Close this window to return to IVIS www.ivis.org Proceedings of the 60th Annual Convention of the American Association of Equine Practitioners - AAEP – December 6-10, 2014 Salt Lake City, UT, USA Next Meeting: Reprinted in the IVIS website with the permission of the AAEP http://www.ivis.org Dec. 3-7, 2016 - Orlando, FL, USA
Transcript
Close this window to return to IVIS www.ivis.org
Proceedings of the 60th Annual Convention of the
American Association of Equine Practitioners
- AAEP –
December 6-10, 2014 Salt Lake City, UT, USA
Next Meeting:
Reprinted in the IVIS website with the permission of the AAEP http://www.ivis.org
Dec. 3-7, 2016 - Orlando, FL, USA
Auditory Loss in Horses, Part I: Adult Horses
Monica Aleman, MVZ Cert., PhD, DACVIM (Internal Medicine, Neurology)*;Terrell A. Holliday, DVM, PhD, DACVIM (Neurology);Jorge E. Nieto, MVZ, PhD, DACVS, DACVSMR; and Colette Williams, PhD
Hearing loss in horses has been seldom investigatedand can be a cause of difficulty in training, de-creased performance, and behavior alterations.Brainstem auditory evoked response (BAER) testingis a noninvasive, objective, and easy to perform di-agnostic modality that evaluates the integrity of theauditory pathway. The objective of the study wasto describe BAER findings, common signs, andcauses of hearing loss in adult horses.
2. Materials and Methods
BAER records from the Clinical NeurophysiologyLaboratory were reviewed from the years of 1982 to2013. Medical records were reviewed, and horseswere grouped under disease categories. Descrip-tive statistics included mean, standard deviation,and range.
3. Results
Fifty-seven of 76 horses that had a BAER had audi-tory deficits. There was no breed, gender, or age
predisposition with the exception of American Painthorses diagnosed with congenital sensorineuraldeafness. Auditory loss was bilateral in 74% andunilateral in 26% of the horses. The most commoncauses of auditory loss included temporohyoid osteo-arthropathy (35%), congenital sensorineural deaf-ness (30%) associated to certain coat and eye colorpatterns, multifocal brain disease (23%), and otitismedia/interna (7%).
4. Discussion
Temporohyoid osteoarthropathy, multifocal braindisease, and otitis are common causes of hearingloss. Hearing should be investigated in horses withextensive white color markings.
Acknowledgments
Conflict of Interest
The Authors declare no conflicts of interest.
AAEP PROCEEDINGS � Vol. 60 � 2014 161
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Research Abstract
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Auditory deficits occur in foals but are rarely recog-nized. In human medicine, several neonatal dis-eases are common causes of permanent hearing lossin infants. Descriptions of auditory loss in neo-natal foals are limited to 3 foals with lethal whitefoal syndrome. The association of auditory losswith common neonatal diseases has not been stud-ied. Therefore, the objective of the study was toinvestigate auditory deficits in ill-neonatal and non-neonatal foals.
2. Materials and Methods
Brainstem auditory evoked response (BAER; a studyto investigate auditory function) records from theClinical Neurophysiology Laboratory were reviewedfrom the years of 1982 to 2013. Clinical data wereextracted from the medical records. Descriptive sta-tistics were performed.
3. Results
Ten of 15 neonatal foals had absent BAER andwere associated with sepsis, neonatal encephalopa-thy, neonatal isoerythrolysis, and prematurity. Au-ditory deficits were also observed in foals with certaincoat and eye color patterns such as completely ormostly white with blue irises and lavender with paleyellowish irises. One non-neonatal foal (n � 1⁄3) withan intracranial abscess had auditory loss.
4. Discussion
Hearing deficits occur in foals and are associated withcommon neonatal diseases and certain coat and eyecolor patterns. Neurologic and intracranial diseasecan also result in auditory loss in foals of any age.
Acknowledgments
Conflict of InterestThe Authors declare no conflicts of interest.
162 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Research Abstract
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
How to Manage Foal Rejection
Mary Stewart E. White, BS; and Charles F. Scoggin, DVM, MS, DACT*
While relatively uncommon, foal rejection is a seri-ous condition that can adversely affect the healthand welfare of an equine neonate. Consequencescan be costly and labor intensive for the humancaretakers and they can cause untoward and some-times fatal injuries to the foal. Foal rejection canbe seen in all breeds of horses, with the highest ratereported in Arabians (5.1%), followed by PaintHorses (1.9%) and Thoroughbreds (�1%).1 An-other important consideration is that a mare thathas previously rejected her foal is at an increasedrisk of doing so again.2
Normal Maternal BehaviorMost signs of normal maternal behavior are fairlyeasy to recognize. Nickering at and licking andnuzzling of the foal are commonly seen traits. Adam will shield her foal from humans and otherhorses and she will often stand over her foal while itis recumbent. More subtle signs include the marestepping a hind leg back to offer greater exposure tothe udder and gently nudging the foal as it is search-ing for a teat. These motherly instincts are
thought to develop from various sensory, tactile, andmental stimuli. Stimulation can occur with olfac-tory recognition of fetal fluids and membranes,physical contact, nursing, and visual exchanges withthe foal. These actions—along with other factorsthat might not be readily apparent—help foster nor-mal attentive and protective maternal behavior.
Endogenous hormones are important for develop-ing a female’s instincts and ability to care for andnurture her offspring. The neuropeptide oxytocinseems to be important in developing proper mater-nal behavior. Oxytocin is synthesized in the hypo-thalamus and released from the posterior pituitarygland. While commonly thought of as an ecbolicagent whose primary target tissue is the myome-trium of the uterus, oxytocin has been demonstratedto have effects within the central nervous system.Indeed, its importance in stimulating maternal be-havior has been described in humans,3 lab animals,4
and farm animals.5,6 In addition, progesterone andestrogen may also play a role in the development ofmaternal behavior. For example, a preliminarystudy showed lower serum concentrations of thesehormones in rejecting mares compared to nonreject-
AAEP PROCEEDINGS � Vol. 60 � 2014 163
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
ing mares.1 Lactation—an important milestone inthe immediate postpartum period—is mediatedthrough a multitude of hormones, including the afore-mentioned sex hormones and oxytocin, as well asgrowth hormone, prolactin, dopamine, and insulin-likegrowth factor 1. Consequently, knowledge of thehormonal events involved in maternal behavior, lac-togenesis, and milk letdown can become importantwhen identifying causes for and managing cases offoal rejection.
Abnormal Maternal Behavior and Foal Rejection
Abnormal maternal behavior and foal rejection canbe perplexing and, at times, disturbing to witness.Mares may kick, squeal, or chase their foal, whileothers may simply seem indifferent to or becomeelusive from their foals. Different forms of foal re-jection have been previously described by Crowell-Davis and Houpt.7 In our practice, we typically seetwo types of foal rejection. The first is aggressiverejection, which is typified by overt violence andhostility towards the foal. Signs include biting,kicking, and savage attacks. The second is avoid-ance rejection and is characterized by disinterest ofthe mare and/or evasion from the foal. For in-stance, the mare may walk away from the foal whenit attempts to nurse or fail to display any interest inthe foal, especially when the two are removed fromeyesight of each other. A salient point regardingthese classifications is that they are not mutuallyexclusive; indeed, variations of the two can occurdepending upon the circumstances and individualsinvolved in each case.
In some cases, the cause for foal rejection is read-ily apparent. For example: the mare could beyoung and/or inexperienced; she could have previ-ously rejected a foal; she could feel anxious or ner-vous around the foal due to a change in environmentor management; she could have poor milk produc-tion secondary to a disease process; she could haveproduced an abnormal or sick foal; or the scent of thefoal could have been altered through drugs, such asdimethyl sulfoxide (DMSO), which could interferewith olfactory recognition.2 All of these instancescan disrupt bonding time or hamper the naturalprogression of motherly behavior, thereby leading tofoal rejection.
Other times, the reasons for rejection are not soclear. The clinician must obtain a thorough historyand perform a careful physical examination of themare and foal to decide if there are any issues thatmay be contributing to the abnormal behavior.Watching the pair interact can be useful for deter-mining certain behavioral cues that might be con-tributing to rejection. It also behooves the clinicianto carefully evaluate the management practices ofthe farm to ascertain whether changes in the envi-ronment have led to maternal aggression oravoidance.
