16
Developing a Capable Dual Diagnosis Strategy A Good Practice Guide Authors: Liz Hughes, Ann Gorry and Tom Dodd
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | cristian-andres-valenzuela-stuardo |
| View: | 216 times |
| Download: | 2 times |

Developing aCapable Dual
Diagnosis StrategyA Good Practice Guide
Authors: Liz Hughes, Ann Gorry and Tom Dodd


Contents
Foreword 2
Introduction 3
Background 4
Getting Started 5
Commissioning 7
Developing Outcomes 8
Operational Policies 8
Process for Managing Disagreements 9
Monitoring Implementation 9
Checklist 9
Conclusion 10
Comments 0n dual diagnosis 10
Useful References and Resources 11
Developing a Capable Dual Diagnosis Strategy 1

2 Developing a Capable Dual Diagnosis Strategy
Foreword
Providing high quality, appropriate services for people with mental illhealth and substance misuse problems (Dual Diagnosis) their carersand families, remains one of the biggest challenges facing frontlinemental health and drug and alcohol services today.
People with mental ill health, substance use and other complex needs are among some of the mostsocially excluded people in our society. Because this group usually need treatment from a variety ofdifferent agencies, they often fall through gaps in services due to lack of clarity about roles andresponsibilities. Dual diagnosis is everyone’s business and all services have a role to play in thetreatment and care for this client group, their carers and families.
The guidance given in this document is designed to support the development of a “capable localdual diagnosis strategy” built on recommendations from national policy guidance and drawing onbest practice from around the country.
Developing a robust local strategy will help to set out the vision and values for local serviceprovision, and be the focal point for collaboration between all stakeholders, including service usersand carers. A successful strategy will be able to address the varying needs of this group by beingcomprehensive and flexible in its approach.
Dr. Sian Rees, Senior Policy Advisor, Mental Health

IntroductionPeople with a dual diagnosis of mentalhealth and substance use often havemultiple and complex long term needs,which require a comprehensive,coordinated, seamless, multi-agencyresponse. However, due to a variety offactors (such as resources, lack of clarityaround local service responses, and a lackof workforce skills), this group often fail toreceive good quality and consistent care. Arobust local Dual Diagnosis Strategy will setout the vision and values for local serviceprovision, and be the focal point forcollaboration between all key stakeholdersat a local level. A successful strategy will beable to account for the varying needs of allgroups and will be comprehensive andflexible in its approach.
This document is designed to support thedevelopment of a “capable local dual diagnosisstrategy” built on recommendations fromnational policy guidance and best practice fromaround the country.
Key points:
• People with mental health substance use andother complex needs (often referred to as“dual diagnosis”) are some of the most sociallyexcluded and vulnerable people in our society.
• Because this group often need treatmentfrom a variety of different agencies, theyoften fall through the net of care due to lackof clarity about roles and responsibilities
• Dual diagnosis is everyone’s business and allservices have a role to play in treatment
• Service user and carer collaboration andinvolvement is essential
• Robust long term monitoring and evaluation ofa strategy will ensure effective implementation.
BackgroundThe term “dual diagnosis” can beproblematic as it refers to the presenceof two clinical diagnoses, whereas inreality people who fall under this ‘term’ often have very complex needs.However, it has been accepted as aconvenient way to define an increasingly large group of service users that have mental health andsubstance use difficulties (where use of drugs/alcohol impacts on mentalhealth and vice versa).
In treatment settings, the prevalence of dualdiagnosis is high. Within the substance misusetreatment sector, the prevalence of dualdiagnosis is estimated to be 75%1 for those indrug services and 85% for those in alcoholservices.2 In mental health settings, prevalencestudies 3 have suggested that around a third ofpeople with serious mental health problems(such as psychosis and bipolar affectivedisorder) have some level of substance useproblems. However, in Assertive OutreachTeams and Early Intervention
1 Weaver et al: 2002 Co-morbidity of substance misuse and mental illness collaborative study: A study of the prevalence andmanagement of co-morbidity amongst adult substance misuse and mental health treatment populations
2 Saunders, B. & Robinson, S. (2002). Co-occurring mental health and drug dependency disorders: workforce development challenges forthe AOD field. Drug and Alcohol Review, 21, 231-237.
3 Menezes, P.R.; Johnson, S.; Thornicroft, G.; Marshall, J.; Prosser, D.; Bebbington, P. and Kuipers, E. (1996) Drug and alcohol problemsamong individuals with severe mental illness in south London The British Journal of Psychiatry 168: 612-619
Developing a Capable Dual Diagnosis Strategy 3

