by the grants fromChristopher Reeve Paralysis Foundation, Heart andStroke Foundation of Canada, and British Columbia Neu-rotrauma Fund.
REFERENCES
AUNG, T.S., and EL MASRY, W.S. (1997). Audit of a BritishCentre for spinal injury. Spinal Cord 35, 147–150.
BARBER, D.B., WOODARD, F.L., ROGERS, S.J., and ABLE,A.C. (1999). The efficacy of nursing education as an inter-vention in the treatment of recurrent urinary tract infectionsin individuals with spinal cord injury. SCI. Nurs. 16, 54–56.
BRACKEN, M.B., FREEMAN, D.H., JR., and HELLEN-BRAND, K. (1981). Incidence of acute traumatic hospital-ized spinal cord injury in the United States, 1970–1977. Am.J. Epidemiol. 113, 615–622.
BRACKEN, M.B., and HOLFORD, T.R. (2002). Neurologicaland functional status 1 year after acute spinal cord injury: es-timates of functional recovery in National Acute Spinal CordInjury Study II from results modeled in National Acute SpinalCord Injury Study III. J. Neurosurg. 96, 259–266.
BRACKEN, M.B., SHEPARD, M.J., HOLFORD, T.R., et al.(1997). Administration of methylprednisolone for 24 or 48hours or tirilazad mesylate for 48 hours in the treatment ofacute spinal cord injury. Results of the third National AcuteSpinal Cord Injury randomized controlled trial. JAMA 277,1597–1604.
CATZ, A., THALEISNUK, M., FISHEL, B., et al. (2002). Sur-vival following spinal cord injury in Israel. Spinal Cord 40,595–598.
CENTERS FOR DISEASE CONTROL AND PREVENTION.(2003). Available: www.cdc.gov/ncipc/fact_book/25_Spinal_Cord_Injury.htm.
DA PAZ, A.C., BERALDO, P.S., ALMEIDA, M.C., NEVES,E.G., ALVES, C.M., and KHAN, P. (1993). Traumatic in-jury to the spinal cord. Prevalence in Brazilian hospitals.Paraplegia 30, 636–640.
DINCER, F., OFLAZER, A., BEYAZOVA, M., CELIKER, R.,BASGÖZE, O., and ALTIOKLAR, K. (1992). Traumaticspinal cord injuries in Turkey. Paraplegia 30, 641–646.
DITUNNO, J.F., DITUNNO, P.L., GRAZIANI, V., et al.(2000). Walking index for spinal cord injury (WISCI): an in-ternational multicenter validity and reliability study. SpinalCord 38, 234–243.
DITUNNO, J.F., YOUNG, W., DONOVAN, W.H., andCREASEY, G. (1994). The international standards bookletof neurological and functional classification of spinal cordinjury patients. Paraplegia 32, 736–742.
DRYDEN, D.M., SAUNDERS, L.D., ROWE, B.H., et al.(2003). The epidemiology of traumatic spinal cord injury inAlberta, Canada. Can. J. Neurol. Sci. 30, 113–121.
EDWARDS, L., KRASSIOUKOV, A.V., and FEHLINGS,M.G. (2002). Importance of access to research informationamong individuals with spinal cord injury: results of an ev-idenced based questionnaire. Spinal Cord 40, 529–535.
EXNER, G., and MEINECKE, F.-W. (1997). Trends in thetreatment of patients with spinal cord lesions seen with a pe-riod of 20 years in German centers. Spinal Cord 35, 415–419.
FAZLUL HOQUE, M.D., GRANGEON, C., and REED, K.(1999). Spinal cord lesions in Bangladesh: an epidemiolog-ical study 1994–1995. Spinal Cord 37, 858–861.
FEHLINGS, M.G., SEKHON, L.H., and TATOR, C. (2001).The role and timing of decompression in acute spinal cordinjury: what do we know? What should be do? Spine 26,S101–S110.
FIEFLER, I.G., LAUD, P.W., MAIMAN, D.J., and APPLE,D.F. (1999). Economics of managed care in spinal cord in-jury. Arch. Phys. Med. Rehabil. 80, 1441–1449.