One factor that is sometimes overlooked, yethighly important, is that of maternal pain. Pain
can be secondary to either normal physiologic pro-cesses or certain disease conditions. Examples ofthe former include pain arising from postpartumuterine contractions or discomfort from a sore udderdue to an aggressively nursing foal.2 Examples ofthe latter include musculoskeletal injury, such aslaminitis or osteoarthritis, and systemic illness,such as metritis associated with retained fetal mem-branes or gastroenterocolitis. Identifying thesource of pain underscores the importance of per-forming a thorough physical examination, whileproper management of the pain can result in a suc-cessful outcome for all parties involved.
The safety and health of the foal should be ofprimary concern when dealing with cases of foalrejection. As such, the foal should be immediatelyremoved from a mare that displays overt aggressiontowards the foal. If necessary, the foal should beadministered at least one pint of good quality colos-trum through a nasogastric tube for passive transferof immunoglobulins and nourishment. Alterna-tively, or in addition, intravenous plasma can beused to provide adequate passive transfer. Subse-quent feedings can be performed every two to threehours with the mare’s own milk (provided she istractable for harvesting milk), goat’s milk, or a com-mercial foal milk replacer formulaa from a pan,bottle, or indwelling nasogastric feeding tube. Sup-portive care, in the form of intravenous fluids, andprophylactic administration of broad-spectrum anti-microbials may also be administered at the discre-tion of the clinician to prevent or treat dehydrationand sepsis.
2. Materials and Methods
Strategies that can be employed to treat and man-age foal rejection include physical restraint, behav-ior modification, pharmaceutical intervention, andsurrogation. Depending on the circumstances andindividuals involved, these strategies can be usedalone or in conjunction with one another. Also,farm management practices and available resourcesmay preclude the use of some of these strategies.The clinician must thus work in cooperation withthe owner or caregivers to determine which strate-gies could be useful, as well as which ones arefeasible with respect to their experience andwherewithal.
Success in establishing normal maternal behavioror adequate surrogation can be determined by usingat least three subjective markers. The first markeris the mare’s response following removal of the foalfrom eyesight. If the mare whinnies, becomes anx-ious, or attempts to follow the foal, then these aregood indicators of the mare’s acceptance of andbonding with the foal. The second marker is leav-ing the mare and foal free from restraint in a stall orsmall enclosed area and observing their interac-tions. Positive indicators include: witnessing thefoal physically contacting the mare without themare showing any signs of aggression or indiffer-
164 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
ence; seeing the mare willingly allow the foal tonurse; and observing the mare standing over the foalas it is lying down. The third positive marker isturning the pair out in a paddock and seeing themremain in close proximity to one another, with themare permitting the foal to nurse her at its ownvolition.
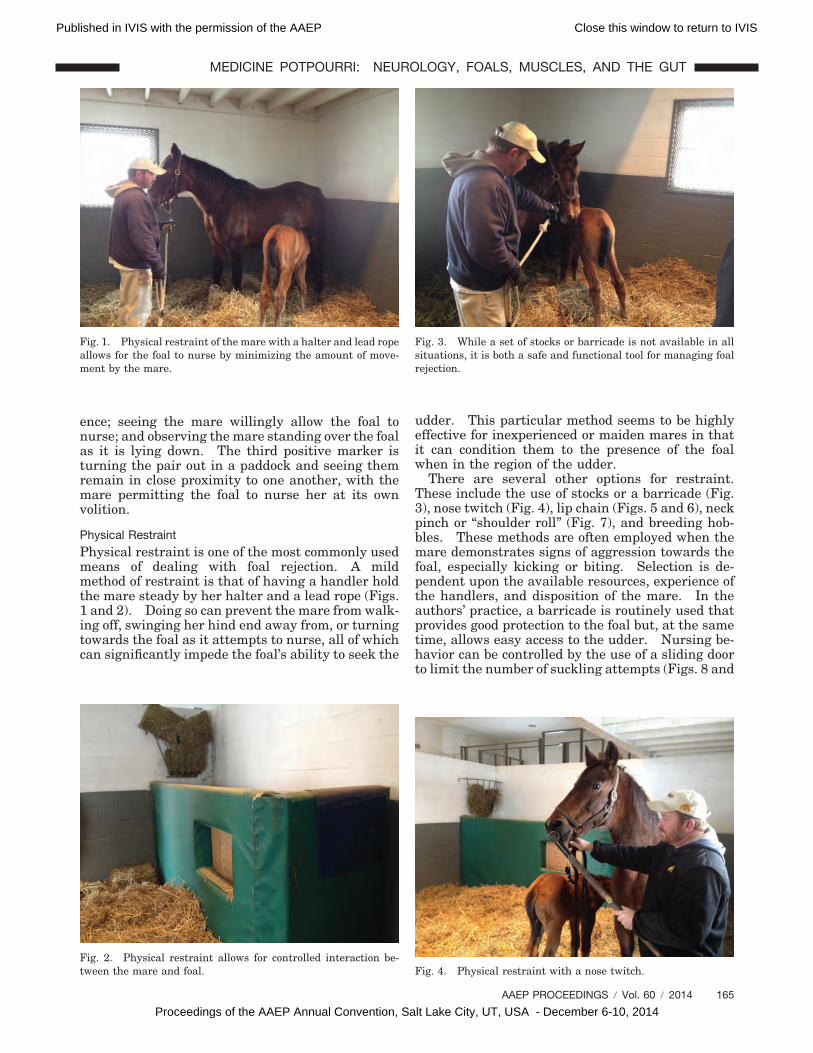
Physical RestraintPhysical restraint is one of the most commonly usedmeans of dealing with foal rejection. A mildmethod of restraint is that of having a handler holdthe mare steady by her halter and a lead rope (Figs.1 and 2). Doing so can prevent the mare from walk-ing off, swinging her hind end away from, or turningtowards the foal as it attempts to nurse, all of whichcan significantly impede the foal’s ability to seek the
udder. This particular method seems to be highlyeffective for inexperienced or maiden mares in thatit can condition them to the presence of the foalwhen in the region of the udder.
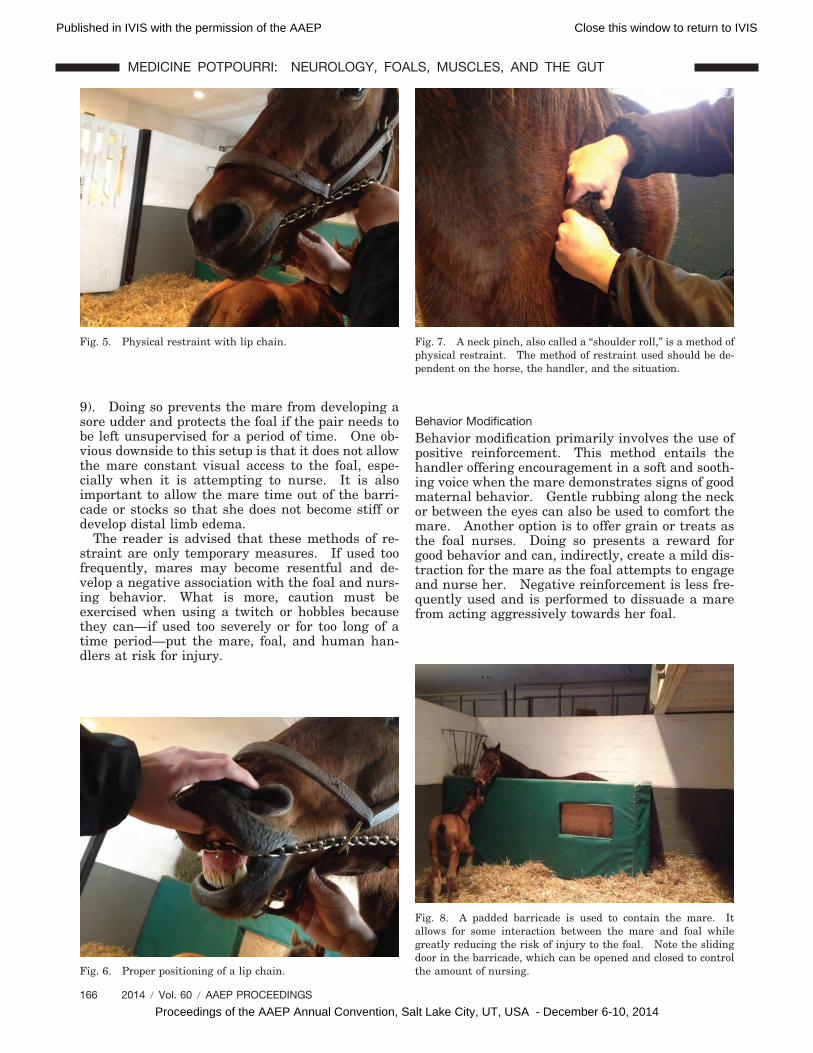
There are several other options for restraint.These include the use of stocks or a barricade (Fig.3), nose twitch (Fig. 4), lip chain (Figs. 5 and 6), neckpinch or “shoulder roll” (Fig. 7), and breeding hob-bles. These methods are often employed when themare demonstrates signs of aggression towards thefoal, especially kicking or biting. Selection is de-pendent upon the available resources, experience ofthe handlers, and disposition of the mare. In theauthors’ practice, a barricade is routinely used thatprovides good protection to the foal but, at the sametime, allows easy access to the udder. Nursing be-havior can be controlled by the use of a sliding doorto limit the number of suckling attempts (Figs. 8 and
Fig. 1. Physical restraint of the mare with a halter and lead ropeallows for the foal to nurse by minimizing the amount of move-ment by the mare.