4 Developing a Capable Dual Diagnosis Strategy
Teams the prevalence is thought to besignificantly higher. The most commonly usedsubstances in this group tend to be alcohol andcannabis. This group is also at high risk ofsuicide and homicide.4
The Department of Health5 Dual DiagnosisGood Practice Guide conceptualises people witha dual diagnosis as comprising of four sub-groups (see figure below). This model alsoprovides some indication of the service likely tobe best placed to lead and/or co-ordinatemeeting the treatment needs of the individual.
4 University of Manchester (2006) The national confidential enquiry into suicide and homicide by those with mental illness.
5 Department of Health (2002) Mental Health Policy Implementation Guide Dual Diagnosis Good Practice Guide
Quadrant A
Substance misuse lead/ co-ordinate care delivery
Advice/support from mental health/dual diagnosis team(s)
Quadrant B
Mental health lead/co-ordinate care delivery
Advice/support from substance misuse/dual diagnosis team(s)
Quadrant C
Primary care lead/co-ordinate care/treatment
Advice/support from mental health and/or substance misuse and/or dual
diagnosis team(s)
Quadrant D
Mental health lead/co-ordinate care delivery
Advice/support from substance misuse/dual diagnosis team(s)
Example 1: a person with schizophrenia whois also regularly smoking cannabis may be besthelped within mainstream mental health servicesand the mental health staff should be able toassess and provide some harm reductioninterventions regarding the cannabis use (healtheducation, motivation, specific strategies if theclient wants to reduce their drug use, orsignpost to other help). Quadrant B
Example 2: a person with a history ofinjecting heroin, and on a methadonemaintenance programme who has symptoms of post-traumatic stress disorder (PTSD) will be best placed within community drugtreatment service, but would also benefit from some input from a clinical psychologistaround PTSD symptoms. Quadrant A
DH (2002)
Mild mental illness (MI) Severe mental illness (MI)
Mild
sub
stan
ce u
se (
SU)
S
ever
e su
bsta
nce
use
(SU
)

The Dual Diagnosis Good Practice Guide (DH2002) recommends that all local implementationteams (LITs) should have a shared definition of“dual diagnosis” and develop appropriate serviceresponses which should form part of a local dualdiagnosis strategy. This can often be a barrierencountered by those trying to develop a strategy.Discussions and reaching agreement on a definitioncan be a lengthy process. It may be easier andmore productive to agree a broad definitionconsistent with a whole systems approach.
In the Autumn Assessment Themed ReviewReport 6 almost 80% of Mental Health LocalImplementation Teams (LITs) reported having alocal definition of dual diagnosis. However,progress on development of strategies in manylocal areas is lagging behind. At the time of theThemed Review on Dual Diagnosis (2006-7)over 40% of LITs did not have a dual diagnosisstrategy agreed with local stakeholders.
What is a Strategy and why do we need one?
A dual diagnosis strategy will provide a clear,local vision, and include the general principalsand direction of service provision for a specifiedperiod of time, often between 5 and 10 years.One of the main reasons why it is vital to havea dual diagnosis strategy is due to the numberof services involved in the client’s journey. Thestrategy will help to clarify roles andresponsibilities along the way and help serviceusers and carers navigate more easily throughservices to get the right help at the right time.
The strategy development process will need totake account of the contextual background,organisational priorities, benefits, and risks. Thestrategy will need all partners to sign up to it,and should include an action plan to deliver adual diagnosis programme that will demonstratea positive impact on the health and quality oflife of service users and carers.
Key drivers:
• Improving local services
• Following national guidance and good practice
• Comply with NHSLA dual diagnosis standards(the scheme is optional but level 1 NHSLA isessential to gain Foundation Trust status)
Getting Started
Establishing leadershipStrong and clear leadership is critical inmotivating people to make changes and ingetting stakeholders to work effectivelytogether. If a strategy is to be successful acrossa number of diverse services and with a numberof stakeholders, it needs to be headed up by asenior leader that possesses knowledge andcapabilities to take the strategy forward. DH(2002) dual diagnosis guidance recommendsthat a lead commissioner and lead clinician withthe requisite knowledge, motivation andinfluence should take this forward.
Steering Group MembershipMembers of the steering group should includepersonnel who are in a position to lead andinfluence service improvement across a varietyof settings. This will include representation frommental health and substance use, but shouldalso include some representation from otheragencies such as:
• Carers groups
• Service user representatives
• Mental health Services
• Substance misuse/ Alcohol services (statutoryand third sector)
6 Department of Health (2008) Autumn Assessment Themed Review Report 2007
Developing a Capable Dual Diagnosis Strategy 5

