Acute Infection with Microbes and Their Consequences Mark Riddle, MD, DrPH Associate Professor Dept. of Preventive Medicine & Biostatistics Uniformed Services University of the Health Sciences Bethesda, Maryland
Transcript
Acute Infection with Microbes and
Their Consequences
Mark Riddle, MD, DrPH
Associate Professor
Dept. of Preventive Medicine & Biostatistics
Uniformed Services University of the Health Sciences
Bethesda, Maryland
Gastrointestinal Tract in Health and Disease
Detoxification
Digestive tract
Immunity
Food allergies
Autoimmune diseases
Mix-ups
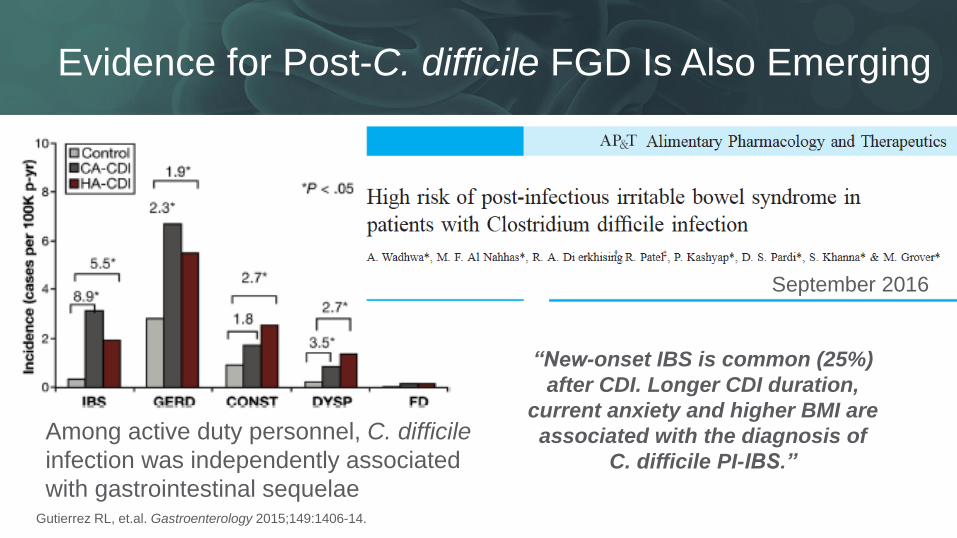
Post-infectious sequelae
Acute enteric infection risk: 50M in US each year
