18
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | tsion-woldetinsae |
| View: | 56 times |
| Download: | 0 times |

HYPERTENSION
OUTLINE
ETIOLOGIES
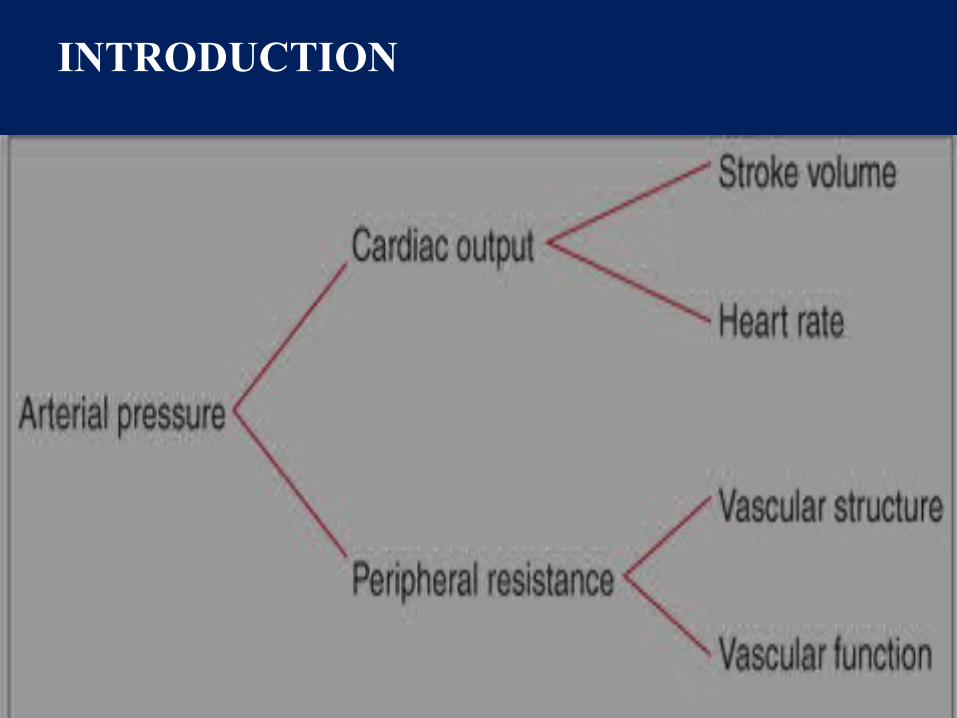
INTRODUCTION
• Cardiac output and peripheral resistance are the two determinants of arterial pressure
ETIOLOGIC CLASSIFICATION OF
HYPERTENSION
• PRIMARY
• SECONDARY

PRIMARY HYPERTESION
80–95% of hypertensive patients are diagnosed as having "essential" hypertension
It tends to be familial.It is the consequence of an interaction between
environmental and genetic factors.Its prevalence increase with age and individual with
high blood pressure at younger age are at increased risk for subsequent development of HTN.
It is likely that essential hypertension represents a spectrum of disorders with different underlying pathophysiologies.
PRIMARY HYPERTESION
Risk factorsIt tends to be both more common & more severe in
blacks Hypertension in maternal, paternal or both parents Excess sodium intakePhysical inactivityExcess alcohol intake Obesity and weight gainsmoking
SECONDARY HYPERTENSION
It occurs secondary to specific underlying disease. 5–20% of hypertensive patients
CAUSES
−Renal paranchymal disease−Renovascular hypertension−Adrenal•Primary aldosteronism•Cushing’s syndrome•Pheochromocytoma
RENAL HYPERTINSION • RENAL PARENCHYMAL DISEASE
Renal disease is the most common cause of secondary hypertension.Hypertension is present in >80% of patients with chronic renal
failure. In general, hypertension is more severe in glomerular diseases than in interstitial diseases such as chronic pyelonephritis.
• RENOVASCULAR HYPERTENSION• Hypertension due to an occlusive lesion of a renal artery,
renovascular hypertension, is a potentially curable form of hypertension
• Two groups of patients are at risk for this disorder:Older aterosclerotic patients andpatients wz fibromuscular dysplasia
Atherosclerosis acounts for the large majority of patients with renovascular HTN.
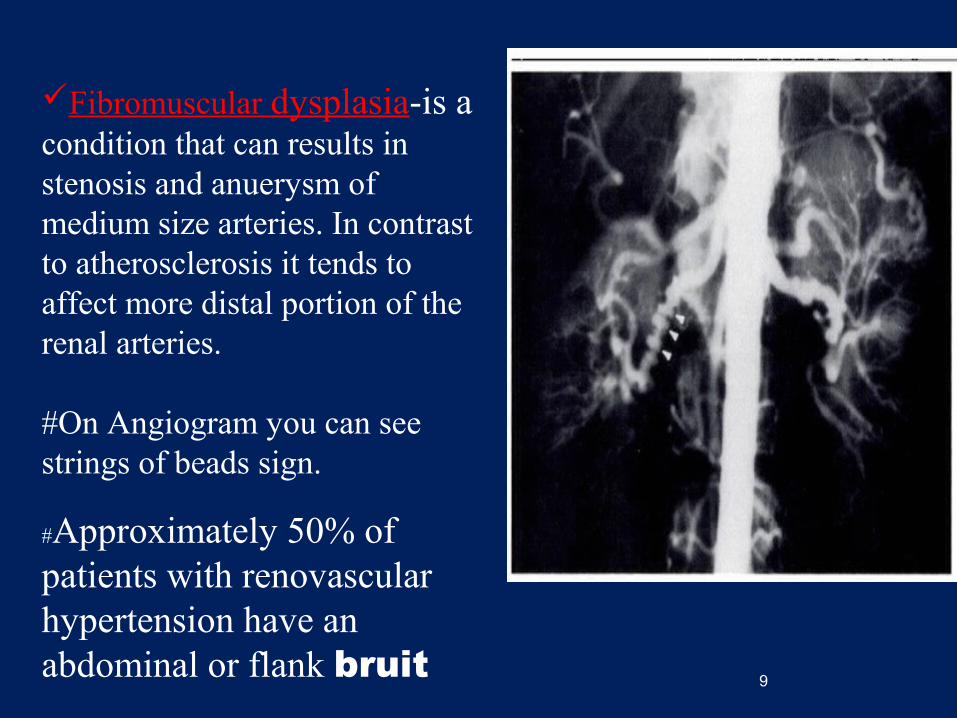
Fibromuscular dysplasia-is a condition that can results in stenosis and anuerysm of medium size arteries. In contrast to atherosclerosis it tends to affect more distal portion of the renal arteries.
#On Angiogram you can see strings of beads sign.
#Approximately 50% of patients with renovascular hypertension have an abdominal or flank bruit
9