FRANKEL, H.L., HANCOCK, D.O., HYSLOP, G., et al.(1969). The value of postural reduction in the initial man-agement of closed injuries of the spine with paraplegia andtetraplegia. Paraplegia 7, 179–192.
GEISLER, F.H., COLEMAN, W.P., GRIECO, G., POONIAN,D., and SYGEN® STUDY GROUP. (2002). Recruitment andearly treatment in a multicenter study of acute spinal cord in-jury. Spine 26, S58–S67.
GEISLER, F.H., DORSEY, F.C., and COLEMAN, W.P.(1992). GM-1 ganglioside: motor recovery after humanspinal cord injury in a randomized, placebo-controlled trial.Fidia Res. Found. Symp. Series 9, 255–259.
HART, C., and WILLIAMS, E. (1994). Epidemiology of spinalcord injuries: a reflection of changes in South African soci-ety. Paraplegia 32, 709–714.
SPINAL CORD INJURY EPIDEMIOLOGY
1369
HARVEY, C., WILSON, S.E., GREENE, C.G., BERKOWITZ,M., and STRIPLING, T.E. (1992). New estimates of the di-rect costs of traumatic spinal cord injuries: results of a na-tionwide survey. Paraplegia 30, 834–850.
HURLBERT, R.J. (2000). Methylprednisolone for acute spinalcord injury: an inappropriate standard of care. J. Neurosurg.93, 1–7.
International Statistical Classification of Diseases (ICD) andRelated Health Problems. (1992). World Health Organiza-tion: Geneva.
KENNEDY, P., BERRY, C., COGGRAVE, M., ROSE, L., andHAMILTON, L. (2003). The effect of a specialist seating as-sessment clinic on the skin management of individuals withspinal cord injury. J. Tiss. Viability 13, 122–125.
KRASSIOUKOV, A.V., FURLAN, J.C., and FEHLINGS,M.G. (2003). Medical co-morbidities, secondary complica-tions, and mortality in elderly with acute spinal cord injury.J. Neurotrauma 20, 391–399.
KWON, B.K., and TETZLAFF, W. (2001). Spinal cord regen-eration: from gene to transplants. Spine 26, S13–S22.
LEVI, R., HULTLING, C., NASH, M.S., and SEIGER, A.(1995). The Stockholm Spinal Cord Injury Study: 1. Med-ical problems in a regional SCI population. Paraplegia 33,308–315.
LEVY, L.F., MAKAROWO, S., MADZIVIRE, D., BHEBHE,E., VERBEEK, N., and PARRY, O. (1998). Problems, strug-gles and some success with spinal cord injury in Zimbabwe.Spinal Cord 36, 213–218.
MARTINS, F., FREITAS, F., MARTINS, L., DARTIGUES,J.F., and BARAT, M. (1998). Spinal cord injuries—epi-demiologies in Portugal’s central region. Spinal Cord 36,574–578.
MAYNARD, F.M., JR., BRACKEN, M.B., CREASEY, G., etal. (1997). International standards for neurological and func-tional classification of spinal cord injury. American SpinalInjury Association. Spinal Cord 35, 266–274.
MCCOLL, M.A., CHARLIFUE, S., GLASS, G., SAVIC, G.,and MEEHAN, M. (2002). International differences in age-ing and spinal cord injury. Spinal Cord 40, 128–136.
MCKINLEY, W.O., JACKSON, A.B., CARDENAS, D.D., andDEVIVO, M.J. (1999). Long-term medical complications af-ter traumatic spinal cord injury: a regional model systemsanalysis. Arch. Phys. Med. Rehabil. 80, 1402–1410.
NOBUNAGA, A.I., GO, B.K., and KARUNAS, R.B. (1999).Recent demographic and injury trends in people served bythe model spinal cord injury care systems. Arch. Phys. Med.Rehabil. 80, 1372–1382.
O’CONNOR, P. (2002). Incidence and patterns of spinal cordinjury in Australia. Accid. Anal. Prev. 34, 405–415.
