ORIGINAL CONTRIBUTION Comparative Evaluation of Three End-Tidal 602 Monitors Used During Air Medical Transport • Catherine Peterson, RRT; Randy Budd, RRT; Kendra Balazs, RN, BSN, CCRN Introduction AN OUTLYING FACILITY REQUESTS THE transport of a 28-year-old male patient involved in a serious motor vehicle accident. The patient has been diagnosed with head injuries. He is intubated, mechanically venti- lated, and arterial blood gases (ABG) have been drawn. The ques- tion arises: During transport, how can the flight respiratory therapist and flight nurse evaluate effective mechanical ventilation? Presently, the flight respiratory therapist uses exhaled tidal volume, chest excursion, breath sounds, oxy- gen saturation, and clinical assess- ment of the patient to determine effective mechanical ventilation. Samaritan AirEvac's Flight Respira- tory Therapy Department investigat- ed using end-tidal carbon dioxide (ETCO2) monitors, a process also known as capnography, as another method of evaluating mechanical ventilation during transport. The purpose of this investigation was to The authors above worlC at Samaritan AirEvac in Phoenix, Ariz. Catherine Peterson is the supervisor of the flight respiratory therapists, Randy Budd is a flight respiratory therapist, and Kendra Balazs is the director of Medical Flight Services. compare ETCO2 monitors to deter- mine which model would be most suitable for the stresses of flight. Methods Several manufacturers were invit- ed to participate in the capnograph evaluation process. Three compa- nies, Ohmeda (Louisville, Colo.), Biochem International Inc. (Waukensha, Wis.), and Novametrix Medical Inc. (Wallingford, Conn.), loaned their capnographs for the study. The length of the loan for each monitor ranged from 1 to 2 months. With the varying length of monitor loans, the entire study last- ed approximately 6 months. The specific monitors used were the Ohmeda 4700, the Biochem 9090, and the Novametrix 1260. All flight respiratory therapists were instruct- ed on the use of each capnograph, and the monitors were used accord- ing to the manufacturers' proce- dures on ETCO2 monitoring. A questionnaire (Table 1) was developed to evaluate the various ETCO2 monitors. The criteria to determine the capnograph function in-flight included warm-up time, weight, size, battery life, and read- ability of the digital readout and graphical waveform. Performance options for each criteria were devel- oped by the investigators based on their past experience in the use of electronic monitoring equipment during air transport. Air medical personnel were instructed to choose the performance option that best described their experience with each capnograph they tested. The ETCO2 monitors were taken on transports in Cessna Conquest 441 pressurized fixed-wing aircraft. When no patients were on the air- craft, the monitors were used on air medical personnel to evaluate the capnograph's function. During patient transport, the monitors were used on ventilated patients, although the capnograph information was used only for the purpose of the study and not to treat the patients. The questionnaires were comp- leted by the flight respiratory thera- pist, the flight nurse, or both, and the results were then compiled by the investigators. Results The ETCO2 monitors were loaned to AirEvac for a limited time, result- ing in only 43 questionnaires being completed. The questionnaires were reviewed and the results tabulated for each criteria category. The 43 questionnaires were separated The Journal of Air Medical Transport ° February 1992 7
Transcript
ORIGINAL CONTRIBUTION
Comparative Evaluation of Three End-Tidal 602 Monitors Used During Air Medical Transport • Catherine Peterson, RRT; Randy Budd, RRT; Kendra Balazs, RN, BSN, CCRN
Introduction AN OUTLYING FACILITY REQUESTS THE t ransport of a 28-year-old male patient involved in a serious motor vehicle accident. The patient has been diagnosed with head injuries. He is intubated, mechanically venti- lated, and arterial blood gases (ABG) have been drawn. The ques- tion arises: During transport, how can the flight respiratory therapist and flight nurse evaluate effective mechanical ventilation?
Presently, the flight respiratory therapist uses exhaled tidal volume, chest excursion, breath sounds, oxy- gen saturation, and clinical assess- ment of the patient to determine effective mechanical ventilation. Samaritan AirEvac's Flight Respira- tory Therapy Department investigat- ed using end-tidal carbon dioxide (ETCO2) monitors, a process also known as capnography, as another method of evaluating mechanical ventilation during transport. The purpose of this investigation was to
The authors above worlC at Samaritan AirEvac in Phoenix, Ariz. Catherine Peterson is the supervisor of the flight respiratory therapists, Randy Budd is a flight respiratory therapist, and Kendra Balazs is the director of Medical Flight Services.
compare ETCO2 monitors to deter- mine which model would be most suitable for the stresses of flight.
