72
Current evidence based guidelines for management of medical emergencies EMERGENCY MANUAL
| Date post: | 29-Nov-2015 |
| Category: |
Documents |
| Upload: | rumana-ali |
| View: | 74 times |
| Download: | 0 times |
Current evidence
based guidelines for
management of
medical emergencies
EMERGENCY MANUAL

FORWARDThis Manual is intended for use by primary carers who are called upon tomanage medical emergencies in both community and hospital settings.
It should be emphasised that the management protocols contained in theManual are intended as a guide and should not be seen as appropriate forevery patient and in all circumstances. In particular, great care should be takento individualise treatments to account for individual patient’s comorbidities, andto ensure familiarity with the doses, indications, contraindications, reactions andinteractions of all medications used.
For many conditions, a distinction has been made between hospital andprehospital treatments. However, as treatment protocols may vary somewhatfrom setting to setting – particularly in more remote areas - it is important tobecome familiar with the way in which emergency services and treatmentprotocols vary in the specific location concerned.
Communication by telephone, fax and internet is now so advanced thatongoing management decisions can often be made in consultation withspecialist colleagues. This should be encouraged as it always improves patientoutcomes, and is essential when transfer of care is contemplated.
Chris CooperConvenor, Course in Emergency MedicineDepartment of General Practice University of Sydney
September 2006

CONTENTS1. CARDIAC ARREST page 5
2. ACUTE CORONARY SYNDROMES 10
3. ATRIAL FLUTTER AND FIBRILLATION 17
4. SUPRAVENTRICULAR TACHYCARDIA (PSVT) 22
5. VENTRICULAR TACHYCARDIA 24
6. CARDIOVERSION 27
7. SINUS BRADYCARDIA 28
8. ATRIOVENTRICULAR RHYTHM AND BLOCK 28
9. ACUTE PULMONARY OEDEMA 31
10. ARRYTHMIAS IN HEART FAILURE 33
11. ACUTE LIMB ISCHEMIA 34
12. TEMPORAL ARTERITIS 35
13. DEEP VEIN THROMBOSIS 36
14. PULMONARY EMBOLISM 38
15. SHOCK 39
16. ACUTE ASTHMA 40
17. CROUP 42
18. COMPLETE UPPER AIRWAY OBSTRUCTION 44
19. ACUTE EXACERBATION OF COPD 48
20. PNEUMOTHORAX 50
21. COMMUNITY ACQUIRED PNEUMONIA 52
22. HYPOGLYCEMIA 53
23. DIABETIC KETOACIDOSIS 54
24. HYPEROSMOLAR HYPERGLYCAEMIA 56
25. LACTIC ACIDOSIS IN DIABETES 56
26. MENINGOCOCCAL DISEASE 57
27. MENINGITIS 58
28. STATUS EPILEPTICUS 59
29. ACUTE STROKE 60
30. ACUTE ANAPHYLAXIS 61
31. DRUG OVERDOSE 62
32. ACUTE UPPER GASTROINTESTINAL BLEED 64
33. HYPERKALEMIA 65
34. URGENT ELECTROLYTE ABNORMALITIES 66
35. PAEDIATRIC FLUID REPLACEMENT 66
36. INTEROSSEOUS INFUSION NEEDLE PLACEMENT 67
APPENDIX 1. IV DRUG INFUSIONS 68
APPENDIX 2. EMERGENCY TELEPHONE NUMBERS 70
APPENDIX 3. PAEDIATRIC DRUG DOSES 71
www.gpkit.com.au 3

CARDIAC ARREST
INITIAL RESPONSE1. Check for responsiveness ‘Shake and shout’
2. Call for help Ring 000. Advise “cardiac arrest, CPR in progress”
3. Look, listen, feel for respirations
COMMENCE BASIC CPRIndication for CPR: not conscious+ not moving + not breathing normally1
Do not attempt to find carotid pulse; difficult, unnecessary, time consuming.2
Any attempt at CPR is better than no attempt at all.1
Early basic CPR increases survival by 50%.
Basic CPR does not restore sinus rhythm – it supports circulation pending thearrival of a defibrillator.
1. External cardiac compression.
Cardiac compression centre of chest ie over lower half of sternum1
Compressions should be delivered hard and fast.1
Ignore number of compressions per minute.1
Compressions to ventilations 30:2 – (for 1 & 2 person, children & adults)1
Interruptions to compressions should be minimised – no pause forventilations1
NOTE: Compressions are more important than ventilations. There is growingevidence that chest compressions alone are as effective as compressions plusventilation in the first 10 minutes of resuscitation. This is of particular relevancewhen lay operators are reluctant to administer mouth-to-mouth resuscitation.
2. Assisted ventilation
Clear airway: head tilt, jaw thrust, clear oropharynx with sweep with indexfinger. Insert Guidels airway or endotracheal tube.
Ventilations by bag and mask, mouth to mouth.
Compressions to ventilations 30:2 – for both 1 or 2 person CPR)1
Ignore number of ventilations per minute.1
Overventilation should be avoided.1
www.gpkit.com.au 5

3. Defibrillation.
If a defibrillator is available, defibrillation shock should be delivered asan initial manouver – before 1 & 2 above.
Give three shocks in quick succession.
Shock strengths:
a. Monophasic defibrillator: all shocks 360 joules1
b. Biphasic defibrillator: all shocks 200 joules1
After each defibrillation attempt, give two minutes of CPR before checkingrhythm.
NOTE: There is some evidence a short period of 5 chest compressions priorto defibrillation improves chances of reverting to sinus rhythm.
4. Adrenaline.
When adrenaline is available it should be given IV every three minutesirrespective of the rhythm, in order to maintain vascular tone.
5. Subsequent treatment
If an electrocardiogram is available, treat according to the rhythm underlyingdisorder (see below).
If rhythm is unknown all subsequent treatment should be based on theassumption that the underlying rhythm is ventricular fibrillation.
REFERENCES1. International liaison committee on Resuscitation (ILCOR) Consensus on Science and
Treatment Recommendations. Resuscitation. 2005: 67(2-3): 157-341.2. Introduction to the International Guidelines 2000 for CPR and ECC Circulation. 2000;102:I-1. 3. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
VENTRICULAR FIBRILLATION(or pulseless ventricular tachycardia)
Treatment should be given on a background of ongoing basic CPR as outlinedabove.
1. Defibrillation. Perform as initial manoeuvre. Single shock (ie not stackedshocks) for VF or pulseless VT.1
2. Adrenaline 1mg (1ml of 1:1000 or 10mls of 1:10000 solution) IV Give every3-5 minutes. Defibrillate within 30secs of each bolus unless found to be inasystole. If there is no venous access, adrenaline can be given via ETT attwice the IV dose.
3. Antiarrhythmic therapy. If still in VF after x3 cycles of adrenaline consider:
a. amiodarone 5 mg/kg IV, via a central line over 20 minutes then 10 to 15mg/kg over 24 hours
6 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

b. sotalol 1 to 2 mg/kg IV, over 10 to 30 minutes, repeat if necessary at 10minute intervals
c. lignocaine 75 to 100 mg IV, over 1 to 2 minutes, followed by 4 mg/minutefor a maximum of 1 hour, then 1 to 3 mg/minute by IV infusion.
4. Sodium bicarbonate. If resuscitation is prolonged beyond 10 to 15 minutes,or if pH<7.2 on blood-gas analysis, use sodium bicarbonate 8.4% (1mmol/mL) 1 mmol/kg IV, over 5 to 15 minutes.
If unable to establish IV access and patient is intubated all drugs (exceptbicarbonate) may be given down ETT at twice normal dose.
REFERENCES1. International liaison committee on Resuscitation (ILCOR) Consensus on Science and
Treatment Recommendations. Resuscitation. 2005: 67(2-3): 157-341.2. Introduction to the International Guidelines 2000 for CPR and ECC Circulation. 2000;102:I-1. 3. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
ASYSTOLETreatment should be given on a background of ongoing basic CPR as outlinedabove.
NOTE: Asystole occurs in about 20% of cardiac arrest, and its prognosis isuniformly poor.
When asystole occurs as the initial rhythm it is often secondary to underlyingproblems which may require specific treatment. These include hypoxia,hyper/hypokalemia, acidosis, drug overdose and hypothermia.
1. Adrenaline 1mg (1ml of 1:1000 or 10mls of 1:10000 solution) IV Give every5 minutes. If there is no venous access, adrenaline can be given byintratracheal administration at twice the IV dose. Evidence regarding efficacyis conflicting.
2. Atropine 1.0mg IV. Repeat every 3-5 minutes to total dose of 0.04mg/kg.(ieabout 3mg for 70kg man).
3. Sodium bicarbonate If resuscitation is prolonged beyond 10 to 15 minutes,or particularly if pH<7.2 on blood-gas analysis, give sodium bicarbonate8.4% (1 mmol/mL) 1 mmol/kg IV, over 5 to 15 minutes.
NB: Defibrillation shocks should not be administered in asystole – it isineffective and shocks may damage the myocardium. However… care must betaken to exclude apparent/artifactual asystole due to:
• incorrect lead placement
• very fine VF
www.gpkit.com.au 7
8 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
If unable to establish IV access and patient is intubated all drugs (exceptbicarbonate) may be given down ETT at twice normal dose.
REFERENCES1. International liaison committee on Resuscitation (ILCOR) Consensus on Science and
Treatment Recommendations. Resuscitation. 2005: 67(2-3): 157-341.2. Introduction to the International Guidelines 2000 for CPR and ECC Circulation. 2000;102:I-1. 3. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
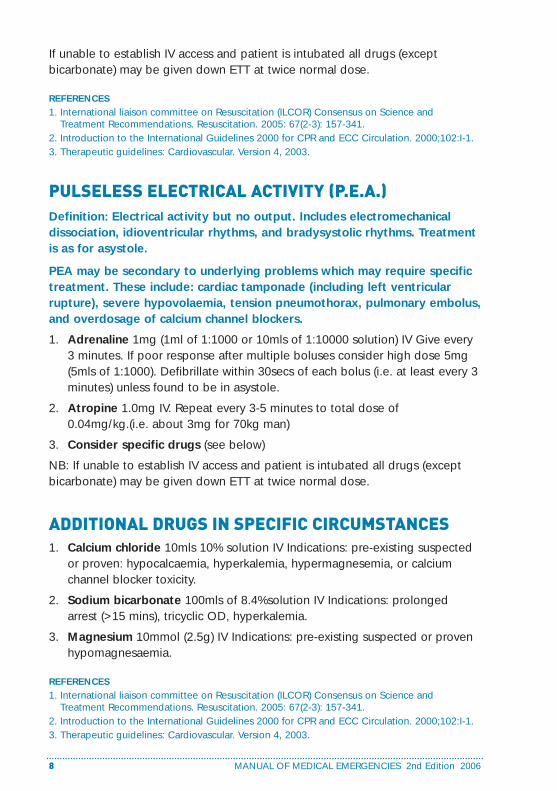
PULSELESS ELECTRICAL ACTIVITY (P.E.A.)Definition: Electrical activity but no output. Includes electromechanicaldissociation, idioventricular rhythms, and bradysystolic rhythms. Treatmentis as for asystole.
PEA may be secondary to underlying problems which may require specifictreatment. These include: cardiac tamponade (including left ventricularrupture), severe hypovolaemia, tension pneumothorax, pulmonary embolus,and overdosage of calcium channel blockers.
1. Adrenaline 1mg (1ml of 1:1000 or 10mls of 1:10000 solution) IV Give every3 minutes. If poor response after multiple boluses consider high dose 5mg(5mls of 1:1000). Defibrillate within 30secs of each bolus (i.e. at least every 3minutes) unless found to be in asystole.
2. Atropine 1.0mg IV. Repeat every 3-5 minutes to total dose of0.04mg/kg.(i.e. about 3mg for 70kg man)
3. Consider specific drugs (see below)
NB: If unable to establish IV access and patient is intubated all drugs (exceptbicarbonate) may be given down ETT at twice normal dose.
ADDITIONAL DRUGS IN SPECIFIC CIRCUMSTANCES1. Calcium chloride 10mls 10% solution IV Indications: pre-existing suspected
or proven: hypocalcaemia, hyperkalemia, hypermagnesemia, or calciumchannel blocker toxicity.
2. Sodium bicarbonate 100mls of 8.4%solution IV Indications: prolongedarrest (>15 mins), tricyclic OD, hyperkalemia.
3. Magnesium 10mmol (2.5g) IV Indications: pre-existing suspected or provenhypomagnesaemia.
REFERENCES1. International liaison committee on Resuscitation (ILCOR) Consensus on Science and
Treatment Recommendations. Resuscitation. 2005: 67(2-3): 157-341.2. Introduction to the International Guidelines 2000 for CPR and ECC Circulation. 2000;102:I-1. 3. Therapeutic guidelines: Cardiovascular. Version 4, 2003.

