23
CONFIDENTIAL Jefferies 2016 Healthcare Conference Greg Weinhoff, Chief Financial Officer
| Date post: | 20-Mar-2018 |
| Category: |
Documents |
| Upload: | truongduong |
| View: | 220 times |
| Download: | 2 times |

CONFIDENTIAL
Jefferies 2016 Healthcare ConferenceGreg Weinhoff, Chief Financial Officer

Statements made in this presentation contain forward-looking statements, including: statements regarding Axovant’sexpectations about timing of the results for the Phase 3 MINDSET study of intepirdine in patients with Alzheimer'sdisease, the Phase 2b HEADWAY-DLB study of intepirdine in patients with dementia with Lewy bodies, the Phase 2study of nelotanserin in patients with DLB or PDD suffering from visual hallucinations, the Phase 2 study of nelotanserinin patients with DLB suffering from RBD and other elements of its clinical development and regulatory strategy; andstatements regarding the size of the market opportunity for one or both drug candidates. Forward-looking statementscan be identified by the words such as “believe,” “anticipate,” “continue”, “estimate”, “project,” “expect,” “plan,”“potential,” “intends,” “may,” “will,” “would”, “could”, “should” or the negative or plural of these words or othersimilar expressions that are predictions or indicate future events, trends or prospects. Forward-looking statements aresubject to risks and uncertainties that could cause actual results and the timing of certain events to differ materiallyand reported results should not be considered as an indication of future performance. These risks and uncertaintiesinclude, but are not limited to: risks associated with the success, cost and timing of our product development activitiesand clinical trials; the approval and commercialization of our product candidates intepirdine and nelotanserin; andincreased regulatory requirements. These statements are subject to the risk that clinical trial data are subject todiffering interpretations, and regulatory agencies, medical and scientific experts and others may not share Axovant’sviews of the clinical study data. There can be no assurance that the clinical programs for intepirdine or nelotanserin willbe successful in demonstrating safety and/or efficacy, that we will not encounter problems or delays in clinicaldevelopment, or that any of our product candidates will ever receive regulatory approval or be successfullycommercialized. For a further description of the risks and uncertainties that could cause actual results to differ fromthose expressed in these forward-looking statements, as well as risks relating to Axovant’s business in general, see the“Risk Factors” section of our annual report on Form 10-K to be filed with the Securities and Exchange Commission onJune 6, 2016, and other filings that Axovant makes with the SEC from time to time. These forward-looking statementsare based on information available to Axovant as of the date of this presentation and speak only as of the date of thispresentation. Axovant disclaims any obligation to update these forward-looking statements, except as may be requiredby law.
June 2016
Forward-Looking Statements
2
• Become the leading company focused on the treatment of dementia by addressing all forms and aspects of the condition
Vision: Dementia Solutions
• Build a late-stage pipeline of CNS drugs in a capital-efficient manner todeliver value to patients and shareholders
Mission: Create Value for Patients and Shareholders
• Intepirdine (RVT-101) is one successful pivotal phase 3 study away from approval by FDA and EMA in Alzheimer’s disease
Lead Drug in Phase 3 for Alzheimer’s Disease
• Intepirdine and nelotanserin could potentially be first two drugs approved by FDA and EMA in Dementia with Lewy Bodies
Global Leader in Lewy Body Dementia
Axovant Sciences – The Dementia Solutions Company
3

Management and Directors
Axovant team includes developers of both Aricept (Dr. Friedhoff) and Namenda (Dr. Olanoff)
*Employee and officer of Axovant Sciences, Inc., a wholly-owned subsidiary of Axovant Sciences Ltd.
Strong Leadership Team
4
Vivek Ramaswamy*Chief Executive Officer
Greg Weinhoff, M.D.*Chief Financial Officer
Mark Altmeyer*President & Chief Commercial Officer
Lawrence Friedhoff, M.D., Ph.D.*Chief Development Officer
Ilise Lombardo, M.D.Vice President, Clinical Research
Atul Pande, M.D.Director
Lawrence Olanoff,M.D., Ph.D.Director