6 Developing a Capable Dual Diagnosis Strategy
• Primary care
• Housing agencies
• Local authority
• Social care
• Criminal justice:
• Police
• Probation
• Prison in-reach mental health
• Integrated Drug Treatment Teams (IDTS)
• Drug Intervention Teams
• Accident and Emergency/Acute Sector
• Ambulance service.
Developing the Aims and ObjectivesThere are some key questions to consider in thedevelopment of a dual diagnosis strategy.
• What are its aims?
• How will these be delivered?
• How will they be evaluated?
• Is it outcome focused?
• Who is responsible for the implementation of the strategy?
A good strategy should identifyaspirations and vision for local services and should:
• Engage all key stakeholders especially thosewho use the services themselves
• Identify shared values for the strategy which reflect those identified by service users and carers.
• Reflect current evidence (research, policyguidance, and good practice examples)
• Develop the potential of the currentstaff/service resources
• Be visionary about future developments
• Provide a focus for local commissioners,providers, users and carers when assessinglocal need and inform wider plans fordevelopments and new ways of working
• Be a working document that is flexible tochanging need, and responsive todevelopments in policy and research
• Reflect the diversity of need within this group within the local area
• Define the roles and responsibilities of service providers for working with peoplewith a dual diagnosis;
• Identify protocols which will be required e.g.referral procedures, information sharing(including confidentiality).
Developing work streamsAs part of the strategy a number ofdevelopments will need to be considered:
A) Local Area Needs assessmentThis can be a fairly simple process drawing ondata that is already available and supplementingthis by seeking the views of service providers,service users and carers when required In termsof identifying needs, a series of key questionsshould be answered:
• How are current services addressing theneeds of people with dual diagnosis?
• What are the gaps/ difficulties/areas of good practice?
• What do service users and carers feel aboutthe quality of care and what do they want to be developed and improved?