PAEDIATRIC CARDIAC ARREST Current guidelines recommend:
• Interosseous access rather than IV access – unless prior IV access
• Mouth-to-nose ventilation is an alternative to mouth to mouth
• Two-thumb, chest-encircling compressions for children <2 yrs
• Compression to ventilation ratio: 15:21
• Adrenaline (1:1000) 0.01 mls/kg
• Adrenaline (1:10000) 0.1 mls/kg
• Cardioversion – initial shock 2 joules/kg1
• Cardioversion – subsequent shocks 5 joules/kg1
• Amiodarone 5mg/kg
• Lignocaine 5 mg/kg
REFERENCES1. International liaison committee on Resuscitation (ILCOR) Consensus on Science and
Treatment Recommendations. Resuscitation. 2005: 67(2-3): 157-341.2. Introduction to the International Guidelines 2000 for CPR and ECC Circulation. 2000;102:I-1. 3. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 9
ACUTE CORONARYSYNDROMESAcute coronary syndromes (ACS) are clinical syndromes consistent withmyocardial infarction or accelerated angina, characterised by chest pain ordiscomfort at rest or for >10 minutes which is unrelieved by anginine, orwhich is associated with syncope or cardiac failure. Associated symptomsof dyspnoea, diaphoresis, nausea or vomiting may be prominent oroccasionally occur in isolation. Atypical presentations are more common inwomen, diabetes, and in the elderly.
IMMEDIATE PREHOSPITAL TREATMENT1. Arrange urgent ambulance transport. 50% of fatalities following ACS
occur within 2 hours of onset of chest pain, and are due to reversiblearrthymias. The immediate and urgent requirement is to ensure access to adefibrillator in order to avoid early avoidable cardiac death from treatablearrthymias. All Australian ambulances now carry defibrillators.
2. Oxygen at least 8L/min.
3. Antiplatelet therapy.
Aspirin 150mg P.O. crushed or dissolved to hasten absorption. This has amajor influence on outcome.
PLUS
Clopidogrel Initial loading dose 300 mg. NB: If early cardiac surgery isconsidered likely clopidogrel should be withheld until the coronary anatomyis known.
4. Nitrates
Providing BP>100 mm HG
a. glyceryl trinitrate spray 400 micrograms sublingually, repeat after 5minutes if pain persists (up to a maximum of 2 metered doses)
OR
b. glyceryl trinitrate tablet 600 micrograms sublingually, repeat every 3 to 5minutes up to a maximum dose of 1800 micrograms (3 tablets) Ifpossible, ensure cannula inserted before giving anginine as may causeprecipitous hypotension. Give 1/2-1 SL (1/4-1/2 if first nitrates or in theelderly). Repeat 5-15mins PRN. providing BP>100 mm Hg. If >3 dosesrequired consider glyceryl trinitrate paste, patch or infusion
c. Glyceryl trinitrate paste 2.5-5cm
10 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
d. Glyceryl trinitrate patch 25 or 50mg. Remove and wipe skin if BP falls<100mmHg. Remove after 18 hours, reapply after 6 hours.
NB: Avoid nitrates if the patient has used sildenafil (Viagra) in the previous 24hours or tadalafil (Cialis) in the previous five days.
5. Morphine 2.5-5mg IV Providing BP>100 mm Hg. (+/- Maxalon 10mg IV q8h)Repeat PRN until pain relieved, and providing BP>100 mm Hg, to max10mg IV.
6. B-blockers: Consider if tachycardic and no contraindications.
a. Metoprolol 5mg q5min IV x3, then 50mg q6h PO, OR
b. Atenolol 5mg q5min IV x2, then 100mg/day PO
7. Take a 12-lead ECG providing it does not delay transfer. The ECG is the soletest which further defines acute coronary syndromes and determines theneed for emergency reperfusion.
8. Telephone receiving facility of incoming patient with ACS.
1. NON-ST SEGMENTELEVATION ACUTECORONARY SYNDROME(NSTEACS)NSTEACS is defined as an acute coronary syndrome which occurs in theabsence of ECG changes of ST segment elevation or left bundle branchblock.
TREATMENT IN HOSPITALRisk stratification.
All patients NSTEACS should undergo risk stratification. Risk stratificationdetermines subsequent management.
(See Table next page)
www.gpkit.com.au 11

12 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
High risk ANY of the following:
• Repetitive or prolonged chestpain.
• At least one elevated cardiacbiomarker.
• Persistent ST segment depressionor new T wave inversion.
• Transient ST elevation in twoleads.
• Hemodynamic compromise.
• Sustained VT
• Syncope
• Left ventricular ejection fraction<0.40
• Prior PCI within last 6/12
• Prior CABG
• Known diabetes
• Chronic kidney disease
Aggressive management with:
• platelet inhibitors,
• antithrombintherapy,
• B blockers,
• glycoproteinIIb/IIIa inhibitors
• Arrange coronaryangiography andrevascularisation.
Intermediate ANY of the following:
Chest pain at rest now resolved.
Age >65 years
Known CAD
No high risk ECG changes (above)
Two or more of the following: HT,family history, current smoking,hyperlipidemia. Presence of knowndiabetes.
Chronic kidney disease
Prior aspirin use
Accelerateddiagnosticevaluation to allowreclassification ashigh or low risk.
Low ACS without high or intermediaterisk features.
May be dischargedwith upgradedmedical assessmentfor followup.
Risk Criteria Management

Management of 'high risk' NSTEACS1. IV glyceryl trinitrate
Indications: Persistent or recurrent rest pain + ischaemic changes on ECG +poor response to glyceryl trinitrate sublingual, paste or patch.
Give: 10 micrograms/minute by IV infusion, increase by 10micrograms/minute every 3 minutes until pain is controlled, providing thesystolic blood pressure (SBP) >95 mm Hg.
Then: titrate to relieve pain and to keep BP>100 mm Hg.
NB: Avoid nitrates if the patient has used sildenafil (Viagra) in the previous24 hours or tadalafil (Cialis) in the previous five days.
2. Antithrombin therapy
Give low molecular weight heparin (LMWH) or unfractionated heparin (UFH):
LMWH is generally preferred. UFH requires constant monitoring, but has theadvantage that may be easily reversed in high-risk patients who may requireurgent intervention.
NB: Care should be taken in the elderly and in those with impaired renalfunction, in whom the dose should be reduced to once daily.
Enoxaparin 1 mg/kg SC, twice daily
OR
Dalteparin 120 international units/kg SC, twice daily to a maximum of 10000 units
OR
dalteparin 120 international units/kg SC, twice daily to a maximum of 10 000units
OR
unfractionated heparin 5000 units bolus IV, followed by 1000 units/hour byIV infusion, then adjust according to APTT. Monitoring: activated partialthromboplastin time (APTT) should be checked initially every 6 hours, aimingfor a range of 60 to 80 seconds, and should be checked daily once therapyhas been stabilised.
3. Beta blocker (Unless contraindicated)
Give:
atenolol 25 to 100 mg orally, once daily
or
metoprolol 25 to 100 mg orally, twice daily.
Patients in whom Bblockers are contraindicated give:
www.gpkit.com.au 13

Nondihydropyridine calcium channel blocker
Give:
diltiazem 30 to 120 mg orally, 3 times daily
OR
diltiazem controlled-release 180 to 360 mg orally, daily
OR
verapamil 40 to 120 mg orally, 2 to 3 times daily
OR
verapamil sustained-release 160 to 480 mg orally, daily.
4. Glycoprotein IIb/IIIa inhibitors
Indications: high risk patients with abnormal ECGs or positive troponin.
a. In the coronary care unit, tirofiban (0.4 micrograms/kg/minute loadingdose administered over 30 minutes, followed by a maintenance infusionof 0.1 micrograms/kg/minute for up to 72 hours), may be given, thenfollowed by percutaneous procedures if indicated.
b. In the cardiac catheterisation laboratory abciximab (250 micrograms/kgbolus loading dose, followed by a maintenance infusion dose of 0.125micrograms/kg/minute to a maximum of 10 micrograms/minute) givenover the 12 hours following the PCI.
5. Revascularisation Revascularisation should be considered in all patientswho are at high risk. Clinical trials have demonstrated the benefit of an earlyinvasive strategy
REFERENCES1. National heart foundation of Australia/ The Cardiac Society of Australia and New Zealand.
'Guidelines for the management of acute coronary syndromes' 2006. Med J Aust 2006; 184;S1-S32
2. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
14 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

2. ST SEGMENT ELEVATIONMYOCARDIAL INFARCTION(STEMI)STEMI is defined as an acute coronary syndrome with ECG featuresincluding any of:
• persistent ST-segment elevation of greater than 1mm in two contiguous limbleads
• ST-segment elevation of greater than 2mm in two contiguous chest leads;
• new left bundle branch block (LBBB) pattern. NB: LBBB is presumed newunless there is evidence otherwise.
MANAGEMENT1. Specific prehospital treatment. Where formal protocols are in place,
prehospital treatment should be given, including fibrinolysis in appropriatecases.
2. Emergency reperfusion ie fibrinolytic therapy OR direct percutaneouscoronary intervention (PCI), is indicated in all patients with STEMI whopresent within 12 hours of the onset of ischaemic symptoms.
a. In general, direct percutaneous coronary intervention (PCI) is thetreatment of choice, providing it can be performed promptly by aqualified interventional cardiologist in an appropriate facility. Themaximum acceptable delay from presentation to balloon inflation is 60minutes if a patient presents within 1 hour of symptom onset; or 90minutes if a patient presents later.
b. Fibrinolytic therapy. Second-generation fibrin-specific fibrinolytic agentsthat are available as a bolus (ie, reteplase, tenecteplase) are thefibrinolytics of choice.
3. Antiplatelet treatment. All patients undergoing reperfusion therapy forSTEMI (PCI or fibrinolysis) should be given aspirin and clopidogrel unlessthese are contraindicated. Clopidogrel should not be given if the need foracute CABG is likely.
a. Aspirin 150mg P.O. crushed or dissolved to hasten absorption. This hasa major influence on outcome.
PLUS
b. Clopidogrel Initial loading dose 300 mg. NB: If early cardiac surgery isconsidered likely clopidogrel should be withheld until the coronaryanatomy is known.
www.gpkit.com.au 15

4. Antithrombin agents.
Give low molecular weight heparin (LMWH) or unfractionated heparin (UFH):
LMWH is generally preferred. UFH requires constant monitoring, but has theadvantage that may be easily reversed in high-risk patients who may requireurgent intervention.
NB: Care should be taken in the elderly and in those with impaired renalfunction, in whom the dose should be reduced to once daily.
Enoxaparin 1 mg/kg SC, twice daily
OR
Dalteparin 120 international units/kg SC, twice daily to a maximum of 10 000 units
OR
dalteparin 120 international units/kg SC, twice daily to a maximum of 10 000units
OR
unfractionated heparin 5000 units bolus IV, followed by 1000 units/hour byIV infusion, then adjust according to APTT. Monitoring: activated partialthromboplastin time (APTT) should be checked initially every 6 hours, aimingfor a range of 60 to 80 seconds, and should be checked daily once therapyhas been stabilised. Care should be taken in patients aged over 75 years, orthose who have significant renal dysfunction — dose adjustment is required.
REFERENCES1. National heart foundation of Australia/ The Cardiac Society of Australia and New Zealand.
'Guidelines for the management of acute coronary syndromes' 2006. Med J Aust 2006; 184;S1-S32.
2. Therapeutic guidelines: Cardiovascular. Version 4, 2003.
16 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

ATRIAL FLUTTER ANDFIBRILLATION
INTRODUCTION1. Atrial fibrillation rarely causes death or serious morbidity except via
thromboembolism.
2. Anticoagulation should be considered in ALL patients in whom AF isdiscovered.
3. Rhythm control is no better than rate control. AF is frequently anasymptomatic finding, especially in the elderly. Many elderly patients andmost younger patients, however, find the arrhythmia itself producesdisturbing symptoms, and it is particularly in this group where one or moreattempts at conversion to sinus rhythm, either electrically orpharmacologically, are commonly employed.
However rate control is a perfectly acceptable first-line strategy and not justa 'fall-back' if rhythm control fails or proves difficult. In either case, dueattention should be given to the question of thromboembolic prophylaxis.
4. Management requires prior assessment of ventricular function and/ orcoronary artery disease. As many of the rhythm control drugs and some ofthose used for rate control have myocardial depressant or proarrhythmicpotential, it is essential to have some idea of whether or not the patient hasnormal left ventricular function and/or coronary disease. This information isnot always available on first presentation however.
5. Recent onset AF generally requires admission to hospital foranticoagulation. This is to avoid thromboembolism arising from 'atrialstunning' which commonly follows spontaneous or induced cardioversion.
ANTICOAGULATIONInitial anticoagulation
Enoxaparin 1 mg/kg SC, twice daily
OR
Dalteparin 120 international units/kg SC, twice daily to a maximum of 10 000 units
OR
Dalteparin 120 international units/kg SC, twice daily to a maximum of 10 000 units.
www.gpkit.com.au 17

Subsequent anticoagulation is dependent on risk stratification.
Anticoagulation with warfarin reduces the risk of stroke by about 70% inpatients with nonvalvular AF.
Aspirin at 325 mg/day seems to provide about one-third to one-half theprotection provided by warfarin.
Indications for warfarin are determined by three risk categories forthromboembolism*.
Warfarin 5 mg orally, daily. (reduced in the very elderly.) Target INR: 2 to 3,or 2.5 to 3.5 (in patients who have already suffered thromboembolic event).
RATE CONTROL1. Obtain and maintain long-term control of ventricular rate, use
a atenolol 25 to 100 mg orally, daily OR
b metoprolol 25 to 100 mg orally OR
c diltiazem controlled-release 180 to 360 mg orally, daily twice daily OR
d verapamil sustained-release 160 to 480 mg orally, daily
18 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
High Intermediate Low
History ofThromboembolicevent orlongstanding mitralvalve disease
HistoryThromboembolicevent or longstandingmitral valve disease
Nil
10-15% 3-5% 0.5-1%
Long-term warfarin(unless strongcontraindications.)
Long-term warfarinbased on clinicaljudgement.
Probably noWarfarin.Consideraspirin.
RiskCategory
Risk Factors
Annual riskof Thromob-oembolism
Management

2. Consider digoxin. In elderly, sedentary patients, additionally, or as stand-alone therapy, consider digoxin 62.5 to 250 micrograms orally, daily,according to age, plasma creatinine and plasma digoxin levels (steady stateis achieved in approximately 5 days). (Digoxin alone frequently fails tocontrol exercise-induced tachycardia. An alternative or additional therapy tocontrol ventricular rate is often indicated.)
3. If the IV route is indicated give:
a metoprolol 5 to 10 mg IV OR esmolol 500 micrograms/kg IV, over 1minute, then titrate to achieve desired ventricular rate, typically 50 to200 micrograms/kg/minute OR
b verapamil 1 mg/minute IV, up to 15 mg with careful blood pressuremonitoring OR
c digoxin 0.5mg in 20mls 5%D IV over 10-30mins. Repeat after 6hr. Thencontinue normal oral dose. CI: Digoxin in preceding 2 weeks. Althoughdigoxin is often given IV in this situation and is unlikely to do any harm(whereas the other agents do have cardiodepressant potential), but isalso very unlikely to have much effect on ventricular rate in the shortterm.
RHYTHM CONTROL: CARDIOVERSIONPharmacological cardioversion:
1. Oral cardioversion give
a flecainide 50 to 100 mg orally, 2 to 3 times daily (if normal left ventricularfunction and no coronary disease) OR
b amiodarone 200 to 400 mg orally, 3 times daily, aiming eventually toreduce to 100 to 200 mg per day
2. If IV cardioversion is indicated give:
a amiodarone 5 mg/kg IV, via a central line over 20 minutes to 2 hours,then 10 to 15 mg/kg over 24 hours. OR
b flecainide 2 mg/kg IV, over 30 minutes.
NB 1. Anticoagulation with warfarin should be started 2-6/52 beforecardioversion. Transoesophageal echocardiography has 95 percentsensitivity for detecting atrial thrombus. In situations where this test isavailable, the demonstrated absence of thrombus at recenttransoesophageal echocardiography—'recent' meaning within 12 to24 hours at most, and preferably within the previous 12 hours—obviates the need for prolonged warfarin therapy prior to attemptedconversion.
www.gpkit.com.au 19