Fig. 2. Physical restraint allows for controlled interaction be-tween the mare and foal.
Fig. 3. While a set of stocks or barricade is not available in allsituations, it is both a safe and functional tool for managing foalrejection.
Fig. 4. Physical restraint with a nose twitch.
AAEP PROCEEDINGS � Vol. 60 � 2014 165
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
9). Doing so prevents the mare from developing asore udder and protects the foal if the pair needs tobe left unsupervised for a period of time. One ob-vious downside to this setup is that it does not allowthe mare constant visual access to the foal, espe-cially when it is attempting to nurse. It is alsoimportant to allow the mare time out of the barri-cade or stocks so that she does not become stiff ordevelop distal limb edema.
The reader is advised that these methods of re-straint are only temporary measures. If used toofrequently, mares may become resentful and de-velop a negative association with the foal and nurs-ing behavior. What is more, caution must beexercised when using a twitch or hobbles becausethey can—if used too severely or for too long of atime period—put the mare, foal, and human han-dlers at risk for injury.
Behavior ModificationBehavior modification primarily involves the use ofpositive reinforcement. This method entails thehandler offering encouragement in a soft and sooth-ing voice when the mare demonstrates signs of goodmaternal behavior. Gentle rubbing along the neckor between the eyes can also be used to comfort themare. Another option is to offer grain or treats asthe foal nurses. Doing so presents a reward forgood behavior and can, indirectly, create a mild dis-traction for the mare as the foal attempts to engageand nurse her. Negative reinforcement is less fre-quently used and is performed to dissuade a marefrom acting aggressively towards her foal.
Fig. 5. Physical restraint with lip chain.
Fig. 6. Proper positioning of a lip chain.
Fig. 7. A neck pinch, also called a “shoulder roll,” is a method ofphysical restraint. The method of restraint used should be de-pendent on the horse, the handler, and the situation.
Fig. 8. A padded barricade is used to contain the mare. Itallows for some interaction between the mare and foal whilegreatly reducing the risk of injury to the foal. Note the slidingdoor in the barricade, which can be opened and closed to controlthe amount of nursing.
166 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Oftentimes, behavior modification is used in con-junction with physical restraint. A good example isholding a mare via a lip chain as the foal attempts toconnect with and nurse the mare. Pressure can bereleased on the chain when the mare demonstratesinterest in the foal and a soothing voice and gentlerub along the neck can reward the mare for goodbehavior.
Pharmaceutical InterventionChemical restraint, through the use of tranquilizersand sedatives, is another option when dealing withmares that are actively rejecting their foals. Thephenothiazine tranquilizer, acepromazine maleateb
(0.05 mg/kg, IV or IM, q 8–12), is advocated by someauthors1 because it can provide both tranquilizationand stimulate lactation via its antidopaminergic ac-tivity. Other agents, such as the �2-agonists, xyla-zinec (0.5–1.1 mg/kg, IV, q 8–12 h) and detomidined
(0.001–0.002 mg/kg, IV or IM, q 8–12 h), and theopioid agonist/antagonist, butorphanole (0.02–0.05mg/kg, IV, q 8–12 h), may also be used either aloneor in conjunction with acepromazine to provide tran-quilization, sedation, and/or analgesia. Prudentuse of tranquilizers and sedatives is important so asto prevent ataxia and ileus. Anecdotally, paradox-ical reactions have been reported in horses admin-istered xylazine whereby they can becomeaggressive and overly sensitive to external stimuli(i.e., the “xyla-mean” effect). Therefore, cliniciansshould be careful in their selection of and criteria forthe use of tranquilizers and sedatives so as not tofurther compound problems associated with foalrejection.
Another means of pharmaceutical intervention isadministration of a relatively high dose of prosta-glandin-F2� (PGF2�). This technique was first de-scribed by Daels and is hypothesized to triggeroxytocin release in the brain to promote concave-ation and normal maternal behavior.7 A hybrid-
ized protocol utilized by the current authors beginswith removing the foal from eyesight of the mareand giving her a large dose of dinoprost tromethami-nef (0.033–0.056 mg/kg, IM). Approximately 15 to20 minutes after receiving PGF2�, mares will showsigns of intense sweating and cramping, as well asstream milk. With one person holding the mareand another leading the foal, the foal is taken backin the stall and presented at the mare’s head. Of-tentimes, the mare will nuzzle and nicker at the foal.The foal is then directed towards the mare’s udderand encouraged to nurse. Within a relatively shorttime period (�15–30 minutes), the mare usuallyaccepts the foal and the two can be turned loose andleft alone to interact and strengthen their bond.This protocol seems to effectively “reprogram” themare’s behavior to where she becomes highly atten-tive to and accepting of the foal. If the mare stillrejects the foal after the first attempt, this methodcan be repeated 24 h later.
The peceding protocol is not without possible com-plications, most of which are often associated withthe administration of exogenous prostaglandins inhorses. These include signs of colic, diarrhea, andanxiety. Because a larger dose is used than what isnormally given to induce luteolysis, these signs canbe more intense but are usually transient and self-limiting. It should be noted that the likelihood andseverity of adverse reactions seem to increase whenmultiple doses of PGF2� are used over the course ofseveral days, so it may be necessary to either scaleback the dose of PGF2� or simply utilize anothermeans to get the mare to accept the foal. The syn-thetic PGF2�-analog, cloprostenol
g (0.001–0.002 mg/kg,IM)8 can be used instead of dinoprost because it isthought to produce less severe side effects comparedto dinoprost.
Administration of progestogens is another optionto promote proper maternal behavior. Use of pro-gesterone in oilh (150 mg/horse IM q 24 h) and thesynthetic progestogen, altrenogesti (0.044 mg/kg POq 24 h), have been recommended by some clini-cians.1,2 These treatments are hypothesized to exerta calming effect, raise the threshold for aggression,promote motherly behavior, or a combination thereof.
Some mares may not produce sufficient amountsof milk to support and satiate their foals. They cansubsequently become “teat sore” due to the foal con-stantly and aggressively attempting to nurse, whichcan cause mares to become aggravated and hostiletowards their foals. In these instances—and aslong as common causes of agalactia have been ruledout (e.g., metritis and fescue toxicosis)—treatmentwith nonsteroidal anti-inflammatory agents, warmcompresses, and the dopamine antagonist, domperi-donej (1.1 mg/kg, PO, q 12–24 h), can be utilized toreduce inflammation and promote lactation. Oxy-tocink (5–20 IU, IM or IV, q 2–6 h) can be adminis-tered to promote milk letdown. Finally, improvingthe plane of nutrition can also be of benefit whenattempting to improve milk quantity.
