997.e78 CHAPTER 35 Functional Appliances L J K M N FN 75% OL P 92% 19.9% 25% Functional correction with growth Functional correction without growth 12.3% 75% -75% -24.5% O FIGURE 35-38, cont’d A B C FIGURE 35-39 JM, a 12½-year-old male patient, had a Class II malocclusion by virtue of retro- gnathic mandible (SNB = 71 degrees, Pogonion to Nasion Perpendicular line = −17 mm), overjet of 9 mm associated with deep bite (6 mm), and hypoplasia of upper lateral incisors. Pretreatment records: A, Profile. B, Smile. C, Frontal view.
Transcript
997.e78 CHAPTER 35 Functional Appliances
LJ K
M N
FN
75%
OLP
92%19.9%
25%
Functional correction with growthFunctional correction without growth
12.3%75%
-75%-24.5%
OFIGURE 35-38, cont’d
A B C
FIGURE 35-39 JM, a 12½-year-old male patient, had a Class II malocclusion by virtue of retro-gnathic mandible (SNB = 71 degrees, Pogonion to Nasion Perpendicular line = −17 mm), overjet of 9 mm associated with deep bite (6 mm), and hypoplasia of upper lateral incisors. Pretreatment records: A, Profile. B, Smile. C, Frontal view.
997.e79CHAPTER 35 Functional Appliances
D E
F G
H I
J K
FIGURE 35-39, cont’d D, E, Treated with the functional magnetic system (approximately 24 months) because of an initial poor compliance that required bonding the appliance for 3 weeks. F, G, The upper central incisors served as abutments for the functional magnetic system appliance by reason of the delayed eruption of the upper canines. H, The bite clearance was increased to facilitate the guidance of eruption of the posterior segment. I, Posttreatment occlusion included restorative recontouring of the lateral incisors with composite. The pubertal gingival hypertrophy was left untreated because of expected self-improvement after bracket debonding. J, K, Post-treatment profile and smile. L, Schematic illustration of functional correction, mandibular skeletal contribution was reduced by one half (20.2%) when growth was considered. This reduction was followed by an increase in upper distalization contribution (from 27.3% to 40%). OLp, Occlusal line perpendicular. (A–H courtesy Costas Ergatoudes; I–K courtesy Vasilis Kalamatas.)
997.e80 CHAPTER 35 Functional Appliances
L
JM
Functional correction with growth
27.3%40%
57%
63.6%
20.2%
−36.4%−17.4%
45.5%
Functional correction without growth
OLP
FIGURE 35-39, cont’d
Max
illa
Man
dibl
e
FIGURE 35-41 Average natural displacement pattern of the maxilla (Point A) and the mandible (pogonion), relative to the anterior cranial base. The horizontal and vertical vectors (white) and the resultant vector of displacement are shown. In an average facial growth pattern, the forward component of the mandibular symphysis displacement is slightly greater than that of the anterior apical base of the maxilla. The differ-ence is marked at the bottom. Of course, as Coben points out, if superimposition occurred on the entire cranial base, includ-ing the sphenooccipital synchondrosis, then the result would be different.
SO
se fe
em lm
fm
pm
zm
ptp
C
NS
FIGURE 35-40 Growth directions of the cranial base and facial sutures, with a resultant expanding V, is accomplished as the cra-nial portion moves upward and forward from the sphenooccipi-tal synchondrosis (SO) and the facial portion moves downward and forward. C, Reflection of condylar and ramal growth; NS, nasal septum growth vector; se, sphenoethmoidal suture; pm, pterygomaxillary fissure; ptp, pterygopalatine suture; fe, frontoethmoidal suture; em, ethmoidal-maxillary suture; lm, lacrimal-maxillary suture; fm, frontomaxillary suture; zm, zygo-maticomaxillary suture. (Adapted from Coben SE: Growth and Class II Treatment, Am J Orthod Dentofacial Orthop 52:5-26, 1966. With permission from the American Association of Ortho-dontists.)
997.e81CHAPTER 35 Functional Appliances
provide the desired correction.* A study by Altenburger and Ingervall,100 comparing combination headgear-activator results with the results achieved using an activator alone, still does not show a significant distalizing effect with combination therapy. However, in a more recent study, Du, Hagg, and Rabie27 show significant molar distalization when incorporating a headgear with the Herbst appliance.
Again, the reader is referred to the excellent chapter by Stöckli and Teuscher in the second edition of this book for techniques and treatment.173 Figures 35-44 and 35-45 illus-trate the activator-headgear appliance. Proper construction implies that the extraoral force component considers any possible rotational effect from extraoral force, which must pass as close as possible through the maxillary center of resistance.
Perhaps the best compromise, ensuring optimal stability of the functional appliance when the headgear is worn, is to place first molar bands and buccal tubes, insert the occipital pull extraoral force arms into the buccal tubes, and have the wire clasps of the functional appliance snap above the buccal tubes to give maximal retention for day and night wear of the func-tional appliance. Three-dimensional control of molar anchor
* References 61, 113, 129, 158, 171, 175–178.
teeth is a top priority, preventing unwanted opening of the bite. This two-jaw approach enhances anchorage and dentoalveolar compensation and provides optimal growth guidance. Various functional appliances can be used—a Bionator, twin block, or monobloc appliance—but with reduced bulk to permit full-time wearing.
Fixed Functional AppliancesHerbst ApplianceAt the International Dental Congress of 1909 in Berlin, Emil Herbst presented a fixed bite-jumping device called Schar-nier, or joint179 (Figs. 35-46 to 35-48). The idea of continually keeping the mandible forward and eliminating the need for patient compliance, as is required with removable functional appliances, appealed to clinicians. In 1934, Herbst and Martin Schwarz wrote a series of articles describing their case selection,
Max
illa
Man
dibl
e
FIGURE 35-42 The concept of stimulating specific forward growth, with mandibular displacement (black) to bring about the so-called jumping of the bite in Class II treatment with functional orthopedics, can be an unfulfilled orthodontic “dream” because the actual change that occurs without appliance interference cannot be measured at the same time. The morphogenetic pattern, treatment timing, appli-ance used, and patient compliance are important determin-ing factors. For these reasons, forecasting is a difficult, if not impossible, task.
Max
illa
Man
dibl
e
FIGURE 35-43 Reduction of the sagittal component of maxil-lary skeletal and dentoalveolar structures (black) is compared with the average values. Stöckli and Teuscher believe that this possibility is more realistic with functional appliances, despite the research of McNamara and others, which shows little effect of functional appliances on the maxilla. The use of an extraoral appliance (headgear) does enhance sagittal withholding or a distalizing effect on the maxilla, hence the justification for combined functional appliances and headgear. In many cases, however, rotational and elongating reactions by the maxilla and dentoalveolar structures create additional vertical demands and reduce the potential sagittal correction, causing an opening mandibular rotation that exacerbates the apical base discrep-ancy (lower diagram). Because of dominant vertical growth, as shown by Buschang, appliance control of this vector is essential (i.e., vertical growth is much greater than sagittal growth).
A B C
GG H I
D E F
J K
FIGURE 35-44 Activator-headgear appliance and extraoral attachments. A, Vestibular extensions and torquing springs are demonstrated. B, The appliance is placed on the lower cast. Note the anterior area with torquing springs, palatal extension of acrylic, and transpalatal wire. C, The appliance is placed on the upper cast with the facebow inserted. Note the lower lingual flange extension for engaging the mandib-ular arch, similar to the Hamilton appliance. D, Appliance view again shows the transpalatal bar, torquing springs, and lingual extensions. E, The activator-facebow is in place. F, The activator is in place on the lower arch, showing the insertion of the facebow. Note the tongue against the transpalatal Coffin spring. In this construction, labial and lingual wires are used instead of torquing springs. G, An anteriorly placed force vector is estimated in this case to pass just anterior to the center of resistance of the maxilla. Some anterior rotation of the dentition must be expected, and ample condylar growth is required. H, Average steepness of the force vector is estimated to pass slightly superior to the center of resistance of the upper dentition. The posterior rotational effect on the maxilla and the anterior rotational effect on the dentition should neutralize each other to ensure that no change is expected in the inclination of the occlusal plane. I, The posteriorly placed force vector is estimated in this case to pass just inferior to the center of resistance of the dentition. Posterior rotation of the maxilla and dentition must be anticipated. This setup is used for patients with an open bite tendency or when the prognosis of condylar growth is poor. J, K, Lateral cephalograms are provided to check force vectors (line connecting the circle at the end of the outer arms of the face-bow and the circle at the springs of the headcap) to the centers of resistance of the maxilla (white circle) and upper dentition (black dot).
997.e83CHAPTER 35 Functional Appliances
A
C
D
B
FIGURE 35-45 Maxillary component of the Stöckli-Teuscher appliance. A, Extension on the pal-atal side. Placement of headgear tubes and palatal wire; retention area of torquing springs. B, Occlusal and incisal replica relief of the upper teeth. C, Interocclusal placement of the headgear tube. D, Design and position of the torquing springs. Only the palatally curved tip should touch the crown, contiguous to the gingival margin. Note buccal tubes.
FIGURE 35-46 Working hypothesis of the Herbst appliance. (Courtesy Dentaurum, Berlin, Germany.)
997.e84 CHAPTER 35 Functional Appliances
experiences, problems, and solutions.180 Patients with retro-gnathic mandibles and TMJ problems responded best. Break-age had been reduced by some design changes of the tube and plunger assembly. However, after this, little appeared in the lit-erature until the concept was resurrected by Hans Pancherz.107 In 1979, Pancherz’s article in the American Journal of Orthodon-tics called attention to the possible stimulation of mandibular growth. Subsequent articles have elaborated on modifications and the short- and long-term effects on jaw relationship, occlu-sion, and masticatory efficiency.31,50,114,181 Ruf and Pancherz’s long-term research53,54 and clinical use have prompted oth-ers to use this approach or modify the appliance (e.g., Jasper Jumper, Eureka Spring).182
The Herbst appliance can be compared with an artificial joint between the maxilla and mandible. The bilateral telescopic mechanism maintains the protracted position of the mandible,
FIGURE 35-47 The disassembled telescopic mechanism (plunger and tube) of the Herbst appliance is available in pairs. (Courtesy Hans Pancherz.)
A BFIGURE 35-48 Anchorage system of Pancherz’s version of the Herbst appliance. A, Partial anchorage (banded appliance). B, Total anchorage (banded appliance). C, Total anchorage (cast splint appliance).
997.e85CHAPTER 35 Functional Appliances
even during function (see Fig. 35-48). This appliance and its use are fully described by Hans Pancherz in an extensive chap-ter in Dentofacial Orthopedics with Functional Appliances, 2nd ed., by Graber and associates.10 Each device consists of a tube, a plunger, two pivots, and two locking screws that prevent the telescoping elements from slipping past the pivots (see Figs. 35-46 and 35-47). The pivot for the tube is usually soldered to the maxillary first molar band, and the pivot for the plunger is attached to the mandibular first premolar band. Pancherz found that waiting until the premolars erupted before start-ing therapy still allows enough time for harnessing adequate remaining growth, particularly in boys.
Generally, the protraction of the mandible for the Herbst appliance is similar to that for the Bionator, with the incisors in an end-to-end relationship, although the incremental advance-ment approach can be used in large sagittal discrepancies (Fig.
35-49). Du, Hagg, and Rabie27 prefer incremental advancement and show significant benefit with this method, duplicating the research of Petrovic and Stutzmann on rats.
The length of the tube-plunger assembly determines the amount of advancement. Although conventional orthodon-tic bands can be used, Pancherz prefers his current approach of casting splints of chromium-cobalt alloy that incorporate molars and premolars and are cemented as units with glass ionomer cement (see Fig. 35-48, C). This method saves chair time and causes few clinical problems. For patients with nar-row arches, a first-phase expansion can be done with a palatal expansion appliance (one or two expansion screws), or a quad helix appliance can be incorporated into the maxillary appli-ance (Fig. 35-50). Construction details, per-visit tasks, and the effects of Herbst therapy are thoroughly described in Dentofa-cial Orthopedics with Functional Appliances, 2nd ed., by Graber and associates10 and in the periodical literature.
The Herbst appliance is a powerful and effective functional system in the treatment of Class II malocclusions.53 As with other functional appliances, viscoelastic stretch is important. Normal-ization of occlusion is generally accomplished in 6 to 8 months. Overcorrection of sagittal arch relationships and incomplete cuspal interdigitation, resulting from slower eruption of poste-rior teeth, are to be expected as settling occurs. Skeletal and den-tal changes contribute to the treatment result.54,127,183 Fränkel93 was critical of the short duration of Herbst appliance wear and recommended prolonged active removable appliance retention and myofunctional exercises during the growth period, as do orthopedic surgeons for growth guidance problems. This prac-tice takes advantage of continued jaw growth. The author of this chapter supports this concept. The downside is that prolonged patient compliance is more difficult.
Sagittal ChangesFigure 35-51 illustrates the restraint of the maxillary arch and the stimulation of mandibular growth.10 Bone remodeling pro-cesses are clearly evident on the lower border of the mandible. Histologic studies confirm these observations.1 The ultimate condylar position in the fossa is unaffected by Herbst appliance therapy, unless the original problem was a Class II, Division 2 malocclusion. However, and this is again emphasized, modifi-cation of the TMJ fossa itself occurs during the growth period. The lower incisors are proclined, and the maxillary molars are posteriorly moved, as with a high-pull headgear.31 During the first year after treatment, the occlusion settles and the sagit-tal relationships recover approximately 30% of their previous dimensions. Approximately 90% of the posttreatment occlusal changes occur during the first 6 months and are primarily of dental origin. Lower incisor procumbency rebounds to a sig-nificant degree. Lower molars and upper molars tend to move posteriorly and anteriorly, respectively, after treatment.53
An unfavorable maxillomandibular growth relationship con-tributes to early posttreatment changes only to a minor degree. A catch-up in maxillary growth and a minor reduction in man-dibular growth increments are apparent in patients treated with the Herbst appliance.31,54 Again, continued functional retention may enhance stability.
Vertical ChangesIn Class II malocclusions with deep bites, overbite may be sig-nificantly reduced with Herbst therapy.31,53 The change primar-ily results from eruption of lower molars and the intrusion of
CFIGURE 35-48, cont’d
997.e86 CHAPTER 35 Functional Appliances
A B
E
G
F
H
DC
FIGURE 35-49 Case report by Rabie shows the protraction of the mandible for the Herbst appli-ance. A, Pretreatment frontal view. B, Pretreatment lateral profile. C, Pretreatment panoramic radiograph. D, Pretreatment cephalometric radiograph. E, Lower occlusal view with the appliance in place. F, Upper occlusal view, noting the space gained by the distalization effect of the Herbst appliance (arrows). G, H, Posttreatment occlusal views. I, Posttreatment frontal view. J, Posttreat-ment lateral profile. K, Superimposition of cephalometric tracing: before treatment, after Herbst appliance, and after full treatment. (Courtesy ABM Rabie, Hong Kong University, Hong Kong.)
997.e87CHAPTER 35 Functional Appliances
I J
KFIGURE 35-49, cont’d
A B
FIGURE 35-50 A, Upper cast splint Herbst appliance is used with quad helix lingual arch for expansion. B, A rapid palatal expansion jackscrew may also be used with cast Herbst appliance.
997.e88 CHAPTER 35 Functional Appliances
the lower incisors. As previously noted, proclination of lower incisors contributes to the seeming intrusion of these teeth. Nevertheless, the appliance has a limited effect on the maxillary and mandibular jaw positions, as expressed by the palatal plane angle and the mandibular plane angle. One must stress again that part of the change is an improvement in the glenoid fossa position and morphologic structure, a change long overlooked until the seminal research of Peter Buschang24 and Hans Ullrich Paulsen.49,50
Long-Term Posttreatment ChangesSeveral effects have been observed 5 to 10 years after treatment in patients treated with the Herbst appliance. A Class I dental arch relationship is maintained by a stable cuspal interdigi-tation of the upper and lower arches, whereas relapse tends to occur in cases with unstable occlusal conditions.54 Teeth locked in a proper relationship are more likely to transfer continuing maxillary growth forces to the mandible. Pancherz emphasized a functionally stable occlusion as possibly more important than posttreatment growth increments. The most common combination of factors leading to varying degrees of relapse are too early treatment, mixed dentition treatment, persistent lip or tongue dysfunction habits, unstable posttreat-ment occlusion, and insufficient length of appliance wear and retention measures. However, in Pancherz’s view, unfavorable posttreatment growth is not a significant factor for occlusal relapse.
Although too early treatment is often associated with relapse, it actually may not be responsible for relapse. More likely, in the mixed dentition, a solid Class I interdigitation is not possible with the deciduous molars. Pancherz believes therefore that the unstable occlusion, not the timing, is responsible.53 Pancherz
notes, however, that the most favorable time to initiate treat-ment is during the peak pubertal growth period.
Pancherz is totally objective in his intensive and impres-sive long-term studies. In addition, Pancherz notes from his own and a number of other studies that the basal skeletal rela-tionship is improved but not totally normalized, whereas the occlusal relationship is essentially normalized.31,46 The impli-cation is that the Herbst appliance is capable of producing sag-ittal changes that can partially compensate for aberrant skeletal relationships.
A recent study by Ruf and Pancherz54 assesses the TMJ adap-tation through prospective magnetic resonance imaging and roentgenographic techniques. A similar paper was accepted for publication in the American Journal of Orthodontics and Dento-facial Orthopedics in 1999. Both papers clearly show significant remodeling with Herbst fixed functional treatment. Strangely enough, comprehensive, long-term studies of the modification of temporomandibular morphologic structure and position in the growing face have yet to be done for fixed appliances, although Paulsen and colleagues49,50 show convincing evidence of fossa remodeling with sophisticated tomography for short-term Herbst treatment. This long-overlooked phenomenon has been emphasized in this chapter, and references to the seminal work done by Bierbaek and colleagues,66 Buschang and Santos- Pinto,24 Decrue and Weislander,69 Droel and Isaacson,70 Hotz,83 Ikai and associates,32 Kantomaa and Pirttiniemi,34 Pancherz,47 and Paulsen49 clearly indicate the tissue changes, as demon-strated by the Buschang study of changes in the position of the glenoid fossa during growth. It is only logical, then, that the same implications should apply for conventional removable functional appliances. Buschang and Santos-Pinto24 show the significant potential to affect the changing position of the mem-branous bone TMJ elements, both fossa and articular eminence. Nature already has pointed the way to this possibility by showing adaptations to deep bite (deep fossa, steep eminence) and Class III malocclusions (shallow fossa, eminently shallow curve).29
In another provocative unpublished study that the author directed some years ago at Northwestern University by Dayton Blume and Vernon Boman, postural resting and habitual occlu-sion condylar and fossa relations were measured in samples of Class I and Class II malocclusions. A significantly higher per-centage of condylar retrusion was noted in the Class II sample (Fig. 35-52). Knowing what orthodontists now know about the potentially deleterious effects of condylar retrusion, the logical question may be, “How much of the underdeveloped mandi-ble resulted from interference with metabolism, as dramatically illustrated by Graber,65 Isberg,139 Jasper and McNamara,140 Ward and associates,80 and others?” (See Fig. 35-20.)
The effects on the facial profile have also been studied by Pancherz and associates.45,48,114 In patients who were treated for 7 to 8 months and reexamined 5 to 10 years after treatment, a general reduction of hard and soft tissue profile convexity was noted (Fig. 35-53). The upper lip becomes less protrusive, whereas the lower lip remains almost unchanged. However, considerable individual variations were noted (Fig. 35-54).
Overall, the following long-term posttreatment changes can be expected: • Reduction of the soft tissue profile convexity (excluding
the nose), with an increase in mandibular prognathism (see Fig. 35-53)
A
B
–2
+2
+1
0
–1
Deg
rees
S-N-A
S-N-B
A-N-B
Herbst appliance (n = 22)Control (n = 22)
Condyle
Pogonion
3
2
1
mm
Herbst appliance (n = 22)Control (n = 20)
FIGURE 35-51 A, Mean and standard deviation changes in SNA angle, SNB angle, and ANB angle over 6 months. B, Increase in mandibular length over a 6-month period is demonstrated.
997.e89CHAPTER 35 Functional Appliances
Case No. 7 24 23 14 16
25 19 17 21 18
4 22 20 15 8
11 13 1 10 9
5 12 3 2 6
Case No. 8 14 9 21 10 15 7
13 6 4 18 1 12 19
20 16 17 3 5 2 11
FIGURE 35-52 Unpublished radiographic research by Dayton Blume and Vernon Boman show the path of closure from the postural resting position (black solid line) to habitual occlusion (red dotted line) in normal patients (left) and those with a Class II malocclusion (right). This evidence indicates significantly more translatory action (functional retrusion) with an upward and backward path of closure for Class II malocclusions. Normally, condylar movement is essentially rotary from postural rest to maximal intercuspation (left). (From Graber TM. Anatomische und physi-ologische aspekte bei der behandlung von kiefergelenksstörungen [The anatomical and physi-ological aspects in the treatment of temporomandibular joint disorders]. Fortschr Kieferorthop 1991;52:126–132.)
5
2
1
–1
–2
3
4
Deg
rees
Originalvalue
Before After Follow-up
FIGURE 35-53 Mean changes in the soft tissue facial profile angles, excluding the nose (dotted line) and including the nose (solid line), in 49 subjects treated with the Herbst appliance. Positive values imply profile convexity reduction. Negative values imply profile convexity increase. Measurements were taken before treatment (original value of 0), after 7 months of appliance wear, when the appliance was removed, and at fol-low-up 5 to 10 years after treatment. (Data from Pancherz H, Fischer S. Amount and direction of temporomandibular joint growth changes in Herbst treatment: a cephalometric long-term investigation. Angle Orthod 2003;73:493–501.)
2.5
2.4
2.3
2.2
2.1
Before After Follow-up
Mill
imet
ers
Originalvalue
E line
FIGURE 35-54 Mean changes in the position of the upper lip (dotted line) and the lower lip (solid line) in relation to the aes-thetic line in 49 subjects treated with the Herbst appliance. Negative values imply lip retrusion. Measurements were taken before treatment, when the appliance was removed, after 7 months of appliance wear, and 5 to 10 years after treatment. (Data from Pancherz H, Fischer S. Amount and direction of temporomandibular joint growth changes in Herbst treat-ment: a cephalometric long-term investigation. Angle Orthod 2003;73:493–501.)
997.e90 CHAPTER 35 Functional Appliances
• Increase in the soft tissue profile convexity (including the nose), largely because of normal nasal growth (see Fig. 35-53)
• Retrusion of the upper and lower lips in relation to the aes-thetic line because of normal nose and chin growth (see Fig. 35-54)
Jasper JumperThe popular Jasper Jumper is a modification of the Herbst appli-ance just described. The interarch flexible force module of the Jasper Jumper allows the patient greater freedom of movement (Fig. 35-55). As with the Pancherz version of the Herbst appli-ance, the Jasper Jumper resorts to pushing forces, in contrast to conventional intermaxillary elastics (Figs. 35-56 to 35-59). Repetitive forward posturing is the key element. Metabolism, again, is stimulated to provide the achievable optimum result.
McNamara41 notes that the treatment response of the Jas-per Jumper is almost equally divided between basal and den-tal effects.10 On average, a 2-mm increase in mandibular length occurs. Little maxillary skeletal change has been noted. As with all functional appliances, the potential for modifica-tion of the fossa in position and morphologic structure exists
in the growing individual. One must analyze this using reli-able three-dimensional landmarks rather than conventional two-dimensional radiographic, cephalometrically constructed measure points and line and angular reconstructions (cephalo-metric tracings).140,184–186
According to McNamara,116 the most pronounced dentoal-veolar change with the Jasper Jumper and similar appliances, is a relative posterior movement of the maxillary buccal seg-ments of approximately 2.5 mm. Proclination of the lower incisors is also reported, as with the conventional Herbst appliance.*
As with the Pancherz version of the Herbst appliance, the Jasper Jumper has the advantage of a shorter active treatment time, which is a double-edged sword because less time is avail-able to harness growth increments. Patient compliance needs are minimal. The appliance is less rigid than the classic Herbst device and uses a flexible pushing device, also enlisting the buc-cinator mechanism (buccal muscle forces) (see Figs. 35-55 to 35-59). In addition to sagittal forces, the Jasper Jumper has a transverse expansion vector acting on the maxillary molars, which must be watched. A transpalatal arch counteracts unwanted buccal malposition of the upper first molars. The use of a lower lingual arch enhances mandibular anchorage (see Fig. 35-59).10,152,184
Most of the Pancherz team’s observations concerning the conventional Herbst appliance apply to the Jasper Jumper, although some clinicians believe that the magnitude of change is less with the Jasper Jumper. John DeVincenzo has designed several fixed functional appliance modifications that could be used, including his own effective Eureka Spring. DeVin-cenzo69,143 attributes the bulk of change to dentoalveolar com-pensation, with minimal skeletal reaction.
Detailed treatment adjustments are presented in Chapter 17 of Dentofacial Orthopedics with Functional Appliances, 2nd ed., by Graber and associates.10 The reader is strongly advised to read Part 2 of that chapter on asymmetric dentofacial ortho-pedics. A significant number of Class II malocclusions are not bilateral mirror images. Barry Mollenhauer’s discussion applies not only to the Jasper Jumper but also to all fixed functional appliance modifications.10,63,184,188
* References 25, 140, 154, 184, 187–189.
FIGURE 35-55 Jasper Jumper essentials. The distal end of the force module is attached to the maxillary dental arch by means of a ball pin and double molar tubes. The appliance can be acti-vated by anteriorly moving the ball pin. The alignment of the spring within the jumper mechanism is shown in the inset.
A BFIGURE 35-56 Outriggers (auxiliary arch wires) are used to anchor the force module. A, The rect-angular auxiliary wire is anteriorly looped over the main archwire and is posteriorly cinched back through the auxiliary tube. B, A ball pin is inserted through the distal hole of the jumper module, anteriorly placed through the face-bow tube on the upper first molar band, and cinched forward to activate the module.
997.e91CHAPTER 35 Functional Appliances
FIGURE 35-57 The force module is used in a patient with mixed dentition. In this instance, a bayonet bend is distally placed to the canine, and a Lexan ball anteriorly acts as a stop for the force module. In this example, the upper and lower rectangular utility arches connect the anterior and posterior teeth.
FIGURE 35-58 Maximal anchorage is set up for the force mod-ule. The maxillary and mandibular archwires extend to the sec-ond molars and are posteriorly cinched back. Tiebacks can also be used. The offset bend in the main archwire (see Fig. 35-59) is obscured by the Lexan ball.
A BFIGURE 35-59 A, The transpalatal arch, combined with fixed appliances, is used to enhance maxillary anchorage. B, A lower lingual arch, combined with fixed appliances, enhances mandib-ular anchorage.