20 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
2. Anticoagulation during and after cardioversion. Atrial stunning. There issignificant risk of thromboembolism in the days following direct currentcardioversion. This may be due to 'atrial stunning' causing weak atrialcontractions for hours or days, despite sinus rhythm. Partly for thisreason, but also because of the high initial incidence of relapse to AFfollowing elective cardioversion, anticoagulation with heparin or warfarinshould be initiated prior to or at the time of cardioversion, even if thetransoesophageal echocardiography confirms no intra-atrial thrombus.There is no consensus on the ideal duration of postcardioversion warfarintherapy if SR is successfully restored and maintained, but current practiceranges anywhere from 1 to 12 months depending on the risk ofembolism—which in turn is a function of the presence of known riskfactors for atrial thrombosis, and the perceived likelihood of relapse intoAF.
3. If using flecainide, thought should be given to the possibility ofaccelerating the ventricular rate (a higher proportion of atrial impulsesbeing conducted through the AV node—especially in atrial flutter).Consider pre-treatment with an AV nodal blocking agent such as digoxinor a beta blocker or nondihydropyridine calcium antagonist.
4. Sotalol is frequently used for attempted pharmacological reversion, butthe evidence suggests it is no more effective than placebo, in contrast toits well-documented efficacy in maintenance of SR long-term. NB: If drugtherapy fails to convert to SR within a reasonable time, synchronisedelectrical cardioversion should be considered.
Long-term antiarrhythmic therapy after cardioversion,
Oral antiarryhmics
a sotalol 40 to 160 mg orally, twice daily (monitor for excessive QTprolongation; cease if QT or QTc exceeds 500 or increases by >20%from baseline; use low doses or not at all in patients with impaired renalfunction), OR
b flecainide 50 to 100 mg orally, twice daily (in patients with normal leftventricular function and no coronary disease), OR
c amiodarone 200 to 400 mg orally, 3 times daily, aiming eventually toreduce to 100 to 200 mg per day.
NB 1. Amiodarone has been shown to be the most effective of these but islisted third because of its long-term adverse effect profile.
2. Long-term antiarrhythmic therapy is not required if atrial flutter or AF isassociated with a transient condition, eg acute myocardial infarction (MI),cardiothoracic surgery, excessive alcohol. Consider whether the risksassociated with recurrence outweigh those of long-term antiarrhythmictreatment.

3. In patients without a precipitating cause, long-term antiarrhythmictherapy will maintain SR in about 50 percent of patients at 12 monthsafter DC cardioversion.
4. There is no consensus about duration of anticoagulation followingsuccessful cardioversion, but as many strokes occur soon after relapseinto AF, a good rule of thumb is to err on the side of continuing warfarinwhenever there is thought to be a reasonable risk of relapse (i.e.generally much longer than the one month which has been commonpractice in the past). More invasive procedures, such as His bundleablation with pacemaker implantation, radiofrequency ablation of atrialflutter pathway, or surgical approaches, may be considered in patientswhose ventricular rate is poorly controlled with antiarrhythmic therapy.
REFERENCES1. Non-valvular atrial fibrillation and stroke prevention. Graeme J Hankey, on behalf of the
National. Blood Pressure Advisory Committee of the National Heart Foundation. MJA 2001;174: 234-348.
2. Therapeutic guidelines: Cardiovascular. Version 4, 2003.3. Consensus guidelines for warfarin therapy. Recommendations from the Australasian Society of
Thrombosis and Haemostasis. Alex S Gallus, Ross I Baker, Beng H Chong, Paul A Ockelfordand Alison M Street on behalf of the Australasian Society of Thrombosis andHaemostasis.MJA 2000; 172: 600-605
www.gpkit.com.au 21

PAROXYSMALSUPRAVENTRICULARTACHYCARDIA
(Narrow complex tachycardia )NOTE: In the presence of a pre-existing (or rate related) bundle branch block,SVT may produce a wide QRS complex (>0.12 seconds) tachycardia which maybe difficult to differentiate from ventricular tachycardia. If the QRS complex iswider than 0.14 seconds, ventricular tachycardia is more likely than PSVT.
Verapamil must never be given to a patient with an undiagnosed wide-complex tachycardia. In such circumstances, either use adenosine, asabove, or treat as sustained ventricular tachycardia.
CONVERSION TO SINUS RHYTHM1. Manoeuvres that enhance vagal tone.
a. Carotid sinus massage (firm pressure; slow circular motions; alternatesides; one side at a time; exercise care in the elderly and avoid if carotidbruit; more effective if lying flat; may reveal atrial flutter by temporarilyslowing rate, even if doesn’t revert),
b. Valsalva manoeuvre or stimulation of nasopharyngeal afferents with ice-cold water.
2. Arrange transport to a hospital with cardiac monitoring facility.
3. Pharmacologic conversion. If the above is ineffective. Use, only undercontinuous ECG monitoring:
a. Adenosine 6 mg bolus IV, over 5 to 10 seconds, if unsuccessful thenfollowed 2 minutes later by a second bolus of 12 mg. If ineffective butwell tolerated a further dose of 18 mg may be given
OR
b. Verapamil 1 mg/minute IV, up to 15 mg with careful blood pressuremonitoring
NB: Verapamil is generally safe in patients with supraventricular arrhythmias, themain concern being its ability to produce profound depression of contractilityand/or heart rate in occasional patients, particularly those who have pre-existentmyocardial disease. The danger of such an adverse response is alsoconsiderably greater in patients taking beta blockers prior to the administrationof verapamil.
22 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

Adenosine may be associated with transient hypotension and/or chest pain.
4. Repeat 1+2 if PSVT persists, vagal manoeuvres may be repeated,followed, if necessary, by further adenosine or verapamil.
5. Direct current cardioversion or overdrive pacing may be required. If PSVTpersists.
PROPHYLAXIS1. Occasional episodes of PSVT generally do not require prophylaxis.
2. Frequent episodes should prompt consideration of electrophysiologicalstudy and radiofrequency ablation therapy.
3. Prophylaxis. Give:
a atenolol 25 to 100 mg orally, daily OR
b metoprolol 25 to 100 mg orally, twice daily OR
c sotalol 80 to 160 mg orally, twice daily OR
d flecainide 100 to 200 mg orally, twice daily OR
e verapamil sustained-release 160 to 480 mg orally, daily.
f. If the above agents fail, and in patients debilitated by recurrentsymptoms, use amiodarone 200 to 400 mg orally, 3 times daily for 2weeks as a loading dose, followed by 100 to 400 mg orally, daily
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 23

VENTRICULAR TACHYCARDIATreat only if:
a prolonged episodes
b with haemodynamic compromise, or
c if significant symptoms are present.
NB: Sustained ventricular tachycardia may initiate cardiac arrest = immediateintervention is essential.= need urgent ambulance transportation to anemergency department.
1. Arrange urgent transport immediately to a facility with cardiac monitoringfacility.
2. In patients who are haemodynamically stable, use
a. lignocaine 1 to 1.5 mg/kg (usually 75 to 100 mg) IV, over 1 to 2 minutesfollowed, if successful, by 4 mg/minute for a maximum of 1 hour, then 1to 3 mg/minute by IV infusion
OR
b. amiodarone 5 mg/kg IV, via a central line over 20 minutes to 2 hours,then 10 to 15 mg/kg over 24 hours
OR
c. sotalol 1 to 2 mg/kg IV, over 10 to 30 minutes, repeat if necessary at 10minute intervals, and if indicated 80 to 160 mg by IV infusion over 12hours.
3. Direct current cardioversion.
Cardioversion should be considered at an early stage if:
a. acute drug therapy is unsuccessful or
b. there is haemodynamic impairment
4. Correct any underlying causes such as ischaemia or electrolytedisturbances, eg hypokalaemia
5. ICD. Several large trials comparing antiarrhythmic drug regimens with ICDhave now suggested that in many patients with recurrent ventriculartachycardia, an ICD may well be the most effective therapeutic option.Unless this possibility is ruled out, eg by extreme old age or coexistentmalignant disease, early referral for cardiac electrophysiological opinionshould be considered.
6. Maintenance. If a decision is taken to continue with long-term oral drugtreatment to maintain SR then the choice of drug may be either empirical ormay be decided after electrophysiological study.
24 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

a In patients with significant left ventricular dysfunction, use
• amiodarone† 200 to 400 mg orally, 3 tds for 2 weeks, followed by 200mg orally, on alternate days OR
• sotalol 80 to 160 mg orally, twice daily
OR
atenolol 25 to 100 mg orally, daily
OR
metoprolol 25 to 100 mg orally, twice daily OR
b Patients with otherwise normal hearts may also be treated withflecainide 100 to 200 mg orally, twice daily
† While there is increasing evidence for greater efficacy for sotalol thanlignocaine in this situation, an initial trial of IV lignocaine has the advantagethat, if successful, there is little toxicity likely, and if unsuccessful, anyunwanted effects of the drug will wear off rapidly and allow the treatingphysician to move on to alternative therapies with minimal risk of additiveadverse effects from multiple antiarrhythmic agents. Sinus rhythm may bemaintained by continuing the successful drug. Breakthrough episodes requireincreased dosage or an empirical change to an alternative drug, orconsideration of insertion of an implantable cardioverter-defibrillator (ICD)
† Criteria for determining the maintenance dosage of amiodarone arecontroversial. The lowest dose providing symptomatic relief may not prevent apotentially fatal episode. Plasma levels of amiodarone and its activemetabolite may be of limited value in guiding dosage or for determiningcompliance.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 25

TORSADES DE POINTESDefinition. A form of polymorphic ventricular tachycardia in which the QRSaxis is constantly shifting, often in patients with a prolonged QTc (>450msec). It may occur spontaneously or during therapy with various drugs orcombinations thereof, eg amiodarone, tricyclic antidepressants,phenothiazines, disopyramide, erythromycin, pentamidine, quinidine,sotalol, ketoconazole, and cisapride. For an up-to-date listing seewww.torsades.org/. Torsades is frequently self-limiting and uncommonlyfatal but can cause haemodynamic collapse or lead to cardiac arrest anddeath.
1. Any drug suspected of causing the arrhythmia should be ceasedimmediately.
2. Serum potassium should be checked urgently and IV potassium chlorideadministered to attain and maintain a level of 5 to 5.5 mmol/L.
3. If there is an underlying bradycardia (PR<60) administer atropine 0.5 to1.5 mg IV, repeat after 15 minutes if necessary
4. The following have been reported to be successful in terminating thecondition:
a temporary transvenous pacing, where easily available, is probably thetreatment of first choice; pace at a rate of 90 to 100 per minute OR
b magnesium sulfate 50% 4 mL (2 g) IV, over 10 to 15 minutes followed, ifindicated, by 1 to 1.5 mL (0.5 to 0.75 g) per hour by IV infusion, for 12 to24 hours OR
c isoprenaline 20 micrograms IV, repeat according to clinical response,followed by an infusion at 1 to 4 micrograms/minute (occasionally higherdoses may be required) OR
d lignocaine 75 to 100 mg IV, over 1 to 2 minutes followed, if successful,by 4 mg/minute for a maximum of 1 hour and then 1 to 3 mg/minute byIV infusion
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
26 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

CARDIOVERSION1. Explain procedure and obtain informed consent (if clinical situation permits).
2. Monitor. Obtain IV access, ECG monitor, pulse oximetry. Ensure facilities forresuscitation.
3. Exclude contraindications: Digoxin toxicity, heart block.
4. Ensure patient is fasting for >6hours. If not fasting and clinical situationnecessitates urgent cardioversion, intubate to protect airway.
5. Sedate with midazolam 2.5-5mg IV slowly (1-2mg increments). Monitor withpulse oximetry.
6. Synchronise defibrillator. Synchronised setting must be selected ondefibrillator panel.
7. Ensure patient is not in contact with any other person or metal object.
8. Initial energies:
a. Atrial flutter 50 joules
b. Supraventricular tachycardia 50 joules
c. Ventricular tachycardia 50-100 joules
d. Atrial fibrillation 100 joules
NB: If no response wait 2-3 minutes. Attempts at cardioversion during thisperiod may be unsuccessful. Then increase energies incrementally to maximumof 360joules.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 27

SINUS BRADYCARDIA1. Treat only if symptomatic. Symptoms are uncommon at rates above 40 to
45 beats per minute.
2. Exclude reversible causes viz hypothyroidism and panhypopituitarism.
3. If acute treatment is required, use atropine 0.5 to 1.5 mg IV, repeat after15 minutes if necessary.
4. Stop drugs which may cause or exacerbate (eg beta blockers, digoxin,sotalol, amiodarone, verapamil, diltiazem).
5. Chronic sinus bradycardia may be a feature of the sick sinus syndrome.Treat with sinoatrial or atrioventricular block or atrial tachyarrhythmia.
6. Pacing may be required if the bradycardia is symptomatic, or if intermittenttachyarrhythmia requires drug treatment which might exacerbate theunderlying bradycardia.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
ATRIOVENTRICULARJUNCTIONAL RHYTHMDefinition: Atrioventricular junctional rhythm (<60 beats per minute) isusually an escape rhythm when the sinus node is suppressed by drugs, byincreased vagal tone or when there is atrioventricular nodal block. Thisrhythm rarely requires treatment.
1. If hypotension occurs, give atropine 0.5 to 1.5 mg IV, repeat after 15minutes if necessary.
2. If atropine fails, use isoprenaline 20 micrograms IV, repeat according toclinical response, followed by an infusion at 1 to 4 micrograms/minute.Occasionally higher doses required especially in patients who have beentaking beta blockers
3. If an isoprenaline infusion is required for more than 30 to 60 minutes, and asfirst choice in acute MI, use temporary transvenous pacing.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
28 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

