An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
Carlo P. Campobasso1*, Massimo F. Colonna2, Fiorenza Zotti2, Sara Sblano2, Alessandro S. Dell’Erba2
_________________________________________________________________________________________ Abstract: SP-A is the most prevalent protein component of pulmonary surfactant which is essential to maintain alveolar stability. SP-A can be detected by immunohistochemistry and in such form it has been previously reported as a useful tool to distinguish aspyxial deaths from other hypoxic cases. The present immunohistochemical study shows the SP-A staining distribution among a selected forensic material to evaluate the effect of fluid accumulation in the lung interstitium and alveoli commonly related to pulmonary edema. A total of 48 cases were examined histologically and immuno-histochemically based on the presence/absence of pulmonary edema and survival time: 10 cases of acute cardiac deaths (ACDs) in which death occurred rapidly, in a few minutes from the beginning of the symptoms and without signs of pulmonary edema, 18 cases of drowning (12 in saltwater and 6 cases in freshwater), 20 cases of narcotic deaths (6 by cocaine and 14 by opiates) with gross pulmonary edema. The results suggest that edema fluid can produce some kind of molecular alterations of SP-A affecting immunostaining expression. The results show also that SP-A immunostaining patterns alone do not meet the requirements for general diagnostic use and cannot differentiate among fatalities. The SP-A expression needs to be preferably associated with the presence and intensity of histological signs according to suspected cause of death as well as type and amount of edema fluid commonly related to cardiac and/or respiratory failure (cardiogenic and non-cardiogenic pulmonary edema). Key Words: Pulmonary surfactant-associated protein A, immunohistochemistry, drowning, narcotic deaths, acute cardiac deaths, pulmonary edema.
1) * Corresponding author: PhD, MD, Department of Health Sciences (S.pe.S), University of Molise – Via De Sanctis, snc., 86100 - CAMPOBASSO - ITALY, Phone: 0039 - 0874 - 404 776, Fax : 0039 - 0874 – 404 778, Email:[email protected], [email protected]) Section of Legal Medicine (Di.M.I.M.P.), University of Bari, Policlinico, Piazza Giulio Cesare, 70124, Bari (Italy)
Pulmonary surfactant is a lipoprotein essential for normal lung function as it
maintains alveolar stability [1]. It covers the surface of the alveoli and prevents alveolar collapse by reducing surface tension at the air-liquid interface [2] . Surfactant-associated proteins (SPs) are very important constituents of pulmonary surfactant since the first successful treatment of neonatal respiratory distress syndrome with surfactant replacement therapy [3]. SP-A is the most prevalent form and the major protein component of pulmonary surfactant [4]. It is a hydrophilic and large collagen-like glycoprotein produced by the alveolar type II cells and by the bronchiolar epithelial Clara cells [5]. The
main function of SP-A in the alveolus is to facilitate the surface tension-lowering properties of surfactant phospholipids, to regulate surfactant phospholipid synthesis, secretion, and recycling by alveolar type II pneumocytes and alveolar macrophages, to resist to the inhibitory effects of plasma proteins released during lung injury [6]. Most of these properties of SP-A seem to be dependent on the presence of calcium which is thought to play a strong role in the structure and function of pulmonary surfactant after secretion into the alveolar space [7]. Surfactant impairment or changes of the proteinaceous fluid into the airspaces can have severe pathological consequences and, in particular, SP-A
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
2
has been found altered in a variety of pulmonary diseases [8]. Pulmonary surfactant abnormalities [9-10] have been demonstrated in patients with acute lung injury (ALI) and its most severe form of acute respiratory distress syndrome (ARDS). Clinical ALI and the ARDS represent a common response of the lung to a variety of insults, including sepsis, trauma, aspiration of water or gastric contents, inhalation of toxic gases, and pneumonia [11-12]. Changes that occur in SP-A concentration in bronchoalveolar lavage fluid (BAL) as well as in serum have been investigated in ARDS/ALI and found useful since correlated significantly with the level of alveolar septal damage [13-14]. However, SP-A is also a typical multi-faceted marker, which can be analyzed not only by molecular biological procedures or by biochemical assay in serum and in BAL but also by immunohistochemistry [15]. Already Morita [16-17] reported that surfactant production and secretion were enhanced in asphyxia deaths suggesting the use of pulmonary surfactant as possible indicator of death from hypoxia including drowning. In forensic context, several studies have also demonstrated that alveolar injury or asphyxiation can cause an increase in the blood level of SP-A and alterations in the immunostaining patterns accompanied by down-regulation of the mRNA [18]. Authors from Japan [19] studied SP-A immunohistochemically as a possible marker of pulmonary function and suggested the possible usefulness for postmortem investigation of death involving asphyxiation and respiratory distress. In particular, the pattern of SP-A staining has been proposed as possible indicator of severity and duration of respiratory distress (agony). Under normal conditions, SP-A is secreted into the alveolus and it is immunohistochemically detected sparse or weak in the alveolar type II cells or macrophages, but also on the alveolar interior surface or on the interface of intra-alveolar effusion resulting in a common membranous or linear pattern of SP-A staining. Increase of the membranous or linear SP-A staining on the intra-alveolar surface or at the interface has been indicated as an increase of surfactant secretion due to various fatal stresses among which acute myocardial infarction and carbon monoxide (CO) intoxication [20-22]. However, SP-A has been also observed in a different immunohistochemical distribution pattern such as aggregated granular staining distributed both intracellular and extracellular in the intra-alveolar
