65
Lecture 11- Mental Disorders Overview 1. Defining Psychopathology 2. Cognitive Disorders Dementia Delirium 3. Other Mental Disorders Depression Anxiety (see text)
| Date post: | 21-Dec-2015 |
| Category: |
Documents |
| View: | 216 times |
| Download: | 1 times |
Lecture 11- Mental DisordersOverview
1. Defining Psychopathology2. Cognitive Disorders
DementiaDelirium
3. Other Mental DisordersDepressionAnxiety (see text)
Lecture 11- Mental DisordersOverview
4. Clinical ConcernsElder AbuseSuicide (see text)
5. Psychological Issues in Long-Term Care
6. Myth Busting: Facts on Aging Revisited

Psychological Disorders in AdulthoodPsychological Disorders in Adulthood
Psychopathology=Science of psychological disorders
Lie outside range of ordinary Lie outside range of ordinary human experiencehuman experienceLie outside range of ordinary Lie outside range of ordinary human experiencehuman experience
•Subjective distressSubjective distress•Impaired in everyday lifeImpaired in everyday life•Cause risk to self or othersCause risk to self or others•Engage in socially or culturally Engage in socially or culturally unacceptable behaviorunacceptable behavior
•Subjective distressSubjective distress•Impaired in everyday lifeImpaired in everyday life•Cause risk to self or othersCause risk to self or others•Engage in socially or culturally Engage in socially or culturally unacceptable behaviorunacceptable behavior

Psychological Disorders in Adulthood:Psychological Disorders in Adulthood:Diagnosis of Psychological DisordersDiagnosis of Psychological Disorders
Diagnostic and Statistical Manual of Diagnostic and Statistical Manual of Mental Diseases (DSM-IV)Mental Diseases (DSM-IV)
•Based on field studies of specific disordersBased on field studies of specific disorders•Not developed specifically for older adultsNot developed specifically for older adults•Based on field studies of specific disordersBased on field studies of specific disorders•Not developed specifically for older adultsNot developed specifically for older adults
Diagnostic processDiagnostic processDiagnostic processDiagnostic process •Match symptoms to those in manualMatch symptoms to those in manual•Must meet specific criteriaMust meet specific criteria•Develop treatment planDevelop treatment plan

Psychological Disorders in Adulthood:Psychological Disorders in Adulthood:Diagnosis of Psychological DisordersDiagnosis of Psychological Disorders
DSM-IV Diagnostic AxesDSM-IV Diagnostic Axes
Axis IAxis I
Axis IIAxis II
Axis IIIAxis III
Axis IVAxis IV
Axis VAxis V
Clinical syndromes or disorders
Personality disorders and mental retardation
Medical conditions
Psychosocial stressors
General level of functioning

TerminologyTerminology
EpidemiologyEpidemiology
•Lifetime prevalenceLifetime prevalence- percentage of people who - percentage of people who ever have had the disorderever have had the disorder•Incidence- Incidence- new cases within given periodnew cases within given period
•Lifetime prevalenceLifetime prevalence- percentage of people who - percentage of people who ever have had the disorderever have had the disorder•Incidence- Incidence- new cases within given periodnew cases within given period

Cognitive Disorders (DSM-IV)Cognitive Disorders (DSM-IV)
1.Dementia
2. Delirium
3. Amnestic Disorder
4.Cognitive Disorder Not Otherwise Specified

Cognitive Disorders: DementiaCognitive Disorders: Dementia
DementiaDementiaDementiaDementia •Clinical condition/syndromeClinical condition/syndrome•Loss of cognitive functionLoss of cognitive function•Interferes with normal activitiesInterferes with normal activities•Interferes with social relationshipsInterferes with social relationships
Common signs
1. Impairment of memory2. Multiple disturbances of cognition3. Impairment of executive function.4. Disorientation.5. Behavioral changes.
Definition of DementiaDefinition of Dementia