INCOMPLETE ATRIOVENTRICULAR BLOCK Indications
Relative indications for treatment include:
1. symptoms such as syncope
2. occurring in the context of an acute MI.
Management
1. Discontinue drugs which may cause AV block (such as digoxin, diltiazem,verapamil or beta blockers)
2. Further treatment depends upon the level in the conducting system at whichthe block is occurring:
a. First-degree atrioventricular block (prolonged PR interval) – requires notreatment.
b. Second-degree heart block may be due to either:
i. Wenckebach block (usually in the atrioventricular node) rarely requirestreatment
ii. Mobitz type 2 block (usually in the more distal conducting tissue)rarely requires treatment
• In chronic cases permanent pacing is recommended for distal block(Mobitz type 2) because of frequent early progression to third-degreeatrioventricular block.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 29

COMPLETE HEART BLOCK1. If acute and located in the atrioventricular node (i.e. normal qrs
complex) – treat conservatively. In this case the junctional escape rhythmhas a rate of 50 to 60 beats per minute. Temporary pacing may be requiredfor slow escape rates originating from a focus at any level if haemodynamicdeterioration occurs.
2. If complicating AMI. Treat with urgent angioplasty i.e. concentrate onurgently reopening the culprit coronary artery (if available, or thrombolysis).
3. If occurring as wide QRS escape rhythm. Treat with urgent externaltranscutaneous pacing. Such a rhythm is often unstable and ventricularstandstill may supervene. Many emergency departments now have facilitiesfor and this can be very useful as a temporising measure while transvenouspacing is being organised.
4. If extreme bradycardia or hypotension
a. Urgent external transcutaneous pacing If temporary pacing facilities are not immediately available, treat with:
b. IV isoprenaline 20 micrograms IV, repeat according to clinical response,followed by an infusion at 1 to 4 micrograms/minute,
5. Chronic complete heart block nearly always involves the distal conductingsystem and permanent pacing is usually indicated.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
30 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

ACUTE PULMONARY OEDEMA
IMMEDIATE PREHOSPITAL TREATMENT1. Sit patient up.
2. Oxygen 100% via non-rebreather
3. Frusemide 40mg IV or twice normal oral dose. Avoid if BP<100 mm Hg
4. Morphine 2mg increments IV titrate to response or maximum of 10mg IV (+Maxalon 10mg IV q8h) Avoid if BP < 100.
5. Nitrates:
a. Glyceryl trinitrate sublingual. Ensure cannula inserted before as maycause hypotension. Give 1/2-1 SL Repeat 5-15mins PRN providingBP>100 mm Hg or
b. Glyceryl trinitrate paste 2.5-5cm or
c. Glyceryl trinitrate patch 25 or 50mg. Providing BP>100 mm Hg.Remove and wipe skin if BP falls <100mmHg. Remove after 18 hours,reapply after 6 hours.
HOSPITAL TREATMENTIn addition to above, and if pulmonary oedema is severe, not responding,or associated with ischaemia or significant hypertension, add
1. Isosorbide dinitrate 5 to 20 mg sublingually, repeat after 30 minutes ifnecessary
or
Glyceryl trinitrate (Tridil) Infusion: 50mg (1amp) in 500mls 5%D. Start at5ug/min (3mls/hour) and titrate to pain and to keep BP>100 mmHg.
2. CPAP at 10cm airway pressure. May need to be started early if treatedbefore arrival. If no response after 15mins increase to 15cm
3. If confined to bed – anticoagulation. When confined to bed all patientsshould receive:
d. unfractionated heparin 5000 units SC, 8- to 12-hourly OR
e. enoxaparin 40 mg (or 20 mg for low body weight) SC, OR
f. dalteparin 5000 international units (or 2500 international units for lowbody weight) SC, daily unless other risk factors, eg AF, dictate fullanticoagulation
www.gpkit.com.au 31

If pulmonary oedema remains severe and not responding, add:
4. Dopamine Must be given via central line Infusion:: 200mg (1amp) in 100mls5%D (2mg/ml). Start at:2.5ug/kg/min (approx 5mls/hr for 70kg man) – renaldose 5 ug/kg/min (approx 10ml/hr for 70kg man) – ionotropic dose Increaseat increments of 5 ug/kg/min (approx 10ml/hr for 70kg man) to max20ug/kg/min (approx 40mls/hr for 70kg man).
If pulmonary oedema is severe and not responding to diuretics andvasodilator, consider adding
5. Dobutamine May be given via peripheral line. Infusion:: 250mg (1amp) in100mls 5%D (2.5mg/ml). Start at 5 ug/kg/min (approx 8ml/hr for 70kg man)Increase at increments of 5 ug/kg/min (approx 8mls/hr for 70kg man) to max40ug/kg/min (approx 80mls/hr for 70kg man).
OR
6. Milrinone 50 micrograms/kg IV, slowly over 10 minutes, followed by 0.375to 0.75 micrograms/kg/minute IV, adjust according to clinical andhaemodynamic response, up to a maximum of 1.13 mg/kg daily.
PULMONARY OEDEMA IN SPECIFIC CIRCUMSTANCES:
Pulmonary oedema + atrial fibrillation with rapid ventricular rate give
Digoxin 0.5mg IV in 20ml 5% Dextrose over 10-30 minutes Repeat after 6hr.Avoid if received any digoxin in the last 2/52. digoxin. The following daydigoxin 62.5 to 500 micrograms orally, daily, according to age, plasmacreatinine and plasma digoxin level.
Pulmonary oedema + hypotension (BP persistently<100 mm Hg).
Dopamine Must be given via central line Infusion:: 200mg (1amp) in 100mls5%D (2mg/ml). Start at:2.5ug/kg/min (approx 5mls/hr for 70kg man) – renaldose 5 ug/kg/min (approx 10ml/hr for 70kg man) – ionotropic dose Increase atincrements of 5 ug/kg/min (approx 10ml/hr for 70kg man) to max 20ug/kg/min(approx 40mls/hr for 70kg man).
OR
Dobutamine May be given via peripheral line. Infusion:: 250mg (1amp) in100mls 5%D (2.5mg/ml). Start at 5 ug/kg/min (approx 8ml/hr for 70kg man)Increase at increments of 5 ug/kg/min (approx 8mls/hr for 70kg man) to max40ug/kg/min (approx 80mls/hr for 70kg man).
When BP restored, give Lasix as above
Pulmonary oedema + hypertension (BP persistently>160 mm Hg).
Glyceryl trinitrate (as above) increase to maintain SBP >100 – 150 mm Hg.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
32 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

ARRHYTHMIAS IN HEARTFAILUREIntroduction
1. Arrhythmias may rarely CAUSE heart failure if they persist for weeks tomonths eg supraventricular tachycardia. Control of the arrhythmia thencompletely reverses heart failure.
2. Arrhythmias may CONTRIBUTE to heart failure. Eg complete heart block,or tachyarrhythmias, (AF or atrial flutter with rapid ventricular response).Treatment of heart failure must then include appropriate treatment of thearrhythmia. Often it is not possible to determine how much the heart failurewas due to the arrhythmia and how much to the underlying heart diseaseuntil the arrhythmia has been controlled for some time.
3. Arrhythmias frequently ARISE from heart failure. The more severe theunderlying heart disease and the heart failure, the more severe and frequentthe arrhythmias.
a. Atrial tachyarrhythmias AF and, to a lesser extent, atrial flutter, arecommon in heart failure. They usually reflect atrial enlargement and are aconsequence of the proarrhythmic effect of atrial stretch. In patients withsubstantial atrial enlargement, maintenance of SR following reversion isunlikely in the longer term. This limits the therapeutic options toventricular rate control combined with judicious use of antithrombotictherapy, see Arrhythmias.
b. Ventricular tachyarrhythmia. Consider an implantable cardioverter-defibrillator in patients with life-threatening ventricular arrhythmias, seeSustained ventricular tachycardia.
Principles of antiarrhythmic therapy
The principles underlying the approach to the treatment and prevention ofarrhythmias in heart failure are listed below.
• Avoid potassium depletion from diuretic therapy. Maintain serum potassiumabove 4 mmol/L, preferably closer to 5 mmol/L. Use potassium-sparingdiuretics freely, while remembering their potential to cause hyperkalaemia anddehydration.
• Avoid magnesium depletion from diuretic therapy.
• Advise patients to follow a prudent diet including at least two fish meals perweek.
• Use ACEI in all patients and in maximum tolerated dose, given their proveneffect in reducing arrhythmias and sudden death.
www.gpkit.com.au 33

• Use beta blockers given their proven effect in reducing arrhythmias andsudden death. Where possible, use standard beta blockers instead of sotalolbecause of the small but definite risk of proarrhythmia with sotalol.
• If sotalol or amiodarone are used, use the minimum effective dose, obtainobjective evidence of antiarrhythmic efficacy and monitor for possibleproarrhythmia.
• Avoid using long-term cardiac stimulants such as beta agonists and cardiacphosphodiesterase inhibitors because of their proven proarrhythmic actions.
• Avoid using class I antiarrhythmic agents such as quinidine, mexilitene andflecainide because of their high proarrhythmic potential.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
ACUTE LIMB ISCHEMIADefinition: sudden onset of severe ischaemia with associated sensory andmotor loss and intense pain. Causes include thrombosis, thromboembolismfrom heart, aneurysm or atheroma, or thrombotic occlusion of ananeurysm. Such a source should always be sought.
IMMEDIATE PREHOSPITAL TREATMENT1. Arrange urgent transport immediately to a facility with angiography and
vascular surgery.
2. Protect limb using a cage and a heel pad, but do not elevate.
3. Analgesia: Morphine 5-10 mg IMI or IV.
INITIAL HOSPITAL TREATMENT1. Anticoagulation with unfractionated heparin should be initiated
unfractionated heparin 5000 units loading dose IV, followed by 1250units/hour by IV infusion, then adjust according to APTT.
2. Thrombolysis is appropriate. Use
a. streptokinase 2500 to 5000 international units/hour by intra-arterialinfusion, with the catheter tip at the occlusion until patency is restored
OR
34 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

b. alteplase 1 to 1.5 mg/hour by intra-arterial infusion, with the catheter tipat the occlusion until patency is restored OR urokinase 50 000 to 100000 international units/hour by intra-arterial infusion, with the catheter tipat the occlusion until patency is restored.
NB: different regimens and techniques are used and expert advice shouldbe sought
2. Warfarin maintaining an international normalised ratio (INR) of 2 to 3.Duration: 3 to 6 months (if due to embolism), long-term if embolism is froma cardiac source
3. Antiplatelet therapy. Commence aspirin if acute ischaemia is due to in situthrombosis or atherosclerosis.
REFERENCESConsensus guidelines for warfarin therapy. Recommendations from the Australasian Society ofThrombosis and Haemostasis. Alex S Gallus, Ross I Baker, Beng H Chong, Paul A Ockelford andAlison M Streeton behalf of the Australasian Society of Thrombosis and Haemostasis.MJA 2000; 172: 600-605Therapeutic guidelines: Cardiovascular. Version 4, 2003.
TEMPORAL ARTERITISDefinition: Temporal arteritis is characterised by inflammation of mediumsize arteries, with the risk of vessel stenosis and occlusion. It occurs inpeople > 50 years causing pain and tenderness over the superficialtemporal arteries with or without polymyalgia rheumatica. Irreversibleblindness is an uncommon but devastating complication. A markedelevation of ESR is almost universal.
1. Prednisolone 1 mg/kg orally daily should be commenced immediately inpatients presenting with typical clinical findings and should not be delayedpending the results of inflammatory markers.
2. Arrange early referral to a rheumatologist to oversee prednisolone therapyand for consideration of the introduction of steroid-sparing agents inselected cases.
REFERENCESTherapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 35

DEEP VEIN THROMBOSISIntroduction
1. The aim of deep vein thrombosis (DVT) treatment is to avoid complicationsof pulmonary embolism (PE) and post-thrombotic syndrome. Post-thrombotic syndrome is characterised by recurrent pain, swelling, andincreased risk of leg ulceration occurring for months or years following theprimary event, and may be confused with recurrent DVT.
2. Risk of pulmonary embolism from deep vein thrombosis (DVT) is dependenton the location of the DVT, and this determines treatment protocols (seeTable below).
3. DVT is confirmed by duplex ultrasound scanning and PE is confirmed byhelical CT or isotope lung scan.
4. Anticoagulation is highly effective in preventing PE .
5. Graduated compression stockings reduce the incidence and severity of thepost-thrombotic syndrome. Anticoagulation does little to prevent the post-thrombotic syndrome.
Treatment of deep vein thrombosis
NB: If duplex USS is not available, and clinical suspicion is high, LMWH may bestarted empirically on outpatient basis, pending USS,then discontinued if USS isnormal
36 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
Iliofemoral DVT 50% risk ofpulmonaryembolism
Anticoagulation Consider…Thrombolysis PLUSCompression stockings
Femoropopliteal DVT 25% risk ofpulmonaryembolism
Anticoagulation PLUSCompression stockings
Isolated calf DVT 5-10% risk ofpulmonaryembolism
Anticoagulation ORUltrasound surveillanceprogram PLUSCompression stockings