Methods Several manufacturers were invit-
ed to participate in the capnograph evaluation process. Three compa- nies, Ohmeda (Louisville, Colo.), Biochem International Inc. (Waukensha, Wis.), and Novametrix Medical Inc. (Wallingford, Conn.), loaned their capnographs for the study. The length of the loan for each monitor ranged from 1 to 2 months. With the varying length of monitor loans, the entire study last- ed approximately 6 months. The specific monitors used were the Ohmeda 4700, the Biochem 9090, and the Novametrix 1260. All flight respiratory therapists were instruct- ed on the use of each capnograph, and the monitors were used accord- ing to the manufacturers ' proce- dures on ETCO2 monitoring.
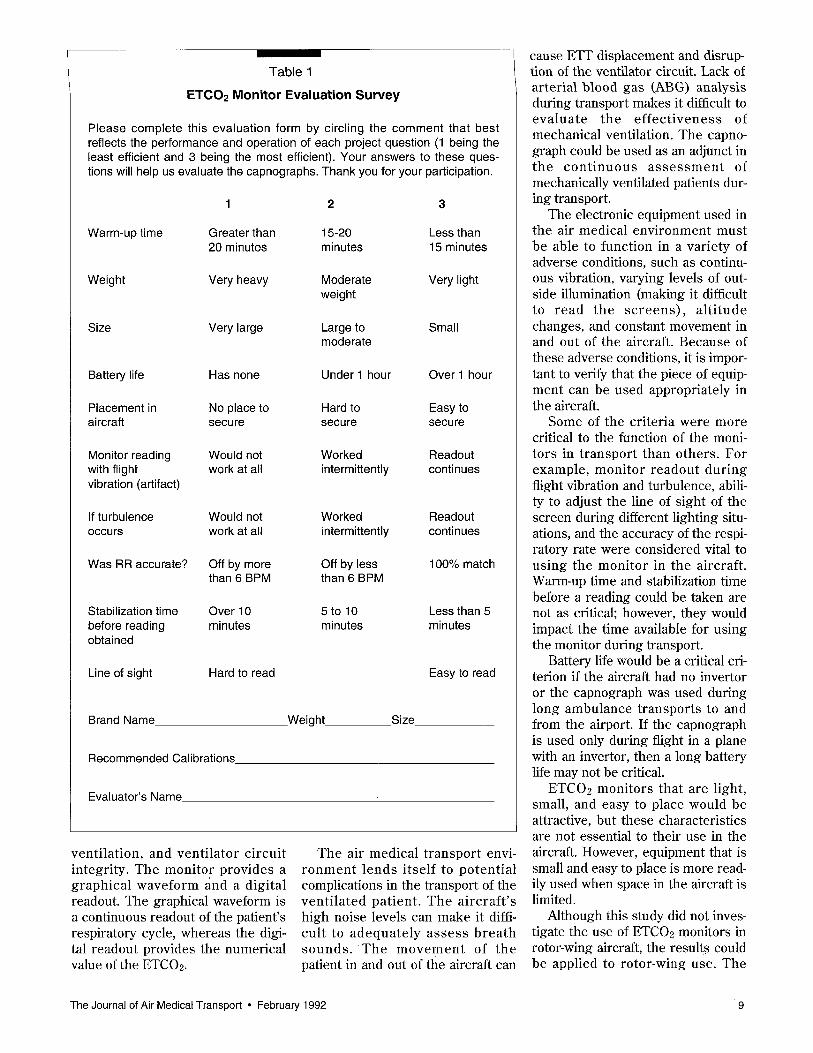
A questionnaire (Table 1) was developed to evaluate the various ETCO2 monitors. The criteria to determine the capnograph function in-flight included warm-up time, weight, size, battery life, and read- ability of the digital readout and graphical waveform. Performance options for each criteria were devel-
oped by the investigators based on their past experience in the use of electronic monitoring equipment during air transport. Air medical personnel were instructed to choose the performance option that best described their experience with each capnograph they tested.
The ETCO2 monitors were taken on transports in Cessna Conquest 441 pressurized fixed-wing aircraft. When no patients were on the air- craft, the monitors were used on air medical personnel to evaluate the capnograph's function.
During patient transport , the monitors were used on ventilated patients, although the capnograph information was used only for the purpose of the study and not to treat the patients.