997.e92 CHAPTER 35 Functional Appliances
S U M M A R YThe author of this chapter hopes that this overview of the biologic approach—enlisting the patient’s own muscles, function, growth pattern, optimal metabolic stimulation, and compliance—will excite the reader enough to stimulate, the reading of the accompanying list of references. Func-tional appliances do not replace fixed attachments. Indeed,
the combined use of brackets, bands, and extraoral force has the potential for the best possible and most stable long-term results. Treatment timing and length of treatment are important considerations for growth guidance as orthopedic surgeons show. The ultimate goal of all orthodontists is to be applied biologists.
REFERENCES 1. Graber TM, Chung DB, Aoba TJ. Dentofacial orthopedics versus ortho-
dontics. J Am Dent Assoc. 1967;75:1145–1166. 2. Wolff J. Gesetz der Transformation der Knochen. Berlin: Hirschwold; 1892. 3. Roux W. Gessamelte Abhandlungen über Entwicklungsmechanik der Or-
ganismen. Leipzig: W. Engelmann; 1895. 4. Graber TM. The unique nature of temporomandibular joint metabolism:
the clinical implications. In: Rabie AM, Urist MR, eds. Bone Formation and Repair. Amsterdam: Elsevier; 1997:143–157.
5. Pilon JJGM. Orthodontic Forces and Tooth Movement, Doctoral disserta-tion. Nijmegen, Netherlands: University of Nijmegen; 1996.
6. Sfondrini G, Reggiani C, Gandini P, et al. Adaptations of masticatory muscles to a hyperpropulsive appliance in the rat. Am J Orthod Dentofa-cial Orthop. 1996;110:612–617.
7. Robin P. Observation sur un nouvel appareil de redressement. Rev Stomatol. 1902;9:423–432.
8. Kingsley NW. Oral Deformities. New York: Appleton & Son; 1880. 9. Case C. Open bite malocclusion. Dent Rev. 1984;6:124. 10. Graber TM, Rakosi T, Petrovic AG, eds. Dentofacial Orthopedics with
Functional Appliances. 2nd ed. St. Louis: Mosby; 1997. 11. Lischer BE. Principles and Methods of Orthodontics. Philadelphia: Lea &
Febiger; 1912. 12. Angle EH. The Treatment of Malocclusion of the Teeth. 7th ed. Philadel-
phia: S. S. White Manufacturing; 1907. 13. Andresen V. Beitrag zur retention. Z Zahnartzl Orthop. 1910;3:121. 14. Andresen V. Über das sogenannte “Norwegische system der funk-
tions-kieferorthopädie.” Dtsch Zahnartzl Wochenschr. 1936;39:235. 15. Andresen V, Häupl K. Funktionskieferorthopädie: die Grundlagen des “Nor-
wegischen Systems.” 2nd ed. Leipzig, Germany: Hermann Meusser; 1936. 16. Andresen V, Häupl K, Petrik L. Funktionskieferorthopädie. 6th ed.
Munich, Germany: Johann Ambrosium Barth Publishing; 1957. 17. Ahlgren J, Bendéus M. Changes in length and torque of masticatory mus-
cles produced by the activator appliance. A cephalometric study. Swed Dent J Suppl. 1982;15:27–35.
18. Baccetti T, Franchi L, McNamara Jr JA, Tollaro I. Early dentofacial features of Class II malocclusion: a longitudinal study from the deciduous through the mixed dentition. Am J Orthod Dentofacial Orthop. 1997;111:502–509.
19. Ballard CF. A consideration of the physiological background of mandib-ular posture and movement. Dent Pract. 1955;6:80–89.
20. Barton S, Cook PA. Predicting functional appliance treatment outcome in Class II malocclusions—a review. Am J Orthod Dentofacial Orthop. 1997;112:282–286.
22. Björk A. The principle of the Andresen method of orthodontic treatment: a discussion based on cephalometric x-ray analysis of treated cases. Am J Orthod. 1951;37:437–458.
23. Brieden CM, Pangrazio-Kulbersh V, Kulbersh R. Maxillary skeletal and dental changes with Fränkel appliance therapy—an implant study. Angle Orthod. 1984;54:226–232.
24. Buschang PH, Santos-Pinto A. Condylar growth and glenoid fossa dis-placement during childhood and adolescence. Am J Orthod Dentofacial Orthop. 1998;113:437–442.
25. Cash RG. Adult nonextraction treatment with a Jasper Jumper. J Clin Orthod. 1991;25:43–47.
26. DeVincenzo JP, Winn MW. Orthopedic and orthodontic effects from the use of a functional appliance with different amounts of protrusive activation. Am J Orthod Dentofacial Orthop. 1989;96:181–190.
27. Du X, Hägg U, Rabie B. Effects of headgear Herbst and mandibular step-by-step advancement versus conventional Herbst appliance and maximum jumping of the mandible. Eur J Orthod. 2002;24:167–174.
29. Graber TM, ed. Physiological Principles of Functional Appliances. St. Louis: Mosby; 1985.
30. Graber TM. The neuromuscular system and its significance for clinical orthodontics. Eur J Orthod. 1998;20:470.
31. Hansen K, Pancherz H. Long-term effects of Herbst treatment in relation to normal growth and development: a cephalometric study. Eur J Orthod. 1992;14:285–295.
32. Ikai A, Sugisaki M, Young-Sung K, Tanabe H. Morphologic study of the mandibular fossa and the eminence of the temporomandibular joint in relation to facial structures. Am J Orthod Dentofacial Orthop. 1997;112:634–638.
33. Kalra V, Burstone CJ, Nanda R. Effects of a fixed magnetic appliance on the dentofacial complex. Am J Orthod Dentofacial Orthop. 1989;95:467–478.
34. Kantomaa T, Pirttiniemi P. Changes in proteoglycan and collagen content in the mandibular condylar cartilage of the rabbit caused by an altered relation-ship between the condyle and glenoid fossa. Eur J Orthod. 1998;20:435–441.
35. Komposch G, Hockenjos C. Die Reaktionsfahrigkeit des temporoman-dibularen Knörpels. Fortschr Kieferorthop. 1977;28:121–132.
36. Lange DW, Kalra V, Broadbent Jr BH, et al. Changes in soft tissue profile following treatment with the Bionator. Angle Orthod. 1995;65:423–430.
37. Lund DI, Sandler PJ. The effects of Twin Blocks: a prospective controlled study. Am J Orthod Dentofacial Orthop. 1998;113:104–110.
38. Mamandras AH, Allen LP. Mandibular response to orthodontic treat-ment with the Bionator appliance. Am J Orthod Dentofacial Orthop. 1990;97:113–120.
39. McDougall PD, McNamara JA. Arch width development in Class II patients with the Fränkel appliance. Am J Orthod. 1982;82:10–22.
40. McNamara Jr JA. Functional adaptations in the temporomandibular joint. Dent Clin North Am. 1975;19:457–471.
41. McNamara Jr JA. Temporomandibular Joint Adaptation to Functional Protrusion. Paper presented at the one hundred third annual session of the American Association of Orthodontists. Honolulu: Hawaii; May 6, 2003.
42. McNamara Jr JA, Bookstein FL, Shaughnessy TG. Skeletal and dental changes following functional regulator therapy on Class II patients. Am J Orthod. 1985;88:91–110.
43. McNamara Jr JA, Hinton RJ, Hoffman DL. Histologic analysis of tem-poromandibular joint adaptations to protrusive function in young adult rhesus monkeys. Am J Orthod. 1982;82:288–298.
44. Mills CM, McCulloch KJ. Treatment effects of the twin block appliance. Am J Orthod Dentofacial Orthop. 1998;114:15–24.
45. Obijou C, Pancherz H. Herbst appliance treatment of Class II, Division 2 malocclusions. Am J Orthod Dentofacial Orthop. 1997;112:287–291.
46. Pancherz H. The effect of continuous bite jumping on the dentofacial complex: a follow-up study after Herbst appliance treatment of Class II malocclusion. Eur J Orthod. 1981;3:49–60.
47. Pancherz H. The effects, limitations, and long-term dentofacial adapta-tions to treatment with the Herbst appliance. Semin Orthod. 1997;3: 232–243.
48. Pancherz H, Fischer S. Amount and direction of temporomandibular joint growth changes in Herbst treatment: a cephalometric long-term investigation. Angle Orthod. 2003;73:493–501.
49. Paulsen HU. Morphological changes of the TMJ condyles of 100 patients treated with the Herbst appliance in the period of puberty to adulthood: a long-term radiographic study. Eur J Orthod. 1997;19:657–668.
50. Paulsen HU, Rabøl A, Sørensen SS. Bone scintigraphy of the human temporomandibular joints during Herbst treatment. Eur J Orthod. 1998;20:369–374.
51. Pirttiniemi P, Kantornaa T, Poikela A, Pietila K. Electrical masseter muscle stimulation alters condylar shape. Eur J Orthod. 1998;20:478–479.
52. Rakosi T. The activator. In: Graber TM, Rakosi T, Petrovic A, eds. Den-tofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997:19–67.
53. Ruf S, Pancherz H. The mechanism of Class II correction during Herbst therapy in relation to the vertical jaw base relationship: a cephalometric roentgenographic study. Angle Orthod. 1997;67:271–276.
54. Ruf S, Pancherz H. Temporomandibular joint growth adaptation in Herbst treatment: a prospective magnetic resonance imaging and cepha-lometric roentgenographic study. Eur J Orthod. 1998;20:375–388.
55. Sander FG. The effects of appliances and Class II elastics on masticato-ry patterns. In: McNamara Jr JA, Ribbens KA, Howe RP, eds. Clinical Alteration of the Growing Face. Monograph 14, Craniofacial Growth Series. Center for Human Growth and Development. Ann Arbor, MI: University of Michigan; 1983:155–178.
56. Sectakof PA. The Effects of Functional Appliances on Functional Activities of Jaw Muscles in Macaca Fascicularis. Master’s thesis. Toronto: University of Toronto; 1992.
57. Stromeyer EL, Caruso JM, DeVincenzo JP. A cephalometric study of the Class II correction effects of the Eureka Spring. Angle Orthod. 2002;72(3):203–210.
58. Tallgren A, Christiansen RL, Ash Jr M, Miller RL. Effects of a myo-functional appliance on orofacial muscle activity and structures. Angle Orthod. 1998;68:249–258.
59. Thilander B, Filipsson R. Muscle activity related to activator and inter-maxillary traction in angle Class II Division 1 malocclusions. An electro-myographic study of the temporal, masseter, and suprahyoid muscles. Acta Odontol Scand. 1966;24:241–257.
60. Vardimon AD, Fricke J, Spack N, et al. Principles and cephalometric assess-ment of functional magnetic correction. Eur J Orthod. 1998;20:483–484.
61. Watted N, Witt E, Koch R, Kenn W. A nuclear magnetic resonance study of the temporomandibular joint changes following functional orthopaedic treatment using the Würzburg approach. Eur J Orthod. 1998;20:484–485.
62. Wieslander L. Long-term effect of treatment with the headgear-Herbst appliance in the early mixed dentition. Stability or relapse? Am J Orthod Dentofacial Orthop. 1993;104:319–329.
63. Yamin-Lacouture C, Woodside DG, Sectakof PA, Sessie BJ. The action of three types of functional appliances on the activity of the masticatory muscles. Am J Orthod Dentofacial Orthop. 1997;112:560–572.
64. Graber TM. The clinical implications of the unique metabolic processes in the human temporomandibular joint. In: Sachdeva RC, Hans-Peter Bantleon, Larry White, Jeff Johnson, et al., ed. Orthodontics for the Next Millennium. Ormco; 1997.
65. Graber TM. Nobel Prize Research and its Impact on Growth Guidance and TMJ Metabolism. Paper presented at the one hundred third annual session of the American Association of Orthodontists; May 6, 2003. Honolulu, Hawaii.
66. Birkebaek L, Melsen B, Terp S. A laminagraphic study of the alterations in the temporo-mandibular joint following activator treatment. Eur J Orthod. 1984;6:257–266.
67. Braun S, Kittelson R, Kim K. The G-axis: a growth vector for the mandi-ble. Angle Orthod. 2004;74:328–331.
68. Chen JY, Will LA, Neiderman R. Analysis of efficacy of functional appliances on mandibular growth. Am J Orthod Dentofacial Orthop. 2002;122:470–476.
69. Decrue A, Wieslander L. Fossa articularis changes using Herbst appliance after mandibular advancement. [Article in German]. Zahnarztl Prax. 1990;41:360–362, 364–365.
70. Droel R, Isaacson RJ. Some relationships between glenoid fossa position and various skeletal discrepancies. Am J Orthod. 1972;61:64–78.
71. el-Bialy T, el-Moneim Zaki A, Evans CA. Effects of ultrasound on rabbit mandibular incisor formation and eruption after mandibular osteodis-traction. Am J Orthod Dentofacial Orthop. 2003;124:427–434.
72. Garattini G, Levrini L, Crozzoli P, Levrini A. Skeletal and dental modifi-cations produced by the Bionator III appliance. Am J Orthod Dentofacial Orthop. 1998;114:40–44.
73. Paulsen HU. Personal communication; Feb 2004. 74. Popowich K, Nebbe B, Major PW. Effect of Herbst treatment on tem-
poromandibular joint morphology: a systematic literature review. Am J Orthod Dentofacial Orthop. 2003;123:388–394.
75. Rabie AB, She TT, Hägg U. Functional appliance therapy acceler-ates and enhances condylar growth. Am J Orthod Dentofacial Orthop. 2003;123:40–48.
76. Vardimon AD, Köklü S, Iseri H, et al. An assessment of skeletal and dental responses to the functional magnetic system (FMS). Am J Orthod Dentofacial Orthop. 2001;120:416–426.
77. Katsavrias EG, Voudouris JC. The treatment effect of mandibular protru-sive appliances on the glenoid fossa for Class II correction. Angle Orthod. 2004;74:79–85.
78. Voudouris JC, Woodside DG, Altuna G, et al. Condyle-fossa modifica-tions and muscle interactions during Herbst treatment, part 1. New tech-nological methods. Am J Orthod Dentofacial Orthop. 2003;123:604–613.
79. Voudouris JC, Woodside DG, Altuna G, et al. Condyle-fossa modifica-tion and muscle interactions during Herbst treatment, part 2. Results and conclusions. Am J Orthod Dentofacial Orthop. 2003;124:13–29.
81. Woodside DG, Metaxas A, Altuna G. The influence of functional appliance therapy on glenoid fossa remodeling. Am J Orthod Dentofacial Orthop. 1987;92:181–198.
82. Xiong H, Hägg U, Tang GH, et al. The effect of continuous bite jumping in adult rats: a morphological study. Angle Orthod. 2004;74:86–92.
83. Hotz R. Orthodontics in Daily Practice. Bern, Switzerland: Hans Huber Publishers; 1974.
84. Igarashi K, Miyoshi K, Shinoda H, et al. Diurnal variation in tooth move-ment in response to orthodontic force in rats. Am J Orthod Dentofacial Orthop. 1998;114:8–14.
85. Korkhaus G. Die Auswertung des Fernröntgenbildes in der Kieferortho-pädie. Dtsch Zahn Mund Kieferheilkd. 1936;3:715.
86. Petrovic AG, Oudet CL, Stutzmann JJ. Temporal organization of rat and human skeletal cells: circadian frequency and organizement of cell generation time. In: Edmunds L, ed. Cell Cycle Clocks. New York: Marcel Dekker, Inc.; 1984:325–349.
87. Selmer-Olsen R. En kritisk bertrakning over “Der Norsk System.” Nor Tannlaegeforen Tid. 1937;47:85–91.
88. Woodside DG. Do functional appliances have an orthopedic effect? Am J Orthod Dentofacial Orthop. 1998;113:11–14.
89. Ryan MJ, Schneider BJ, BeGole EA, Muhi ZF. Opening rotations of the mandible during and after treatment. Am J Orthod Dentofacial Orthop. 1998;114:142–149.
90. Johnston LE. Personal communication on unloading the condyle. Sept. 1998.
91. Slagsvold O, Kolstad I. Class II Division 1 Malocclusion Treated with Activators: A Study of Posttreatment Stability. Unpublished. 1978.
92. Grude R. Myo-functional therapy: a review of various cases some years after their treatment by the Norwegian system had been completed. Nor Tanlaegeforen Tid. 1952;62:1–7.
93. Fränkel R. Technik und Handhabung der Funktionsregler. Berlin: VEB Verlag Volk & Gesundheit; 1973.
94. Harvold EP. The Activator in Interceptive Orthodontics. St. Louis: Mosby; 1974.
95. Herren P. The activator’s mode of action. Am J Orthod. 1959;45(7):512–527. 96. Schmuth GPF. Consideration of Functional Aspects in Dentofacial Or-
thopedics and Orthodontics. Sheldon Friel Memorial Lecture. Presented at the 94th European Orthodontic Congress in Mainz, Germany, June 1998. Am J Orthod Dentofacial Orthop. 1999;116(4):373–381.
97. Huggare JA, Laine-Alava MT. Nasorespiratory function and head pos-ture. Am J Orthod Dentofacial Orthop. 1997;112:507–511.
997.e94 CHAPTER 35 Functional Appliances
98. Ono T, Ishiwata Y, Kuroda T. Inhibition of masseteric electromyo-graphic activity during oral respiration. Am J Orthod Dentofacial Orthop. 1998;113:518–525.
99. Ozbek MM, Memikoglu TU, Gögen H, et al. Oropharyngeal airway di-mensions and functional-orthopedic treatment in skeletal Class II cases. Angle Orthod. 1998;68:327–336.
100. Altenburger E, Ingervall B. The initial effects of treatment of Class II, Division 1 malocclusions with the van Beek activator compared with the effects of the Herren activator and an activator-headgear combination. Eur J Orthod. 1998;20:389–397.
101. Clark GT, Arand D, Chung E, Tong D. Effect of anterior mandibular positioning on obstructive sleep apnea. Am Rev Respir Dis. 1993;147: 624–629.
102. Scholle HC, Schurmann NP, Kopp S. Selective masseter and temporal muscle activation depending on the morphofunctional situation in the orofacial region. Eur J Orthod. 1998;20:482.
103. Tourne L, Schweiger J. Immediate postural response to total nasal ob-struction. Am J Orthod Dentofacial Orthop. 1996;110:606–611.
104. Vig KD. Nasal obstruction and facial growth: the strength of evidence for clinical assumptions. Am J Orthod Dentofacial Orthop. 1998;113:603–611.
105. Yamada T, Tanne K, Miyamoto K, Yamauchi K. Influence of nasal respiratory obstruction on craniofacial growth in young Macaca fuscata monkeys. Am J Orthod Dentofacial Orthop. 1997;111:38–43.
106. Cevidanes L, Franco AA, Scanavini A, et al. Clinical outcomes of Fränkel appliance therapy assessed with a counterpart analysis. Am J Orthod Dentofacial Orthop. 2003;123:379–387.
107. Pancherz H. Treatment of class II malocclusions by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod. 1979;76:423–442.
108. Pancherz H. The modern Herbst appliance. In: Graber TM, Rakosi T, Petrovic A, eds. Dentofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997:336–366.
109. Bishara S. Mandibular changes in persons with untreated and treated Class II, Division 1 malocclusion. Am J Orthod Dentofacial Orthop. 1998;113:661–673.
110. Bishara S, Zaher AR, Cummins DM, Jakobsen JR. Effects of orthodontic treatment on the growth of individuals with Class II, Division 1 maloc-clusion. Angle Orthod. 1994;64:221–230.
111. Björk A, Palling M. Adolescent age changes in sagittal jaw relations, alveolar prognathy, and incisal inclination. Acta Odontol Scand. 1955;12:201–232.
112. Gianelly A, Brosnan P, Martignoni M, Bernstein L. Mandibular growth, condyle position, and Fränkel appliance therapy. Angle Orthod. 1983;53:131–142.
113. Hamilton D. Early treatment: the emancipation of dentofacial orthope-dics. In: Graber TM, Rakosi T, Petrovic A, eds. Dentofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997.
114. Konik M, Pancherz H, Hansen K. The mechanism of Class II correction in late Herbst treatment. Am J Orthod Dentofacial Orthop. 1997;112:87–91.
115. Kusumoto K, Sato A, Mitani H. The evaluation of the orthopedic appliances by using standard growth curves of maxilla and mandible. J Jpn Orthod Soc. 1996;55(4):311–321.
116. Lundström A. Malocclusion of the Teeth as Regarded as a Problem with the Apical Base. Doctoral dissertation. Stockholm: Karolinska University; 1923.
117. Melanson E, Van Dyken C. Studies in Condylar Growth. Master’s thesis. Ann Arbor, MI: University of Michigan; 1972.
118. Graber TM. The anatomical and physiological aspects in the treatment of temporomandibular joint disorders. Fortschr Kieferorthop. 1991;52: 126–132.
119. Haralabakis NB, Halazonetics DJ, Sifakakis IB. Activator versus cervical headgear: superimposed cephalometric comparison. Am J Orthod Dento-facial Orthop. 2003;123:296–305.
120. Graber TM. The Effect of Buccal Shields on the Maxillary Dental Arch Width in the Squirrel Monkey (Saimiri Sciureus). Paper presented at the eighty-third annual session of the American Association of Orthodon-tists. Boston: May 4–10, 1983.
121. Graber TM. Experimental and Clinical Studies of the Effect of the Fränkel FR Appliance in Primates and Humans. Annual meeting of the American Association of Orthodontists. Boston: May 4–10, 1983.
122. Graber TM. Combined extraoral and functional appliances. In: Graber TM, Rakosi T, Petrovic A, eds. Dentofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997.
123. Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Clin Orthod. 1983;17:266–269.
124. Ricketts RM. Orthopedics in the Eyes of the Clinician. Symposium on Clin-ical and Bioengineering Aspects of Dentofacial Orthopedics. Farmington, CT: University of Connecticut; 1981.
125. Enlow DH. Growth and the problem of local control mechanism. Am J Anat. 1973;136(4):403–405.
126. Clark WJ. Twin Block Functional Therapy: Applications in Dentofacial Orthopaedics. 2nd ed. London: Mosby; 2002.
127. Coelho Filho CM. The mandibular protraction appliance no 3. J Clin Orthod. 1998;32:379–384.
128. Dischinger T. Edgewise Herbst appliance. J Clin Orthod. 1995;29:738–742. 129. Ghafari J, Shofer FS, Jacobsson-Hunt U, et al. Headgear versus function
regulator in early treatment of Class II Division 1 malocclusion: a ran-domized clinical trial. Am J Orthod Dentofacial Orthop. 1998;113:51–61.
130. Eschler J. Die Kieferdehnung mit funktionskieferorthopädischen Ap-paraten: der Funktionator. Zahnarztl Welt. 1962;63:203.
131. Schwarz AM. The effects of the activator. Fortschr Kieferorthop. 1952;13:117–138.
132. Baume LJ, Derichsweiler H. Is the condylar growth center responsive to orthodontic therapy? An experimental study in Macaca mulatta. Oral Surg Oral Med Oral Pathol. 1961;14:347–362.
133. Charlier JP, Petrovic A, Hermann-Stutzmann J. Effects of mandibular hyperpropulsion on the prechondroblastic zone of young rat condyle. Am J Orthod. 1969;55:71–74.
134. McNamara Jr JA, Huge SA. The functional regulator (FR-3) of Fränkel. Am J Orthod. 1985;88:409–424.
136. Tulloch JF, Phillips C, Koch G, Proffit WR. The effect of early interven-tion on skeletal pattern in Class II malocclusion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997;111:391–400.
137. Burkhardt DR, McNamara Jr JA, Baccetti T. Maxillary molar distalization or mandibular advancement: a cephalometric comparison of compre-hensive orthodontic treatment including the pendulum and the Herbst appliances. Am J Orthod Dentofacial Orthop. 2003;123:108–116.
138. Enlow DH, DiGangi D, McNamara Jr JA, Mina M. An evaluation of the morphogenic and anatomic effects of the functional regulator utilizing the counterpart analysis. Eur J Orthod. 1988;10:192–202.
139. Isberg A, Isacsson G. Tissue reactions associated with internal derangement of the temporomandibular joint. Acta Odontol Scand. 1986;44:160–164.
140. Jasper JJ, McNamara Jr JA. The correction of interarch malocclusions using a fixed force module. Am J Orthod Dentofacial Orthop. 1995;108: 641–650.
141. Balters W. Eine Einführung in die Bionatorheilmethode: ausgewählte Schriften und Vorträge. Heidelberg, Germany: C Hermann; 1972.
142. Moss ML. The functional matrix hypothesis revisited.1. The role of mechanotransduction. Am J Orthod Dentofacial Orthop. 1997;112:8–11.
143. DeVincenzo J. The Eureka Spring: a new interarch force delivery system. J Clin Orthod. 1997;31:454–467.
144. Eirew HL, McDowell F, Phillips JG. The Fräenkel appliance—avoidance of lower incisor proclination. Br J Orthod. 1981;8:189–191.
145. Fleischer E, Fleischer A. Bionator modification: the Bio-M-S therapy. In: Graber TM, Neumann B, eds. Removable Orthodontic Appliances. 2nd ed. Philadelphia: W.B. Saunders; 1984:387–409.
146. Miyamoto K, Yamada K, Ishizuka Y, et al. Masseter muscle activity during the whole day in young adults. Am J Orthod Dentofacial Orthop. 1996;110:394–398.
147. Tulloch JF, Phillips C, Proffit WR. Benefit of early Class II treatment: progress report of a two-phase randomized clinical trial. Am J Orthod Dentofacial Orthop. 1998;113:62–72.
148. Rakosi T, Jonas I, Graber TM. Orthodontic Diagnosis (Color Atlas of Dental Medicine. Berlin: Thieme; 1993.
149. Rabie AB, Wong L, Hägg U. Correlation of replicating cells and osteo-genesis in the glenoid fossa during stepwise advancement. Am J Orthod Dentofacial Orthop. 2003;123:521–526.
997.e95CHAPTER 35 Functional Appliances
150. Rabie AB, Wong L, Tsai M. Replicating mesenchymal cells in the condyle and the glenoid fossa during mandibular forward positioning. Am J Orth-od Dentofacial Orthop. 2003;123:49–57.
151. McNamara JA. Fabrication of the acrylic splint Herbst appliance. Am J Orthod Dentofacial Orthop. 1988;94:10–18.
152. Moffett BC. A research perspective on craniofacial morphogenesis. Acta Morphol Neerl Scand. 1972;10:91–101.
153. Graber TM. The Fränkel function regulator. In: Graber TM, Rakosi T, Petrovic A, eds. Dentofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997:219–274.
154. Cope JB, Buschang Ph, Cope DD, et al. Quantitative evaluation of cranio-facial changes with Jasper Jumper therapy. Angle Orthod. 1994;64:113–122.