MANAGEMENT1. Anticoagulation
Low molecular weight heparin (LMWH) LMWH has been shown to be atleast as effective and as safe as an IV unfractionated heparin infusion in theinitial management of deep vein thrombosis and allows treatment on anoutpatient basis. Collect blood for activated partial thromboplastin time(APTT), international normalised ratio (INR) and platelet count. Give:
a. Enoxaparin (clexane) 1.5 mg/kg SC, daily (maximum dose 150 mg daily)
OR
b. dalteparin 100 international units/kg SC, twice daily (maximum dose10,000 international units twice daily)
OR
c. Enoxaparin (clexane) 1 mg/kg SC, twice daily (maximum dose 100 mgtwice daily).
Oral anticoagulation may be commenced on the same day as LMWH.Warfarin should not be commenced alone (i.e. without LMWH) as this isassociated with a high rate of subsequent DVT recurrence. Give warfarin 5mg orally, daily for 2 days. This initial dose of warfarin should be reduced inthe elderly.
Monitoring. LMWH should be given for a minimum of 5 days and until theINR has been above 2.0 on two consecutive days. The INR should bemonitored daily and the dose adjusted according to INR until a therapeuticlevel is achieved.
2. Thrombolysis. Possible indications: ongoing hypotension, right heart failureor severe hypoxaemia, and no contraindications. Give:
a. alteplase 10 mg bolus IV, followed by 90 mg by IV infusion over 2 hours(in patients below 65 kg in weight, the total dose should not exceed 1.5mg/kg)
OR
b. streptokinase 250 000 international units IV, over 30 minutes, followedby 100 000 international units/hour by IV infusion for 24 to 48 hours. NBStreptokinase therapy may cause anaphylactic reactions and should notbe given to patients who have previously had streptokinase therapy,because of the likely presence of neutralising antibodies.
REFERENCESConsensus guidelines for warfarin therapy. Recommendations from the Australasian Society ofThrombosis and Haemostasis. Alex S Gallus, Ross I Baker, Beng H Chong, Paul A Ockelford andAlison M Streeton behalf of the Australasian Society of Thrombosis and Haemostasis.MJA 2000; 172: 600-605Therapeutic guidelines: Cardiovascular. Version 4, 2003.
www.gpkit.com.au 37
PULMONARY EMBOLISM A clinical syndrome of dyspnoea, chest pain, cough, tachypnoea,tachycardia, and hypoxia (low Sa02, low Pa02) typically in association with:
• a normal or near normal chest examination
• a normal or near normal CXR
specific clinical contexts (immobility, post surgery, postpartum) or riskfactors (obesity, cigarette smoking, age>50) in >90% cases.
PE is common, underdiagnosed and potentially fatal. Diagnosis, by V/Q orhelical CT scan is dependent on consideration of the diagnosis and mainte-nance of a high index of suspicion. Treatment reduces mortality to < 10%.
MANAGEMENT1. Oxygen
2. Analgesia
3. Anticoagulation
If no evidence of hemodynamic compromise give low molecular weight heparin (LMWH) Give:
a. Enoxaparin (clexane) 1.5 mg/kg SC, daily (maximum dose 150 mg daily)
OR
b. Dalteparin 100 international units/kg SC, twice daily (maximum dose 10000 international units twice daily)
OR
c. Enoxaparin (clexane) 1 mg/kg SC, twice daily (maximum dose 100 mgtwice daily).
4. If evidence of hemodynamic compromise:
i. Anticoagulation with unfractionated heparin (UFH) 5000 units IV, as aloading dose, followed by 1250 units/hour by IV infusion. The APTTshould be checked after 4 to 6 hours and the dose adjusted if not in thetherapeutic range. If in the therapeutic range, the dose should bereviewed daily.
ii. Consider thrombolysis. Possible indications: ongoing hypotension, rightheart failure or severe hypoxaemia, and no contraindications. Give: alteplase 10 mg bolus IV, followed by 90 mg by IV infusion over 2hours (in patients below 65 kg in weight, the total dose should notexceed 1.5 mg/kg) OR streptokinase 250 000 international units IV, over30 minutes, followed by 100 000 international units/hour by IV infusionfor 24 to 48 hours.
38 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

NB: Streptokinase therapy may cause anaphylactic reactions and shouldnot be given to patients who have previously had streptokinase therapy,because of the likely presence of neutralising antibodies.
iii. Consider surgical thrombectomy. Possible indications: ongoinghypotension, right heart failure or severe hypoxaemia, and nocontraindications.
iv. Oral anticoagulation may be commenced on the same day as LMWH.Warfarin should not be commenced alone (i.e. without LMWH) as this isassociated with a high rate of subsequent DVT recurrence. Give warfarin5 mg orally, daily for 2 days. This initial dose of warfarin should bereduced in the elderly.
REFERENCESConsensus guidelines for warfarin therapy. Recommendations from the Australasian Society ofThrombosis and Haemostasis. Alex S Gallus, Ross I Baker, Beng H Chong, Paul A Ockelford andAlison M Street on behalf of the Australasian Society of Thrombosis and Haemostasis.MJA 2000;172: 600-605 Therapeutic guidelines: Cardiovascular. Version 4, 2003.
SHOCKA clinical syndrome characterised by hypotension and inadequate tissueperfusion (ie falling urine output, impaired consciousness, cold extremities),due, usually, to uncontrolled haemorrhage, sepsis or anaphlaxis.
MANAGEMENT1. Establish IV access with x2 large bore cannulas.
2. Infuse Gelofusine at 10-20 mls/kg.
3. If cause is not immediately apparent, perform rapid, full body survey toestablish underlying cause:
a. Blood loss (hypotension, cold extremities, pallor)
b. Sepsis (hypotension, warm extremities, fever)
c. Anaphylaxis (hypotension, uricaria, wheeze, stridor)
If no specific features are present, consider other causes: coronary syndromes, massive pulmonary embolism, tension pneumothorax.
4. If evidence of sepsis, take blood cultures x2 and commence:
Benzylpenicillin 1200 mg IV
PLUS.
Ceftriaxone 50 mg/kg up to 2 g IV..
5. If evidence of anaphyaxis treat as for Anaphlaxis.
www.gpkit.com.au 39

40 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
ACUTE ASTHMA1. Assess severity of the attack.
Admission criteria:
Patient should generally be referred to hospital if:
• Nebulised bronchodilators fail to relieve wheeze/SOB for >4 hours.
• Initial PEFR is < than 50% best/ideal reading.
NB: Many other factors will reduce admission threshold: previoussevere/precipitate attack, doubtful compliance, poor previous response etc.etc.
Clinical features Mild Moderate Severe
Physicalexhaustion
No No Yes
Talks in Sentences Phrases Words
Pulse rate [NB1] <100/minute 100–120/minute >120/minute
PEF (% predicted)
>75% 50%–75% <50%
FEV1 (% predicted)
>75% 50%–75% <50%
Oximetry onroom air
>95% 92%–95% <92%
Arterial bloodgases
Not needed Perform if initialtreatment responseis poor (if PaCO2>40 mm Hg treatas severe attack)
PaCO2 >42 mm Hg;elevated or high-normal PaCO2indicates ventilatoryinsufficiency requiringclose monitoring andpossibly ventilatorysupport
Hospitaladmissionneeded?
No Probably Yes, consider ICU

Assessment of acute asthma in children
Admission criteria:
Patient should generally be referred to hospital if:
• Nebulised bronchodilators fail to relieve wheeze/SOB for >4 hours.
• Initial PEFR is < than 50% best/ideal reading.
NB: Many other factors will reduce admission threshold: previoussevere/precipitate attack, doubtful compliance, poor previous response etc.etc.
MANAGEMENT OF ACUTE ASTHMA Management of acute asthma is the same in adults and children.
1. Oxygen at least 8L/min to maintain PO2>94%.
2. Bronchodilators via SPACER*
Salbutamol .100 micrograms MDI, 4–12 inhalations via a spacer**
PLUS (optional)
Ipratropium bromide 20 micrograms MDI, 4–8 inhalations (via a large-volume spacer)**
Reassess immediately if no or poor response, repeat salbutamol immediatelyor after 20,30,60 or 120 minute intervals. In severe asthma salbutamolshould be given continuously until control is achieved. Ipratropium shouldbe repeated q2-4h.
*NB Giving bronchodilators via nebulisers offers no advantage overspacers in either children or adults.
If a nebuliser is used it should be driver by O2 at 8 liters/min if available.
Give salbutamol 1ml (5mg) nebuliser solution+2mls NS (or one 5mg nebule)via nebuliser**
www.gpkit.com.au 41
Clinical features Mild Moderate Severe
Altered consciousness No No Yes
Use accessory muscles No Some Marked
Talks in Sentences Phrases Words
Pulse rate >60 40-60 <40
PEF (% predicted) >75% 50%–75% <50%
FEV1 (% predicted) >60 40-60 <40
SaO2 on room air >94% 90-94 <90
Hospital admission needed? No Probably Yes
42 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
PLUS (optional)
Ipratropium bromide 2mls (500 ug) nebuliser solution (or X1 500 ugnebule) via nebuliser.
3. Hydrocortisone 100-250mg Children: 5mg/kg (max 100mg), Repeat q6hthereafter.
OR
Prednisone 50-75mg. Children 1 mg/kg. PO. Repeat daily.
If response to 1-3 above is inadequate give the following:
4. Salbutamol IV 300ug over 5minutes, then as infusion (See IV Drug Infusions)Requires close monitoring in hospital setting.
If response to 1-4 above is poor consider:
5. Magnesium sulfate 1.2–2 g IV Children 25–100 mg/kg IV over 20 minutes.
6. Continuous Positive Airways Pressure (CPAP) if hypoxic (eg Sa02<90mmHg, Pa02<55 mmHg) and exhausted. Start at 10cm airway pressure. If noresponse after 15mins increase to 15cm. Arrange CXR prior to CPAP to ruleout pneumothorax.
7. If hypoxic (exhausted, shallow respiration, Pa02<50 mmHg, bradycardia)give:
Adrenaline 0.3-0.5mg (0.3-0.5 ml of 1:1000 solution) IV over 1 minute.
OR (if no IV access)
Adrenaline 0.3-0.5mg (0.3-0.5 ml of 1:1000 solution) SC subcutaneouslyor via endotracheal tube for imminent cardiorespiratory arrest (exhausted,shallow respiration, Pa02<50 mmHg, bradycardia).
REFERENCES1. Therapeutic guidelines: Respiratory. Version 3., 2003.2. National asthma council. Asthma management handbook 2002.
CROUPPoor prognostic indicators:
• Presentation early in the illness (within 24 hours of onset) ie likely to progressover 1-2 days.
• Younger child (smaller airway, greater obstruction).
• Known structural airway abnormality [eg subglottic stenosis]
• Past severe attack

Admission criteria:
• Persistent stridor at rest.
• Other indications include:
age less than 1 year
symptoms progressed despite systemic corticosteroids
doubtful parental compliance etc.etc.
NB: Upper airway obstruction is made worse by changes in position andemotional distress. The child should be seated upright on its mothers lapwith mother holding O2 mask away from face. Procedures causing distressshould be avoided eg IMI injections.
MILD CROUP (90% of cases) = barking 'croupy' cough alone
1. Paracetamol
2. Corticosteroids. Good evidence now exists for a single dose of oralprednisone 1mg/kg in most, if not all, cases of mild croup, as a means ofpreventing the progression to moderate or severe croup.
3. Advice to parents. Parents should be advised if cough progresses tostridor they should present directly to hospital.
NB. Steam inhalation. There is anecdotal information but no clear evidenceof the efficacy of steam inhalation (administered with child seated on parentslap in steamy bathroom). Boiling water should never be used for steaminhalation.
Moderate croup (<5% of cases) = persistent inspiratory stridor at rest.
NB This is an indication for hospital admission:
While awaiting hospital transfer, give:
1. Oxygen
2. Corticosteroids: Oral: prednisone 1mg/kg or dexamethasone at 0.15 to0.6 mg/kg. both once daily for 1 to 2 days.
OR
Nebulised budesonide (2mg b.d). Consider only if oral steroids notavailable or for children who have vomited after oral steroids.
SEVERE CROUP (<1% of all cases) = biphasic stridor at rest + chest wallretractions
PLUS, while waiting for hospital transfer, give the following:
Nebulised adrenaline (1:1000 concentration at a dose of 0.5 ml/kg of bodyweight to a maximum dose of 4-5 ml delivered neat in the nebuliser bowl)
REFERENCESTherapeutic guidelines: Respiratory. Version 3., 2003.
www.gpkit.com.au 43

44 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
COMPLETE UPPER AIRWAYOBSTRUCTION Definition: Signs of advancing upper airway obstruction (biphasic stridor)and hypoxia (agitation -> bradycardia, obtunded, cyanotic etc)
1. The invasive procedure described below should only be considered when allother attempts to relieve airway obstruction have failed and patient isshowing signs of severe advancing hypoxia.
2. In patients with impaired consciousness attempts should first be made torelieve obstruction by head tilt, jaw thrust, followed by gentle positivepressure ventilation with bag and mask. If this is not rapidly effective, moveto cricothyroidotomy.
EMERGENCY NEEDLE CRICOTHYROIDOTOMYIndication: Children < 10 years with complete upper airway obstructionwhich fails to respond to alternate measures.
a. Position patient as above: neck extended.
b. Identify landmarks: The cricothyroid membrane is identified between thelower border of the thyroid cartilage and the upper border of the cricoidcartilage.

c. Prep skin and infiltrate with Xylocaine 1% (If clinical situation permits).
d. Insert 12-14 gauge cannula through the cricothyroid membrane, angledat 90˚ to skin. When needle is placed in trachea, rotate cannula so that itis angled at approximately 45˚ and directed towards the lungs.
e. Once placement is complete, remove needle, leaving plastic cannula insitu.
www.gpkit.com.au 45
Mandible
Thyroid Cartilage
Cricoid Cartilage
CricothyroidMembrane
Trachea

f. A makeshift connection canbe fashioned between thecannula and Ambubag (seediagram below). Thecannula (1) is attached to a3 ml syringe (3). Theplunger of the 3 ml syringeis removed and attached toa bag-valve-mask device(Ambubag) via an 8 mmendotracheal connector.
3. Oxygen tubing on theAmbubag is connected to anoxygen source with a flow at10–15 L/min. Manual ventilationshould be at a rate of 1-secondcompression with 4-secondrelaxation (guided with chestrise).
4. If required, a 3 way stop cock or Y connector (2) can be placed between thecannula and syringe to facilitate the escape of air in between insufflations.Lateral compressions of the chest will facilitate the escape of air.
NOTE: Ventilating a patient with complete upper airway obstruction via aneedle cricothyroidotomy is a life saving but time limited procedure which willlead to hypercapnea and hypoxia after 30-45 minutes – after which intubationor a surgical tracheotomy will be required.
REFERENCESManagement of the Airway. The American College of Surgeons Committee on Trauma.September 2002. Chee-Fah C. Tzong-Luen W Hang C. Percutaneous transtracheal ventilation without a jetventilator The American Journal of Emergency Medicine Vol 28, 2003 507-508.
46 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