space but the exact mechanism of massive aggregates production remains to be determined [23]. This aggregated form of SP-A has been previously reported as a useful tool to distinguish mechanical asphyxia from other hypoxic cases and the effect of drugs and poisons on respiratory function [24]. Massive aggregates of granular SP-A staining were found in 70.4% of mechanical asphyxia victims (including hanging, strangulation, smothering and choking) compared with a control group of fatal intoxication by sedative-hypnotic drugs and ethanol. An high score of intra-alveolar aggregates of SP-A was more frequently observed also in freshwater (66.6%) than saltwater (6.25%) drowning victims [22]. Such findings have suggested a molecular alteration caused by a direct effect of aspirated water or metabolic disorder in the alveolar type II cells more frequently and intensely produced by freshwater than saltwater according with partial differences in pulmonary pathophysiology depending on the immersion medium. Therefore, granular SP-A staining was assumed to be the result of an enhanced secretion caused by strong forced breathing or over-excitement of the autonomic nervous system that often take place in the mechanical asphyxia such as drowning. According with this hypothesis, intense and dense granular SP-A staining was also observed in the hyaline membrane syndrome, perinatal aspiration of amniotic fluid, CO-intoxication with COHb level <60% and protracted drowning victims [18, 20-22] considered to be accompanied by a substantial duration of severe respiratory distress (agony). The membranous or linear pattern was then referred to inhibition of the central nervous system that often take place in fatal poisoning with sedative-hypnotic drugs (CNS depressants) and alcohol, in CO-intoxication with COHb >60% or even in the rapid death with very short survival time such as in acute cardiac deaths, cerebral lacerations and brain stem contusion [19, 22]. But, even if an intense and dense granular immunostaining was never observed in acute cardiac deaths, a relatively low score of intra-alveolar aggregates of SP-A has been reported among fatalities from acute myocardial infarction in which survival time was <6-18h suggesting the partial contribution of secondary respiratory distress involving pulmonary micro-vascular injury and consistent with a direct alveolar damage due to terminal cardiogenic pulmonary edema [21-22].
In this regard, congestion and pulmonary edema are very common to drug overdoses and other acute poisoning victims as well as to several asphyxia deaths and drowning victims but not pathognomonic for either because they can also be seen in natural deaths and in any death associated with agonal heart failure [25-26]. Such histological findings usually reflect agonal changes and the pre-final lack of oxygen due to the inhalation of large volume of water passing through the alveolar-capillary interface. Pulmonary edema is also very common in drowning victims or can be related to cardiac and/or respiratory failure (cardiogenic and non-cardiogenic pulmonary edema) due to the accumulation of fluid with a low-protein content in the lung interstitium and alveoli. Therefore to evaluate the effect on the SP-A distribution pattern by plasma proteins exuded into the alveolar space in pulmonary edema as well as by the accumulation of external fluid in the lung alveolus (see drowning), we have retrospectively investigated a total of 48 forensic autopsy cases based on the presence/absence of pulmonary edema, its pathogenesis, post-mortem interval (PMI) and survival time.
Material and Methods Totally 48 forensic autopsy cases were divided into three main groups: 18 cases of drowning (12 in salt -water and 6 cases in fresh -water), 20 cases of narcotic deaths (6 by cocaine and 14 by opiates) showing gross pulmonary edema consistent with a final impairment of respiratory function due to central nervous system depression rather than a pulmonary disorder itself, and 10 cases of acute cardiac deaths (ACDs) in which death occurred rapidly, in a few minutes from the beginning of the symptoms, and without signs of pulmonary edema. Selection of cases was mainly based on histological findings such as congestion, intra-alveolar and interstitial edema, and hemorrhages preliminary observed in the hematoxylin-eosin (H&E) stained sections. Congestion as well as local atelectasis and local emphysema areas were observed in quite all cases but not in ACDs. Pulmonary edema was visible in all samples taken from drowning and narcotic deaths (NDs). Intra-alveolar hemorrhagic edema was found in approximately 55% of drowning victims consistent with dilatation and rupture of alveoli due to violent asphyxial process. No intralobular hemorrhages or alveolar septal damage were observed in non-mechanical
asphyxia deaths. ACDs were selected based on the absence of cardiogenic pulmonary edema (CPE) and the very short survival time <1h according to witnesses. According to witnesses and emergency reports it was possible to determine the survival time <1h only for few overdoses and drowning cases. In no one case cardiopulmonary resuscitation (CPR) with artificial ventilation was adopted. Non-drowning cases were recruited also based on a relatively short PMI no longer than 72h in ACDs and no longer than 96h in NDs. Regarding the drowning samples, it was decided to insert also four cases with a relatively long PMI ranging between 6 and 8 days to focus on distribution pattern of SP-A even in decomposed tissues. The lungs were fixed with buffered neutral formalin and embedded in paraffin. Serial sections of about 4-5 micron thick were used for H&E and immunostaining. The sections were dried on glass slides coated with a suitable tissue adhesive, deparaffinated with xylene and alcohol series and rehydrated in distilled water. The sections were then incubated in 0,3% H2O2 in methanol for inhibition of endogenous peroxidase for 30 minutes, and again incubated in diluted normal serum for 10 minutes to prevent the background staining. Next incubation with the anti-human SP-A mouse monoclonal antibody (Surfactant Protein A- NCL – SP-A; Novocastra Laboratories LTd. NewCastle. U.K.) at 150-fold dilution for 60 minutes at room temperature and then in an appropriate biotinylated secondary antibody for 30 minutes (Vector Laboratories, Inc., Burhingame, Calif). The sections were incubated with universal Avidine-Biotine-Complex (ABC) for 30 minutes (Vector Laboratories, Inc., Burhingame, Calif). Peroxidase activity was revealed by incubating the sections in AEC (3-amino-9-ethylcarbazole). Finally, the sections were counterstained with hematoxylin for 1 minute. All the incubations were followed by three rinses in TBS buffer. To evaluate the postmortem changes of the tissues, the sections which were adjacent to those stained by immunoperoxidase staining were stained by H&E in all cases. SP-A staining in the inter-alveolar spaces and alveolar type II epithelial cells was used as internal staining control. SP-A was commonly stained in type II cells and macrophages but also on the alveolar interior surface irrespective of the causes of death. The expression of SP-A immunostaining was scored semi-quantitatively on two main staining
Romanian Journal of Legal Medicine Vol. XX, No 1(2012)
3
4
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
patterns and classified into three grades according with Zhu et al. [24] as follows:
- Membranous or linear staining: sparsely and weakly positive (score 1, +/-), diffusely and clearly positive (score 2, +), strongly positive (score 3, + +);
- Granular staining: almost negative or with few aggregates in alveolar space (score 1, +/-), some aggregates in almost all alveoli (score 2, +), many aggregates in almost all alveoli (score 3, ++). The immunostaining assessment was made by two examiners, separately and at different times. Even if scoring systems introduce a considerable subjectivity into the SP-A immunostaining analysis, the preliminary results have showed a correct classification in almost 75% of the samples since the beginning. Inter-examiner variability was no longer than one score both for linear and granular staining only in 12 cases, all belonging to drowning and NDs. For those assessments not in agreement, a re-evaluation was then performed till final correspondence.