(Centers for Disease Control & Prevention, 2015)
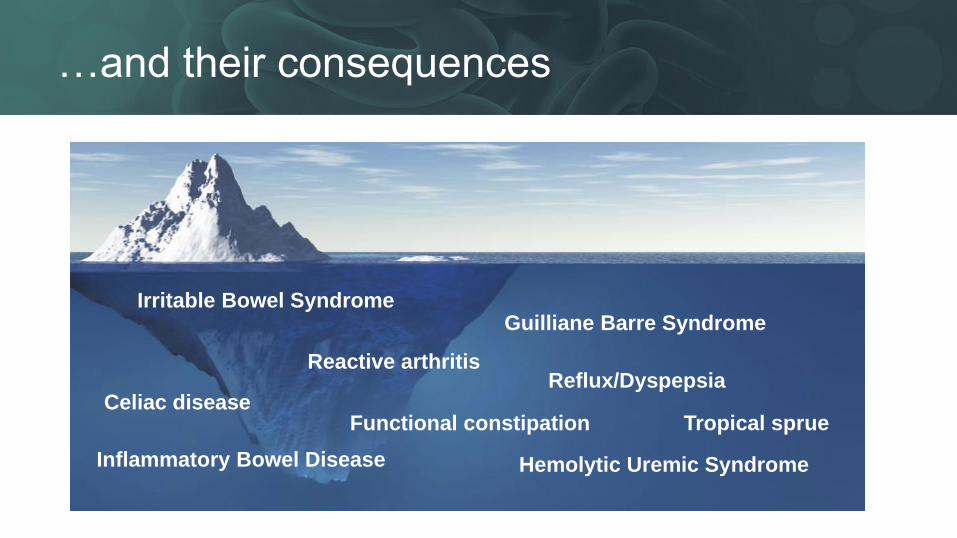
…and their consequences
Irritable Bowel Syndrome Guilliane Barre Syndrome
Functional constipation
Reactive arthritis
Hemolytic Uremic Syndrome
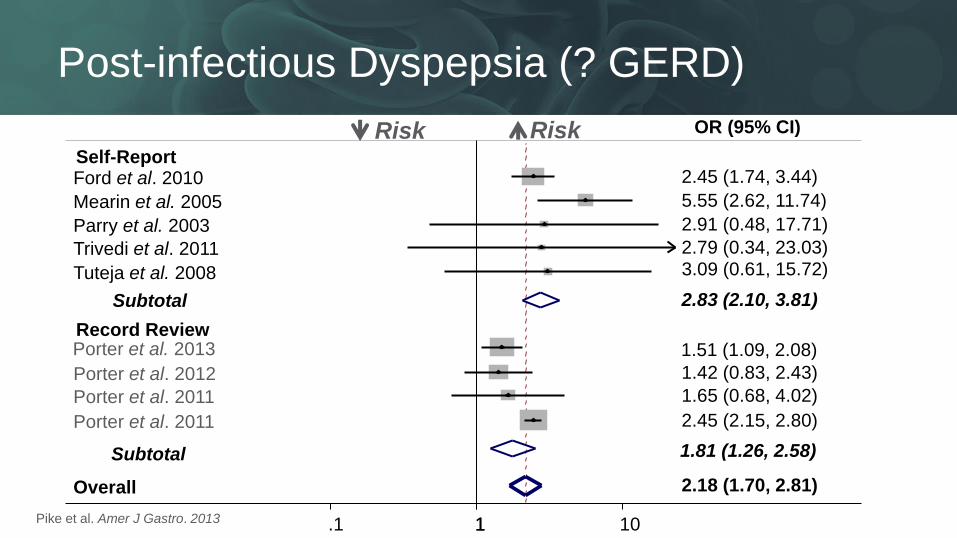
Reflux/Dyspepsia Celiac disease
Inflammatory Bowel Disease
Tropical sprue
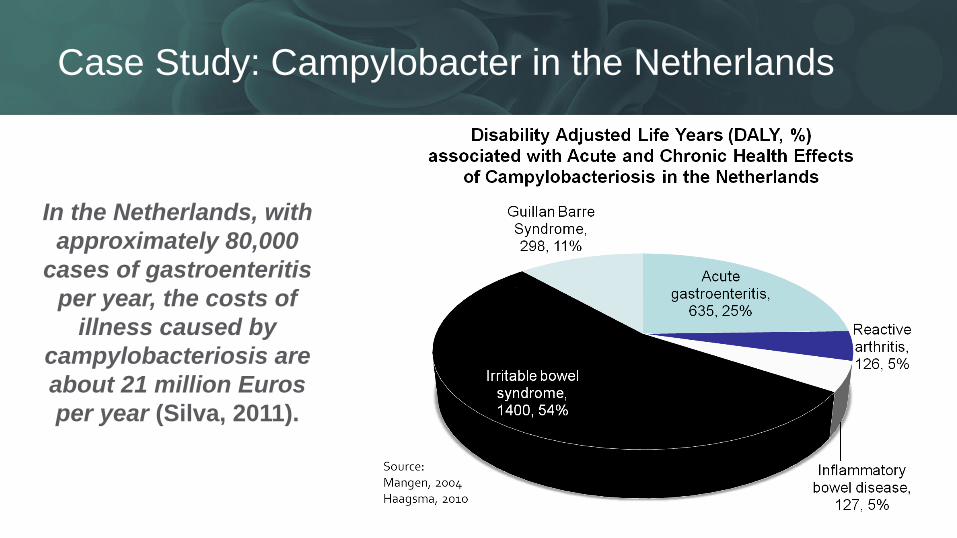
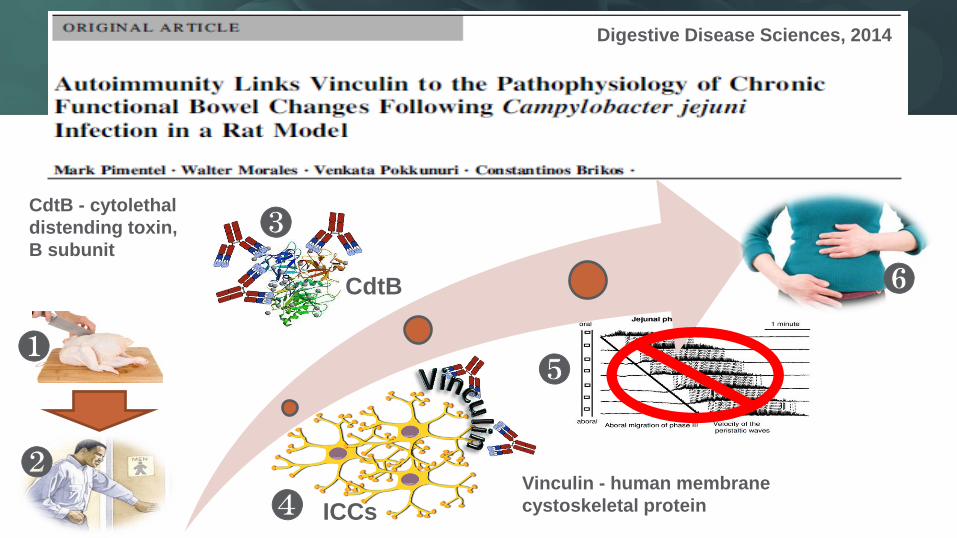
Case Study: Campylobacter in the Netherlands
In the Netherlands, with
approximately 80,000
cases of gastroenteritis
per year, the costs of
illness caused by
campylobacteriosis are
about 21 million Euros
per year (Silva, 2011).
