40
Lever, galle og pancreas – maligne strikturer Truls Hauge Gastromedisinsk avdeling OUS - Ullevål

Lever, galle og pancreas – maligne strikturer
Truls HaugeGastromedisinsk avdeling
OUS - Ullevål
Maligne strikturer: galle og duodenum - stentbehandling
• Endoskopisk stentbehandling• Stenting av galleveier• Stenting av duodenum (GOO)• Praktisk - tips

Indications for GI stenting
• Oesophagus and cardia tumours• Gastric outlet obstructions• Tumour recurrence after surgery • Mal obstruction of the small intestine• Biliary obstruction• Colorectal obstruction

AA confusing huge numberconfusing huge number ofof stentsstents

Stent implantationStent implantation
commoncommonopinionopinion
is :is :
easyeasyquickquick
effectiveeffectivesafesafe
criticalcriticalanalysisanalysis
may be :may be :
difficultdifficulttime consumingtime consuming
ineffectiveineffectivedangerousdangerous

RoutineRoutine
CenterCenter
ExpertExpert
Which strictures can I start with?
Prof KE Grund, Univ hospital, Tuebingen
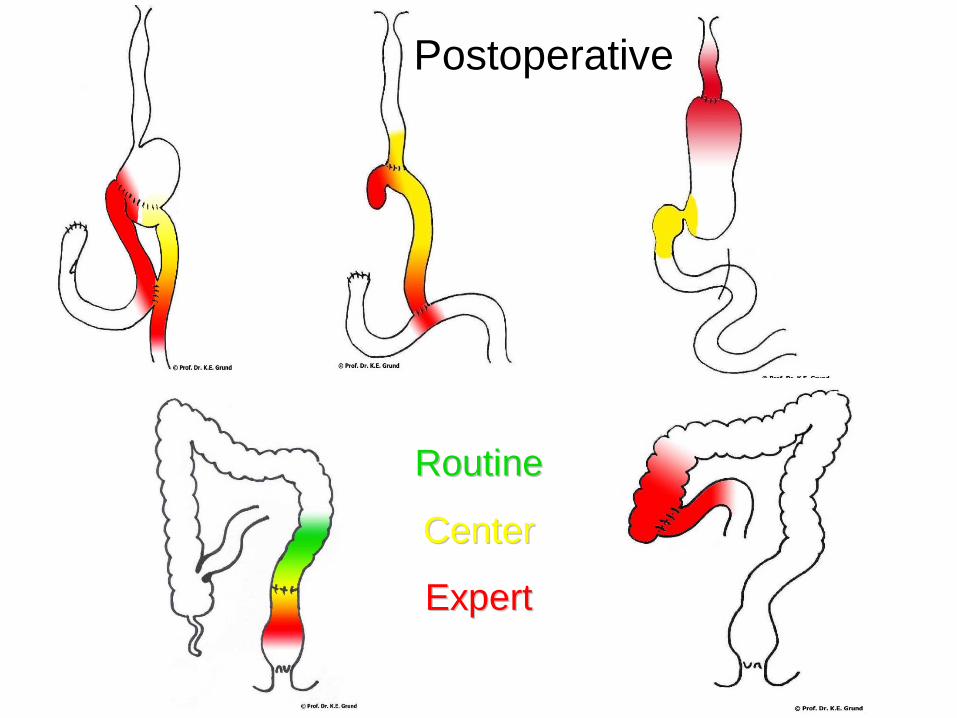
RoutineRoutine
CenterCenter
ExpertExpert
Postoperative

To consider before starting the procedure‐ equipment
• If endoscopic (TTS), appropriate biopsy channel (3.5 mm) ‐ check it
• A stiffer guidewire is better
• Pretreatment? Dilatation?
• Radial stent force? Flexibility?
• Covered / noncovered?
• Available lenghts? Removability?

To consider before starting 2
• Radiology is required
• Premedication / anaesthesia is required
• Two assistents
• How to mark and measure the stricture? Lipiodol, balloon, clip
• Be familiar with the releasement system
• Symptomatic stricture?
Unsuccessful stent implantationwhat to do?
• Position wrong
Remove, correct, overlap immediately
• Expansion unsufficient
Wait and see, strengthen with a second
• Kinking
Remove, pretreatment, another stent
• Complications: perforation, bleeding

Oesophagus - kinking

Removal of SEMS
• Earlier is easier
• Covered stent
• Grasp the tread and pull
• Cut the treads with APC
• Stent cutter
Necessary for a good clinical resulttake home messages
• Have a good indication
• An accurate analysis of the anatomy
• Proper choice of stent
• Gain experience in trainingcourses
• Exact and precise implantation
• It is easier to insert than to remove
• Start with the ”easy” strictures

Biliary metal stent

Plastic stents

Plastic, SEMS – and what to choose?
• Plastic
Diameter, lenght, straight, pigtail?
• SEMS
Diameter, lenght, covered, non‐covered?
• Indication? What will we achieve?
• Where is the stricture?
• Koledochus, uni/bilateral? metastasis?