Market Leading Dementia Pipeline
5
Compound Indication Phase 1 Phase 2 Phase 3
Intepirdine (RVT-101)
Mild-to-moderate Alzheimer’s disease
Nelotanserin
Visual hallucinations in Lewy body dementia• DLB and Parkinson’s
disease dementia (PDD)
Dementia with Lewy bodies (DLB)
REM behavior disorder (RBD)• DLB

Key Highlights of Intepirdine in Mild-to-Moderate Alzheimer’s Disease
• Confirmatory MINDSET Phase 3 trial started in October 2015• Agreement with FDA on Special Protocol Assessment • Data and potential NDA filing expected in 2017
Intepirdine May be OneSuccessful Trial from Approval
• 16 clinical studies complete with > 1,300 human subjects exposed • Three new studies completed by Axovant, including at 70 mg QD dose• Dosing for 48 weeks with low dropout and adverse event rates
Favorable Safety and Tolerability Profile
• Benefits compared to donepezil alone are above baseline at earliest time points measured
• Benefits sustained for at least 48 weeks vs. donepezil alone
Immediate Benefit that is Sustained over Time
• Once-daily oral dosing• Potential for fixed-dose combination with donepezil at launch• No requirement for PET imaging, MRI monitoring, or IV infusions
Ease of Use for Patients
• Composition of matter IP protection through 2029 (including PTE)• Pending applications may extend patent life through 2035• Axovant owns global rights
Strong Intellectual Property Position
6

Proven Mechanism of Action with DonepezilMechanism Supports Potential Utility in Multiple Forms of Dementia
7
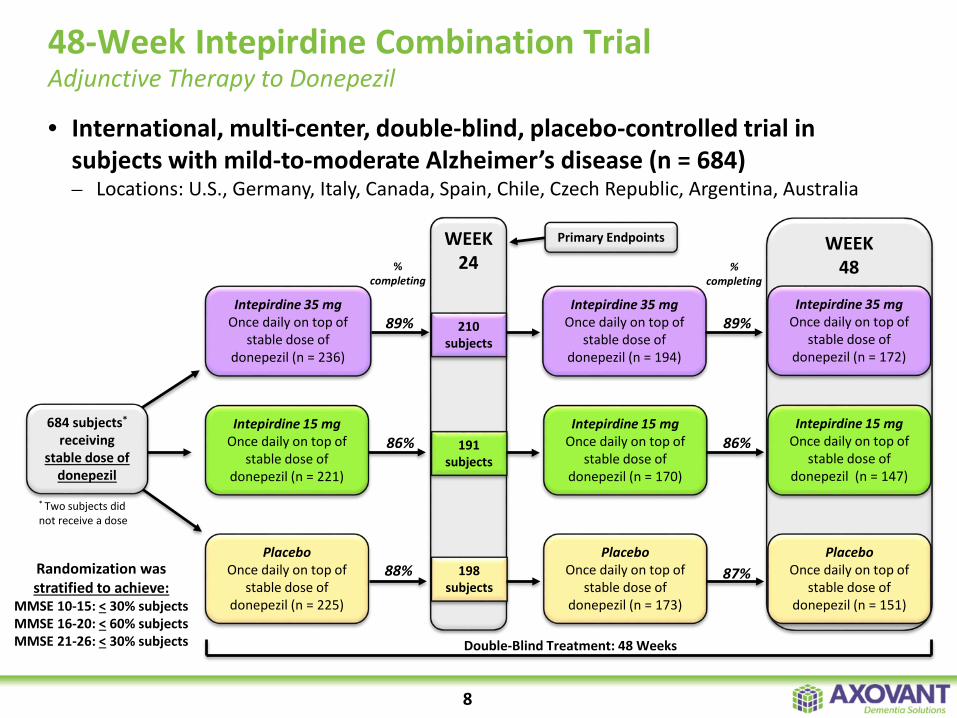
48-Week Intepirdine Combination TrialAdjunctive Therapy to Donepezil
Randomization was stratified to achieve:
MMSE 10-15: < 30% subjectsMMSE 16-20: < 60% subjectsMMSE 21-26: < 30% subjects
684 subjects*
receiving stable dose of
donepezil
* Two subjects did not receive a dose
Intepirdine 35 mgOnce daily on top of
stable dose of donepezil (n = 236)
PlaceboOnce daily on top of
stable dose of donepezil (n = 225)
% completing
89%
86%
88%
WEEK24
210 subjects
191 subjects
198 subjects
Double-Blind Treatment: 48 Weeks
Intepirdine 35 mg Once daily on top of
stable dose of donepezil (n = 194)
Intepirdine 15 mgOnce daily on top of
stable dose of donepezil (n = 170)
PlaceboOnce daily on top of
stable dose of donepezil (n = 173)
WEEK 48%
completing
89%
86%
87%
Intepirdine 35 mg Once daily on top of
stable dose of donepezil (n = 172)
Intepirdine 15 mg Once daily on top of
stable dose of donepezil (n = 147)
Placebo Once daily on top of
stable dose of donepezil (n = 151)
Intepirdine 15 mgOnce daily on top of
stable dose of donepezil (n = 221)
Primary Endpoints
• International, multi-center, double-blind, placebo-controlled trial in subjects with mild-to-moderate Alzheimer’s disease (n = 684)– Locations: U.S., Germany, Italy, Canada, Spain, Chile, Czech Republic, Argentina, Australia
8