The questionnaires were comp- leted by the flight respiratory thera- pist, the flight nurse, or both, and the results were then compiled by the investigators.
Results The ETCO2 monitors were loaned
to AirEvac for a limited time, result- ing in only 43 questionnaires being completed. The questionnaires were reviewed and the results tabulated for each criteria category. The 43 quest ionnaires were separated
The Journal of Air Medical Transport ° February 1992 7
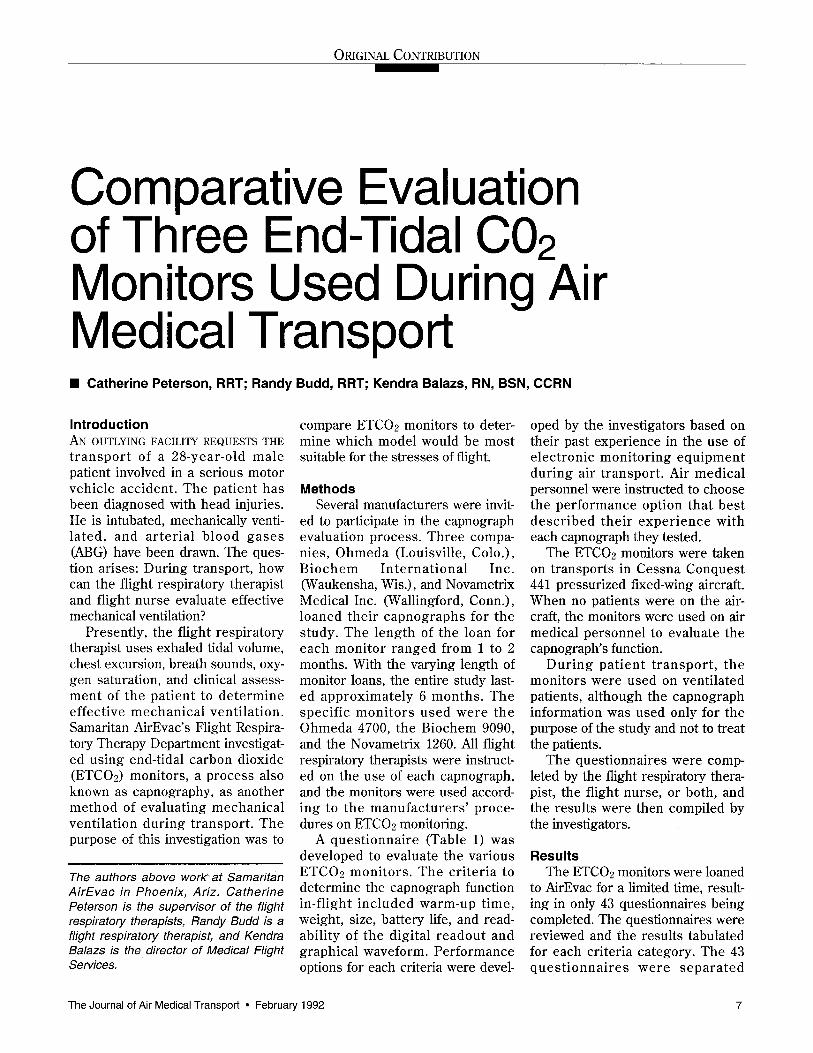
100
Figure 1
ETC02 Monitor Compar ison
80
60
40
20
Category
1. Warm-up time 2. Weight 3. Size 4. Battery life 5 . Placement in aircraft 6. Monitor readout
during flight vibration 7. Monitor readout
during turbulence 8. Respiratory rate accurate 9. Stabilization time
10. Line of sight
3 4 5 6 7 8 9 10
Legend 10hmeda ~ Biochem Novametrix
Bars based on percentage of "yes" answers.
Most Desirable Option
Less than 15 minutes Very light Small Over 1 hour Easy to secure Readout continuous
Readout continuous
100% match Less than 5 minutes Easy to read
accord ing to the th ree d i f ferent manufacturers (Figure 1).
The percentages on the bar graph r ep resen t the number of des i red responses selected by the evalua- tors . Since t h e mos t de s i r ab l e options determine the practicality of each capnograph in air transport, only the mos t des i r ab l e opt ions were reported on the bar graph. For example, the category of warm-up time had these options for the evalu- ator to choose from: (1) greater than 20 minutes, (2) 15 to 20 minutes, and (3 ) l e s s than 15 minutes. The most desirable option 6f less than 15 minutes appears on the bar graph.
