of diabetic foot ulcers (infected and uninfected) will be colonized with MRSA. Appropriate antibiotic thera- py usually involves culturing the wound and choosing an antimicro- bial based on sensitivity testing. However, wound cultures are not used to diagnose an infection, just to direct therapy. This makes the initial choice of antibiotic impera- tive to the rapid resolution of the infection. Empiric antibiotic thera- py choice is based on several fac- tors: risk factors for MRSA, infec- Continued on page 128 Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin- uing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (you save $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred- its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 202. Other than those entities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be accept- able by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensure the widest acceptance of this program possible. This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected]. An answer sheet and full set of instructions are provided on pages 202-204.—Editor NOVEMBER/DECEMBER 2009 • PODIATRY MANAGEMENT www.podiatrym.com 127 pressive process, predisposing the patient to infection, and leading to a more severe infection when one occurs. Abnormalities include gran- ulocyte adherence, chemotaxis, and phagocytosis. Acute hyperglycemia is also associated with post-opera- tive infection rates of up to 30%. 1 Skin and skin structure infec- tions (SSSI) are predominately caused by Gram positive bacteria. This, however, includes resistant Gram positive bacteria such as me- thicillin-resistant Staphylococcus aureus (MRSA). Approximately 30% By Lee C. Rogers, DPM and Nicholas J. Bevilacqua, DPM D iabetic foot infections (DFI) are the common prequel to amputation. The destruc- tive nature of these infections in the presence of an immunopathic process, such as diabetes, is a mor- bid combination. Certainly bacteri- al resistance worsens the outcome since the empiric therapy may be ineffective, delaying appropriate antibiotics. Diabetes acts as an immunosup- Here is a primer on de-escalation therapy. Goals/Objectives After completing this CME: 1) The reader will gain insight into the prevalence of MRSA in diabetic foot wounds and how diabetes wors- ens the prognosis. 2) The reader will be able to classify diabetic foot infections and choose em- piric treatments for MRSA based on this classification. 3) The reader will be presented in- formation on the most commonly used FDA approved drugs for MRSA, their dosages and adverse effects. Continuing Medical Education MRSA in the Diabetic Foot
Transcript
of diabetic foot ulcers (infected anduninfected) will be colonized withMRSA. Appropriate antibiotic thera-py usually involves culturing thewound and choosing an antimicro-bial based on sensitivity testing.However, wound cultures are notused to diagnose an infection, justto direct therapy. This makes theinitial choice of antibiotic impera-tive to the rapid resolution of theinfection. Empiric antibiotic thera-py choice is based on several fac-tors: risk factors for MRSA, infec-
Continued on page 128
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (yousave $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 202. Other than those entitiescurrently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be accept-able by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best effortsto ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars.The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high qualitymanuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write orcall us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us [email protected].
An answer sheet and full set of instructions are provided on pages 202-204.—Editor
pressive process, predisposing thepatient to infection, and leading toa more severe infection when oneoccurs. Abnormalities include gran-ulocyte adherence, chemotaxis, andphagocytosis. Acute hyperglycemiais also associated with post-opera-tive infection rates of up to 30%.1
Skin and skin structure infec-tions (SSSI) are predominatelycaused by Gram positive bacteria.This, however, includes resistantGram positive bacteria such as me-thicillin-resistant Staphylococcusaureus (MRSA). Approximately 30%
By Lee C. Rogers, DPM and Nicholas J.Bevilacqua, DPM
Diabetic foot infections (DFI)are the common prequel toamputation. The destruc-
tive nature of these infections inthe presence of an immunopathicprocess, such as diabetes, is a mor-bid combination. Certainly bacteri-al resistance worsens the outcomesince the empiric therapy may beineffective, delaying appropriateantibiotics.
Diabetes acts as an immunosup-
Here is a primer on de-escalationtherapy.
Goals/ObjectivesAfter completing this CME:
1) The reader will gain insight intothe prevalence of MRSA in diabeticfoot wounds and how diabetes wors-ens the prognosis.
2) The reader will be able to classifydiabetic foot infections and choose em-piric treatments for MRSA based on thisclassification.
3) The reader will be presented in-formation on the most commonly usedFDA approved drugs for MRSA, theirdosages and adverse effects.
