Health & Demographic Surveillance System Profile Health & Demographic Surveillance System Profile: The Ifakara Rural and Urban Health and Demographic Surveillance System (Ifakara HDSS) Eveline Geubbels, 1,2,3 * Shamte Amri, 2,4 Francis Levira, 1,3,4 Joanna Schellenberg, 5 Honorati Masanja 1,2 and Rose Nathan 1,2 1 Ifakara Health Institute, Mikocheni, Dar es Salaam, Tanzania, 2 INDEPTH Network, Kanda, Accra, Ghana, 3 ALPHA Network, London School of Hygiene and Tropical Medicine, London, UK, 4 Ifakara Health Institute, Ifakara Branch, Morogoro Region, Tanzania and 5 Department of Disease Control and Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK *Corresponding author. Ifakara Health Institute (IHI), Coordination Office, Plot 463, Kiko Avenue, off Old Bagamoyo Road, Mikocheni P.O Box 78373, Dar es Salaam, Tanzania. E-mail: [email protected]Accepted 24 March 2015 Abstract The Ifakara Rural HDSS (125 000 people) was set up in 1996 for a trial of the effectiveness of social marketing of bed nets on morbidity and mortality of children aged under 5 years, whereas the Ifakara Urban HDSS (45 000 people) since 2007 has provided demographic indicators for a typical small urban centre setting. Jointly they form the Ifakara HDSS (IHDSS), located in the Kilombero valley in south-east Tanzania. Socio-demographic data are collected twice a year. Current malaria work focuses on phase IV studies for antimal- arials and on determinants of fine-scale variation of pathogen transmission risk, to inform malaria elimination strategies. The IHDSS is also used to describe the epidemi- ology and health system aspects of maternal, neonatal and child health and for interven- tion trials at individual and health systems levels. More recently, IHDSS researchers have studied epidemiology, health-seeking and national programme effectiveness for chronic health problems of adults and older people, including for HIV, tuberculosis and non-communicable diseases. A focus on understanding vulnerability and designing methods to enhance equity in access to services are cross-cutting themes in our work. Unrestricted access to core IHDSS data is in preparation, through INDEPTH iSHARE [www.indepth-ishare.org] and the IHI data portal [http://data.ihi.or.tz/index.php/catalog/ central]. V C The Author 2015; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association 848 International Journal of Epidemiology, 2015, 848–861 doi: 10.1093/ije/dyv068 Advance Access Publication Date: 15 May 2015 Health & Demographic Surveillance System Profile Downloaded from https://academic.oup.com/ije/article-abstract/44/3/848/632298 by London School of Hygiene & Tropical Medicine user on 12 June 2020
Transcript
Health & Demographic Surveillance System Profile
Health & Demographic Surveillance System
Profile: The Ifakara Rural and Urban Health
and Demographic Surveillance System
(Ifakara HDSS)
Eveline Geubbels,1,2,3* Shamte Amri,2,4 Francis Levira,1,3,4
Joanna Schellenberg,5 Honorati Masanja1,2 and Rose Nathan1,2
1Ifakara Health Institute, Mikocheni, Dar es Salaam, Tanzania, 2INDEPTH Network, Kanda, Accra,
Ghana, 3ALPHA Network, London School of Hygiene and Tropical Medicine, London, UK, 4Ifakara
Health Institute, Ifakara Branch, Morogoro Region, Tanzania and 5Department of Disease Control and
Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine,
London, UK
*Corresponding author. Ifakara Health Institute (IHI), Coordination Office, Plot 463, Kiko Avenue, off Old Bagamoyo Road,
Mikocheni P.O Box 78373, Dar es Salaam, Tanzania. E-mail: [email protected]
Accepted 24 March 2015
Abstract
The Ifakara Rural HDSS (125 000 people) was set up in 1996 for a trial of the effectiveness
of social marketing of bed nets on morbidity and mortality of children aged under 5 years,
whereas the Ifakara Urban HDSS (45 000 people) since 2007 has provided demographic
indicators for a typical small urban centre setting. Jointly they form the Ifakara HDSS
(IHDSS), located in the Kilombero valley in south-east Tanzania. Socio-demographic data
are collected twice a year. Current malaria work focuses on phase IV studies for antimal-
arials and on determinants of fine-scale variation of pathogen transmission risk,
to inform malaria elimination strategies. The IHDSS is also used to describe the epidemi-
ology and health system aspects of maternal, neonatal and child health and for interven-
tion trials at individual and health systems levels. More recently, IHDSS researchers have
studied epidemiology, health-seeking and national programme effectiveness for chronic
health problems of adults and older people, including for HIV, tuberculosis and
non-communicable diseases. A focus on understanding vulnerability and designing
methods to enhance equity in access to services are cross-cutting themes in our work.