EMERGENCY INCISSIONAL CRICOTHYROIDOTOMYIndication: Children > 10 years and adults.
1-3 As ABOVE
4. Transverse incision 1 cm through cricothyroid membrane. NB some means ofmaintaining patency of incision will be necessary, and should be obtained inadvance eg 3-5 gauge endotracheal tube (depending on patient age) , orimprovise with cut tube of giving set, stethoscope, outer casing of ballpointpen etc. if nothing else available.
REFERENCESManagement of the Airway. The American College of Surgeons Committee on Trauma.September 2002.
www.gpkit.com.au 47

48 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
ACUTE EXACERBATION OFCOPDNB: Arrange CXR to rule out pneumothorax and to look for radiologicalevidence of pneumonia.
1. Controlled oxygen.
Indicated for hypoxia, with the aim of achieving achieving SaO2 88-92%,PaO2 55 mmHg. Note however, patients with COPD are typically chronicallyhypoxic, and tolerant of low PaO2. No further benefit is gained in trying toobtain SaO2 >92%
If patient is known to be a chronic CO2 retainer in the past, or if statusunknown give LOW DOSE oxygen via NASAL PRONGS at 0.5-2 L/min, or24% via VENTURI MASK.
Monitor with ABGs and increase to 28% then 35% at hourly intervals in orderto maintain Pa02>55%, providing PaCO2 does not increase >10mmHg witheach increment.
2. Bronchodilators
Beta2 agonists and ipratropium bromide work equally well, although somemay respond better to one type of medication than the other, so treatmentshould be tailored to individual response. The onset of effect of salbutamolis more rapid than that of ipratropium bromide.
Give via SPACER
salbutamol 100 micrograms MDI, up to 8 to 10 inhalations repeated asrequired
PLUS (optional)
ipratropium bromide 20 micrograms MDI, up to 4 to 6 inhalations repeatedas required
*NB Generally, nebulisers offer no advantage over MDI with spacers,although the evidence for this comes from studies in patients with asthma.Nebulisers may be indicated in very unwell patients in hospital, and if usedshould be driven by air at 8 liters/min.
Give salbutamol 1ml (5mg) nebuliser solution+2mls NS (or one 5mg nebule)via nebuliser, continuously or repeated as required.
PLUS (optional)
Ipratropium bromide 2mls (500 ug) nebuliser solution (or X1 500 ug nebule) via nebuliser.

3. Hydrocortisone 100-250mg or dexamethazone 4mg IV. Repeat q6hthereafter.
or
Prednisone 60mg PO. Repeat daily.
4. If evidence of infection (fever, purulent sputum, leukocytosis) give:
amoxicillin 500 mg orally, 8-hourly for 5 days
or
doxycycline 200 mg orally, as 1 dose on the first day, then 100mg orally,x1-2/day for a further 5 days.
or
cefriaxone 1g IV plus roxithromycin 300mg PO daily
5. If rising PCO2, increasing respiratory acidosis, or exhaustion startContinuous Positive Airways Pressure (CPAP) at 10cm airway pressure. Ifno response after 15mins increase to 15cm. Nebulised medications can begiven via the assisted ventilation circuit.
6. If respiratory arrest immanent (exhausted, shallow respiration, Pa02<50mmHg, bradycardia) give:
Adrenaline 0.3-0.5mg (0.3-0.5 ml of 1:1000 solution) IV over 1 minute.
or (if no IV access)
Adrenaline 0.3-0.5mg (0.3-0.5 ml of 1:1000 solution) SC
REFERENCES1.Australian and New Zealand Guidelines for the management of Chronic ObstructivePulmonary Disease 2003. MJA 2003 178(6 Suppl 17 Mar)2.Therapeutic guidelines: Respiratory. Version 3., 2003.
www.gpkit.com.au 49

PNEUMOTHORAX
EMERGENCY NEEDLE DECOMPRESSION of TENSIONPNEUMOTHORAXSigns of tension pneumothorax: absent breath sounds PLUS hypotension,syncope, tracheal shift, cyanosis etc
Identify landmarks: 2nd intercostal space, mid clavicular line, above
3rd rib (rather than below 2nd rib).
1. Prep skin and infiltrate with Xylocaine 1% (if patient conscious and clinicalsituation permits).
2. Insert12-14G cannula full length of needle to pleura. Remove metaltrochar/needle, leaving plastic cannula is situ. This should be followed byrush of air and sudden clinical improvement.
3. Leave plastic cannula open and in situ until formal intercostal drain can beinserted
SIMPLE (NON-TENSION) PNEUMOTHORAXIf SMALL (<2cm rim of air around lung i.e. < 50% collapse) and no shortness ofbreath OBSERVATION alone is usually all that is required.
If LARGE (>2cm rim of air around lung i.e. > 50% collapse) or shortness ofbreath SIMPLE ASPIRATION or INTERCOSTAL DRAIN.
50 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

SIMPLE ASPIRATION
1,2,3 – As above.
• Attach cannula to 3 way tap. Attach 3 way tap to large (50-100ml) syringeand Heimlich valve.
• Aspirate gently 60mls at a time; turn 3 way tap each time to expel airthrough Heimlich valve.
• Cease when resistance to aspiration is encountered, or when 2 litres havebeen aspirated
• Repeat CXR. If <20% observe. If >20% proceed to intercostal drain.
INTERCOSTAL DRAIN
NB: Indications: if simple aspiration fails, pre-existing lung disease, traumaticpneumothorax, tension pneumothorax.
1,2 – As above.
• Make 1.5cm transverse incision (along direction of rib). Incisesubcutaneous tissue to muscle.
• Use haemostat or finger to dissect through muscle. Should feel ‘pop’ andrush of air.
• Sweep finger inside cavity to check for adherent lung tissue.
• Insert chest tube posteriorly and superiorly, making sure all holes are insidecavity.
www.gpkit.com.au 51
• Double clamp tube (clamps at right angles to each other)
• Attach free end of tube to underwater drain. Remove clamps.
• Secure tube with purse string suture firmly tied around tube (circle tube x3,knots x3).
• Cut gauze to fit around tube. Cover with adhesive tape extending inairtight series of strips from skin onto tube.
• Tape tube to chest.
REFERENCESTherapeutic guidelines: Respiratory. Version 3., 2003.
COMMUNITY ACQUIREDPNEUMONIACAP is usually caused by a single organism, the most common beingStreptococcus pneumoniae. Other important causes include Mycoplasmapneumoniae, Chlamydophila pneumoniae and Legionella species.Haemophilus influenzae is responsible for less than 5% of cases of CAP andis seen predominantly in chronic obstructive pulmonary disease.
NB: Hospital admission is usually indicated but ultimately dependent onfactors such as age and presence of intercurrent medical problems.
1. Benzylpenicillin 1.2 g IV, 6-hourly OR amoxy/ampicillin 1 g IV, 6-hourly untilsignificant improvement THEN amoxicillin 1 g orally, 8-hourly ORamoxicillin 1 g orally, 8-hourly for a total of 7 days.
PLUS
Doxycycline 200 mg orally, for 1 dose, then 100 mg orally, daily for a further5 days OR roxithromycin 300 mg orally, daily for 7 days.
2. If Gram-negative bacilli are identified in the sputum or blood, gentamicinshould be added to the above regimen (see recommendations for risk classV).
3. If hypersensitive to penicillin ceftriaxone 1 g IV, daily OR cefotaxime 1 gIV, 8-hourly until significant improvement THEN cefuroxime 500 mg orally,12-hourly for a total of 7 days.
REFERENCESTherapeutic guidelines: Respiratory. Version 3., 2003.
52 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

HYPOGLYCEMIARECOGNITION
Symptoms of hypoglycemia are of two types:
1. adrenergic symptoms: palor, sweating, shaking, palpitations, anxiety
2. neuroglycopenic symptoms: impaired cognition, confusion, seizures, coma.
B blockers mask adrenergic symptoms leading to precipitous onset ofneuroglycopenic symptoms.
MANAGEMENT
Mild to moderate hypoglycaemia
If the patient is conscious and cooperative, give sugar-containing food (fruit juice,jelly beans, honey), followed by a long-acting carbohydrate (sandwich, dried fruit).
Severe hypoglycaemia
1. Adult: glucose 50% 20 to 30 mL IV given into large vein because risk ofsuperficial thrombophlebitis. Patients should wake within 4 to 5 minutes.ORChild: glucose 10% 2 to 5 mL/kg bolus IV, then 0.1 mL/kg/minute.(Glucose 10% is recommended in children as the excessive use of glucose50% carries the risk of deaths due to hyperosmolality.) .OR
2. Adult: glucagon 1 mg SC or IMORChild: glucagon 0.5 mg SC or IMFollowed by oral feeding as above when conscious. Patients should wakewithin approximately 6 minutes following glucagon administration.
Sulfonylurea-induced hypoglycaemia
Hypoglycaemia due to sulfonylurea overdose causes long lasting hypoglycemia:
1. Arrange urgent hospital admission.
2. Glucose 10% 2 to 5 mL/kg bolus IV, then 0.1 mL/kg/minute – oftenprolonged treatment is required
3. Frequent monitoring of blood glucose to exclude a recurrence ofhypoglycaemia.
4. Octreotide 50 micrograms SC, 8-hourly for up to 3 doses. Octreotide canreduce both the duration of intravenous therapy and the need for addedboluses of 50% glucose.
REFERENCESTherapeutic guidelines: Endocrinology, Version 3, 2004.
www.gpkit.com.au 53

DIABETIC KETOACIDOSISNB: Arrange urgent hospital admission. IV rehydration using normal salineshould be commenced prior to transfer.
1. Oxygen 6L/min
2. Fluid resuscitation.
Monitor BP, PR, UO
Give normal saline 1L stat, 1L over 1 hour, 1L over 2 hours, 1L over 4 hours,1L over 8 hours.
Give hypotonic saline initially if Na>150 or serum osmolality>320mOsm/kg
3. Potassium replacement.
Monitor K hourly.
Start replacement when K<5.
Give 20mmol (1.5g)/K/hr for first 6 hrs then 10mmol(0.75g)K/hr for next12hrs according to clinical response.
4. Insulin infusion
Monitor venous BSL hourly (ward capillary BSL readings may be inaccurate).
• Infusion: 20 units Actrapid in 20mls.
Start at 3 units(3mls)/hr. BSL should fall at approx. 5 mmol/L/hr.
If BSL not falling after 2 hours* increase infusion rate 1 unit per hour untilclinical response.
When BSL reaches approx 15 mmol/L:
i. halve insulin infusion rate (to approx. 0.5-2.0 units/hour) and
ii. start 5%Dextrose at 1L q6h
Continue insulin infusion and 5%D to maintain BSL at approx 10 mmol/l untilketosis is has resolved.
If sliding scale order is required, make an estimate based on clinicalresponse or give:
If BSL>22 mmol/L, give 4 units/hr
If BSL18-21 mmol/L, give 3 units/hour
If BSL 12-17 mmol/L, give 2 units/hour
If BSL 8-11 mmol/L, give 1 unit/hour with 5%D at 50-100mls/hr.
54 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
OR
Subcutaneous insulin
Monitor BSL q2h .
Give sliding scale as follows:
If BSL> 20 mmol/L, give 10units of Actrapid.
If BSL 10-20 mmol/L, give 5units of Actrapid.
If BSL> 10 mmol/L, give no Actrapid.
*NB If high doses (5-50 units/hr) required to cause drop in BSL, think ofinadequate resuscitation, sepsis, thyrotoxicosis, Cushings, steroids, or B-blockers.
5. Magnesium replacement
Monitor Magnesium q4h and replace PRN (See Electrolyte Abnormalities)
6. Phosphate replacement
Monitor Phosphate q4h and replace PRN (See Electrolyte Abnormalities)
7. Sodium bicarbonate 8.4% 70 to 100 mL IV, over 20 to 30 minutes.Treatment with bicarbonate should be reserved for those patients withsevere ketoacidosis and considered only if the pH is below 7 and creating animmediate cardiovascular risk. Sodium bicarbonate should be given as aninfusion of 1 to 2 mmol/kg with strict attention to potassium levels, whichmay fall precipitately. The aim of this treatment is to reduce the immediaterisks of extremely low pH, not to normalise pH.
REFERENCESTherapeutic guidelines: Endocrinology, Version 3, 2004.
www.gpkit.com.au 55

56 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
HYPEROSMOLARHYPERGLYCAEMIAHyperglycaemic hyperosmolar state occurs primarily in type 2 diabetesespecially in the elderly, and is characterised by marked hyperglycaemiaand dehydration but not ketoacidosis. The major laboratory findings areextreme hyperglycaemia and plasma osmolarity over 350 mosm/L; theserum sodium is frequently 140 mmol/L or higher.
Management is similar to DKA. Differences in treatment are:
1. More dilute solutions such as sodium chloride 0.45% should be usedinitially and given slowly.
2. Lower doses of insulin. These patients are more sensitive to insulin andrequire lower doses eg 0.05 to 0.1 units/kg/hour. It is not advisable to lowerblood glucose rapidly.
3. Confusion may be prolonged for several days after blood glucose isrestored to normal. Careful follow-up is essential.
4. Oral hypoglycaemic drugs should not be started immediately becausemany patients may be subsequently managed just with diet and exercise.
REFERENCESTherapeutic guidelines: Endocrinology, Version 3, 2004.
LACTIC ACIDOSIS INDIABETESLactic acidosis is most common in the setting of tissue hypoxia secondaryto shock and hypotension. It also occurs in liver disease and diabetesespecially if treated with metformin when renal function is impaired or inhypoxic states.
Treatment is directed at removing the cause, eg restoring circulating volume inthe hypotensive dehydrated patient. With severe lactic acidosis, bicarbonatetherapy is mandatory and several hundred mmol may be required.
REFERENCESTherapeutic guidelines: Endocrinology, Version 3, 2004.