The method chosen to gather such informationwill depend on resources. One option is to holda one day event which comprises of a set offocus groups to discuss the questions above.Another option would be to interview a seriesof key informants. An external consultant maybe commissioned to conduct a needsassessment and produce a report.
B) Workforce DevelopmentOnce a vision for service delivery has beenidentified the next step is to develop astrategy to ensure the workforce caneffectively deliver. This will include trainingand staff development, creation of new rolesand the development of a robust trainingstrategy.
The Dual Diagnosis Capability Framework(Hughes, 2006) was developed to define thecapabilities required at 3 levels (core, generaland specialist). The framework can be used toaudit the workforce, highlight gaps incapability, and devise targeted training. Amulti-agency training strategy should bedevised and this may comprise of:
• training needs analysis
• a dual diagnosis development pathway,delivering differing levels of training (frombasic awareness training (‘core’) to complextherapeutic interventions (‘specialist’)
• Identify which personnel/organisations canprovide training and how this will befunded
• Devise a plan for implementation- will itfocus on whole teams, multi-agency groupswithin a locality, specific groups with mostneed (e.g. inpatient mental health staff,forensic teams, assertive outreach teams)
• Long term plans for supervision and supportin clinical practice.
There will need to be systems for appraisal andsupervision, as well as opportunities for further
learning such as special interest forums,secondments to other services (e.g. a mentalhealth nurse seconded one day per week tolocal drug/alcohol agency) or mentoring andshadowing experiences.
c) Creation of new roles
Specialist “dual diagnosis workers” exist insome areas of the country, but there is a widevariation in their remit and fundingarrangements. The Dual Diagnosis GoodPractice Guidance (DH 2002) recommendsspecialist practitioners in areas of high need. Interms of implementation, specialist practitionerscan provide a number of key interventions toenhance and embed a dual diagnosis strategy inclinical settings. These include:
• Delivery of training
• Supervision
• Role-model in practice
• Making links between theory and practice(for example by attendance at teammeetings)
• Encourage implementation in practice.
CommissioningThe existing services may have to be re-commissioned to some degree to alignmore with the strategy. If there is to bespecialist workers, they will need to befunded and decisions about this willneed to be made. It may be that mentalhealth and substance use budgets arecombined to create new roles. Jointcommissioning between DAAT’s, PCT’s,local authorities and other organizationswill demand the development of sharedprotocols and robust care pathways.
Developing a Capable Dual Diagnosis Strategy 7