Dementia: CausesDementia: Causes
1.Reversible
2. Irreversible

Reversible Dementia (some causes)Reversible Dementia (some causes)
Dementia due to treatable condition:Dementia due to treatable condition:•infectionsinfections•toxic effects of drugs (polypharmacy)toxic effects of drugs (polypharmacy)•normal pressure hydrocephalusnormal pressure hydrocephalus•head injuryhead injury•nutritional deficiencies
Korsakoff’s syndrome (vitamin B1)Wernicke’s disease
•metabolic problems (e.g., hypothyroidism)metabolic problems (e.g., hypothyroidism)•mental and sensory deprivationmental and sensory deprivation•Depression (pseudodementia)*Depression (pseudodementia)*•Delirium*Delirium*
Important to Important to treat earlytreat early
Important to Important to treat earlytreat early
Can become Can become irreversibleirreversible

Irreversible: Irreversible: Neurological Diseases that Neurological Diseases that Can Cause DementiaCan Cause Dementia
DisorderDisorder CauseCause Major symptomsMajor symptoms
Vascular Vascular dementiadementia
Transient ischemic attacks
More rapid decline than AD, decline occurs in spurts
Frontal lobe Frontal lobe dementiadementia
Damage to frontal lobes
Personality changes- apathy, lack of inhibition, obsessiveness, loss of judgment
Parkinson’s Parkinson’s diseasedisease
Lack of dopamine in basal ganglia
Tremors, shuffling gait, postural instability, speech problems
Lewy Body Lewy Body dementiadementia
Accumulation of Lewy bodies
Confusion, hallucinations, motor deficits
HIV dementiaHIV dementia
Accumulation of Pick bodies
Frontal and temporal lobe deterioration, personality changes, loss of speech.
Pick’s Pick’s diseasedisease
Final stages of AIDS Apathy, confusion, concentration problems, flattened emotions
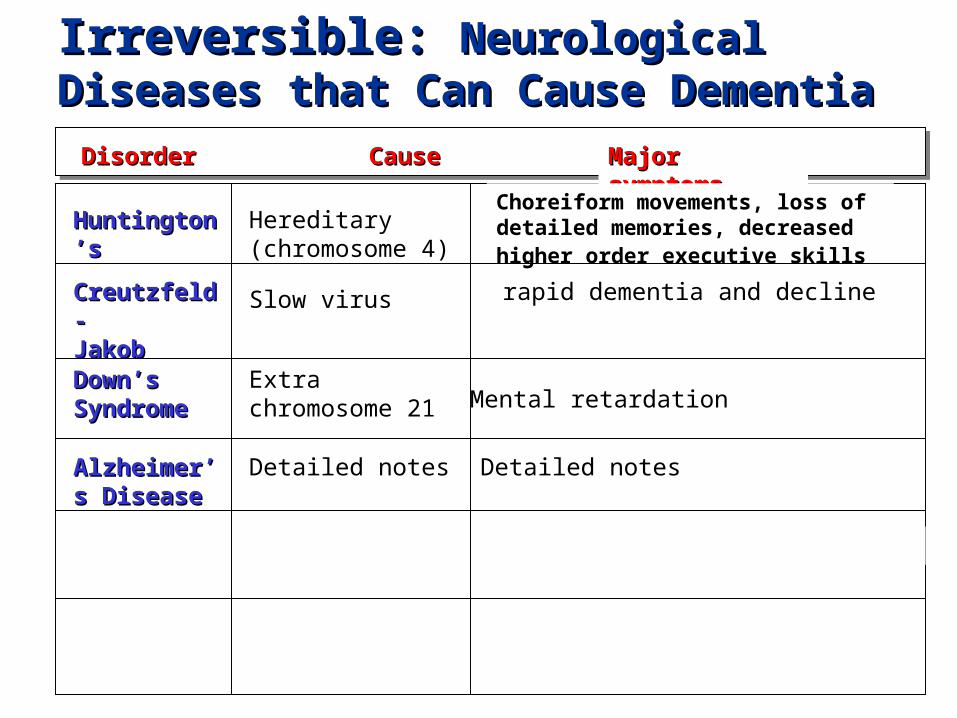
Irreversible: Irreversible: Neurological Diseases that Neurological Diseases that Can Cause DementiaCan Cause Dementia
DisorderDisorder CauseCause Major symptomsMajor symptoms
Huntington’sHuntington’s Hereditary (chromosome 4)
Choreiform movements, loss of detailed memories, decreased higher order executive skills
Creutzfeld-Creutzfeld-JakobJakob
Slow virus rapid dementia and decline
Down’sDown’sSyndromeSyndrome
Extra chromosome 21
Alzheimer’s Alzheimer’s DiseaseDisease
Detailed notes Detailed notes
Mental retardation

