Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011 CAPHRI Day: Healthy Aging Maastricht University, May 19, 2011 Strategies of disability prevention in older people Andreas E. Stuck, MD [email protected]Geriatrics University of Bern, Switzerland Spital Netz Bern (Ziegler and Belp) and Inselspital, Bern
Transcript
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
CAPHRI Day: Healthy AgingMaastricht University, May 19, 2011
Strategies of disability prevention in older people
- social aspects (e.g., network, support, finances)
- emotional and cognitive health (depression, dementia)
- psychological aspects (adherence)
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Differences in actions per domain between programs
- Selection of domainse.g. physical activity (yes/ no)e.g. colon cancer screening (yes no)e.g. hypertension control (yes no)
- What is done per domain?- diagnostic, and criterion for risk- initial intervention- follow-up
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Epidemiology of Hypertension
JNC 7 Report
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Variability within one home visit program
Nurse (code) A and B C
No of problems (for which nurse intervened) 5.5 3.6
Effect on disability 0.5 (0.2-1.2) 1.0 (0.5-1.8) Older persons’ satisfaction with visit 52% 69%
Stuck A et al. Archives of Internal Medicine, 2000
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Meta-analysis of preventive home visits
Preventive home visits21 randomised controlled trials
Outcomes (OR) death 0.92, 0.80–1.05nursing home admission 0.86, 0.68–1.10functional status decline 0.89, 0.77–1.03
Significant heterogeneity
Huss A et al. JGMS 2008
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
.
.
0.48 (0.26, 0.88)
0.83 (0.54, 1.29)
1.10 (0.92, 1.32)1.02 (0.68, 1.55)
1.32 (0.92, 1.91)
0.42 (0.23, 0.76)
1.00 (0.88, 1.14)
0.96 (0.62, 1.51)0.56 (0.34, 0.94)
0.97 (0.66, 1.44)
0.87 (0.60, 1.26)
1.16 (0.86, 1.56)
1.24 (0.76, 2.03)1.24 (0.69, 2.23)
0.64 (0.48, 0.87)
0.68 (0.43, 1.06)
0.80 (0.53, 1.19)
0.69 (0.47, 1.02)
Stuck (1995)
Kono (2004)
Byles (2004)Carpenter (1990)
Vetter, Gwent (1984)
Tinetti (1994)
Subtotal
Hébert (2001)
Multidimensional assessment with clinical examinationFabacher (1994)
Bouman (2007)
Vetter (1992)
van Rossum (1993)
Multidimensional assessment without clinical examination
Pathy (1992)Melis (2008)
Subtotal
van Haastregt (2000)
Stuck (2000)
Vetter, Powys (1984)
0.48 (0.26, 0.88)
0.83 (0.54, 1.29)
1.10 (0.92, 1.32)1.02 (0.68, 1.55)
1.32 (0.92, 1.91)
0.42 (0.23, 0.76)
1.00 (0.88, 1.14)
0.96 (0.62, 1.51)0.56 (0.34, 0.94)
0.97 (0.66, 1.44)
0.87 (0.60, 1.26)
1.16 (0.86, 1.56)
1.24 (0.76, 2.03)1.24 (0.69, 2.23)
0.64 (0.48, 0.87)
0.68 (0.43, 1.06)
ES (95% CI)
0.80 (0.53, 1.19)
0.69 (0.47, 1.02)
Less functional status decline More functional status decline 1.25 .5 1 2 4
Risk of functional status decline
Huss A et al. JGMS 2008
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Conclusion: Meta-analysis preventive home visites
Heterogeneity among trials
Criteria for favourable effect - multidimensional approach including medical component - long-term intervention- persons initially not disabled
If criteria are met: Potential is one third reduction of nursing home admission
Conclusions based on subgroup analyses
Huss A et al. JGMS 2008
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Practice/ policy implication
Home visits have potential and limitations
Consider alternatives- “home visits” not at home- use of information technology- group sessions - start below age of 75