Fig. 9. A foal nursing through an opening in the barricade.
AAEP PROCEEDINGS � Vol. 60 � 2014 167
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
SurrogationSurrogate mares are often utilized when a foal’s damexperiences severe illness or death. In these in-stances, one of two options exists. The first is toutilize a wet nurse mare from either a commercialsupplier or another mare that has recently lost herfoal. Commercial nurse mare operations are fairlyprevalent in Central Kentucky but are scarce inother parts of the country. As such, the other op-tion is to stimulate lactation in a barren mare.Preferably, the mare should have raised foals in thepast, possess an even temperament, be tractable tohandling and restraint, have good udder conforma-tion, and be free of disease and musculoskeletalissues.
Methods to induce lactation in nonpregnantmares have been described previously.8,9 Lacta-tion is stimulated with a combination treatment ofprogesterone and estrogen, as well as antidopamin-ergic agents, such as domperidone or sulpiride.Progesterone is responsible for promoting lobuloal-veolar growth within the mammary gland, whileestrogen stimulates cellular division and develop-ment of the mammary ducts. When combined withtreatment with a dopamine antagonist, this protocolcan be used successfully to promote lactogenesis inbarren mares. The reader is directed to publica-tions by Daels8 and Steiner9 for specific informationregarding these protocols.
The actual grafting process utilizes many of thesame previously described methods to counteractfoal rejection. Moreover, since olfactory recogni-tion plays an important role in stimulating normalmaternal behavior, the authors find it useful tomask or alter the scent or smell of both the mare andfoal. If a lactating mare is going to be used andfresh fetal fluids and membranes are available, theycan be applied to the body of the foal and around thenostrils of the mare. If these are not available, or ifthe mare is barren, then a grafting sprayl can beused to disguise the smell of the foal. Muzzling thefoal for one to two hours is commonly done prior tointroducing it to the surrogate. A hungry foal willusually seek the udder immediately upon presenta-tion to the mare.
3. Results
Several of the previously described techniques havebeen utilized in the authors’ practice for the past sixyears. During this time, we have treated eightmares (average age 5.6 years; range 4–6 years) thatinitially rejected their foals and required some formof intervention to make them accept their foals.Physical restraint alone was used in one case(12.5%), a combination of physical restraint withtranquilization was used in five of the eight cases(62.5%), and the high-dose PGF2� method was usedin two of the eight cases (25%). In all instances, weachieved a 100% success rate in inducing propermaternal behavior and foal acceptance within 72hours (average � 52.5 h; range � 12–72 h) of foaling.
We have also employed these techniques on a totalof 24 lactating nurse mares (ages unknown) with 22foals (range of 6 h– to 32 days of age). All but twomares accepted the foals within five days (average �59.0 h; range � 2–120 h) of first introducing a foal tothem, for a grafting success rate of 91.7%. Physicalrestraint in combination with tranquilization wasall that was required in 10 of these mares (10/24 or42.0%). The high-dose PGF2� method was used inthe remaining 14 mares, and 12 of these mares(12/14 or 85.7%) adequately bonded with the foalwithin five days of being introduced to the foals.All of these mares were actively lactating, so exoge-nous progesterone and estrogen were not utilized inany of the mares. However, in three of the cases inwhich high-dose PGF2� was administered (3/14 or21.4%), domperidone was administered for two tothree days following grafting because these mares’milk production was judged to be less than adequate.
4. Discussion
Foal rejection is a relatively uncommon occurrencein clinical equine practice. Nevertheless, when itdoes happen, it can be frustrating to deal with andunsettling to witness. Fortunately, several differ-ent options exist for treating and managing foalrejection, which range from physical restraint, tobehavior modification, to pharmaceutical interven-tion. These methods can be used alone or in com-bination to fit each individual case or remain withinthe limits of available resources. We recommendstarting with the simple methods (e.g., physical re-straint with or without tranquilization) and thenprogressing to more involved techniques, such asbehavior modification and high-dose PGF2� admin-istration, if the circumstances dictate the use ofmore aggressive tactics. Our experience indicatesthat avoidance rejection is easier and quicker toreconcile compared to aggressive rejection. Inmany cases, light manual restraint with light tomoderate sedation works well in mares that areavoiding but not aggressive towards their foals.Aggression oftentimes requires more forceful andinvolved measures, such as moderate restraint (e.g.,nose twitch or lip chain), behavior modification, andhigh-dose PGF2�, but not necessarily in that order.Luckily, we have been able to successfully treat all ofour foal rejection cases within 72 hours from thebirth of the foal, which is a shorter period of timethan the two to three weeks previously reported inthe literature.1
With respect to surrogation, there are a couple ofconcluding thoughts. First, the age of the foal andtime frame in which the surrogate had her foalseems to impact the time required for adequatebonding. If the foal is relatively young (e.g., lessthan 7 days) and the mare has recently foaled (e.g.,24–48 h), the grafting process is often very swift andseamless. Older foals or mares that have been rais-ing a foal for several days appear to require moretime and effort. However, with persistence and pa-
168 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
tience, success can often be achieved within fivedays of introduction. Second, the authors are of theopinion that surrogation is a much better optionthan attempting to hand-raise an orphan foal.Anecdotally, orphan foals seem to display unsafeand unusual behavioral traits towards humans andother horses as they mature. This phenomenonhas been coined the “orphan foal” syndrome. It islikely a manifestation of overly intensive handlingand rearing by humans, as well as inadequate so-cialization with other horses during an early yethighly formative time period. Foals raised bynurse mares seem—on average—more respectful to-wards humans and better adjusted to a herd envi-ronment compared to orphan foals. Finally,surrogation does not appear to hinder foals’ devel-opment or place them at a higher risk for diseaserelative to other foals. In the authors’ practice, therate of growth and adverse health events appear tobe equivocal between foals raised on a nurse mareand those raised by their own dams.
Acknowledgments
Conflict of Interest
The Authors declare no conflicts of interest.
References and Footnotes1. Houpt KA. Foal rejection. In: Robinson NE, Sprayberry
K, eds. Current therapy in equine medicine 6th ed. Phila-delphia: WB Saunders, 2009;116–118.
3. Ross HE, Young LJ. Oxytocin and the neural mechanismsregulating social cognition and affiliative behavior. FrontNeuroendocrinol 2009;30:534–547.
4. Shahrokh DK, Zhang TY, Diorio J, et al. Oxytocin-dopa-mine interactions mediate variations in maternal behavior inthe rat. Endocrinology 2010;151:2276–2286.
5. Kaverne EB, Kendrick KM. Oxytocin facilitation of mater-nal behavior in sheep. Ann NY Acad Sci 1992;652:83–101.
6. Williams GL, Gazal OS, Leshin LS, et al. Physiological reg-ulation of maternal behavior in heifers: roles of genitalstimulation, intracerebral oxytocin release, and ovarian ste-roids. Biol Reprod 2001;65:295–300.
7. Crowell-Davis SL, Houpt KA. Maternal behavior. In:Crowell-Davis SL, Houpt KA, eds. The veterinary clinics ofNorth America equine practice. Philadelphia: Saunders,1986;557–571.
8. Daels PF. Induction of lactation and adoption of an orphanfoal, in Proceedings. Belgian Equine Pract Soc 2009;26:28–33.
9. Steiner JV. How to induce lactation in non-pregnant mares,in Proceedings. Am Assoc Equine Pract 2006;52:259–260.
aFoal-Lac Powder, Pet Ag, Hampshire, IL 60140.bAceproject, Henry Schein Animal Health, Dublin, OH 43017.cAnaSed®, Lloyd Laboratories, Shenandoah, IA 51601.dDormosedan®, Zoetis, Florham Park, NJ 07932.eTorbogesic®, Zoetis, Florham Park, NJ 07932.fLutalyse®, Zoetis, Florham Park, NJ 07932.gEstrumate®, Merck Animal Health, Millsboro, DE 19966.hProgesterone in oil, Rood and Riddle Veterinary Pharmacy, Lex-ington, KY 40511.iRegumate®, Merck Animal Health, Millsboro, DE 19966.jEquidone®, Dechra Veterinary Products, Overland Park, KS66211.kOxoject, Henry Schein Animal Health, Columbus, OH 43204.lMotherUp®, Pierre, SD 57501.
