47
Everything you Everything you wanted to know wanted to know about CKD about CKD SUE GILDERSLEVE SUE GILDERSLEVE RENAL NURSE RENAL NURSE SPECISLIST SPECISLIST
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | griffin-sullivan |
| View: | 216 times |
| Download: | 1 times |

Everything you Everything you wanted to know wanted to know
about CKDabout CKDSUE GILDERSLEVESUE GILDERSLEVE
RENAL NURSERENAL NURSE
SPECISLISTSPECISLIST

eGFR
eGFR
CKD NSFCKD NSF►Part 1 launched January 2004Part 1 launched January 2004
Dialysis and transplantationDialysis and transplantation
►Part 2 launched February 2005Part 2 launched February 2005 Chronic kidney diseaseChronic kidney disease Acute renal failureAcute renal failure End of life care End of life care
eGFRGood things about NSFGood things about NSF
Raised profile of chronic kidney diseaseRaised profile of chronic kidney disease Opportunity for education of primary care Opportunity for education of primary care
teamsteams Promotes the use of eGFRPromotes the use of eGFR Improve management particularly blood Improve management particularly blood
pressure controlpressure control Reduce morbidity and mortalityReduce morbidity and mortality Promote appropriate referralsPromote appropriate referrals
eGFR
Problems since NSFProblems since NSF Confusion re eGFR resultsConfusion re eGFR results Concern at high prevalenceConcern at high prevalence Confusion re use of ACE-I and ARBConfusion re use of ACE-I and ARB Confusion over urinary Confusion over urinary
albumincreatinine resultsalbumincreatinine results Increase in inappropriate referralsIncrease in inappropriate referrals Raised patient anxietyRaised patient anxiety
eGFR
Known CKD <1% of
population
Unrecognised CKD
10% of population
eGFR
►0.05% of UK population on dialysis or 0.05% of UK population on dialysis or with a kidney transplant with a kidney transplant (1 in 2000)(1 in 2000)
►1-2% of NHS budget1-2% of NHS budget►£25-30,000 per dialysis patient per year£25-30,000 per dialysis patient per year
Preventing 33 cases of established Preventing 33 cases of established renal failure per year saves ~£1m per renal failure per year saves ~£1m per annumannum
eGFR
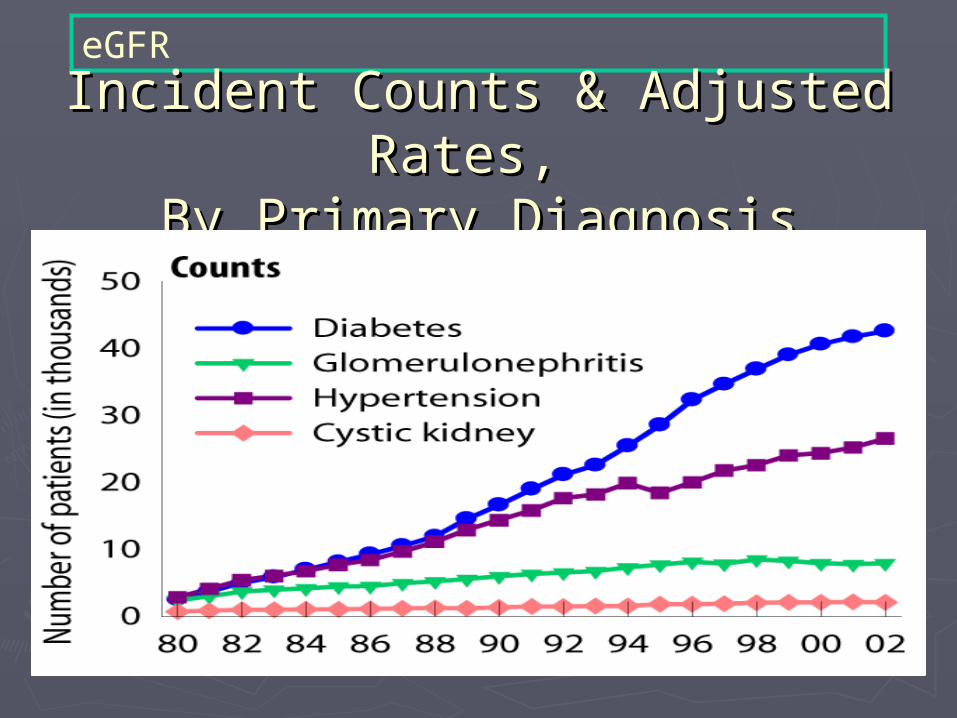
Incident Counts & Adjusted Rates, Incident Counts & Adjusted Rates, By Primary DiagnosisBy Primary Diagnosis
eGFR
GMS ContractGMS Contract►ChKD 1: The practice can produce a ChKD 1: The practice can produce a
register of patients aged 18 years and over register of patients aged 18 years and over with ChKD (US NKF Stage 3-5) 6 pointswith ChKD (US NKF Stage 3-5) 6 points
►ChKD 2: The percentage of patients on the ChKD 2: The percentage of patients on the ChKD register whose notes have a record ChKD register whose notes have a record of blood pressure in the past 15 months of blood pressure in the past 15 months (40-90%) 6 points(40-90%) 6 points
eGFR
►ChKD 3: The % of patients on the ChKD ChKD 3: The % of patients on the ChKD register in whom the last blood register in whom the last blood pressure reading, measured in the pressure reading, measured in the previous 15 months is 140/85 or less previous 15 months is 140/85 or less (40-70%) 11 points(40-70%) 11 points
►ChKD4: The % of patients on the ChKD ChKD4: The % of patients on the ChKD register who are treated with an ACEi register who are treated with an ACEi or ARB (unless contra-indication or side or ARB (unless contra-indication or side effects are recorded) (40-80%) 4 pointseffects are recorded) (40-80%) 4 points