Results The results of immunohistochemical scoring for ACDs without signs of pulmonary edema are reported in Table 1. The immunohistochemical distribution of intra-alveolar SP-A for drowning has shown in Table 2. Immunostaining intensity of SP-A for NDs with gross pulmonary edema is illustrated in Table 3. The samples taken from the four drowning cases with PMI between 6 to 8days revealed that SP-A distribution patterns can be easily detected also in lungs with advanced autolysis confirming that SP-A immunohistochemical properties seem to be relatively stable against decomposition [20]. The overall results are in agreement with those illustrated in other previous studies especially for drowning and ACDs [19, 22]. They provide further confirmation of the validity of SP-A immunohistochemical staining in the diagnosis of lung injury and respiratory distress. Distribution of SP-A immunostaining patterns among the samples is summarized in Table 4. In the group of ACDs without signs of pulmonary edema granular deposits of SP-A in the intra-alveolar space were almost negative and the membranous or linear staining pattern was sparsely positive according with the rapid death occurred in a few minutes from the beginning of the symptoms. In no one case massive aggregates of granular SP-A as well as strongly positive linear staining pattern were clearly found and, therefore, score 3 was never
assigned for either immunostaining patterns. The results of SP-A staining for this group show a low score resembling that one observed by other Authors in peracute deaths due to cranio-cerebral injuries [19] or myocardial infarction [21-22, 24]. Histological absence of pulmonary edema and rapidity of death excluded in ACDs a relevant alveolar damage due to secondary respiratory distress. No visible molecular alterations of SP-A and no enhanced secretion of SP-A usually related to a possible agonal CPE involving pulmonary micro-vascular injury were found except for some aggregated granular SP-A staining in the intra-alveolar space present in very few cases of ACDs (3 out of 10). SP-A aggregates in the intra-alveolar space were more frequently observed in drowning sample. A high intensity of this pattern was more often found in such victims (7 cases out of 18, approximately 38.8% of the total) in particular, in atelectatic areas related to the alveolar injury and molecular disorder caused by aspirated water. These results are consistent with the previous hypothesis of an SP-A impairment
_____________________________________________# Case Sex Age PMI SP-A_______ linear granular_____________________________________________ 1 M 25y 24h + / - + / - 2 M 30y 48h + / - + / - 3 M 32y 36h + + 4 M 49y 24h + / - + / - 5 M 28y 24h + + / - 6 M 38y 48h + / - + 7 M 27y 48h + / - + / - 8 M 44y 72h + / - + 9 M 32y 36h + + / - 10 M 37y 36h + + / -_____________________________________________
Table 1. Immunostaining intensity of intraalveolar SP-A for acute cardiac deaths without signs of pulmonary edema
LEGEND:M: male F: female y: years h: hours PMI: post-mortem interval
Score for membranous or linear pattern:+ / - score 1: sparsely and weakly positive; + score 2: diffusely and clearly positive;+ + score 3: strongly positive.
Score for granular pattern:+ / - score 1: almost negative or with few aggregates in
alveolar space; + score 2: some aggregates in almost all alveoli;+ + score 3: many aggregates in almost all alveoli.