Continuing
Medical Education
MRSA in theDiabetic Foot
MSSA. We also know from animalmodels that untreated MRSA bac-teremia leads to death about twiceas fast as untreated MSSA bac-teremia.4 MRSA baceremia in dia-betics with foot infections is associ-ated with a 43% mortality ratecompared with a 20% mortalityrate in MSSA bacteremia.5
Outcomes are worse when awound is infected with a resistantbacteria. In those with diabetic footinfections caused by MRSA under-going amputation, the mortality
rate was higher (43% MRSA vs 9%non-MRSA).6 In another study fol-lowing amputations in MRSA posi-tive patients, post-operative stumpinfections occurred in 24%, over2/3rd of which were a re-infectionwith MRSA.7
There is no way to determine asensitive from a resistant infectionby physical examination. The his-tory may help to uncover a previ-ous resistant infection or risk fac-tors for MRSA, such as recent an-tibiotic use or hospitalization.Other risk factors for MRSA infec-
tions include nursing home resi-dence, incarceration, and lockerroom environments.
In some facilities, DNA probesfor the MRSA Cepheid mecA geneare available. These are rapid testswith results usually within twohours and give the clinician a “pos-itive” or “negative” result for MRSAin the wound. In situations wherethese advanced tests are not avail-able, empiric therapy must be start-ed based on the patient’s risk fac-tors and clinical suspicion. A propertissue specimen should be taken forculture and sensitivity. The mostaccurate results are obtained bysending a piece of deep tissue fromthe ulcer/infection site. A superfi-cial swab will usually confound theresult by returning a C&S with mul-tiple contaminants.
IDSA ClassificationsThe severity of the infection is
important to guide empiric thera-py. The Infectious Diseases Societyof America (IDSA) classificationstratifies diabetic foot infectionsinto four categories (Figure 1).8
IDSA uninfected is a wound with-out signs or symptoms of infection.IDSA mild infection is a woundwith less than 2 cm of surroundingerythema, but no deep spread orsystemic signs/symptoms of infec-tion. IDSA moderate infection is awound with greater than 2 cm sur-rounding erythema, possible deepspread, including osteomyelitis, butno systemic signs/symptoms of in-fection. An IDSA Severe infection isthe same as a moderate, except
and inpatient/outpatient therapy.MRSA is increasing in preva-
lence in many centers. The Manch-ester UK group reported a near dou-bling in their diabetic foot ulcerMRSA prevalence between 1999and 2003.2,3 In our own past experi-ence in a public county hospital,we reviewed data for the past 10years. The number of new MRSAcases jumped from about 20 peryear to over 200 per year. Ninety-five percent of the cases were fromwound culture isolates. Additional-ly, stories of the bacteria affectingless typical populations, like youngathletes, are circulating.
Common Resistance PatternsWhile there are certainly many
genotypes of MRSA, two commonresistance patterns are often seen.Community-associated (formerlycommunity acquired) and health-care-associated (formerly hospitalacquired) are the most commonisolates. The newer “-associated”names are preferable since bothbacterial strains can cause infec-tions in either the community orhospital setting. Another name forhealthcare-associated MRSA is resis-tant MRSA because it is sensitive tofewer agents. Community-acquiredMRSA is generally susceptible totetracyclines, fluoroquinolones,sulfa drugs, and rifampin. Health-care-associated MRSA requires van-comycin, linezolid, daptomycin,tigecycline, or some other neweranti-MRSA specific drugs.
Former prevailing thought wasthat MRSA is no more virulent thana normal Staphylococcus aureusbacterium, just that it was resistantto many antibiotics, delaying initialeffective therapy—thus causingmore tissue damage. It is nowknown that MRSA is, in fact, morevirulent than methicillin-sensitiveStaphylococcus aureus (MSSA).MRSA contains vanton valentineleukocidin (VVL), and also newlydiscovered enzymes that can de-stroy white blood cells. Together,these virulence factors can be quitedestructive to the body tissue, insome cases causing a true necrotiz-ing fasciitis—otherwise rare with
Continuing
MedicalEducation
Figure 1: The Infectious Diseases Society of America (IDSA) classification of diabeticfoot infections.
from a panel of experts recom-mends the same.9 De-escalationtherapy is a concept where broad-spectrum antibi-otics with anti-MRSA coverageare started first,then narrowed, ifneed be, after theculture and sensi-tivity is reported.Tigecycline canbe used asmono th e r a p y ,since it is broad-spectrum and hasactivity againstMRSA. Other op-tions must use combination thera-py such as piperacillin/tazobactam,ertapenem, or levafloxacin plus ananti-MRSA agent like linezolid, dap-tomycin for injection (Cubicin), orvancomycin. See the algorithm inFigure 2 as a guide to decision-mak-ing of empiric therapy for diabeticfoot infections.