Improvements on ADAS-cog and ADCS-ADL at 48 WeeksPre-Specified ITT Method of Analysis
9
Weeks
-1.5
-0.5
0.5
1.5
2.5
3.5
0 12 24 36 48
Change from Baseline: ADAS-cog
-6
-5
-4
-3
-2
-1
0
1
2
0 12 24 36 48
Change from Baseline: ADCS-ADL
Week 35 mg Intepirdine Difference vs. Donepezil Alone P- value
12 1.72 0.019
24 2.00 0.024
36 1.93 0.038
48 1.94 0.088
Week 35 mg Intepirdine Difference vs. Donepezil Alone P- value
12 1.30 0.006
24 1.50 0.013
36 1.21 0.057
48 1.64 0.024
Weeks
15 mg Intepirdine Plus Donepezil
35 mg Intepirdine Plus Donepezil
Donepezil Alone
15 mg Intepirdine Plus Donepezil
35 mg Intepirdine Plus Donepezil
Donepezil Alone

Intepirdine Phase 3 Confirmatory MINDSET TrialInitiated in October 2015
10
Intepirdine 35 mg Once daily on top of
stable dose of donepezil
PlaceboOnce daily on top of
stable dose of donepezil
WEEK 24
Primary Endpoints
Double-Blind Treatment: 24 Weeks
1,150 subjects receiving stable
dose of donepezil
Intepirdine 35 mg Once daily on top of any cholinesterase
inhibitor and/or memantine
Open-Label Extension: 52 Weeks
WEEK 76
Safety and Tolerability
Completing Subjects
Eligible for Open-Label Extension
Phase 3 MINDSET Design and Key Assessment Timeline
• FDA confirmed a single successful phase 3 trial may be sufficient to support regulatory filing
• Special Protocol Assessment (SPA) with FDA for MINDSET phase 3 trial
• Co-primary endpoints: ADAS-cog and ADCS-ADL Gold standard measures of cognition and function
• Two arms: intepirdine 35 mg and placebo May reduce residual placebo response
• 500+ subjects per arm (>2x as many as prior trial) Added statistical power relative to prior trial
Clear Regulatory Guidance: Designed to Replicate Success:
CONFIDENTIAL
Lewy Body Dementia

Lewy Body Dementia has both cognitive and behavioralaspects that have largely been unaddressed
What is Lewy Body Dementia?
Dementia with Lewy Bodies (DLB)
1.1 million patientsCognitive decline must occur
within one year of the onset of movement disorder symptoms
Umbrella term for two related diagnoses with
similar pathology and clinical presentation
Parkinson’s Disease Dementia (PDD)
300,000 patientsMovement disorder symptoms must precede cognitive decline
by more than one year
80% have visual hallucinations65% have RBD
70% have visual hallucinations30% have RBD
12