Unrestricted access to core IHDSS data is in preparation, through INDEPTH iSHARE
[www.indepth-ishare.org] and the IHI data portal [http://data.ihi.or.tz/index.php/catalog/
central].
VC The Author 2015; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association 848
International Journal of Epidemiology, 2015, 848–861
doi: 10.1093/ije/dyv068
Advance Access Publication Date: 15 May 2015
Health & Demographic Surveillance System Profile
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
In the 1990s, malaria transmission in the Kilombero valley
was among the highest in subSaharan Africa, with an average
entomological inoculation rate of 300 infectious bites per per-
son per year.1 As a result, malaria was the most important
health problem in the area (Tanner 19912). The Ifakara Rural
HDSS (IR-HDSS) was set up in 1996 as the basis for a field
trial on effectiveness of social marketing of bed nets on mor-
bidity and mortality of children aged under 5 years, the
Kilombero and Ulanga Net project (KINET). A number of
large-scale field intervention trials, epidemiological studies
and impact evaluations for malaria followed. Current malaria
work in humans focuses on Phase IV studies, providing effect-
iveness and safety data for antimalarials. The area of the rural
Ifakara HDSS is also home to one of the largest entomolo-
gical and environmental research programmes in Africa, pro-
viding detailed information on vector ecology and behaviour.
Currently, the environmental malaria research programme in-
vestigates ecological determinants of fine-scale within-village
variation of pathogen transmission risk, which is needed to
prepare for malaria elimination.
Small urban centres are home to around 25% of the
African population and are of social, economic, political
and demographic importance,3 yet few HDSS sites are
located in such settings. The Ifakara Urban HDSS
(IU-HDSS) was set up in 2007 to provide demographic
indicators in a typical small urban centre setting. The
IU-HDSS operates in five areas of Ifakara town, which is
the district capital of Kilombero District.
Both rural and urban HDSS sites are managed by the
Ifakara Health Institute (IHI), which has its coordination
office in Dar es Salaam and runs a further four branches in
the south of Tanzania (Ifakara, Rufiji, Bagamoyo,
Mtwara). At over 50 years, Ifakara is the oldest branch
and forms part of a unique cluster of organizations provid-
ing health services, training and research. As part of the
Ifakara branch, the Ifakara HDSS (IHDSS) is the central
platform for research in six themes along the research to
policy and practice pipeline. Within these themes, projects
are centred on a particular health problem (Figure 1).
What does it cover?
In the late 1990s, maternal, neonatal and child health
(MNCH) became a second focus of the IR-HDSS, first by
describing the epidemiology of and barriers to access to care
and quality of care. These were followed by intervention tri-
als at individual and health systems levels. More recently, IHI
researchers have studied chronic health problems of adults
and older people as a third focus in the IHDSS. These include
HIV, tuberculosis and non-communicable diseases (NCDs).
Last, a programme on neglected tropical diseases was added,
notably on the epidemiology and control of rabies and Rift
Valley Fever. In addition, the core Ifakara HDSS generates
patterns and trends of fertility and mortality, as well as cause-
specific mortality for all age groups, by socioeconomic status.
Table 1 gives a more detailed overview of the aims of the cur-
rent and future studies, addressed in our four programmes.
Population-based survey data will be linked to detailed clin-
ical data from the KIULARCO HIV cohort at the Chronic
Disease Clinic Ifakara4 to facilitate studies on linkage into
care and on retention in care and treatment.