While vancomycin is still usedfrequently in MRSA cases, new evi-dence is showing reduced efficacyversus newer agents. There arepoorer outcomes when treatingMRSA septicemia and a higher re-currence rate. Vancomycin is prob-ably considered the “gold standard”
there are systemic signs/symptomsof infection, such as fever, tachy-cardia, or bacteremia.
IDSA mild infections are pre-dominantly caused by Gram posi-tive bacteria, which can includeMRSA. Moderate and severe infec-tions are more polymicrobial withGram positive, negative, aerobic,and anaerobic bacteria, usually re-sulting in three to six different bac-terial species on culture report. Assuch, Mild infections can be treatedwith agents for Gram positive bac-teria as an outpatient. If there arerisk factors for MRSA, empiric ther-apy should be modified to use orallinezolid, minocycline/doxycycline,or trimethoprim/sulfa. Clin-damycin should be avoided in sus-pected MRSA cases since it canrapidly become resistant. Most labsperform a D-test on MRSA isolate todetermine if clindamycin can beused. But the drawback is that theD-test takes an extra 24 hours afterthe culture is reported, possibly cre-ating a longer delay in appropriatetreatment.
Patients with moderate and se-vere infections should have broad-spectrum coverage and are usuallyhospitalized for treatment. There isno clear consensus on whether tostart anti-MRSA therapy from thebeginning of treatment. Since theseinfections are limb-threatening, we
MRSA... for MRSA since it wasthe only effective agent forhealthcare-associated MRSAfor many years.
Side-effects include renal andototoxicity, and thus care must beused in the diabetic patient with
renal impair-ment. For skinand skin structureinfections, it isonly available inIV form. Withnewer, more ef-fective agents,many with feweradverse effectsand easier todose, cliniciansshould migrateaway from thisaminoglycoside.
LinezolidLinezolid is the first drug is a
new class called oxazolidinones. Ithas activity for Gram positive bac-teria, including MRSA, and is alsoactive against VRE. It is FDA-ap-proved for skin and skin structureinfections (SSSI) and is the onlydrug with specific indication for di-abetic foot infections. It is uniquein that it is available in both IVand oral formulations. The oralform has just as much bio-avail-ability as the parenteral form. Itcan cause bone marrow suppres-sion resulting in pancytopenia, soa weekly CBC should be checked iflinezolid is used for longer thantwo weeks. There have also beensome reported cases of peripheralsensory neuropathy secondary tolinezolid use.
TigecyclineTigecycline is a glycylcycline
antibiotic related to the tetracyclineclass. It is broad-spectrum and anti-MRSA, allowing it to be used asmonotherapy for de-escalation. It isonly available in IV form. It hassimilar side-effects to tetracyclines,but also causes nausea and vomit-ing in approximately 18% of thosewho take it. It is sometime prudentto treat patients prophylacticallywith an anti-emetic.
DaptomycinDaptomycin is a lipopeptide
Continued on page 130
Continuing
Medical Education
Figure 2: Algorithm on recommended empiric treatment of diabetic foot infections,based on severity.
MRSA is, in fact,
more virulent than
methicillin-sensitive
Staphylococcus
aureus (MSSA).
ments for MRSA that have been re-ported in the literature includemedical maggots. The larvae candebride wounds, removing necrofi-brotic tissue that leads to infection.They can also digest many types ofbacteria, including MRSA.12
Patients with MRSA generallybecome colonized, usually in theirnares or nasal pharynx, and they
can re-infect themselves at a laterdate or transfer the bacteria by di-rect contact to family members.There was some initial considera-tion given to cohorting MRSA pa-tients in hospitals to certain wingsor floors.
