en :z 2 g} " ." 0 • "10(.,,, un II Ie! quebuorl-fTldrK ICOflb \U UlbfJlay nell) 29 Ll 92 025 03605 Q l "he Inff)rmatlon provided will enoblo you to file a fTlorc complete r-etllrn .:\I:d I ,,,duCt; tile Li "II:;! IRS will neon to contact you, OMS No 1545-0047 Form -99b-EZ Short Form Return of Organization Exempt From Income Tax Under section 501 (c), 527, or 4947(a)(1) of the Internal Revenue Code (except private foundations) I ' : Open to Public Do not enter social security numbers on this form, as it may be made public. Department of the Treasury Internal Revenue Service Go to www.irs.govIForm990EZ for instructions and the latest information. Inspection i" I , A For the 2019 calendar year, or tax year beginning ,2019, and ending ,20 B Check If apphcable C Name of organization Ii D Employer Identification number Ii o Add, ass change Challenged Athletes Playing Equally (C.A.P.E.) _ 20-380861 1- LJ Name change Number and street (or P a box If mall IS not delivered to street address) Ii I Room/SUite E Telephone number o Initial retum 2120 Dothan Dr, 615-238-7372 o Final retum/tennlnated City or town, state or prOVince, country, and ZIP or foreign postal code 01; o Amended return F Group Exemption o App!lcatlon pending Murfreesboro, TN 37128 , Number a G Accounting Method: o Cash o Accrual Other (specify) H Cheek 0 If the organization IS not I reqUired to attach Schedule 8 B .1 Tax-exempt status (check only one) - 0 501 (c)(3) o 501 (c) ( ) .. (Insert no) 0 494 7{a)(1) or 0527 (Form 990, 990-EZ, or 990-PF). K Form of organization 0 Corporation 0 Trust 0 ASSOCiation 0 Other L Add hnes 5b, 6c, and 7b to hne 9 to determine gross receipts. If gross receipts are $200,000 or more, or If total assets (Part II, column (8)) are $500,000 or more, file Form 990 of Form _ $ "Hln Revenue,"Expenses, and Chan'ge$ in Net' Assets or Fund· Baiances (see the instructions for Part I) IBI II) CI> II) t: CI> c. >< w . II) ... CI> II) IJl <t Check If the or anization used Schedule 0 to res and to any question in thiS Part I 0 1 2 3 Contributions, gifts, grants, and Similar amounts received. Program service revenue including government fees and contracts Membership dues and assessments . 4 Investment Income 5a Gross amount from sale of assets other than Inventory b Less: cost or other baSIS and sales expenses . c Gain or (loss) from sale of assets other than inventory (subtract line 6 Gaming and fundralsing events: • ., a Gross Income from gaming (attach Schedule. G If $15,000) . . b Gross Income from fundralstng events (not I,:"cluding from fundralslng events reported on line 1) (attach Schedule G If the sum of such gross Income and contributions exceeds $15,000) . 15720 c Less: direct expenses from gaming and fundraising events 3833 9097 d Net income or (loss) from gaming and fundralslng events (add lines 6a and 6b and subtract line 6c) 7a b c a 9 10 11 12 13 14 15 16 17 i8 19 Gross sales of Inventory, less returns and allowances , Less: cost of goods sold 6d 11887 Gross profit or (loss) from sales of Inventory (subtract line 7b from line 7a) 1--7_c-+- ______ _ Other revenue (describe In Schedule 0) . _______ _ Total revenue. 2, 3, 4, 5c, 6d, 7e, and 8 9 20984 9875 Grants and similar amounts paid (list In Sch6dule 0) r-:- • ..:.,O-+-______ _ Benefits paid to or for members . r-:-1..:..1-+-______ _ Salaries, other compensation, and employee benefits II 12 ProfeSSional fees and other payments to Independent contractors II _______ _ Occupancy, rent, utilities, and maintenance 1--'1....:4-+ _______ ::-:- Printing, publications, postage, and shiPPing j-:.1=.5+-_______ 66_ Other expenses (describe in Schedule 0) lEI ______ 1_5_5_44_ Total expenses. Add lines 10 throu h 16 , 17 25485 Excess or (deficit) for the year (subtract line 17 from line 9) _____ -,(,--45_0_1.:.) Net assets or fund balances at beginning of year (from line ,27, column (A)) (must agree With end-of-year figure reported on prior year's return) 19 4501 -a; 120 z. 21 Other changes In net assets or fund balances (explain 111 Schedule 0) , _______ _ Net assets or fund balances at end of ear. Combine lines 18 throu h 20 21 o For Paperwork Reduction Act Notice, see the separate instructions. Cat No 106421 Fonm 990-EZ (2019) I I
Transcript
en ~ :z 2 g}
" ." 0
• "10(.,,, un II Ie! quebuorl-fTldrK ICOflb \U UlbfJlay nell) WIII(1GW~. 29 Ll 92 025 03605 Q l "he Inff)rmatlon provided will enoblo you to file a fTlorc complete r-etllrn .:\I:d I ,,,duCt; tile Li IdIILl:J~ "II:;! IRS will neon to contact you,
OMS No 1545-0047
Form -99b-EZ Short Form
Return of Organization Exempt From Income Tax ~(Q)19 Under section 501 (c), 527, or 4947(a)(1) of the Internal Revenue Code (except private foundations)
I ' : Open to Public
~ Do not enter social security numbers on this form, as it may be made public. Department of the Treasury Internal Revenue Service ~ Go to www.irs.govIForm990EZ for instructions and the latest information.
Inspection i" I ,
A For the 2019 calendar year, or tax year beginning ,2019, and ending ,20 B Check If apphcable C Name of organization Ii D Employer Identification number Ii o Add, ass change Challenged Athletes Playing Equally (C.A.P.E.) _ 20-380861 1-LJ Name change Number and street (or P a box If mall IS not delivered to street address) Ii I Room/SUite E Telephone number o Initial retum 2120 Dothan Dr, 615-238-7372 o Final retum/tennlnated
City or town, state or prOVince, country, and ZIP or foreign postal code 01; o Amended return F Group Exemption
o App!lcatlon pending Murfreesboro, TN 37128 ,
Number ~ a G Accounting Method: o Cash o Accrual Other (specify) ~ H Cheek ~ 0 If the organization IS not I Website:~ reqUired to attach Schedule 8 B .1 Tax-exempt status (check only one) - 0 501 (c)(3) o 501 (c) ( ) .. (Insert no) 0 494 7{a)(1) or 0527 (Form 990, 990-EZ, or 990-PF).