AAEP PROCEEDINGS � Vol. 60 � 2014 169
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
How to Build an Automatic Milk Feeding Devicefor Orphan Foals
Veterinarians often face the dilemma of having anewborn foal in their care that may require roundthe clock feedings of a supplemental milk source.Foals whose dams are deceased, have rejected them,or are simply not producing enough milk normallyrequire either a nurse mare or an alternative supplyof milk or milk replacer. Once a foal’s antibodyrequirements have been met with the ingestion ofcolostrum or the delivery of an IV hyperimmuneplasma, a decision will need to be made regardingthe source and delivery method of its nutrition.A foal will require some form of milk for the first 2 to5 months of life.1 A commercially available nursemare or an open mare who has been hormonallyinduced to lactate are two options that offer both along-term source of naturally balanced nutrition andsocial upbringing. Unfortunately, both of these al-ternatives take valuable time to arrange, can bevery costly, and still run the risk of foal rejection.In the meantime, it is necessary to provide feedingsat 1–2 hour intervals for at least the first few days ofthe foal’s life.2 Owners may quickly become ex-hausted by feeding foals this frequently and payingstaff can rapidly become cost prohibitive. Somecaretakers are tempted to leave out large volumes ofmilk in the stall overnight for the foal to consume atwill. This practice can lead to spoilage of the milk
or overconsumption by the foal, which can causecolic, diarrhea, gastric ulceration, and lack of weightgain.3 Constructing a relatively inexpensive auto-mated device to store, refrigerate, and distribute aprogrammed volume of milk into a small receptaclefor consumption at timed intervals can save thepractitioner or owner time, money, and provide amore natural digestive process for the foal.
2. Materials and Methods
An area with a 110 V electrical outlet and protectionfrom rain is required to run and maintain the feed-ing device. Always use caution to avoid flammablematerials around any electrical device, and be surethe device does not sit in wet conditions. The ma-terials required are readily available online, andovernight shipping can be used to expedite delivery.A busy breeding farm or veterinary hospital canconstruct the device before the beginning of foalingseason to ensure it will be ready when needed.The unit as described here costs less than $400 insupplies to build, and our hospital was quickly ableto reimburse costs by charging a deposit andmonthly rental fee for at home use. Equipment tobe purchased includes the following:
1. A compact (dormitory) refrigerator. We use aKenmore Chill 3.3 cu. ft. model no. 93382a,
170 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
which averages $143.99 at www.sears.com,$129.99 at www.amazon.com, or is availableat Sears appliance stores. This fridge allowsa larger milk receptacle to be used inside, assome compact refrigerators do not provide alarge enough ventral footprint on which toplace a container large enough to store milkfor 12 hours of use.
2. A rectangular milk storage container that fitsinside the chosen compact refrigerator. Weuse a 2.5 gallon Steriliteb plastic trash canfound at Dollar General or Walmart foraround $2.00.
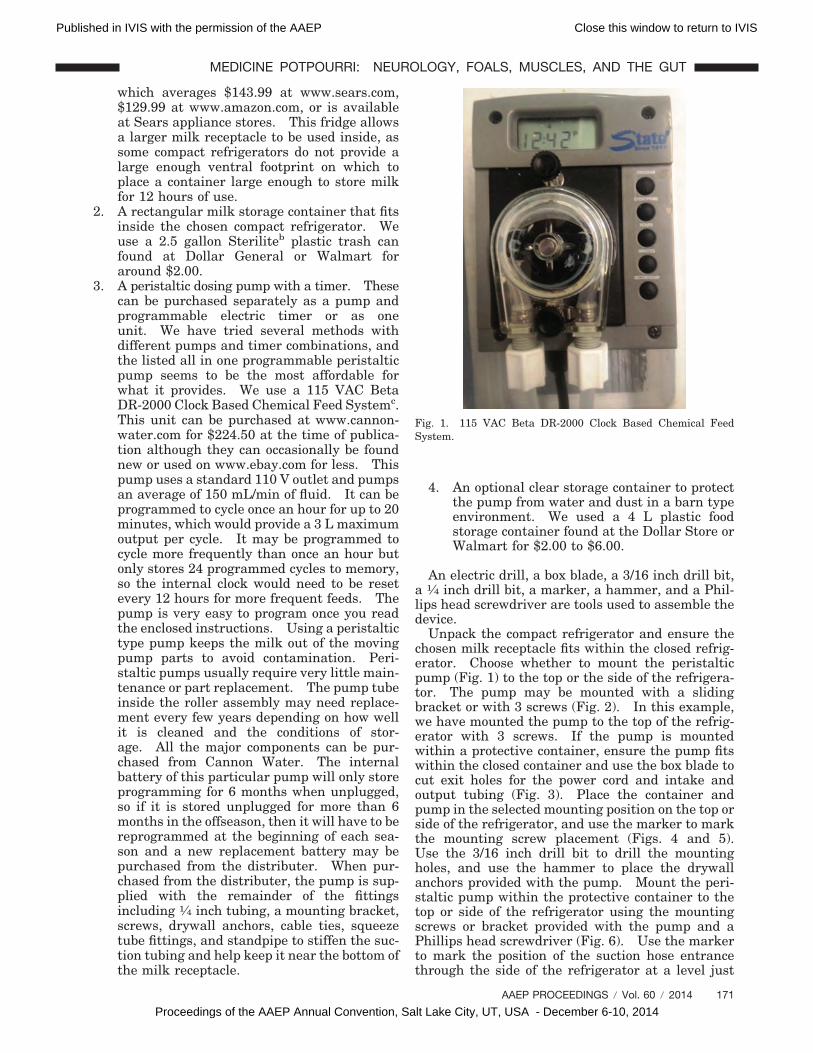
3. A peristaltic dosing pump with a timer. Thesecan be purchased separately as a pump andprogrammable electric timer or as oneunit. We have tried several methods withdifferent pumps and timer combinations, andthe listed all in one programmable peristalticpump seems to be the most affordable forwhat it provides. We use a 115 VAC BetaDR-2000 Clock Based Chemical Feed Systemc.This unit can be purchased at www.cannon-water.com for $224.50 at the time of publica-tion although they can occasionally be foundnew or used on www.ebay.com for less. Thispump uses a standard 110 V outlet and pumpsan average of 150 mL/min of fluid. It can beprogrammed to cycle once an hour for up to 20minutes, which would provide a 3 L maximumoutput per cycle. It may be programmed tocycle more frequently than once an hour butonly stores 24 programmed cycles to memory,so the internal clock would need to be resetevery 12 hours for more frequent feeds. Thepump is very easy to program once you readthe enclosed instructions. Using a peristaltictype pump keeps the milk out of the movingpump parts to avoid contamination. Peri-staltic pumps usually require very little main-tenance or part replacement. The pump tubeinside the roller assembly may need replace-ment every few years depending on how wellit is cleaned and the conditions of stor-age. All the major components can be pur-chased from Cannon Water. The internalbattery of this particular pump will only storeprogramming for 6 months when unplugged,so if it is stored unplugged for more than 6months in the offseason, then it will have to bereprogrammed at the beginning of each sea-son and a new replacement battery may bepurchased from the distributer. When pur-chased from the distributer, the pump is sup-plied with the remainder of the fittingsincluding 1⁄4 inch tubing, a mounting bracket,screws, drywall anchors, cable ties, squeezetube fittings, and standpipe to stiffen the suc-tion tubing and help keep it near the bottom ofthe milk receptacle.
4. An optional clear storage container to protectthe pump from water and dust in a barn typeenvironment. We used a 4 L plastic foodstorage container found at the Dollar Store orWalmart for $2.00 to $6.00.
An electric drill, a box blade, a 3/16 inch drill bit,a 1⁄4 inch drill bit, a marker, a hammer, and a Phil-lips head screwdriver are tools used to assemble thedevice.