PAGLIACCI, M.C., GRAZIA CELANI, M., ZAMPOLINI, M.,et al. (2003). An Italian survey of traumatic spinal injury.The Gruppo Italiano Studio Epidemiologico MielolesioniStudy. Arch. Phys. Med. Rehabil. 84, 1266–1275.
PRIEBE, M., and WARING, W.P. (1991). The interobserverreliability of the revised American Spinal Injury Associationstandards for neurological classification of spinal injury pa-tients. Am. J. Phys. Med. Rehabil. 70, 268–270.
RAMER, M.S., HARPER, G.P., and BRADBURY, E.J. (2000).Progress in spinal cord research—a refined strategy for theInternational Spinal Research Trust. Spinal Cord 38,449–472.
RAVAUD, J.-F., DELCEY, M., DESERT, J.-F., andTETRAFIGAP GROUP. (2000). The Tetrafigap Survey onthe long-term outcome of tetraplegic spinal cord injured per-sons. Part II: Demographic characteristics and initial causeof injury. Spinal Cord 38, 164–172.
SEKHON, L.H., and FEHLINGS, M.G. (2001). Epidemiology,demographics, and pathophysiology of acute spinal cord in-jury. Spine 26, S2–12.
SHINGU, H., IKATA, T., KATOH, S., and AKATSU, T.(1994). Spinal cord injuries in Japan: a nationwide epidemi-ological survey in 1990. Paraplegia 32, 3–8.
SILBERSTEIN, B., and RABINOVICH, S. (1995). Epidemi-ologies of spinal cord injuries in Novosibirsk, Russia. Para-plegia 33, 322–325.
TATOR, C.H. (1995). Update on the pathophysiology andpathology of acute spinal cord injury. Brain Pathol. 5,407–413.
TATOR, C.H. (2000). Epidemiology and general characteris-tics of the spinal cord–injured patient, in: ContemporaryManagement of SCI: From Impact to Rehabilitation. C.H.Tator and E.C. Benzel (eds), AANS: Park Ridge, IL, pps.15–19.
TATOR, C.H., DUNCAN, E.G., EDMONDS, V.E.,LAPCZAK, L.I., and ANDREWS, D.F. (1993). Changes inepidemiology of acute spinal cord injury from 1947 to 1981.Surg. Neurol. 40, 207–215.
WALSH, J. (1988). Costs of spinal cord injury in Australia.Paraplegia 26, 380–388.
WINSLOW, C., BODE, R.K., FELTON, D., CHEN, D., andMEYER, P.R. (2002). Impact of respiratory complicationson length of stay and hospital costs in acute cervical spineinjury. Chest 121, 1548–1554.
WORLD BANK GROUP. (2003). Available: www.worldbank.org/data.
WORLD HEALTH ORGANIZATION. (2003). Available:www.who.int.en/.