155. Creekmore TD, Radney LJ. Fränkel appliance therapy: orthopedic or orthodontic? Am J Orthod. 1983;83:89–108.
157. Clark WJ. The twin-block technique. In: Graber TM, Rakosi T, Petrovic AG, eds. Dentofacial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997:268–298.
158. Bondevik O. Treatment needs following activator-headgear therapy. Angle Orthod. 1995;65:417–422.
159. Vardimon K, Köklü A, Iseri H, Shpack N, Fricke J, Mete L. An assessment of skeletal and dental responses to the functional magnetic system (FMS). Am J Orthod Dentofacial Orthop. 2001;120(4):416–426.
160. Moss JP. Personal communication; Oct. 21, 1999. 161. O’Brien K, Wright J, Conboy F, et al. Effectiveness of early orthodontic
treatment with the twin-block appliance: a multicenter, randomized, controlled trial. Part I. Dental and skeletal effects. Am J Orthod Dentofa-cial Orthop. 2003;124:234–243.
162. O’Brien K, Wright J, Conboy F, et al. Effectiveness of treatment of Class II malocclusion with the Herbst or twin-block appliances: a randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2003;124:128–137.
163. Blechman AM. Magnetic force systems in orthodontics. Clinical results of a pilot study. Am J Orthod. 1985;87:201–210.
164. Blechman AM, Steger ER. A possible mechanism of action of repelling, molar distalizing magnets. Part I. Am J Orthod Dentofacial Orthop. 1995;108:428–431.
165. Bondemark L, Kurol J. Distalization of maxillary first and second molars simultaneously with repelling magnets. Eur J Orthod. 1992;14:264–272.
166. Darendeliler MA, Sinclair PM, Kusy RP. The effects of samarium-cobalt magnets and pulsed electromagnetic fields on tooth movement. Am J Orthod Dentofacial Orthop. 1995;107:578–588.
167. Darendeliler MA, Joho JP. Magnetic activator device II (MAD II) for correction of Class II, Division 1 malocclusions. Am J Orthod Dentofacial Orthop. 1993;103:223–229.
168. Blechman AM. Pain-free and mobility-free orthodontics? Am J Orthod Dentofacial Orthop. 1998;113:379–383.
169. Golyakhovsky V. Local and Continuous Exposure to a Permanent Magnetic Field as a Means of Boosting Reparative Osteogenesis. Proceedings of the Kubyshev Regular Conference on Magnetic Fields. Kubyshev, USSR: June 1976 (as translated from Russian by AM Blechman in Blechman AM. Pain-free and mobility-free orthodontics? Am J Orthod Dentofacial Orthop. 1998;113:379–383).
170. Vardimon AD, Graber TM, Drescher D, Bourauel C. Rare earth magnets and impaction. Am J Orthod Dentofacial Orthop. 1991;100(6):494–512.
171. Bondevik O. How effective is the combined activator-headgear treat-ment? Eur J Orthod. 1991;13:482–485.
172. Coben SE. The spheno-occipital synchondrosis: the missing link between the profession’s concept of craniofacial growth and orthodontic treat-ment. Am J Orthod Dentofacial Orthop. 1998;114:709–712.
173. Stöckli PW, Teuscher UM. Combined activator headgear orthopedics. In: Graber TM, Vanarsdall RL, eds. Orthodontics: Current Principles and Technique. 2nd ed. St. Louis: Mosby; 1994:437–506.
174. Tanne K, Matsubara S, Sakuda M. Stress distribution in the max-illary complex from orthopedic-headgear forces. Angle Orthod. 1993;63:111–118.
175. Battagel JM. The relationship between hard and soft tissue changes fol-lowing treatment of Class II, Division 1 malocclusion using Edgewise and Fränkel appliance techniques. Eur J Orthod. 1990;12:154–165.
176. Braun S, Johnson B, Hnat WP, Gomez JA. Evaluation of the ver-tical forces generated by cervical biteplate facebow. Angle Orthod. 1993;63:119–126.
177. Dugoni SA, Lee JS, Varela J, Dugoni AA. Early mixed dentition treat-ment: postretention evaluation of stability and relapse. Angle Orthod. 1995;65:311–320.
178. Keeling SD, Wheeler TT, King GJ, et al. Anteroposterior skeletal and dental changes after early Class II treatment with Bionators and headgear. Am J Orthod Dentofacial Orthop. 1998;113:40–50.
179. Herbst E. Atlas und Grundriss der Zahnärtzlichen Orthopädie. Munich, Germany: JF Lehmann Verlag; 1910.
180. Herbst E. Dreissigjahrige erfahrungen mit demretentionscharnier. Zahnartzl Rundsch. 1934;43:1515–1524.
181. West RP. The adjustable bite corrector. J Clin Orthod. 1995;29:650–657. 182. Greenfield RL. Fixed piston appliance for rapid Class II correction. J Clin
Orthod. 1995;29:174–183. 183. Coelho Filho CM. Clinical applications of the mandibular protraction
appliance. J Clin Orthod. 1997;31:92–102. 184. Jasper JJ, McNamara JA, Mollenhauer B. The modified Herbst appliance
(Jasper Jumper). In: Graber TM, Rakosi T, Petrovic A, eds. Dentofa-cial Orthopedics with Functional Appliances. 2nd ed. St. Louis: Mosby; 1997:367.
185. Weiland FJ, Bantleon HP. Treatment of Class II malocclusions with the Jasper Jumper appliance—a preliminary report. Am J Orthod Dentofacial Orthop. 1995;108:341–350.
186. Weiland FJ, Ingervall B, Bantleon HP, Droacht H. Initial effects of treat-ment of Class II malocclusion with the Herren activator, activator-head-gear combination, and Jasper Jumper. Am J Orthod Dentofacial Orthop. 1997;112:19–27.
187. Blackwood 3rd HO. Clinical management of the Jasper Jumper. J Clin Orthod. 1991;25:755–760.
188. Erdogan E, Erdogan E. Asymmetric application of the Jasper Jumper in the correction of midline discrepancies. J Clin Orthod. 1998;32:170–180.
Treatment of the Face with Biocompatible OrthodonticsDwight Damon
THE DAMON SYSTEM CONCEPTThe philosophy underlying the intended use of the Damon System (Ormco Corporation, Orange, CA) is to approximate biologically induced, tooth-moving forces in each phase of orthodontic treatment. The Damon System achieves this goal by means of a passive, virtually friction-free, self-locking, fixed-appliance conduit that maximizes the full potential of today’s high-tech archwires. By doing so, the Damon System provides a reliable and simple means of achieving the best possible facial balance for each patient through the use of light forces that foster corrective functional adaptation of the arch-form while maximizing patient comfort during treatment. This functional adaptation is similar to the Fränkel effect in its posterior arch-widening results. Traditional treatment plan-ning has long been based on maintaining the original archform for stability. In patients with muscle imbalance and collapsed archforms, tooth mass often had to be eliminated. Exten-sive clinical results indicate that clinicians can now maintain most complete dentitions, even in severely crowded arches, by using very light–force, high-tech archwires in the passive Damon appliance that alter the balance of forces among the lips, tongue, and muscles of the face. This alteration creates
a new force equilibrium that allows the archform to reshape itself to accommodate the teeth; the body, not the clinician, determines where the teeth should be positioned. The author refers to this phenomenon as “physiologically determined” tooth positioning. Computed tomographic (CT) scans taken of patients just debonded and those in retention for longer than 5 years demonstrate that using light forces in a passive tube with a small wire-to-lumen ratio enables teeth to be bodily moved, without excessive tipping, in all planes of space and that alveolar bone will follow. This compelling research calls for a significant shift in thinking and treatment planning, reducing and even eliminating the need for molar distaliza-tion, extractions (excluding those deemed appropriate for bimaxillary protrusive cases), and rapid palatal expansion.
Practicing orthodontist Alan Pollard describes the Damon appliance system as unique in offering “rapid alignment with gentle forces, functional adaptation and accurate, predictable tooth positioning with micro precision.” He continues, “It pro-vides a well-documented means, a virtually friction-free tube, by which the most advanced wire technologies can work to their maximum advantage, an aim most of us have aspired to but have not been able to achieve in conventionally ligated edgewise systems.”1
36
O U T L I N EThe Damon System Concept, 997.e96Early Observations of Damon System Treatment, 997.e97Contemporary Orthodontic Philosophies, 997.e98
Achieve Facial Harmony via Facially Driven Treatment Planning, 997.e98
Use of Nonextraction Therapy Where Possible and Light-Force Mechanics, 997.e113
Force Management, 997.e113Achieving Extremely Light-Force Mechanics: A Passive
Tube, 997.e113A Look at Sliding Mechanics, 997.e114Case for Using Extremely Light Forces in Passive Tubes,
997.e115Computed Tomographic Scans Demonstrate Healthy Bone
Structure after Treatment with the Low-Force Damon Tube System, 997.e118
Case Presentations and Clinical Analyses, 997.e118Treatment with the Herbst Appliance of Growing Patients
with Skeletal Class II Dentition, 997.e144
Clinical Principles for Using the Herbst Appliance, 997.e144
Clinical Application of the Herbst Appliance, 997.e145Damon System Essentials, 997.e160
Damon System Appliance, 997.e160Damon Standard Prescription, 997.e160High-Torque and Low-Torque Alternatives to the Damon
Standard Prescription, 997.e161Damon System Archwires and Archwire Sequencing,
Tieback Usage with the Damon System, 997.e163Using Elastics with the Damon System, 997.e163Lingual Retainer Wire and Splint Retainer, 997.e163
Summary, 997.e165
997.e97CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
Pollard refers to the Damon appliance as a tube. Tube is a useful and accurate geometric description of this passive appliance. The appliance is a tube with tie-wings rather than a bracket and, as such, has a static facial wall when its locking mechanism is closed. To emphasize the important difference between this passive appliance and active self-locking brackets, the Damon bracket appliance is referred to as a tube throughout this discussion.
This chapter presents documentation that substantiates existing clinical findings on patients treated with extremely light forces via the Damon System. Before doing so, the author reviewed the early observations he made in using the system and the two important governing principles (achieving facial harmony and using nonextraction therapy where possible, about which most orthodontists agree today) and their close alignment with Damon System principles. Review of these prin-ciples leads to a systematic discussion of the vascularity of the periodontal ligament and alveolar complex. CT scans of various types of cases demonstrate stable and even improved alveolar bone formation after bodily tooth movement with light forces via the Damon System. Treatment results of a wide range of malocclusions demonstrate the application and versatility of the system. After these presentations, the section, “Damon Sys-tem Essentials,” touches on torque selection, the Damon arch-form and archwire sequencing, interarch elastic configurations, and the use of the retention splint.
EARLY OBSERVATIONS OF DAMON SYSTEM TREATMENTWhen the author first started using this new passive tube technology in the mid-1990s, it became obvious that alve-olar bone, tissue, and teeth responded differently from those treated with conventional high-force mechanics. The follow-ing observations were made from some of the earliest cases treated with the first Damon SL tubes. These observations totally changed the author’s treatment planning and have led to improvements in bracket-tube geometries and materials.
Most of the photographs in this section exhibit much earlier and larger iterations of the Damon tube appliance. 1. The system offers minimal negative impact on the archform
when aligning severely malpositioned teeth. When using conventionally tied appliances and engaging a high upper canine, the expected impact would be for the adjacent lateral incisor and first premolar to intrude or superiorly move with the incisors anteriorly flaring. With this tube technology and low-force, low-friction mechanics, these adverse responses are minimized or eliminated (Fig. 36-1).
2. The appropriate force and wire-to-lumen ratio produces a Fränkel-type, arch-widening effect in the posterior, whereas lower canine width stays approximately the same. The action of the small round archwire (0.014 inch) in the large lumen produces posterior transverse arch-widening that accom-modates most complete dentitions, even in severely crowded arches and without the use of high-force palatal expansion (Fig. 36-2, A and B). Usually minimal change occurs in lower incisor position on the composite head film tracing (Fig. 36-2, C). (The only exception is when the canines are severely positioned anteriorly or lingually to the lateral inci-sors, which is consistent with other types of clinical mechan-ics with or without extractions.) Establishing the appropriate force and wire-to-lumen ratio in the initial phase of treat-ment is critical for the orthodontist. The initial archwire (Ni-Ti Align SE or Damon Copper Ni-Ti (Ormco Corporation, Orange, CA) must not exceed 0.014 inch in diameter and must remain an adequate time to allow its full expression (Fig. 36-3). Moving too quickly or forcing archwire changes through the Ni-Ti Align SE or the Damon Copper Ni-Ti phases may disrupt the adaptation process, totally altering the impact on the face, bone, muscles, and soft tissues.
3. The orbicularis oris and mentalis muscles create a lip bumper effect, which minimizes anterior movement of the incisors. Based on experience with conventional mechan-ics, orthodontists expect to see labial movement of ante-rior teeth when trying to accommodate teeth in a crowded arch without making room for them via extractions. In
A B
FIGURE 36-1 A, B, When bringing a high canine into position, light-force tube technology pro-duces minimal impact on the adjacent teeth and little flaring of the incisors.
997.e98 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
using the tube system, the author noticed that the ante-rior movement of the incisors was minimal, and the lips and muscles of the face become powerful allies with this low-force system. The patient in Figure 36-4, A and B, is an early example of this phenomenon. Because of her flat midface, treating this patient without extractions was essential. With a minimal incisor inclination change, treatment brought a pleasing dental result (Fig. 36-4, C-H). The composite head film shows minimal anterior movement of the incisors (see Fig. 36-4, D). The patient also had excellent tissue and periodontal response (see Fig. 36-4, E) 3½ years in retention.
4. In cases treated with nonextraction, as the arch widens in the posterior, the tongue usually lifts and moves forward, creating a new force equilibrium between it and the lips and muscles of the face. This phenomenon provides the muscles of the face and tongue a second chance to balance themselves and for the archform to continue to reshape itself to accommodate the teeth (Fig. 36-5).
5. In bimaxillary protrusive cases treated through extraction ther-apy, treatment mechanics are greatly simplified with the lip bumper or headgear effect of the facial muscles, thus minimiz-ing the demand on posterior anchorage. The crowded anterior teeth, engaged with an archwire no stronger than 0.014-inch Ni-Ti or Copper Ni-Ti, take the path of least resistance into the extraction site (Fig. 36-6).
CONTEMPORARY ORTHODONTIC PHILOSOPHIESAchieve Facial Harmony via Facially Driven Treatment PlanningMost contemporary clinicians have expanded their primary focus toward creating beautiful and handsome faces, with “put-ting plaster on the table” filling a vital but contributory role. Treatment planning is now concentrated on developing a result that is conducive, rather than detrimental, to long-term matu-ration of the face; that is, treating the 13-year-old patient with the future 50-year-old adult in mind.
A
C
B
FIGURE 36-2 A, B, The action of the small round archwire (0.014 inch) in the large lumen of the Damon System tube appliance produces a Fränkel-type arch-widening effect in the posterior, usually with minimal change in the lower incisor position on the composite head film tracing (C).
997.e99CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
A B
C D
E F
FIGURE 36-3 Lower canine width stays approximately the same if the initial nickel-titanium (Ni-Ti) archwire does not exceed 0.014 inch in size. This early case demonstrates a −1-mm change in canine width, an 8-mm change in first premolar width, and a 5-mm change in first molar width. A, Pretreatment. Canines: 23.5 mm. B, Posttreatment. Canines: 22.5 mm; change: −1 mm. C, Pretreatment. First premolars: 28 mm. D, Posttreatment. First premolars: 36 mm; change: 8 mm. E, Pretreatment. First molars: 36 mm. F, Posttreatment. First molars: 41 mm; change: 5 mm.
997.e100 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
A B
C
E F
G H
D
FIGURE 36-4 The lip bumper effect of the orbicularis oris and mentalis muscles precludes dump-ing of the incisors. A, B, Pretreatment records. C-E, Posttreatment records. F, Pretreatment lower arch. G, Third appointment after 3½ months of treatment. H, Retention record at 3½ years.
997.e101CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
BA
E
F
D
C
IHG
LK
MJ
FIGURE 36-5 In cases treated with nonextraction, as the arch widens in the posterior, the tongue lifts and moves forward, creating a new force equilibrium between it and the lips and muscles of the face. A-E, Pretreatment. F, Tongue responds to the change in the posterior arch width and lifts into new position, often creating a posterior open bite. G-I, Posttreatment. J-M, Results after 4 years and 3 months in retention with no retainer wear for the last 2 years.
997.e102 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
A B
FIGURE 36-6 Bimaxillary protrusive extraction case. Treatment mechanics were greatly sim-plified with the lip bumper or headgear effect of the facial muscles minimizing the demand on posterior anchorage. As the crowded teeth aligned, they took the path of least resistance, which was into the extraction space. A, Pretreatment. B, At 6 months, 2 weeks.
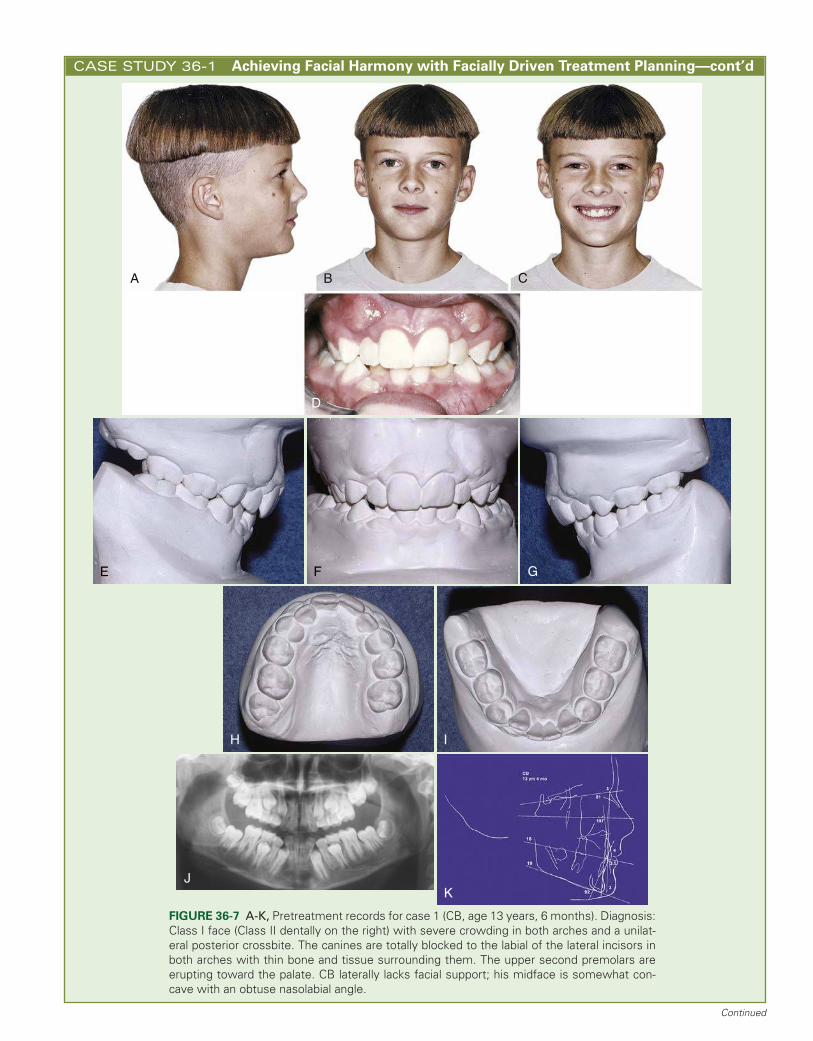
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment PlanningCase 1 (CB) demonstrates a good prospect for this method of treatment planning, which provides expanded options for extremely low-force mechanics. CB exhibits a Class I face (Class II dentally on the right) with severe crowding in both arches and a unilateral posterior crossbite. His canines were totally blocked and had erupted labially to the lateral incisors in both arches with minimal bone and thin labial tissue (Fig. 36-7). The upper second premolars were erupting toward the palate. CB resembles his father, who is tall with a strong nose and chin, so one can assume that his well-proportioned nose and chin buttons will dramatically change as his face matures. He lacks facial support laterally; his midface is some-what concave with an obtuse nasolabial angle. Along with a thinning of the lips, such common facial traits are prevalent in patients with collapsed and crowded dental arches.
The treatment objectives were as follows: 1. Gain maxillary and mandibular arch length to achieve facial balance with
a positive impact on patient profile. 2. Establish upper and lower incisor position to provide lip support. 3. Establish maxillary and mandibular posterior arch width to support mid-
face. 4. Establish ideal maxillary lip-to-tooth relationship. 5. Design treatment mechanics to eliminate the need for high-force rapid
palatal expansion. 6. With low-force mechanics working with the orofacial muscle complex,
bone, and tissue, establish a physiologically determined tooth position.Conventional treatment planning would suggest that four first premo-
lars should be extracted, and early in the author’s career, the extractions would have been done without thinking about the long-term impact on this young man’s profile. The long-term result of many such treatment plans produced flat or dished-in faces. In this case, evaluating where this profile could be at 30 years of age is absolutely critical. Even with extractions, a lower bonded retainer would still have been necessary to maintain lower incisor position over the long term. If lower bonded retainers are required for stability, then why not treat the face using light-force archwires in a passive tube system to gain arch length, especially when one can do so with far less trauma than higher force extraction therapy?
Box 36-1 outlines the treatment sequence of the case. Special torques were selected for this case: +7 degrees for the upper central incisors and +3 degrees for the upper lateral incisors. The torque used on the lower central incisors and lateral incisors was −6 degrees. Before beginning orthodontic treatment, the author prescribed that the patient have his pri-mary second molars extracted. Because of the severe labial position of the canines, extraction was necessary to gain space immediately; con-sequently, the author began treatment in the maxilla with a rectangular
wire (0.014- × 0.025-inch Ni-Ti Align SE) with medium-light Ni-Ti springs activated 1.5 to 2.0 times the width of a bracket (Fig. 36-8). Beginning treatment with a rectangular Ni-Ti wire is not a recommended treatment protocol for Damon System mechanics; but, in this case, the upper ante-rior teeth were well aligned and the canines were rapidly erupting through the cortical plate. The author needed to apply the gentle space-opening mechanism of Ni-Ti coil springs from the four anterior teeth to the molars to gain arch length and transverse arch width, making room for the canines to descend into their normal position. The protocol mandates a 0.014-inch Ni-Ti archwire as the initial archwire; however, because of the interbracket distance and the need to engage a Ni-Ti coil spring, the case required the stability of a rectangular wire. As the space became available, the canines came down naturally and were not bracketed until they were well- positioned in the archform. A mandibular 0.014-inch Ni-Ti Align SE sec-tional archwire was placed in the more crowded lower arch only lateral to lateral incisor because, with a span so great, the archwire would have disengaged had the wire engaged the first molars (Fig. 36-9 to Fig. 36-11; see also Fig. 36-8).
Given the opportunity, this case should have been started long before the canines erupted through the tissue; however, it does provide an excel-lent example of why orthodontists should design treatment mechanics that do not overpower the biologic system. At the beginning of treatment, the canines are labial to the lateral incisors in both arches. With conven-tional mechanics, the challenge is gaining room for them to be included in the arch without negatively affecting the lateral roots. With light-force tube mechanics, the orbicularis oris and mentalis muscles minimize the anterior flaring of the incisors but also encourage the distal positioning of the canines as space is gained in the arch with posterior adaptation. Using this treatment protocol for 8 years, the author has not observed a negative impact on the roots of the lateral incisors.
The Damon System treated this patient to a dentally and facially pleasing result without extractions or other high-force mechanics (Fig. 36-12). One should think how differently this 18-year-old’s profile, and indeed his entire face, would have looked had four premolars been removed. Figure 36-13 tracks the maturation of the profile of this patient from 13 years, 4 months to 20 years, 8 months of age, clearly demonstrating how well this system served him in precluding extraction therapy.
Years after this case was completed, the author decided that taking CT scans of patients after treatment would be helpful in demonstrating the health of the bony architecture when treated with low-force tube mechan-ics. Figures 36-14 and 36-15 compare plaster models of the upper and lower arches taken initially and on the day of debonding with CT scans taken 5 or more years after treatment. Without high-force rapid palatal
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
A B C
D
H I
JK
E F G
FIGURE 36-7 A-K, Pretreatment records for case 1 (CB, age 13 years, 6 months). Diagnosis: Class I face (Class II dentally on the right) with severe crowding in both arches and a unilat-eral posterior crossbite. The canines are totally blocked to the labial of the lateral incisors in both arches with thin bone and tissue surrounding them. The upper second premolars are erupting toward the palate. CB laterally lacks facial support; his midface is somewhat con-cave with an obtuse nasolabial angle.
Continued
997.e104 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
First appointment: Banded maxillary and mandibular first molars. Bonded central and lateral incisors (see Fig. 36-8). Because of the severe labial position of the canines, it was necessary to gain space, therefore began treatment with a maxillary rectangular wire (0.014- × 0.025-inch Ni-Ti Align SE) with medium-light Ni-Ti springs activated 1.5 to 2.0 times the width of a bracket. Placed mandibular 0.014-inch Ni-Ti Align SE sectional archwire.
Second appointment at 2 months, 1 week: Placed maxillary and man-dibular 0.016- × 0.025-inch Ni-Ti Align SE. Activated Ni-Ti springs 1.5 width of the bracket.
Third appointment at 4 months, 1 week: Checked only the status (see Fig. 36-9).
Fourth appointment at 6 months, 1 week: Activated the springs.Fifth appointment at 8 months: Placed maxillary and mandibular
0.019- × 0.025-inch stainless steel arch wire (see Fig. 36-10). Took a panoramic radiograph to evaluate the position of erupting permanent teeth.
Sixth appointment at 10 months, 2 weeks: Adjusted the maxillary archwire.
Seventh appointment at 12 months, 2 weeks: Bonded maxillary canines and first and second premolars. Placed continuous 0.014-inch Ni-Ti Align SE in the maxillary arch.
Eighth appointment at 14 months, 3 weeks: Repositioned maxillary left lateral. Waiting on the eruption of the permanent teeth. Patient did not keep appointments for the next 5 months.
Ninth appointment at 19 months, 3 weeks: Bonded mandibular canines and first and second premolars. Placed continuous mandib-ular 0.014-inch Ni-Ti Align SE. Placed maxillary 0.016- × 0.025-inch Ni-Ti Align SE.
Tenth appointment at 22 months, 1 week: Placed maxillary 0.019- × 0.025-inch stainless steel posted archwire. Placed mandibular 0.016- × 0.025-inch Ni-Ti Align SE. Took head film.
Eleventh appointment at 24 months, 3 weeks: Took panoramic radio-graph to evaluate root position (see Fig. 36-11). Adjusted maxillary archwire.