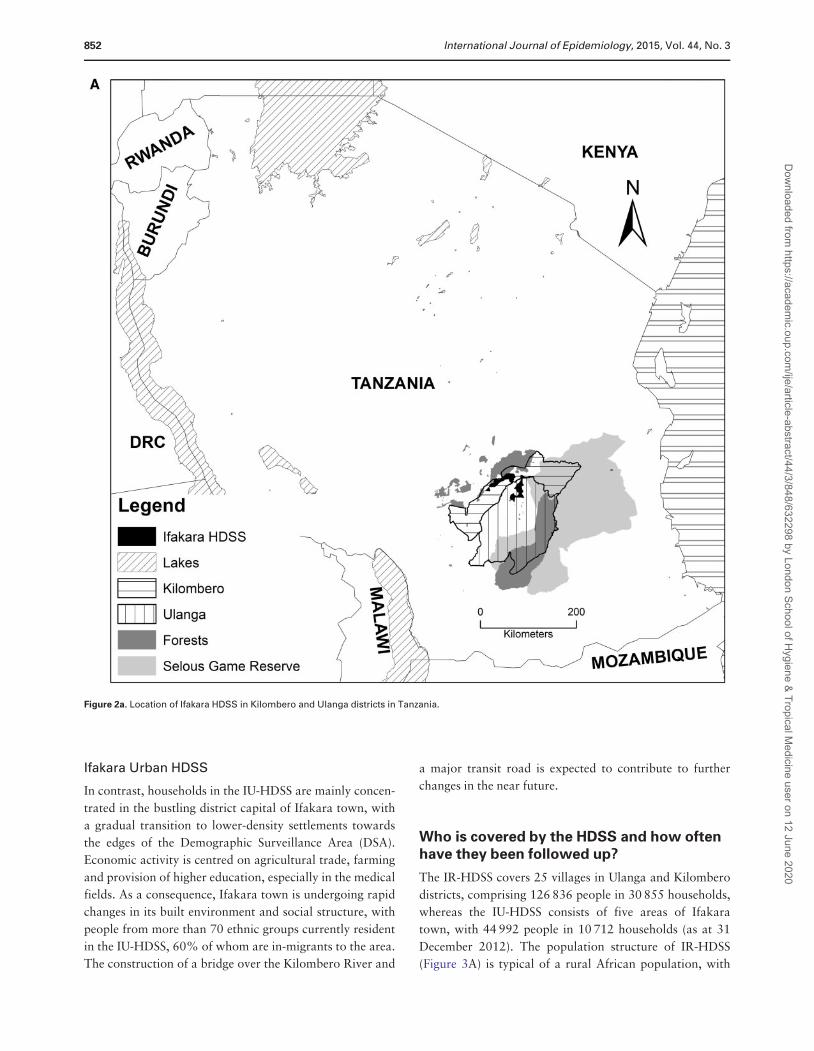
Where is the HDSS area?
The IHDSS is located approximately 450 km by road from
Tanzania’s commercial capital, Dar es Salaam. The HDSS
covers an area of 2400 km2 across two districts,
Kilombero and Ulanga in Morogoro Region, and lies
between latitudes 8�00’S and 8�35’S and longitude
35�58’E to 36�48’E at the altitude of 270–1000 m above
sea level. The mean household size is 4.2 and people usu-
ally live in a compound with one or two houses. The HDSS
area encompasses nine dispensaries, one health centre and
one referral hospital (Figure 2).
Ifakara Rural DSS
Households in the IR-HDSS are scattered in the Kilombero
Valley, wedged in between the Udzungwa Mountains trop-
ical rainforest, the grassland-covered Mahenge Mountains
and the woodland Selous Game Reserve. The valley forms
a seasonal flood plain of up to 52 km wide at high water,
Key Messages
• IHI’s multidisciplinary skills set, good research infrastructure, coupled with the unique position of IHDSS in a cluster
of research, health service delivery and health training organizations at district level allow for research along the en-
tire pipeline of intervention development to impact evaluation.
• Our experience in the malaria and child health fields demonstrates capacity to translate knowledge into action and to
influence policy at district, national and international levels, and has brought notable health improvements to the
HDSS area and beyond.
• The Ifakara urban HDSS is among the few HDSS sites located in small urban settings, which are estimated to be
home to 25% of Africa’s population.
International Journal of Epidemiology, 2015, Vol. 44, No. 3 849
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
and has an annual rainfall of 1200–1800 mm and tempera-
tures that range between 25�C and 32�C. During the rainy
season from November to May, households in some
villages are not accessible by motor vehicle. The main
economic activity is subsistence farming, especially of rice.