Sudden, permanent sequelae
Progressive disease
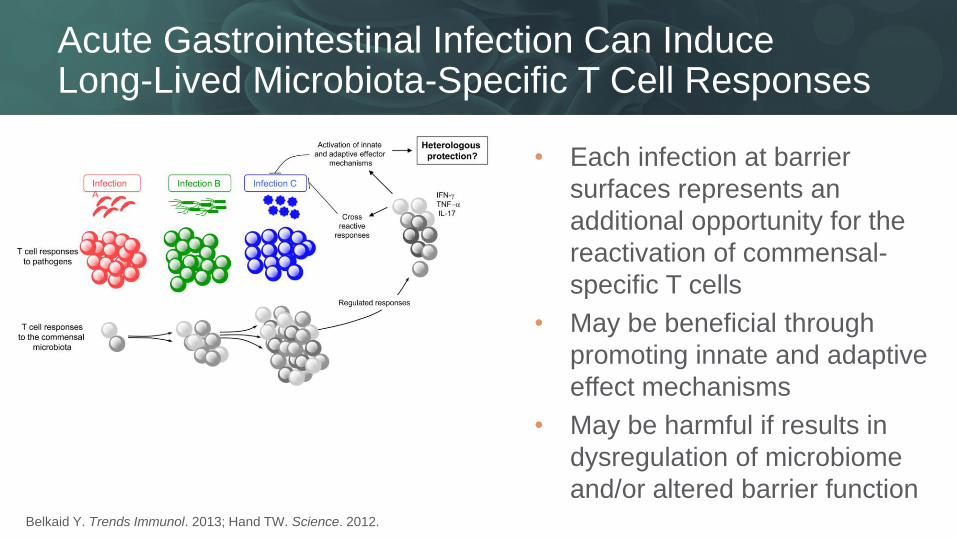
Immune process
Persistent infection
Infe
cti
on
Symptomatic disease
Symptomatic disease
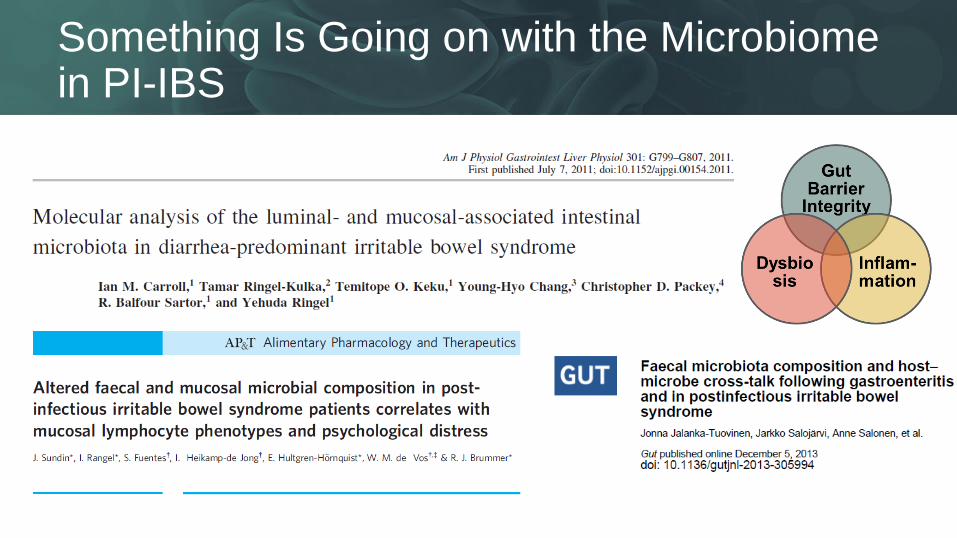
Dysbiotic process Symptomatic disease
Infectious Causes of Chronic Disease Association Causation Mechanism
EXAMPLES
•polio, malaria, meningitis
•histoplasmosis,
lyme disease
•rheumatic arthritis,
systemic lupus, GBS
•Hepatitis B virus, H. pylori,
HPV, HIV
•IBS, obesity, ? mood
disorders…
Adapted from O’Conner, et al, EID, Vol. 12, No. 7, July 2006.