Twelfth appointment (at 26 months, 2 weeks): Bonded mandibular second molars. Placed 0.016-inch Ni-Ti Align SE overlay to engage mandibular second molars.
Thirteenth appointment at 29 months: Bonded upper second molars. Placed maxillary 0.016-inch Ni-Ti SE overlay. Placed crimpable hooks on 0.016- × 0.025-inch Ni-Ti Align SE. Started full-time bilateral V-elastics and anterior trapezoid elastics.
Fourteenth appointment at 30 months, 3 weeks: Adjusted maxillary archwire. Placed mandibular 0.016- × 0.025-inch posted stainless steel archwire in lower arch because additional play between arch-wire and bracket slot was needed for settling. Continued bilateral V-elastics full time.
Fifteenth appointment at 32 months, 1 week: Adjusted maxillary and mandibular archwires. Continued V-elastics full time.
Sixteenth appointment at 33 months, 2 weeks: Debonded both arches, and placed retention wires. Bonded 0.016- × 0.022-inch Bond-a-Braid braided wire to the maxillary arch lateral to lateral incisor. Placed 0.026-inch round stainless steel wire on the man-dibular arch canine to canine, bonding only the canines (see Fig. 36-12). Prescribed upper and lower slipcover retainers for night wear only.
BOX 36-1 Case 1 (CB) Treatment Sequence
expansion, the maxillary first premolar width increased by 11 mm and the maxillary first molars increased by 14 mm with desired tipping. An estimation of the second premolar change is 12 to 13 mm. The lower first premolar width increased by 11 mm, and the lower first molar width increased by 5 mm. Canines had erupted high through the cortical plate in both arches and could not be measured.
The plaster models and the horizontal CT scans of the upper arch (Fig. 36-16) demonstrate that the majority of tooth movement occurred with minimal tipping, resulting in a well-shaped archform. Figure 36-17 demon-strates that the arch length gain was in the transverse and was achieved through bodily movement of teeth and desirable tipping of posterior teeth. In addition, the palatal anatomic improvement is also evident. Figure 36-18 shows vertical CT scans of the upper second premolars and upper sec-ond molars. All the vertical CT scans illustrate excellent tooth position and health of the surrounding bone structure that resulted from bodily tooth movement without high-force rapid palatal expansion. Moreover, the scans illustrate the delicacy of the bony architecture in this area and should challenge all clinicians to consider lowering forces and using an alternative to rapid palatal expansion.
Orthodontists can make a number of interesting observations from the CT scans. The vertical CT scan of the lower second molar (Fig. 36-19) was eye opening for the author. Before using low-force tube mechanics, the author had always assumed that in trying to gain lower arch length, conventional mechanics caused the second molars to erupt lingually; how-ever, in looking at the CT scans, the author came to another conclusion. In crowded cases, the tongue is more passive than normal and typically does not lift or function into the palate. In swallowing at least 1000 times a day and articulating sounds, a normally functioning tongue continually moves up and down in the palate, thus shaping the architecture of the lingual cortical plate, especially in the lower second molar area. In a normal
functioning case, the lingual cortical plate is more upright than in crowded cases where the tongue is passive, sitting low in the mouth; thus in such cases, the cortical plate is lingually inclined in the second molar area. The net result is that as the second molar erupts, its crown follows the path of least resistance between the buccal and lingual cortical plate, which usually results in a lingually tipped clinical crown. A second observation is that on nearly all CT scans taken, the apex of the lower second molar root is usually positioned within the lingual cortical plate. This observa-tion supports the recommended treatment protocol of the system to cut the stainless steel working archwire between the first and second molars when applying Class II elastic mechanics. Because the apex of the second molar is sitting in cortical bone, which has low vascularity, orthodontists only need to engage it in cases of maximum anchorage. Ricketts spoke of the anchorage value present when tipping the lower roots against or into the buccal cortical plate.
The horizontal CT scan of the lower arch (Fig. 36-20) offers an important vantage point when considering orthodontic force. The bony contours on the labial, buccal, and lingual sides are demonstrated. Much of the tooth structure normally sits within the thin-layer, low-vascular cortical bone, which supports the concept of using extremely low forces. The scan lends support to the idea that in using low-force mechanics, cortical bone will follow tooth movement in all planes of space. The author believes that when orthodontists can simulate the forces of natural tooth movement—as orthodontists have done over the years with the Fränkel appliance—the body has an incredible ability to adapt. An interesting analogy is how the cortical plate adapts (Fig. 36-21) around a horizontally impacted tooth as it slowly develops. Figure 36-22 shows records taken after 5 years, 3 months in retention. Despite the fact that CB had not worn his retainers for more than 4 years, the dentition remained stable.
997.e105CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
A B
E
C DD
FIGURE 36-8 A-E, Bonding appointment for CB.
Continued
997.e106 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
A B
DC
E
A B
EE
FIGURE 36-9 A-E, Third appointment for CB at 4 months, 1 week.
997.e107CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
A B
C D
E
A B
FIGURE 36-10 A-E, Fifth appointment for CB at 8 months.
FIGURE 36-11 Panoramic radiograph taken during the eleventh appointment for CB at 24 months, 3 weeks.
Continued
997.e108 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
C D E
H
I
F G
A BA B
FIGURE 36-12 A-I, Posttreatment records of CB. Total treatment time: 33 months, 2 weeks with 16 appointments. The length of treatment was dictated, in part, by the time required for the canines to erupt into the arch and the fact that the patient did not keep his appointments for 6 months during midtreatment.
997.e109CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
FIGURE 36-13 These photographs track the maturation of CB’s profile from 13 years, 4 months to 20 years, 8 months, clearly demonstrating how well the Damon System served CB in precluding extraction therapy.
45 mm
A
C
B
D
34 mm
FIGURE 36-14 Comparisons of pretreatment and posttreatment upper arch plaster models for CB with computed tomographic scans. Pretreatment and posttreatment plaster models of the upper arch show 11-mm change in first premolar width (and an estimated 12- to 13-mm change in second premolar width) and 14-mm change in first molar width. The bony contours on the buccal of the first premolars and first molars are evident. Vertical scans taken 5 years, 3 months into retention show healthy alveolar bone. A, Scan of upper first premolars at 5 years, 3 months in retention. B, Pretreatment. First premolars: 34 mm; first molars: 41 mm. C, Posttreatment. First premolars: 45 mm; first molars: 55 mm. D, Scan of upper first molars 5 years, 3 months in retention.
Continued
997.e110 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
38 mm
A
C
B
D
27 mm
C
FIGURE 36-15 Comparisons of pretreatment and posttreatment lower arch plaster models for CB with computed tomographic scans. Pretreatment and posttreatment models of lower arch show 11-mm change in first premolar width and 5-mm change in first molar width. Ver-tical scans, taken 5 years, 3 months into retention, show healthy alveolar bone. A, Scan of lower first premolars 5 years, 3 months in retention. B, Pretreatment. First premolars: 27 mm; first molars: 44.5 mm. C, Posttreatment. First premolars: 38 mm; first molars: 49.5 mm. D, Scan of lower first molars 5 years and 3 months in retention.
FIGURE 36-16 The horizontal computed tomographic scan of CB’s upper arch illustrates the well-shaped archform.
997.e111CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
A B
FIGURE 36-17 A, B, Plaster models demonstrate that the arch length gain was in the trans-verse achieved through bodily movement of the teeth and desirable tipping of the posterior teeth. The improvement in palatal contours is also evident.
A B
FIGURE 36-18 Computed tomographic scans of CB taken 5 years, 3 months into retention. A, Scan of upper second premolars illustrates the excellent tooth position and surround-ing bone structure that resulted from bodily movement without a high-force rapid palatal expander. B, Scan of upper second molars illustrates the delicate bony architecture of this area and challenges clinicians to consider lowering forces and using an alternative to rapid palatal expansion.
FIGURE 36-19 The bony architecture in the second molar area of a collapsed arch encour-ages second molars to erupt lingually inclined. By helping the tongue assume a normalized position via posterior arch adaptation, second molars have a greater chance of erupting in a more upright position.
Continued
CASE STUDY 36-1 Achieving Facial Harmony with Facially Driven Treatment Planning—cont’d
FIGURE 36-20 The fact that much of the tooth structure nor-mally sits in a thin layer of cortical bone of low vascularity sup-ports the concept of using extremely low forces.
FIGURE 36-21 Computed tomographic scan depicts how the corti-cal bone has adapted to the third molar (arrow) and supports the idea that cortical bone will follow tooth movement in all planes of space.
D E F
G H
A B CA
FIGURE 36-22 A-H, Retention records of CB taken at 5 years, 3 months into retention. Despite the fact that the patient did not wear night retainers for more than 4 years, the dentition remains stable.
997.e113CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
Use of Nonextraction Therapy Where Possible and Light-Force MechanicsA second trend—toward nonextraction therapy—is an admi-rable orthodontic goal. The principle means of achieving non-extraction, however, negates another important biologically sound principle: that of using low-force orthodontic mechan-ics. Heretofore, other than the Fränkel and similar appliances that have proved difficult to apply and to clinically manage, the principal means of orthodontically gaining arch length were distalizing molars or using high-force rapid palatal expansion devices. Each of these methods has its drawbacks because the forces are high when one considers the fragile vascular architec-ture (illustrated later in Fig. 36-28). CBCT scans of the mid-face after rapid palatal expansion show wide ranging effects on skeletal and dental structures. Distalizing molars is also time consuming. Although Damon System practitioners are some-times reluctant to relinquish their rapid palatal expanders, the author believes that their use has an unnecessarily detrimen-tal effect on the biologic structure and function of the entire dentofacial system. Rather than causing patients to suffer the trauma of opening the palatal sutures, distalizing the molars, or extractions (and the subsequent closure of the extraction sites and adding treatment length), clinicians can now maintain many complete dentitions by using very light-force, high-tech archwires in passive tubes, thus gaining arch length.
FORCE MANAGEMENTAchieving Extremely Light-Force Mechanics: A Passive TubeThe author has spent nearly 20 years carefully evaluating the rationale for his clinical mechanics. Early on, it became appar-ent that using a force system was not “biologically sensible.” To use a bracket system to move teeth along an archwire that was tightly tied and nearly locked the wire to the base of the bracket slot made little sense. To reach orthodontic goals, orthodontists are challenged to use forces that are consistent with biologically sound principles of tooth movement.
The author believed that an appliance capable of accommo-dating a biologically attuned system might best be developed by looking into the field of self-locking brackets. Orthodontic history indicates that, from its early years, clinicians perceived the advantages of engaging archwires in tubes rather than ligating them into brackets. One of the earliest tube systems, the twin-wire cap-and-channel appliance, possessed some of the attributes of current self-locking systems but was limited by hard-to-place caps and the absence of space-age wires, pre-adjusted slots, and modern mechanics. In 1966, the Snap Ring appliance was introduced (3M Unitek, Monrovia, CA). This appliance was not self-locking in today’s sense of the term, but it simulated the concept.2 A staple applicator attached a metal C-ring that locked over the outer portion of a round bracket. The system was limited by the large bracket size and the same shortcomings of the earlier cap-and-channel system.
A later example was the Edgelok bracket (Ormco Corpo-ration, Orange, CA), which was introduced in the late 1960s (Fig. 36-23). Craig Andreiko, director of research and devel-opment at Ormco, described the bracket as the “first true self-ligating tube-type appliance.” He went on to explain that, “It was comfortable, had a positive-seating mechanism that formed the facial wall that was easy to open and close. It had the misfortune of being introduced around the same time as
the StraightWire appliance from ‘A’ Company. It also suffered from the prevailing edgewise treatment sentiment of the time that dictated an archwire selection and timing that stifled the effectiveness of even the more resilient and efficient archwires that were becoming available; nevertheless, it enjoyed wide-spread usage for a number of years, waning as preadjusted appliances took hold in the marketplace.”3
Another major advancement of that era was the SPEED appliance (Strite Industries, Cambridge, Canada), an active self-ligating appliance. The use of the SPEED appliance has been shown to reduce archwire changing chair time to as little as 25% of that of conventional twin brackets. The evolution of self-locking appliances greatly accelerated after 1995 with the introduction of active and passive appliances, including the Damon System.
Coinciding with the advances in self-locking appliances has been the evolution of the space-age nickel-titanium wires introduced by George Andreasen and the University of Iowa in cooperation with 3M Unitek. Although the profession widely recognized this development as a landmark advance in provid-ing appropriate, light, continuous orthodontic force, it has been slow to realize its full potential. Ray Morrow, former 3M Unitek research and development project manager for Nitinol wire, related the early problems with usage of the archwires that are analogous with today’s failures to take full advantage of their remarkable potential: “Initially, just as they were accustomed to using stainless steel archwires, many clinicians tried to place bends in the wires, so many complaints were received about breakage from what actually was the result of improper usage of the early, somewhat brittle wires. In response, Unitek altered its manufacturing process in order to produce less elastic wires that permitted more bending without breaking. It was some time before proper usage of the wires ended the complaints, even as wires with greater elasticity and resistance to bending were introduced by Unitek and, later, by other companies.”4
The author has included this bit of history because, even today, the ultimate clinical benefits attainable with the remark-able space-age wires are being severely limited. Steel and elas-tomeric ligations are primary causes of this problem because they create binding and friction; active self-locking appliances provide a significant improvement but still exert facial-side pressure in many phases of treatment that limit the freedom of
FIGURE 36-23 The Ormco Edgelok self-ligating bracket was introduced in the late 1960s.
997.e114 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
the archwire to perform. Maximizing treatment results requires a passive self-locking appliance (tube), combined with careful selection of archwires (allowing plenty of play in early treat-ment and in midtreatment) and timing (allowing the wires to work and fully express their potential). The Damon System meets these demands to reach the optimal force range that stimulates cellular activity without occluding blood flow in the periodontium.
A Look at Sliding MechanicsMany types of space-closure mechanics that require sliding the brackets along the wire as they start to level and align have been used for years, so achieving space closure with the Damon
tube is easy for clinicians to visualize and accept. Over the past 30 years, clinicians have moved away from starting cases with multiloop stainless steel archwires in favor of using high-tech continuous wires free of any loops or bends. For teeth to align in the early phases of treatment, sliding mechanics must take place. Leveling the arch, aligning high canines, correcting tooth rotations, and changing archform (Fig. 36-24) are good examples of the use of sliding mechanics. Orthodontists have accepted and used tubes on molars for many years with great success. Passive self-ligation gives the clinician the opportu-nity to have a tube on every tooth, enhancing the performance of low-force high-tech archwires with low-friction sliding mechanics.
A B
C
D EE
FIGURE 36-24 Sliding mechanics is involved with (A) leveling the arch, (B) aligning high canines, (C) correcting tooth rotations, and (D, E) changing archform.
997.e115CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
The Damon System (Fig. 36-25) has been developed to align each phase of treatment with these natural force systems of normal growth and development. It became apparent that the application of biologically appropriate forces at each stage of treatment is essential for a long-term favorable outcome. As pre-viously mentioned, the Damon appliance is commonly referred to as a bracket, but the term tube is a more useful description for this passive appliance. The appliance is a tube with tie-wings rather than a conventional bracket and, as such, has a static facial wall when the self-locking slide is closed. Vourdouris5 com-pared the friction produced by passive and active conventional and self-locking brackets. With the use of a 0.019- × 0.025-inch stainless steel archwire, conventional brackets with elastomeric ties showed 400 (125.42 g/cm2) to more than 600 (152.30 g/cm2) times greater friction; steel ties showed 400 (97.07 g/cm2) times greater friction; and active self-ligating brackets showed 216 (54.12 g/cm2) times the friction of the passive self-ligat-ing Damon tube (0.25 g/cm2). With conventionally tied fixed appliances and active self-ligating brackets, the archwire is totally seated against the base of the bracket slot during some or all phases of treatment. The resulting binding and friction make closing spaces, leveling, archform changes, and closing of open bites, as well as the finishing, settling, and detailing of the occlusion, far more challenging. Passive self-ligation maintains play in the mechanical system during all stages of treatment. Figure 36-26 illustrates the degree of freedom of the initial round wire in a Damon tube. The small wire-to-lumen ratio is essential to leveling, aligning, and arch adaptation in a friction-free environment but initially limits rotational control. Rotational control is primarily achieved with the second, larger archwire, but the lack of friction and binding enables the overall correc-tion to proceed faster. The short treatment times in the illus-trative cases typify results obtained with consistent, biologically sensible forces. Figure 36-27 demonstrates that accurate tooth positioning, including rotational control, requires a full-depth archwire to fill the slot in a passive system. The play in the system when using 0.014- × 0.025-inch, 0.016- × 0.025-inch, 0.017- × 0.025-inch, and 0.019- × 0.025-inch rectangular wires in a 0.022-inch slot provides the needed rotational control and allows for 7 to 10 degrees of torque play in both directions with excellent rotational control later in the wire progression.
One must think of this new therapy as a complete system and not simply a new passive self-ligating bracket. With this new low-force, low-friction technology (tubes on each tooth instead of brackets with ligature ties and elastomerics), the clinician can apply very light forces that closely match normal biologic tooth-moving forces. These properly attuned forces, not the clini-cian, allow the muscles of the face and tongue, bone, and soft tissue to determine the archform.
An examination of what is known about the fragility of the vascular system and the bony architecture that support the dental arches is a necessary consideration for any orthodontic treatment.
Case for Using Extremely Light Forces in Passive TubesUsing scanning electron microscopy and the corrosion resin cast method, Brazilian researchers M.C. Kronka, I. Watanabe, and M.C. Pereira da Silva6 have published images of the angio-architecture of the palatine gingival in young rabbits. These photographs clearly illustrate the fragility of the vascular archi-tecture entering the alveolar bone on one side of the periodon-tal space (Fig. 36-28, A) and the lacelike network on the root of the tooth on the other side (Fig. 36-28, B). Figure 36-28, C, illustrates an even closer view of the vascular network of the
FIGURE 36-25 The passive Damon System 3 tube and bracket from Ormco.
FIGURE 36-26 The small wire-to-lumen ratio of the Damon tube is essential to leveling, aligning, and arch adaptation in a friction-free environment.
FIGURE 36-27 With larger archwires, the Damon conduit pro-vides excellent torque and rotational control without lodging the system.
997.e116 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
periodontal ligament, with Figure 36-28, D, showing the tooth, sulcus, and vascular network. Such images should challenge all orthodontists to reevaluate their clinical force systems. Clini-cal mechanics and force systems are too often based on patient tolerance rather than on their impact on the periodontium and cellular biologic structure. Orthodontists continually ask the question, “What is the largest archwire I can get in?” If teeth do not move, then often orthodontists simply apply more force, yet they recognize the detrimental effects of excessive force on vascularity of the dentoalveolar complex. The cellular structure of orthodontically induced tooth movement is complex, and
researchers are still challenged to unravel all the cellular mech-anisms in play.
The modeling events of tooth movement are commonly referred to as areas of compression and tension within the periodontal ligament. Simply put, membranous bone growth is appositional with alveolar bone being resorbed on the mov-ing front and new bone being laid down on the trailing side. Just more than 100 years ago, Carl Sandstedt7 discovered the different responses of tissue to heavy and light orthodontic forces. He determined that on the tension side of the tooth, the responses to strong and weak orthodontic forces were
C
D
AA BB
C
D
FIGURE 36-28 A, Lacelike vascular architecture of the tooth of a young rabbit reveals its fragility and susceptibility to destruction by high forces. B, Blood vessels are shown entering the alveolar bone. C, Image is a close up of the network. D, Tooth, sulcus, and vascular network are visualized.
997.e117CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
similar. Bone deposition occurred with spicules forming along the direction of the strained periodontal fibers. The old bone was unchanged in appearance, whereas the new bone growth was easy to recognize. Responses on the pressure side of the tooth varied significantly, however, between light and heavy forces. No root resorption occurred with light forces because new bone was equally resorbed along the entire socket surface. The response to heavy forces was notably different, which led Sandstedt to coin the often-heard phrase “undermining resorption.” The underlying bone was not resorbed in areas where the periodontal ligament was overcompressed. Rather, active resorption of bone and tooth root took place in the still vital areas surrounding the damaged membrane. Sandstedt’s findings have been well recognized in academia and in the lit-erature but have been widely ignored in the clinic for more than a century.
In 1932, A.M. Schwarz8 found that very light forces of 20 to 26 g/cm2, the same pressure in the capillaries of the periodon-tal ligaments, afforded safe and effective tooth movement. The obvious conclusion is to not exceed the outward pressure of the blood vessel if one does not wish to collapse it. Anything greater strangles the capillaries and generates necrotic tissue at the pres-sure sites.
Perhaps the greatest contributions to understanding the mechanisms of structural changes and tissue behavior caused by excessive orthodontic forces were produced by K. Reitan.9-13 His publications from the late 1940s through the early 1970s revealed the strangulation of periodontal ligament capillaries, damage to the tissues, and resulting necrosis of the periodontal ligament and root resorption caused by conventional ortho-dontic forces.
In 1973, P. Rygh14,15 summed up the consequences of the conventional orthodontics (high force) of the day: With conventional forces, this destructive process occurs at each appointment, and the wire is activated through a distance wider than the periodontal ligament space. At each wire change, teeth slam against the wall of the socket, and the intricate network of blood vessels is crushed yet again. Each time this trauma occurs, it takes weeks for the periodontal ligament to revascularize at the cellular level.
In 1992, Tuncay and colleagues16 observed that oxygen is the trigger mechanism for remodeling the periodontium. If vascu-larity is interrupted in the periodontal space between bone and teeth, then oxygen is no longer available and cellular activity is slowed or stopped. In 1993, W.R. Proffit and H.W. Fields17 advocated that, “Optimum force levels for orthodontic tooth movement should be just high enough to stimulate cellular activity without completely occluding blood vessels in the peri-odontal ligament.” The author has named this threshold force the biozone or optimal force zone. Proffit9 also stated, “If the applied force is great enough to totally occlude blood vessels and cut off the blood supply, a hyalinized avascular necrotic area is formed. This area must revascularize before teeth start to move.”
Regarding Rygh’s and Reitan’s findings, Bob Borkowski18 stated, “This healing time is, in essence, a big timeout in the progress of treatment. Understanding this phenomenon makes me wonder if this healing time isn’t the reason why, in conventional mechanics, adult treatment takes longer than adolescent treatment.” Borkowski postulated that this dif-ference is due to children healing from their wounds faster than adults.
The issue of oxygen supply raises questions about what is happening with the use of light, high-tech archwires in a pas-sive tube where play between the wire and the lumen size of the tubes is considerable. The response to very light, high-tech wire used in low-friction, passive tubes is different from the use of the same high-tech wires in conventionally ligated or active self-ligating appliances. Certainly the adaptation phenomenon is occurring at the cellular level, and perhaps this phenomenon has something to do with oxygen supply. At this stage, the phe-nomenon is not clear. What orthodontists can verify is that the response is similar to that seen in patients treated with the Frän-kel appliance.
Patients such as CB (see Case Study 36-1) have always prompted the author to question the cause of crowding. Given the cause, orthodontists can better assess what methods to use to stimulate the best possible resolution. As in most such cases, the shape and size of the body of the mandible is normal, but the alveolar process is severely constricted. The author’s opin-ion is that this condition often results from lips and muscles of the face being out of balance with the tongue. The tongue is passive or sitting too low in its cavity, and without the exertion of the strong outward force of the tongue on the arches, the muscles of the face dominate, thus constricting the lower arch and allowing the maxilla to collapse inward. Fränkel19 capably demonstrated that keeping the buccal tissues away from the dental arches fosters a redistribution of forces between the lips and muscles of the face and the tongue, generating greater arch length. Fränkel used buccal shields to increase arch width. The absence of cheek forces enabled the tongue to generate buccal drift of posterior teeth. Long-term studies on patients under-going treatment with the Fränkel appliance have proved the results to be stable.
The Damon System, when properly applied, provides patients with the physiologic improvements possible with the Fränkel appliance and other muscular imbalance corrective appliances, plus the precision finishing attainable with pread-justed edgewise appliances. Because form follows function, the author considers many malocclusions to be functional abnor-malities. Light wires acting in an almost friction-free envi-ronment in the Damon tube appear to be able to correct the functional imbalance and allow the alveolar process to create a new, individualized archform. The author’s explanation for this phenomenon is that the friction and binding of the arch-wire in conventionally ligated appliances (and active self-ligat-ing appliances) preclude functional adaptation. Orthodontists recognize the power of sliding mechanics to close space, with buccal tubes being essential to this process. Sliding mechanics also offers the most efficient means of aligning and leveling teeth in the early phases of treatment. Clinicians often use edgewise wires to unravel and level malposed teeth. Minimal play exists between the archwire and the bracket slot, and the wire becomes bound up in a tightly ligated system. In a nearly friction-free environment with the appropriate amount of play between the archwires (a 0.014-inch round nickel-tita-nium wire is essential to this process) and the passive bracket tube, teeth begin to level and unravel, and the arch begins to widen in the transverse. Alan Bagden20 suggests that this beginning adaptation “wakes up the tongue.” This phenom-enon allows the tongue to seek a higher level in the oral cav-ity, thus instigating a new force interplay among the tongue, cheeks, and lips. With this gentle force of a small round wire in large fixed passive tubes, transverse arch adaptation occurs
997.e118 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
similar to the Fränkel effect. Although the technique is too new to substantiate improved long-term stability, results to date have been encouraging. Apparently, moving teeth with high-tech archwires in passive self-locking tubes generates a healthy alveolar bone and periodontium support that is not as susceptible to relapse as the typical repositioning of the denti-tion with more traumatic forces.
After treating several thousand patients with this low-force tube system, the author noted the significant variation in the rate of tooth movement from patient to patient. In most patients the rapid rate of tooth movement with such light forces is impres-sive. Using high-force conventional mechanics for years, the author found the response among patients to be approximately the same, with the greatest variable being between adults and children. Now the slowest and most challenging cases are in those who have had previous extractions and conventional higher-force orthodontics. The alveolar bone appears to have been altered, which affects subsequent treatment planning and length of treatment.
COMPUTED TOMOGRAPHIC SCANS DEMONSTRATE HEALTHY BONE STRUCTURE AFTER TREATMENT WITH THE LOW-FORCE DAMON TUBE SYSTEMOver the years, the author has observed that the kindest movers of teeth are normally functioning muscles of the face and tongue. Orthodontists have recognized the Frän-kel effect in first-phase treatment using the 2 × 4 method (with fixed appliances only on the four anterior teeth and molars), which alters the impact of the facial musculature, allowing the premolars to move laterally. The author’s expe-rience has been that over several months, premolar width usually increases 6 to 8 mm with little tipping. This same type of bodily movement of teeth with extremely light, high-tech archwires in the passive Damon tube appliance has been verified on CT scans of patients who experienced posterior width change. The scans also document that the bone devel-opment tracked with the teeth movement and arch adapta-tion. Rather than using high-force expansion, this research suggests that trying to match this natural force adaptation with all clinical mechanics makes sense.
