24
Exploring the Feasibility of a Living Donor Registry Bertram Kasiske & SRTR Co-Workers ACOT 11/17/2015
| Date post: | 13-Dec-2015 |
| Category: |
Documents |
| Upload: | edward-richardson |
| View: | 217 times |
| Download: | 0 times |

Exploring the Feasibility of a Living Donor Registry
Bertram Kasiske & SRTR Co-WorkersACOT 11/17/2015
2
The first living donor
Ronald (left ) and Richard
Richard and Ronald (right)
Ronald Herrick (1931-2010)
Died of CVD complications while receiving maintenance hemodialysis.
3
Feasibility of a living donor registry
•Background•Proposal from HRSA•Designing the ideal registry•Feasibility study
4
What do we want to know?•How does donating affect the donor?
•Are there populations that are affected differently?
How will we use the information?
• To better estimate risks & improve informed consent.
• To optimize the donor evaluation and follow-up, especially in high-risk populations.
5
Questions are difficult to answer without
• Large numbers (important events are rare)
• Long term follow-up (events accrue slowly)
• Comparable controls (donor selection bias)
We need a registry with controls!
6
• Delegate LD follow-up beyond 3 months to a third party organization, with consent for follow-up obtained before donation. Follow-up through this mechanism would include maintenance of contact information on LDs, surveillance for the development of specified comorbidities, serious and rare events, and facilitation of future investigations of donor outcomes.
• Provide additional ascertainment of serious events (e.g. deaths, end stage renal disease) through linkage of the OPTN/SRTR database with existing public databases including the SSDMF, the National Center for Healthcare statistics and CMS…
• Include psychosocial and socioeconomic outcomes assessment in the mid- and long-term follow-up of LDs.
September 2010
7
Feasibility of a living donor registry
•Background•Proposal from HRSA•Designing the ideal registry•Feasibility study

8
Feasibility study requirementsThe feasibility plan will include:
• identification of donor and control cohorts• development of consent form• frequency of follow-up• development of survey instruments and data collection
forms to monitor the intermediate- to long-term development of comorbidity and serious events
• assessment of psychosocial and socioeconomic consequences of donation
• methods of data collection• detailed estimates of the first year start-up cost and
subsequent annual operating cost
9
Feasibility study time line
Final report on feasibility assessment
due to HRSA by June 20, 2016
10
Feasibility of a living donor registry
•Background•Proposal from HRSA•Designing the ideal registry•Feasibility study
11
•All living donors in the US- Use only TIEDI® LDR and LDF forms (?)
• Controls- Need to determine which donor candidates are controls- Collect same data as collected for donors (LDR)- Obtain consent at initiation of evaluation
• Consent for follow-up data linkages and possible surveys- No additional follow-up data from transplant programs
• Consent for blood storage for future DNA analysis- Analyze only “worrisome” genes, e.g. APOL1
What should a registry include?
12
•Option #1:- Collect data only when it is determined that donation will
not take place due to factors that will cause least bias.- Pro: data collection minimized- Con: difficult for centers to select controls
•Option #2:- Collect data on all who come to the center for evaluation.- Center subsequently records reasons for not donating.- Pro: outcomes of all candidates can be determined- Con: increases data collection burden
What is the best way to register controls?
13
Are current TIEDI® forms adequate for baseline data collection?
•Living donor registration (LDR):- Demographics & socioeconomics- History of transmissible disease- Pre-donation kidney function- CV risk factors, but no events- Post-Op Complications (1st 6 weeks)
•Living donor follow-up (LDF):- Status last known at 6, 12, and 24 months- Serum creatinine, BP, diabetes, dialysis
14
What are the outcomes of interest?
•Outcomes important to patients:- Morbidity - All-cause mortality- ESRD- Cardiovascular disease events- Hospitalizations- Health care cost- Quality of life
15
What should a follow-up survey of donors include?
•Standardized health outcomes, e.g. SF36
• Information unique to donors- If you had it to do over again would you?
- What financial difficulties have you had?
- Difficulty obtaining insurance?
- Other …
•Ask donors what to ask donors!