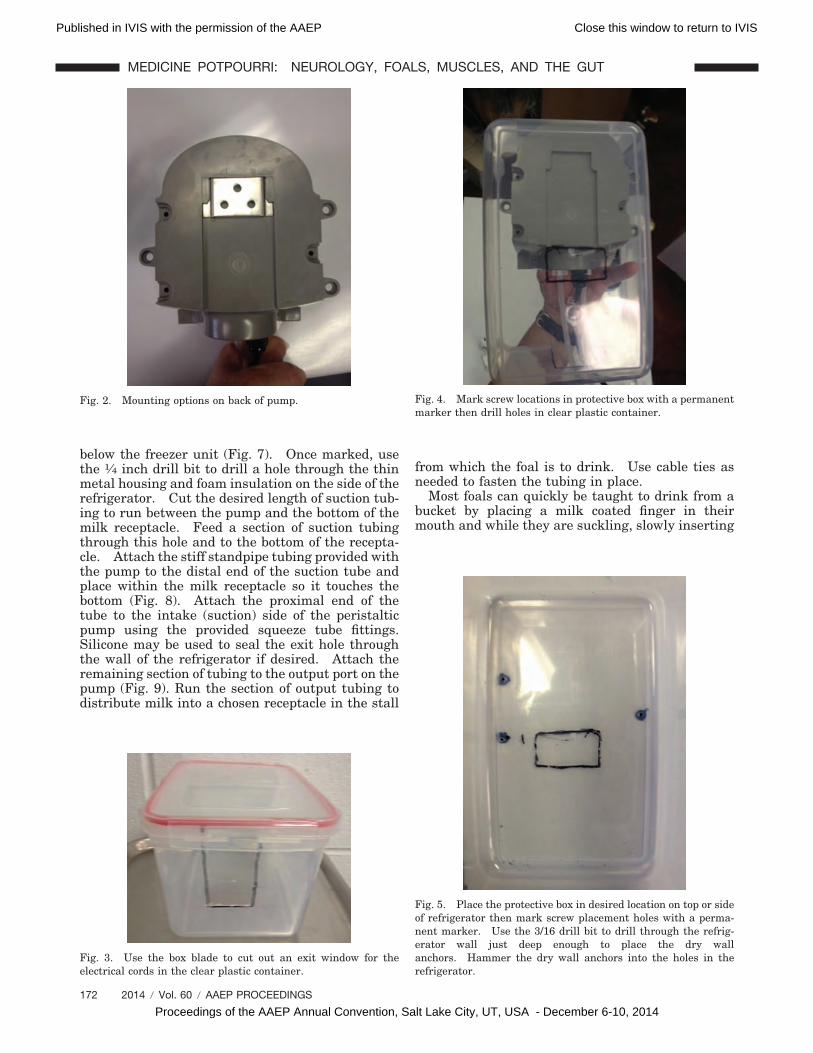
Unpack the compact refrigerator and ensure thechosen milk receptacle fits within the closed refrig-erator. Choose whether to mount the peristalticpump (Fig. 1) to the top or the side of the refrigera-tor. The pump may be mounted with a slidingbracket or with 3 screws (Fig. 2). In this example,we have mounted the pump to the top of the refrig-erator with 3 screws. If the pump is mountedwithin a protective container, ensure the pump fitswithin the closed container and use the box blade tocut exit holes for the power cord and intake andoutput tubing (Fig. 3). Place the container andpump in the selected mounting position on the top orside of the refrigerator, and use the marker to markthe mounting screw placement (Figs. 4 and 5).Use the 3/16 inch drill bit to drill the mountingholes, and use the hammer to place the drywallanchors provided with the pump. Mount the peri-staltic pump within the protective container to thetop or side of the refrigerator using the mountingscrews or bracket provided with the pump and aPhillips head screwdriver (Fig. 6). Use the markerto mark the position of the suction hose entrancethrough the side of the refrigerator at a level just
Fig. 1. 115 VAC Beta DR-2000 Clock Based Chemical FeedSystem.
AAEP PROCEEDINGS � Vol. 60 � 2014 171
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
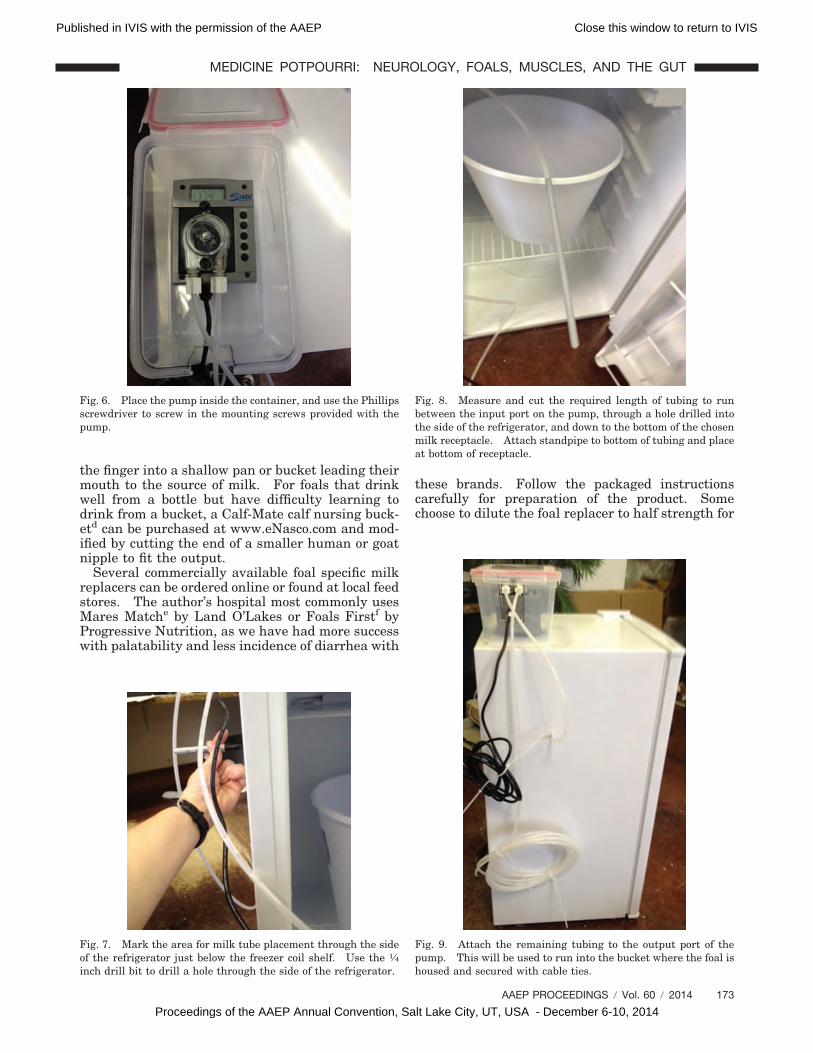
below the freezer unit (Fig. 7). Once marked, usethe 1⁄4 inch drill bit to drill a hole through the thinmetal housing and foam insulation on the side of therefrigerator. Cut the desired length of suction tub-ing to run between the pump and the bottom of themilk receptacle. Feed a section of suction tubingthrough this hole and to the bottom of the recepta-cle. Attach the stiff standpipe tubing provided withthe pump to the distal end of the suction tube andplace within the milk receptacle so it touches thebottom (Fig. 8). Attach the proximal end of thetube to the intake (suction) side of the peristalticpump using the provided squeeze tube fittings.Silicone may be used to seal the exit hole throughthe wall of the refrigerator if desired. Attach theremaining section of tubing to the output port on thepump (Fig. 9). Run the section of output tubing todistribute milk into a chosen receptacle in the stall
from which the foal is to drink. Use cable ties asneeded to fasten the tubing in place.
Most foals can quickly be taught to drink from abucket by placing a milk coated finger in theirmouth and while they are suckling, slowly inserting
Fig. 2. Mounting options on back of pump.
Fig. 3. Use the box blade to cut out an exit window for theelectrical cords in the clear plastic container.
Fig. 4. Mark screw locations in protective box with a permanentmarker then drill holes in clear plastic container.
Fig. 5. Place the protective box in desired location on top or sideof refrigerator then mark screw placement holes with a perma-nent marker. Use the 3/16 drill bit to drill through the refrig-erator wall just deep enough to place the dry wallanchors. Hammer the dry wall anchors into the holes in therefrigerator.