eGFR
Assessment chronic kidney Assessment chronic kidney diseasedisease
►Assessment of severity of CKD is Assessment of severity of CKD is more accurate when based on more accurate when based on eGFR rather than plasma creatinine eGFR rather than plasma creatinine (Renal NSF 2005) (Renal NSF 2005)
►eGFR takes into account creatinine, eGFR takes into account creatinine, age and sex using the MDRD age and sex using the MDRD equation(equation(MModification of odification of DDiet in iet in RRenal enal DDisease study)isease study)
eGFR
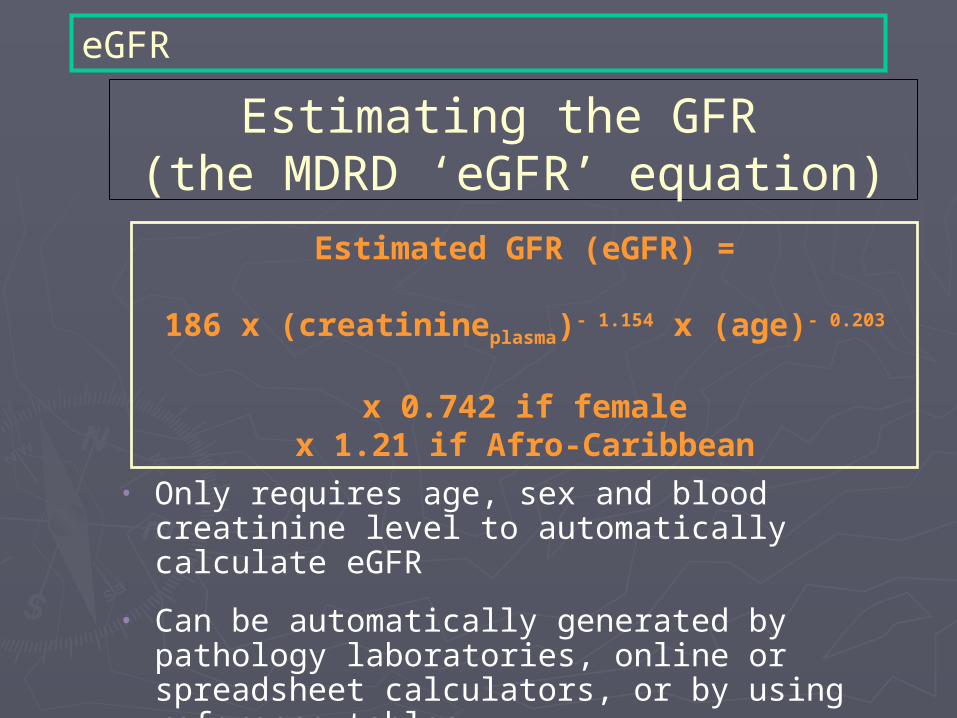
Estimating the GFR (the MDRD ‘eGFR’ equation)
• Only requires age, sex and blood creatinine level to automatically calculate eGFR
• Can be automatically generated by pathology laboratories, online or spreadsheet calculators, or by using reference tables
• Allows direct lab reporting to clinicians of estimated GFR
Estimated GFR (eGFR) =
186 x (creatinineplasma)- 1.154 x (age)- 0.203
x 0.742 if femalex 1.21 if Afro-Caribbean