• No drugs approved in the U.S. or EU• Aricept was approved in Japan for the treatment of DLB in 2014
Significant Unmet Need
• A prominent feature of DLB• Cholinergic neurotransmission is more dysfunctional in DLB than Alzheimer’s
diseaseCholinergic Deficits
• Increasing acetylcholine improves cognition and function in DLB• Intepirdine promotes the release of acetylcholine
Cognition and Function
• 5HT2A activity is a potential driver of visual hallucinations1
• In addition to 5HT6 activity, intepirdine is an antagonist of the 5HT2A receptorBehavioral
Disturbances
13
Intepirdine in Dementia with Lewy Bodies (DLB)Potential First-in-Class Therapy
Evaluating 35mg and 70mg dose of intepirdine to increase 5HT2A receptor occupancy
1Ballanger et al., Arch Neurol 2010. Vol. 67:4, 416-421.

Intepirdine HEADWAY-DLB ProgramAddressing Cognition and Function
14
240 subjects with diagnosis of DLB
Intepirdine 70 mg
Placebo
Intepirdine 35 mg
WEEK 24
Primary Endpoints
Double-Blind Treatment: 24 Weeks
Completing Subjects Eligible
for Active Treatment Extension
Active Treatment Extension
• 240 subjects with diagnosis of DLB• MMSE score: 14 – 26 (inclusive)• Stable background therapy will be allowed
• Change from baseline on CIBIC+ and a computerized cognitive battery
• Safety, tolerability, and change in behavioral symptoms
Population: Key Endpoints:
Single successful study could serve as basis for approval of intepirdine in DLB when combined with Alzheimer’s NDA filing