K Form of organization 0 Corporation 0 Trust 0 ASSOCiation 0 Other L Add hnes 5b, 6c, and 7b to hne 9 to determine gross receipts. If gross receipts are $200,000 or more, or If total assets (Part II, column (8)) are $500,000 or more, file Form 990 In~tead of Form ~90-EZ _ ~ $
"Hln Revenue,"Expenses, and Chan'ge$ in Net' Assets or Fund· Baiances (see the instructions for Part I) IBI
II) CI> II)
t: CI> c. >< w .
II) ... CI> II) IJl <t
Check If the or anization used Schedule 0 to res and to any question in thiS Part I 0
1
2 3
Contributions, gifts, grants, and Similar amounts received.
Program service revenue including government fees and contracts
Membership dues and assessments .
4 Investment Income
5a Gross amount from sale of assets other than Inventory
b Less: cost or other baSIS and sales expenses .
c Gain or (loss) from sale of assets other than inventory (subtract line 6 Gaming and fundralsing events: • .,
a Gross Income from gaming (attach Schedule. G If $15,000) . .
b Gross Income from fundralstng events (not I,:"cluding ~$:---:-:---:::--:c-:-:--",,""~ from fundralslng events reported on line 1) (attach Schedule G If the sum of such gross Income and contributions exceeds $15,000) . 15720
c Less: direct expenses from gaming and fundraising events 3833
9097
d Net income or (loss) from gaming and fundralslng events (add lines 6a and 6b and subtract line 6c)
7a
b c
a 9
10
11
12
13
14
15
16
17 i8 19
Gross sales of Inventory, less returns and allowances ,
Less: cost of goods sold
6d 11887
Gross profit or (loss) from sales of Inventory (subtract line 7b from line 7a) 1--7_c-+-______ _ Other revenue (describe In Schedule 0) . 1---'8~ _______ _
Total revenue. A_<!d..!!!!~~1, 2, 3, 4, 5c, 6d, 7e, and 8 ~ 9 20984
9875
Grants and similar amounts paid (list In Sch6dule 0) r-:-• ..:.,O-+-______ _
Benefits paid to or for members . r-:-1..:..1-+-______ _
Salaries, other compensation, and employee benefits II 12 r-:-~--------
ProfeSSional fees and other payments to Independent contractors II r-:-13~ _______ _
Occupancy, rent, utilities, and maintenance 1--'1....:4-+ _______ ::-:-
Printing, publications, postage, and shiPPing j-:.1=.5+-_______ 66_
Other expenses (describe in Schedule 0) lEI r-:-16~ ______ 1_5_5_44_
Total expenses. Add lines 10 throu h 16 , ~ 17 25485
Excess or (deficit) for the year (subtract line 17 from line 9) r-:-18~ _____ -,(,--45_0_1.:.) Net assets or fund balances at beginning of year (from line ,27, column (A)) (must agree With end-of-year figure reported on prior year's return) 19 4501
-a; 120 z. 21
r-:-~--------Other changes In net assets or fund balances (explain 111 Schedule 0) , ~2..:..0-+-_______ _
Net assets or fund balances at end of ear. Combine lines 18 throu h 20 ~ 21 o For Paperwork Reduction Act Notice, see the separate instructions. Cat No 106421 Fonm 990-EZ (2019)
I
I
Form 990-EZ (2019)
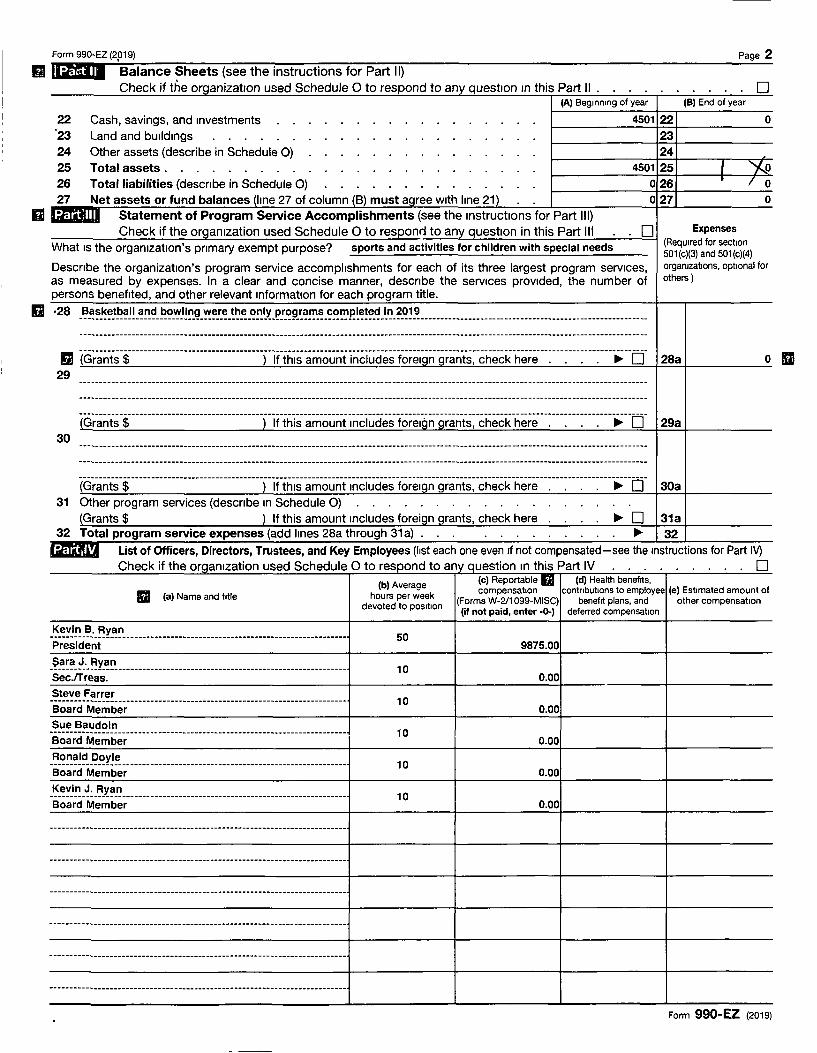
n 10111 'Balance Sheets (see the instructions for Part II) Page 2
Check if the organization used Schedule 0 to respond to any question In this Part II IA) Beginning of year (8) End of year
22 '23 24 25
Cash, savings, and Investments Land and bUildings Other assets (describe in Schedule 0) Total assets.