Small-scale fishing, hunting and pastoral livestock rearing
are also practised. The main vector species are Anopheles
spp., Culex spp, Aedes spp. and Mansonia spp.5
Figure 1. (A) Position of Ifakara HDSS in the Ifakara research, training and service delivery structure; (B) Research pipeline of the Ifakara HDSS six
research thematic groups and their topic areas.
850 International Journal of Epidemiology, 2015, Vol. 44, No. 3
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
Table 1. Current and future programme aims of studies based at Ifakara HDSS
Programme aims Study type
Malaria
Current
Assess effectiveness and safety of newly introduced antimalarials Phase IV observational cohort, surveillance
Develop novel vector control interventions, including spatial repellents,
odour-baited devices, mosquito filial infanticides and insect growth
regulators, botanical and biological control agents
Entomological cohort studies
Determine ecological determinants of variation in pathogen transmission
risk
Entomological field studies
Future
Test the malaria transmission impact of the above novel vector control
interventions
Field trials
Maternal neonatal and child health
Current
Describe patterns of maternal, neonatal and infant morbidity and
mortality and their structural associates
Demographic studies
Understand individual and health systems delays in delivery care Implementation studies
Test efficacy of neonatal vitamin A supplementation on neonatal
survival
Field trial
Test efficacy on maternal and child mortality of deploying paid
community health workers for providing preventive, promotionaL
and curative antenatal, new-born, child, and reproductive health care
Field trial
Future
Assess the determinants of early child development Population-based cohort study
Evaluation the impact of community-based family planning
service delivery
Population-based cohort study and implementation
science studies
Chronic disease
Current
Describe prevalence and incidence, comorbidity and mortality for
HIV and selected NCDs
Population-based cohort study
Understand impact of biological, lifestyle-related and social determinants
of chronic disease and healthy ageing
Population-based cohort and cross-sectional studies,
sociological studies
Assess changes in sexual behaviour, attitudes and risk perception Epidemiological and sociological studies
Explore community perceptions around emerging chronic diseases such
as diabetes and their impact on health seeking behaviourS
Sociological studies
Assess constraints and opportunities to adapt the health system architecture
to deal with chronic illness
Implementation science studies
Identify factors affecting antiretroviral treatment (ART) adherence and
occurrence of drug resistance
Clinical cohort study
Evaluate the impact of the ART programme Population-based cohort study and implementation
studies
Future
Dynamics of couple communication in relation to sexual risk-taking and
VCT testing
Sociological study
Health systems intervention for diabetes Field trial
Female cancer risk factors, burden, suffering and pathways to care Population-based cohort study
Health systems intervention studies for female cancers Implementation science studies
Neglected tropical diseases
Current
Epidemiology of inter-epidemic transmission of Rift Valley Fever Population- and livestock-based cross-sectional studies
Burden of rabies and impact on communities Surveillance and implementation science studies
Future
Understanding transmission dynamics between epidemics Entomological, facility- and community-based surveillance,
mathematical modelling
VCT, Voluntary Counseling and Testing.
International Journal of Epidemiology, 2015, Vol. 44, No. 3 851
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
Ifakara Urban HDSS
In contrast, households in the IU-HDSS are mainly concen-
trated in the bustling district capital of Ifakara town, with
a gradual transition to lower-density settlements towards
the edges of the Demographic Surveillance Area (DSA).
Economic activity is centred on agricultural trade, farming
and provision of higher education, especially in the medical
fields. As a consequence, Ifakara town is undergoing rapid
changes in its built environment and social structure, with
people from more than 70 ethnic groups currently resident
in the IU-HDSS, 60% of whom are in-migrants to the area.
The construction of a bridge over the Kilombero River and
a major transit road is expected to contribute to further
changes in the near future.
Who is covered by the HDSS and how oftenhave they been followed up?
The IR-HDSS covers 25 villages in Ulanga and Kilombero
districts, comprising 126 836 people in 30 855 households,
whereas the IU-HDSS consists of five areas of Ifakara
town, with 44 992 people in 10 712 households (as at 31
December 2012). The population structure of IR-HDSS
(Figure 3A) is typical of a rural African population, with
Figure 2a. Location of Ifakara HDSS in Kilombero and Ulanga districts in Tanzania.