5
Romanian Journal of Legal Medicine Vol. XX, No 1(2012)
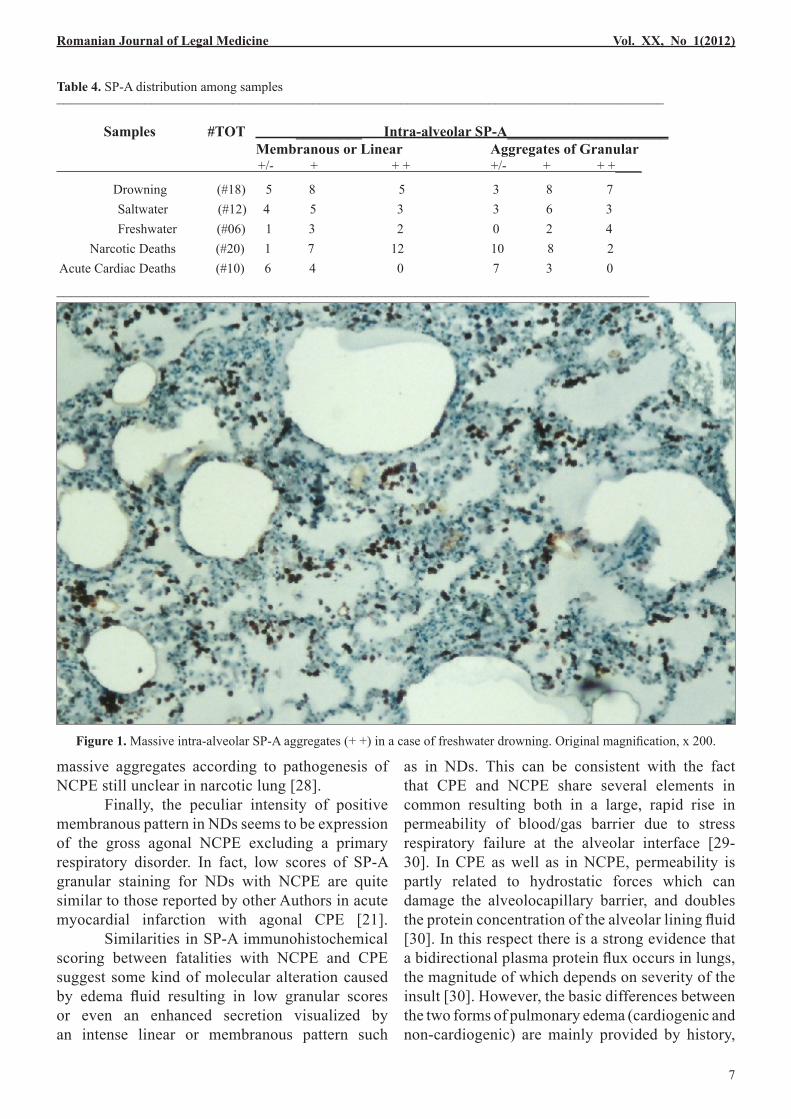
due to molecular alteration or enhanced secretion caused by the inhalation of water or by strong forced breathing and/or excitement of sympathetic and parasympathetic nervous system [19, 22]. 4 cases out of 6 totally were from fresh-water victims but unfortunately no reliable differences have been noted between salt-water and freshwater medium probably due to the poor number of cases available or the protracted hypoxia depending on the survival time. In fact, 3 cases of salt-water drowning out of 12 also showed dense aggregates in almost all alveoli. Worth of mentioning score 1 for granular staining was never assigned in freshwater victims resulting in a high proportion of diffuse SP-A aggregates (Figure 1) in a hypotonic medium compared with salt-water. Differences in SP-A distribution after drowning
in liquids of different osmolarity can be partially explained by hemodynamically disordered regulation and agonal chemical changes during the asphyxial process [25]. Both drowning mechanisms by salt and freshwater injure the alveolar/capillary unit, resulting in a lower functional residual capacity and pulmonary edema mainly depending on the amount and type of fluid aspirated [26]. The result of the accumulation of external and internal fluid into the lung alveolus is a profound surfactant dysfunction at the air-liquid interface of alveoli visualized immunohistochemically in intra-alveolar SP-A aggregates, more represented in proportion in freshwater (hypotonic relative to plasma) rather than saltwater (hyperosmolar relative to blood). In fact, freshwater can cause a severe loss and disruption of alveolar surfactant resulting in alveolar instability and collapse, atelectasis, and hemodilution with substantial changes of serum and intraalveolar electrolytes more represented in hypotonic medium compared with saltwater which draws proteinaceous fluid into the alveoli [25-27]. The results of SP-A expression in NDs with gross intra-alveolar and interstitial edema are consistent with a respiratory failure due to inhibitory effect on the central nervous system, rather than a pulmonary disorder itself. They are in agreement with previous reports for fatal intoxication by sedative-hypnotic drugs showing low granular scores [19-
# Case Sex Age PMI Water SP-A________ linear granular
____________________________________________________________________________________________ 1 F 41y 48h salt + + + 2 M 56y 7d salt + + / - ° 3 M 21y 36h salt + / - + + 4* M 42y 24h salt + + ° 5 F 28y 5d salt + + + + 6 M 38y 48h salt + / - + 7* M 19y 48h salt + + / - 8 M 56y 8d salt + + + ° 9 M 32y 96h salt + + / - 10* F 37y 36h salt + / - + 11 F 35y 36h salt + + + 12* F 34y 24h salt + / - + ° 13 F 51y 36h fresh + + + 14 M 34y 72h fresh + + + ° 15* F 15y 24h fresh + + 16 M 53y 6d fresh + / - + + 17 F 75y 48h fresh + + + + ° 18* M 40y 24h fresh + + + ____________________________________________________________________________________________
Table 2. Immunohistochemical distribution of intra-alveolar SP-A for drowning cases
LEGEND:M: male F: female y: years h: hours d: daysPMI: post-mortem interval* survival time <1h according to witnesses° cases with interobserver variability in which a re-evaluation was necessary.
Score for membranous or linear pattern:+ / - score 1: sparsely and weakly positive; + score 2: diffusely and clearly positive;+ + score 3: strongly positive.
Score for granular pattern:+ / - score 1: almost negative or with few aggregates in alveolar space; + score 2: some aggregates in almost all alveoli;
+ + score 3: many aggregates in almost all alveoli.