26 Total liabilities (descnbe in Schedule 0) 27 Net assets or fund balances (line 27 of column (B) must agree With line 21)
II l:F.TiiillliD Statement of Program Service Accomplishments (see the Instructions for Part III) Check if the organization used Schedule 0 to responn to any question in this Part III
4501 22
23 24
4501 25 , 026 • 027
o Expenses
(ReqUired for section
o o
I 0
o
What IS the organization's pnmary exempt purpose? sports and activities for children with special needs
Descnbe the organization's program service accomplishments for each of its three largest program services, as measured by expenses. In a clear and concise manner, descnbe the services proVided, the number of persons benefited, and other relevant information for each program title.
501 (c)(3) and 501 (c)(4) organizations, optional for others )
g (G~a~-ts-$----------------------------------)-if-th~san;o~ntinciuciesf~~elgn-g~a~-ts~-che~k-he~e--------------------.;--[r 28a o III 29
30
31 Other program services (descnbe In Schedule 0) (Grants $ ) If this amount Includes foreign grants, check here ~ 0 31a
32 Total program service expenses (add lines 28a through 31 a) ~ 32 l::F.TiilU'. List of Officers, Directors, Trustees, and Key Employees (list each one even If not compensated-see the Instructions for Part IV)
Check if the organization used Schedule 0 to respond to any question In this Part IV 0 Ib) A Ie) Reportable U Id) Health benefrts,
If!'II verage compensation contributions to employee Ie) Estimated amount of l1li (a) Name and title hours per week
devoted to position (Forms W-2J1099-MISC) benefit plans, and other compensation (if not paid, enter -()..) deferred compensation
Steve Farrer ----------.. _--------------------- ... ----------------------------------------Board Member
10
Sue Baudoin Board Member
10 0.00
_'='_~~~~~_E~¥~!: _______________________________________________________ _ Board Member
10 0.00
_~_-:~!~_~:_'='.x~_~ ______________________________________ _________________ _ Board Member
10 0.00
Form 990-EZ (2019)
--- -- ------------------- --- --------
Form 990-EZ (2019)
~I "Other Information (Note the Schedule A and personal benefit contract statement requirements In the
Page 3
instructions for Part V. Check if the used Schedule a to to in this Part V
33 Did the organization engage in any significant activity not previously reported to the IRS? If "Yes," provide a detailed description of each activity in Schedule a .. ....... ...... 33
~ 34 Were any significant changes made to the organizing or governing documents? If "Yes," attach a conformed copy of the amended documents If they reflect a change to the organization's name. Otherwise, explain the change on Schedule O. See instructions ................... 34 t/
35a Old the organlz~tlon have unrelated bUSiness gross income of $1,000 or more dUring the year from bUSiness 1-----11-----1r---
activities (such as those reported on lines 2, 6a, and 7a, among others)?. ....... .
b If "Yes" to line 35a, has the organization filed a Form 990-T for the year? If "No," provide an explanation In Schedule 0 c Was the organization a section 501 (c)(4), 501 (c)(5), or 501 (c)(6) organization subject to section 6033(e) notice,
reporting, and proxy tax requirements during the year? If "Yes," complete Schedule C, Part III. . . . .
36 Old the organization undergo a liqUidation, dissolution, termination, or significant dispOSition of net assets during the year? If "Yes," complete applicable parts of Schedule N . . . .
37a Enter amount of political expenditures, direct or indirect, as described In the instructions ~ 1..!3~7~a~ _____ ~:.l.::...:....\ .... :..::....q~~ b Old the organization file Form 1120-POL for thiS year? . . . . .
38a Old the organization borrow from, or make any loans to, any officer, director, trustee, or key employee; or were any such loans made In a prior year and stili outstanding at the end of the tax year covered by thiS return?
b If "Yes," complete Schedule L, Part II, and enter the total amount Involved 1--'3c-:8;.,::b;,t-_____ " 39 Section 501 (c)(7) organizations. Enter:
a Initiation fees and capital contributions Included on line 9 . . . . . b Gross receipts, included on line 9, for public use of club faCilities
.40a Section 501 (c)(3) organizations. Enter amount of tax Imposed on the organization dUring the year under: section 4911 !» ; section 4912 I> ; section 4955 ~ -------
b S~ctlon 501 (c)(3), 501 (c)(4), and 501 (c)(29) organizations. Old the organization engage In any section 4958 eXGess benefit transaction during the year, or did It engage in an excess benefit transaction In a prior year th~t has not been reported on any of ItS prior Forms 990 or 990-EZ? If "Yes," complete Schedule L, Part I
c SeCtion 501 (c)(3), 501 (c)(4), and 501 (c)(29) organizations. Enter amount of tax imposed ~o[1jorganlzation managers or disqualified persons during the year under sections 4912, 4955, and 4958. . . . . . . . . . . . . . . . . ~ 0.00
d S~Rtlon 501 (c)(3), 501 (c)(4), and 501 (c)(29) organizations. Enter amount of tax on line 40.(; reimbursed by the organization .. ........ . ~ 0.00
,CJ I\lIforganizatlonc. I\t any timo dUring tho tax yoar, wac the organization a party to a prohibited tax chelter transaction? If "Yes," complete Form 8886-T . . . . . . . . . . . . .
41 List the states with which a copy of this return is filed ~ Tennessee ---------------------------42a The organization's books are In care of'" _~_':~j.!!_~.x~_~____________________________________________ Telephone no. ,.. _______ ~~~:~~~:!_~!_~ _____ _
Located at ,.. 2120 Dothan Dr, Murfreesboro TN ZIP + 4 ~ 37128 b I\t any time durlrig-the-caien(jar-yeiij.~-dld-ttle-orgi;riizatlon-have-an-interestiri-or-ZislgrintLire or other Guthorlty Qvcr----------r--.---
a financial account In a foreign country (such as a bank account, securities account, or other finanCial account)?