eGFR
Glomerular Filtration RateGlomerular Filtration Rate►Sum of all nephron Sum of all nephron
filtration ratesfiltration rates►Best index of overall Best index of overall
functionfunction►Reduction implies a Reduction implies a
problemproblem►Translatable conceptTranslatable concept►Equates to percentage Equates to percentage
Kidney functionKidney function

eGFR
Problems with plasma creatinineProblems with plasma creatinine
Plasma creatinine determined by muscle mass as well as renal function
Normal plasma creatinine higher in:
Males vs Females
Younger vs Older
Afro-Caribbeans vs Others

eGFR
Creatinine 200umol/LCreatinine 200umol/L
eGFR 55ml/min
eGFR 5ml/min

eGFR
Influencing factors on Influencing factors on eGFReGFR
►Obesity no effect Obesity no effect ►Big muscle mass Big muscle mass creat creat eGFReGFR►Muscle wasting Muscle wasting creat creat eGFReGFR►Large meat intake Large meat intake creat creat eGFReGFR►Vegetarian Vegetarian creat creat eGFReGFR►Drugs Trimethoprin & Cimetidine Drugs Trimethoprin & Cimetidine creat creat eGFReGFR

eGFR
Chronic Kidney Disease StagesChronic Kidney Disease Stages::
Stage 1 – GFR > 90 ml/min. No kidney Stage 1 – GFR > 90 ml/min. No kidney damagedamage
Stage 2 – GFR 60 – 90 ml/min. Evidence of Stage 2 – GFR 60 – 90 ml/min. Evidence of kidney damagekidney damage
Stage 3a– GFR 45 – 60 ml/minStage 3a– GFR 45 – 60 ml/min
Stage 3b – GFR 30 - 45 ml/min Stage 3b – GFR 30 - 45 ml/min
Stage 4 – GFR 15 – 30 ml/min Stage 4 – GFR 15 – 30 ml/min
Stage 5 – Established renal failure (GFR Stage 5 – Established renal failure (GFR <15)<15)