1. B B Lee, R A Cripps, M Fitzharris, P C Wing. 2013. The global map for traumatic spinal cord injury epidemiology: update2011, global incidence rate. Spinal Cord . [CrossRef]
2. H F Wang, Z S Yin, Y Chen, Z H Duan, S Hou, J He. 2013. Epidemiological features of traumatic spinal cord injury in AnhuiProvince, China. Spinal Cord 51:1, 20-22. [CrossRef]
3. Wen-Jie Li, Shu-Min Li, Ying Ding, Bing He, Jack Keegan, Hongxin Dong, Jing-Wen Ruan, Yuan-Shan Zeng. 2012. Electro-acupuncture upregulates CGRP expression after rat spinal cord transection. Neurochemistry International 61:8, 1397-1403.[CrossRef]
4. Andrea J. Mothe, Charles H. Tator. 2012. Advances in stem cell therapy for spinal cord injury. Journal of Clinical Investigation122:11, 3824-3834. [CrossRef]
5. Guillermo J. Cruz, Rodrigo Mondragón-Lozano, Araceli Diaz-Ruiz, Joaquín Manjarrez, Roberto Olayo, Hermelinda Salgado-Ceballos, Maria-Guadalupe Olayo, Juan Morales, Laura Alvarez-Mejía, Axayacatl Morales, Marisela Méndez-Armenta, NoelPlascencia, Maria Carmen Fernandez, Camilo Ríos. 2012. Plasma polypyrrole implants recover motor function in rats after spinalcord transection. Journal of Materials Science: Materials in Medicine 23:10, 2583-2592. [CrossRef]
6. L Sabre, G Pedai, T Rekand, T Asser, Ü Linnamägi, J Kõrv. 2012. High incidence of traumatic spinal cord injury in Estonia.Spinal Cord 50:10, 755-759. [CrossRef]
7. H S Chhabra, M Arora. 2012. Demographic profile of traumatic spinal cord injuries admitted at Indian Spinal Injuries Centrewith special emphasis on mode of injury: a retrospective study. Spinal Cord 50:10, 745-754. [CrossRef]
8. Christine Boldt, Inge-Marie Velstra, Mirjam Brach, Elisabeth Linseisen, Alarcos Cieza. 2012. Nurses' intervention goal categoriesfor persons with spinal cord injury based on the International Classification of Functioning, Disability and Health: an internationalDelphi survey. Journal of Advanced Nursing n/a-n/a. [CrossRef]
9. Susan E. Mackinnon, Andrew Yee, Wilson Z. Ray. 2012. Nerve transfers for the restoration of hand function after spinal cordinjury. Journal of Neurosurgery 117:1, 176-185. [CrossRef]
10. Andrew J. Shoffstall, Dawn M. Taylor, Erin B. Lavik. 2012. Engineering therapies in the CNS: What works and what can betranslated. Neuroscience Letters 519:2, 147-154. [CrossRef]
11. Elizabeth Nicholls, Tara Lehan, Silvia Leonor Olivera Plaza, Xiaoyan Deng, Jose Libardo Perdomo Romero, Jose Anselmo ArangoPizarro, Juan Carlos Arango-Lasprilla. 2012. Factors influencing acceptance of disability in individuals with spinal cord injury inNeiva, Colombia, South America. Disability and Rehabilitation 34:13, 1082-1088. [CrossRef]
12. Peter Bragge, Marisa Chau, Veronica Jean Pitt, Mark Theodore Bayley, Janice Jennifer Eng, Robert William Teasell, Dalton LouisWolfe, Russell Lindsay Gruen. 2012. An Overview of Published Research about the Acute Care and Rehabilitation of TraumaticBrain Injured and Spinal Cord Injured Patients. Journal of Neurotrauma 29:8, 1539-1547. [Abstract] [Full Text HTML] [FullText PDF] [Full Text PDF with Links] [Supplemental Material]
13. J R Wilson, A Singh, C Craven, M C Verrier, B Drew, H Ahn, M Ford, M G Fehlings. 2012. Early versus late surgery fortraumatic spinal cord injury: the results of a prospective Canadian cohort study. Spinal Cord . [CrossRef]
14. Maya Srikanth, John A. Kessler. 2012. Nanotechnology—novel therapeutics for CNS disorders. Nature Reviews Neurology 8:6,307-318. [CrossRef]