Normal Dementia
8% of all Canadians aged 65+ meet 8% of all Canadians aged 65+ meet the criteria for dementia.the criteria for dementia.8% of all Canadians aged 65+ meet 8% of all Canadians aged 65+ meet the criteria for dementia.the criteria for dementia.
Canadian Study of Health and Aging Canadian Study of Health and Aging (1991-1992)(1991-1992)
PrevalencePrevalence
Prevalence of dementia in Canada: Canadian Study of Health and Aging (1991-1992)
• Female to male ratio is 2:1
• 2.4 % for 65-74 years
• 34.5% for those aged 85+
• If prevalence estimates remain constant, 592,000 persons will have dementia by 2021

Prevalence of Alzheimer’s Disease and Vascular Dementia in Canada
• Alzheimer’s 5.1% for 65+– 1.0% for 65-74 years– 26% for 85+ years
• Vascular dementia 1.5% for 65+– 0.6 % for 65-74 years– 4.8 % for 85+ years

FeaturesFeatures
•Associated with damage to the cerebral blood vessels Associated with damage to the cerebral blood vessels through arteriosclerosisthrough arteriosclerosis•found in middle and later life (age of onset between 50-70)found in middle and later life (age of onset between 50-70)•accumulated effect of multiple cortical and subcortical infarctsaccumulated effect of multiple cortical and subcortical infarctslead to clinical presentationlead to clinical presentation•incidence higher in menincidence higher in men•first sign delirium or small strokefirst sign delirium or small stroke
Dementia: Vascular DementiaDementia: Vascular Dementia

Clinical PresentationClinical Presentation
•Abrupt onsetAbrupt onset•step-wise deteriorationstep-wise deterioration•somatic complaintssomatic complaints•emotional incontinenceemotional incontinence•history of hypertensionhistory of hypertension•history of cebrovascular accidentshistory of cebrovascular accidents•focal neurological symptomsfocal neurological symptoms•focal neurological signsfocal neurological signs
Dementia: Vascular DementiaDementia: Vascular Dementia

•Patient Auguste D. had dementia Patient Auguste D. had dementia symptomssymptoms•Brain studies after her death revealed Brain studies after her death revealed microscopic changes microscopic changes
Alois Alzheimer (1864-1915)Alois Alzheimer (1864-1915)
•Symptoms due to neuronal changesSymptoms due to neuronal changes
Dementia:Dementia:Alzheimer’s Disease HistoryAlzheimer’s Disease History

NINCDS/ADRDA GuidlinesNINCDS/ADRDA Guidlines
•DementiaDementia•Significant cognitive deficienciesSignificant cognitive deficiencies•Progressive deteriorationProgressive deterioration•No loss of consciousnessNo loss of consciousness•40-90 years of age40-90 years of age•No other diseasesNo other diseases
Criteria for probable Alzheimer’s diagnosis=Criteria for probable Alzheimer’s diagnosis=
Also includesAlso includes
•Medical testsMedical tests•Family historyFamily history•Brain scansBrain scans•Other symptomsOther symptoms
Dementia and Related Neurological Dementia and Related Neurological Disorders: Disorders: Alzheimer’s DiseaseAlzheimer’s Disease