eGFR
Stage 3 is now divided into 2 groups 3A and 3B
3A lower risk eGFR 45-59
3B higher risk eGFR 30-44
2 occasions over minimum 3 month period
eGFR
Feb 2007 Improving classification Dipstick test for proteinuria
If positive then quantify using PCR Protien Creatinine RatioThose with Proteinuria have higher risk and are classified with the addition of suffix “p” ie 2p 3Ap 4p
eGFR
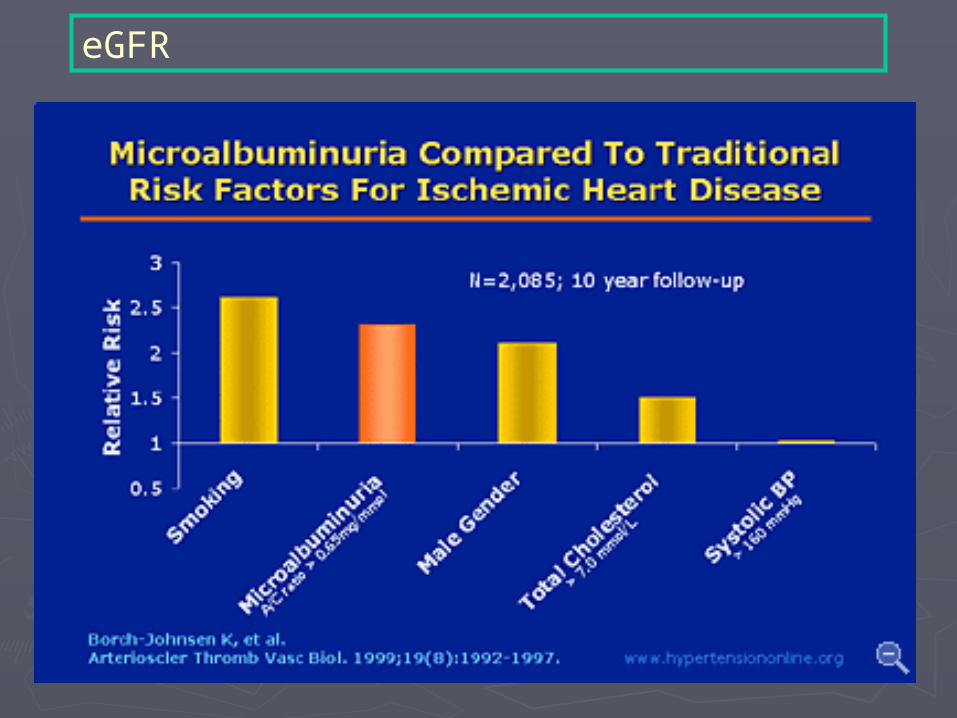
MicroalbuminuriaMicroalbuminuria►Is the first marker of diabetic Is the first marker of diabetic
nephropathynephropathy►Early detection and treatment can Early detection and treatment can
delay or prevent progression to delay or prevent progression to ESRDESRD
►Valuable marker of CV risk in T2DMValuable marker of CV risk in T2DM►All patients with diabetes should be All patients with diabetes should be
screened annuallyscreened annually
eGFR
►Ratio of albumin to creatinine in Ratio of albumin to creatinine in single urine sample (Early single urine sample (Early morning) morning)
►Test only in absence of urinary Test only in absence of urinary tract infectiontract infection
►2 out of 3 +ve tests indicate need 2 out of 3 +ve tests indicate need for treatmentfor treatment
eGFR
Meaning of results
+ve > 2.5 mg/mmol in men +ve > 3.5 mg/mmol in women
eGFR
►Unable to calculate result with Unable to calculate result with urine urine microalbuminuriamicroalbuminuria <3 means <3 means negativenegative
►Unable to calculate with Unable to calculate with urine urine microalbuminuriamicroalbuminuria >100mg/l, >100mg/l, comments will be:- suggestive of comments will be:- suggestive of proteinuria. Protein level to followproteinuria. Protein level to follow
►Results can be high in people who Results can be high in people who exercise heavily, avoid testing after exercise heavily, avoid testing after heavy exercise if you suspect this may heavy exercise if you suspect this may be the casebe the case
eGFR
Microalbuminuria Then monitor yearly for regression or
progression Microalbuminuria is likely progress to
proteinuria, unless well managed Microalbuminuria is reversible Established Proteinuria is NOT
reversible If a person has proteinuria then testing
for microalbuminuria is of NO VALUE