20, 24]. Cocaine and opiate related-deaths showed a prevalent and intense distribution of membranous or linear staining pattern (Figure 2). Only scattered SP-A aggregates in the intra-alveolar space were found. No clear relationship between SP-A patterns and drugs (cocaine and heroin) have been quantitatively demonstrated due to the poor number of cases available (6 cases related to cocaine out of 12 heroin overdoses). The
strongly positive linear pattern visualized on the alveolar interior surface or on the interface of intra-alveolar effusion suggests an enhanced secretion of SP-A stimulated by the inhibition of the central nervous system or by the gross non-cardiogenic pulmonary edema (NCPE). Only in two cases of overdoses out of 20 massive aggregates were observed probably related to survival time and/or protracted hypoxia. In fact, in the two cases of NDs with prominent and dense aggregates as well as in most of drowning cases with massive SP-A aggregates, numerous intra-alveolar macrophages containing granular SP-A deposits have been found confirming the hypothesis of a strong forced breathing (often observed in drowning) or better of a protracted hypoxia depending on the longer survival time [19-20, 22]. However, in no one of the drowning cases and NDs with diffuse aggregates the survival time was testimonied as very short. Therefore, in cases with diffuse SP-A aggregates a protracted oxygen lack during agony commnonly related to NDs could explain the presence of
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
# Case Sex Age PMI Drugs SP-A________ linear granular
_______________________________________________________________________________________ 1 M 36y 24h opiate + + + 2* M 57y 24h opiate + + + / - ° 3 M 30y 24h cocaine + + / - 4 M 29y 72h opiate + + + 5* M 33y 24h cocaine + + + / - 6 F 36y 24h opiate + + + 7 M 23y 48h opiate + + + ° 8 M 51y 96h cocaine + + + / - 9 M 32y 72h opiate + +
10 M 28y 96h opiate + + + 11* M 35y 24h cocaine + + + / - ° 12 M 34y 24h opiate + / - + / - ° 13 M 30y 72h opiate + + + / - 14 M 29y 24h opiate + + 15 M 23y 72h opiate + + + ° 16 M 30y 24h opiate + + / - 17 M 26y 24h opiate + + + / - 18 M 40y 24h opiate + + + 19* M 23y 24h cocaine + + / - 20 M 32y 24h cocaine + + + °_________________________________________________________________________________________
Table 3. SP-A immunhistochemical scoring for narcotic deaths with gross pulmonary edema
LEGEND:M: male F: female y: years h: hours d: daysPMI: post-mortem interval* survival time <1h according to witnesses° cases with interobserver variability in which a re-evaluation was necessary.Score for membranous or linear pattern:
Score for granular pattern:+ / - score 1: almost negative or with few aggregates in alveolar space; + score 2: some aggregates in almost all alveoli;
+ + score 3: many aggregates in almost all alveoli.
massive aggregates according to pathogenesis of NCPE still unclear in narcotic lung [28]. Finally, the peculiar intensity of positive membranous pattern in NDs seems to be expression of the gross agonal NCPE excluding a primary respiratory disorder. In fact, low scores of SP-A granular staining for NDs with NCPE are quite similar to those reported by other Authors in acute myocardial infarction with agonal CPE [21]. Similarities in SP-A immunohistochemical scoring between fatalities with NCPE and CPE suggest some kind of molecular alteration caused by edema fluid resulting in low granular scores or even an enhanced secretion visualized by an intense linear or membranous pattern such
as in NDs. This can be consistent with the fact that CPE and NCPE share several elements in common resulting both in a large, rapid rise in permeability of blood/gas barrier due to stress respiratory failure at the alveolar interface [29-30]. In CPE as well as in NCPE, permeability is partly related to hydrostatic forces which can damage the alveolocapillary barrier, and doubles the protein concentration of the alveolar lining fluid [30]. In this respect there is a strong evidence that a bidirectional plasma protein flux occurs in lungs, the magnitude of which depends on severity of the insult [30]. However, the basic differences between the two forms of pulmonary edema (cardiogenic and non-cardiogenic) are mainly provided by history,
Romanian Journal of Legal Medicine Vol. XX, No 1(2012)
Figure 1. Massive intra-alveolar SP-A aggregates (+ +) in a case of freshwater drowning. Original magnification, x 200.
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
8
Figure 2. Immunohistochemistry of pulmonary surfactant-associated protein (SP-A): A) Moderate membranous or linear staining pattern (+) on the surface of alveolar epithelia in a case of narcotic death, accompanied by some intra-alveolar SP-A aggregates (+). Original magnification, x 200. B) Magnification of intense membranous or linear staining pattern (+ +) on the intra-alveolar interior surface and on the interface of intra-alveolar effusion in a case of narcotic death. Original magnification, x 400.