PRIMARY ALDOSTERONISM• Also known as conn’s syndrome or primary
hyperaldosteronism
• It is an excessive production of the hormone aldosterone.
• In patients with primary aldosteronism, increased aldosterone production is independent of the renin-angiotensin system, and the consequences are
sodium retention,
hypertension,
hypokalemia, and low PRA Hypertension in these patients may be associated with
glucose intolerance.

PRIMARY ALDOSTERONISM
• Most patients are asymptomatic but may have polyuria, polydypsia, parasthesia or muscle weakness as a consequence of hypokalemic alkalosis.
• The ratio of plasma aldosterone to plasma renin activity (PA/PRA) is a useful screening test.
• 60–70% of patients have an aldosterone-producing adrenal adenoma and most of the remainders have bilateral adrenocortical hyperplasia.
•
CHUSHING SYNDROME
• related to excess cortisol production due either to excess ACTH secretion or to ACTH-independent adrenal production of cortisol.
• Hypertension occurs in 75–80% of patients with Cushing's syndrome.
• Appropriate therapy depends on the etiology.
PHEOCHROMOCYTOMA
• Catecholamine-secreting tumors are located in the adrenal medulla (pheochromocytoma) or in extra-adrenal paraganglion tissue (paraganglioma)
• account for hypertension in ~0.05% of patients.
• Approximately 20% of pheochromocytomas are familial with autosomal dominant inheritance.
• Surgical excision is the definitive treatment of pheochromocytoma and results in cure in ~90% of patients.
OBESITY AND THE METABOLIC SYNDROME
• The constellation of insulin resistance, abdominal obesity, hypertension, and dyslipidemia has been designated as the metabolic syndrome
• There is a well-documented association between obesity (body mass index >30 kg/m2) and hypertension.
• It has been established that 60–70% of hypertension in adults may be directly attributable to adiposity.
• Hypertension and dyslipidemia frequently occur together and in association with resistance to insulin-stimulated glucose uptake.

MISCELLANEOUS CAUSES OF HYPERTENSION
• Hypertension due to obstructive sleep apnea is being recognized with increasing frequency
• Independent of obesity, hypertension occurs in >50% of individuals with obstructive sleep apnea.
• Hypertension related to obstructive sleep apnea also should be considered in patients with drug-resistant hypertension and patients with a history of snoring.

Coarctation of the aorta the most common congenital cardiovascular cause of
hypertension The incidence is 1–8 per 1000 live births. Even when the anatomic lesion is surgically corrected
in infancy, up to 30% of patients develop subsequent hypertension and are at risk of accelerated coronary artery disease and cerebrovascular events.
Several additional endocrine disorders, including thyroid diseases and acromegaly, cause hypertension.
References• Harrison 18th edition• Up-to-date


