Until now, orthodontic research has been primarily lim-ited to clinical observations and long-term retention stud-ies, with conventional radiographs and periodontal findings serving as the evaluation technologies. With the technical advancements of three-dimensional CT scans for the mid-face, orthodontists now have the means to determine the posttreatment health of the alveolar bone. The author has spent hundreds of hours evaluating CT scans taken on 13 patients treated with low-force mechanics in a passive tube system where functional adaptation accommodated teeth in a crowded arch using nonextraction therapy. These findings are encouraging and should challenge clinicians everywhere to reevaluate their management of clinical forces and stim-ulate them to consider a paradigm shift of their treatment planning. These CT scans were taken on young and adult patients, from those just debonded to one patient in reten-tion for longer than 5 years.
Most clinicians have believed that with clinical mechanics, at best, teeth can be tipped only in the transverse, not bodily
moved as well. These CT scans conclusively show that alveo-lar bone can be altered and reshaped with low clinical forces. This low-force and passive tube technology and the clinical research that substantiates it call for changes in treatment planning and the mechanics of tooth movement. Other find-ings from the CT scans demonstrate how thin the alveolar bone is on the labial, buccal, and lingual aspects of the teeth that orthodontists are trying to move. These CT scans make it apparent that every effort should be made to take great care of the thin cortical plate. In viewing the scans of patients in long-term retention, the reader will note that the architecture and thickness of the alveolar bone appears to improve over time after low-force orthodontics. Recognizing that low-force orthodontics can have a positive impact on the periodontium is encouraging. The reason bone may regenerate in some areas of the mouth in periodontally challenged patients and not in others is not understood. The periodontist who conducted connective tissue grafts on patients during or after treatment with low-force and passive tube technology commented on observing an improved vascular environment. After having evaluated CT scans of several crowded cases in retention, the author recommends that orthodontists make every effort for early tooth guidance in children to keep permanent teeth from erupting through the labial, lingual, and buccal cortical plates. Obviously, teeth erupting in the center of the alveolar ridge usually have far improved bone on the labial and buccal aspects.
CASE PRESENTATIONS AND CLINICAL ANALYSESThe following cases graphically demonstrate how facial treat-ment planning should and can be the primary focus. The den-titions of these patients are obviously crowded. The dentitions beg the question, “Why are these patients so crowded?” Are the bones of the midface and body of the mandible smaller than normal, or has there been an adaptation of the alveo-lar process because of abnormal muscle forces affecting arch development? Most orthodontists have been trained to evalu-ate the patients only from head films. As mentioned in the case of CB, early in the author’s career, extraction therapy would have been used to treat CB, despite the body of his mandi-ble being exactly the same size as the author’s, which is an exceedingly wide archform. To see that more and more ortho-dontists around the world realizing the impact that treatment decisions have on the maturing profile, for good or for ill, is exciting. With improvements in technique and technology, orthodontists now can plan and execute treatment by evalu-ating its long-term implications on profile (lateral view) and arch width and facial support (frontal view). In the author’s estimation, designing treatment mechanics that do not over-power the biologic system in any phase of treatment is critical, and doing so requires the use of low-force archwires in a pas-sive tube. In reviewing these case studies, the reader should note that great care has been given to using treatment forces that are “just high enough to stimulate cellular activity with-out overpowering the periodontium and orofacial muscular complex.”17 If orthodontists maintain force levels in the opti-mal force zone, the alveolar bone and tissue can be moved with teeth. With the Damon System, the art of clinical orthodontics is to match treatment mechanics with the natural low-force systems of the body and to learn how to read and react to how the alveolar process and muscles adapt.
997.e119CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction TherapyCase 2 (AH) provides another example of how the transverse dimension and severe upper anterior crowding can be satisfactorily treated with sim-ple low-force and tube mechanics. This case is a good example of facially driven treatment achieved by converting anterior crowding into posterior adaptation of bone, muscle, and soft tissues. Arch length gain is illustrated along with the correction of the Class II dentition. At 16 years, 5 months of age, AH had a Class II dental bilateral posterior crossbite and crowded maxillary arch. She was midface deficient but with a good profile and an aesthetically pleasing obtuse nasolabial angle.
The treatment objectives were as follows: 1. Gain maxillary arch width to support the midface. 2. Correct midface deficiency. 3. Maintain nasolabial angle while improving the midface.
4. Develop an ideal tooth-to-lip relationship. 5. Transpose the malpositioned upper right canine distolingually without
damaging the root of the lateral directly lingual to the canine root.Pretreatment records (Fig. 36-29) demonstrate the substantial Class II
arch relationship and severely crowded maxillary dentition. Only low-force Damon System mechanics were used throughout treatment. No pala-tal expanders, distalizers, headgear, implants, lingual holding arches, or removable appliances were used. Using low-force mechanics, the result was far superior patient comfort throughout treatment and improved bone and tissue at the end of treatment.
Tom Pitts, a former member of Robert Ricketts’ Bioprogressive Study Club, reported that in a study of the relationship between tooth-to-tooth gain in arch width and overall increase in arch length, Ricketts found specific
A B C
D
H
IJ
E F G
FIGURE 36-29 A-J, Pretreatment records for case 2 (AH, age 16 years, 5 months). Diagnosis: Class II with bilateral posterior crossbite and crowded maxillary arch and midface deficiency but good profile and obtuse nasolabial angle.
Continued
997.e120 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’dratios occurred with changing archform and orthodontic treatment.21 This research indicates that a 1-mm gain in canine width, a 1.5-mm gain in first premolar width, a 2-mm gain in second premolar width, or a 4-mm gain in molar width each yields a 1-mm increase in arch length. The light-force Damon System maximizes the potential of each individual’s anatomic and physiologic structure in delivering a natural archform. The system provides nature a second chance to correct inherent or habit-generated deficiencies. The crowding in this case indicates a tongue trapped low in the mouth and unable to provide the necessary facial thrust for normal maxillary arch formation (Fig. 36-30). The Damon System helps correct nature’s muscle imbalances with gentle forces. The long intervals between appointments allow the light archwires to work to their full potential in the almost friction- and binding-free tubes.
Posttreatment records (Fig. 36-31) were taken after 22 months, 3 weeks of treatment in 11 appointments. Figure 36-32 shows that bodily tooth movement along with minimal corrective tipping created a 9- to 12-mm upper arch width adaptation and tremendous palatal change. The patient was happy to report that she could now breathe through her nose and sleep with her mouth closed. The intraoral photographs reveal healthy bone and tissue with significant alveolar improvement. Figure 36-33 com-pares the plaster models of the upper arches taken initially and the day of debonding with the CT scans taken 7 months after treatment. Initial and final comparisons of the plaster models clearly reveal the posterior arch widening, anterior unscrambling, and arch shape improvements. CT scans
demonstrate healthy alveolar bone in all areas. Unfettered light wires worked to develop what nature and a trapped, underactive tongue failed to produce; that is, an appropriate archform for AH and a pleasing final result.
Archwires adapted to the initial and final upper archforms (Fig. 36-34) make apparent what happened to the anterior crowding. Adapting the final archwire to the initial archform demonstrates an arch length gain of 13 mm, yet the measurement distal of the first molars to the labial of the incisors at the beginning and end of treatment is only 1 mm, which explains why the existing attractive profile was maintained while the midface deficiency was improved. These measurements indicate that the anterior crowding was accommodated by transverse posterior adaptation. An observation in other patients is that a change in the posterior arch width of only 1 or 2 mm can have a favorable impact on the midface. The horizontal CT scans (Fig. 36-35) illustrate that the pleasant midface change is not simply a result of the expansion of the dental arch but the entire alveolar process high in the vestibule, which provides improved facial support.
Initial and final comparisons of the plaster models of the lower arch demonstrate the minimal change (0 to 2.5 mm) in posterior arch width (Fig. 36-36). The horizontal CT scan taken 7 months in retention (Fig. 36-37) demonstrates how the roots of the lower teeth sit in the cortical plate. Considering that the change in the lower arch width or anteropos-terior tooth movement was small, it is interesting to note in the CT scans that so much of the tooth structure is sitting in cortical bone with low vas-cularity, again supporting Rygh’s notion of low-force mechanics.
A B
FIGURE 36-30 A, B, The trapped tongue is unable to normalize posterior maxillary arch width. The lower arch shape indicates low tongue posture.
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’d
A B C
D E F
G H
I
J
B C
FIGURE 36-31 A-J, Posttreatment records of AH. Total treatment time: 22 months, 3 weeks with 11 appointments. Midfacial aesthetics improved while maintaining favorable profile. Min-imal tipping with 9- to 12-mm upper posterior adaptation and improved tongue position are evident.
FIGURE 36-32 The pretreatment and posttreatment plaster models of AH demonstrate bodily tooth movement and tremendous palatal change with minimal corrective tipping that resulted in a significant improvement of articulation and easier breathing.
Continued
997.e122 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’d
A B
C D
E
30.5 mm
32 mm
37 mm
34 mm
42.5 mm
48 mm
FIGURE 36-33 Comparisons of pretreatment and posttreatment upper arch plaster mod-els for AH with computed tomographic scans. Initial and final models of upper arch show a 2-mm change in canine width, 12-mm change in first premolar width, 11-mm change in second premolar width, and 9-mm change in first molar width. Vertical scans taken 7 months into retention show healthy alveolar bone. A, Scan of upper first premolars at 7 months in retention. B, Scan of upper second premolars at 7 months in retention. C, Pretreatment. Canines: 32 mm; first premolars: 30.5 mm; second premolars: 37 mm; first molars: 44 mm. D, Posttreatment. Canines: 34 mm; first premolars: 42.5 mm; second premolars: 48 mm; first molars: 53 mm. E, Scan of upper first molars at 7 months in retention.
997.e123CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’d
A B
C D
E F
FIGURE 36-34 Adapting the final archwire to the initial archform demonstrates an arch length gain of 13 mm in AH, yet the measurement distal of the first molars to the labial aspect of the incisors at the beginning and end of treatment is only 1 mm, which explains why the existing attractive profile was maintained while the midface deficiency was improved. These measurements indicate that the anterior crowding was accommodated by transverse poste-rior adaptation. A, Final archwire adapted to the initial archform. B, Final archwire adapted to the final archform. C, Comparison of initial and final archwires. D, Comparison of initial and final archwires lengths shows 13 mm of change. E, Measurement from distal aspect of first molars to labial aspect of incisors of initial archform is 37 mm. F, Measurement from distal aspect of first molars to labial aspect of incisors of final archform is 38 mm.
Continued
997.e124 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’d
A B
FIGURE 36-35 A, B, The horizontal computed tomographic scans of AH’s upper arch illus-trate that the pleasant midface change is not simply a result of the expansion of the dental arch, but it is also the result of the entire alveolar process high in the vestibule, which provides better facial support.
A B
27 mm
34 mm
40 mm
27 mm
36.5 mm
42 mm
FIGURE 36-36 Comparisons of pretreatment and posttreatment lower arch plaster models for AH. Pretreatment and posttreatment models of the lower arch show no change in canine width, 2.5-mm change in first premolar width, 2-mm change in second premolar width, and 0.5-mm change in first molar width. A, Pretreatment. Canines: 27 mm; first premolars: 34 mm; second premolars: 40 mm; first molars: 46.5 mm. B, Posttreatment. Canines: 27 mm; first premolars: 36.5 mm; second premolars: 42 mm; first molars: 47 mm.
997.e125CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-2 Treatment with Nonextraction Therapy—cont’d
FIGURE 36-37 Horizontal computed tomographic scan of AH’s lower arch taken at 7 months into retention shows healthy labial and buccal bone with minimal change in tooth position. The fact that so much tooth structure sits in cortical bone with low vascularity supports Rygh’s notion of low-force mechanics.
CASE STUDY 36-3 Treatment with Extraction TherapyDespite orthodontists’ desire to treat with nonextraction therapy, it should be strongly emphasized that certain types of cases warrant extraction therapy. The philosophy of the Damon System is not founded on the idea of nonextraction therapy at any cost. The intent of the system is to achieve pleasing facial symmetry with a long-term healthy periodontium. Bimaxil-lary protrusive cases with full lip posture require extractions. In addition, on rare occasions, patients may not have the lip competence to keep the dentition from flaring forward with nonextraction therapy because the sys-tem heavily counts on the lip bumper or headgear effect. This lack of mus-cle competence must be recognized early in treatment, and extractions are recommended to avoid round tripping of the anterior teeth.
Case 3 (KH) was selected to demonstrate how the face determines treatment planning and that there is a time to extract. KH was 9 years, 8 months of age when she exhibited a Class II, Division 1 protrusive den-tition with a severely deficient mandible, disproportionate lower facial height, and petite facial features. She had a small nose and a lack of lip seal. Her genetic potential was greatly limited from significant growth, the father’s height being 5 feet 4 inches and the mother’s height at 5 feet 1 inch. Both parents displayed refined features. Her dentition evaluation noted generalized spacing in the maxillary arch. Upper incisors were labi-ally inclined, and the central incisors were large. She also had a significant overjet with a normal overbite.
The treatment objectives were as follows: 1. Achieve a Class I face, and then reevaluate protrusion and profile in an
attempt to create facial balance and symmetry. 2. Anticipate the impact of treatment on the patient’s maturing profile. 3. Leave the Herbst appliance on at least 16 to 18 months because of the
severity of the Class II and the petite size of the slow-growing patient. 4. If necessary, extract four premolars before initiating phase 2 to achieve
the best possible facial aesthetics.Pretreatment records, which are shown in Figure 36-38, include tomo-
grams taken before initiating phase 1 Herbst appliance treatment. In accord with the author’s Herbst philosophy of slowly activating over a
long time, the initial advancement was limited to 4 mm. The Herbst appli-ance treatment sequence (Box 36-2) reveals the small advancements that work along with the facial muscles in developing lateral upper arch expan-sion. Tomograms were taken again at the seventh appointment to check the condylar position. The Herbst appliance was removed on the eighth appointment, completing 18 months of functional Herbst appliance ther-apy. Progress records were taken at this time (Fig. 36-39). A comparison of the pre-Herbst and post-Herbst cephalometric tracings and facial pho-tographs revealed an ANB (A point–nasion–B point) change of 3 degrees. Although the chin position improved with Herbst appliance treatment, this petite girl was still protrusive, and it continued to be a challenge for her to fit her lips over her teeth. In view of her genetic growth potential and the refined features of her parents, the girl was scheduled for four first premolar extractions.
The patient waited 5 months before starting phase 2 treatment. After the premolar extractions, the upper and lower arches were bonded 6 to 6 (second molars had not erupted). A special prescription of +7 degrees of torque was selected for the upper and lower canines, which is strongly recommended on all extraction cases to prevent lingual tipping of the clini-cal crowns during space closure. Maxillary and mandibular 0.014-inch Ni-Ti Align SE archwires were placed. Bonded treatment required 11 appoint-ments and 21 months; the treatment sequence is shown in Box 36-3.
Figure 36-40 shows the placement of the 0.019- × 0.025-inch stain-less steel archwires with Ni-Ti springs hooked on them distal to the first molars. The distal eyelets were bent 90 degrees before placing over the distal ends of the cut archwires. To avoid flaring the second molars to the buccal, springs were not attached to the second molar hooks. The preceding procedure should be followed in cases of minimum anchorage. In cases of maximum anchorage retraction, ligation of the first and second molars together while attaching the springs to the hooks of the first molars is recommended (Fig. 36-41).
KH demonstrates how simple mechanics work at their best in an unbound mechanical system with light application of force. Archwire posts evenly
Continued
997.e126 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
A
I J
F G H
B C
D
E
FIGURE 36-38 A-L, Pretreatment records of case 3 (KH, age 9 years, 8 months). Diagnosis: Class II, Division 1 bimaxillary protrusive with severely deficient mandible, disproportionate lower facial height, and petite facial features.
997.e127CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
K
L
FIGURE 36-38, cont’d
Start: Initial records, including tomograms, taken before beginning treatment.First appointment: Placed Herbst appliance, and advanced 4 mm.Second appointment at 2 months 2 weeks: Checked Herbst appliance.Third appointment at 5 months: Advanced Herbst appliance 3 mm.Fourth appointment at 7 months 2 weeks: Checked Herbst appliance.Fifth appointment at 10 months 2 weeks: Checked Herbst appliance, and added 1-mm shim.Sixth appointment at 13 months: Checked Herbst appliance.Seventh appointment at 15 months: Checked Herbst appliance, and took tomograms.Eighth appointment at 18 months: Removed Herbst appliance, took progress records, and
scheduled four premolar extractions and full bonding (see Fig. 36-39).
997.e128 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
A B CC
D
E
FIGURE 36-39 A-G, Phase 1 posttreatment records of KH with Herbst appliance (phase 1 treatment time: 18 months with eight appointments).
997.e129CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
F
G
FIGURE 36-39, cont’d
Start: Extracted upper and lower first premolars.First appointment: Bonded upper and lower arches 6 to 6. Used
+7-degree torque on upper and lower canines. Placed 0.014-inch Ni-Ti Align SE maxillary and mandibular archwires.
Second appointment at 2 months 2 weeks: Placed maxillary and man-dibular 0.016- × 0.025-inch Ni-Ti Align SE archwires.
Third appointment at 5 months: Placed maxillary and mandibular posted 0.019- × 0.025-inch stainless steel archwires with Ni-Ti clos-ing springs hooked onto archwire distal to first molars(see Fig. 36-40).
Fourth appointment at 7 months, 1 week: Activated Ni-Ti springs, and clipped archwires distal to first molars (see Fig. 36-41).
Fifth appointment at 9 months, 3 weeks: Activated Ni-Ti springs, and started Class II elastics (Fig. 36-42).
Sixth appointment at 12 months: Bonded upper and lower second molars. Placed 0.016-inch Ni-Ti Align SE overlay archwire.
Seventh appointment at 14 months, 2 weeks: Adjusted maxillary archwire, and continued Class II elastics (night only), including anterior trapezoid.
Eighth appointment at 16 months: Adjusted both archwires. Started nighttime V-elastics and continued trapezoid elastics.
Ninth appointment at 17 months, 2 weeks: Adjusted maxillary arch-wire and continued V-elastics and anterior trapezoid elastics full time.
Tenth appointment at 19 months: Adjusted both archwires and contin-ued V-elastics and anterior trapezoid elastics.
Eleventh appointment at 20 months, 2 weeks: Adjusted maxillary archwire. Continued V-elastics and anterior trapezoid elastics, and scheduled debonding.
Twelfth appointment at 21 months, 2 weeks: Debonded both arches (see Fig. 36-43). Bonded 0.016-× 0.022-inch Bond-a-Braid braided wire onto the maxillary teeth lateral to lateral incisor. Bonded 0.026-inch stainless steel round wire onto the mandibular teeth canine to canine.
997.e130 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
A BFIGURE 36-40 A, B, To close space, the distal eyelet of nickel-titanium (Ni-Ti) coil spring was bent 90 degrees before its placement over the distal end of the cut archwire on the first molars.
A BFIGURE 36-41 A, In minimum anchorage retraction cases, cutting the archwire distal to the first molar and attaching the spring to the distal end of the first molar tube are recommended. B, In maximum anchorage retraction cases, ligating the first and second molars together while attaching the spring to the hook of the first molar is recommended.
FIGURE 36-42 Tenth appointment at 19 months for KH. V-elastics and anterior trapezoid elastics are configured.
distribute forces over all teeth. Eliminating bracket hooks keeps the appli-ance clean and promotes healthy tissue response and patient comfort.
Posttreatment records were taken at 21 months, 2 weeks (Fig. 36-43). Figure 36-44 provides a summary of the wire progression of phase 2 treat-ment. The author does not see how this favorable of a result could have been achieved without the premolar extractions. Maxillary retention was achieved with 0.016-× 0.022-inch Bond-a-Braid braided wire (Reliance
Orthodontic Products, Itasca, IL) bonded to each tooth lateral to lateral incisor. Mandibular retention was achieved with 0.026-inch stainless steel wire placed canine to canine and bonded to only the canines. Clear slip-cover retainers were made for both arches to help hold the extraction sites closed while the Class II splint was being fabricated (Fig. 36-45). To retain the Class II correction, the splint was worn nightly for 1 year, after which time the patient began wearing the slipcover retainers again only at night.
997.e131CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
A B C
D E F
G H
I
J
FIGURE 36-43 A-J, Posttreatment records for KH. Total treatment time: 18 months with 8 appointments of phase 1 treatment and 21 months, 2 weeks with 12 appointments of phase 2 treatment.
Continued
997.e132 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-3 Treatment with Extraction Therapy—cont’d
FIGURE 36-44 Summary of phase 2 wire progression treat-ment for KH is demonstrated.
FIGURE 36-45 Damon splint to retain Class II corrections (see description of appliance construction on page …)
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III DentitionsOne of the greatest challenges in clinical orthodontics is planning the treat-ment of nongrowing patients with a Class II dentition. So often, these cases have significant overbite or overjet in which the profile and lateral facial support will be greatly affected by treatment planning decisions. Most adults seeking orthodontic treatment desire far more than simply straight teeth. They are keenly aware of what the aging process is doing to their bite and face. With this system, the clinician now has many more opportunities to meet this challenge without negatively affecting the pro-file and lateral facial support and can, in fact, sometimes improve it.
Some clinicians consider dental correction of Class II and III cases with nothing more than elastics impossible, but with the use of the tube sys-tem and high-tech archwires, orthodontists around the world are able to treat certain patients with Class II and III elastics that conventional mechanics precludes. Case 4 (TBM) was selected to demonstrate how the Damon System and Class II elastics can correct a nongrowing patient with a Class II dentition if certain principles are followed. Using a Herbst appliance attached to the archwire was obviously the author’s first treat-ment choice, but the patient preferred to use elastics.
Patient TBM illustrates a combination of factors: a full Class II, Division 2 dentition; the necessity to level the curve of Spee; and moderate anterior crowding. Orthodontists using conventional mechanics would be neces-sarily apprehensive about treating such a case with Class II elastics for fear of severely dumping the lower anteriors. With traditional mechanics, the archwire is securely tied into each bracket and acts like a bridge beam. Each arch operates as a rigid unit against the other; any interference sig-nificantly slows anteroposterior correction. The Damon System functions similar to multiloop archwires, given the play between the archwire and the tube. With independent movement at every bracket, slight interferences do not shut down anteroposterior correction with Class II elastics. At the same time, using very low forces allows the lips and muscles of the face to act as a lip bumper, which precludes dumping the anteriors. Moreover, because second molars sit in cortical bone, the archwire is clipped distal to the first molars, allowing the second molars to drift independently. The gain in the transverse arch width not only helps accommodate the crowd-ing, but it also helps correct the Class II dentition.
TBM was a 40-year-old patient exhibiting a Class II, Division 2 dentition with a pleasing upper lip–to–nose relationship and a strong chin button (Fig. 36-46). She had a 100% overbite with overerupted incisors with
the upper central incisors too upright and labially inclined lower anterior teeth. The lower lip was slightly everted because of the position of the anterior dentition. She exhibited moderate crowding of both arches and a significant curve of Spee. Her lower left second premolar was congenitally missing, with a retained second primary molar occupying its space. Third molars had been extracted before treatment. The upper right central and lower right first molar had full porcelain crowns. Earlier in the author’s career, the author would have tried to distalize the molars or would have extracted upper first premolars. Either of these treatment options would have had a significant detrimental impact on the profile with the loss of upper lip support.
The treatment objectives were as follows: 1. Correct Class II molar and canine, eliminate crowding, and level the
curve of Spee without further dumping of the lower incisors. 2. Eliminate the option of extracting maxillary first premolars because of
the negative impact on the face. 3. Establish archform to give lateral facial support. 4. Control torque of maxillary and mandibular anterior segments. 5. Maintain attractive nose-to-lip relationship. 6. Minimize everting of lower lip.
Box 36-4 outlines the treatment sequence. With this low-force and tube technology, the overbite and torque were corrected with the selection of high-torque anterior brackets and tubes and a reverse curve Ni-Ti archwire with 20 degrees of torque. These appliance choices saved considerable time and allowed the clinician to start Class II elastics as soon as a 0.019- × 0.025-inch stainless steel wire is placed in the upper arch. This size of stainless steel archwire is strongly recommended to maintain the vertical dimension in the maxillary arch when pulling Class II elastics. Figure 36-50 provides a summary of the wire progression. Correcting the Class II molar and canine relationships, eliminating the crowding in both arches, and lev-eling the curve of Spee without severely dumping the lower incisors were encouraging results. In this case, the lower incisors actually uprighted slightly with only minimal anterior bodily movement. Cutting the lower archwire distal to the first molars before placing Class II elastics is always important (see Case Study 3). In some cases, the patient will position the jaw forward when sleeping, minimizing the effect of elastic wear. If so, then instructing the patient to wear two elastics on each side during sleep is important.
997.e133CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
Figure 36-51 illustrates comparisons of pretreatment and posttreatment upper arch plaster models, which show 3.5-mm change in canine width, 2-mm change in first premolar width, and 2.5-mm change in first molar width. Figure 36-52 illustrates comparisons of pretreatment and posttreat-ment models of lower arch plaster models, which show 1.5-mm change in canine width, 1.5-mm change in first premolar width, and 1.0-mm change in first molar width.
To be able to exceed this patient’s expectations for orthodontics by com-pleting treatment in 18 months, 1 week and with only 11 total appoint-ments was gratifying (see Fig. 36-49). With such treatment, outstanding patient cooperation is obviously required. Figure 36-53 shows the facial and intraoral results taken 19 months into retention that illustrate excellent stability.
G H I
D E F
A B C
FIGURE 36-46 A-K, Pretreatment records for case 4 (TBM, age 40 years). Diagnosis: Class II, Division 2 dentally; pleasing upper lip–to–nose relationship and strong chin button; 100% overbite, overerupted incisors, upper central incisors too upright, and labially inclined lower incisors with everted lower lip; moderate crowding in both arches and significant curve of Spee; lower left second premolar congenitally missing with retained second primary molar. Upper right central and lower right first molar had full porcelain crowns. Third molars were extracted before treatment.
Continued
997.e134 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
First appointment: Because this patient elected to wear Class II elas-tics rather than a Herbst appliance, she wore them for an extended period; consequently, high-torque brackets on the upper incisors (+17 degrees on the upper central incisors and +12 degrees on the upper lateral incisors) were selected to prevent the central incisors from uprighting too much. Low-torque brackets were selected for the lower incisors (−6 degrees) to keep them from flaring during extended Class II elastics wear. Bonded upper and lower arches 7 to 7, except for broken-down lower left first molar where a band was placed for support. Placed separators for band. Placed a 0.014-inch Ni-Ti Align SE archwire in the upper arch and a 0.014-inch Ni-Ti Align SE sectional archwire in the lower arch (the lower left first molar was not bondable). Made night-time soft splint for lower arch.