Romanian Journal of Legal Medicine Vol. XX, No 1(2012)
9
clinical/radiological examination and laboratory tests but they are very difficult to diagnose due to overlapping of pathogenic mechanisms [31]. Discussion Based on such results and those reported by other Authors, granular SP-A staining alone is not a diagnostic criteria because it is not simply related to drowning or asphyxiaton. Similar immunostaining pattern has been also reported in non asphyxial deaths such as fire victims, electrocution, CO-intoxication, NDs and fatal poisoning by muscle relaxant, pesticides and petroleum gas [19-21, 24, 32]. Massive and dense intra-alveolar SP-A aggregates can only support the final diagnosis of drowning as well as duration and severity of respiratory distress. Intense membranous or linear SP-A pattern as well as low granular scores can only support the detection of pulmonary edema fluid on the intra-alveolar surface or at the alveolar interface due to primary or secondary respiratory insult and even agonal changes. Low scores for SP-A granular staining in salt-water victims are consistent with this hypothesis assuming that the spectrum of pulmonary edema in drowning can consist not only of water aspiration but also of NCPE [30-31]. NCPE is also represented in NDs due to massive diffusion or transudation of plasma proteins into the alveolar spaces [33-35] according with intense membranous or linear SP-A pattern. Once plasma proteins leak into alveolar spaces as a result of pulmonary edema, they have been shown to inhibit surfactant activity both in vitro and in vivo [6]. Therefore, alterations in type II cell function, inactivation of surfactant or surfactant composition changes may be easily due to dilution by any edema fluid liquid in the alveolar spaces and have been often described as secondary effects due to intra-alveolar edema formation. In this respect, SP-A has been found to aggregate into a multimolecular form in the presence of calcium which levels in the alveolar space can be easily altered by edema fluid [36]. Differences in SP-A immunostaining expression can be explained by the profound increase in alveolo-capillary permeability which is the hallmark of ALI and ARDS, and the result of pulmonary insults either directly via the airway or indirectly via the blood [14]. However, even if ALI and ARDS are commonly associated with
differences in surfactant composition changes, the role of the surfactant system as primary event in the pathogenesis of ALI/ARDS is poorly defined [14]. Intuitively surfactant dysfunction should be the last of a sequence of pathophysiological events following the primary insult with related perturbations of the air-liquid interface, alveolar septal membrane, type II cell numbers, surfactant homeostasis, and surface tension. But surfactant alterations in lung injury are not only a secondary consequence due to inactivation by intra-alveolar edema fluid with plasma protein leakage but rather sometimes a primary effect that contributes to an increased permeability of the blood-air barrier and further edema formation resulting in a vicious cycle with progressing surfactant impairment [37-38]. In this respect, SPs may be important clinical markers of injury or for prognosis and the diagnostic usefulness of SP-A as good monitor of alveolocapillary membrane injury has to be emphasized [37, 39]. Unfortunately, up-to-date no clear relationship between serum SP-A levels and SP-A immunostaining patterns has been quantitatively documented [15, 21] probably due to still unknown factors affecting SP-A expression. Further detailed analyses are required 23 to explain the differences in SP-A immunohistochemical expression and, in particular, the exact mechanism of massive aggregates which may be a result of enhanced secretion due to ALI rather than fatal intoxication. Based on the results of this study, they might be also affected by type and amount of edema fluid and its pathogenesis. In fact, in our opinion, morphological differences in SP-A immunostaining expression among the fatal events analyzed need to be related to histological findings first (atelectasis, emphysema, intra-alveolar hemorrhages) focusing on fluid accumulation in the interstitium and alveoli due to CPE or NCPE. Intra-alveolar fluid seems to affect SP-A immunostaining according with different pathogenesis of pulmonary disorder: see strongly positive membranous or linear pattern in NDs with NCPE consistent with inhibition of the central nervous system and respiratory function, high intensity of SP-A aggregates in drowning victims due to strong force breathing and primary alveolar injury. Low scores of two main SP-A staining patterns in cases without signs of pulmonary edema (ACDs) are consistent with such hypothesis supporting the important role of pulmonary edema
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
10
in the SP-A immunostaining expression. Therefore, SP-A immunostaining distribution can confirm in some fatalities the primary (intense granular pattern) or secondary respiratory damage (membranous or linear pattern and/or low granular scores) assuming that the production and secretion of SP-A can be stimulated by drowning and/or mechanical asphyxia and possibly enhanced by longer survival time in natural deaths associated with agonal CPE as well as in fatal intoxication or NDs with massive NCPE. The comparative SP-A expression among fatalities with gross NCPE due to overdoses and fatalities without signs of CPE (as in rapid ACDs) supports the strong effect of the intra-alveolar edema fluid in producing molecular alterations of SP-A visualized by immuno-histochemistry in granular or linear patterns. Unfortunately pulmonary edema is a too generalized descriptive term for the accumulation of fluid within the interstitial and/or the alveolar spaces of the lung due to cardiogenic causes (failure of the left side of the heart) but also non-cardiogenic causes where it is usually a complication of heroin overdose or other drug intoxication (antidepressants). Pulmonary edema can be also related to a variety of diseases [31] such as pulmonary embolism, eclampsia or central nervous system disorders (neurogenic pulmonary edema as occurred in head trauma, grand mal seizures, increase intracranial pressure), and even to water aspiration as in drowning. Therefore, the presence of congestion or pulmonary edema in any ALI needs to be related first to its pathogenesis since it can affect SP-A immunohistochemical distribution, sometimes resulting in SP-A staining pattern common to other fatal events [18-19]. SP-A immunohistochemistry alone cannot differentiate among fatalities [23] since it can be also affected by internal or external fluid accumulation in the lung alveoli according with severity of primary or secondary respiratory distress.