8 Developing a Capable Dual Diagnosis Strategy
Developing OutcomesIn order to evaluate the impact of a localstrategy, outcomes will need to beidentified, and regularly audited. Theseshould reflect issues pertinent to thevarious stakeholders. Examples ofoutcomes might include:
AssessmentOutcome: everyone coming into mental healthservices has an assessment of their substance use
Evidence: audit of assessment documentation
Outcome: service users feel that their substanceuse has been asked about in a sensitive andnon-judgmental manner
Evidence: service user satisfaction survey.
Outcome
The right services, in the right place, at the right time
Improved health and wellbeing for dualdiagnosis service users and their carers
Better communication between stakeholders
Clarity of roles and responsibilities
Clear standards and high quality care
Improved access to a range of services
Improved service user and carer experiencethrough greater choice and control
Single point of access to services whereverpeople enter the system.
Examples of evidence
care pathways, service mapping, service userand carer feedback
Comparison of routinely collected data at settime points
Audit of correspondence/ focus groups
CPA documentation; focus groups
Audit services against standards
How many people in services have dualdiagnosis- snapshot audits
Focus groups, feedback forms, CPAdocumentation
Can this be identified, is it working?
Operational PoliciesOn the basis of the needs assessmentthe strategic vision of the dual diagnosisstrategy needs to be embedded intopolicy across a number of areas and beat the core of a series of operationalpolicies which will need to be developed,
including working agreements/protocolsbetween all agencies as to:
• Newly defined remits of service
• referral criteria
• care pathways
• confidentiality and sharing of information
• joint working arrangements.
Process for ManagingDisagreementsWith such a wide range of stakeholdersbringing different perspectives andagendas, disagreements about aspectsof the strategy are likely to occur.
It is hoped that constructive discussions canresolve these. However, there may be issues thatcan’t easily be resolved. There needs to be amechanism by which differences of opinion andconflict can be resolved within the steering group.Ultimately the steering group lead should begiven the authority to make the final decisions.
MonitoringImplementationA strategy is a medium to long-termvision of service change and delivery.
Therefore the strategy group shouldmonitor progress against a set of agreed targets.
The steering group should meet regularly tomonitor progress and address areas of difficulty.One of the most important steps is to ensurethat all stakeholders are aware of and signed upto the strategy. This may include holding astrategy launch event, distribution of documentsto all services and groups, and running an auditon the impact of the new strategy. It is veryimportant that no one service can opt out of thestrategy and that dual diagnosis is everyone’sbusiness. It is not just a specialist field and allmainstream services have a key role to play.
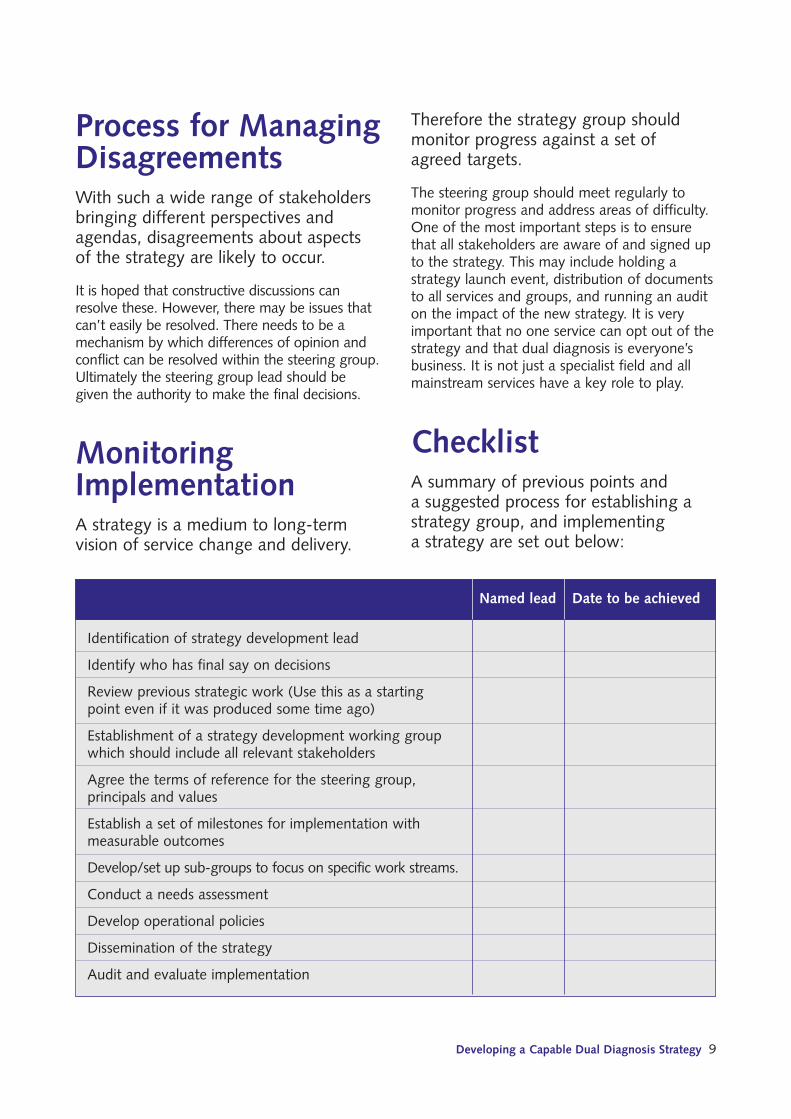
ChecklistA summary of previous points and a suggested process for establishing astrategy group, and implementing a strategy are set out below:
Identification of strategy development lead
Identify who has final say on decisions
Review previous strategic work (Use this as a starting point even if it was produced some time ago)
Establishment of a strategy development working group which should include all relevant stakeholders
Agree the terms of reference for the steering group, principals and values
Establish a set of milestones for implementation with measurable outcomes
Develop/set up sub-groups to focus on specific work streams.
Conduct a needs assessment
Develop operational policies
Dissemination of the strategy
Audit and evaluate implementation
Named lead Date to be achieved
Developing a Capable Dual Diagnosis Strategy 9