EarlyEarly
MiddleMiddle
LateLate
Memory loss for familiar Memory loss for familiar objects and eventsobjects and events
Personality changesPersonality changesBehavior changesBehavior changes
Loss of ability to perform simple Loss of ability to perform simple everyday functionseveryday functions
Regular progressionof loss
Alzheimer’s Disease: “Stages” of ProgressionAlzheimer’s Disease: “Stages” of Progression
Psychological SymptomsPsychological Symptoms
People do not die of Alzheimer’s per se.People do not die of Alzheimer’s per se.
Clinical Presentation:Clinical Presentation:
•Memory lossMemory loss•AphasiaAphasia•ApraxiaApraxia•AgnosiaAgnosia•Disturbance in executive functioningDisturbance in executive functioning
Diagnosisdone byexclusion
Diagnosisdone byexclusion
Autopsy is onlyAutopsy is onlyreliable methodreliable method

Clinical Presentation

Amyloid PlaquesAmyloid Plaques
•Collection of waste Collection of waste products of dead neurons products of dead neurons around a core of around a core of amyloid.amyloid.•Formation occurs long Formation occurs long before symptoms are before symptoms are evidentevident
•Amyloid-42 most common form found in plaquesAmyloid-42 most common form found in plaques
Alzheimer’s DiseaseAlzheimer’s Disease
Amyloid plaqueAmyloid plaque

•Beta amyloid fragments eventually Beta amyloid fragments eventually clump together.clump together.
•Proteases snip the APP into fragments.Proteases snip the APP into fragments.
•If APP is snipped at wrong place, If APP is snipped at wrong place, beta amyloid 42 is formed.beta amyloid 42 is formed.
Alzheimer’s DiseaseAlzheimer’s Disease
Formation of amyloid plaquesFormation of amyloid plaques

http://www.ahaf.org/alzdis/about/AmyloidPlaques.htm
Alzheimer’s DiseaseAlzheimer’s Disease
TanglesTangles

Neurofibrillary TanglesNeurofibrillary Tangles
•Made up of tau proteinMade up of tau protein•Tau maintains microtubules Tau maintains microtubules within axonswithin axons•Tangles form when tau Tangles form when tau changes chemically and can changes chemically and can no longer support the no longer support the microtubulesmicrotubules•Leads to collapse of Leads to collapse of transport system within transport system within neuronneuron
Neurofibrillarytangle
Neurofibrillarytangle
Alzheimer’s DiseaseAlzheimer’s Disease

http://www.alzheimers.org/tangle.html
Neurofibrillary TanglesNeurofibrillary Tangles
Alzheimer’s DiseaseAlzheimer’s Disease

ApoE gene 19
APP gene 21
Presenilin 1 14
Presenilin 2 1
GeneGene ChromosomeChromosome
Genetic theoryGenetic theoryGenetic theoryGenetic theoryFamilial Familial Alzheimer’s Alzheimer’s DiseaseDisease
Familial Familial Alzheimer’s Alzheimer’s DiseaseDisease
•Early onsetEarly onset•Late onsetLate onset
supports
Alzheimer’s DiseaseAlzheimer’s Disease
Causes of Alzheimer’s DiseaseCauses of Alzheimer’s Disease

Genetic theoryGenetic theoryGenetic theoryGenetic theoryFamilial Familial Alzheimer’s Alzheimer’s DiseaseDisease
Familial Familial Alzheimer’s Alzheimer’s DiseaseDisease
ApoE gene 19
APP gene 21
PresenilinPresenilin 11 1414
Presenilin 2 1
GeneGene ChromosomeChromosome
•Early onsetEarly onset•Late onsetLate onset
supports
Alzheimer’s DiseaseAlzheimer’s Disease
Causes of Alzheimer’s DiseaseCauses of Alzheimer’s Disease
Majority of early-onset cases
Majority of early-onset cases

EnvironmentalEnvironmental
Life styleLife style Head injury Head injury •Twin dataTwin data•Japanese men who moved Japanese men who moved to Hawaiito Hawaii•Nun Study on mental Nun Study on mental activityactivity
•Severe injuries Severe injuries involving loss of involving loss of consciousnessconsciousness•Causes damage to Causes damage to neuronsneurons
Alzheimer’s DiseaseAlzheimer’s Disease
Causes of Alzheimer’s DiseaseCauses of Alzheimer’s Disease