CONFIDENTIAL
Nelotanserin

Nelotanserin: Potential Best-in-Class 5HT2A Inverse Agonist Initial Focus on Behavioral Disturbances in Lewy Body Dementia
5HT2A Antagonism
5HT2C Antagonism
Known risk of motor symptoms?
D2 Antagonism
Nelotanserin
NO
“Next Generation” 5HT2A Inverse Agonist
Atypical Antipsychotics1
YES
Strong Binding Affinity
Weak Binding Affinity
Pimavanserin2
NO
“1st Generation” 5HT2A Inverse Agonist
Known risk of QTc prolongation? MIXED YES NO
Drug Profile:
MIXED
16
1Richtand et al., Neuropsychopharmacology 2007. Vol. 32:8, 1715-1726.2Nordstrom et al., Int J Neuropsychopharm 2008. Vol. 11:2, 163-171.
17
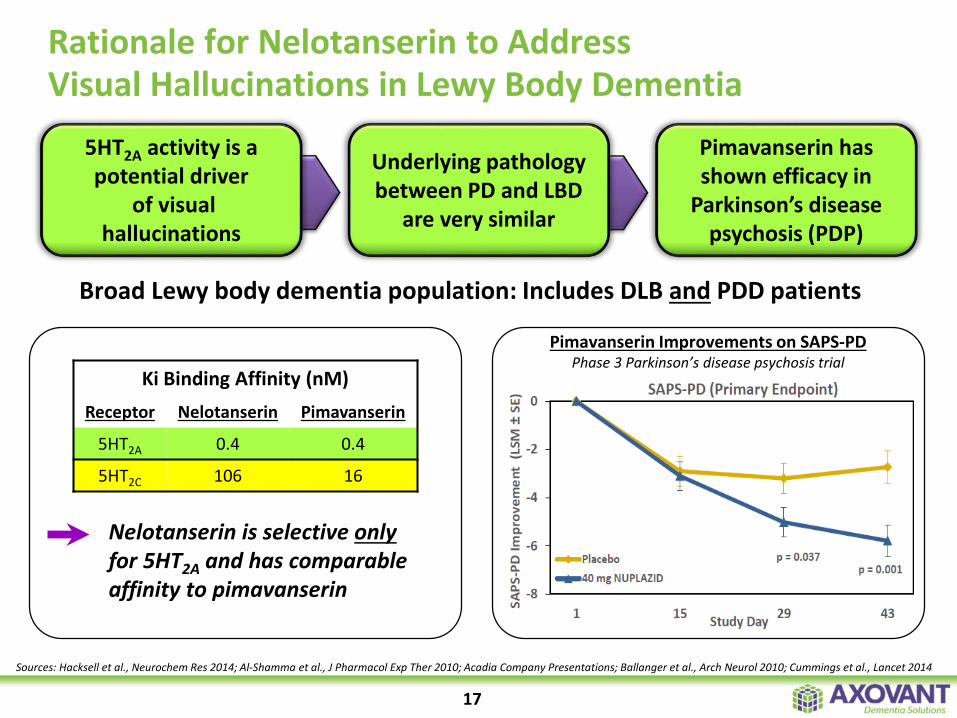
Sources: Hacksell et al., Neurochem Res 2014; Al-Shamma et al., J Pharmacol Exp Ther 2010; Acadia Company Presentations; Ballanger et al., Arch Neurol 2010; Cummings et al., Lancet 2014
5HT2A activity is a potential driver
of visual hallucinations
Underlying pathology between PD and LBD
are very similar
Pimavanserin has shown efficacy in
Parkinson’s disease psychosis (PDP)
Ki Binding Affinity (nM)Receptor Nelotanserin Pimavanserin
5HT2A 0.4 0.4
5HT2C 106 16
Pimavanserin Improvements on SAPS-PDPhase 3 Parkinson’s disease psychosis trial
Broad Lewy body dementia population: Includes DLB and PDD patients
Nelotanserin is selective onlyfor 5HT2A and has comparable affinity to pimavanserin
Rationale for Nelotanserin to Address Visual Hallucinations in Lewy Body Dementia
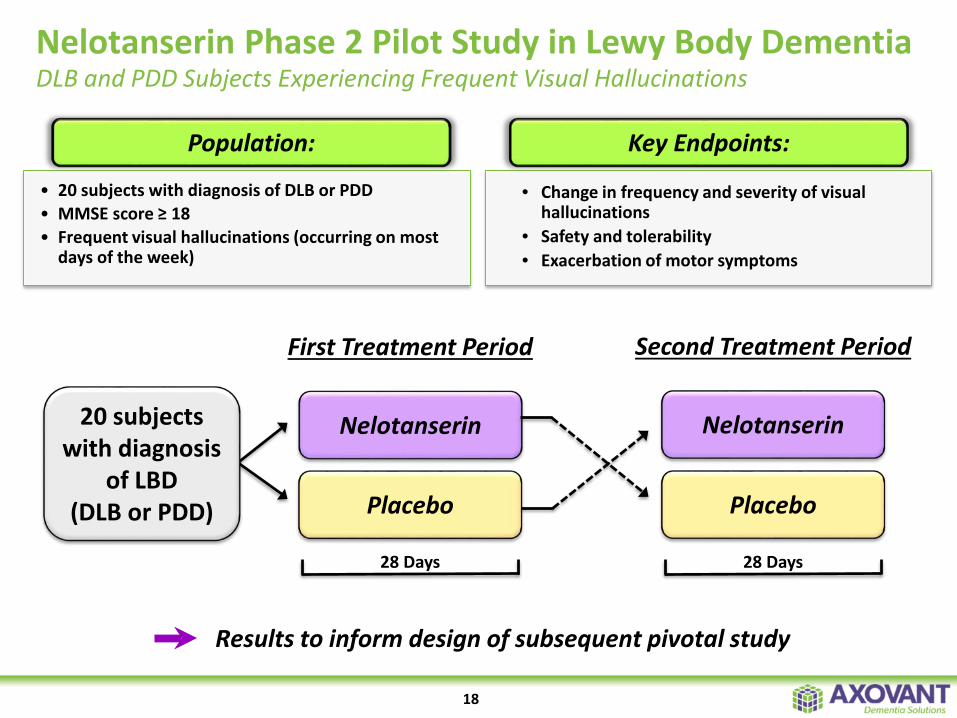
Nelotanserin Phase 2 Pilot Study in Lewy Body DementiaDLB and PDD Subjects Experiencing Frequent Visual Hallucinations
18
Results to inform design of subsequent pivotal study
• 20 subjects with diagnosis of DLB or PDD• MMSE score ≥ 18• Frequent visual hallucinations (occurring on most
days of the week)
• Change in frequency and severity of visual hallucinations
• Safety and tolerability• Exacerbation of motor symptoms
Population: Key Endpoints:
Nelotanserin20 subjects with diagnosis
of LBD (DLB or PDD)
28 Days
Placebo
Nelotanserin
Placebo
First Treatment Period Second Treatment Period
28 Days