15. Jared T. Wilcox, David Cadotte, Michael G. Fehlings. 2012. Spinal cord clinical trials and the role for bioengineering. NeuroscienceLetters . [CrossRef]
16. Ellen Hagen, Tiina Rekand, Nils Gilhus, Marit Grønning. 2012. Traumatiske ryggmargsskader - forekomst, skademekanismerog forløp. Tidsskrift for Den norske legeforening 132:7, 831-837. [CrossRef]
17. Patrick Shih, Richard G. FesslerTrauma of the Nervous System 957-983. [CrossRef]18. David W. Cadotte, Michael G. FehlingsSpinal Cord Injury 445-454. [CrossRef]19. N. Paul Rosman, Chellamani HariniSpinal Cord Injury 1198-1220. [CrossRef]20. Jefferson R. Wilson, Michael G. Fehlings. 2011. Adrenal Insufficiency as a Cause of Refractory Hypotension in the Acute Period
After Spinal Cord Injury: A Perspective Statement. World Neurosurgery . [CrossRef]21. N Draulans, C Kiekens, E Roels, K Peers. 2011. Etiology of spinal cord injuries in Sub-Saharan Africa. Spinal Cord . [CrossRef]22. S Knútsdóttir, H Thórisdóttir, K Sigvaldason, H Jónsson, A Björnsson, P Ingvarsson. 2011. Epidemiology of traumatic spinal
cord injuries in Iceland from 1975 to 2009. Spinal Cord . [CrossRef]
23. J Li, G Liu, Y Zheng, C Hao, Y Zhang, B Wei, H Zhou, D Wang. 2011. The epidemiological survey of acute traumatic spinalcord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord 49:7, 777-782. [CrossRef]
24. P R Lucareli, M O Lima, F P S Lima, J G de Almeida, G C Brech, J M D'Andréa Greve. 2011. Gait analysis following treadmilltraining with body weight support versus conventional physical therapy: a prospective randomized controlled single blind study.Spinal Cord . [CrossRef]
25. R A Cripps, B B Lee, P Wing, E Weerts, J Mackay, D Brown. 2011. A global map for traumatic spinal cord injury epidemiology:towards a living data repository for injury prevention. Spinal Cord 49:4, 493-501. [CrossRef]
26. Jefferson R. Wilson, Michael G. Fehlings. 2011. Emerging Approaches to the Surgical Management of Acute Traumatic SpinalCord Injury. Neurotherapeutics 8:2, 187-194. [CrossRef]
27. K H Herrmann, I Kirchberger, G Stucki, DF Swaab. 2011. The Comprehensive ICF core sets for spinal cord injury from theperspective of physical therapists: a worldwide validation study using the Delphi technique. Spinal Cord 49:4, 502-514. [CrossRef]
28. Syed Johar Raza, Muhammad Shahzad Shamim, Saniya Siraj Godil, S. Raziuddin Biyabani, Muhammad Ehsan Bari, RajeshKumar, Atta ul Aleem Bhatti, Saeed Soomro. 2011. Lack of improvement after audit assessing the management of voidingdysfunction in patients with spinal cord injury: Necessity for institutional guidelines. International Journal of Surgery 9:4, 302-305.[CrossRef]
29. Maya Siman-Tov, Dena H. Jaffe, Kobi Peleg. 2010. Bicycle injuries: A matter of mechanism and age. Accident Analysis & Prevention. [CrossRef]
30. G Zeilig, H P Weingarden, M Zwecker, D Rubin-Asher, A Ratner, MH Libenson. 2010. Civilian spinal cord injuries due toterror explosions. Spinal Cord 48:11, 814-818. [CrossRef]
31. M. Brett Runge, Mahrokh Dadsetan, Jonas Baltrusaitis, Andrew M. Knight, Terry Ruesink, Eric A. Lazcano, Lichun Lu, AnthonyJ. Windebank, Michael J. Yaszemski. 2010. The development of electrically conductive polycaprolactone fumarate–polypyrrolecomposite materials for nerve regeneration. Biomaterials 31:23, 5916-5926. [CrossRef]