16
Feasibility of a living donor registry
•Background•Proposal from HRSA•Designing the ideal registry•Feasibility study
17
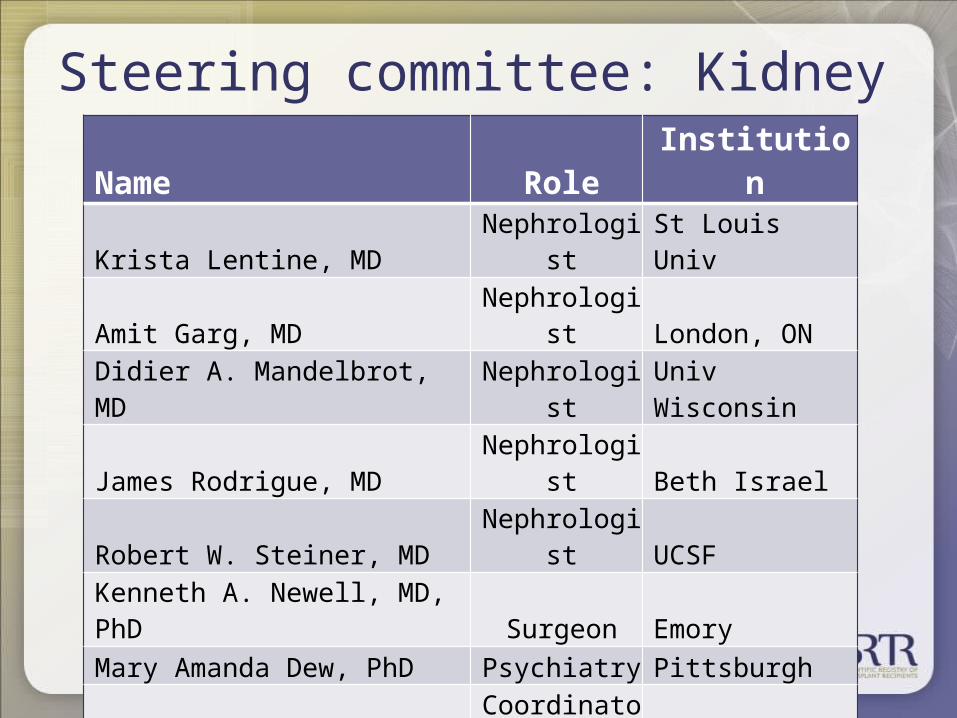
Steering committee: KidneyName Role InstitutionKrista Lentine, MD Nephrologist St Louis UnivAmit Garg, MD Nephrologist London, ONDidier A. Mandelbrot, MD Nephrologist Univ WisconsinJames Rodrigue, MD Nephrologist Beth IsraelRobert W. Steiner, MD Nephrologist UCSFKenneth A. Newell, MD, PhD Surgeon EmoryMary Amanda Dew, PhD Psychiatry PittsburghKathy Schwab, RN Coordinator MayoDeonna Moore, PhD(c), MSN Coordinator VanderbiltCheryl Jacobs, MSW Social Worker UMNSheila Adams-Leander R.N., Ph.D. Patient MilwaukeeElisa J Gordon, PhD, MPH Ethicist Northwestern

18
Steering committee: Liver
Name Role InstitutionDianne LaPointe Rudow, DNP Coordinator NY Mt SinaiAbhinav Humar, MD Surgeon PittsburghRobert Merion, MD Surgeon MichiganKim Oltoff, MD Surgeon PennRyutaro Hirose, MD Surgeon UCSFJim Trotter, MD Hepatologist Baylor, DallasMichael R. Charlton, MD Hepatologist UtahRobert S. Brown, Jr., MD, MPH Hepatologist CornellDonald Olenick, ESQ Patient New York
19
Pilot survey of donors• 8 feasibility study sites• Obtain expedited IRB review for a brief patient survey• New donor candidates January 1st to April 30st
• Sites will survey and complete one-page form on all incident donor candidates asking willingness (or if not why not) to:
- have data collected,- be contacted in the future to determine well-being,- have extra tube of blood stored for possible DNA testing.
• Estimate time, effort and costs (minimal reimbursement).• Ascertain by reviewing records the reasons for not donating
among potential donors evaluated in 2010 to estimate possible control sample size.
20
Survey programs
•Develop and distribute a brief survey•Would your program agree (and if not why not) to:
- Consent each donor at start of on-site evaluation?- Complete a LDR for patients who do not donate purely
for non-medical reasons?- Collect blood?- Maintain and periodically provide living donor contact
information to a HRSA contractor?• Tabulate results of the survey to gauge participation
21
Perform pilot SRTR analysis
• Establish retrospective living donor cohort• Link to SRTR data for transplants • Link to CMS data for deaths, ESRD and causes, etc.• Link to NDI data for deaths and causes of death• Link to Pharmacy Claims data to explore what can
be learned about living donor health over time• Explore feasibility of linking to other databases in
the future
22
Determine methods for storing samples for future DNA analysis• Locate secure site• Determine logistics and costs for
- shipping,- -80 degree freezers,- security and back-up plans.
• Establish committee to recommend to HRSA when samples should be analyzed (prototypical example APOL1)
23
Summary
•We need a national registry to obtain long term follow up data on living donor outcomes.•A feasibility study for a registry should include:
- A survey of patients - A survey of programs- Establishing data linkages for follow up information- Determining logistics and costs of DNA sample storage- Determining mechanisms and costs of data reporting
Thank You!








![21 st Century Kids Notes from a keynote by Dr. David Dwyer [ACOT] Department of Education Meeting July 2002 Washington, D.C.](https://static.documents.pub/doc/80x56/56649ec95503460f94bd6db8/21-st-century-kids-notes-from-a-keynote-by-dr-david-dwyer-acot-department.jpg)