852 International Journal of Epidemiology, 2015, Vol. 44, No. 3
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
46% of participants under 15 years old. In IU-HDSS only
38% of inhabitants are younger than 15, and 7% are 60
years or older (Figure 3B). Both HDSS sites show evidence
of net out-migration for young men, mainly for the pur-
pose of finding employment in more urbanized areas to
support themselves and their extended families.
The main ethnic groups in the valley are traditionally
farmers, with smaller proportions of pastoralists who
migrated into the area from the north and centre of
Tanzania. Over three-quarters of participants have had at
least some schooling, though only 23% have gone beyond
primary school.
Figure 2b. Map of Ifakara Urban and Rural DSS showing villages and town areas under surveillance, the Kilombero floodplain, primary and secon-
dary roads and location of health facilities.
Figure 3. Population pyramid of (A) Ifakara Rural HDSS; (B) Ifakara Urban HDSS, 2012.
International Journal of Epidemiology, 2015, Vol. 44, No. 3 853
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
Table 2. Additional variables collected in the IHDSS
Variable Location and
population
Period Modality R¼ HDSS
rounds
S ¼ special survey
Update frequency
Environmental risk factors
Latitude, longitude and altitude Households in both
HDSS
2006 – on-going R 2 per year
House building materials Households in both
HDSS
2007 (IU) - on-going R 1 per year
2000 (IR) - on-going
Malaria risk factors
Bed net ownership Households in both
HDSS
2007 (IU) - on-going R 1 per year
2003 (IR) - on-going
Bed net use Households in both
HDSS
2007 (IU) - on-going R 1 per year
2003 (IR) - on-going
MNCH risk factors
Pregnancy outcome Newborns in both
HDSS
2007 (IU) - on-going R 3 per year till 7/13
1997 (IR) - on-going 2 per year from 7/13
Birthweight Newborns in both
HDSS
2010 - on-going R 3 per year till 7/13
2 per year from 7/13
Family planning use Women in both HDSS 2011 – on-going R 3 per year till 7/13
2 per year from 7/13
Family planning intentions Women in both HDSS 2011 – on-going R 3 per year till 7/13
2 per year from 7/13
Child vaccination status U5 in both HDSS 2000- on-going R 3 per year till 7/13
2 per year from 7/13
Pregnant women’s anthropometrics Pregnant women in
both HDSS
2012 – 2013 S 3 per year till 7/13
2 per year from 7/13
Pregnant women’s nutritional intake Pregnant women in
both HDSS
2012 – 2013 S 3 per year till 7/13
2 per year from 7/13
HIV and STI risk factors
Sexual behaviour Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
HIV and STI KAP Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
NCD risk factors
Height, weight, WC, HC Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Smoking Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Alcohol use Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Diet Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Physical exercise Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Family history of NCD Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Sleep patterns Adults 15þ in part of
IU-HDSS
2014/5 S Once every 2 years
(Continued)
854 International Journal of Epidemiology, 2015, Vol. 44, No. 3
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
Despite the variety of ethnic groups, Swahili is the main
language of communication in both parts of the HDSS,
whereas English is also spoken by professionals living in
the urban HDSS.
For the IR-HDSS the baseline census happened between
September and December 1996, and for the IU-HDSS the
census was done between January and April 2007. All indi-
viduals who were intending to be resident in the DSA for
at least 4 months were eligible for inclusion. Verbal
consent to participate in the census was sought from the
head of every family. After the census, the study popula-
tion was visited three times a year in January–April,
May–August and September–December, to document
demographic events in each household including
in-migration, out-migration, births and deaths. From mid
2013 onward, both HDSS sites switched to two data
collection rounds per annum, which happen in
July–December and January–June.
