24
Immunohistochemistry Dr. Rikin Hasnani
| Date post: | 21-Jan-2018 |
| Category: |
Healthcare |
| Upload: | rikin-hasnani |
| View: | 367 times |
| Download: | 0 times |
Immunohistochemistry Dr. Rikin Hasnani
Introduction
• Definition : Immunohistochemistry (IHC) refers to the process of detecting antigens (e.g. proteins) in cells of a tissue section by exploiting the principle of antibodies binding specifically to antigens in biological tissues.
• Immunohistochemistry Combines histological, immunological and biochemical techniques for the identification of specific tissue components by means of a specific antigen/antibody reaction tagged with a visible label
• It was invented by Albert Coons in1941.
• It is widely used for diagnosis of cancers because specific tumor antigens are expressed de novo or up-regulated in certain cancers.

Principle
• The principle of immunohistochemistry is the localization of antigens in
tissue sections by the use of labeled antibodies as specific reagents
• Antigen-antibody interactions that are visualized by a marker such as
fluorescent dye, enzyme, radioactive element or colloidal gold.

Procedure
• Sample preparation - tissue collection, fixation and sectioning
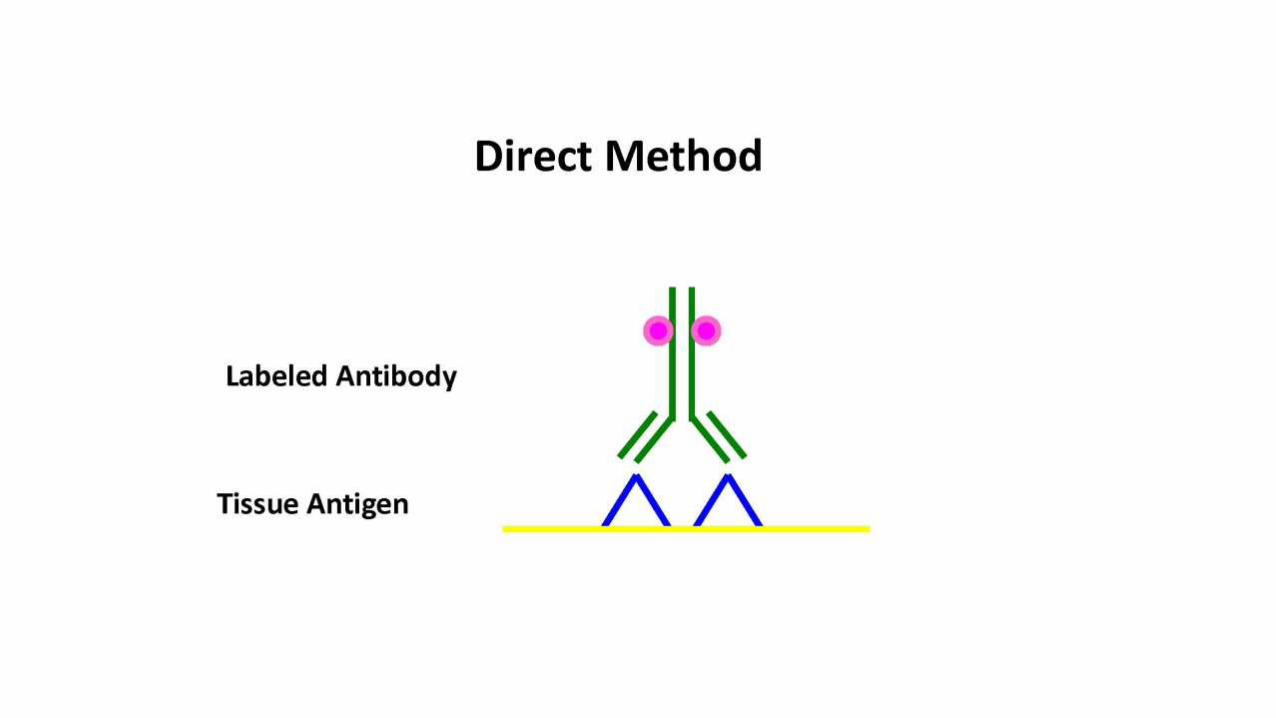
• Sample labelling – direct , indirect, PAP method

Reporter molecule • These are molecules that report the presence or absence of Ag-Ab
reaction.
• It can be chromatogenic or flouroscent.
• With chromogenic reporters, an enzyme label is used that reacts with a substrate to yield an intensely colored product that can be analyzed with an ordinary light microscope.
• Alkaline phosphatase (AP) and horseradish peroxidase (HRP) are the two most commonly used enzymes.
• Fluorescein isothiocyanate (FITC), Rhodamine are commonly used fluoroscent molecules.