CategoryCategory
Labazimide
AnticholinesteraseAnticholinesterase
GlutamateGlutamate
enhancersenhancers
ActionAction NameName
Nerve growthNerve growth
factorsfactors
Stimulate
neuron growth
Increases
available
acetylcholine
Tacrine
No trade name
AntioxidantsAntioxidants
Anti-inflammatoryAnti-inflammatory Not known Advil
HRTHRT Not known Estrogen
Facilitate
glutamate
SeligilineStop free radicals
Treatment: Alzheimer’s DiseaseTreatment: Alzheimer’s Disease

Psychosocial TreatmentsPsychosocial Treatments
•PersonPerson
•Prompts, cues, and guidancePrompts, cues, and guidance•ModelingModeling•Positive reinforcementPositive reinforcement•Structure daily activitiesStructure daily activities•modifications to environmentmodifications to environment
•caregivercaregiver•Respite careRespite care•Provide educationProvide education
•info on the disease progressioninfo on the disease progression•communication strategiescommunication strategies•support groupssupport groups
Caregiver Caregiver burdenburden
Alzheimer’s Disease: Care for Person and Alzheimer’s Disease: Care for Person and CaregiverCaregiver

Lecture 11- Mental DisordersOverview
1. Defining Psychopathology2. Cognitive Disorders
DementiaDelirium
3. Other Mental DisordersDepressionAnxiety (see text)

DefinitionDefinition
•Fluctuating clinical state characterized byFluctuating clinical state characterized bydisturbances of attention, cognition, arousal,disturbances of attention, cognition, arousal,mood and self-awarenessmood and self-awareness
•common in the elderlycommon in the elderly
•often undiagnosedoften undiagnosed
Delirium (confusional state)Delirium (confusional state)

SymptomsSymptoms
•Impairment in attention and disorientationImpairment in attention and disorientation-distracted, slowed, disorganized thinking-distracted, slowed, disorganized thinking
•Hallucinations may be present Hallucinations may be present -usually more visual than auditory-usually more visual than auditory
•Fluctuating level of awareness Fluctuating level of awareness -mild confusion to stupor or active delirium-mild confusion to stupor or active delirium
•Speech may be incoherentSpeech may be incoherent•Confusion regarding day-to-day procedures or rolesConfusion regarding day-to-day procedures or roles•Remote and recent memory impairedRemote and recent memory impaired
Delirium (confusional state)Delirium (confusional state)

SymptomsSymptoms
•Restlessness, aggressiveness, frightenedRestlessness, aggressiveness, frightened•Delusions of persecution possibleDelusions of persecution possible•Disturbance of sleep-wake cycleDisturbance of sleep-wake cycle•Anxiety and lack of cooperativenessAnxiety and lack of cooperativeness•Fluctuations throughout dayFluctuations throughout day
•worse in the eveningworse in the evening•can be lucid intervalscan be lucid intervals
Delirium (confusional state)Delirium (confusional state)

CausesCauses
•Infections or feverInfections or fever•strokes/cardiovascular disordersstrokes/cardiovascular disorders•drug intoxication (polypharmacy or abuse) or withdrawldrug intoxication (polypharmacy or abuse) or withdrawl•exacerbation of underlying medical illnessexacerbation of underlying medical illness•metabolic and nutritional disordersmetabolic and nutritional disorders
•postoperative stress*postoperative stress*•or other factors related to hospitalization such asor other factors related to hospitalization such assleep loss, excessive sensory inputsleep loss, excessive sensory input
Delirium (confusional state)Delirium (confusional state)

Course and TreatmentCourse and Treatment
•Brief duration (usually less than a week) Brief duration (usually less than a week) •some forms resolve on ownsome forms resolve on own•other forms, treatment depends on causeother forms, treatment depends on cause
•while deliriouswhile delirious•carefully-controlled environment (not too stimulating)carefully-controlled environment (not too stimulating)•brief and continued reassurancebrief and continued reassurance•monitor nutritional and fluid status of personmonitor nutritional and fluid status of person
•help the caregivers understand what is goinghelp the caregivers understand what is going
Delirium (confusional state)Delirium (confusional state)