Table 2. Continued
Variable Location and
population
Period Modality R¼ HDSS
rounds
S ¼ special survey
Update frequency
Social determinants
Occupation Adults in both HDSS 2000 - on-going R Once per year
Education All 6þ in both HDSS 2000 - on-going R Once per year
Household wealth Households in both
HDSS
2000 - on-going R Once per year
Gender attitudes Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Social group membership Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Social capital Adults 15þ in part of
IU-HDSS
2014/5 S Once every 2 years
Religion and ethnic group Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Health seeking
HIV testing history Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
NCD testing history Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Mother’s ANC attendance Newborns in both
HDSS
2000 - on-going R 3x per year till 7/13
2x per year from 7/13
Place and mode of delivery Newborns in both
HDSS
2000 - on-going R 3 per year till 7/13
2 per year from 7/13
Skilled assistance at delivery Newborns in both
HDSS
2000 - on-going R 3 per year till 7/13
2 per year from 7/13
Health outcomes
Height/length, weight and MUAC U5 in both HDSS 2010 S Once
History of fever, diarrhoea, respiratory
problems in past 2 weeks
U5 in both HDSS 2011 – on-going R 3 per year till 7/13
2 per year from 7/13
Blood pressure Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
Blood glucose Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
HIV status Adults 15þ in part of
IU-HDSS
2012/3 and 2014/5 S Once every 2 years
MNCH, maternal, neonatal and child health; STI, sexually transmitted infection; KAP, knowledge, attitudes and practices; WC, waist circumference; HC, hip
circumference; MUAC, mid upper arm circumference; ANC, antenatal clinic; 15þ, aged 15 years and over (¼ ‘adult’); 6þ, aged 6 years and over; U5, aged under
5 years.
International Journal of Epidemiology, 2015, Vol. 44, No. 3 855
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
What has been measured and how are HDSSdatabases constructed?
Interviewers collect information on core HDSS data that
identify households and individuals, spousal relationships,
maternal and paternal parenthood and observe pregnancy,
birth, death and migration events, using standard
INDEPTH definitions and procedures.6
Physicians code cause of death (COD) as based on
standardized INDEPTH Network verbal autopsy (VA)
forms version 2007, using the 10th revision of the
International Classification of Diseases. A wide range of
other information on household characteristics, disease-
specific risk factors, social determinants, health-seeking
behaviours and health outcomes has been collected in all
or parts of the DSS population, be it as part of routine
HDSS rounds or in special surveys (Table 2). In the
IR-HDSS, VA interviews only started in 2000.
We actively engage the community through key inform-
ants and ‘balozi’: local leaders of typically between 10 and
50 houses. Findings are fed back to the community
through these channels and in newsletters. Specific com-
munity sensitization events are held at the time of introduc-
ing new studies.
As from 1 July 2013, data collection and storage in the
IHDSS have been using the open-source OpenHDS system.7
Data are collected through tablets incorporating real-time
validity checks and uploaded to the database server daily,
which improves quality, timeliness and efficiency of data
collection. Though part of the HDSS is very remote, all field
interviewers are able to charge their tablets and upload
data, be it sometimes in creative ways (Figure 4).
Key findings and publications
The decline in under-five mortality in IR-HDSS was 51%
between 2000 and 2012, but was almost negligible in IU-
HDSS. Adult mortality declines were also higher in IR-
HDSS (19%) than IU-HDSS (14%). Neonatal mortality
has remained relatively stable over time in both sites.8
These changes have resulted in mortality rates that are
now higher in IU-HDSS than IR-HDSS and a life expect-
ancy at birth that is higher for the rural population than
for inhabitants of Ifakara town (Table 3). With a sustained
total fertility rate (TFR) of 4.4, no clear evidence of demo-
graphic transition is evident yet in IR-HDSS, but a much
lower TFR of 3.0 is observed in IU-HDSS.