The results of the survey are as follows: In c a t e g o r y 1, mon i to r warm-up time, the Ohmeda and the Biochem warmed up in less than 15
minutes 100% of the time. In cate- gories 2 and 3, weight and size of the monitors were evaluated. The options given to the evaluator were subjective; for example, the terms "very light" and "small" were used. The overall responses indicated that the monitors were too large and too heavy.
In category 4, battery life, none of the three monitors had a battery life over 1 hour. Category 5 identified the flight ,personnels' ability to easily place and secure the monitor in the aircraft,
The moni to r s w e r e s e c u r e d inside the patient platform box locat- ed in the fixed-wing aircraft. The eva lua to r s ind ica ted that the Ohmeda and the Biochem were easy to secure over 88% of the time.
The two critical criteria, monitor readout during normal flight vibra- tion and turbulence, are shown in categories 6 and 7. The Ohmeda and the Novametrix graphical waveform and digital readout functioned con- tinuously over 89% of the time.
Category 8, accuracy of the respi- ratory rate, was evaluated by com-
-paring the actual patient respiratory rate to the moni tor readout ; the Novametrix was accurate over 80% of the time.
Category 9 evaluated the t ime needed for the monitor to stabilize before a reading could be obtained; all three monitors obtained a read- ing in less than 5 minutes 100% of the time.
Category 10 evaluated the ability to adjust the line of sight and read- ability of the numerical values of the monitors during different times of the day and night. The responses for ca tegory 10 showed the Ohmeda and Novametrix performed desir- ably over 90% of the time.
Discuss ion Due to the annual n u m b e r of
anes the t i c or ven t i l a to r - re la ted dea ths and incidents of ce rebra l damage related to hypoxia, many personnel in hospital areas such as anesthesia, neonatal intensive care, and adult critical care now routinely use ETC02 monitors in the care and treatment of the mechanically venti- lated patient. 1;2
End-tidal CO2 monitoring is cur- rently used to verify endotracheal tube (ETT) placement, determine appropriate mechanical ventilator management, monitor ventilator cir- cuit integrity, and de termine the effect iveness of card iopulmonary resusc i ta t ion (CPR)3,4 Al though ETCO2 monitor use in the hospital setting has been well-documented, little literature on ETCOe monitor use in the air medical transport envi- ronment was found. 2-4
End-tidal CO2 moni tor ing is a non-invasive method of monitoring concentration in expired respiratory gases during each respiratorycycle. Capnography can provide instanta- neous information on metabolism,
8 The Journal of Air Medical Transport ° February 1992
Table 1
ETCO2 Monitor Evaluation Survey
Please complete this evaluation form by circling the comment that best reflects the performance and operation of each project question (1 being the least efficient and 3 being the most efficient). Your answers to these ques- tions will help us evaluate the capnographs. Thank you for your participation.
1 2 3
Warm-up time Greater than 15-20 Less than 20 minutes minutes 15 minutes
Weight Very heavy Moderate Very light weight
Size Very large Large to Small moderate
Battery life Has none Under 1 hour Over 1 hour
Placement in No place to Hard to Easy to aircraft secure secure secure
Monitor reading Would not Worked Readout with flight work at all intermittently continues vibration (artifact)
If turbulence Would not Worked Readout occurs work at all intermittently continues
Was RR accurate? Off by more Off by less 100% match than 6 BPM than 6 BPM
Stabilization time Over 10 5 to 10 Less than 5 before reading minutes minutes minutes obtained
Line of sight Hard to read Easy to read
Brand Name Weight_ Size
Recommended Calibrations
Evaluator's Name
ventilation, and venti lator circuit integrity. The monitor provides a graphical waveform ~{nd a digital readout. The graphical waveform is a continuous readout of the patient's respiratory cycle, whereas the digi- tal readout provides the numerical value of the ETCO2.
The air medical t ransport envi- ronmen t lends i tself to potent ial complications in the transport of the vent i la ted patient. The aircraft 's high noise levels can make it diffi- cult to adequa te ly a s se s s b rea th sounds . T h e m o v e m e n t of the patient in and out of the aircraft can
cause ETT displacement and disrup- tion of the ventilator circuit. Lack of arterial blood gas (ABG) analysis during transport makes it difficult to eva lua te the e f f ec t i venes s of mechanical ventilation. The capno- graph could be used as an adjunct in the c o n t i n u o u s a s s e s s m e n t of mechanically ventilated patients dur- ing transport.