eGFR
ProteinuriaProteinuria►24 hr protein estimations are no 24 hr protein estimations are no
longer requiredlonger required►Protein creatinine ratio can be Protein creatinine ratio can be
measured in an early morning urine measured in an early morning urine samplesample
►This x 10 gives daily protein excretionThis x 10 gives daily protein excretion►I.e. PCR = 100mg/mmol x 10 = I.e. PCR = 100mg/mmol x 10 =
1000mg= 1g1000mg= 1g
eGFR
►It is anticipated that most patients with an It is anticipated that most patients with an eGFR less than 30 ml/min will be managed eGFR less than 30 ml/min will be managed primarily by secondary care in primarily by secondary care in collaboration with primary care colleagues. collaboration with primary care colleagues. Lesser degrees of renal impairment will be Lesser degrees of renal impairment will be managed in primary care with guidance managed in primary care with guidance and protocols from secondary care. and protocols from secondary care.
Web address for eGFR calculator:Web address for eGFR calculator:
http://www.nkdep.nih.gov/professionals/gfr_calculators/mdrd_si.htm
eGFR
Why is CKD Stage 3 Why is CKD Stage 3 important:important:Stage 3A eGFR 45-59 ml/min indicates only
slight increased CV risk
Stage 3B eGFR 30-44 is associated with x5 increase in CV risk
This is very similar to patients with a previous history of myocardial infarction.
p=proteinuria further doubles current risk ie stage 3Bp
eGFR
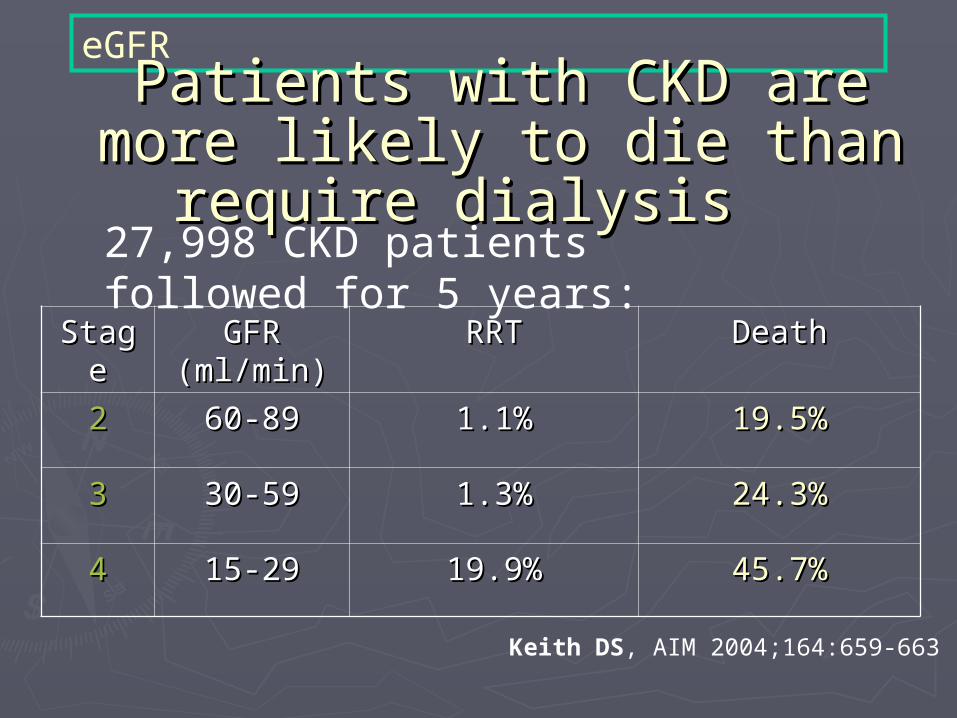
eGFRPatients with CKD are more Patients with CKD are more
likely to die than require likely to die than require dialysisdialysis
StageStage GFR GFR (ml/min)(ml/min)
RRTRRT DeathDeath
22 60-8960-89 1.1%1.1% 19.5%19.5%
33 30-5930-59 1.3%1.3% 24.3%24.3%
44 15-2915-29 19.9%19.9% 45.7%45.7%
27,998 CKD patients followed for 5 years:
Keith DS, AIM 2004;164:659-663
eGFR
eGFR
Why is hypertension important?Why is hypertension important?►Control of HypertensionControl of Hypertension
Reduces or halts eGFR declineReduces or halts eGFR decline Control reduces risk of Control reduces risk of
cardiovascular diseasecardiovascular disease
Just as effective in the elderlyJust as effective in the elderly Most of the projected increase in Most of the projected increase in
dialysis is amongst the elderlydialysis is amongst the elderly

eGFR
Practical guidance:Practical guidance:
►Refer all patients with CKD Stage Refer all patients with CKD Stage 4 and 54 and 5
►Consider referral of Stage 3 if:Consider referral of Stage 3 if:

eGFR
Stage 3 Practical Stage 3 Practical management:management:
After excluding acute cause of After excluding acute cause of decline, refer if: decline, refer if: Younger (<55 years)Younger (<55 years) Protein 2+ or more (dipstick; Protein 2+ or more (dipstick;
PCR.100mg/mmol)PCR.100mg/mmol) GFR has fallen by more than 10 GFR has fallen by more than 10
ml/min in 1 yearml/min in 1 year Haematuria – refer urologyHaematuria – refer urology
eGFRAcute deterioration of renal Acute deterioration of renal
functionfunctionConsider possible causes for deterioration:Consider possible causes for deterioration:►Prescribed and non prescribed drugs are Prescribed and non prescribed drugs are
responsible for up to 30% of acute renal responsible for up to 30% of acute renal failurefailure
►Recent introduction of ACE/ARB allow Recent introduction of ACE/ARB allow rise of up to 30% creatinine or fall of up rise of up to 30% creatinine or fall of up to 20% eGFRto 20% eGFR
►NSAID’s or other nephrotoxic drugs NSAID’s or other nephrotoxic drugs including penicillin (gentamycin) and including penicillin (gentamycin) and chinese herbal remedies chinese herbal remedies