It is still general practice to iso-late admitted patients to a privateroom or place them in a room withanother known MRSA patient.Some facilities are performingMRSA decolonization. While it hasnot been shown to make much dif-
ference in the long-term, it mightbe able to reduce person-to-persontransmission in the home. The rec-ommendations for MRSA decolo-nization include:
1) Treat the underlying infec-tion.
2) Prescribe mupirocin oint-ment in both nares three timesdaily.
3) Remove piercing and fakenails during decolonization.
4) Shower every other day withHibiclens; pay extra attention tothe hairline.
5) Gargle with Peridex mouth-wash for 60 seconds and spit, twotimes daily.
6) Use clean clothes and towelsdaily during treatment.
7) Perform the above for twoweeks.
The nares can be swabbed forMRSA screening before and afterdecolonization. Repeat if necessary.
For general guidelines, the CDCrecommends patients wash theirhands frequently, or use an alco-hol-based hand sanitizer. Don’tshare razors, towels, or other per-sonal items. Wipe down equipmentwith an antiseptic before use at apublic gym.
Diabetic Foot InfectionsDiabetic foot infections should
be treated aggressively, since thehost is immune-suppressed, thecausative micro-organism can be re-
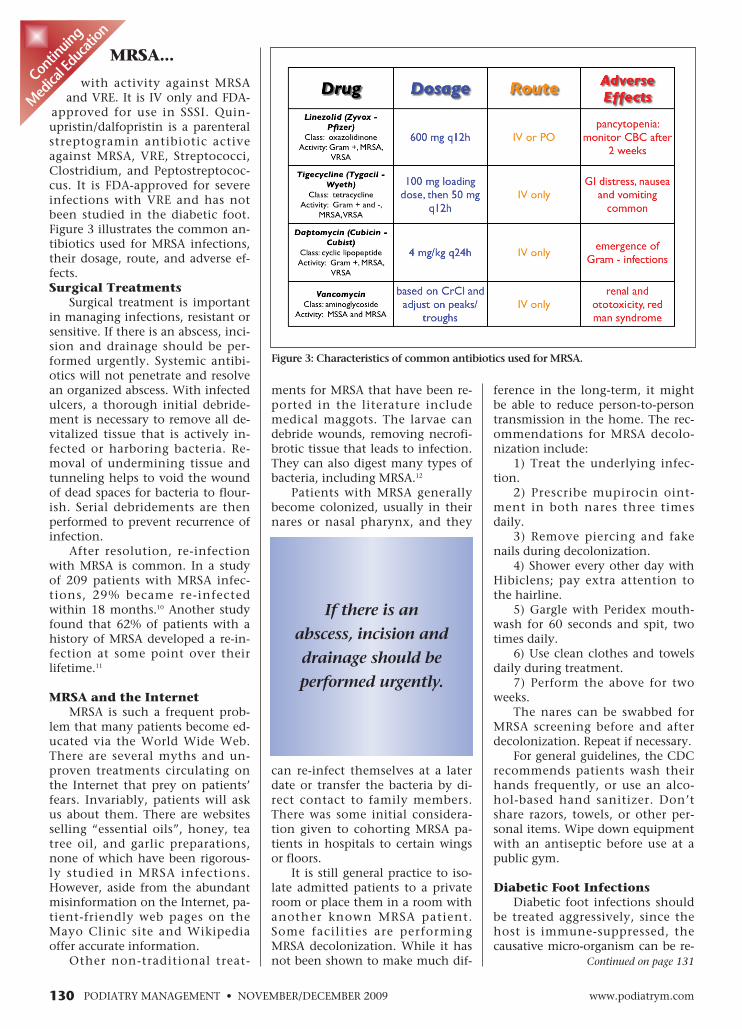
with activity against MRSAand VRE. It is IV only and FDA-
approved for use in SSSI. Quin-upristin/dalfopristin is a parenteralstreptogramin antibiotic activeagainst MRSA, VRE, Streptococci,Clostridium, and Peptostreptococ-cus. It is FDA-approved for severeinfections with VRE and has notbeen studied in the diabetic foot.Figure 3 illustrates the common an-tibiotics used for MRSA infections,their dosage, route, and adverse ef-fects.Surgical Treatments
Surgical treatment is importantin managing infections, resistant orsensitive. If there is an abscess, inci-sion and drainage should be per-formed urgently. Systemic antibi-otics will not penetrate and resolvean organized abscess. With infectedulcers, a thorough initial debride-ment is necessary to remove all de-vitalized tissue that is actively in-fected or harboring bacteria. Re-moval of undermining tissue andtunneling helps to void the woundof dead spaces for bacteria to flour-ish. Serial debridements are thenperformed to prevent recurrence ofinfection.