-9
-7
-5
-3
-1
1
3
Placebo 10 mgnelotanserin
40 mgnelotanserin
Num
ber o
f Aro
usal
s
Number of Arousals Change from Screening
(Pre-Specified Modified ITT Population)
Night 1 and 2
Night 6 and 7
Nelotanserin produced statistically significant improvements on objective measures of sleep maintenance and consolidation
Rationale for Nelotanserin in DLB Patients Experiencing REM Behavior Disorder (RBD)
19
Sources: Rosenberg et al., SLEEP 2008; McKeith et al., Neuropsychopharmacology 2002.
Positive NelotanserinPhase 2 Objective Sleep Study
• n = 173 adult subjects with primary insomnia• Compared placebo to 10 mg and 40 mg nelotanserin• Subjects spent nights 1 and 2 and nights 6 and 7 combined in
a sleep laboratory• Both doses of nelotanserin showed robust benefits on wake
time after sleep onset, the primary endpoint (p < 0.0001)
Mean of:
Improvement
Blocking the 5HT2A receptor reduces visual hallucinations
Overlap between visual hallucinations and dream
content during REM behaviorsIn clinical studies, nelotanserin has shown robust
reductions in the number of arousals and awakenings
Arousals from sleep may trigger disruptive REM
behaviors
**
**
* = p < 0.0001