MENINGOCOCCAL DISEASEMeningococcal disease is a hyperfulminent and uniformly fatal syndrome ifuntreated, which is manifest as meningitis alone (1/3 cases), septicemiaalone (1/3 cases), or a combination of meningitis and septicemia (1/3cases).
Most cases appear in spring and autumn with a bimodal age distributionwith peaks in early childhood and early adolescence.
Effective treatment is dependent on early recognition, but this is oftendifficult because early presentations (mean 4-6 hours after onset) aretypically non-specific and indistinguishable from other, self-limiting, febrileillnesses, such as influenza.
Classic symptoms of purpuric rash, meningism, drowsiness appear late inthe course of the illness (mean 13-22 hours after onset) when potentiallycurative treatment with penicillin is often not possible.
Early diagnosis is on average dependent on recognition of symptoms ofsepsis, which commence 6-8 hours after onset, are present in 70% ofcases, and consist of:
• leg pains,
• cold hands and feet
• abnormal skin colour
TREATMENT If menigococcal disease is suspected immediate prehospital treatment ismandatory and may be lifesaving.
1. Give benzylpenicillin 1200 mg IV immediately. (Child <1y 300mg, Child 1-9 years 600mg, Child >10 years).
2. In patients hypersensitive to penicillin or in remote areas where furtherparenteral therapy may be substantially delayed (>6 hours) give ceftriaxone50 mg/kg up to 2 g IV..
3. Arrange urgent transportation to hospital.
REFERENCES1.Thompson MJ. Ninis N Perera R .Clinical recognition of meningococcal disease in children andadolescents. Lancet. 367(9508):397-403, 2006 Feb 4.2.Therapeutic guidelines: Neurology. Version 2, 2002
www.gpkit.com.au 57

MENINGITIS1. Prehospital treatment. If meningitis is suspected immediate prehospital
treatment is mandatory and may be lifesaving.
a. Give benzylpenicillin 1200 mg IV or IM immediately. (Child <1y300mg, Child 1-9 years 600mg, Child >10 years).
b. Give ceftriaxone 50 mg/kg up to 2 g IV. In patients hypersensitive topenicillin or in remote areas where further parenteral therapy may besubstantially delayed (>6 hours).
2. Hospital treatment based on known or probable pathogen.
c. Meningitis caused by Neisseria meningitidis (meningococcalmeningitis). Give benzylpenicillin (child: 60 mg/kg up to) 1.8 to 2.4 gIV, 4-hourly for 5 to 7 days.For patients hypersensitive to penicillin(excluding immediate hypersensitivity), use cefotaxime (child: 50 mg/kgup to) 2 g IV, 6-hourly for 5 to 7 days OR ceftriaxone (child: 100 mg/kgup to) 4 g IV, daily OR (child: 50 mg/kg up to) 2 g IV, 12-hourly for 5 to 7days.
d. Meningitis caused by Streptococcus pneumoniae. For penicillin-susceptible strains (MIC <0.125mg/L), give benzylpenicillin (child: 60mg/kg up to) 1.8 to 2.4 g IV, 4-hourly for 10 days. For strains with an MIC>0.125 mg/L use vancomycin plus either cefotaxime or ceftriaxone,Specialist advice must be sought particularly if the MIC of thesecephalosporins is elevated. Rifampicin is a possible alternative tovancomycin.
e. Meningitis caused by Haemophilus influenzae type b (Hib) givecefotaxime (child: 50 mg/kg up to) 2 g IV, 6-hourly for 7 to 10 days orceftriaxone (child: 100 mg/kg up to) 4 g IV, daily OR (child: 50 mg/kg upto) 2 g IV, 12-hourly for 7 to 10 days.
REFERENCESThompson MJ. Ninis N Perera R .Clinical recognition of meningococcal disease in children andadolescents. Lancet. 367(9508):397-403, 2006 Feb 4.Therapeutic guidelines: Neurology. Version 2, 2002.
58 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

STATUS EPILEPTICUS1. Protect and maintain airway. Lie in recumbent (L) lateral position, suction,
insert Guedels airway.
2. Protect patient from self injury.
3. Oxygen 6-8L/min
4. Dextrostix: if low give glucose 50mls 50% solution IV.
5. To terminate convulsion give:
a. Diazepam 10 to 20mg bolus IV, not exceeding 2 to 5mg/minutetitrating to response; repeat once 15 minutes later if status epilepticuscontinues (child: 0.1 to 0. 25mg/kg bolus IV, over 2 to 5 minutes).Monitor with pulse oximetry.OR
b. Clonazepam 1 to 2mg bolus IV, not exceeding 0.5mg/minute; repeatonce 15 minutes later if status epilepticus continues (child: 0.25 to 0.5mgbolus IV, over 2 to 5 minutes)OR
c. Midazolam 5 to 10mg (child: 0.2mg/kg) IM, repeat once 15 minuteslater if status epilepticus continues.NB if IV access not possible giveDiazepam 10mg RECTALLY, either as suppository or administered PR bysyringe (without needle!)ORIntranasal midazolam (0.3 to 0.5mg/kg/dose up to a maximum of 10mg).
If seizures persist after repeated diazepam (eg 5mg x4 = 20mg doses) give:
6. Phenytoin 15mg/kg in 100mls NS over 1 hour (but no faster than50mg/min). (child: 20mg/kg IV, not exceeding 25mg/minute), providing nophenytoin has been given in the preceding week.
If seizures persist after valium and phenytoin, transfer to ICU or:
7. Intubation and barbiturate anaesthesia. Give thiopentone 3-5mg/kg at25mg/min for intubation followed by infusion (See IV Drug Infusions). Plusappropriate muscle relaxant.
8. Consider and treat causes: Poor compliance ; sleep deprivation (in knownepileptics); hypoxia (eg following bcardiac arrest); meningitis; drug overdose(tricyclics, theophyline, amphetamines); drug withdrawal (alcohol, benzodi-azepines); metabolic (hypoglcemia, hyperthyroid); electrolyte disturbances(hyponatremia, hypocalcemia, hypomagnesemia); CVA; cerebral tumour.
REFERENCESTherapeutic guidelines: Neurology. Version 2, 2002.
www.gpkit.com.au 59

ACUTE STROKEUrgent transport to hospital with neuroimaging facilities. Stroke should beconsidered as urgent as AMI or acute trauma.
Urgent CT or MRI scan. To differentiate between ischemic or hemorrhagicstroke.
If CT/MRI confirms ischemic stroke give:
1. Aspirin OR clopidogrel OR aspirin + dipyridamole. Aspirin given within 48hours reduces mortality by 20%.
2. Admission to stroke unit (>20% overall reduction in mortality) Adequateoxygenation, hydration, control of BSL, nursing care.
3. Antihypertensives. Cautious use in consultation with stroke physician ifmarkedly elevated blood pressure (systolic greater than 220 mm Hg).
4. Unfractionated IV heparin is indicated for patients at very high risk ofrecurrent embolism in consultation with stroke physician.
5. Tissue plasminogen activator (alteplase, rt-PA). alteplase 0.9mg/kg(maximum of 90mg), over 1 hour with 10% of the dose given as an initialbolus. Each 50mg vial is reconstituted using the 50mL diluent provided bythe manufacturer, and then the appropriate dose is administered with nofurther dilution. Give only in consultation with stroke physician. Improvesoutcomes if given to selected patients within 3 hours of onset of acuteischaemic stroke. Improved outcomes may come at the risk of symptomaticintracerebral haemorrhage (5% to 7%).
REFERENCESTherapeutic guidelines: Neurology. Version 2, 2002.
60 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

ACUTE ANAPHYLAXISDefinition: bronchospasm, stridor, hypotension or severe generalisedurticaria.
1. Oxygen 6L/min
2. Adrenaline 0.3 to 0.5mg (0.3-0.5 ml of 1:1000 sol) SC. Repeat at 15-30min
OR (if severe)
Adrenaline 0.3 mg (3 ml of 1:10000 sol) IV over 1 minute followed byinfusion
Adrenaline 1mg in 250 mls 5%D (4ug/ml) as infusion at 1-10ug (0.25 -2.5mls) /min, titrating to maintain BP.
3. Hydrocortisone 100mg IV or Prednisone 1mg/kg PO
4. Phenergan (H1 blocker) 12.5-25mg IV
Plus
5. Cimetidine (H2 blocker) 300mg IV or Ranitidine 50mg IV
If the above fails to reverse anaphylaxis, individual manifestations ofanaphylaxis of hypotension, bronchospasm, stridor, should be treated asrequired.
6. Fluid resuscitation. If in shock fluid resuscitation with multiple IV access andtransfusion. Very large volumes may be required. Should be given withadrenaline infusion as above.
7. Bronchodilators. If in bronchospasm and poor response to adrenaline, treatas for asthma (viz. continuous nebulised salbutamol, steroids, IV salbutamol)
8. Maintain upper airway. If severe upper airway obstruction (increasingstridor and hypoxia) not relieved by adrenaline consider intubation oremergency cricothyrotomy.
9. Admit for 24 hours following major anaphylaxis (stridor, bronchospasm,shock)
10. Discharge on diphenhydramine 25mg q6h and predisone 60mg/day, for3 days.
www.gpkit.com.au 61

62 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
DRUG OVERDOSE1. Contact Poisons Centre. Ph (02) 131126 for details of toxicology, specific
and supportive treatment.
2. Activated charcoal. 1g/kg (+Sorbitol 1ml/kg of 70% solution) as slurry. Maybe swallowed or administered via nasogastric tube. Multiple doses (0.25g/kgat q2h) are indicated in overdose of barbiturates, theophylline, digoxin,salicylates, carbamazepine, phenytoin. NB Activated charcoal not useful foracids, alkalis, ethanol, ethylene glycol, methanol, lithium or iron.
3. IV Fluids: 1-2L NS at q2-4h depending on age, hydration, cardiovascularstatus.
4. Paracetamol level on all patients presenting with overdose.
NOTE: a. Gastric lavage is generally not recommended unless overdose<1 hour
and potentially very toxic (eg TCA or Ca channel blocker OD). Ifindicated, lavage via orogastric or nasogastric tube. Aspirate beforelavage, then lavage with water (1ml/kg) at body temperature. Recoverlavage before repeating until lavage aspirates clear.
Contraindicationsi. corrosives. ii. petroleum derivatives. Airway must be protected with cuffed
endotracheal tube where consciousness is impaired or gag reflex isabsent.
b. Ipecac is generally no longer used (less effective, risk of aspiration), butmay be justified in serious OD when lavage not available, consciousnessis not impaired and transfer to hospital is likely to be delayed (>1-2hr)

Specific treatmentsNarcotics.
Naloxone (Narcan)0.4mg IV (+flush)
May also be give 0.4mg IM concurrently. Repeat 0.4mg (1 amp) IV every 1-2minutes until response. Large initial dose of 2mg (x5 amps) may also be given. Ifno response after maximum 10mg, suspect combined drug effect or othercauses of coma.
Benzodiazepines.
Flumazenil (Anexate) 0.2mg IV. Repeat at 0.1mg / minute until response or total1mg. Avoid if multiple drug OD, particularly TCAs, as flumazenil may effectivelylower the seizure threshold.
Paracetamol.
N-acetyl-cysteine (Parvolex)
150mg/kg in 200mls 5%D over 30mins, followed by
50mg/kg in 500mls 5%D over 4 hours, followed by
100mg/kg in 1litre 5%D over 16 hours.
Indication: serum paracetamol >200 mg/L (or 1300 umol/L) at 4 hours postingestion.
Warfarin:
If patient normally requires anticoagulation give Vitamin K 1mg IV slowly over10 minutes. Avoid completely if prosthetic values (give FFP only).
Otherwise give Vitamin K. 5-10mg SC.
PLUS
Fresh frozen plasma (FFP) 2 units stat.
Check INR at 3-4 hours and repeat Vitamin K and FFP prn.
Heparin
If APPT raised above therapeutic range in the course of normal dose schedule:Stop heparin 1/2-1hr, then adjust infusion rate according to specific protocol..
If massive inadvertent overdose: Give protamine sulphate (1mg protamine/100units of heparin given in the preceding 15 minutes to max 50mg.) no faster than50mg protamine over 10 minutes.
www.gpkit.com.au 63

64 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
ACUTE UPPERGASTROINTESTINAL BLEED1. Fluid resuscitation. Monitor BP, CVP, UO. If hypotensive or postural drop
(postural drop of 10mmHg=1 liter blood loss) give Hartmans solution torestore BP,CVP,UO. Start with 1 unit bolus then repeat based on clinicalresponse.
2. Transfuse. If bleeding severe and persistent consider transfusion with Onegative blood. Otherwise X-match 4-8 units. Monitor Hb and transfuse tomaintain Hb>10g/dl.
3. H2 Antagonist IV. eg Zantac 50mg IV q8h, Famotidine 20mg IV q12h
4. Correct coagulopathy.
i. Correct clotting abnormality.Monitor INR and APPT. If any clottingabnormality give Vitamin K 10mg IV over 10 minutes and Fresh FrozenPlasma (FFP) 2 units stat.
ii. Platetlet transfusion. If platelets<50,000 give platelets 2 units stat.
5. Maintain nil by mouth. This is usually sufficient (with bed rest) to stopbleeding.
6. Arrange endoscopy within 24hours. Arrange urgently if bleeding ispersistent to locate bleeding point pending laparotomy (or to scleroseesophageal varices).
7. Obtain surgical consult if:
i. Massive bleed.(eg hypotension or transfusion>5 units)
ii. Recurrence of bleeding during hospitalisation
iii. Bleeding for >12h
iv. Age>50
v. Past history of previous bleed.
8. Octreiotide. If varices known or suspected and bleeding uncontrolled by 1-5 above give: Octreotide 50mcg IV over 5 mins followed by infusion250mcg in 100mls NS at 25mcg (10mls)/hr. If no response increase to 50mcg(20mls)/hr.
9. Insertion of Sengstaken-Blackmore tube for 48hours if bleeding due tovarices and no response to 1-5,8 above.