Is SEMS more expensive? Some answers
• Of course, more than ten times !
• SEMS: stainless‐steel or nickel‐titanium alloy
• Depends on the costs of stents and procedure
• Life expectancy > 4 months favourable SEMS*
• Life expectancy < 3 months plastic
• Covered SEMS?
Better for distal strictures (pancreatic ca)**
*Moss. Eur J Gastroenterol Hepatol 2007 **Stern. EJSO 2007

Covered
Uncovered

Biliary stenting ‐ techniques
• Use papillotom and guidewire
• ”Short” or ”long” wire system
• Papillotomy if necessary (complications)*
• Less contrast prevents cholangitis
• Guidewire across the stricture
• Dilatation? Hilar stenosis?
• If more stents – left side first !
*Everson. J Clin Gastroenterol 2008
Malignant biliary obstruction – preop?
• Adverse impact of early postop survival*
• Plastic, 7F OK, no ES
• Not more than necessary
• If only percutaneous access:
• Combine with endoscopic (rendezvous)
Safer – less bile leak, infection, bleeding**
*Smith. Annals of Surgical Oncology 2008 **Stern. EJSO 2007

Specific strictures
• Biliar hilar obstruction is more difficult
• The left side most important
• Bilateral stenting best
Two guidewires in place is required
• Dilatation necessary?
• Start with the left (or more difficult side)
• Contrast after the guidewire has passed
Stern N. EJSO 2008
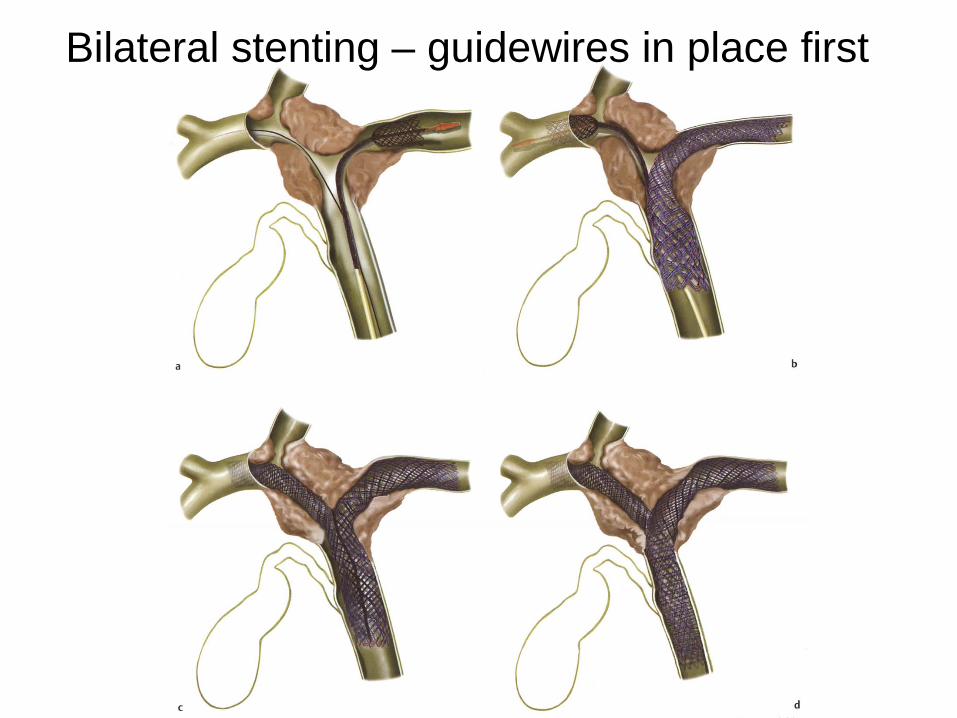
Bilateral stenting – guidewires in place first
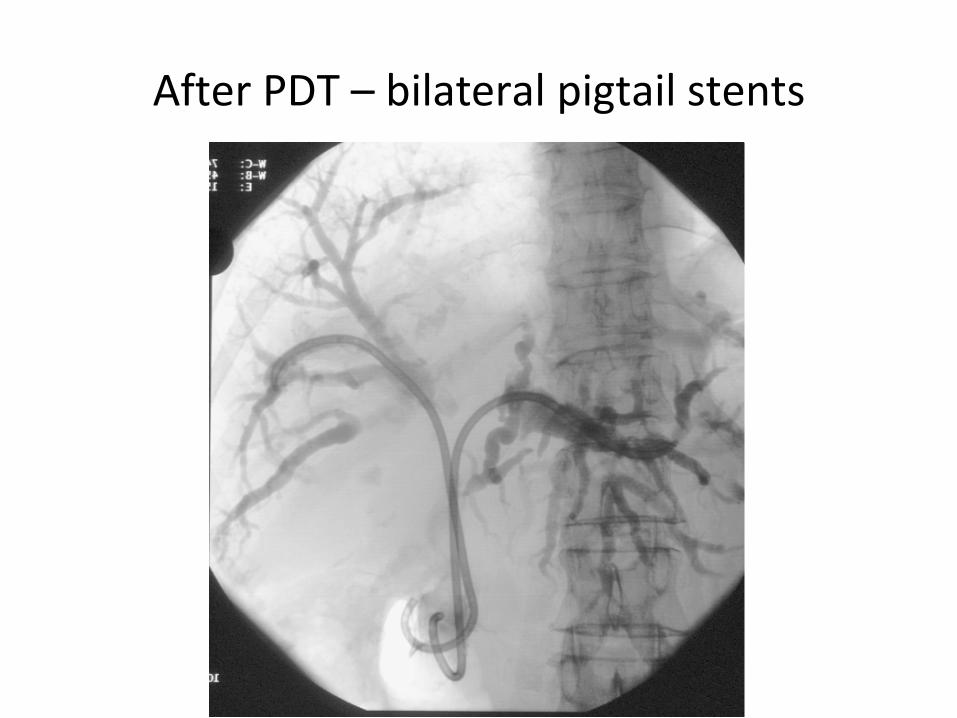
After PDT – bilateral pigtail stents