eGFR
►Bladder outflow obstruction (any urinary Bladder outflow obstruction (any urinary symptoms?) may need renal US symptoms?) may need renal US
►Check diuretic dose. Consider reducing or Check diuretic dose. Consider reducing or stopping diuretic if no longer needed stopping diuretic if no longer needed (check ankles, JVP, postural hypotension (check ankles, JVP, postural hypotension and any other symptoms of overload or and any other symptoms of overload or dehydration) Has diabetes been poorly dehydration) Has diabetes been poorly controlled lately?controlled lately?
►Recent angiogram? Nephrotoxic Recent angiogram? Nephrotoxic dye/contrastdye/contrast
eGFR
Stage 3 Practical Management (if not Stage 3 Practical Management (if not referred)referred) Repeat dipstick or PCR - 3A annually Repeat dipstick or PCR - 3A annually
and 3B 6monthlyand 3B 6monthly Repeat creatinine, potassium, Ca/PORepeat creatinine, potassium, Ca/PO44, ,
Hb annuallyHb annually Monitor BP annually if stable (aim Monitor BP annually if stable (aim
<130/80 or 120/70 mmHg? if <130/80 or 120/70 mmHg? if progressive proteinuria)progressive proteinuria)
Recent data suggests optimal BP is Recent data suggests optimal BP is around 132/70 as low BP can reduce around 132/70 as low BP can reduce perfusion of major organsperfusion of major organs
eGFR
VaccinationsVaccinations Smoking cessation, weight Smoking cessation, weight
reduction, low salt dietreduction, low salt diet USS renal tract only if:USS renal tract only if:
►Fall in eGFRFall in eGFR►HaematuriaHaematuria►Resistant hypertensionResistant hypertension►Bladder outflow symptomsBladder outflow symptoms
eGFR
Stage 3 and DIABETESStage 3 and DIABETES As before plusAs before plus Microalbuminuria / ACRMicroalbuminuria / ACR ACEi or ARB – ACEi or ARB – creatinine can rise up creatinine can rise up
to 30%to 30% ACEi/ARB need NOT be stopped ACEi/ARB need NOT be stopped
unless potassium rises >6.0 ( could unless potassium rises >6.0 ( could try low K+ diet before stopping) try low K+ diet before stopping)
Consider stopping potassium Consider stopping potassium sparing diuretics BEFORE sparing diuretics BEFORE introducing ACEi/ARBintroducing ACEi/ARB
eGFR
Primary prevention of Primary prevention of nephropathy in diabeticsnephropathy in diabetics
► Control BP aiming for <130/70Control BP aiming for <130/70► Improve glycaemic control aim Improve glycaemic control aim
for Hba1c 6.5-7.5% recent data for Hba1c 6.5-7.5% recent data also indicates too low can be as also indicates too low can be as bad as too highbad as too high

eGFR
Type 1 DiabetesType 1 Diabetes
►1/31/3rdrd all Type 1 DM develop all Type 1 DM develop diabetic renal diseasediabetic renal disease
►Reach stage 3 approx 10yrs after Reach stage 3 approx 10yrs after diagnosisdiagnosis
►After 20yrs they will have After 20yrs they will have progressed to overt diabetic progressed to overt diabetic nephropathynephropathy
eGFR
Type 2 DiabetesType 2 Diabetes
►Type 2 DM follow a similar Type 2 DM follow a similar pattern though are not generally pattern though are not generally diagnosed until middle agediagnosed until middle age
►Type 2 diabetics with diabetic Type 2 diabetics with diabetic nephropathy often present with nephropathy often present with microalbuminuria and microalbuminuria and hypertensionhypertension