32. Jennifer C. Fleming, Feng Bao, Gediminas Cepinskas, Lynne C. Weaver. 2010. Anti-α4β1 integrin antibody induces receptorinternalization and does not impair the function of circulating neutrophilic leukocytes. Inflammation Research 59:8, 647-657.[CrossRef]
33. Wen-Jie Li, San-Qiang Pan, Yuan-Shan Zeng, Bao-Gui Su, Shu-Min Li, Ying Ding, Yan Li, Jing-Wen Ruan. 2010. Identificationof acupuncture-specific proteins in the process of electro-acupuncture after spinal cord injury. Neuroscience Research 67:4, 307-316.[CrossRef]
34. M Scheuringer, I Kirchberger, C Boldt, I Eriks-Hoogland, A Rauch, I-M Velstra, A Cieza. 2010. Identification of problems inindividuals with spinal cord injury from the health professional perspective using the ICF: a worldwide expert survey. Spinal Cord48:7, 529-536. [CrossRef]
35. Vibhu Sahni, John A. Kessler. 2010. Stem cell therapies for spinal cord injury. Nature Reviews Neurology 6:7, 363-372. [CrossRef]36. Ward T. Plunet, Clarrie K. Lam, Jae H. T. Lee, Jie Liu, Wolfram Tetzlaff. 2010. Prophylactic dietary restriction may promote
functional recovery and increase lifespan after spinal cord injury. Annals of the New York Academy of Sciences 1198, E1-E11.[CrossRef]
37. E M Hagen, G E Eide, T Rekand, N E Gilhus, M Gronning. 2010. A 50-year follow-up of the incidence of traumatic spinal cordinjuries in Western Norway. Spinal Cord 48:4, 313-318. [CrossRef]
38. Nuno A. Silva, Antonio J. Salgado, Rui A. Sousa, Joao T. Oliveira, Adriano J. Pedro, Hugo Leite-Almeida, Rui Cerqueira,Armando Almeida, Fabrizio Mastronardi, João F. Mano, Nuno M. Neves, Nuno Sousa, Rui L. Reis. 2010. Development andCharacterization of a Novel Hybrid Tissue Engineering–Based Scaffold for Spinal Cord Injury Repair. Tissue Engineering Part A16:1, 45-54. [Abstract] [Full Text HTML] [Full Text PDF] [Full Text PDF with Links]
39. Kim D. Anderson, Kelli G. Sharp, Maura Hofstadter, Karen-Amanda Irvine, Marion Murray, Oswald Steward. 2009. Forelimblocomotor assessment scale (FLAS): Novel assessment of forelimb dysfunction after cervical spinal cord injury. ExperimentalNeurology 220:1, 23-33. [CrossRef]
40. Seung-Hoon Lee, You-Nam Chung, Yoon-Ha Kim, Young-Ju Kim, Jong-Pil Park, Dae-Kee Kwon, Oh-Seo Kwon, Jae-HyeokHeo, Yoon-Hee Kim, Sun Ryu, Hyo-Jin Kang, Sun Ha Paek, Kyu-Chang Wang, Seung U. Kim, Byung-Woo Yoon. 2009. Effectsof human neural stem cell transplantation in canine spinal cord hemisection. Neurological Research 31:9, 996-1002. [CrossRef]
41. Michael G. Fehlings, Allyson Tighe. 2009. Editorial. Journal of Neurosurgery: Spine 11:3, 253-254. [CrossRef]42. A E Tawashy, J J Eng, K H Lin, P F Tang, C Hung. 2009. Physical activity is related to lower levels of pain, fatigue and depression
in individuals with spinal-cord injury: a correlational study. Spinal Cord 47:4, 301-306. [CrossRef]
43. Andrei Krassioukov, Darren E. Warburton, Robert Teasell, Janice J. Eng. 2009. A Systematic Review of the Management ofAutonomic Dysreflexia After Spinal Cord Injury. Archives of Physical Medicine and Rehabilitation 90:4, 682-695. [CrossRef]
44. Daniel Garcia-Ovejero, Angel Arevalo-Martin, Stefania Petrosino, Fabian Docagne, Carlos Hagen, Tiziana Bisogno, MasahikoWatanabe, Carmen Guaza, Vincenzo Di Marzo, Eduardo Molina-Holgado. 2009. The endocannabinoid system is modulated inresponse to spinal cord injury in rats. Neurobiology of Disease 33:1, 57-71. [CrossRef]
45. Michael G. Fehlings, Allyson Tighe. 2008. Spinal Cord Injury: The Promise of Translational Research. Neurosurgical FOCUS25:5, E1. [CrossRef]