Second appointment at 2 months, 2 weeks: Placed a 0.017- × 0.025-inch Ni-Ti reverse curve with 20-degree torque in the upper arch. Banded lower left first molar. Placed a 0.016-inch Ni-Ti Align SE in the lower arch.
Third appointment at 5 months: Inserted a 0.018- × 0.025-inch Ni-Ti Align SE in the maxilla as a transitional wire between the 0.017- × 0.025-inch Ni-Ti reverse curve and the 0.019- × 0.025-inch stainless steel finishing archwire. Without this transitional wire, going from the reverse curve to the finishing archwire would have been too uncom-fortable for the patient. (The reverse curve with +20-degree torque placed at the previous appointment worked exceptionally well in this instance. Sometimes a 0.019- × 0.025-inch reverse curve with torque is needed.) Placed a 0.016- × 0.025-inch Ni-Ti Align SE in the man-dible.
Fourth appointment at 7 months, 1 week: Placed a 0.019- × 0.025-posted stainless steel archwire in both arches. Took pan-oramic radiograph. Started full-time Class II elastics (5⁄16-inch, 6-oz) wear. Clipped lower archwire distal to lower first molars. Doing so is
critically important to be able to correct Class II dentitions with elas-tics because the second molar roots are usually positioned in cortical bone of low vascularity.
Fifth appointment at 9 months, 1 week: Continued Class II elastics. Recommend two elastics on each side at bedtime if patient postured mandible forward while sleeping.
Sixth appointment at 10 months, 3 weeks: Checked patient. Contin-ued Class II elastics.
Seventh appointment at 12 months, 1 week: Adjusted maxillary arch-wire with tiebacks (Fig. 36-47). Continued Class II elastics.
Eighth appointment at 14 months: Placed a 0.014- × 0.025-inch Ni-Ti Align SE in the mandible with tiebacks. Used a 0.014- × 0.025-inch Ni-Ti Align SE to incorporate second molars. Left for one appoint-ment. Continued Class II elastics.
Ninth appointment at 15 months, 2 weeks: Maintained the 0.019- × 0.025-inch posted stainless steel archwires in the maxilla. Placed a 0.016- × 0.025-inch posted stainless steel archwire in the mandi-ble for desired play between the archwire and the bracket lumen to improve settling and finishing. Began full-time V-elastics. Changed Class II elastics wear from full time to night only.
Tenth appointment at 17 months: Adjusted maxillary and mandibular archwires (Fig. 36-48). Maintained same elastic wear. Prepared to debond.
Eleventh appointment at 18 months, 1 week: Debonded both arches and placed retention wires (Fig. 36-49). Bonded a 0.016- × 0.022-inch Bond-a-Braid braided wire onto the maxillary teeth lateral to lateral incisor. Bonded 0.026-inch stainless steel round wire onto the man-dibular teeth canine to canine. Prescribed the Damon splint be worn nightly for 10 to 12 months (length of time prescribed for each patient depends on the severity of the case). Also prescribed regular slip-cover retainers in addition to splint.
BOX 36-4 Case 4 (TBM) Treatment Sequence
J
K
FIGURE 36-46, cont’d
997.e135CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
B
DD
A
C
E
FIGURE 36-47 A-E, Seventh appointment for TBM at 12 months, 1 week.
Continued
997.e136 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
B
EE
DD
A
C
FIGURE 36-48 A-E, Tenth appointment for TBM at 17 months.
997.e137CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
C D E
IH
GF
A B
FIGURE 36-49 A-I, Posttreatment records for TBM. Total treatment time: 18 months, 1 week with 11 appointments.
Continued
997.e138 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
FIGURE 36-50 Archwire sequence for TBM is demonstrated.
39.5 mm
30 mm
41.5 mm
33.5 mm
A
B
FIGURE 36-51 Comparisons of pretreatment and posttreat-ment upper arch plaster models for TBM. A, Pretreatment. Canines: 30 mm; first premolars: 39.5 mm; first molars: 49.0 mm. B, Posttreatment. Canines: 33.5 mm; first premolars: 41.5 mm; first molars: 51.5 mm. Pretreatment and posttreat-ment models of upper arch show 3.5-mm change in canine width, 2-mm change in first premolar width, and 2.5-mm change in first molar width.
39.5 mm
25 mm
41 mm
26.5 mm
A
B
FIGURE 36-52 Comparisons of pretreatment and posttreat-ment lower arch plaster models for TBM. A, Pretreatment. Canines: 25 mm; first premolars: 39.5 mm: first molars: 50.0 mm. B, Posttreatment. Canines: 26.5 mm; first premolars: 41.0 mm; first molars: 51.0 mm. Pretreatment and posttreat-ment models of lower arch show 1.5-mm change in canine width, 1.5-mm change in first premolar width, and 1.0-mm change in first molar width.
997.e139CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-4 Treatment with Elastics of Nongrowing Patients with Class II and III Dentitions—cont’d
D E F
GG H
A CB
FIGURE 36-53 A-H, Comparisons of facial and intraoral results at 19 months into retention for TBM demonstrate excellent stability.
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open BiteCase 5 (AB) was selected to show how low-force and tube treatment mechanics affect alveolar bone. The patient strongly opposed the surgi-cal options presented. Before the advent of the Damon System technol-ogy, this patient could only have been treated surgically. CT scans taken the day of debonding clearly illustrate that if forces are biologically sensi-ble, then the alveolar bone will follow the bodily movement of the teeth. AB was nearly 37 years old when he sought treatment after observing the results his brother experienced in the author’s practice. He had Class III dentition with a severe open bite and a bilateral posterior crossbite (Fig. 36-54). He complained of airway problems and said he was chal-lenged to enunciate clearly when making presentations. Both brothers were severe tongue thrusters, and to close the right posterior open bite was challenging for both of them. He is a vertical grower with a long lower facial height, long tooth roots, and midface deficiency. His upper and lower midline was off when placing the mandible in centric relation.
The treatment objectives were as follows: 1. Using low-force, low-friction mechanics, allow the orofacial muscu-
lature, bone, and soft tissue to establish a new physiologically deter-mined tooth position that allows more room for the tongue.
2. Correct Class III molar relationship and bilateral posterior crossbite. 3. Increase maxillary posterior arch width to accommodate crowding. 4. Improve midface support by moving maxillary dentition forward. 5. Improve cant of occlusal plane, if possible. 6. Correct anterior open bite. Retain case to preclude tongue thrust from
reopening bite.Box 36-5 outlines the treatment sequence for this patient. Special
torques were selected: +17 degrees for the upper central incisors, +10 degrees for the upper lateral incisors, and +7 degrees for the upper and lower canines. Figure 36-56 compares the plaster models of the upper arches taken initially and on the day of debonding with vertically cut
Continued
997.e140 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open Bite—cont’d
D
E F G
A CB
FIGURE 36-54 A-K, Pretreatment records for case 5 (AB, age 36 years, 11 months). Diagnosis: Class III dentally, severe open bite, bilateral posterior crossbite, midline off center with long lower facial height, long tooth roots, and midface deficiency; airway and enunciation problems. Patient desired an alternative to surgery.
997.e141CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open Bite—cont’d
I
K
H
J
FIGURE 36-54, cont’d
First appointment: Bonded maxillary and mandibular arches 7 to 7. Placed 0.014-inch Ni-Ti Align SE in both arches.
Second appointment at 2 months, 2 weeks: Rebonded lower right lat-eral and replaced 0.014-inch Ni-Ti Align SE. Placed maxillary 0.014- × 0.025-inch Ni-Ti Align SE.
Third appointment at 4 months, 1 week: Placed mandibular 0.016-inch Ni-Ti Align SE. Patient missed appointments for the next several months.
Fifth appointment at 10 months, 2 weeks: Placed maxillary 0.019- × 0.025-inch posted stainless steel. Placed mandibular 0.016- × 0.025-inch stainless steel. Bonded lingual buttons to upper first molars. Started full-time posterior cross elastics and full-time Class III 5⁄16-inch, 6-oz elastics.
Sixth appointment at 13 months: Adjusted upper and lower archwire. Continued full-time wear of Class III elastics. Changed posterior cross elastics to nighttime wear.
Seventh appointment at 14 months, 2 weeks: Adjusted maxillary arch-wire. Started full-time 5⁄16-inch, 6-oz posterior V-elastics and anterior trapezoid elastics.
Eighth appointment at 16 months: Adjusted maxillary archwire. Con-tinued same elastics wear.
Ninth appointment at 17 months, 3 weeks: Adjusted maxillary and mandibular archwires. Continued same elastics wear.
Tenth appointment at 19 months, 1 week: Adjusted maxillary and man-dibular archwire. Continued same elastics wear.
Eleventh appointment at 20 months, 3 weeks (Fig. 36-55): Debonded both arches. Bonded 0.016- × 0.022-inch Bond-a-Braid braided wire onto the maxillary teeth lateral to lateral incisor. Bonded 0.026-inch stainless steel round wire onto the mandibular teeth canine to canine. Fabricated slipcover retainers for upper and lower arches. Fabricated Damon splint for nighttime wear.
BOX 36-5 Case 5 (AB) Treatment Sequence
CT scans also taken the day of debonding. The maxillary canine width increased 3 mm, the first premolar width increased 8 mm, the second premolar width increased 5 mm, and the first molar width increased 4.5 mm. The CT scans show positive alveolar bone response to signif-icant lateral and vertical tooth movement, once again demonstrating that using biologically sensible forces will cause the alveolar bone to follow the movement of teeth in all planes of space with minimal tip-ping. (Note that the cut of the horizontal CT scans are tipped toward
the anterior segment of the arch.) Using simple mechanics, this patient was treated in 20 months, 3 weeks with 11 office visits (see Fig. 36-55). Retaining these types of complex cases with a night muscle-training splint and lingually bonded wires on both the upper and lower anteri-ors is essential. Despite significant tooth movement, the photographs taken the day of debonding show a positive tissue response. The hor-izontal CT scan of the upper arch taken at debonding (Fig. 36-57) illus-trates the well-shaped archform.
Continued
997.e142 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open Bite—cont’d
I
GG H
D E F
A B C
FIGURE 36-55 A-I, Posttreatment records for AB. Total treatment time: 20 months, 3 weeks with 11 appointments.
997.e143CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open Bite—cont’d
B
D
E
33.5 mm
33.5 mm
41.5 mm
48.5 mm
30.5 mm
43.5 mm
A
C
FIGURE 36-56 Comparisons of pretreatment and posttreatment upper arch plaster models for AB with computed tomographic scans. A, Pretreatment. Canines: 30.5 mm; first premo-lars: 33.5 mm; second premolars: 43.5 mm; first molars: 49 mm. B, Posttreatment. Canines: 33.5 mm; first premolars: 41.5 mm; second premolars: 48.5 mm; first molars: 53.5 mm. Initial and final models of upper arch show a 3-mm change in canine width, 8-mm change in first premolar width, 5-mm change in second premolar width, and 4.5-mm change in first molar width. Vertical computed tomographic scans taken the day of debonding show healthy alveo-lar bone. C, Scan of upper first premolars at debonding. D, Scan of upper second premolars at debonding. E, Scan of upper first molars at debonding.
Continued
997.e144 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-5 Treatment of a Nongrowing Patient with a Class III Severe Posterior Crossbite and Anterior Open Bite—cont’d
Treatment with the Herbst Appliance of Growing Patients with Skeletal Class II DentitionThis section includes some of the author’s findings with the Herbst appliance after using it for longer than 24 years, treating more than 3000 patients, and following many of these patients for a number of years. Obviously, improvement in the technol-ogy continues to affect how orthodontists use and apply any appliance system. The author intends to give an overview of how this technology is used to treat some of the most challeng-ing cases. (See also Chapter 16.)
The Herbst appliance is one of the most powerful treat-ment options in orthodontics. Combining the low-force and tube system with the Herbst appliance gives the clinician the opportunity to convert complex and long-term treatment situations into straightforward treatment using noncom-pliance mechanics for superior clinical results. After hav-ing the opportunity to lecture around the world, the author has found that many clinicians have a negative view of the Herbst appliance and its clinical application. Many of these views are justified when discussions center only around its impact on the A point–nasion–B point (ANB) angle. The author has observed great variation in what does or does not happen to the ANB angle with the use of the Herbst appli-ance. The author’s interest in using the appliance focuses far more on its functional impact on the entire orofacial com-plex rather than its effect on the ANB. Although a positive response in the ANB angle is helpful, the ANB simply does not change in some cases. Although the ANB angle may not
be positively affected, so many positive things do happen when the patient is given a second chance for the entire den-tofacial complex to function in a more normal manner. If the mandible is slowly advanced over an extended period, then the impact can be dramatic in growing and nongrowing patients. Orthodontists have seen patients who had a narrow upper arch and a severe Class II skeletal pattern. This situa-tion is an example of a functional adaptation of the alveolar process and dentition reacting to the musculature altered by the anteroposterior position of the mandible. If the man-dibular position is slowly normalized, then clinicians often observe teeth and alveolar process responses even without orthodontic intervention.
Clinical Principles for Using the Herbst ApplianceOrthodontists know that growth of young patients occurs over a long period. Recognizing that the body needs time to react to a given functional change has always seemed logical. The form-follows-function adage is appropriate when using the Herbst appliance. The author’s favorite time to start Herbst appliance treatment is when the young patient’s growth starts to accelerate. Some exceptions are severe cases and those patients with self-esteem and special growth issues. The average Herbst appliance starting age for girls is 10½ to 11 years; boys are later at 11 to 11½ years of age.
The author strongly recommends advancing the Herbst appliance only 4.0 to 4.5 mm at the beginning of treatment. Slowly activating the appliance over a long period has many
FIGURE 36-57 The horizontal computed tomographic scan of upper arch at debonding illus-trates the well-shaped archform in AB.
997.e145CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
advantages. The author prefers not to advance the condyle more than two thirds of the way down the articular eminence. This small advancement of the mandible lessens the Class II elastic effect on the musculature and thereby minimizes the for-ward proclination (dumping) of the lower incisors. With this small advancement, the author relies on the functional effect of the Herbst appliance and muscles to initiate lateral upper arch adaptation naturally, negating the need for high-force pala-tal expansion before placing the Herbst appliance. As the Herbst appliance advances the mandible, the combined impact of the V-shape of the mandible, the usual presence of an upper arch-wire connecting the four anteriors to the molars, and the Herbst rods foster a slow and natural lateral change in the maxilla with little dental tipping. Surprisingly, this lateral adaptation of the palate is not age specific.
The second Herbst appliance advancement of approximately 3 mm is performed 5 to 6 months into treatment. Once again, the activation is allowed an interval of approximately 5 months for the muscles to adapt. Using the same principles, activations thereafter are applied according to each patient’s specific needs for skeletal correction. In most cases, activation is terminated when the upper and lower anterior teeth are end to end. The average length of treatment is 14 to 16 months. (In severe appli-cations, treatment time is extended to 2 years or longer.) If a patient relapses during the full-bonded phase of treatment, then the author gives the Herbst appliance a second opportunity to work directly on the archwire. Some of the most successful cases the author has treated have resulted from more than one appli-cation of the Herbst appliance.
Patients treated with the Herbst appliance require special retention that is critical to long-term success. The length of time specified for a nightly splint to be worn after debonding in the case studies is an example. The activator-type retainer is most important to the success of this type of treatment.
Working together, the low-force and tube technology and the Herbst appliance provide a powerful combination that allows the clinician to simplify treatment mechanics and con-vert the most challenging cases to routine clinical orthodontics. Slowly advancing the Herbst appliance, allowing it work for a long period, and retaining it with a night splint are the key ele-ments for success. Most of the Herbst appliance research to date has been on patients who have been rapidly activated, treated over a significantly shorter period, and released without antero-posterior retention.
Clinical Application of the Herbst ApplianceThe author uses the Herbst appliance in several different ways in timing and treatment application: • Mixed dentition Herbst appliance therapy with and without
anterior brackets • Archwire Herbst appliance therapy in patients with full den-
tition • Archwire Herbst appliance therapy for patients with tem-
poromandibular joint problems • Archwire Herbst appliance therapy with coil springs as a
supplement for Class II elasticsThe following two cases demonstrate Herbst application in
the author’s practice.
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical ResponseCase 6 (KP) 12 years, 5 months of age was selected to demonstrate the typical response to standard Herbst appliance treatment. Pretreatment records (Fig. 36-58) indicate her to be a Class II, Division 1 case with a retrusive mandible and narrow midface. She exhibited a good chin button but with poor tissue contour under her chin. She demonstrated a mod-erate overeruption of lower incisors, flared upper incisors, and lingually inclined upper and lower canines with the typical narrowing of the anterior maxillary arch in patients with a Class II dentition.
The treatment objectives were as follows: 1. Achieve facial balance and symmetry of nose, lips, and chin. 2. Create maxillary and mandibular posterior arch width to support mid-
face with low-force mechanics. 3. Establish maxillary and mandibular incisor position to give natural lip-to-
tooth relationship. 4. Exert a positive impact on the archwires.
The pretreatment profile makes it apparent that the mandible is growing slower than the maxilla. Treatment plans that attempt to move the maxilla or dentition distally to meet a deficient mandible often leave patients with a prominent nose, lack of upper lip support, and a weak chin. In such cases, the author has always found it more conducive to create an environment for mandibular change. Box 36-6 outlines the phase 1 Herbst appliance treatment sequence. The impact Herbst appliance treatment had on this patient’s facial balance and dentition is positive. Using Herbst appliance
therapy before bonding means that the orthodontic treatment is initiated on a simple Class I case with the increased maxillary arch width, eliminat-ing the need for high-force palatal expansion (see Fig. 36-61). An interest-ing note is that this patient’s upper first premolar width change was less than is normally observed with Herbst appliance treatment. The tongue did not completely reposition itself until after fully bonded treatment was started, which added an additional 5-mm width gain after Herbst appliance treatment. Combining the Damon System with Herbst appliance therapy simplifies treatment planning, minimizes the need for patient cooperation, and yields rewarding results. Box 36-7 outlines the phase 2 posttreatment Herbst appliance sequence.
The combination of Herbst appliance therapy and Damon System mechanics achieved excellent facial balance (see Fig. 36-64). Figure 36-65 outlines the posttreatment sequence with the Herbst appliance archwire. Figure 36-66 illustrates the comparisons of the initial and final models of upper arch, which show 5.5-mm change in canine width, 10.5-mm change in first premolar width, and 7-mm change in first molar width. Figure 36-67 illustrates the comparisons of the initial and final models of lower arch, which show 0.5-mm change in canine width, 2-mm change in first pre-molar width, and 0.5-mm change in first molar width. One-year retention records illustrate good stability (Fig. 36-68). CT scans taken 2 years, 6 months into retention (Fig. 36-69) signify healthy alveolar bone and good archform.
Continued
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
A
D E
G H
JI
F
B C
FIGURE 36-58 A-L, Pretreatment records for case 6 (KP, age 12 years, 5 months). Diagno-sis: Class II, Division 1 with retrusive mandible, narrow midface, a good chin button but with excessive tissue under her chin; moderate over-eruption of lower incisors, flared upper inci-sors, and lingually inclined upper and lower canines with the narrowing of anterior maxillary arch that is typical in patients with Class II dentition.
997.e147CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
Start: Took tomograms.First appointment: Placed Flip-Lock Herbst appliance (TP Orthodontics,
Inc., La Porte, IN) (Fig. 36-59). Selected special high torques for upper central incisors (+17 degrees) and lateral incisors (+12 degrees). Bonded upper central and lateral incisors. Placed sectional 0.014-inch Ni-Ti Align SE extending from maxillary right canine to maxillary left lateral incisor with the ends of the wire heat treated and bent for comfort, leaving enough room for the anterior teeth to align. Initially activated Herbst appliance 4.5 mm.
Second appointment at 2 months, 3 weeks: Placed maxillary and man-dibular 0.017- × 0.025-inch titanium molybdenum alloy (TMA) arch-wire with moderate intrusive bends anterior to the molar tubes. This wire was inserted in tubes soldered to the first molar Herbst crowns.
Third appointment at 6 months: Placed maxillary and mandibular 0.019- × 0.025-inch TMA archwire with moderate intrusive bends to intrude anterior teeth. This wire was inserted in the tubes of the first molar Herbst appliance crown. Added 2-mm shims.
997.e148 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
FIGURE 36-59 Flip-Lock Herbst appliance used to treat KP.
A
B
FIGURE 36-60 A, B, Tomograms taken at the sixth appointment of phase 1 Herbst appliance treatment for KP.
997.e149CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
Continued
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
A B
DC
FIGURE 36-61 A-D, Phase 1 posttreatment records of KP with Herbst appliance (Herbst appliance treatment time: 16 months with seven appointments). Records taken after Herbst appliance treatment demonstrate Class I dentition and improved facial symmetry.
This patient’s canines were slightly toed in. Selected special torques (+7 degrees) for upper and lower canines to help upright them.
First appointment: Bonded maxillary and mandibular 7 to 7. Placed continuous maxillary and mandibular 0.014-inch Ni-Ti Align SE archwires with crimpable stops.
Third appointment at 4 months, 3 weeks: Took panoramic radiograph to evaluate root angulations and bracket positions (Fig. 36-62).
Fourth appointment at 7 months, 2 weeks: Placed maxillary 0.019- × 0.025-inch posted stainless steel archwire with tiebacks. Placed mandibular 0.016- × 0.025-inch posted stainless steel archwire with tiebacks, which kept the play in the bracket tube to help elim-inate binding and help close the posterior occlusion when trying to close the bite vertically. Started bilateral V-elastics.
Fifth appointment at 9 months, 3 weeks: Adjusted upper and lower archwires. Continued full-time V-elastics. Added Class II elastics for night wear only.
Sixth appointment at 12 months: Adjusted maxillary and mandibular archwires. Posterior occlusion was hard to close because of tongue repositioning.
Seventh appointment at 13 months, 2 weeks: Checked occlusion. Continued full-time elastics.
Eighth appointment at 15 months, 1 week: Adjusted maxillary and mandibular archwires. Continued full-time elastics.
Ninth appointment at 17 months: Debonded arches (Fig. 36-64). Initiated fixed retention by bonding 0.016- × 0.022-inch Bond-a-Braid braided wire onto the maxillary teeth lateral to the lateral incisor and bonding 0.026-inch stainless steel round wire onto the mandibular teeth canine to canine because of the severity of the initial crowding. The patient was instructed to wear clear plastic overlay retainers for upper and lower arches and the Damon splint for night retention for an activator type of effect until patient is finished growing.
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
FIGURE 36-62 Phase 2 Panorex for KP.
B
D
A
E
C
FIGURE 36-63 A-E, Phase 2 fourth appointment at 7 months, 2 weeks for KP.
997.e151CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
C D E
H
A B
GF
FIGURE 36-64 A-H, Posttreatment records for KP. Total phase 1 and phase 2 treatment time: 33 months with 16 appointments.
Continued
997.e152 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
FIGURE 36-65 Post–Herbst appliance archwire sequence for KP is demonstrated.
A BA
29.5 mm
35.5 mm
35 mm
46 mm
FIGURE 36-66 Comparisons of pretreatment and posttreatment upper arch plaster models for KP. A, Pretreatment. Canines: 29.5 mm; first premolars: 35.5 mm; first molars: 48.5 mm. B, Posttreatment. Canines: 35 mm; first premolars: 46 mm; first molars: 55.5 mm. Initial and final models of upper arch show 5.5-mm change in canine width, 10.5-mm change in first premolar width, and 7-mm change in first molar width.
A BA
25.5 mm
33 mm
26 mm
35 mm
FIGURE 36-67 Comparisons of pretreatment and posttreatment lower arch plaster models for KP. A, Pretreatment. Canines: 25.5 mm; first premolars: 33 mm; first molars: 44.5 mm. B, Posttreatment. Canines: 26 mm; first premolars: 35 mm; first molars: 45.0 mm. Initial and final models of lower arch show 0.5-mm change in canine width, 2-mm change in first premo-lar width, and 0.5-mm change in first molar width.
997.e153CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-6 Youth with Herbst Appliance Treatment Demonstrates Typical Response—cont’d
G H
A B C
D E F
FIGURE 36-68 A-H, Retention records for KP at 1 year in retention.
A B
FIGURE 36-69 Horizontal computed tomographic scans of KP’s upper arch (A) and lower arch (B) taken after 2 years, 6 months in retention.
997.e154 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive ResponseThis case was selected because it definitively demonstrates what the Damon System has to offer: a gold standard for gaining space in a full Class II occlusion. By simply normalizing the position of the mandible, the muscles of the face and tongue have a completely different impact on the surrounding structures, which gives the patient a second chance for nor-mal physiologic adaptation to take place. This case is also a great example
of form after function. What is exciting is that with a little time and effort, using simple mechanics, and allowing physiologic adaptation to occur, the patient can be treated with respect for the maturing face and profile.
Case 7 (KR) was 11 years, 6 months of age with a Class II, Division 2 crowded dentition (Fig. 36-70). She had a prominent nose but a good chin button. She lacked lateral facial support and arch length and width in both
A B C
D E F
G H
I
JK
E
B C
FIGURE 36-70 A-M, Pretreatment records for case 7 (KR, age 12 years, 5 months). Diagno-sis: Class II, Division 2 crowded dentition; retrusive mandible and lacking lateral facial support, arch length and arch width in both arches; 100% overbite, overerupted upper and lower inci-sors; prominent nose and good chin button.
997.e155CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
arches. She had 100% overbite with overerupted upper and lower central and lateral incisors. Her retrusive mandible was likely to become more pronounced with maturity. What happens long-term to the maturing pro-file is well documented. This anticipated profile change calls for treatment mechanics that will move the upper incisors forward, giving increased den-tal support to the upper lip and, at the same time, helping minimize the prominence of the nose. As the nasolabial angle decreases, room is being made for the erupting upper canines. This anterior dental movement also allows room for Herbst appliance therapy to slowly position the mandible forward into a more normal anteroposterior position. In other words, the lower arch is fitted to the upper as much as growth and development will allow.
The treatment objectives were as follows: 1. Design treatment mechanics in anticipation of the long-term impact on
the patient’s face and profile. 2. Achieve facial balance and symmetry.