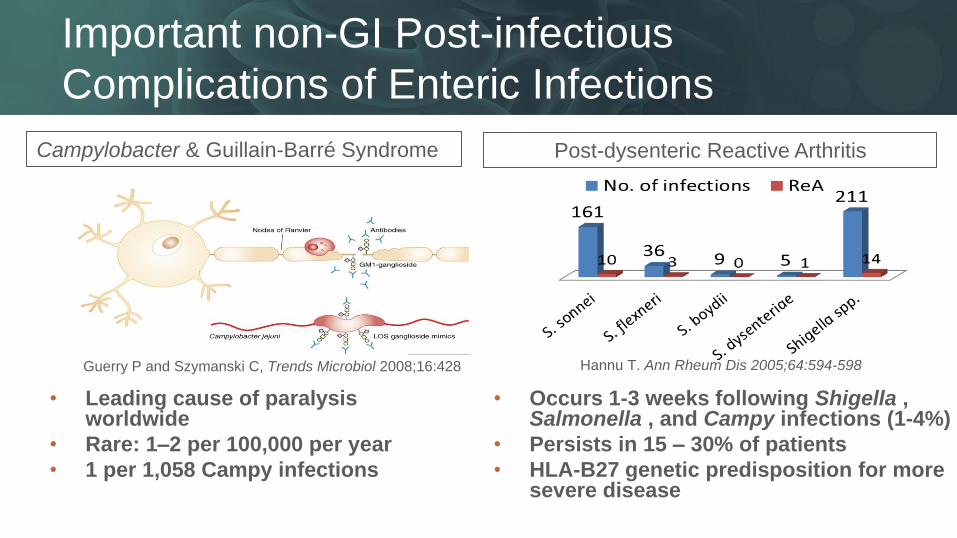
Important non-GI Post-infectious
Complications of Enteric Infections
• Leading cause of paralysis worldwide
• Rare: 1–2 per 100,000 per year
• 1 per 1,058 Campy infections
• Occurs 1-3 weeks following Shigella , Salmonella , and Campy infections (1-4%)
• Persists in 15 – 30% of patients
• HLA-B27 genetic predisposition for more severe disease
Guerry P and Szymanski C, Trends Microbiol 2008;16:428
• Prebiotics/synbiotics: preventive effects in TD is limited and mixed – Cummings J et al. Aliment Pharmacol Ther. 2001
– Drakoularakou A et al. Eur J Clin Nutr. 2010
– Virk A et al. Journal of Travel Medicine. 2013
Am J Gastro, April 2016
Practical Advice for the Clinician (Part 1)
Diagnosis
• Work-up cases of dysentery, moderate–severe disease, and symptoms lasting >7 days to clarify the etiology and enable specific directed therapy.
Treatment
• Don’t use antibiotics routinely for community acquired diarrhea (mostly viral)
• Do encourage use of single dose antibiotic therapy (with loperamide) for treatment of travelers’ diarrhea
Counseling
• Prevention counseling of acute enteric infection is not routinely recommended but may be considered in the individual or close contacts of the individual who is at high risk for complications.
Practical Advice for the Clinician (Part 2)
Prophylaxis
• Bismuth subsalicylates have moderate effectiveness and may be considered for travelers who do not have any contraindications to use and can adhere to the frequent dosing requirements
• Probiotics, prebiotics, and synbiotics for prevention of TD are not recommended.
• Antibiotic chemoprophylaxis has moderate to good effectiveness and may be considered in high-risk groups for short-term use.
Gaps
• No current guidelines on work-up of post-infectious FGD
• No unique studies evaluating therapeutic effectiveness in PI-FGD
• No studies evaluating effect of TD prevention on reduction of PI-FGD risk
• Studies evaluating TD prevention in IBS patients are needed
• Naval Medical Research Center
– Chad Porter, Brian Pike, Ramiro Gutierrez
• Armed Forces Health Surveillance Center
– Angie Eick-Cost and entire staff AFHSC/DoDSR staff
• University of Alabama
– Chuck Elson, Ben Christmann
• Uniformed Services University
– David Tribble
• The study protocols of presenter’s data were approved by institutional review boards in compliance with
all applicable Federal regulations governing the protection of human subjects.
• Funding: Department of Defense, International Society of Travel Medicine