46. Ward T. Plunet, Femke Streijger, Clarrie K. Lam, Jae H.T. Lee, Jie Liu, Wolfram Tetzlaff. 2008. Dietary restriction started afterspinal cord injury improves functional recovery. Experimental Neurology 213:1, 28-35. [CrossRef]
47. Vishal C. Gala, Jean-Marc Voyadzis, Dae-Hyun Kim, Alparslan Asir, Richard G. FesslerTrauma of the Nervous System 1115-1144.[CrossRef]
48. E V Sidorov, A F Townson, M F Dvorak, B K Kwon, J Steeves, A Krassioukov. 2008. Orthostatic hypotension in the first monthfollowing acute spinal cord injury. Spinal Cord 46:1, 65-69. [CrossRef]
49. Shucui Jiang, Farid Bendjelloul, Patrizia Ballerini, Iolanda D’Alimonte, Elenora Nargi, Cai Jiang, Xinjie Huang, Michel P.Rathbone. 2007. Guanosine reduces apoptosis and inflammation associated with restoration of function in rats with acute spinalcord injury. Purinergic Signalling 3:4, 411-421. [CrossRef]
50. Jozef Paulus Henricus Johannes Rutges, F. Cumhur Oner, Luke Peter Hendrik Leenen. 2007. Timing of thoracic and lumbarfracture fixation in spinal injuries: a systematic review of neurological and clinical outcome. European Spine Journal 16:5, 579-587.[CrossRef]
51. Grégoire Courtine, Mary Bartlett Bunge, James W Fawcett, Robert G Grossman, Jon H Kaas, Roger Lemon, Irin Maier, JohnMartin, Randolph J Nudo, Almudena Ramon-Cueto, Eric M Rouiller, Lisa Schnell, Thierry Wannier, Martin E Schwab, VReggie Edgerton. 2007. Can experiments in nonhuman primates expedite the translation of treatments for spinal cord injury inhumans?. Nature Medicine 13:5, 561-566. [CrossRef]
52. A HOL, J ENG, W MILLER, S SPROULE, A KRASSIOUKOV. 2007. Reliability and Validity of the Six-Minute Arm Testfor the Evaluation of Cardiovascular Fitness in People With Spinal Cord Injury. Archives of Physical Medicine and Rehabilitation88:4, 489-495. [CrossRef]
53. Peter ReillyThe impact of neurotrauma on society: an international perspective 161, 3-9. [CrossRef]54. Victoria E. Claydon, Andrei V. Krassioukov. 2006. Orthostatic Hypotension and Autonomic Pathways after Spinal Cord Injury.
Journal of Neurotrauma 23:12, 1713-1725. [Abstract] [Full Text PDF] [Full Text PDF with Links]55. K D Anderson, J F Borisoff, R D Johnson, S A Stiens, S L Elliott. 2006. The impact of spinal cord injury on sexual function:
concerns of the general population. Spinal Cord . [CrossRef]56. P L Ditunno, M Patrick, M Stineman, B Morganti, A F Townson, J F Ditunno. 2006. Cross-cultural differences in preference
for recovery of mobility among spinal cord injury rehabilitation professionals. Spinal Cord 44:9, 567-575. [CrossRef]57. F Biering-Sørensen, M Scheuringer, M Baumberger, S W Charlifue, M W M Post, F Montero, N Kostanjsek, G Stucki. 2006.
Developing core sets for persons with spinal cord injuries based on the International Classification of Functioning, Disability andHealth as a way to specify functioning. Spinal Cord 44:9, 541-546. [CrossRef]
58. V CLAYDON, A HOL, J ENG, A KRASSIOUKOV. 2006. Cardiovascular Responses and Postexercise Hypotension After ArmCycling Exercise in Subjects With Spinal Cord Injury. Archives of Physical Medicine and Rehabilitation 87:8, 1106-1114. [CrossRef]
59. V E Claydon, J D Steeves, A Krassioukov. 2006. Orthostatic hypotension following spinal cord injury: understanding clinicalpathophysiology. Spinal Cord 44:6, 341-351. [CrossRef]
60. Marca L. Sipski, J Scott Richards. 2006. Spinal Cord Injury Rehabilitation. American Journal of Physical Medicine & Rehabilitation85:4, 310-342. [CrossRef]