Malaria
It is plausible that the dramatic decrease in child mortality
nationally between 1999 and 2010 can be attributed in
large part to a series of malaria prevention and health
systems interventions developed and scaled up in the past
one and a half-decade.9 IHI researchers and collaborators
in the KINET project showed that locally contextualized
social marketing of insecticide-treated bed nets was associ-
ated with a 27% increase in survival in children aged 1
month to 4 years.10 This was achieved because the pro-
gramme dramatically increased net ownership and
improved equity of ownership.11
In other studies related to the KINET project, we
showed that treated nets had a protective efficacy of 62%
and 63% for parasitaemia and anaemia, respectively,
among children under 2 years of age.12 Among pregnant
women, protective efficacy was 23% for parasitaemia and
38% for severe anaemia, respectively.13 We demonstrated
that discount vouchers are a feasible approach to target
subsidies for bed nets.14 The KINET studies informed the
design of the Tanzania National Voucher Scheme, the
scale-up and effect of which IHI and partners are now
monitoring and evaluating.15
Ifakara HDSS has also been used for evaluating new
diagnostics, treatment regimens and delivery strategies as
they are rolled out nationally. Between 1997 and 2009,
child mortality decreased by 42.5% in the Ifakara rural
DSS. The increase in mosquito net coverage, the switch to
sulfadoxine-pyrimethamine (SP) as first line treatment, the
introduction of Integrated Management of Childhood
Illnesses (IMCI) and the start of a social marketing cam-
paign and drug distribution through Accredited Drug
Dispensing Outlets in private pharmacies16 all contributed
to this decline.17 Despite higher rates of adequate clinical
and parasitological response under artemisinin combination
therapy (ACT) compared with SP,18 the effect of introduc-
tion of ACT on the child mortality trend was minimal.18
Possibly this is because over 50% of patients do not access
an authorized ACT provider promptly19 and because of
challenges in health system design and governance.20,21
Over-prescription of ACT exists alongside challenges in
timely access. Masanja et al reported though, that the intro-
duction of malaria rapid diagnostic tests for parasitological
confirmation reduced over-prescription of ACT.22
Alongside impact on morbidity and mortality, IHI
researchers have documented the impact of various malaria
interventions on vector behaviour and malaria transmission.
The introduction of ACT in the Tanzanian health system
only modestly decreased prevalence of asexual parasit-
aemia23 and did not influence the overall infectiousness of
the human population.24 High usage of insecticide-treated
bed nets (ITNs) leads to greatly reduced indoor transmission
and a relatively larger proportion of residual transmission
happening outdoors.25 Both indicate that additional control
tools are needed to eliminate malaria.
856 International Journal of Epidemiology, 2015, Vol. 44, No. 3
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
Maternal, neonatal and child health
Tanzania’s maternal mortality ratio and neonatal mortality
rate remain high.26 Women with mistimed or unwanted
pregnancies initiate antenatal care later, thereby denying
themselves access to early detection and management of
potential pregnancy complications.27 We showed that in
the period 2005–07, i.e. before quality improvement
programmes started, delivery in health facilities was not
associated with better neonatal survival.28 Met need for
comprehensive emergency obstetric care (CEmOC) is
unacceptably low, especially in remote areas, against a
background of severe shortage of physicians. IHI’s
EMPOWER project showed that non-physician health
workers can effectively deliver CEmOC and anaesthesia
in remote health centres, when trained by a competence-
based in-service course.29 EMPOWER also demonstrated
that distribution of misoprostol (a uterotonic drug)
to expectant mothers for use after home delivery is a
Figure 4. HDSS field interviewer climbing up a palm tree to access network to upload data.
Table 3. Demographic characteristics of the Ifakara HDSS, 2012
Ifakara Rural HDSS Ifakara Urban HDSS
General Fertility Rate (GFR) 142.1 95.1
Total Fertility Rate (TFR) 4.4 3.0
Neonatal mortality rate per 1000 live births 22.7a 34.0
Infant mortality rate per 1000 live births 43.4a 63.4
Child mortality rate per 1000 live births 24.7a 27.0
Under-five mortality rate per 1000 live births 66.6a 88.7
Adult mortality rate (15–59 years) 243.0 260.5
Life expectancy, males 63.4 60.1
Life expectancy, females 69.0 65.4
GFR: number of live births per 1000 person-years of women of reproductive age (15–49); TFR, projected total number of births by end of a woman’s childbear-
ing period at current age-specific fertility rates.a2011 estimate.