HYPERKALAEMIAUrgent treatment: If K>7 or signs of cardiac toxicity (peaked T waves,prolonged PR, deep S, ventricular arrhythmias). Give:
Intravenous calcium gluconate 10% 10 mL IV, over 2 to 3 minutes into a largevein (with ECG monitoring of the response, if possible). Calcium alleviates thecardiac complications by reversing the membrane depolarisation of severehyperkalaemia. In the presence of life-threatening cardiac arrhythmia or severeECG changes of acute hyperkalaemia. The effect is short-lived and the dosemay need to be repeated in 30 to 60 minutes.
Intravenous sodium bicarbonate 8.4% (1 mmol/mL) 50 mL IV over 5 to 10minutes under ECG control. Indic: if metabolic acidosis is associated withvolume depletion. This may be repeated in 60 to 120 minutes. (NOTE: toprepare an approximately isotonic bicarbonate solution, add 50 mL 8.4%sodium bicarbonate to 500 mL 0.45% sodium chloride)
Glucose 50% 50 to 100 mL TOGETHER WITH a short-acting insulin 10 to 20units, IV over 5 to 10 minutes. Insulin action promotes cellular uptake ofpotassium. Serum potassium will decrease by 0.5 to 1.5 mmol/L over 30minutes. NB Hypoglycaemia, possibly due to adrenal insufficiency, must beruled out before insulin is given.
Consider:
Salbutamol 0.5 mg IV (4 micrograms/kg in children) OR salbutamol 10 mgby nebuliser (2 to 5 mg in children) Beta2-adrenergic agonists promote tissueuptake of potassium, but have the potential disadvantage of precipitatingcardiac arrthythmia. Either can be expected to decrease serum potassium by 0.5to 1.5 mmol/L in 30 to 90 minutes.
Other treatments: Consider if K<7 and no signs of cardiac toxicity
1. Correction of volume depletion. Any volume depletion should be corrected,to optimise renal function.
Sodium polystyrene sulfonate (Resonium A) 25 to 50 g in suspension.Each gram removes about 1 mmol of potassium from the bowel, and lowersthe serum potassium by 0.5 to 1 mmol/L over 1 to 6 hours.
For intractable hyperkalcemia
Dialysis. Where hyperkalaemia is extreme, as in extensive tissue breakdowndue to rhabdomyolysis, none of the above approaches may be effective anddialysis will be required.
www.gpkit.com.au 65

URGENT ELECTROLYTEABNORMALITIESHypokalemia. If in context of cardiac arrythmias give 10 mmol (0.75g) KCl over1/2 hr in 100mls NS (less rapidly in less urgent settings).
Hypocalcemia. Estimate corrected Ca = Ca + [(40-Albumin (g/L) x 0.02] If low incontext of cardiac arrythmias or tetany give: Loading: Calcium chloride 10mls10% over 10-15mins (ECG monitor) then infusion: 20mls 10% CaCl in 100mls NSover 4 hours.
Hypomagnesemia. Loading: Mg 10mmol in 20mls NS over 1 hour theninfusion: Mg 20mmol in 100mls NS over 4 hours.
Hypophosphatemia. Infusion: Phosphate 10mmol in 20mls NS over 2 hours
PAEDIATRIC FLUIDREPLACEMENT1. Maintenance
Give: N/4 if maintenance alone
If <10kg: 100mls/kg/day
If 10-20kg: 1000mls + 50mls/kg/day for every kg over 10kg
If >20kg: 1500mls + 20mls/kg/day for every kg over 20kg
PLUS
2. Replacement:
Give: N/2 if clinically dehydrated
% Dehydration x Kg X 10 over 24 hours.
3. If circulatory collapse:
Give IV fluids (normal saline) initially 10-20 ml/Kg as rapid infusion (over 15minutes).
66 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006

INTEROSSEOUS NEEDLEPLACEMENTINDICATIONS
To establish parenteral means to administer fluids and IV medications inchildren in whom IV access is difficult or impossible.
PROCEDURE1. Sterile technique as situation permits.
2. Local anaesthetic if patient is conscious.
3. Preferred site: the proximal anteromedial tibia, 1-3 cm below the tibialtuberosity
4. Angle 14-16 g cannula at 90 degree angle to the skin surface, approximatelyone to two finger breadths distal to the tibial tuberosity. With a straightsteady push and/or rotary motion, push needle through subcutaneous tissueand bone until a drop or pop is felt. Once the needle has reached the bonemarrow, it should be held by the bone cortex, but if necessary may beanchored with tape and/or plaster of paris.
5. Fluids usually require injection using 60 ml syringe. All fluids or drugs whichare injected IV may be injected through interosseous needle, and enter thecirculation at rates comparable to IV administration.
www.gpkit.com.au 67
Tibial Tuberosity
Anterior Border
90˚ to MedialSurface

68 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
APPENDIX 1. IV DRUG INFUSIONSNote: Drug infusion regimes may vary at different centres.
AdrenalineMust be given via central line
Infusion: 4mg (4 amps of 1:1000) in 100mls 5%D. Start at 10mls/hr and titrate toBP and PR, to maximum of 50mls/hour.
AmiodaroneLoading: 300mg (x2 amps) in 20mls NS or 5%D IV over 60 mins.
Infusion: 600mg in500mls 5%D over 12 hours.
Dobutamine May be given via peripheral line.
Infusion:: 250mg (1amp) in 100mls 5%D (2.5mg/ml). Start at 5 ug/kg/min(approx 8ml/hr for 70kg man)
Increase at increments of 5 ug/kg/min (approx 8mls/hr for 70kg man) to max40ug/kg/min (approx 80mls/hr for 70kg man).
Dopamine Must be given via central line
Infusion: 200mg (1amp) in 100mls 5%D (2mg/ml). Start at:
2.5ug/kg/min (approx 5mls/hr for 70kg man) – renal dose
ug/kg/min (approx 10ml/hr for 70kg man) – ionotropic dose
Increase at increments of 5 ug/kg/min (approx 10ml/hr for 70kg man) to max20ug/kg/min (approx 40mls/hr for 70kg man).
Glyceryl Trinitrate (Tridil). Infusion: 50mg (1amp) in 500mls 5%D. Start at 5ug/min (3mls/hour) and titrateto pain and to keep BP>100 mmHg.
Heparin Loading: 5000 units IV as bolus (take blood for coags first!)
Infusion: 25000 units in 500mls NS Start at 20mls (1000 units)/hour and titrate toAPTT

IsuprenalineLoading: 0.2mg (1 amp) in 10mls NS and give 1-3mls
Infusion: 1mg in 100mls 5%D (10ug/ml). Start at 5mls/hr (50ug/hr) and increasein increments to maximum of 100mls/hr, titrating to PR and BP.
LignocaineLoading: 1mg/kg IV over 1 minute.
Infusion: 2g in 500mls 5% D (preloaded bag). Start at 4mg/min (60mls/hr) for 2hours, then 3mg/min (45mls/hr) for 2 hours, then 2mg/min (30mls/hr) for 24hours.
ManitolLoading: 1g/kg over 20 minutes.
Infusion: 100g in 500mls (20% solution) at 10mls/hour
NoradrenalineMust be given via central line
Infusion: 4mg in 100mls 5%D. Start at 10mls/hr and titrate to response tomaximum of 50mls/hour.
Salbutamol Loading: 250ug (1amp) in 10mls 5%D over 5minutes
Infusion: 3mg (6amps) in 100mls 5%D (30mg/ml). Start at 5ug/min (=10mls/hr).Increase in 5ug/min increments every 15-30mins until control achieved tomaximum of 40mls/hour.
SotololLoading: 0.5mg/kg IV in 10mls 5%D over 10-30 minutes
Infusion: 80mg (8mls) into 72mls 5%D = 80mls = 1mg/ml. Give 160-240mg(160-240mls) /day
Thiopentone Loading: 3-5mg/kg at 25mg/min
Infusion: 10g in 500mls NS or 5% D (20mg/ml). Start at 2.5mg /kg/hr (ie8.75mls/ hr for 70 kg man)
www.gpkit.com.au 69

APPENDIX 2.EMERGENCY TELEPHONENUMBERSPoisons information centre (National): 131126
Hospitals
Other emergency numbers
Commonwealth Carer Respite Centre 1800 059 059
70 MANUAL OF MEDICAL EMERGENCIES 2nd Edition 2006
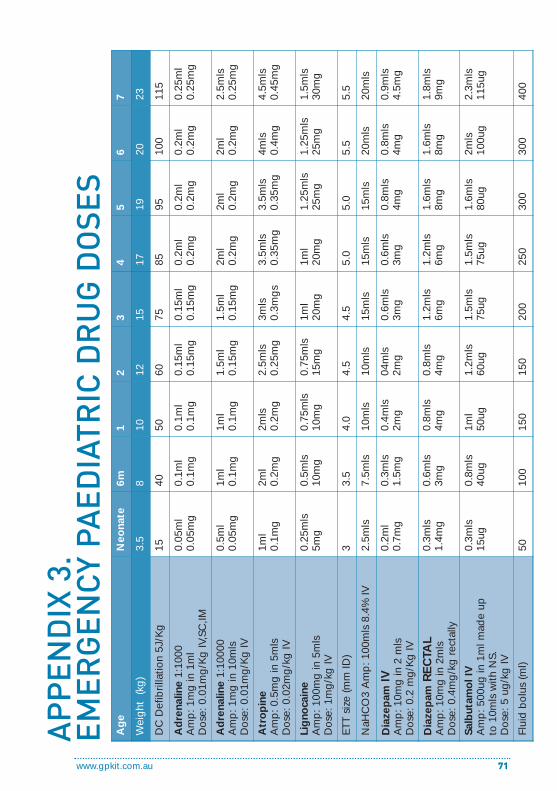
www.gpkit.com.au 71
AP
PE
ND
IX 3
. E
ME
RG
EN
CY
PA
ED
IAT
RIC
DR
UG
DO
SE
S
Ag
eN
eona
te6m
12
34
56
7
Wei
ght
(k
g)
3.5
810
1215
1719
2023
DC
Def
ibril
latio
n 5J
/Kg
1540
5060
7585
9510
011
5
Ad
rena
line
1:10
00A
mp
: 1m
g in
1m
l D
ose:
0.0
1mg
/Kg
IV,S
C,IM
0.05
ml
0.05
mg
0.1m
l0.
1mg
0.1m
l0.
1mg
0.15
ml
0.15
mg
0.15
ml
0.15
mg
0.2m
l0.
2mg
0.2m
l0.
2mg
0.2m
l0.
2mg
0.25
ml
0.25
mg
Ad
rena
line
1:10
000
Am
p: 1
mg
in 1
0mls
Dos
e: 0
.01m
g/K
g IV
0.5m
l0.
05m
g1m
l0.
1mg
1ml
0.1m
g1.
5ml
0.15
mg
1.5m
l0.
15m
g2m
l0.
2mg
2ml
0.2m
g2m
l0.
2mg
2.5m
ls0.
25m
g
Atr
op
ine
Am
p: 0
.5m
g in
5m
lsD
ose:
0.0
2mg
/kg
IV
1ml
0.1m
g2m
l0.
2mg
2mls
0.2m
g2.
5mls
0.25
mg
3mls
0.3m
gs
3.5m
ls0.
35m
g3.
5mls
0.35
mg
4mls
0.4m
g4.
5mls
0.45
mg
Lig
noca
ine
Am
p: 1
00m
g in
5m
lsD
ose:
1m
g/k
g IV
0.25
mls
5mg
0.5m
ls10
mg
0.75
mls
10m
g0.
75m
ls15
mg
1ml
20m
g1m
l20
mg
1.25
mls
25m
g1.
25m
ls25
mg
1.5m
ls30
mg
ETT
size
(mm
ID)
33.
54.
04.
54.
55.
05.
05.
55.
5
NaH
CO
3 A
mp
: 100
mls
8.4
% IV
2.5m
ls7.
5mls
10m
ls10
mls
15m
ls15
mls
15m
ls20
mls
20m
ls
Dia
zep
amIV
A
mp
: 10m
g in
2 m
lsD
ose:
0.2
mg
/Kg
IV
0.2m
l0.
7mg
0.3m
ls1.
5mg
0.4m
ls2m
g04
mls
2mg
0.6m
ls3m
g0.
6mls
3mg
0.8m
ls4m
g0.
8mls
4mg
0.9m
ls4.
5mg
Dia
zep
amR
EC
TAL
Am
p: 1
0mg
in 2
mls
Dos
e: 0
.4m
g/k
g r
ecta
lly
0.3m
ls1.
4mg
0.6m
ls3m
g0.
8mls
4mg
0.8m
ls4m
g1.
2mls
6mg
1.2m
ls6m
g1.
6mls
8mg
1.6m
ls8m
g1.
8mls
9mg
Salb
utam
ol I
VA
mp
: 500
ug in
1m
l mad
e up
to
10m
ls w
ith N
S.
Dos
e: 5
ug
/kg
IV
0.3m
ls15
ug0.
8mls
40ug
1ml
50ug
1.2m
ls60
ug1.
5mls
75ug
1.5m
ls75
ug1.
6mls
80ug
2mls
100u
g2.
3mls
115u
g
Flui
d b
olus
(ml)
5010
015
015
020
025
030
030
040
0

To doctors who go out into the community - along city streets,suburban thoroughfares and country roads, at all times of theyear and all hours of the day and night; to manage medicalemergencies in shopping centres, boarding houses and loungerooms; who work alone, without the assistance or council ofcolleagues, using only what equipment they can carry, and whatskills they have gained through experience; whose dedicationwill go unwitnessed, whose consideration will go unrecognised,who will receive no professional accolade, no great honor, andno reward - other than the gratitude of their patients. To thosebrave, dedicated and worthy colleagues - this manual isrespectfully dedicated.

Emergencies can occur at any time, and when they do, a GP is
often first on the scene. gpkit makes it easy to prepare for
medical emergencies. Designed by GPs for GPs, gpkit brings
together emergency equipment, accessories and emergency
drugs in a well designed accessible kit.
Unique features of gpkit include:
• essential emergency equipment
and accessories organised and
displayed in specially adapted case
with 3 fold out trays maximising
visibility and accessibility
• Labelled spaces for doctors bag
PBS drugs
the essential all-in-oneemergency kit for GPsgpkit
visit www.gpkit.com.au or call 02 9918 5256
• Includes all airways, adaptors, bag-
mask resuscitator, spacer, dwellcaths,
cannulae, IV fluids and more
• Manual of current evidence
based emergency guidelines
• Easy web based re-ordering
of all components
Endorsed by the RACGP

