Conclusion SP-A is a complex regulated molecule with surprising properties and essential importance for pulmonary development, structure and function [40]. It is certainly a reliable marker of lung injury detectable in BAL, serum as well as in tissues. In this respect, SP-A immunohistochemistry can be a very useful indicator of respiratory distress and
alveolar injury but SP-A immunohistochemical expression alone cannot have diagnostic value in differentiating asphyxia and drowning as well as NDs and fatal poisoning. According with other Authors [23, 41] it should be preferably associated with the presence and intensity of histological signs such as, atelectasis and/or emphysema, congestion, hemorrhage, and edema in particular. Congestion and pulmonary edema are very common pathological findings in natural and violent deaths as well as in any death associated with agonal heart failure affecting SP-A immunohistochemistry based on type and amount of intra-alveolar fluid and its pathogenesis (cardiogenic and non-cardiogenic). Our results suggest that edema fluid can produce some molecular alterations or enhanced secretion of SP-A affecting its immunostaining pattern to be related with the cause of death or protracted hypoxia. They are not so clearly quantitatively interpretable as they do not meet the requirements for general diagnostic use. However, based on the comparison of SP-A distribution patterns among fatalities analyzed and also previously reported, the expression of SP-A immunohistochemical staining can be certainly considered a good monitor of lung function and alveolo-capillary membrane injury resulting in pulmonary edema. Massive and dense SP-A aggregates may be only a possible indicator of severity and duration of acute respiratory distress (agony) due to a direct alveolar damage like in drowning and other asphyxial deaths, especially in those cases where specific pathomorphological evidence and circumstancial data are usually very poor. Intense membranous or linear pattern can be referred to the enhanced secretion of SP-A stimulated by inhibition of the central nervous system as in NDs with massive NCPE but also in natural deaths with agonal CPE. Therefore, low granular scores might be expression of the presence of pulmonary edema caused by a primary respiratory insult (as observed in high proportion in salt-water victims) or a secondary pulmonary disorder resulting in alveolar fluid accumulation commonly related to prolonged death with hypoxia or heart failure (see fatal intoxications or agonal changes). Prolonged alveolo-capillary barrier damage is clinically and forensically relevant as increased pulmonary microvascular hydrostatic pressure in the presence of increased lung permeability is a mechanism
by which a large volume of cardiogenic or non-cardiogenic edema fluid collects in the lungs [29] affecting SP-A immunohistochemical expression. Little is still known of surfactant status in ALI as well as in edema fluid and changes in surfactant pool size have not been consistently demonstrated
[14, 30]. Despite half a century of investigation, some of the most fundamental aspects of pulmonary surfactant’s function remain poorly understood. Recent advances suggest that most existing models require re-evaluation [42] and other still unknown factors can be related with the SP-A immunostaining intensity.
References1. Georke J. Lung surfactant. Biochim Biophys Acta. 1974; 344: 241-246.2. Hawgood S, Clements JA. Pulmonary surfactant and its apoproteins. J Clin Invest. 1990; 86: 1-6.3. Fujiwara T, Maeta H, Chida S, Morita T, Wataba Y, Abe T. Artificial surfactant therapy in hyaline membrane disease. Lancet. 1980; 1:
55–59.4. King RJ, Clements JA. Surface active materials from dog lung. Am J Physiol. 1972; 223 (3): 707–733.5. Creuwels LA, van Golde LM, Haagsman H.P. The pulmonary surfactant system: biochemical and clinical aspects. Lung. 1997; 175: 1–39.6. Khubchandani KR, Snyder JM. Surfactant protein A (SP-A): the alveolus and beyond. FASEB J. 2001; 15 (1): 59-69. 7. Eckenhoff RG. Perinatal changes in lung surfactant calcium measured in situ. J Clin Invest. 1989; 84: 1295-1301.8. Kuroki Y, Takahashi H, Chiba H, Akino T. Surfactant proteins A and D: disease markers. Biochim Biophys Acta. 1998; 1408: 334-345. 9. Jobe AH, Ikegami M. Surfactant and acute lung injury. Proc Assoc Am Physicians. 1998; 110 (6): 489-495.10. Greene KE, Wright JR, Steinberg KP, Ruzinski JT, Caldwell E, Wong WB, Hull W, Whitsett JA, Akino T, Kuroki Y, Nagae H, Hudson
LD, Martin TR. Serial changes in surfactant-associated proteins in lung and serum before and after onset of ARDS. Am J Respir Crit Care Med. 1999; 160 (6): 1843-50.
11. Pison U, Obertacke U, Seeger W, Buchhorn R, Joka T, Brand M, Obertacke U, Neuhof H, Schmit-Neuerburg K-P. Surfactant protein A (SP-A) is decreased in acute parenchymal lung injury associated with polytrauma. Eur J Clin Invest. 1992; 22(11): 712-8.
12. Günther A, Siebert C, Schmidt R, Ziegler S, Grimminger F, Yabut M, Temmesfeld B, Walmrath D, Morr H, Seeger W. Surfactant alterations in severe pneumonia, acute respiratory distress syndrome, and cardiogenic lung edema. Am J Respir Crit Care Med. 1996; 153 (1):176-84.
13. Shimura S, Masuda T, Takishima T, Shirato K. Surfactant apoprotein-A concentration in airway secretions for the detection of pulmonary edema. Eur Respir J. 1996; 9 (12): 2525-2530.
14. Doyle IR, Nicholas TE, Bersten AD. Partitioning lung and plasma proteins: circulating surfactant proteins as biomarkers of alveolocapillary permeability. Clin Experim Pharmacol Physiol. 1999; 26:185–197.
15. Maeda H, Zhu BL, Ishikawa T, Michiue T. Forensic molecular pathology of violent deaths. Forensic Sci Int. 2010; 203: 83-92.16. Morita M, Tabata N, Maya A. Studies on asphyxia: on the changes of the alveolar walls of rats in the hypoxic state. Forensic Sci Int. 1985;
27: 81-92.17. Morita M, Tabata N. Studies on asphyxia: on the changes of the alveolar walls of rats in the hypoxic state. II. The hypoxic state produced
by carbon dioxide and methane gases. Forensic Sci Int. 1988; 39: 257-262.18. Maeda H, Fujita MQ, Zhu BL, Ishida K, Quan L, Oritani S, Taniguchi M. Pulmonary surfactant-associated protein A as a marker of
respiratory distress in forensic pathology: assessment of the immonohistochemical and biochemical findings. Legal Med. 2003; 5: S318-S321.