If "Yes," enter the name of the foreign country ~ See the instructions for exceptions and filing requirements for FInCEN Form 114, Report of Foreign Bank and Financial Accounts (FBAR).
o I\t any time dUring the calendar year, did the organization maintOin an office outcide the United Statec? If "Yes," enter the name of the foreign country ~
.43 Section 4947(a}(1) nonexempt charitable trusts filing Form 990-EZ In lieu of Form 1041-Check here and enter the amount of tax-exempt interest received or accrued during the tax year. . . '.' ~ '----'43~'--_ ___r-___r--
, 44a Old the organization maintain any donor advised funds dUring the year? If "Yes," Form 990 must be
completed Instead of Form 990-EZ . . . . . . . . . . . . . . .
b Old the organization operate ono or more hoepltal faCIlities dUring the year? If "Yee," Form D90 muet be completed instead of Form 990-EZ . . . . . . . . . . . . . .
c Did the organization receive any payments for Indoor tanning services dUring the year? . . . . . d If "Yes" to line 44c, has the organization filed a Form 720 to report these payments? If "No," provide an
explanation In Schedule a . . . . . . . . . . . . . . . . . . 45a Old the organization have a controlled entity within the meaning of section 512(b)(13)? . . . . . .
b Did the organization reoelva any payment from or engage In any transaction With a controllod ontity within the meaning of section 512(b)(13)? If "Yes," Form 990 and Schedule R may need to be completed Instead of Form 990-EZ. See instructions. . . . . . . . . . . . . . . . .
Yes No
Form 990-IEZ (2019)
Form 990-EZ (2019) Page 4
46
.~ .
47
·48
Yes No Did the organization engage, directly or indirectly, in political campaign activities on behalf of or In opposition ,.-~ :tt!'4 to candidates for public office? If "Yes," complete Schedule C, Part I . . . . . . . . . . . ., I 46 II' II
Section 501 (c)(3) Organizations Only All section 501 (c)(3) organizations must answer questions 47-49b and 52, and complete the tables for lines
50 and 51. Ch k'f h ec I t e organization use dShdlO C e u e to respon d h' P to a~ question In t IS art VI D
Yes No Did the organization engage in lobbying activities or have a section 501 (h) election In effect dunng the tax year? If "Yes," complete Schedule C, Part II 47 II' Is the organization a school as described In section 170(b)(1)(A)(II)? If "Yes," complete Schedule E 48 II'
400 Did the organization make any trancferc to an exempt non-ch::mtable related organization? 49a II' b If "Yes," was the related organization a section 527 organization? 4gb
50 Complete this table for the organization's five highest compensated employees (other than officers, directors, trustees, and key employees) who each received more than $100,000 of compensation from the organization. If there IS none, enter "None."
(a) Name and title of each employee (b) Average
hours per week devoted to position
(d) Health benefits, (e) Reportable contributions to employee (e) Estimated amount of compensallon
(Forms W-2/1 099-MISC) benefit plans, and deferred other compensation compensallon
f Total number of other employees paid over $100,000 ..... 0,00 . ~---------------
51 Complete this table for the organization's five highest compensated Independent contractors who each received more than $100,000 of compensation from the organization. If there IS none, enter "None."
(a) Name and bUSiness address of each Independent contractor (b) Type of service (e) Compensation
d Total number of other Independent contractors each receiving over $100,000
52 Did the organization complete Schedule A? Note: All section 501 (c)(3) completed Schedule A
.... 0.00 .~----------------------------
organizations must attach a .~0 Yes D No
Under penalties of perJury, I declare that I have_~x~lned thiS return, Including accompanying schedules and statements, and to the best of my knowledge and behef, It IS true, correct, and complete ~on SJ} prep?," (other than officer) IS based on all Information of which preparer has any knowledge
~ ~--?/..:> I /-"/ --?~~ Sign Here WI
r SI9mltl1'1'0T OTTl~ Date
l\ Kevin B. Ryan, President ,. Type OT pnnt name and title
Paid Pnnt/Type preparer's name Ipreparer's signature I Date I Check D If I PTIN Preparer ~ __________________________ ~ __________________________ ~ ______ -. __ ~~s_e_'~_e_m_p_'o~ye_d~II ____________ _
I Phore no Firm's address ~ May the IRS diSCUSS this return with the preparer shown above? See instructions ~ DYes D No
Form 990-EZ (2019)
SCHEDULE A (Form 990 or 990-EZ)
~ublic Charity Status and Public Support Complete If the organization is a section 501 (c)(3) organization or a section 4947(a)(1) nonexempt charitable trust
~ Attach to Form 99tJ or Form 990-EZ.
OMS No 1545-0047
~@19 Department of the Treasury Internal Revenue Service ~ Go to www.irs.govIForm990 for instructions and the latest information. I
Open to public , Inspection'
Name of the organization Employer identification number Challenged Athletes Playing Equally (C.A.P.E) 20-3808612
Reason for Public Charity Status (All organizations must complete this part.) See instructions. Tho org:mizatlon in not a pnvate foundation becauso It 13: (For linc::; 1 through 12, check only one box.)
1 o A church, convention of churches, or association of churches descnbed In section 170(b)(1)(A)(i). 2 0 A school descnbed In section 170(b)(1)(A)(ii). {Attach Schedule E (Form 990 or 990-EZ).) 3 0 A hospital or a cooperative hospital service organization described In section 170(b)(1)(A)(iii). 4 0 A medical research organization operated In conjunction With a hospital described In section 170(b)(1)(A)(iii). Enter the
hospital's name, City, and state:
5 0 An organization operated for the-benE;fit-of"i;-coile~je--or-unliiersity-ownE;d-or-operate(n;y-a--governrrientai"lin-li"describeci-i-ri section 170(b)(1)(A)(iv). (Complete Part 11.)
6 0 A federal, state, or local government or governmental unit descnbed In section 170(b)(1)(A)(v). 7 0 An organization that normally receives a substantial part of ItS support from a governmental Unit or from the general public
described In section 170(b)(1)(A)(vi). (Complete Part 11.)
8 0 A community trust descnbed In section 170(b)(1)(A}(vi). (Complete Part 11.)