172 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
the finger into a shallow pan or bucket leading theirmouth to the source of milk. For foals that drinkwell from a bottle but have difficulty learning todrink from a bucket, a Calf-Mate calf nursing buck-etd can be purchased at www.eNasco.com and mod-ified by cutting the end of a smaller human or goatnipple to fit the output.
Several commercially available foal specific milkreplacers can be ordered online or found at local feedstores. The author’s hospital most commonly usesMares Matche by Land O’Lakes or Foals Firstf byProgressive Nutrition, as we have had more successwith palatability and less incidence of diarrhea with
these brands. Follow the packaged instructionscarefully for preparation of the product. Somechoose to dilute the foal replacer to half strength for
Fig. 6. Place the pump inside the container, and use the Phillipsscrewdriver to screw in the mounting screws provided with thepump.
Fig. 7. Mark the area for milk tube placement through the sideof the refrigerator just below the freezer coil shelf. Use the 1⁄4inch drill bit to drill a hole through the side of the refrigerator.
Fig. 8. Measure and cut the required length of tubing to runbetween the input port on the pump, through a hole drilled intothe side of the refrigerator, and down to the bottom of the chosenmilk receptacle. Attach standpipe to bottom of tubing and placeat bottom of receptacle.
Fig. 9. Attach the remaining tubing to the output port of thepump. This will be used to run into the bucket where the foal ishoused and secured with cable ties.
AAEP PROCEEDINGS � Vol. 60 � 2014 173
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
the first few feedings to acclimate the foal to taste ifit was originally nursing from a mare and to avoidconstipation. Avoid any sudden change in brandsof milk replacer. The average foal requires 10 to15% of its body weight in milk the first few feedingsand then 25 to 35% of its body weight after that untilit gradually begins to be able to digest disaccharidesand fiber between 2 and 4 months when the Maltaseand Sucrase enzymes increase in levels and cecalmicroflora are established.4 The weight of milk isapproximately 1 kg/1 L so a 50 kg foal will need atleast 5 L a day in the first few days and gradually beincreased to 12.5 to 15 L as it grows. The averagefoal will gain 2 to 3 pounds a day.3 The timer onthe machine is set to dispense the desired amount ofmilk per hour. We begin by setting the timer at 2minutes per hour, which will dispense an approxi-mated 300 mL an hour or 7.2 L a day. The chosenreceptacle needs to be small enough, placed at theproper height, and possibly placed at a slight angleso that the foal’s muzzle can fit to the bottom anddrink the entire amount. As the foal grows, thetimer is changed to pump for longer time periodsdistributing larger volumes of milk and at decreasedintervals. The pump can be used until it is possibleto get down to a more owner manageable 5 times aday feeding at around 6 weeks old or used for thefirst several months until it is eating a normal diet.Once the pump is done being used for a particularfoal, 10% bleach water is pumped through the pumptubing followed by distilled water and then air todisinfect and store.
3. Results
The described device has worked well in our hospitalsetting, and as previously described, we often sendthem home with orphan foals for a monthly rentalfee or more distant clients chose to purchase thedevice. We have used this automated method forover 20 orphan foals in our practice. The foalsquickly learn the sound of the pump when it isactivated and run to the bucket to drink. The foalsgained weight at an average pace and no significantdiarrhea, colic, or constipation was encountered.The owners gave positive reviews regarding thefunctionality and convenience of the device when itwas returned for a deposit refund. We did have aninstance in which the tubing required replacementdue to damage by mice trying to reach the milkinside. The programmable pump was programmedas needed to gradually increase the volume and de-crease the frequency of feedings as the foal grew and
the intestines adapted to the introduction of rough-age and grains.
4. Discussion
Having a programmable automated device availableto offer allocated amounts of milk replacer to anorphaned foal can be a very convenient time andmoney saving option. Additionally, it can mimic amore natural feeding schedule. This can help avoidoverfilling of the stomach, which can lead to delayedgastric emptying and proliferation of enteric patho-gens.3 More frequent meals can decrease the inci-dence of gastric ulceration as well as maintainglucose levels and gut motility in the foal.3 Thefoals will also avoid being exposed to frequent hu-man bonding as in a bottle feeding situation, whichcan lead to later behavioral problems. Presentingthe option of a relatively inexpensive automaticfeeding device is a good way to offer clients somepeace of mind in a stressful situation. Althoughtheir mare may have passed away or rejected herfoal, they do not need to worry about the foal’sgrowth potential. Owners that typically visit thebarn twice daily for morning and evening feeds havethe ability to program and fill the device at thesetimes without missing work or hiring extra staff tofeed an orphaned foal. Veterinary hospitals with-out 24 hour staff can also benefit from the availabil-ity of this device for overnight feedings.
Acknowledgments
Conflict of InterestThe Author declares no conflicts of interest.
References and Footnotes1. Paradis MR. Feeding the orphan foal, in Proceedings.
Am Assoc of Equine Pract 2012;58:402–406.2. Dunkel B. Nutrition of the neonatal orphaned foal, in Pro-
ceedings. Brit Equine Vet Assoc Congress 2010;49:192.3. Knottenbelt DC, Holdstock N. Madigan J. Equine Neonatol-
ogy Medicine and Surgery. London: Saunders; 2004:459–469.
4. Paradis MR. Normal Foal Nutrition, in Proceedings. AmAssoc of Equine Pract 2012;58:399–401.
aKenmore 3.3 cu.ft. Compact Refrigerator, Kenmore, HoffmanEstates, IL 60169.
bSterilite Corporation, Townsend, MA 01469.cCannon Water Technology Inc., Rocklin, CA 95765.dCalf-Mate Calf Feeder, Fortiflex, Miami, OK 74354.eMares Match foal milk replacer, Land O Lakes Animal Milk
Percutaneous liver biopsy is regarded as the bestantemortem test for equine hepatopathy. Blindliver biopsies are still performed by practitioners,despite potential associated risks such as pneumo-thorax or hemorrhage. Direct or indirect ultra-sound guidance allows for identification of the mostappropriate site for liver biopsy. Our goal was toidentify the frequency of sonographic identificationof adequate liver tissue for biopsy in the publishedblind liver biopsy locations.
2. Materials and Methods
Serum liver parameters were evaluated in 36 mid-dle-aged Quarter Horses to ensure that only horseswith normal liver function were included in thestudy. The published blind liver biopsy region, justbelow a line drawn between the dorsal aspect of thetuber coxae and the point of the elbow in the right11th to 14th intercostal spaces, was examinedsonographically.
3. Results and Discussion
Only 39% of horses had liver visualized in the pub-lished blind liver biopsy region. None of the 36horses had liver of adequate thickness for biopsy inthe published region. When liver was not visible,lung was visualized instead in 55% of horses, bowelin 36% of horses, and both bowel and lung in 9% ofhorses. In many horses, liver tissue may be inade-quate for biopsy in the published blind biopsylocations.
Acknowledgments
Supported by a grant from the Department of Vet-erinary Large Animal Clinical Sciences, College ofVeterinary Medicine and Biomedical Sciences,Texas A&M University.
Conflict of Interest
The Authors declare no conflicts of interest.
AAEP PROCEEDINGS � Vol. 60 � 2014 175
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Research Abstract
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Owner-Reported Response to Treatment of130 Headshaking Horses
Kirstie J. Pickles, BVMS, MSc, PhD, CertEIM, DECEIM;Monica Aleman, MVZ Cert, PhD, DACVIM†; David J. Marlin, BSc(Hons), PhD;Vicki J. Adams, BSc, DVM, MSc, PhD, MRCVS; andJohn Madigan, DVM, MS, DACVIM, DACAW*
Idiopathic headshaking has been recognized for overa hundred years1,2 and is a spontaneously occurringdisorder of mature horses causing violent head flick-ing, snorting, and muzzle rubbing. Due to this lo-calization of clinical signs to the head, and inparticular muzzle area, it has long been suspectedthat the disease pathogenesis involves the trigemi-nal nerve.1,3,4 Recently a decreased threshold fortrigeminal nerve activation has been confirmed inheadshaking horses compared to controls.5 Thelimited pathological studies performed to date havefailed to determine any structural abnormalities ofthe trigeminal nerve, and therefore a functional dis-order is proposed.5,6 Other unexplained features ofheadshaking include the predisposition of geldings
to the disease and the seasonality of clinical signs.7,8
This seasonality and the fact that some horses gointo spontaneous remission suggests that the docu-mented aberrant activity of the trigeminal nervemay be reversible. However, due to our limitedunderstanding of the etiopathogenesis of headshak-ing, current treatments are primarily directed atminimizing clinical signs and discomfort rather thancorrecting anomalous trigeminal neurophysiologyand, consequently, have limited efficacy in manyhorses.4,9 There are few large scale studies report-ing success rates of the various treatments for head-shaking, which makes it difficult for veterinarians toprovide such advice to owners. The aim of thisstudy was to undertake a survey of owners of head-shaking horses to determine the reported successrate of commonly utilized therapies.