After resolution, re-infectionwith MRSA is common. In a studyof 209 patients with MRSA infec-tions, 29% became re-infectedwithin 18 months.10 Another studyfound that 62% of patients with ahistory of MRSA developed a re-in-fection at some point over theirlifetime.11
MRSA and the InternetMRSA is such a frequent prob-
lem that many patients become ed-ucated via the World Wide Web.There are several myths and un-proven treatments circulating onthe Internet that prey on patients’fears. Invariably, patients will askus about them. There are websitesselling “essential oils”, honey, teatree oil, and garlic preparations,none of which have been rigorous-ly studied in MRSA infections.However, aside from the abundantmisinformation on the Internet, pa-tient-friendly web pages on theMayo Clinic site and Wikipediaoffer accurate information.
Other non-traditional treat-
Continuing
MedicalEducation
Figure 3: Characteristics of common antibiotics used for MRSA.
Medical Educationsistant, and the infection can lead to amputation. Clini-cians should classify the infection according to the IDSAand prescribe the appropriate treatment based on the classof infection. There are many agents active against MRSA,but allergies, route of administration, and adverse effectsneed to be considered. Patients should be cautioned aboutfinding misinformation on the Internet and directed to re-liable websites. Once the MRSA infection resolves, the doc-tor should be vigilant in preventing re-infections. �
References1 McMahon MM, Bistrian BR. Host defenses and susceptibili-
ty to infection in patients with diabetes mellitus. Infect Dis ClinNorth Am. Mar 1995;9(1):1-9.
2 Tentolouris N, Jude EB, Smirnof I, Knowles EA, Boulton AJ.Methicillin-resistant Staphylococcus aureus: an increasing prob-lem in a diabetic foot clinic. Diabet Med. 1999;16(9):767-771.
3 Dang CN, Prasad YD, Boulton AJ, Jude EB. Methicillin-re-sistant Staphylococcus aureus in the diabetic foot clinic: a wors-ening problem. Diabet Med. Feb 2003;20(2):159-161.
5 Talon D, Woronoff-Lemsi MC, Limat S, et al. The impact ofresistance to methicillin in Staphylococcus aureus bacteremia onmortality. Eur J Intern Med. Feb 2002;13(1):31-36.
6 Grimble SA, Magee TR, Galland RB. Methicillin resistantStaphylococcus aureus in patients undergoing major amputation.Eur J Vasc Endovasc Surg. Sep 2001;22(3):215-218.
7 Richards T, Pittathankel AA, Pursell R, Magee TR, GallandRB. MRSA in lower limb amputation and the role of antibioticprophylaxis. J Cardiovasc Surg (Torino). Feb 2005;46(1):37-41.
8 Lavery LA, Armstrong DG, Murdoch DP, Peters EJ, LipskyBA. Validation of the Infectious Diseases Society of America’s dia-betic foot infection classification system. Clin Infect Dis. Feb 152007;44(4):562-565.
9 Armstrong DG, Boulton AJM, Joseph WS, Lipsky BA, RogersLC. A closer look at the prevalence of MRSA and its impact onempiric therapy. Wounds. 2008;8(12 Suppl):S5-10.
10 Huang SS, Platt R. Risk of methicillin-resistant Staphylo-coccus aureus infection after previous infection or colonization.Clin Infect Dis. Feb 1 2003;36(3):281-285.
12 ArmstrongDG, Salas P, ShortB, et al. Maggottherapy in“lower-extremityhospice” woundcare: fewer ampu-tations and moreantibiot ic- freedays. J Am Podia-tr Med Assoc.M a y - J u n2005;95(3):254-257.
MRSA...