9 0 An agricultural research organization described In section 170(b)(1)(A)(ix) operated In conjunction with a land-grant college or university or a non-land-grant college of agriculture (see instructions). Enter the name, City, and state of the college or univerSity:
10 0 An organ Izafion"tliaf-rioriTiciTry-re-ceTveis:TiY-moreUiari-3"31i31Vo-ofIts-sui:'-pornrom-confr1l5uffons~-iTiem1iersliipTees~-~iricrgyoss---receipts from activities related to its exempt functions-subject to certain exceptions, and (2) no more than 33'/3% of its support from gross Investment income and unrelated business taxable income (less section 511 tax) from businesses acquired by the organization after June 30, 1975. See sectiun 509(a)(2). (Complete Part 111.)
11 o An organization organized and operated exclUSively to test for publiC safety. See section 509(a)(4).
12 0 An organization organized and operated exclUSively for the benefit of, to perform the functions of, or to cany out the purposes of one or more publicly supported organizations descnbed in section 509(a)(1) or section 509(a)(2). See section 509(a)(3).
(A)
tB)
(C)
(D)
(E)
a Check the box In lines 12a through 12d that descnbes the type of supporting organization and complete lines 12e, 12f, and 12g. :;:
o Type I. A supporting organization operated, supervised, or controlled by ItS supported organlzation{s), typically by giving the supported organlzation{s) the power to regularly appoint or elect a majority of the directors or trustees of the
, supporting organization. You must complete Part IV, Sections A and B.
b G Type II. A supporting organization supervised or controlled In connection With ItS supported organlzatlon{s), by having control or management of the supporting organization vested in the same persons that control or manage the supported organizatlon{s) You must complete Part IV, Sections A and C.
c 0 Type III functionally integrated. A supporting organization operated In connection with, and functionally Integrated with, ItS supported organlzation{s) (see instructions). You must complete Part IV, Sections A, D, and E.
d 0 Type III non-functionally integrated. A supporting organization operated In connection With ItS supported organlzatlon{s) that IS not functionally Integrated. The organization generally must satisfy a distribution reqUirement and an attentiveness requirement (see Instructions). You must complete Part IV, Sections A and D, and Part V.
e 0 Check thiS box If the organization received a wntten determination from the IRS that It IS a Type I, Type II, Type III functionally integrated, or Type III non-functtonally Integrated supporting organization.
f Enter the number of supported organizations . . g Provldo tho follOWing Information about the nupportod organlzatlon{::;).
(i) Name of supported organization (ii) EIN (ill) Type of organization Ov) Is the organization (v) Amount of monetary (vi) Amount of (deSCribed on lines 1-10 listed In your governing support (see other support (see above (see Instructions)) document? instructions) instructions)
Yes No
Total IRHt3JH--~'VNi t4' ~iit b1 !U'f; :,f. : ~" ' j:l " ! ' > ! L~ For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 99O-EZ. Cat No 11285F Schedule A (Form 990 or 99O-EZ) 2019
I·
~ .
- -------------
Schedule A (Form 990 or 990-EZ) 2019 ' > ,Page 2 ~~ Support Schedule for Orgilniziltions Described in Sections 170(b)(1)(A)(iv) arid 170(b)(1)(A)(vi)
. (Complete only if you checked the box on line 5, 7, or 8 of Part I or if the ,organization failed to qualify un Part III. If the anization fails to under the tests IIsted'below lete Part III
Calendar year (or fiscal year beginning in) .. 1-~,-=:..:..:'-+-....!;:e<...::~'::--+---'-::L.:.::":::"';~-I----''-=!..='':''''::''---1r-''>'':;'<-==:'':'':;--!r---''''-'-:''="'---1 GiftS, grants, contributions, and
membership fees received.' (Do not include ~ny "unusual grants.")'. .
2 Tax revenues levied for the organization's benefit and either paid to or expended on ItS behalf
3 The value of services or facilities furnished by a governmental unit to the organization without charge. .
4 Total. Add lines 1 through 3. .
5 The portion of total contribution's by each person (other than a governmental Unit or publicly supported organization) Included on hne 1 that exceeds 2% of the amount shown on line 11, column (f). .
6 Public
Calendar year (or fiscal year beginning in) .. I-~,-=:..:..:'-+-....!;:e<...::~'::--+--+::L.:.::":::"';~-I----''-=!..='':''''::''-:-lr-,,>,,:;,<-==:,,:,,:;-+-....>;;!,-,-:,,=",---
.
7 Amounts from line 4
8 Gross Income from Interest, diVidends, payments received on seCUrities loans, rents; royalties, and income from Similar sources . '. . . . . .
9
10
11 12 13
14 15 16a
b
17a
Net income from un'related business activities, whether or not the business is regularly carned on
Other' Income. Do not Include gain or . los~ :trom the sale of capital assets (Explain In Part VI.). .
~ Total support. Add hnes 7 through 10 Gross receipts from related activities, etc. lFir,st five years. If the Form 990 IS for the org organization, check thiS box and stop here
on's 'first, second, third, fourth, or fift~ tax'year as a section 501 (c)(3) . . . . . . . . ~
umn (f) divided by hne 11 , column (f)) v"I""'UIU'C A, Part II, hne 14 .'. . . . . l'L"'7",t',nn did not check the box 01'1 line 13, ar:ld line 1.1 Is'331/3% or more, check thiS
ifles as a publicly supported organization . . .. ....... D r.frr,,,,n,i7,,,tin,n qid not check a box on line 13 or 16a, and hne 15 IS 331/3% or more, check
a!il'izat:ion qualifies as a pubhcly supported organization . . . . . . ~ D 10%-facts-and-circlJmsumc:e.s test-2019. If the organization did not check a box on hne 13, 16a, or 16b, and line 14 is 10% or more, and If the nrn,,,,nI17,,,1r,nn meets the "facts-and-circumstances" test,' check this box and stop here. Explain In Part VI how the organ meets the "facts-and-clrcumstances" test. The organization qualifies as a publicly supported organization. . .' . . . " ........... ~ D
b 1 ""d.",n,.","", test-2018. If the organization did not check a box on hne 13, 16a, 16b, or Ha, and line 15 is 10% or more, If the organization meets the "facts-and-clrcumstances" test, check this box and stop here. Explain In Part VI organization meets the "facts-and-clrcumstances" test. The organization qualifies as a publicly supported . . . . . . . . . . ." ~ D
18 If the organization did not check a box on line 13, 16a, 16b, 17 a, or 17b, check thiS box and see
Schedule A (Fonn 990 or 990-EZ) 2019
-....