Consider Health Risk Appraisal with reinforcement modules- group sessions- practice system changes- brief home visits- long home visits (for highly selected subgroup only)- practice consultation (physician assistant)
Stuck A et al. BMC Research Methods, 2008
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Development of a HRA-O(Health Risk Appraisal for Older People)
Literature review of risk factors for functional decline
Criteria for selection of HRA domains Criteria for selection items measuring domains Identification of domains and survey items Prototype, focus group Pilot version, software development, testing Extensive field testing, updating
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Domains of HRA-O
Physical Activity Nutrition Injury Prevention Smoking Alcohol Use Self-Perception of Health Medical Conditions Preventive Care Medications Signs and Symptoms (of possible
adverse drug reactions)
Geriatric Syndromes- bladder control- memory
Depression Vision, hearing Oral health Pain Functional Status Psychosocial Health, Social Support/
Network Occupation, Retirement Demographic Information
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Software system
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Use of HRA-O in PRO-AGE study
Funded by European Union (Fifth Framework Program)
Randomised controlled study of effects of HRA-O based interventions on preventive care use and health behaviour:
London, UK (N=2503)Hamburg, Germany (N=2580)Solothurn, Switzerland (N=2284)
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
HRA-O intervention in PRO-AGE
Training of health professionals
Use of the HRA-O instrument
Personal reinforcement of HRA-O by GP
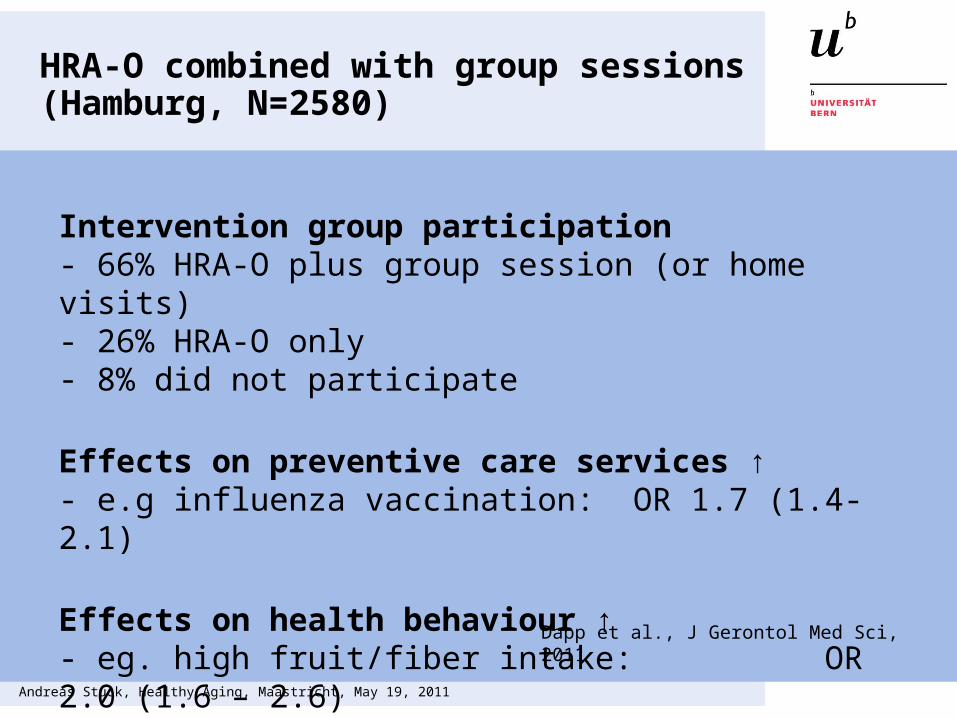
Additional site specific reinforcement- London: electronic reminders to GP- Hamburg: one group session with follow-up- Solothurn: home visits over two years
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Colon cancer screen 28% 21% 1.5 (1.1, 1.9)(persons aged < 80 years) Stuck et al., submission
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
PRO-AGE: HRA-O randomised controlled studies: What we learnedSelf-administered tool is feasible; acceptance among older persons and general practitioners
Effects of HRA-O combined with reinforcement (home visits/ group sessions): improvement of uptake of preventive care and favourable change in health behaviour
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Multiple Risk Factor Intervention
Multiple risk factor interventions address the multidimensional causes of functional status decline. Therefore, multiple risk factor interventions have the best chance to result in an optimal clinical effect.
However, multiple risk factor intervention trial have several disadvantages, including:- black box problem: if favorable finding: what worked?- replication: often difficult to replicate
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Advantages of Single Risk Factor Interventions
- It is possible to target single risk factors even if the underlying problem is multifactorial
- Clear design (comparable to drug trial)
- If favourable effects- mechanism of effect understandable
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Disadvantages of Single Risk Factor Interventions
Do not take into account multifactorial etiology of syndromes/ functional disability
Effect of intervention package may not be equal to the sum of the individual package components
Potential ethical problems if other problems are detected
Andreas Stuck, Healthy Aging, Maastricht, May 19, 2011
Clinical Conclusion, Three Groups withDifferent Approaches for Disability Prevention