10 Developing a Capable Dual Diagnosis Strategy
ConclusionDevelopment of a local dual diagnosisstrategy is the lynchpin to coordinatingand providing comprehensive, highquality services for people with dualdiagnosis. It is no longer an area of“specialist” interest; it affects everyoneusing and working in mental health andsubstance use services, as well as thewider health, social care and criminaljustice system.
The mainstream mental health policy andguidance drivers support the development ofdual diagnosis strategy in all areas. Theimportant factors for successful strategydevelopment seem to be willingness for agenciesto work together, put aside professional andideological constraints, and develop new rolesand new ways of working for the benefit ofservice users and carers. All this cannot happenwithout dedicated, motivated experienced local“champions” such as dual diagnosis senor leads(including consultant nurses). Commissionersand senior managers should consider theimportance of the long term fundingcommitment of such posts, as without theleaders, the strategy is likely to fail.
Comments on dual diagnosis Experts/nurse consultants from aroundthe country on their experiences ofdeveloping a local dual diagnosis strategy:
“The implementation plan for the strategy wasdivided into two section; actions specific to
Oxleas NHS Foundation Trust and actionswhich were to be led and delivered by the local
borough steering groups, in order to preventthe need for the borough steering to repeat the
exercise in order to develop their local strategies.It was agreed however that local boroughs willhowever still need to develop a commissioningstrategy to monitor and review services availableto service users who are not seen within Oxleas
services. Progress of implementation plan isreviewed quarterly by Trust dual diagnosis
steering group, where local boroughmanagement reps self rate their progress using
a traffic light system. Also the dual diagnosisspecialist practitioners and the local borough
steering groups present a formal yearly updatefrom within their boroughs to the steering group.”
Justine Trippier
“The city councilors decided to conduct a scrutinyreview of dual diagnosis service provision. Thisraised the profile of the strategy and the needfor integrated care in Nottingham city andNottinghamshire. We are now developing a‘live’ action plan which has been shared withmany partners and supports a wide range ofactivity including the development of DD link-workers or champions across partner agencies.”
David Manley
“Anything (events to promote the strategyimplementation) will do providing the staff/
resource and senior support is in place tofollow it through. I liked the network approach
we adopted because I gave out leafletsexplaining what dual diagnosis was and thepart ‘we’ all needed to play in it to be moreinclusive. The leaflet had a tear off strip forpeople to complete and join. Our network
coordinator then, and now, communicates withthem about new developments.”
Mark Holland

“The strategy was launched at a conferencewhich was open to staff from both the Trustand partner agencies, carers and service users.We commissioned a theatre group to do a playon dual diagnosis for the conference, the writer/director of the piece created it after discussionwith some of our dual diagnosis service users.The strategy was placed on the Trust intranet aswell as being disseminated to all clinical teams.Each borough were encouraged to also put on a local event aimed at front line staff andservice users and were supported in doing thisby having the opportunity to use the theatregroup at their event.”
Justine Trippier
Useful Referencesand ResourcesAppleby, L.,Shaw, J.,Sherratt, J.,Amos, T.,Robinson, J., McDonnell, R., McCann, K.,Parsons, R.,Burns, J., Bickley, H., Kiernan, K.,Wren, J.,Hunt, I. M., Davies, S.and Harris, C.Safety First, Report of the NationalConfidential Inquiry into Suicide and Homicideby People with Mental Illness. London:Stationery Office (2001). http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4008914
Department of Health (1999a) National ServiceFramework for Mental Health. London:Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009598
Department of health (1999b) Safer Services.Report of the National Confidential Inquiryinto Suicide and Homicide by People withMental Illness. Department of Health
Department of Health (2000) The NHS Plan.Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4002960
Department of Health (2001) The MentalHealth Policy Implementation Guide.Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009350http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009350
Department of Health (2002) Mental HealthPractice Implementation Guide: Dual DiagnosisGood Practice Guide. Department of Health.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009058
Department of Health (2005) National ServiceFramework for Mental Health – 5 years on.Department of Health, London.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4099120
Department of Health (2006a) From Values toAction: The Chief Nursing officers review ofmental health nursing. Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4133839
Department of Health (2006b) Dual diagnosisin mental health inpatient and day hospitalsettings. Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_062649
Department of Health (2007) Safe. Sensible. Social. The Next Steps in the National Alcohol Strategy.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyandGuidance/DH_075218
Developing a Capable Dual Diagnosis Strategy 11