3. Establish maxillary anteroposterior position and posterior width to sup-port the midface.
4. Gain maxillary arch length. 5. Establish ideal maxillary tooth-to-lip relationship. 6. Achieve physiologically sound tooth position. 7. Design treatment mechanics to position the deficient mandible to the
maxilla as growth and development permit.Tomograms were taken before starting phase 1 Herbst appliance ther-
apy. Special high-torque central incisors (17 degrees) and lateral incisors (10 degrees) were selected. These central torques are selected for Divi-sion 2 cases. High torques are also the choice for central and lateral inci-sors for cases requiring Class II elastics to prevent loss of torque control from the elastic wear; they also are suitable for most extraction cases to prevent loss of torque control when retracting anterior teeth. At the start of treatment, a maxillary 0.014-inch Ni-Ti Align SE sectional archwire was placed lateral to lateral incisor, and the Herbst appliance was placed
M
L
FIGURE 36-70, cont’d
Continued
997.e156 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’dand advanced just short of the incisors. At the second appointment (2 months, 2 weeks), a 0.017- × 0.025-inch TMA archwire (Ormco Corpo-ration, Orange, CA) with light intruding bends was placed. Light intrusion bends were used to minimize molar tube binding, and medium-light Ni-Ti coil springs were placed on the wire (engaging the molars) and activated twice the width of the bracket. Light C-chains were placed lateral to lateral incisor to consolidate space. Box 36-8 presents the phase 1 Herbst appli-ance treatment sequence.
Phase 1 therapy was completed in 18 months with nine appointments. KR had responded well with impressive lateral arch development resulting
from the Fränkel effect of the Herbst appliance and archwire —a natu-ral expander without force. Initial and after treatment, Herbst appliance upper model comparisons (see Fig. 36-74) reveal increases of 8 mm in first premolar width and 6 mm in first molar width, with Figure 36-75 illustrat-ing the posttreatment Herbst appliance cephalometric tracing composite. Before the use of the Herbst appliance and tube technology, the author’s usual treatment options were headgear, upper first premolar extractions, or distalizing upper molars to make room for blocked-out canines. These types of treatment had a detrimental long-term impact on the nasolabial angle and profile of the maturing face.
Phase 2 treatment was immediately initiated after phase 1, with full bonding of upper and lower arches and placement of 0.014-inch Ni-Ti Align SE archwires. Phase 2 treatment was completed in 14 months, 2 weeks with eight appointments. Box 36-9 shows the phase 2 Herbst appliance posttreatment sequence. Posttreatment records (see Fig. 36-76) include a cephalometric tracing composite and a panoramic radio-graph. Comparing these records with pretreatment records reveals a pleasing result that accommodated the maturing profile changes seen in retention. Initial and final upper model comparisons (Fig. 36-77) reveal increases of 11 mm in first premolar width, 10 mm in second premolar width, and 7.5 mm in first molar width. Bodily movement and limited cor-rective tipping are apparent. Lower model comparisons (Fig. 36-78) show a 0.5-mm arch width increase in the canines and 5-mm width increase in the first molars.
With the Damon System, teeth can be moved and bone will follow; how-ever, the muscles must be given time to adapt, which is why a splint was required for retention. The Damon splint (See Finishing Phase discussion) is made for nightly wear to provide an activator-type effect until the patient has completed growing. The author uses splints in 30% of all cases, 100% of Herbst appliance and Class II elastic cases, and for anyone with muscle dys-function or temporomandibular joint problems. KR wore her splint at night for 12 months after debonding.
Maxillary retention was achieved with 0.016- × 0.022-inch Bond-a-Braid braided wire bonded to each tooth lateral to lateral incisor and left in place for approximately 2 years. Permanent mandibular retention was achieved with 0.026-inch stainless steel wire placed canine to canine and bonded to only the canines. Clear slipcover retainers were fabricated for use after nightly splint wear. Figure 36-79 shows facial photographs 20 months in retention. Horizontal CT scans of upper and lower arches (Fig. 36-80) were taken 3 years in retention. The healthy alveolar bone and excellent arch-forms are evident.
Start: Took tomograms.First appointment: Placed Herbst appliance, and bonded upper cen-
tral and lateral incisors (high torques). Placed 0.014-inch Ni-Ti Align SE sectional archwire lateral to lateral incisor. Advanced Herbst appliance just short of incisors (Fig. 36-71).
Second appointment at 2 months, 2 weeks: Placed maxillary 0.017- × 0.025-inch TMA archwire with light intruding bends. Placed medium-light Ni-Ti coil springs and activated 2 times width of bracket. Placed light C-chain lateral to lateral incisor to consolidate space (Fig. 36-72).
Third appointment at 5 months: Activated Herbst appliance with shims just short of anterior teeth. Placed maxillary 0.019- × 0.025-inch TMA archwire with light intruding bends. Activated medium-light Ni-Ti coil springs.
Fourth appointment at 7 months, 2 weeks: Added 3-mm shims, and checked length of archwire in molar tube.
Fifth appointment at 10 months: Replaced maxillary 0.019 × 0.025 TMA with a longer one.
Sixth appointment at 12 months, 2 weeks: Added 3-mm shims.Seventh appointment at 15 months: Checked appliance and
increased intrusion bends in upper archwire.Eighth appointment at 16 months, 2 weeks: Took tomograms and
added 1-mm shims (Fig. 36-73).Ninth appointment at 18 months: Removed Herbst appliance, took
progress records (Figs. 36-74 and 36-75), conducted progress con-sultation, and arranged for full bonding.
FIGURE 36-71 First appointment. Herbst appliance disarticu-lated and bonded upper anteriors are used to start KR in phase 1 treatment.
FIGURE 36-72 Second appointment at 2 months, 2 weeks for KR.
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
A
B
FIGURE 36-73 A, B, Tomograms taken during the eighth appointment at 16 months, 2 weeks for KR.
A B
30 mm 38 mm
FIGURE 36-74 Comparisons of pretreatment and posttreatment with Herbst appliance upper arch plaster models for KR. A, Pretreatment. First premolars: 30 mm; first molars: 45 mm. B, Posttreatment. First premolars: 38 mm; first molars: 51 mm. Before and after treatment with Herbst appliance plaster models of upper arch show 8-mm change in first premolar width and 6-mm change in first molar width.
Continued
997.e158 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
FIGURE 36-75 Cephalometric tracing composite at posttreat-ment with Herbst appliance for KR.
First appointment: Fully bonded upper and lower arches, and placed 0.014-inch Ni-Ti Align SE archwires.
Second appointment at 2 months, 2 weeks: Placed maxillary 0.016- × 0.025-inch and mandibular 0.014- × 0.025-inch Ni-Ti Align SE archwires.
Third appointment at 5 months: Placed maxillary 0.019- × 0.025-inch posted stainless steel archwire and mandibular 0.018- × 0.025-inch Ni-Ti Align SE archwire. Took panoramic radiograph and checked root position and bracket placement.
Fourth appointment at 7 months, 2 weeks: Placed mandibular 0.019- × 0.025-inch posted stainless steel archwire, and started full time Class II elastics.
Fifth appointment at 10 months: Adjusted maxillary archwire, and con-tinued full time Class II elastics.
Sixth appointment at 11 months, 2 weeks: Adjusted archwires, and cut Class II elastic wear to half time.
Seventh appointment at 13 months: Adjusted maxillary archwire torque, and added bilateral V-elastics.
Eighth appointment at 14 months, 2 weeks: Debonded both arches. Bonded 0.016- × 0.022-inch Bond-a-Braid braided wire onto the max-illary teeth lateral to lateral incisor and placed a 0.026-inch stainless steel wire onto the mandibular teeth canine to canine, bonding only the canines. Made upper and lower slipcover retainers for full-time wear and Damon splint for nightly wear (Fig. 36-76).
BOX 36-9 Case 7 (KR) Treatment Sequence: Phase 2 After Herbst Appliance Treatment
997.e159CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
A B C
D E F
G H I
J
K
FIGURE 36-76 A-K, Posttreatment records for KR. Total treatment time: 14 months, 2 weeks with eight appointments.
Continued
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
A B
30 mm
38 mm
41 mm
48 mm
FIGURE 36-77 Comparisons of pretreatment and posttreatment upper arch plaster models for KR. A, Pretreatment. First premolars: 30 mm; second premolars: 38 mm; first molars: 45 mm. B, Posttreatment. First premolars: 41 mm; second premolars: 48 mm; first molars: 52.5 mm. Pretreatment and posttreatment plaster models of upper arch show 11-mm change in first premolar width, 10-mm change in second premolar width, and 7.5-mm change in first molar width.
B
25.5 mm
A
25 mm
FIGURE 36-78 Comparisons of pretreatment and posttreatment lower arch plaster models for KR. A, Pretreatment. Canines: 25 mm; first molars: 41 mm. B, Posttreatment. Canines: 25.5 mm; first molars: 46 mm. Pretreatment and posttreatment plaster models of lower arch show 0.5-mm change in canine width and 5-mm change in first molar width.
A CB
FIGURE 36-79 A-C, KR at age 16 years, 3 months with longer than 20 months in retention.
997.e161CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
CASE STUDY 36-7 Youth with Herbst Appliance Treatment Demonstrates the Definitive Response—cont’d
A B
C
FIGURE 36-80 A-C, Computed tomographic scans of KR’s upper and lower arches 3 years in retention. The healthy medullary bone and excellent archforms are evident.
DAMON SYSTEM ESSENTIALSDamon System ApplianceThe preadjusted Damon appliance (Fig. 36-81) is available in 0.022- and 0.018-inch slots. The author prefers the 0.022-inch dimension because the larger slot allows greater flexibility in the selection of archwire sizes and materials. Considering the arch-wire progression possibilities for each size, the author believes that the 0.022-inch slot maximizes the potential for keeping forces in the optimal force zone. A small wire in a large lumen is most favorable for tooth movement because it diminishes the divergence of angles in the archwire slot, allowing freer move-ment. Those who prefer the 0.018-inch slot to work with lighter forces will find that with the Damon System, the 0.022-inch slot affords that advantage. When used with the recommended archwire progression, the greater play allows faster, unrestricted tooth movement and a more comfortable patient.
The Damon tube is manufactured by metal injection mold-ing, which is the most precise process today to manufacture metal brackets and tubes. The metal injection molding process makes it possible to manufacture exceedingly small, accurate parts that allow movement of the slide and to provide the close tolerances of the archwire slot. Opening the slide in the latest D3 version is achieved with an opening tool, whereas closing requires only finger pressure. Upper tubes open incisally and lower tubes open gingivally to provide the best visibility when checking archwire placement.
Damon Standard PrescriptionThe Damon standard prescription is recommended for all molars and premolars, all incisors and canines in good position, and labially inclined canines (Table 36-1). Careful selection of specific torque prescriptions is strongly encouraged before starting treatment.
997.e162 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
High-Torque and Low-Torque Alternatives to the Damon Standard PrescriptionIncisors and canines are available with torque variances for spe-cific malalignments to shorten treatment times through greater torque control.
sion 2 cases, cases requiring extensive Class II elastics, and most extraction cases
• +7-degree torque, +5-degree tip, 0-degree rotation: cen-tral incisors requiring extensive uprighting, cases requiring extensive Class III elastics, extremely crowded cases com-bined with anterior tongue thrusting or thumb or finger habit, and when extensive arch length needs to be gained and the incisors have near normal angulationUpper lateral incisors
• +10-degree torque, +9-degree tip, 0-degree rotation: Divi-sion 2 cases, cases requiring extensive Class II elastics, and most extraction cases
• +3-degree torque, +9-degree tip, 0-degree rotation: lateral incisors requiring extensive uprighting, blocked lateral inci-sors in lingual crossbite that will have too much torque from standard prescription as they move into normal position, cases needing extensive Class III elastics, extremely crowded cases combined with anterior tongue thrusting or thumb/finger habit, and where extensive arch length needs to be gained and the incisors have near normal angulationUpper and lower canines
• +7-degree torque, +6-degree tip, 0-degree rotation: canines needing coronal uprighting and most extraction cases requiring first premolar space closureLower central and lateral incisors
• −6-degree torque, +2-degree tip, 0-degree rotation: extreme crowding in lower anterior segment, cases needing extensive Class II elastics, any lower incisor initially positioned lingual with labial root position, and cases needing a Herbst appli-ance on the archwire
Damon System Archwires and Archwire SequencingThe Damon System has been carefully designed and developed to take advantage of play in the mechanical system and yet maintain superb control of teeth in the working and finishing stages of treatment. The amount of play between the bracket tube and archwire is critical and must be understood to take advantage of this new technology. Archwire sequencing is a critical element in managing clinical forces. In the early align-ing phase, minimization of binding and friction is important and accomplished by placing a small high-tech archwire in a large lumen or tube of the bracket. This method is particu-larly significant in the lower anterior segment where teeth are usually crowded and the interbracket distance is minimal. The applied force can be less if the divergence of the bracket slots is minimized when a small flexible archwire is positioned on either side of the large bracket tubes. This concept is similar to driving a car down a winding highway by using both sides of the road to minimize the curves and to allow for faster travel. This mechanical advantage allows the clinician significant advan-tages to apply a force just high enough to stimulate cellular activity without crushing the lacelike network of blood vessels around the roots in the periodontal ligament and surrounding alveolar bone. One of the key mistakes clinicians make when starting to use this technology is not allowing enough time for
A BFIGURE 36-81 The Damon 3 tube and bracket in the (A) open and (B) closed positions.
TABLE 36-1 Standard Torques for the Damon Prescription
997.e163CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
these light archwires to work. The author encourages clini-cians to resist the temptation to change archwires constantly. Proffit stated, “Activating an appliance too frequently, short circuiting the repair process, can produce damage to the teeth or bone that a longer appointment cycle would have prevented or at least minimized.”17 Observing the root proximity in or adjacent to the alveolar cortical plate on lower CT scans makes a strong case for using biologically sensible forces and paying close attention to how forces are applied. Most clinicians using traditional mechanics select archwires based on patient toler-ance rather than selecting forces based on biologic principles. Those clinicians who use conventional archwire sequencing or force archwire changes in the bracket tubes severely compro-mise the clinical response of this new technology.
The Damon archform has been developed over many years but is used in a single form and size only during the first two phases of high-tech archwires. The first two high-tech arch-wire phases are intended to give the body a second chance to find a new physiologically determined tooth position and archform dictated by the muscles of the face and tongue, bone, and soft tissue. This is a functional or natural arch-form, not a forced archform. The art of new clinical ortho-dontics is to learn how to read and react to how the body responds to these very light forces. The teeth are not being driven into a predetermined archform. The shape of the work-ing and final archform is copied from the lower arch after the high-tech edgewise phase (Fig. 36-82). Instead of treating to a small, medium, and large archform, each archform is patient specific (Fig. 36-83). After using this new technology for more than 8 years, the author realized that predicting the shape and size of the final archform is impossible before treatment. This is a significant advantage over traditional mechanics and other current treatment techniques. (Note that the Ni-Ti wires specified throughout the cases presented are Ni-Ti Align SE wires. The author has worked with Ormco to develop Copper Ni-Ti archwires for the initial light round wire and high-tech edgewise phases that the author now uses.)
Light Round Wire PhaseBy the end of the light round wire phase, the orthodontist will have achieved significant leveling and aligning, begun rotational control, and begun arch development.
The orthodontist should consider the following: • Use a 0.014-inch Copper Ni-Ti initial archwire to start tooth
movement, level, begin archform development, and prepare for the next archwire.
• Use a 0.016-inch Copper Ni-Ti archwire for a second arch-wire in severely crowded adult patients who are not ready for the second phase archwire.
High-Tech Edgewise PhaseBy the end of the high-tech edgewise phase, the orthodontist will have completed leveling and aligning, completed rotational control, begun torque control, begun space consolidation, and continued arch development.
The orthodontist should consider the following: • Place 0.016- × 0.025-inch Copper Ni-Ti wires in primarily
young patients with well-prepared upper arches. • Place 0.014- × 0.025-inch Copper Ni-Ti when archwire is
too difficult to engage in the upper arch. In all lower arches, because of interbracket distance, 0.014- × 0.025-inch Cop-per Ni-Ti is strongly recommended. In all adults, 0.014- × 0.025-inch Copper Ni-Ti is recommended as the second archwire in upper and lower arches. Space is consolidated in the anterior segments.
• Use a 0.018- × 0.025-inch Copper Ni-Ti archwire after a 0.014- × 0.025-inch Copper Ni-Ti archwire. The archwire is well suited for preparing for the insertion of the working stainless steel wire.
• A 20-degree pretorqued reverse curve 0.017- × 0.025-inch Copper Ni-Ti archwire serves well as a Division 2 second wire. Use the same wire without the torque if only intru-sion is needed. A 0.019- × 0.025-inch version of the same wire is available for more challenging cases or a follow-up archwire.
• Take a panoramic radiograph, and assess root positions after the use of high-tech edgewise wire to determine the need to reposition brackets.
Major Mechanics PhaseBy the end of the major mechanics phase, the ortho-dontist will have completed or nearly completed torque control, completed space consolidation, corrected buc-colingual discrepancies, and finalized the patient-specific archform.
A 0.019- × 0.025-inch posted stainless steel archwire is used to maintain arch integrity and should be used during antero-posterior correction and closure and also to maintain the ante-rior vertical and posterior buccolingual.
FIGURE 36-82 The shape of the working and final archform are copied in stainless steel from the lower archform that results from the high-tech archwire edgewise phase of treatment.
FIGURE 36-83 Examples of two cases treated with the same high-tech archform.
997.e164 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
Finishing PhaseBy the end of the finishing phase, the orthodontist will have conducted final detailing.
In most cases the working archwires are kept in place to fin-ish the case. If more bending or torquing of archwires is needed to finish, then the orthodontist should use 0.019- × 0.025-inch or 0.017- × 0.025-inch TMA archwire.
Tieback Usage with the Damon SystemOnce all the spaces are closed, modules, elastic chains, or lig-ature wires are typically used in the major mechanics and final stages of treatment to keep all spaces closed. Available in a variety of sizes and strengths, tieback modules are extended intraarch from the posted hook on a 0.019- × 0.025-inch arch-wire, occlusally passing beneath the first premolar tie-wings to the hook of the first molar in the same arch. Tiebacks are strongly recommended in this low-force, low-friction system because space easily opens.
Using Elastics with the Damon SystemMany ways exist to achieve good clinical results with elastic wear. The elastics most frequently used in the author’s clinic have proved effective in the passive self-locking system. The author keeps treatment mechanics simple and has been impressed with what can be achieved with elastic wear when biologically sensible forces are applied to a mechanical system with greatly reduced friction and binding. Posts on the archwires used for elastic wear are preferred so as to evenly distribute force over all teeth. Eliminating bracket hooks keeps the appliance clean and more comfortable and promotes healthy tissue response. Because the bracket is self-ligating, the tie-wings are free for elastic attachment.
Lingual Retainer Wire and Splint RetainerUsing this tube technology and low-force, low-friction mechan-ics, clinicians now are able to treat many patients who, in the past, would have been scheduled for surgery. To retain these challenging patients who have had severe muscle imbalances, the author strongly recommends the placement of temporary upper and permanent lower lingual retainer wires and nightly use of a splint.
As an outstanding muscle trainer, the splint not only main-tains the alignment of teeth and dental arches, but it also helps
maintain the orientation of the occlusion. Approximately 30% of the author’s patients today are retained with this special splint for at least 1 year or longer. Without the use of the splint, the long-term stability of many cases would be compromised. Surprisingly, patients adapt well to splints, and many mention an improvement in nightly sleep patterns.
Splints are recommended in patients with: 1. Severe muscle dysfunction (buccolingual coordination chal-
lenges) 2. Herbst appliance 3. Severe posterior crossbite 4. Lateral tongue-thrust 5. Severe Class II or III dentitions corrected with elastics 6. Temporomandibular joint disorders 7. Some sleep apnea
For maximum retention, the orthodontist places lingual retention wires after debonding and bonds a 0.016- × 0.025-inch Bond-a-Braid braided wire to each upper tooth lateral to lateral incisor. (The orthodontist removes the upper retention wire 2 to 3 years into retention, depending on the severity of the original anterior tooth position and patient stability in reten-tion.) The orthodontist takes an impression of the lower arch. The orthodontist fabricates a canine-to-canine lingual retainer on the model with a 0.026-inch round stainless steel wire. In normal cases the orthodontist bonds the retainer to only the canines. In severe cases the orthodontist bonds the retainer to each tooth canine to canine. (The lower lingual retainer is per-manently left in.)
After the lingual bonded retainers are in place, the ortho-dontist takes impressions of the upper and lower dental arches. Thick pink base plate wax is heated in a hot water bath and folded end to end twice to create four thicknesses of wax. (The orthodontist must make certain that the wax is soft to pre-vent distortion of the condyle when taking a bite registration.) The orthodontist instructs the patient to bite slowly into the wax, carefully aligning the midlines and leaving 3 to 4 mm of bite opening for airway and thickness of the upper and lower retainer materials. In all Class II retention cases, the orthodon-tist takes the bite registration in a slightly overcorrected man-dibular position. Figure 36-84 illustrates the fabrication and seating of this valuable retention splint.
997.e165CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
I
A
B
C
DE F
J
K
G
H
FIGURE 36-84 Fabrication of the splint retainer. A, Trim models and remove any occlusal bub-bles. Cut groove in base of models with acrylic bur in alveolar ridge area (arrows). B, Apply sticky wax to the models together with three toothpicks. Paint Al-Cote separating agent (Dentsply, York, PA) on both model bases. C, Mount upper and lower models on simple articulator. D, Care-fully separate models from their bases at the separating agent joint. E, Remove plaster from the center of both models, and use vacuum application of Essex A+ (Raintree Essix, Metairie, LA) or Biocryl (Great Lakes Orthodontics, Tonawanda, NY). Block out undercuts with Wonderfill (Dental Creations, Waco, TX). F, Trim retainer material on the model, and place the models back on the articulator with sticky wax. G, Mix acrylic, and place it between the models from middle canine to posterior canine on the buccal and lingual aspects. H, Leave airway in anterior area canine to canine. Amount of airway is determined by the needs of the patient. I, Place acrylic beyond the tip of the upper canine. Leave it short of the cusp tip (arrow). A fracture line sets up if patients clench their teeth. J, Relieve any undercuts with acrylic bur on upper canine. K, Note how tongue is contained (arrows).
997.e166 CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
REFERENCES 1. Pollard A. Capturing the essence of the Damon approach. Clin Impres-
sions. 2003;12(2):4–11. 2. Whitehall W. Personal communication; March 2004 (Whitehall is former
executive vice president of Unitek.). 3. Andreiko C. Personal communication; March 2004. 4. Morrow R. Personal communication; March 2004.
5. Voudouris JC. Interactive edgewise mechanisms: form and function comparison with conventional edgewise brackets. Am J Orthod Dentofacial Orthop. 1997;111:119–140.
6. Kronka MC, Watanabe IS, da Silva MC. Scanning electron microscopy of angioarchitecture of palatine gingiva in young rabbits. Braz Dent J. 2001;12(3):163–166.
7. Sandstedt C. Einige Beiträge zur Theorie der Zahnregulierung. Nord Tandlaek Tidskr. 1904;5:236–256.
S U M M A R YThe philosophy underlying the intended use of the Damon System is to approximate the forces that normal functioning muscles have on tooth position and the developing archform. The system is a blend of high-technology archwires and passive self-ligating tubes (brackets) carefully matched to produce great finishes while maintaining an appreciable amount of play in the mechanical system, especially in the initial stages of treatment. This new way of thinking about clinical mechanics is based on trying to achieve the following two clinical principles: 1. Do not overpower the biologic system with high-force
mechanics during any phase of treatment. 2. Work with the orofacial musculature, allowing it to deter-
mine the new physiologically based tooth position and arch-form balanced among the facial muscles, tongue, bone, and soft tissue.For many years, clinicians have based most of their treat-
ment planning decisions on maintaining the patient’s original archform. Determining the appropriate force level was often based on patient tolerance rather than its impact on the bio-logic cellular composition of bone and tissue. Conventional thinking also ascribed stable results to the elimination of tooth mass to maintain the original archform. Long-term retention studies have not shown a statistically significant correlation between tooth extraction and stability. For years, orthodontists have observed that many malocclusions are simply the result of functional abnormalities. With muscle-imbalance corrective appliances, Fränkel demonstrated that the posterior archform could be altered long-term stability. The reason why the Damon System appears to have an effect similar to the Fränkel effect with its concomitant impact on the physiologic adaptation of the muscles is not completely understood. With the use of very light, biologically sensible forces to start to unravel crowding, the changing archform appears to “wake up the tongue” and, in most patients, creates a new balance of the orofacial mus-culature. This newly created balance of the muscles, bone, and soft tissue is what determines the new tooth position and arch-form. With the Damon System and the philosophy of low-force mechanics, the art of clinical orthodontics is learning how to read and react to what the body determines for each individual patient. Extensive clinical results indicate that complete den-titions can be maintained, even in many crowded arches. In most cases, the body—not the clinician—determines the final archform.
The most significant impact of this new, passive technology is the myriad of additional options available to the clinician for facially driven treatment planning. Clinicians around the world are acutely aware of the long-term impact of traditional extraction therapy on the maturing face. (The philosophy of
the Damon System still strongly recommends extraction ther-apy in bimaxillary protrusive cases.) By designing new treat-ment mechanics that consider the biologic impact of low-force treatment over the lifetime of a patient, orthodontists now have the opportunity to consider what the patient will look like at 50 years of age and design treatment plans in which most complete dentitions are preserved.
CT scans taken of patients just debonded and compared with scans taken 5 years and longer in retention show prom-ising results from the low-force therapy offered via the Damon System and its underlying treatment philosophy. The following observations were made from studying the results of Damon System therapy on 13 patients ranging in ages from 13 years, 6 months to 56 years of age: 1. Alveolar bone can be altered and reshaped with low clinical
forces. 2. With low-force, low-friction orthodontics via the Damon
System, the alveolar bone will allow the movement of teeth with minimal tipping in all planes of space.
3. Alveolar bone is exceedingly thin on the labial, buccal, and lingual aspects of teeth that clinicians are trying to move. This observation calls for low-force therapy that respects the delicate nature of this bony architecture.
4. In many lower arches, pretreatment roots are routinely posi-tioned within the cortical plate. This observation mandates the deployment of extremely low clinical force systems that take into account the low vascularity of cortical plate.
5. The architecture and thickness of alveolar bone appears to improve over time in retention after low-force orthodontics.
6. The low-force mechanics used through the Damon System indicate improved bone response for teeth that have not been allowed to erupt through the facial or lingual cortical plate. For this reason, early tooth guidance is strongly encouraged.
7. Low-force orthodontics can have a positive impact on the bone of periodontal patients.
8. Several hundred thousand patients have now been treated worldwide with the Damon System technology. In com-promised dentitions, periodontists following complex cases treated with this light-force system have been impressed with the positive bone and tissue response. Although the clinical results are promising, further research and long-term reten-tion studies are encouraged.
AcknowledgmentThe author would like to acknowledge Robert Borkowski for his input about the physiologic functioning of tooth movement and contribution to this chapter in that regard, much of which comes from his postgraduate orthodontic thesis.