eGFR
Diabetic NephropathyDiabetic Nephropathy►Diabetic nephropathy is Diabetic nephropathy is
progressiveprogressive►Good BP control reduces the Good BP control reduces the
decline in eGFR from 12ml/min decline in eGFR from 12ml/min per year to 5ml/min per yearper year to 5ml/min per year
►ACEi/ARB may reduce this further ACEi/ARB may reduce this further to as little as 0.3ml/min per yearto as little as 0.3ml/min per year
►Correct dyslipidaemiaCorrect dyslipidaemia
eGFR
WHY ACEi or ARB?WHY ACEi or ARB?►Management of nephropathy centres Management of nephropathy centres
on aggressive treatment of BPon aggressive treatment of BP►Inhibition of renin-angiotensin systemInhibition of renin-angiotensin system►Studies show that they reduce Studies show that they reduce
intraglomerular pressure over and intraglomerular pressure over and above their effect on systemic BPabove their effect on systemic BP
►They have been shown to reverse They have been shown to reverse microalbuminuria, reduce proteinuria microalbuminuria, reduce proteinuria and reduce the rate of decline in eGFRand reduce the rate of decline in eGFR
eGFR
DUAL BLOCKADE COMBINING DUAL BLOCKADE COMBINING ACEi AND ARBACEi AND ARB
►Can be used for further control of Can be used for further control of Hypertension if other options exhaustedHypertension if other options exhausted
►Used to reduce high levels of proteinuriaUsed to reduce high levels of proteinuria►Angiotensin II can be produced by non Angiotensin II can be produced by non
ACE pathwaysACE pathways►This has been described as the ‘ACE This has been described as the ‘ACE
escape’escape’►ARB blocks the ‘ACE escape’ ARB blocks the ‘ACE escape’
eGFR
►Cooperate study looked at dual Cooperate study looked at dual blockade in non diabetic patients, blockade in non diabetic patients, this showed a significant benefit this showed a significant benefit in dual therapyin dual therapy
►Combination may have additive Combination may have additive effects in slowing progressioneffects in slowing progression
►More study is required in DMMore study is required in DM
eGFR
Difficult to treat Difficult to treat hypertensionhypertension
►Non complianceNon compliance►White coat hypertensionWhite coat hypertension►Fluid imbalanceFluid imbalance►High salt dietHigh salt diet►Renal artery stenosisRenal artery stenosis
eGFR
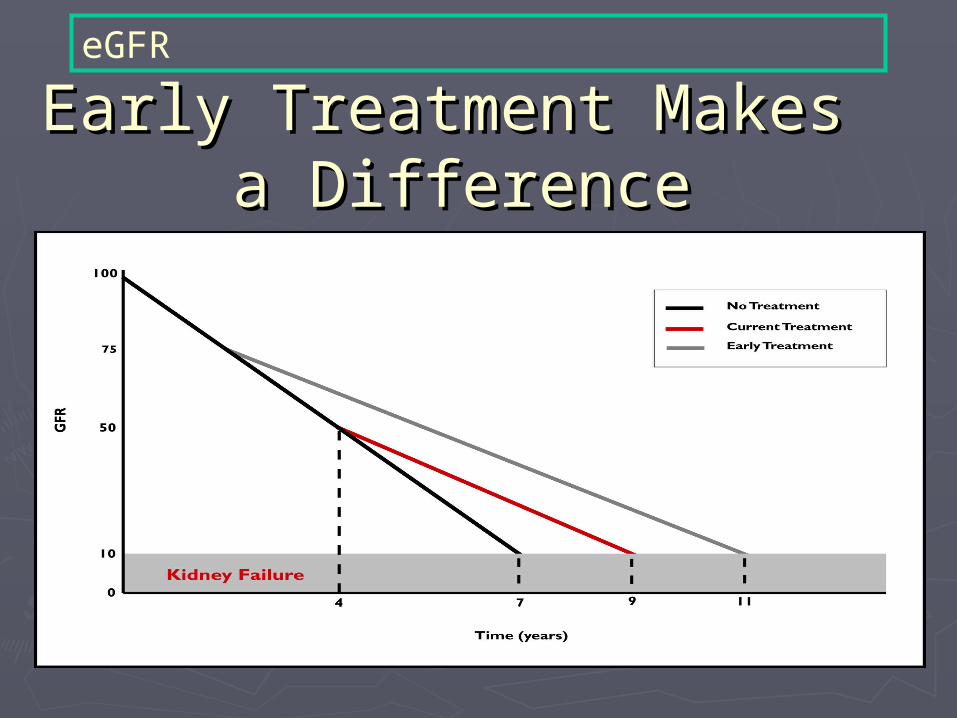
Early Treatment Makes Early Treatment Makes a Differencea Difference

