Schedule A (Form 990 or ~90-EZ) 2019 Page 3
~I Support Schedule for Organizations Described ;n Section 509(a)(2) (Complete only If you checked the box on line 10 of Part I or if the organization failed to qualify under Part II. If the organization fails to qualif;t under the tests listed below, elease complete Part 11.)
Section A. Public Support Calendar year (or fiscal year beginning in) ~ • 1 Gifts, grants, contnbutions, and membership fees
received. (Do not Include any "unusual grants.'1 2 Gross receipts from admissions. merchandise
sold or services performed. or facilities furnished In any activity that IS related to the organization's tax-exempt purpose .
3 Gross receipts from activities that are not an unrelated trade or business under section 513
4 Tax revenues levied for the organlzatlon's benefit and either paid to or expended on its behalf
5 The value of services or facilities furnished by a governmental unit to the organization without charge .
6 Total. Add lines 1 through 5 . 7a Amounts Included on lines 1, 2, and 3
received from disqualified persons
b Amounts included on lines 2 and 3 received from other than disqualified persons that exceed the greater of $5,000 or 1 % of the am~unt on line 13 for the year
'.~. 8 Public support. (Subtract line 7c from {. • line 6.). Ii. 128213 ~ .. ' '~~Section B. TotarSupport
* ..... .. ' '. , ,
.Calendar year (Of fiscal year beginning in) ~ (a) 2015 (b) 2016 (c) 2017 (d) 2018 (e) 2019 (f) Total 9 Amounts fr9rTI line 6 38572 36068 32589 n/a 20984 128213
i0a Gross Incom'lffrom Interest, diVidends, payments rec,elved on securities loans. rents. royalties. and)ncome from Similar sources.
• b Unrelated bUSiness taxable Income (less section 511 taxes) from businesses acquired after June 30, 1975 .
c Add lines 10a and 10b 11 Net income from unrelated bUSiness
activities not Included in line 10b. whether or not the bUSiness IS regularly carned on
12 Other Incom,e. Do not include gain or loss from the sale of capital assets (Explain In Part VI.) .
13 Total support. (Add lines 9, 10c. 11. and 12.) 38572 36068 32589 n/a 20984 128213
14 First five years. If the Form 990 IS for the organlzatlon's first, second. third. fourth. or fifth tax year as a section 501 (c)(3) organization. check thiS box and stop here . . . . . ~ D
Section C. ComputOltion of Public Support Percentage 15 Public support percentage for 2019 (line 8. column (f). diVided by line 13, column (f)) 100 % 16 Public support percentage from 2018 Schedule A. Part III. line 15 100 %
Section D. Computation of Investment Income Percentage 17 Investment Income percentage for 2019 (line 10c. column (f), divided by line 13, column (f)) . % 18 Investment Income percentage from 2018 Schedule A. Part III, line 17. . . , , , , , % 19a 331/3% support tests-2019. If the organization did not check the box on line 14, and line 15 IS more than 331/3%. and line
17 is not more than 331/3%, check thiS box and stop here. The organization qualifies as a publicly supported organization " ~ 0 b 331/3% support tests-2018. If the organization did not check a box on line 14 or line 19a. and line 16 IS more than 331/3%, and
line 18 IS not more than 331/3%. check this box and stop here. The organization qualifies as a publicly supported organization 'I> 0 20 Private foundation. If the organization did not check a box on line 14. 19a, or 19b. check this box and see Instructions '~D
Schedule A (Fonn 990 or 990-EZ) 2019
Schedule A (Form 990 or 990-EZ) 2019 pag'e 4 ~ Supporting Organiza~ions I •
. (Complete only if you checked a box In line 12 on Part I. If you checked 12a of Part I, complete Sections A and B. If you checked 12b of Part I, complete Sections A and C. If you checked 12c of Part I, complete
.'
Sections and E. If checked 12d of Part com Sections Aand D 'and lete Part V
1 Are all of the organization's supported -organizations listed by name In the organization's governing documents? If "No," describe In Part VI how the supported organizations are des/g,!ated. If designated by class or purpose, describe the deSignation. If historic and continuing relationship, explain.
2 Old the organization have any supported organization that does not have ~n IRS determination of status under section 509(a)(1) or (2)? If "Yes," explain in Part VI how the organization determined that the supported organization was descflbed In seCtion 509(a)(1) or (2).
3a Old the organization have a supported organization descnbed in: section 501 (c)(4), (5), or (6)? If "Yes," answer (b) and (c) below. -
b Old the organization confirm that each supported organization qualified under section 501 (c)(4), (5), or (6) and satisfied the public support tests under section 509(a)(2)? If "Yes," descnbe In Part VI when and how the organization made the determination. .
C Old the organization ensure that all support to such organizations was used exclUSively for section 170(c)(2)(8) p,urposes? If "Yes, ",explain in"Part VI what contr~/s rhE! organization put ~:? place to ensure such use.
4a Was any supported organization not organized In the United States ("foreign supported organization")? If "Yes," and If you checked 12a or 12b In Part I, answer (b) and (c) below.
b Old the organization have ultimate control and discretion In deciding whether to make grants to the foreign supported organization? If "Yes," describe In Part VI how the organization had such control and discretion despite being controlled or supervised by or In connection with its supported organizations. •
-, .. - C Old the organization support any foreign supported organization that does not have an IRS determination
,.
;\ under sec~lons 501 (c)(3) and 569(a)(1) or (2)? ~f "Yes," explain In Part VI what controls the organization used to ensure;that al/ support to the foreign supported organization was used exclusively for section 170(c)(2)(8) . ".... . 1'" I
purposes. .
;, Sa - Old the organization add, substitute, or remove any supported organizations dunng the tax year?" If "Yes," answer (b) and (c) below (if applicable). Also, prOVide detail In Part VI, Including'(i) the names and EIN numbers (2,f the supported organizations added, substituted, or r~moved; (II) the reasons for each such action; (ill) the QutlJ,oflty under the organizatIOn's organizing document authoriZing such action; and (IV) how thl? action waa accofTlPIi::;hcd (such aa by amendment to tho organizing document).
b Type', or..« Type II only. Was any added or substituted supporteq organization part of a class deSignated In the organization's organlzuilg document? .