Differential DiagnosisDelirium Dementia
• Rapid onset
• marked attentional disturbance
• confusion prominent/clouding of consciousness
• fluctuating clinical course
• agitation and behavioral symptoms
• potentially reversible
• Usually insidious onset
• memory systems impaired
• consciousness intact
• slower, progressive course
• subtle behavioral symptoms
• can be irreversible

Lecture 11- Mental DisordersOverview
1. Defining Psychopathology2. Cognitive Disorders
DementiaDelirium
3. Other Mental DisordersDepressionAnxiety (see text)

DepressionDepression
Mood Disorders and featuresMood Disorders and features
•Depressive disorders- sad moodDepressive disorders- sad mood
•Bipolar disorders- involve manic episodeBipolar disorders- involve manic episode
•Dysthymic Disorder-chronic but less severeDysthymic Disorder-chronic but less severe
•Mood disorders due to a general medicalMood disorders due to a general medical conditioncondition

Diagnostic Features of Major Depressive Episode (DSM-IV)
Essential Features Associated Symptoms(1 of 2 required) (5 of 9 required)
• Depressed mood
• Loss of interest or pleasure
• Depressed mood for most of the day
• marked reduction in interest in daily activities
• 5% weight loss or significant change in appetite (increase or decrease)
• almost daily insomnia or hypersomnia
• almost daily physical agitation or retardation
• almost daily decreased energy or fatigue
• almost daily feelings of worthlessness or feelings of guilt
• almost daily decreased concentration or decreased decisiveness
• frequent thoughts of death or suicide

NCS= NCS= 13% men13% men21% women21% women
NCS= NCS= 13% men13% men21% women21% women
Lifetime prevalence:Lifetime prevalence:
Persons over 65:Persons over 65:
1% major depressive disorder1% major depressive disorder2% dysthymia (chronic but less severe depression)2% dysthymia (chronic but less severe depression)1% major depressive disorder1% major depressive disorder2% dysthymia (chronic but less severe depression)2% dysthymia (chronic but less severe depression)
DepressionDepression
Prevalence of Depressive DIsordersPrevalence of Depressive DIsorders
However, 8-20% of older adults report symptomsHowever, 8-20% of older adults report symptoms

•12-20% in clinics and hospitals12-20% in clinics and hospitals•30% in long-term care settings30% in long-term care settings
Higher Prevalence of Mood Disorders in Higher Prevalence of Mood Disorders in Medical Settings:Medical Settings:
DepressionDepression
Can lead to greater risk of more Can lead to greater risk of more serious disorder and even fatal serious disorder and even fatal impairmentimpairment
Can lead to greater risk of more Can lead to greater risk of more serious disorder and even fatal serious disorder and even fatal impairmentimpairment
DepressionDepression
Prevalence of Depressive DIsordersPrevalence of Depressive DIsorders
Myth: Myth: aging leads to depression- old age aging leads to depression- old age is depressingis depressing
Reality: Reality: rates for major depression are rates for major depression are lower in the elderly compared to younger lower in the elderly compared to younger adultsadults

DepressionDepression
Features of Mood Disorders in Older AdultsFeatures of Mood Disorders in Older Adults
•Less likely to report traditional symptoms Less likely to report traditional symptoms involving negative feelingsinvolving negative feelings•More likely to seek treatment for bodily More likely to seek treatment for bodily complaintscomplaints•Seek treatment for disorders other than mood Seek treatment for disorders other than mood (anxiety, cognitive, bodily delusions)(anxiety, cognitive, bodily delusions)

DepressionDepression
Features of Mood Disorders in Older Features of Mood Disorders in Older Adults/causesAdults/causes
Depletion syndromeDepletion syndromeDepletion syndromeDepletion syndrome •Lack of energyLack of energy•HopelessnessHopelessness•Loss of appetiteLoss of appetite
Late-onset depressionLate-onset depressionLate-onset depressionLate-onset depression•Mild or moderateMild or moderate•First appears after age First appears after age 6565