International Journal of Epidemiology, 2015, Vol. 44, No. 3 857
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H
ygiene & Tropical Medicine user on 12 June 2020
feasible, safe, effective and acceptable way to protect
against life-threatening post-partum haemorrhage.30
Early studies of child mortality demonstrated that most
of the children had sought treatment at a health facility
during their fatal illness episode.31 This suggested that
interventions to improve case management, such as IMCI,
might be beneficial. In subsequent studies in collaboration
with the Rufiji HDSS, we showed that the introduction of
IMCI led to improvement in child health that was good
value for money and did not occur at the expense of
equity.32,33 IMCI was implemented as national policy in
2004 and IHI researchers and partners continue to investi-
gate the barriers to scale-up34 and best support strategies
for implementation.35
Chronic diseases
In Tanzania, as in many other African countries, NCDs are
increasing as a result of demographic and epidemiological
transitions. We documented that whereas HIV and malaria
were the two most common causes of death among adults,
NCD deaths increased from 16% to 24% of all adult
deaths in the IR-HDSS between 2003 and 2007. Contrary
to popular belief, adults with lower education had higher
hazard of dying from an NCD. Cerebrovascular disease
and epilepsy were among the more common NCD-related
causes of deaths.36 The SEEDS study showed that
IR-HDSS had the highest prevalence of active convulsive
epilepsy among five sites in subSaharan Africa (SSA) at
14.8 [95% confidence interval (CI): 13.8–15.4] per 1000
population screened. Population attributable fractions
indicated that interruption of transmission of parasitic
disease and improved antenatal and perinatal care would
prevent the majority of adult-onset epilepsy and half of
childhood-onset disease.37
The Innovative Care for Chronic Conditions framework
of the World Health Organization (WHO)38 calls for a pre-
pared, motivated and informed triad of patients with fam-
ily members, community partners and health care teams
who interact in an environment supported by a health sys-
tem linked to the community in a positive policy environ-
ment. For infectious chronic diseases, a few studies in the
IHDSS addressed elements of this framework. Community-
based directly observed treatment (DOT) for tuberculosis
was shown to be acceptable and to produce patient out-
comes as good facility-based DOT.39 Conditional cash
transfers used to incentivize safer sexual practices may be
an appropriate tool in prevention of HIV and other sexu-
ally transmitted infections.40 The current public policy,
health system and community actions against NCDs are
still far from adequate, though, to prevent and control the
rapidly rising burden of NCDs in our population.41
As is the case for many communicable diseases, demo-
graphic disparities exist in burden of disease and suffering.
In the 2007, the WHO-INDEPTH-SAGE study on health
status and quality of life among people of 50 years and
over, men, married people and the younger age categories
in IR-HDSS reported better quality of life and health status
than did women, single people and older age groups.42
Lower reported health status was most strongly associated
with the domains of pain and reduced mobility, whereas
the domains of interpersonal relations and level of self-care
affected health status the least.43 This is possibly a reflec-
tion of the fact that the vast majority of older people in IR-
HDSS live in extended families, and illustrates that social
capital alone, without sufficient access to diagnosis and
care for chronic health problems, is not sufficient to ensure
a healthy old age.
Neglected tropical diseases
Rift Valley Fever (RVF) is a zoonotic disease formerly
believed to occur mainly in epidemics triggered by unusu-
ally high rainfall. Recently, we demonstrated existence of
constant inter-epidemic exposure to RVF virus in both ani-
mals44 and humans45 in the Kilombero Valley. Research
on rabies in the IHDSS demonstrated that whereas most
patients live below the poverty line, an average patient
would need to spend more than US $100 to complete rec-
ommended post-exposure prophylaxis. This high cost,
coupled with stock-outs and diagnostic delays, led to
increased risk of death.46 A national mass dog vaccination
campaign against rabies had low coverage in the study
area and operational research suggested that mass inter-
ventions for neglected diseases need to better involve the
community and take into account project organization and
delivery capacity.47
All publications from the Ifakara HDSS and the wider
Tanzanian health research community can be accessed
through [http://digitallibrary.ihi.or.tz].
Future analysis plans
In the short term we will do a comparative analysis of
patterns and drivers of fertility trends in the past decade,
with the Rufiji HDSS. We are developing a mathematical
model for projection of mortality due to febrile illness. We
also plan to quantify and qualify the effects of NCDs on
fertility and birth outcomes. We will characterize
HIV-NCD comorbidity patterns and mortality impacts and
will analyse health-seeking trajectories for fatal chronic
disease. Risk factor analysis will focus on the social deter-
minants of sexual and lifestyle behaviour and consequent
health outcomes. We welcome collaborations on these and
other not yet identified secondary analyses.
858 International Journal of Epidemiology, 2015, Vol. 44, No. 3
Dow
nloaded from https://academ
ic.oup.com/ije/article-abstract/44/3/848/632298 by London School of H