1) Which of the following is NOT a known riskfactor for MRSA?A) Recent hospitalizationB) Incarceration in a prisonC) Multiple recent antibiotic usageD) Owning a pet
2) Which of the following drugs is NOT a goodchoice for MRSA?A) LinezolidB) Trimethoprim/sulfaC) MethicillinD) Minocycline
3) Healthcare-associated (formerly hospital-acquired) MRSA can be treated with all BUTwhich of the following?A) CephalexinB) LinezolidC) VancomycinD) Tigecycline
4) De-escalation therapy for diabetic footinfections is:A) Using a broad-spectrum anti-MRSA agentfirst, then narrowing the spectrum after cul-ture and sensitivity is reportedB) Using a broad-spectrum oral antibioticand not checking the culture and sensitivityC) Using a narrow-spectrum agent and thenswitching to a broad-spectrum if neededD) Just performing an incision and drainagewithout antibiotics
5) The D-test is used to determine if which an-tibiotic can be used for MRSA?A) PenicillinB) MethicillinC) ClindamycinD) Cephalexin
6) Which of the following tests can identifyMRSA in two hours or less?A) DNA swab for MRSAB) Culture and sensitivityC) Complete blood count (CBC)D) Erythrocyte sedimentation rate (ESR)
See instructions and answer sheeton pages 202-204.
Continued on page 132
E X A M I N A T I O N
Dr. Rogers is an Associ-ateMedical Director ofthe Amputation Pre-vention Center at Val-ley PresbyterianHospi-tal in Los Angeles, CA.He serves as the Chairof the Foot Care Coun-cil for the AmericanDiabetes Association.He is board certified byABPOPPM and a fel-lowofACFAOM.
Dr. Bevilacqua isan Associate MedicalDirector of the Ampu-tation Prevention Cen-ter at Valley Presbyteri-an Hospital in Los An-geles, CA. He is boardcertified by ABPS anda fellowofACFAS.
11) What is the proper way toculture a wound?A) Swab the surfaceB) Send a deep tissuespecimenC) Send purulent drainageD) Do a bone biopsy
12) What is the only FDA ap-proved antibiotic for MRSA skininfections available in oral form?A) VancomycinB) TigecyclineC) DaptomycinD) Linezolid
13) Which antibiotic requirespeaks and troughs to appropri-ately dose?A) VancomycinB) TigecyclineC) DaptomycinD) Linezolid
14) Which antibiotic can causerenal or ototoxicity?A) VancomycinB) TigecyclineC) DaptomycinD) Linezolid
15) Which recommendationscan help prevent spread ofMRSA colonization?A) Washing handsfrequentlyB) Don’t share razors orother personal itemsC) Wipe down gym equip-ment before useD) All of the above
16) Where is the most commonsite of MRSA colonization?A) Nares and nasopharynxB) RectumC) Arm pitD) Lateral nail folds
7) What is the most urgenttreatment for an MRSA abscess?A) Warm compressesB) AntibioticsC) HeparinD) Incision and drainage
8) Which of the following de-scribes an IDSA severe infec-tion?A) A wound with noerythemaB) A wound with less than 2cm of erythemaC) A wound with greaterthan 2 cm of erythema andosteomyelitisD) A wound with greaterthan 2 cm of erythema inthe presence of a fever,tachycardia, and bacteremia
9) Which of the following de-scribes an IDSA Mild infection?A) A wound with noerythemaB) A wound with less than 2cm of erythemaC) A wound with greaterthan 2 cm of erythema andosteomyelitisD) A wound with greaterthan 2 cm of erythema inthe presence of a fever,tachycardia, and bacteremia
10) According to this article,which describes the best treat-ment for an IDSA moderateinfection?A) Incision and drainage, ad-mission to the hospital, IVantibiotics with MRSAde-escalationB) Incision and drainageand dischargeC) Oral antibioticsD) Tetanus prophylaxis
E X A M I N A T I O N(cont’d)
SEE INSTRUCTIONSAND ANSWER SHEETON PAGES 202-204.
17) Which of the followingis true, regarding MRSAprevalence?A) MRSA is becomingcontrolledB) MRSA has beeneradicatedC) MRSA infections aresteadyD) MRSA prevalence isincreasing
18) Which does NOT predis-pose a patient with diabetesto an infection?A) Immunopathy (immunesuppression)B) Open ulcerC) Poor glucose controlD) Good glucose control
20) Which of the followingtreatments are available forsale to patients on the Inter-net without having provenefficacy for MRSA?A) Medical maggotsB) LinezolidC) Tea tree oil and garlicpreparationsD) Vancomycin