12 Developing a Capable Dual Diagnosis Strategy
Department of Health (2007) World ClassCommissioning.http://www.institute.nhs.uk/world_class_commissioning/world_class_commissioning/world_class_commissioning_home.htmlhttp://www.dh.gov.uk/en/managingyourorganisation/commissioning/worldclasscommissioning/index.htm
Department of Health (2008) Refocusing theCare Programme Approach: policy and positivepractice guidance. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_083647
Department of Health/ CSIP (2008) ThemedReview Report – Dual Diagnosis. Department of Health http://www.csip.org.uk/resources/publications/dual-diagnosis.html
Health Advisory Service (2001) SubstanceMisuse and Mental Health co-morbidity (dual diagnosis) standards for mental healthservices. London: HAS.
Healthcare Commission (2008) Survey of Usersof mental health services 2007.http://www.healthcarecommission.org.uk/healthcareproviders/nationalfindings/surveys/healthcareproviders/surveysofpatients/mentalhealth.
Home office (1998) Tackling drugs to build a better Britain. The Governments 10 year’sstrategy for tackling drugs misuse. HMStationary Office.http://drugs.homeoffice.gov.uk/drug-strategy/overview/
Home Office/ACMD (2003) Hidden Harm.Responding to the needs of children ofproblem drug users.http://drugs.homeoffice.gov.uk/publicationsearch/acmd/hidden-harm?view=Binary
Home Office (2008) Drugs – protectingfamilies and communities. 2008-2018 strategy.http://drugs.homeoffice.gov.uk/publication-search/drug-strategy/drug-strategy-2008-2018
Hughes, E (2006) Closing the Gap: A capabilityframework for working with combined mentalhealth and substance use (dual diagnosis).CCAWI, University of Lincoln.http://www.lincoln.ac.uk/ccawi/publications/DD%20Capbility%20Framework.pdf And DualDiagnosis Training Materials available from:http://www.lincoln.ac.uk/ccawi/ESC-DD.htm
London Drug and Alcohol Network/AlcoholConcern (2004) Local Alcohol Strategy toolkit.http://www.localalcoholstrategies.org.uk/index.php
National Treatment Agency (2002) Models ofcare for the treatment of drug misuse.Department of Healthhttp://www.nta.nhs.uk/publications/documents/nta_modelsofcare2_2002_moc2.pdf
National Treatment Agency (2006) Models ofCare for Alcohol Misusers (MoCAM).Department of Healthhttp://www.nta.nhs.uk/publications/documents/nta_modelsofcare_alcohol_2006_mocam.pdf
National Treatment Agency (2007) Drug Misuseand Dependence – Guidelines on ClinicalManagement: Update 2007. Department of Healthhttp://www.nta.nhs.uk/publications/documents/clinical_guidelines_2007.pdf
NIMHE (2003) Preventing Suicide: a toolkit formental health services.http://213.121.207.229/upload/SuicidePreventionToolkitweb.pdf
University of Manchester (2006) AvoidableDeaths: five year report of the nationalconfidential inquiry into suicide and homicideby people with mental illness.http://www.medicine.manchester.ac.uk/suicideprevention/nci/Useful/avoidable_deaths.pdf


This document is for commissioners and leadproviders of services involved in the care andtreatment of people with a dual diagnosis (co-existing mental health and substance useproblems) including statutory, third sectorand private organisations. It will be ofparticular relevance to those who are leadingdevelopment of local dual diagnosisstrategies. It builds on recommendationsfrom best practice and national guidance andaims to promote the development ofrelationships and understanding between keystakeholders in order to improve serviceprovision and the experience of service usersand carers. It also includes comments fromkey national experts in dual diagnosis whohave successfully implemented strategies intheir local areas.
Acknowledgements
Tom Dodd and Ann Gorry for commissioning thispiece of work. The following people also contributedto the development of the document: : MarkHolland; David Manley, Justine Trippier, CherylKipping, Mandy Barratt, Kevin Heffernan, MarkNorman and Patrick McGlynn.

