The electronic equipment used in the air medical environment must be able to function in a variety of adverse conditions, such as continu- ous vibration, varying levels of out- side illumination (making it difficult to read the s c r eens ) , a l t i tude changes, and constant movement in and out of the aircraft. Because of these adverse conditions, it is impor- tant to verify that the piece of equip- ment can be used appropriately in the aircraft.
Some of the criteria were more critical to the function of the moni- tors in t ransport than others. For example, monitor readout during flight vibration and turbulence, abili- ty to adjust the line of sight of the screen during different lighting situ- ations, and the accuracy of the respi- ratory rate were considered vital to using the monitor in the aircraft. Warm-up time and stabilization time before a reading could be taken are not as critical; however, they would impact the time available for using the monitor during transport.
Battery life would be a critical cri- terion if the aircraft had no invertor or the capnograph was used during long ambulance transports to and from the airport. If the capnograph is used only during flight in a plane with an invertor, then a long battery life may not be critical.
ETCO2 monitors that are light, small, and easy to place would be attractive, but these characteristics are not essential to their use in the aircraft. However, equipment that is small and easy to place is more read- ily used when space in the aircraft is limited.
Although this study did not inves- tigate the use of ETCO2 monitors in rotor-wing aircraft, the results could be applied to rotor-wing use. The
The Journal of Air Medical Transport • February 1992 9
limitations for rotor-wing aircraft would probably be the large size and weight of the monitors. Capnographs may be useful for patients on ventilators during long distance transport in large rotor- wing aircraft.
Some limitations of this study are the low numbers of completed ques- tionnaires per capnograph and the subjective criteria determined by the investigators.
Summary The purpose of this investigation
on ETCO2 monitoring was to deter- mine if the monitors would function effectively in the aircraft. When compared in a cumulative manner, little difference between the three monitors was noted. The ETCO2 monitor appears to function in the fixed-wing aircraft when transport- ing critically ill, mechanically venti- lated patients. Although this study does not address the accuracy of the ETCO2 monitor during changes in altitude, a base-line reading can be
establ ished during flight. Light weight, small size and extended bat- tery life appear to be the criteria most lacking in these three capno- graphs reviewed in this study.
This study demonstrates the com- patibility of three capnographs with the aircraft environment. Manufac- turers will hopefully continue to develop ETCO2 monitors to meet the space and weight needs of flight personnel in the difficult conditions of the air medical enviroment. •
References 1. Weingarten M: Anesthetic and ventila-
tor mishaps: Prevention and detection. Crit Care Med 1986; 14:1084-86.
2. Guggenberger H, Lenz G, Federle R: Early detection of inadvertent oesophageal intubation: Pulse oximetry vs. capnography. Acta Anaesthesiol Scand 1989; 33:112-5.
3. Lillie PE, Roberts JG: Carbon dioxide monitoring. Anaesth Intens Care 1988; 16:41- 44.
4. Garnett AR, Ornato JP, Gonzales ER, et al: End-tidal carbon dioxide monitoring dur- ing cardiopulmonary resuscitation. JAMA 1987; 257:512-15.
Upcoming Feature Schedule
- M a r c h - H A l C o n v e n t i o n I s s u e
Weather-reporting systems; 1991 transport summary
- A p r i l - A d v a n c e s in C l i n i c a l C a r e
Airframe/Biomedical interface; medical crew
salaries/duties
- M a y - M i d - Y e a r C o n f e r e n c e I s s u e
Air transport economics; transport charge survey
- J u n e -
O p e r a t o r N e g o t i a t i o n s Choosing an aircraft operator
L_Z__ The Nat ional EMS Pilots Associat ion
Is proud to offer the pamphlet, I.Z Preparing • Landing Zone. This pamphlet has become the standard for providing Information and guidance to user agencies for conducting safe operations around helicopters and establishing safe landing sites. The pamphlet addresses such Issues as: Selecting an on- scene I.Z, wind direction and touchdown area, per- sonnel safety and night landing, ground guide, assisting the crew, and general helicopter safety rules. Designed as a teaching aid, the pamphlet Is Ideal for conducting classes for user agencies. Space is provided on the back cover for individual hospital Iogos, dispatch phone numbers, etc. For pricing and orders contact: The NaUonal EMS Pilots Association P.O. Box 8272 Rapid City, South Dakota 57709 (605) 341-0273
10 The Journal of Air Medical Transport • February 1992