Uses of IHC
• The most important are:
• 1) histogenetic diagnosis of morphologically non-differentiated neoplasias
• 2) subtyping of neoplasias (such as lymphomas, for example);
• 3) characterization of primary site of malignant neoplasias;
• 4) prognostic factors and therapeutic indications of some diseases;
• 5) discrimination of benign versus the malignant nature of certain cell proliferations

Histogenetic diagnosis of morphologically non-differentiated neoplasias

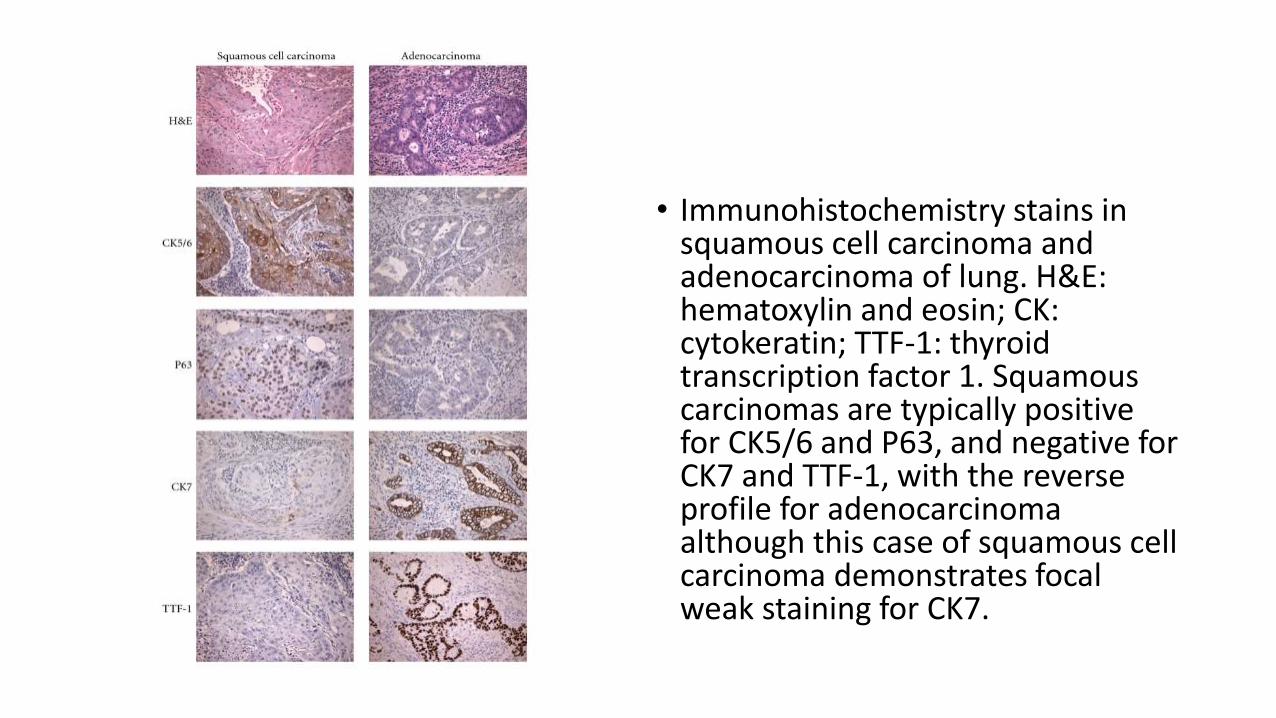
• Immunohistochemistry stains in squamous cell carcinoma and adenocarcinoma of lung. H&E: hematoxylin and eosin; CK: cytokeratin; TTF-1: thyroid transcription factor 1. Squamous carcinomas are typically positive for CK5/6 and P63, and negative for CK7 and TTF-1, with the reverse profile for adenocarcinoma although this case of squamous cell carcinoma demonstrates focal weak staining for CK7.
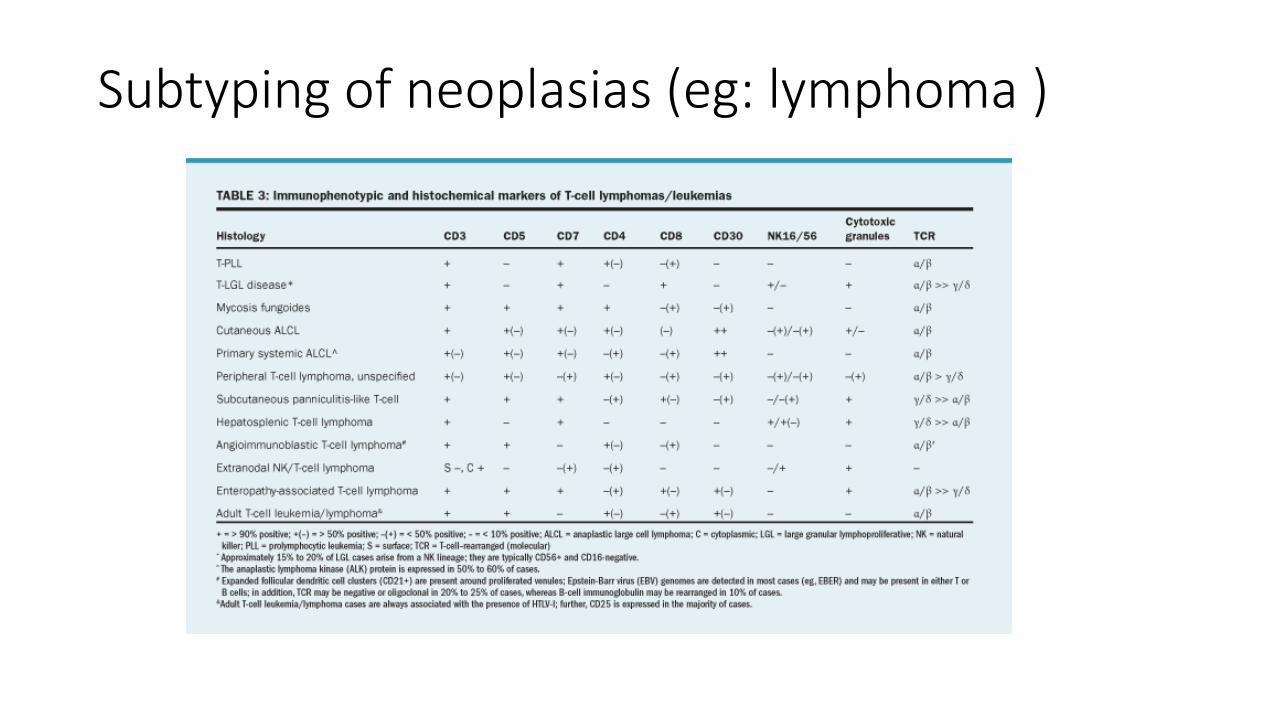
Subtyping of neoplasias (eg: lymphoma )