19. Zhu BL, Ishida K, Fujita MQ, Maeda H. Immunohistochemical investigation of a pulmonary surfactant in fatal mechanical asphyxia. Int J Leg Med. 2000; 113:268-271.
20. Zhu BL, Ishida K, Quan L, Fujita MQ, Maeda H. Immunohistochemistry of pulmonary surfactant apoprotein A in forensic autopsy: reassessment in relation to the causes of death. Forensic Sci Int. 2000; 113: 193-197.
21. Zhu BL, Ishida K, Oritani S, Quan L, Taniguchi M, Li D-R, Fujita MQ, Maeda H. Immunohistochemical investigation of pulmonary surfactant-associated protein A in fire victims. Legal Med. 2001; 3: 23-28.
22. Zhu BL, Ishida K, Quan L, Li D-R, Taniguchi M, Fujita MQ, Maeda H, Tsuji T. Pulmonary immunohistochemistry and serum levels of a surfactant-associated protein A in fatal drowning. Legal Med. 2002; 4: 1-6.
23. Stemberga V, Stifter S, Cuculic D, Coklo M, Bosnar A. Immunohistochemical surfactant protein-A expression: fatal drowning vs post-mortem immersion. Medical Hypotheses. 2009; 72: 413-415.
24. Zhu BL, Ishida K, Oritani S, Quan L, Fujita MQ, Maeda H, Ogawa M, Tanaka N, Komura S, Tsuji T. Immunohistochemical investigation of pulmonary surfactant-associated protein A in fatal poisoning. Forensic Sci Int. 2001; 117: 205-212.
25. Saukko P, Knight B. Knight’s Forensic Pathology, 3rd ed., Hodder Arnold, London, UK, 2004.26. Dolinak D, Matshes EW, Lew EO. Forensic Pathology: principles and practice. Elsevier Academic Press, 2005.27. Di Maio VJ, Di Maio D. Forensic pathology. CRC Press, Boca Raton, FL, 2001.28. Dettmeyer R, Schmidt P, Musshoff F, Dreisvogt C, Madea B. Pulmonary edema in fatal heroin overdose: immunohistological investigations
with IgE, collagen IV and laminin – no increase of defects of alveolar-capillary membranes. Forensic Sci Int. 2000; 110: 87-96.29. De Pasquale CG, Arnolda LF, Doyle IR, Grant RG, Aylward PE, Bersten AD. Prolonged alveolo-capillary barried damage after acute
cardiogenic pulmonary edema. Crit Care Med. 2003; 31 (4): 1060-1067.30. Doyle IR, Bersten AD, Nicholas TE. Surfactant proteins-A and -B are elevated in plasma of patients with acute respiratory failure. Am J
Respir Crit Care Med. 1997; 156: 1217–29.31. Kakouros NS, Kakouros SN. Non-cardiogenic pulmonary edema. Hellenic J Cardiol. 2003; 44: 385-391. 32. Michiue T, Ishikawa T, Zhao D, Kamikodai Y, Zhu BL, Maeda H. Pathological and biochemical analysis of the pathophysiology of fatal
electrocution in five autopsy cases. Legal Med. 2009; 11: S549-S552.33. Rumbak MJ. The etiology of pulmonary edema in freshwater near-drowning. Am J Emerg Med. 1996; 14 (2): 176-179. 34. Cohen DS, Matthay MA, Cogan MG, Cogan MG, Murray JF. Pulmonary edema associated with salt water near-drowning: new insights.
Am Rev Respir Dis. 1992; 146 (3): 794-6. 35. Modell JH, Moya F. Effects of volume of aspirated fluid during chlorinated freshwater near-drowning. Anesthesiology 1966; 27: 662-672.36. Haagsman HP, van Golde LM. Synthesis and assembly of lung surfactant. Annu Rev Physiol. 1991; 53: 441-464.
Romanian Journal of Legal Medicine Vol. XX, No 1(2012)
11
Campobasso C.P. et al An immunohistochemical study of pulmonary surfactant apoprotein A (SP-A) in forensic autopsy materials
37. Hastings RH. Monitoring alveolar epithelial function in acute lung injury. J Clin Monit Comput. 2000; 16 (5-6): 385-392.38. Ochs M, Nenadic I, Fehrenbach A, Albes JM, Wahlers T, Richter J, Fehrenbach H. Ultrastructural alterations in intraalveolar surfactant
subtypes after experimental ischemia and reperfusion. Am J Respir Cell Mol Biol. 1999; 160: 718-724.39. Eisner MD, Parsons P, Matthay MA, Ware L, Greene K. Plasma surfactant protein levels and clinical outcomes in patients with acute lung
injury. Thorax 2003; 58: 983-988. 40. Goldmann T, Kahler D, Schultz H, Abdullah M, Lang DS, Stellmacher F, Vollmer E. On the significance of surfactant protein-A within
the human lungs. Diagnostic Pathol. 2009; 4-8.41. Perez-Carceles MD, Sibon A, Vizcaya MA, Osuna E, Gomez-Zapata M, Luna A, Martinez-Diaz F. Histological findings and
immunohistochemical surfactant protein A (SP-A) expression in asphyxia: its application in the diagnosis of drowning. Histol Histopathol. 2008; 23: 1061-1068.
42. Piknova B, Schram V, Hall SB. Pulmonary surfactant: phase behavior and function. Curr Opin Struct Biol. 2002; 12 (4): 487-94.