DepressionDepression
Causes of Age Differences in Mood DisordersCauses of Age Differences in Mood Disorders
•Personality and emotional changes associated Personality and emotional changes associated with agingwith aging•Cohort differences in experience of depressionCohort differences in experience of depression

•Older adults do not report symptoms accuratelyOlder adults do not report symptoms accurately•Professionals not attuned to diagnosis of older adultsProfessionals not attuned to diagnosis of older adults•Not enough time spent with older adultsNot enough time spent with older adults•Wish to avoid stigmatizationWish to avoid stigmatization•Therapists unaware of benefitsTherapists unaware of benefits
•cognitive difficulty can accompany depressioncognitive difficulty can accompany depression•dementia and depression can both be presentdementia and depression can both be present
““pseudodementia”pseudodementia”
Problems in Diagnosis of Mood Disorders:Problems in Diagnosis of Mood Disorders:
DepressionDepression

•Dementia has insidious onset (years)Dementia has insidious onset (years)•history of psychiatric problems more common in history of psychiatric problems more common in
pseudodementiapseudodementia
•dementia (mild) complains little about memory/concealmentdementia (mild) complains little about memory/concealment•depressive pseudodementia complains depressive pseudodementia complains
•dementia- behavior in line with clinical severitydementia- behavior in line with clinical severity•depression- incongruities between behavior and depression- incongruities between behavior and
severity of cognitive deficitseverity of cognitive deficit
Differentiating Dementia and PseudodementiaDifferentiating Dementia and Pseudodementia
DepressionDepression

•Drug therapiesDrug therapies•PsychotherapyPsychotherapy
TreatmentTreatment
DepressionDepression

Lecture 11- Mental DisordersOverview
4. Clinical ConcernsElder AbuseSuicide (see text)
5. Psychological Issues in Long-Term Care
6. Myth Busting: Facts on Aging Revisited

Elder AbuseElder Abuse
Types of Types of AbuseAbuseTypes of Types of AbuseAbuse
•PhysicalPhysical•SexualSexual•Emotional or psychologicalEmotional or psychological•NeglectNeglect•AbandonmentAbandonment•Financial or materialFinancial or material
Actions taken against older adults through inflicting psychological or physical harm

Elder AbuseElder Abuse
Prevalence Estimates in CanadaPrevalence Estimates in Canada
•Podnieks et al. (1989) interviewed (by phone) Podnieks et al. (1989) interviewed (by phone) community dwelling seniors community dwelling seniors •Rate for abuse and neglect among seniors Rate for abuse and neglect among seniors
is 4% overallis 4% overall
•material abuse (2.5%)material abuse (2.5%)•chronic verbal agression (1.4%)chronic verbal agression (1.4%)•physical violence (.5%)physical violence (.5%)•neglect (.4%)neglect (.4%)

Elder AbuseElder Abuse
Prevalence Estimates in Canada (region)Prevalence Estimates in Canada (region)
•B.C. 5.3%B.C. 5.3%•Prairies 3.0%Prairies 3.0%•Ontario 4.0%Ontario 4.0%•Quebec 4.0%Quebec 4.0%•Atlantic 3.8%Atlantic 3.8%

Elder Abuse (see this table in the text)Elder Abuse (see this table in the text)
Children most frequent abusersChildren most frequent abusersChildren most frequent abusersChildren most frequent abusers
Highest risk for oldest oldHighest risk for oldest old

Lecture 11- Mental DisordersOverview
4. Clinical ConcernsElder AbuseSuicide (see text)
5. Psychological Issues in Long-Term Care
6. Myth Busting: Facts on Aging Revisited