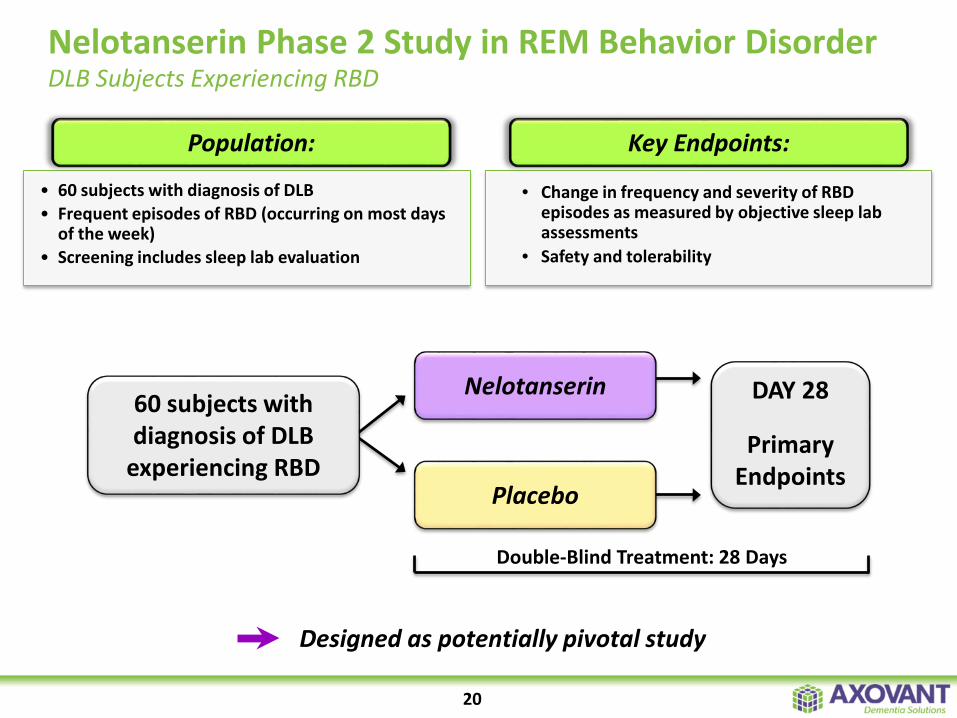
Nelotanserin Phase 2 Study in REM Behavior DisorderDLB Subjects Experiencing RBD
20
DAY 28
Primary Endpoints
Double-Blind Treatment: 28 Days
Nelotanserin
Placebo
60 subjects with diagnosis of DLB
experiencing RBD
• 60 subjects with diagnosis of DLB• Frequent episodes of RBD (occurring on most days
of the week)• Screening includes sleep lab evaluation
• Change in frequency and severity of RBD episodes as measured by objective sleep lab assessments
• Safety and tolerability
Population: Key Endpoints:
Designed as potentially pivotal study
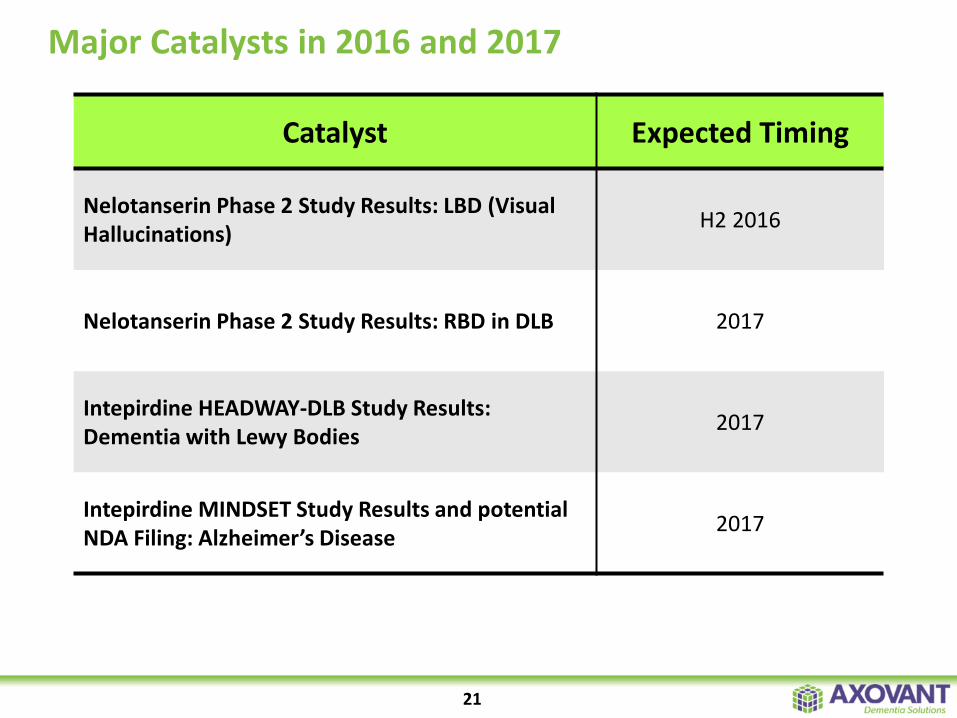
Major Catalysts in 2016 and 2017
Catalyst Expected Timing
Nelotanserin Phase 2 Study Results: LBD (Visual Hallucinations) H2 2016
Nelotanserin Phase 2 Study Results: RBD in DLB 2017
Intepirdine HEADWAY-DLB Study Results:Dementia with Lewy Bodies 2017
Intepirdine MINDSET Study Results and potential NDA Filing: Alzheimer’s Disease 2017
21

Axovant Sciences – The Dementia Solutions Company
22
Axovant is Uniquely Positioned as the Leader in Dementia Solutions

CONFIDENTIAL
Jefferies 2016 Healthcare ConferenceGreg Weinhoff, Chief Financial Officer
