Biliary duct stenting –when we do not get access?
• Difficult papilla (or to reach), stricture?
• Discuss with your collegues – try again?
PTC? +/‐ ERC? – rendezvous? + stent
• A duodenal stent overlap: rendezvous
• Papilla located in a tumour: rendezvous
• Hilar tumor and insufficient drainage?
Insert what is possible and discuss PTC


The randezvous technique

Endoscopic treatment of biliary duct obstruction ‐ Conclusions
• A proper diagnostic before stenting (MRCP, US)
• What will you achieve? – have a plan
• Use papillotom and guidewire to get access
• SEMS if life expectancy > (3‐)4 months
• Covered SEMS for the distal main bil duct
• ES if necessary for the stent
• Two stents requires 2 guidewires
• Consider combined procedure if you fail


GOO – stent insertion

GOO – different malignancies
• Pancreatic cancer (head)
• Biliary duct cancer
• Papilla of the Vateri
• Distal stomach cancer
• Duodenal cancer
• Metastatic
• Anastomosis relapse

Technical considerations 1
• Biliary obstruction?
• Insert a CBD stent first?
• If not possible to reach the papilla, insert the duodenal stent first
• Possible, but difficult to cannulate through the metal mesh
• Rendevous technique may be better
Technical aspects 2
• Type I (+II) stent oral to the pylorus
• Better curve
• Redused risk for migration, perforation and ”kinking”
• Be aware of the papilla – overlapping
• Is it the symptomatic stenosis? Distal?

Duodenal stenosis Duodenal stenosis –– how to stent?how to stent?

Stenting of GOO ‐ results
• Safe and effective
• Acceptable complication rate
• Superior to sugical bypass
• Cost‐effective
• 12% unable to resume oral intake
• Improved survival remains speculative
Havemann MC. SJG 2009, Fockens P. Gastrointest Endosc 2009

Endoscopic stenting ‐ complications
• Perforation
• Stent ingrowth
• Migration
• Bleeding
• Sepsis
• Pancreatitis
Fockens P. Gastrointest Endosc 2009. Havemann MC. SJG 2009

Biliary stent
Biliary and duodenal stent
Biliary markers
Biliary markers

Stenting of GOO ‐ conclusions
• The procedure is safe and effective
• Acceptable complication rate
• Superior to surgical bypass
• Cost‐effective
• Missing clinical effect reported in 10‐20%
• Improved survival not demonstrated


Technical aspects 3
• Be careful / avoid dilatation of the duodenum
• Insert the duodenal stent first
• Prepare one attempt cannulating the papilla through the mesh
• Rendevous is a good alternative
• Dilatate the mesh (balloon) or rat‐tooth


