Psychological Issues in Long-Term CarePsychological Issues in Long-Term Care
Biopsychosocial FactorsBiopsychosocial Factors
Differences among residents in physical Differences among residents in physical functioningfunctioning
BIO-BIO-BIO-BIO-
PSYCHO-PSYCHO-PSYCHO-PSYCHO- Variations in psychological resources Variations in psychological resources and needsand needs
SOCIALSOCIALSOCIALSOCIAL Cultural factors further influence Cultural factors further influence relationshipsrelationships
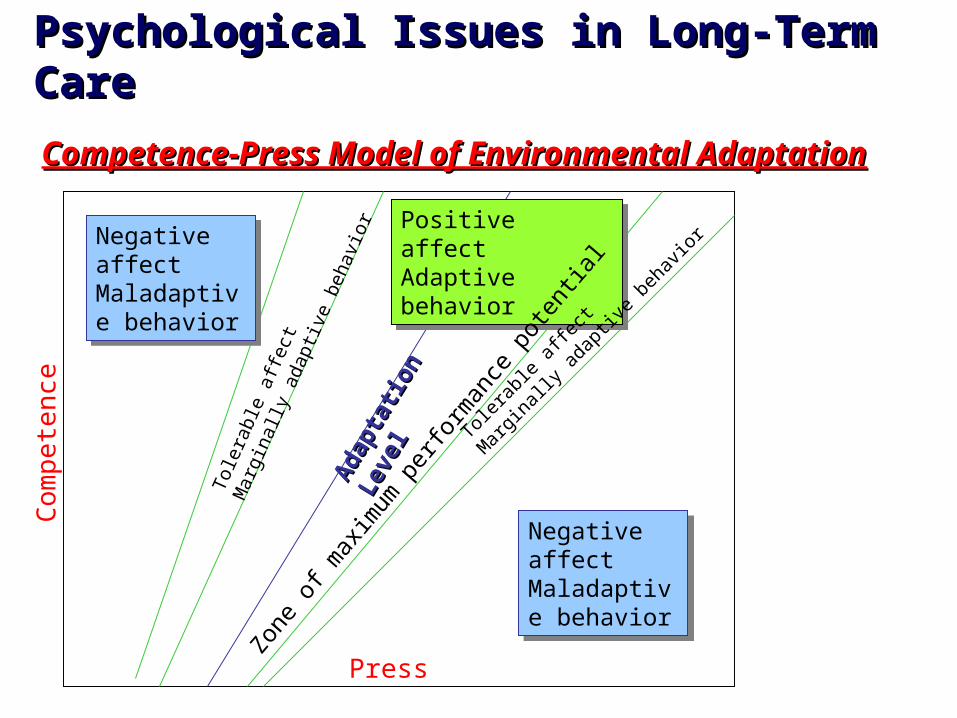
Psychological Issues in Long-Term CarePsychological Issues in Long-Term Care
Competence-Press Model of Environmental AdaptationCompetence-Press Model of Environmental Adaptation
Negative affectMaladaptive behavior
Negative affectMaladaptive behavior
Negative affectMaladaptive behavior
Negative affectMaladaptive behavior
Positive affectAdaptive behavior
Positive affectAdaptive behavior
Ada
ptat
ion
Leve
l
Ada
ptat
ion
Leve
l
Zone
of m
axim
um p
erfo
rman
ce p
oten
tial
Tolera
ble a
ffect
Mar
ginall
y ada
ptive
beh
avior
Tole
rabl
e af
fect
Mar
gina
lly a
dapt
ive
beha
vior
Press
Co
mp
ete
nce

Lecture 11- Mental DisordersOverview
4. Clinical ConcernsElder AbuseSuicide (see text)
5. Psychological Issues in Long-Term Care
6. Myth Busting: Facts on Aging Revisited

Myth Busting: Facts on Aging Revisited
#1 The majority of old people (age 65+) are senile (have defective memory, are disoriented, or demented)
False

Myth Busting: Facts on Aging Revisited
#5 The majority of old people feel miserable most of the time.
False

Myth Busting: Facts on Aging Revisited
#7 At least one tenth of the aged are living in long-stay institutions (such as nursing homes, mental hospitals, homes for the aged, etc.)
False (see text)

Myth Busting: Facts on Aging Revisited
#10 Over three fourths of the aged are healthy enough to do their normal activities without help.
True

Myth Busting: Facts on Aging Revisited
#13 Depression is more frequent among the elderly than among younger people.
False

