997.e167CHAPTER 36 Treatment of the Face with Biocompatible Orthodontics
8. Schwarz AM. Tissue changes incidental to orthodontic tooth movement. Int J Orthod Oral Surg Radiogr. 1932;18:331–352.
9. Reitan K. Continuous bodily tooth movement and its histological signifi-cance. Acta Odontol Scand. 1947;7:115–144.
10. Reitan K. The initial tissue reaction incident to orthodontic tooth movement as related to influence of function. Acta Odontol Scand Suppl. 1951;6:1–240.
11. Reitan K. Tissue behavior during orthodontic tooth movement. Am J Orthod. 1960;46:881–900.
12. Reitan K. Initial tissue behavior during apical root resorption. Angle Orth-od. 1974;44:68–82.
13. Reitan K, Kvam E. Comparative behavior of human and animal tissue during experimental tooth movement. Angle Orthod. 1971;41:1–14.
14. Rygh P. Elimination of hyalinized periodontal tissues associated with orthodontic tooth movement. Scand J Dent Res. 1974;82:57–73.
15. Rygh P, Reitan K. Ultrastructural changes in periodontal ligament incident to orthodontic tooth movement. Trans Eur Orthod Soc. 1972:393–405.
16. Tuncay OC, Ho D, Barker MK. Oxygen tension regulates osteoblast func-tion. Am J Orthod Dentofacial Orthop. 1994;105:457–463.
17. Proffit WR, Fields Jr HW. The biological basis of orthodontic therapy. In: Profitt WR, Fields Jr HW, eds. Contemporary Orthodontics. 3rd ed. St Louis: Mosby; 2000:296–325.
18. Borkowski RN. The biologically based case for truly light-force mechanics. Clin Impressions. 2004;13(1):19–22.
19. Fränkel R, Müller M, Falck F. The uprighting effect of the Fränkel appli-ance on the mandibular canines and premolars during eruption. Am J Orthod Dentofacial Orthop. 1987;92:109–116.
20. Bagden A. Personal communication; March 2004 (Bagden is a practicing orthodontist in Springfield, VA.).
21. Pitts T. Personal communication; March 2004 (Pitts is a practicing ortho-dontist in Reno, NV.).
998
AAAPD. see American Academy of Pediatric Dentistry
(AAPD)Abuse, and dental avulsion, 885Abutment teeth, parallelism of, adult interdisciplinary
therapy in, 571, 573fAcceleDent device, 918–919, 919f
effect of, on alignment of lower anterior teeth, 919patient’s comfort and ease of using, 920
AcceleDent Type I appliance, 93Acetaminophen, for micro-osteoperforations, 915–916Acid etching, conventional, for enamel conditioning,
819–820alternatives to, 820amount of enamel removed by, 820gels for, 820optimal time for, 820prolonged, with fluoride pretreatment, 820surfaces for, 820on teeth with internal white spots, 820
Ackerman-Proffit classification, 226–229, 230fAcoustic rhinometry, for upper airway, 327–329, 328fACPA. see American Cleft Palate-Craniofacial Association
Active clips, 740–741Active members, of orthodontic appliance, 164Active self-ligating brackets, new prescriptions for, 479ADA. see American Dental Association (ADA)Adaptive prescription, in targeted therapeutics, 946–947,
Adult patientschanges, in craniofacial growth and development, 25lingual treatment of, 768f–772f, 768btreatment objectives, in adult interdisciplinary therapy,
571–583, 573f–582f, 573b, 584f–585fAerosol, 195Aesthetic considerations, in periodontal-orthodontic
interrelationships, 642–643, 646fAesthetic line, of the dentition, 230fAesthetic self-ligating brackets, 735–736Aesthetic/functional improvement, adult interdisciplinary
therapy in, 583, 584fAgenesis, dental, 42–43Aggressive periodontitis, 624, 625fAHI. see Apnea-Hypopnea Index (AHI)Aligning, with lingual appliances, 764–765
type 1, 765, 765ftype 2, 765, 766ftype 3, 765, 767f
Alignment, of active clips and passive slides, 741Alleles, 34Allergy-immune problems, 695tAlloy soldering, 188–189
Alveolar decortication, 661–665alveolar bone biological response in, 661–662patient management in, 663surgical technique in, 662–663, 662ftreatment indications and limitations of, 663–665,
663f–664fAlveolar fracture, 881Alveolar process, density of, versus maxillary molars,
131–132Amalgam, bonding to, 827–829, 827f–828f
procedures for, 828, 829fAmerican Academy of Pediatric Dentistry (AAPD), 395American Cleft Palate-Craniofacial Association (ACPA), 367American Dental Association (ADA), 200–201
Center for Evidence-Based Dentistry, 200–201, 205Analysis system, differential diagnosis of, 493, 494tAnchorage
alveolar bone biological response in, 661–662patient management in, 663surgical technique in, 662–663, 662ftreatment indications and limitations of, 663–665,
663f–664fAustenitic active, NiTi archwires, 192–193Australian didgeridoo, 344Autoradiography, in bone physiology, 104Autosomal dominant inheritance, 35, 35fAutosomal recessive inheritance, 35Autosomal recessive traits, 36f, 37Autosomes, 32–33, 33fAuxiliaries, Tweed-Merrifield edgewise appliance and, 495Auxiliary appliances, 950Avulsion, in permanent dentition
BBackscatter emission, 106Banner advertising, in orthodontics, 205Bariatric surgery, 343Basal bone
discrepancy, 703lower incisors placement in, 983
Basal plate, development of, 8, 8fBase-wing joint, of stainless steel brackets, 188–189, 189bBDD. see Body dysmorphic disorder (BDD)Beam filtration, 304Beck Depression Inventory, 295Begg, Raymond, 730Begg brackets, 739
Begg mechanics, with straight-wire control, 757, 758f–759fBegg pins, 730Behavior guidance, for child and adolescent patient,
395–396Behavior management, differences between pediatric
dentistry and orthodontics, 396–397Behavioral disorders, 695tBending, 165Berlin questionnaire, 338, 339tBeta-titanium (TMA), 168, 169fBilateral symmetry, environmental and genetic influences
on, 44Biodigital orthodontics, 926–980
case study for, 959f–979f, 959bin clinical practice, 930–942craft-based care model in, 926–927, 928fefficacy and effectiveness of, 957integrated digital technology platform in, 927–930patient-centered model of care, 927, 929fproactive decision making and, 942–944professional-based model of care, 927, 929fand targeted therapeutics, 946–957
Biological factors, of radiation dose risk, 303Biological responses, by orthodontic forces, 85–87Biomechanical considerations, in temporary anchorage
devices, 511–568, 517f–518f. see also Temporary anchorage devices (TADs)
Biomechanics, straight wire, contemporary, 437–454Biotype, in periodontal-orthodontic interrelationships,
626, 626fBipolar disorder, 292–293Birthday party air balloon, for air volume, 326–327, 327fbis-GMA/TEGDMA mixture, 193–194Bisphenol A-glycidyl methacrylate (bisGMA), 813–814Bisphenol-A (BPA), 195Bite plane therapy, 592Bite splint, 706tBiting strength, of human masticatory apparatus, 119Bleeding disorders, 695tBlue light
biological properties of, 194–195effects, 194–195
Bodily movementinto defects, 637–640, 643ftooth movement and, 69, 69f, 76f
cleaning in, 819curing in, 824, 824fenamel conditioning in, 819–821excess in, removal of, 823–824, 823ffitting in, 823positioning in, 823premedication for, 819procedure for, 823sealing and priming in, 821, 822ftransfer in, 823
of large acrylic appliance, 855for deciduous or mixed, 859–860, 861ffor permanent dentition, 859technical procedures for, 859–860
materials and devices used in, 813–818adhesives as, 813–817brackets as, 813fluoride in, 893–894, 893f–894flight sources as, 817–818light-emitting diodes as, 818, 819f
of molars, 832–833for occlusal buildup of posterior teeth, 860–861to porcelain, 825–827
clinical prediction of, 336clinical presentation of, 335–336definitions and testing reports in, 333–334epidemiologic factors in, 335pathophysiologic factors in, 335physical characteristics of, 336preventative management in, 344tests and questionnaires in, 336–340
Canine-to-canine lingual retainer bar, 842–847, 846f–847fbonding of, 845–847, 848f–849ffailure analysis and long-term experience with, 847retention period for, 847
Cantilever testing, of archwires, 193α-Cardiac muscle isoforms, 39Cardiovascular computed tomography (cine CT), 326Caries Balance concept, 888–889, 892fCarrier, 35fCAS. see Computer-aided surgery (CAS)Case report, 202Case/control study, in orthodontics, 202Casein phosphopeptide-amorphous calcium phosphate
(CPP-ACP), 895for demineralized white lesions, 896
Casein phosphopeptides (CPPs), 895Casts
analysis, for diagnosis, in orthodontics, 223posttreatment, 490f, 504f, 508fpretreatment, malocclusion correction with edgewise
appliance and, 502f, 506fCBCT. see Cone beam computed tomography (CBCT)CBT. see Cognitive-behavioral therapy (CBT)Cell kinetics, in bone physiology, 106Cementum, root, 53, 55fCenters of rotation, 156–158, 159f
lingual force in, 156, 156fmoment-to-force (M/F) ratio against, 157, 158fpure moment in, 156three-dimensional finite element method for, 158, 159ffor translation, 156, 156f
Central fifth, of face, 262Central hypopneas, 334Central incisors, maxillary, impacted, 870Central nervous system, increase peripheral input to, 362Central sleep apnea syndrome, 335Centric relation (CR), 442
habitual occlusion and, in debonding or debanding, 602Cephalogram, 223, 255
for upper airway, 326Cephalometric analysis, 338, 383–387
for diagnosis, in orthodontics, 223–226, 233fCephalometric head-holders, 253Cephalometric tracing
with all values and planes, 491fmalocclusion correction with edgewise appliance and,
503fposttreatment, 490f, 505f, 508fpretreatment, malocclusion correction with edgewise
appliance and, 503f, 507fCephalometric values, pretreatment and posttreatment
Class II mandibular deficiency, diagnosis of, 695, 696f–701fClass II skeletal patterns, 224, 323Class III deep bite cases, muscle fibers of, 39Class III elastics, 468Class III malocclusion, 41–42, 209
cephalometric analysis of, 224components of, 427FR-3 appliance of Fränkel, 429mandibular growth effects in, 984maxillary skeletal retrusion associated with, 427spontaneous improvement of, after rapid maxillary
expansion, 418–419timing of treatment of, 409treatment of, 427–432
Class III mandibular excess, diagnosis of, 695, 696f–701fClass III skeletal patterns, 211Cleaning, in bonding to enamel, 819Clear aligner treatment, 778–811
appliances used in, 778, 783biomechanics of, 783–786brief history of, 778–780, 779t–780tcase study of, 800b, 801f–810f, 805b, 807bClinCheck and, 782–783, 783t, 784fdiagnosis and treatment planning for, 782difficult movements using, 785–786, 785f–786finterproximal tooth reduction and, 778low-level mechanical vibrations and, 921, 921f–922fperiodontal considerations of, 800simple movements using, 785–786, 785f–786fsimultaneous staging of, 786, 786f–788fstaging of, 786–788, 786f–788fterminology associated with, 778–780torque control and, 791–792, 792fvirtual models and, 789f
management of missing lateral incisor space, 390–392, 392fmixed dentition stage (7 to 12 years of age), 375–382,
377f–380fnasomaxillary complex, 372neonate and infant (birth to 2 years of age), 369–372orthodontist’s role in, 369–390permanent dentition stage, 382–390, 382f–383fprimary dentition stage (2 to 6 years of age), 372–375,
373f–376fsurgical lip adhesion, 371–372team approach to, 368–369
Cleidocranial dysplasia, 869, 870f
ClinCheck, 782–783, 783t, 784fClinical cephalometrics, development of, 223Closed eruption exposure technique, for impaction, 874, 874fClosest point measurements, in CBCT, 309, 309f, 312,
312f–313fClose-up images
with black background, for microaesthetics, 252, 254fof posed smile, in facial photographs, 248, 249f
Cochrane Collaboration, for orthodontics, 205CODA. see Council on Dental Accreditation (CODA)Coffin loop, 456, 457f, 462fCognitive awareness, TMJ and, 362Cognitive-behavioral therapy (CBT), 292Cohort study, in orthodontics, 202, 202f
systematic review and, 204, 204fCoil activation, Niti thermal-activated, 444Collagen fibers, in gingiva, 52, 53fColor-coded maps, in CBCT, 311, 311f–312fColumella, 264Combination facebow headgear, 419Commissure height, 270, 271fCommon coordinate system, in CBCT, 310–311Communication
in adult interdisciplinary therapy, 614guidance, for child and adolescent patient, 396–397between orthodontist and patient, 289reports used in, 673–674
Complementary force system, in targeted therapeutics, 950, 954, 958f
Completely customized lingual appliances, 761, 762finnovation in, 764
Completion conference report, in adult interdisciplinary therapy, 618f
302–318, 303f, 432f, 442, 871, 872fin biotype, 626, 626fchallenges to advance understanding of growth and
treatment responses in, 307–309clinical applications, and potential limitations of, 304–306
airway assessment in, 305–306, 306fcraniofacial anomalies in, 306, 307fdentofacial deformities in, 306, 307ftemporomandibular joint health and disease in,
304–305, 305f–306ftooth morphology in, 304, 304f
for facial structure, 691image analyses in, 307–313three-dimensional surface models and superimpositions
in, 307–313of TMJ degeneration, 101–102, 104f–105ffor upper airway, 326–327
Consanguineous mating, 37
1002 INDEX
Consistent force systems, in targeted therapeutics, 954, 954f–957f
Consonant smile arc, 270Constraint recognition and management
in proactive decision making, 944, 947fin targeted therapeutics, 950, 951f
Consultation, in adult interdisciplinary therapydevices, 596techniques, 595
516–517, 517f–518f, 519Corpus, of mandible, 18Cortical bone, 54, 56f
bone remodeling in, 107f–108f, 108–110growth and maturation of, 111–116, 113f–115fstructural and metabolic fractions of, 113–116, 116fin temporary anchorage device, 522
Council on Dental Accreditation (CODA), 201Couple-to-force ratio, 157, 157fCoupling factors, of bone modeling, 111, 112fCPAP. see Continuous positive airway pressure (CPAP)CPP-ACP. see Casein phosphopeptide-amorphous calcium
phosphate (CPP-ACP)
CPPs. see Casein phosphopeptides (CPPs)CR. see Centric relation (CR)Craft-based care model, 926–927, 928fCranial base, 8–12
development of, 8, 8fpostnatal growth of, 10–12, 11f
Craniofacial anomalies, 306, 307fteam approach to patients with, 370f
Craniofacial complex, 3–4, 3ffunctional units of, 4, 4fstructural units of, 3–4
Craniofacial deformities, patients with, 298–299Craniofacial growth and development, 1–17
adult changes in, 25arch development, 23–25, 23f–24fcranial base, 8–12. see also Cranial basecranial vault, 5–8. see also Cranial vaultcraniofacial complex, 3–4, 3f
functional units of, 4, 4fstructural units of, 3–4
Craniosynostosis, 6–7Crib appliance, 607–609, 612fCritical point, in patient cooperation, 404Critical sections, 175Crossbite
anterior, 373–374unilateral, 458
Crouzon syndrome, and upper airway, 332fCrowded lower arch, treated without extraction, 747f–751f,
747b–748bCrowding
alleviation, of NiTi archwires, 193case study of, 747f–751f, 747b–748bmanagement of, in orthodontics, 232–233self-ligation for, 746–756treated with lingual appliance treatment, 765
Crown tipping, 164Crown-to-root ratio, adult interdisciplinary therapy in,
574–575, 581fCurve of Wilson, 441Custom milling, in orthodontics, 236Customized lingual appliance, 761–762
decalcification risk reduced with, 762illustration of, 762finnovation in, 764target setup model system in, 761treatment goals realized with, 761–762
Cutting/filling cones, 113–116in bone remodeling, 110, 110f, 112fperivascular process and, 122, 125f
CYP19A1, 41Cytokines, in tooth movement, 914Cytotoxicity, of orthodontic resins, 816
Definitive lip repair, 372Degeneration, in hyalinization phase, 60, 61fDegree of cure-conversion, 816DeLaire face mask, 706tDelayed healing, 720–722Delayed pain, 162–163Demand, versus need, in orthognathic surgery, 672–676Demineralization
prevention of, 889–892tooth movement and, 147
Demineralized white lesionsdetection and measurement of, 888
with quantitative light-induced fluorescence, 888, 890f–891f
with quantitative light-induced fluorescence-digital, 888, 891f
with transverse microradiography, 888, 889floss of mineral from enamel (demineralization) in,
prevention of, 889–892prevalence of, 887–888prevention and management of, 887–896, 888fpromoting uptake of mineral into enamel
(remineralization) in, 892–895treatment of, 895–896
with casein phosphopeptide-amorphous calcium phosphate, 896
Dental materials, in orthodontics, 187–199adhesives for, 193–195archwires for, 192–193blue light in, 194–195mechanics of, appliance properties on, 187–192NiTi archwires, 192–193photocuring in, 193–195retainers for, fixed, 195–197stainless steel brackets for, 187–190summary in, 197
Dental microaesthetics, 276–282bracket placement in, 281–282, 282fgingival shape and contour in, 276–281, 279f–281f
Diagnosis, in orthodontics, 208–244Angle classification in, 226camouflaging discrepancies on, 210–211cephalometric analysis for, 223–226class II malocclusion for, evaluation of, 224classification in, 226–229clinical evaluation for, 217–219
face in, 217facial proportions in, 217intraoral examination in, 217–219jaw function in, 218–219soft tissue function in, 218TM joints in, palpated, 219
concepts of, 208–215database for, 226–229dental compensations in, 210–211first contact interview for, 216interview at first appointment for, 216interview data for, collection of, 216–217modern health care paradigm of, 208–209
goals of, 209patient evaluation for, 215–230patient meeting for, 216–217problem-list as, 215
prioritizing, 230–232problem-oriented approach to, 215, 230–236problem-oriented treatment planning in, 246, 246f–247f, 258profile for, 233quality of life in, 208–209records needed for, 219–222skeletal compensations in, 210–211special considerations in, 245–288speech evaluation for, 218summary of, 229–230systematic description for, 226–229
Diagnostic facial triangle, Tweed’s, 484fDiagnostic records, in orthodontics, 219–222
additional, 219analysis of, 222–226
cast, 223cephalometric, 223–226class II malocclusion, 224class III malocclusion, 224clinical cephalometrics in, 223skeletal and dental units in, relationships of, 223, 224fvertical dental problems in, 225–226vertical skeletal problems in, 224–225
computer imaging in, 220cone beam computed tomography in, 220data from, 215fhead orientation, for cephalograms, 219intraoral scanning in, 220–222photography in, 219–220physical dental casts in, virtual versus, 219technologic advances in, 219–2223D facial photography in, 220videography in, 219–220
long-term results of, 855, 859f–860ftechnical procedure for, 855
Directional force, 495, 496fDisarticulation, in adult interdisciplinary therapy, 591,
592f–593fDisc displacement
joint sounds caused by, 361without reduction, 711
Displacement, lateral, 881Distalization
en masse, 528, 541fmolar, temporary anchorage devices in, 515
archform control in, 538f–540fbiomechanics in, 528decision making in, 528, 531fmechanical efficiency in, 528, 532f–536fmesiodistal axis control in, 537fmethods for, 522fthree-dimensional control in, 528torque control in, 538fvertical control in, 539f–540f
Distalizing buccal segments, sagittal appliance for, 591Distalizing forces, molar resistance to, reduction of,
Electromagnetic tracking, tracking technology in, 315Embrasure space, adult interdisciplinary therapy in, 571, 576fEn masse distalization, 528, 541fEnamel
bonding to, 819–824, 822fcleaning in, 819curing in, 824, 824fenamel conditioning in, 819–821excess in, removal of, 823–824, 823ffitting in, 823positioning in, 823premedication for, 819procedure for, 823sealing and priming in, 821, 822ftransfer in, 823
conditioning of, before bonding, 819–821enamel pretreatment in, 819–821moisture control and, 819, 819f
debonding and, amount lost during, 837sealing of, 892tearouts and cracks, in debonding, 834, 835f
Endocrinology, of calcium conservation, 117Endosseous implants, 136–140, 139f–140f, 391–392Endothelial nitric oxide synthase (eNOS), 914Enlow’s classic diagram, 223, 224feNOS. see Endothelial nitric oxide synthase (eNOS)Entitled demanders, 294Envelope of discrepancy, 213–214, 213f
for maxillary and mandibular arches, 607, 611fEpigenetic landscape, 38Epworth Sleepiness Scale, 338ERT. see Estrogen replacement therapy (ERT)Eruption. see also Extrusion.
maxillary. see Maxillary excessExcessive lip projection, versus inadequate lip projection,
265, 266f–267fExcessive submental fat, throat form and, 265Excessive vertical disproportionality, 260, 261fExcursive movements, in debonding or debanding, 605Expedited tooth movement, 145–149
from experimental studies on rodents and canines, 148–149
External apical root resorption (EARR), 897, 897fapical root displacement in, 900, 901f–905fdemographic factors in, 897–898diagnostic factors, 897–899
patient medical history and habits in, 899tooth anatomy in, 897, 898f–899f
early treatment as, 900etiologic factors of, 896–897expansion in, 900extractions and, 900genetic factors and, 44–45, 45fintermittent versus continuous force in, 900low-level mechanical vibrations and, 919–920magnitude of applied force in, 900malocclusion factors in, 898
history in, 901imaging in, 901progress review in, 902root resorption, detection of, at progress, 902, 906f–907f
mechanical, 900prolonged treatment time for, 900risk factors for, 897–900, 901bstart of occurrence of, 902–903stopping of occurrence, 903and teeth with short roots, 903–904, 907ftreatment factors for, 900
role of, 182–183self-ligation and, 736–739of stainless steel brackets, 189–190, 189bin vivo: occlusal and masticatory forces, 738–739
Friedman classification, of OSA, 336–337Frontal at rest, in frontal photographs, 248, 249fFrontal cephalogram, 690f, 692fFrontal dynamic (smile), in frontal photographs, 248,
249fFrontal photographs, 248, 249fFrontal vertical facial relationships, 259–261Frontal view with teeth in maximal intercuspation, in facial
Great Extraction Debate, 329Grinding, selective, in adult interdisciplinary therapy, 591Growth
centers, skeletal, 10considerations, in permanent dentition stages, 382–383,
384f–387fcorrections carried out during periods of, 983craniofacial, modification of, 404differences in, during puberty, 41face, 714tfacial, pattern of, 383factors, 718, 984family data for, 40mandibular
for disarticulation, 577f, 591, 595Hawley retainer, 991–992, 991f–992fHBSS. see Hanks Balanced Salt Solution (HBSS)Head orientation, for cephalograms, 219Headgear
Height measurements, maturation and, 3Helical coils, in wire, 173, 174f
vertical loop with, 176, 176fHemophilia, 695tHerbst appliance, 331Heritability, estimation of, 39–40HGP. see Human Genome Project (HGP)Hierarchy of evidence, in orthodontics, 201–203High filling effect, of occlusion, 210High-efficiency mechanics, in temporary anchorage devices,
511–513, 512fHigh-pull headgear, 462, 463f, 465f
orthopedic effect, 706tHistone deacetylase 4 (HDAC4), 39Histones, 32–33H-MP. see Hyoid to mandibular plane (H-MP)Homeobox genes, in craniofacial growth and development, 5Homologous chromosomes, 32–33Homologous pairs, of chromosomes, 32–33Hormones, in tooth movement, 914Human Genome Project (HGP), 32–33Hyalinization phase, 59–64, 60f–62fHyalinized zones, 60, 61f
root resorption and, 60–64, 62f–65fHydrofluoric acid, as etchant, 825–826Hygienist, of orthodontist, in adult interdisciplinary
therapy, 596
Hyoid bone, position and morphologic features of, 322–323Hyoid to mandibular plane (H-MP), 322Hyperactivity, during orthodontic treatment, 291Hyperplasia, gingival, in periodontal-orthodontic
clear aligner treatment and, 778Intra-arch symmetry, analysis of, 229Intracortical compartment, of cortical bone, 108–111Intracortical secondary osteonal bone remodeling, 108–110Intraoral appliances, removable, 398–399Intraoral elastics, 400Intraoral examination, for diagnosis, in orthodontics,
217–219Intraoral photographs, 252, 254f, 674f–675fIntraoral scanning, for diagnosis, in orthodontics, 220–222Intrusion
of maxillary and mandibular dentitions, temporary anchorage device in, 550b, 551f–558f, 554b–555b
maxillary molar, with mandibular molar extrusion, temporary anchorage device in, 559b, 560f–562f
molar, temporary anchorage device in, 524–541archform control during, 525fbiomechanics of, 525–526, 541decision making in, 524–525, 528–541general effects of, 524flocal effects of, 524fmandibular, 528maxillary, 526mechanical efficiency in, 525–526posterior torque during, 525frotation control in, 542fthree-dimensional control in, 526, 526f–527ftreatment mechanics in, 526–528vertical control in, 542f
of tooth, 636–637, 640f–642fas tooth movement, 70f–71f, 71
with class I molar, 460fwith class II molar, 458f, 470f–472felimination of cause of, 982etiology of, 31–32factors of, 31Hapsburg jaw and, 41heritability studies in, 31overcorrection of, 982ranges of correction in, 213–214reassessment of, in debonding or debanding, 605, 606fskeletal, 673–676, 673b, 674f–675f, 676tskeletal component of, in adult interdisciplinary therapy,
586f, 596–597Mandible, 16–23
bending and torsion in, 100–101, 102fdevelopment of, 16–18, 17fdifferential osteology, 100–101, 101ffunctional units of, 18, 18fpostnatal growth of, 20–23, 21f–23f
loose, rebonding of, 831Metal injection molding (MIM), 189Metals, mechanical properties of, 166–168Metamorphosizers, 296Methylation, 38MIC. see Maximum intercuspation (MIC)Microabrasion, 838–840, 839fMicroaesthetics
close-up images with black background for, 252, 254f
dental, 276–282bracket placement in, 281–282, 282fgingival shape and contour in, 276–281, 279f–281f
smile refinement in, 284b, 285f–287fMicrocomputed tomography, in bone physiology, 106Microdamage, in bone remodeling, 110Microelectrodes, in bone physiology, 106MicroEtcher, 825, 825fMicroindentation testing, in bone physiology, 106Micro-osteoperforations, 913–918
anesthetic for, 914biologic mechanism of, 913–914, 915feffect of, on tooth movement, 916perforations in, distribution of, 915, 916ftechnique and indications for, 914–918, 916f–918f