C Substitutio'ns only. Was the'substltution the result of an event beyond the orgarllzatlon's control? -6 Old t~e organization provide support (whether in the form of grants or the provIsion of services or facilities) to
anyone other than (I) ItS supported organizations, (II) IndiViduals that are part of the chantable cldss benefited by one 'or more of ItS supported organizations, or (Iii) other supporting organizations that also support or benefit one or more of the filing organization's supported organizations? If "Yes, II prOVide detail m Part VI.
7 Old the organization prOVide a grant, loan, compensation, or other Similar payment to a substantial contnbutor (as defined In section 4958(c)(3)(C)), a family member of a substantial contnbutor, or a 35% controlled entity With regard to _a sUbstantial contributor? If "Yes, II complete Part I of Schedule i.. (Form 990 or 990-EZ).
8 Old the organization make a loan to a disqualified-person (as defined in section 4958) not deSCribed In line 7? If "Yes, " complete Part I of Schedule L (Form 990 or 990-EZ). . •
9a Was the ~rganl~~tlon controlled directly or indirectly at any tlm'e dUring the tax year by one or more disqualified persons as defined In section 4946 (other than foun'dation managers and organizations deSCribed in section 509(a)(1) or (2))? If "Yes, II prOVide detail In Part VI.
b Old one or more disqualified persons (as defined in line,9a) hold a controlling interest 10 any entity in which the supporting organization had an Interest? If "Yes, II prOVide detail In Part VI. .
C Did a disqualified person (as defined in line 9a) have an ownership Interest In, or derive any personal benefit from, assets In which the supporting organization also had an Interest? If "Yes, .. provide detail In Part VI • .
'10a Was the organization subject to the excess bUSiness holdings rules of section 4943 because of section 4943(f) (regarding certain Type II supporting organlzatlon~, and all Type III non-functionally Integrated supporting organizations)? If "Yes, II answer 10b below. • .
b Did the organization have any excess business holdings In the tax' year? (Use Schedule C, For,!, 4720, to determine whether the organization had excess busmess holdings.)
S~hedule A (Form 990 or 990-EZ) 20~
'" " ,~ .,
. ,~~,
!~
;:'
j'
'. ,~"
~,t"'}
"'~ . . " ,y'
l: r
Schedule A (Form 990 or 990-Ell 2019
Supporting Organizations (continued)
11 Has the organization accepted a gift or contribution from any of the following persons? a 'A person who directly or Indirectly controls, either alone or together with persons described In (b) and (c)
below, the governing body of a supported organization?
b A family member of a person described in (a) above? c A 35% controlled enti of a erson described In a or b above? If "Yes" to a, b, or c, rovlde detail In Part VI.
Section B. anizations
1 Old the directors, trustees, or membership of one or more supported organizations have the power to regularly appoint or elect at least a majority of the organization's directors or tr!-lstees at all times dUring the tax year? If "No, " describe in Part VI how the supported organization(s) effectively operated, supervised, or controlled the organization's activities. If the organization had more than one supported organization, describe how the powers to appoint and/or remove directors or trustees were allocated among th"e supported organizations and what conditions or restrictIOns, If any, applied to such powers dUring the tax year
2 Old the organization operate for the benefit of any supported organization other than the supported organlzation(s) that operated, supervised, or controlled the supporting organization? If "Yes," explain in Part VI how providing such benefit camed out the purposes of the supported organlzatlon(s) that operated, supervised,' or controlled the supporting organization '
1 Were a majority of the organization's directors or trustees during the tax year also a majority of the directors or trustees of each of the organization's supported organization(s)? If "No," describe In Part VI how control or management of the supporting organization was vested in the same persons that control/ed 01 managed the supported organizatlOn(s).
1
2
3
Old the Qrganization provide to each of Its supported organizations, by the last day of the fifth month of the organization's tax year, (i) a written notice descnblng the type and amount of support provided during 'the pnor tax
; year, (Ii)'a, copy of the Form 990 that was most recently filed as of the date of notification, and (ill) copies of the organlza~I,on's governing documents In effect on the' date of notification, to the extent not previously provided?
Were any;of the organization's officers, directors, or trustees either (i) apPointed or elected by the supported organrza!lon(s) or (II) serving on the governing body of a supported organization? If "No, " explam In Part VI how the organization maintained a close and continuous working relationship with the supported organlzation(s).
By reacon of the relatlonchlp described In (2), did the organizatlOn'c cupported organizatlonc have a significant vOice in the organization's Investment poliCies and In directing the use of the organization's income or assets at all times dunng the tax year? If "Yes," descnbe In Part VI the role the organization's supported organizations played In this regard.
E. Type III Functionilily Integrated Supporting Orgilnizations
PageS
1 Check the box next to the method that the organization used to satisfy the Integral Part Test dunng the year (se~ instructions)
.
a b c
2 a
o The organization satisfied the Activities Test. Complete line 2 below. o The or,ganlzation IS the parent of each of ItS s,upported organizations. Complete line 3 below. o The organrzatlon supported a governmental entity. Describe in Part VI hqw you supported a government entity (see
Activities Test. Answer (a) and (b) below. '
Did substantially all of the organrzatlon's activities during the tax year directly further the exempt purposes of the supported organrzatlon(c) to which the organization waG rosponGlve? If "Yoa, " then in Part Vf. identify those supported organizations and explain how these activities directly furthered their exempt purposes, how the orgamzatlon was responsive to those supported orgamzatlons, and how the organization determined that these activities constituted substantially all of its actIVIties.
b Old the activities descnbed In (a) constitute activities that, but for the organization's involvement, 6ne or more of the organization's supported organlzation(s) would have been engaged In? If "Yes," explain In Part VI the roasons for tho orgamz:Jtion '$ poaltlon that ita aupportod org:Jniz:Jtlon(a) would havo ongaged In those actiVities but for the organization's involvement.