Characterization of primary site of malignant neoplasias• Metastatic Adenocarcinoma of
unknown originwith site specific markers

Prognostic factors and therapeutic indications of some diseases• 1. Genetic predisposition (e.g., BRCA1/2, p53)
• 2. identification of genes involoved in carcinogenesis (e.g., BCR-ABL TyrosinKinase Inhibitor in CML, HER-2/neu in Breast Ca , RAS in Colo Rectal Cancer)
• 3.Environmental factors and lifestyle (e.g., HPV or HBV infection)

Role of Immunohistochemistry in Lung Cancer
• It is used to confirm the diagnosis of undiagnosed lung cancer
• To prognosticate the disease
• To evaluate the therapeutic potential of targeted therapy


• CK5 is a very sensitive marker for squamous cell carcinoma and also a more specific marker than P63. The combination of CK5 and P63 was not more informative than CK5 alone.
• TTF1 and NAPA are very sensitive markers for adenocarcinoma. • Furthermore, the combination of both markers was even more sensitive. • The sensitivity of TTF1 and NAPA is lower for large-cell carcinomas.• Mucinous adenocarcinomas and poorly differentiated adenocarcinomas
are known to be positive less often as well, although only a limited number of cases have been specifically reported
• Apart from lung cancer, NAPA is mainly positive in renal cell carcinoma and a few cases of thyroid cancer.
• 15% were positive for ER.


• The goals of this study were to evaluate a panel of molecular biologic markers in patients with stage I NSCLC after resection and to develop a prognostic model based on the involvement of these molecular variables, independent of other variables.
• The factor with the strongest independent prognostic value was p53. 52 vs 70
• angiogenesis factor viii was associated with significantly decreased survival.56vs 70
• The presence of the protooncogene erb-b2 was also a strong negative prognostic factor.47 vs 67
• The metastatic adhesion protein CD-44. 54 vs 67
• absence of rb was associated with significantly decreased survival 55 vs 63

• No. of markers positive and 5 years survival
• 0-3 – 76 %
• 4-5 – 62%
• 6-9 – 48%

Targeted Therapy
THANK YOU

