3 Parent of Supported Organizations. Answer (a) and (b) below. ~ Did the organization have the power to regularly appoint or elect a maJonty of the offlcerG, dlroctorG, or
trustees of each of the supported organizations? Provide details In Part VI •
. b Old the organization exercise a substantial degree of direction over the poliCies, programs, and actiVities of each of ItS ? If " descnbe In Part VI the role the In thiS
Schedule A (Fonn 990 or 990-EZ) 2019
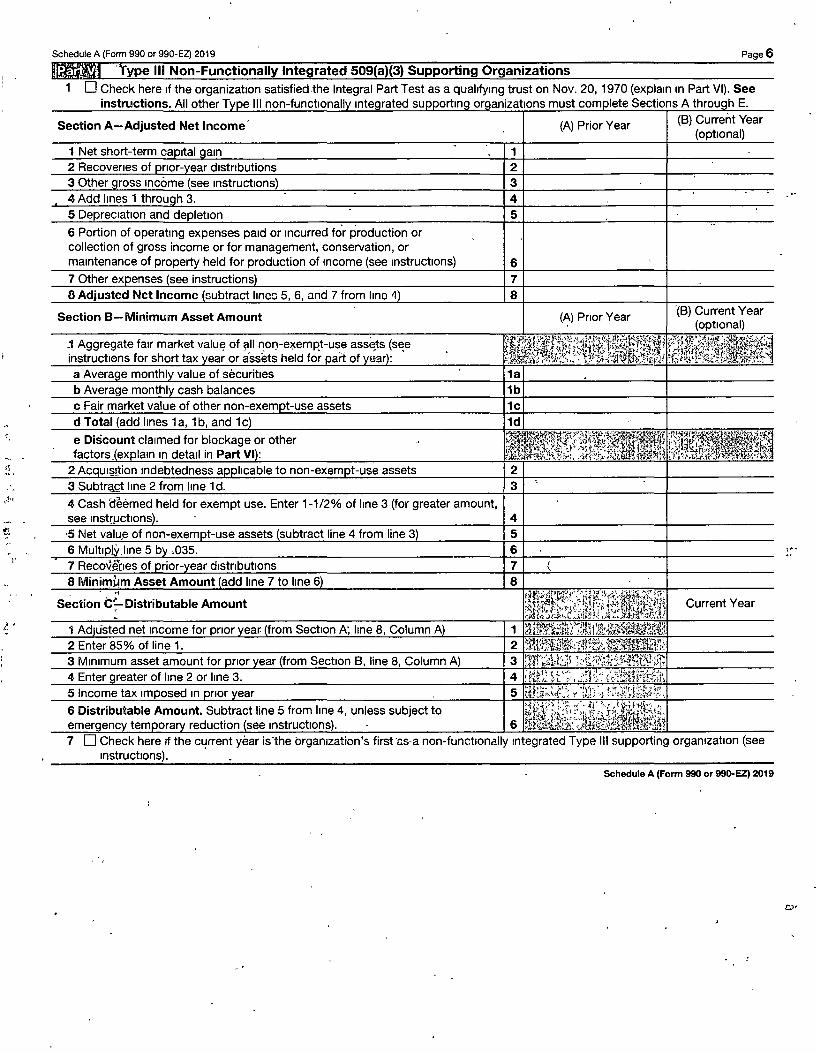
Schedule A (Form 990 or 990-EZ) 2019 Page 6 ~~J 'Type III Non-Functionally Integrated 509(a)(3) Supporting Organizations
1 0 Check here If the organization satisfied the Integral Part Test as a qualifying trust on Nov. 20, 1970 (explain In Part VI). See "."',ULI,L;lIU .. ,... All other T III non-functl rated must com Sections A E.
Section A-Adjusted Net Income' (8)
6 Portion of operating expenses paid or Incurred fo'r production or collection of gross income or for management, conservation, or maintenance of held for production of Income {see Instructl
Section 8-Minimum Asset Amount
,~" 4 Cash aeemed held for exempt use. Enter 1-1/2% of line 3 (for greater amount,
.. "
Current Year
6 Distributable Amount. Subtract line 5 from line 4, unless subject to reduction Instruction
Check here If the current year is·the brganlzatron's first'<~s·a non-functionally Integrated Type III supporting organization (see Instructions). .
Schedule A (Form 990 or ggD-EZ) 2019
, , . ..
Schedule A (Form 990 or 990-EZ) 2019
Section D-Distributions
Section E-Distribution Allocations (see instructions)
Remaining underdlstnbutlons for years pnor to 2019, if any. Subtract lines 3g,and 4a frqm line 2. For result
reater than zero, lain in Part VI. See Instructions.
6 Remaining underdlstnbutlons for 2019. Subtract-lines 3h and 4b from line '1. For result greater than zero, explain I Part VI. See instructions.
7 Excess distributions carryover to 2020. Add lines 3J and 4c.
, (i) Excess Distributions
(ii) Underdistributions
Pre-2019
Page 7
Current Year
(iii) Distributable
Amount for 2019
Schedule A (Fonn 990 or 99O-EZ) 2019
Schedule A (Form 990 or 990-EZ) 2019 Page 8 Supplemental Information. Provide the explanations required by Part II, line 10; Part II, line 17a or 17b; Part III, line 12; Part IV, Section A, lines 1, 2, 3b, 3c, 4b, 4c, 5a, 6~ 9a, 9b, 9c, 11 a, 11 b, and 11 c; Part IV, Section B, lines 1 and 2; Part IV, Section C, line 1; Part IV, Section D, lines 2 and 3; Part IV, Section E, Imes 1 c, 2a, 2b, 3a, and 3b; Part V, line 1; Part V, Section B, line 1 e; Part V, Section D, lines 5, 6, and 8; and Part V, Section E, lines 2, 5, and 6. Also complete this part for ~ny additional information. (See Instructions.)
















![I WIII MMWWWW| · United States Patent [19] Leeet al. I USOOS6 WIII MMWWWW| 33793A [11] Patent Number: 5,633,793 [45] Date ofPatent: May27, 1997 [54] SOFTSWIICHEDTHREE-PHASEBOOST](https://static.documents.pub/doc/80x56/5f08172e7e708231d42049b6/i-wiii-mmwwww-united-states-patent-19-leeet-al-i-usoos6-wiii-mmwwww-33793a.jpg)