176 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
2. Materials and Methods
Questionnaires
An online questionnaire was designed using SurveyMonkeya. The questionnaire contained 3 sections.The first section comprised 27 questions regardingthe horse’s signalment and general management.Section 2 contained 15 questions regarding thehorse’s headshaking including if the horse was cur-rently headshaking, which months of the year head-shaking occurred, which month headshaking wasworst, evidence of seasonality and weather relatedheadshaking behavior, and if headshaking hadbeen diagnosed by a veterinarian. Additionally,owners were asked to complete a checklist of 20particular headshaking behaviors for their horseand a 15 item checklist about activities associatedwith their horse’s headshaking. Section 3 com-prised 11 subsections regarding 11 possible head-shaking treatments: nose net, face mask, fly control,cyproheptadine, carbamazepine, corticosteroids,non-steroidal anti-inflammatories (NSAIDs), anti-histamines, melatonin, magnesium, and combinedmelatonin and magnesium therapy. If a particulartreatment had not been used, the respondent wasdirected to the next treatment subsection. Withineach treatment subsection, owners were asked tospecify what time of year the treatment had beentrialed, describe the particular treatment (e.g., typeof nose net) and dosage and administration details ifappropriate (including if product was generic orcompounded), if any response was observed (com-pletely stopped headshaking, marked improvement,some improvement, no change, or worsened head-shaking), and if any side effects of treatment werenoted. The questionnaire was advertised via head-shaking website forums and via Facebookb. Linksto the questionnaire remained open for 2 months.
Data Analysis
Results are reported descriptively. A positivetreatment outcome was deemed as improvement inheadshaking behavior and was calculated as thesum of completely stopped headshaking, marked im-provement, and some improvement responses. Anegative treatment outcome was described as noimprovement or worsening of headshaking and wascalculated as the sum of no change and worsenedheadshaking responses. For geographical compar-isons, data was assigned a location of North Amer-ica, Europe, or Australasia. Mann Whitney testswere used to examine 2 non-paired variables.
3. Results
Questionnaire Response
Questionnaires were completed by 137 respondents.The treatment section was not completed by 7 re-spondents giving 130 useable question-naires. Some respondents gave incomplete detailsfor a particular treatment giving a useable response
range of 122 to 130 (median 127) for individualtreatments. Responses were received from the UK(n � 49), U.S. (n � 45), Canada (n � 8), mainlandEurope (n � 11, 3 each from France and Germanyand 2 from The Netherlands), Australia (n � 3), andNew Zealand (n � 5).
Description of Headshaking HorsesThe median (range) age of the population of head-shaking horses was 11 (2–27) years with a median(range) length of ownership of 6 (0–20) years. Mostbreeds were represented with Thoroughbred (in-cluding crosses) and Quarter Horse being most fre-quent comprising 22% and 14% of the population,respectively. Almost half of the horses were usedfor light activities only with 24% used for hacking/trail riding, 16% for pleasure riding, and 8% beingretired/companion animals. Dressage was themost frequent competitive discipline performed byheadshakers, reported by 13% of owners.
Of the 132 horses for which data were available,84 (64%) had been diagnosed with idiopathic head-shaking by a veterinarian. Headshaking behaviorwas seasonal in 79/132 (60%) horses whilst 53/132(40%) displayed clinical signs all year or randomlyintermittently, without any apparent predictability.The most common headshaking signs displayedwere “vertical shaking of the head” (121/132; 92%),“acting as if an insect flew up its nose” (112/132;
Table 1. Prevalence of Owner-Reported Clinical Signs and Effect ofWeather in 132 Headshaking Horses
Clinical sign Prevalence (%)
Shaking or flipping the head in a verticalplane 121 (92)
Acting as if an insect had flown up thenose 112 (85)
Rubbing the nose/muzzle on objects 108 (82)Snorting 92 (62)Rubbing nose/muzzle on ground while
moving 81 (61)Striking at nose/muzzle with front foot 70 (53)Anxious expression 59 (45)Headshaking reduced at night 59 (45)Stumbling 42 (32)Staring into space 38 (29)Horizontal headshaking 37 (28)Reluctance to move 36 (27)Panic following staring episodes 32 (24)Avoids light 32 (24)Seeks shade 32 (24)Licking or smacking of lips or excessive
opening and closing of mouth 28 (21)Worse when sunny 33 (25)Worse when windy 29 (22)Worse when rainy 13 (10)Worse when humid 7 (5)Better when cloudy 14 (11)Better when rainy 13 (10)
AAEP PROCEEDINGS � Vol. 60 � 2014 177
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
85%), and “rubbing of the muzzle on objects” (108/132; 82%). Headshaking clinical signs varied withthe weather in 91/132 (69%) of horses and was worsewhen exposed to bright light in 52 horses (39%).The prevalence of headshaking clinical signs isshown in Table 1. Horses with a veterinary diag-nosis of headshaking were more likely to show ex-cessive snorting of the nose (P � 0.05), reluctance tomove (P � 0.007), striking at nose/muzzle with frontfoot (P � 0.02), have an anxious facial expression(P � 0.0009), and stare out into space as if seeingimaginary objects (P � 0.009) compared to owner-diagnosed headshaking horses. These horses werealso more likely to display clinical signs when at restin the stable (P � 0.05), when lunged without tack(P � 0.01), when ridden at canter (P � 0.003), whenwalked in hand in a bridle (P � 0.04) or halter (P �0.02), and when eating grass (P � 0.05).
For the 131 owners that gave data, 9 (7%) de-scribed their horse’s headshaking as mild (occa-sional headshaking, rarely interferes with ridingactivity), 35 (27%) as moderate (some headshaking,interferes somewhat with riding activity), 41 (31%)as severe (frequent headshaking, interferes greatlywith riding activity), and 46 (35%) as very severe(frequent headshaking, impossible to perform ridingactivity). Owners of horses with a veterinary diag-nosis rated their horse’s headshaking as more se-vere than owner-diagnosed horses (P � 0.007).
Treatment Outcome
Nose NetNose nets had been used by 110/128 (86%) respon-dents. Of those that had tried nose nets, 91 (83%)had used half nets extending from the noseband tocover the upper jaw and lip, 43 (39%) had used fullnose nets covering both the upper and lower jawsand lips below the noseband, and 24 (22%) had triedboth types of nose nets. A further 4 owners had
used homemade nose nets made from nylon stock-ings, 1 used ropes dangling from the noseband and 1used a dangling fringe from the browband.
A positive outcome was reported by 58/110 (53%)owners; 6 horses (5%) completely stopped headshak-ing, 21 (19%) showed marked improvement, and 31(28%) showed some improvement (Table 2). Anyimprovement was seen immediately upon placementof the nose net although some horses required sev-eral sessions of wearing the net to accommodate itsuse. Six respondents said that the positive effect ofthe nose net had waned over time. A negative out-come was reported by 52 (47%) of owners with 40horses (36%) showing no response and 12 horses(11%) headshaking worse with use of a nose net(Table 1). Negative side effects were shown by 32horses (29%) of horses using nose nets with irrita-tion by the net (24 horses) and panic (5 horses)described most frequently. There was no signifi-cant difference between half or full nets in outcomeor the presence of adverse effects.
Face Mask
Face masks had been used as a treatment on 83/130(64%) headshaking horses with 42 (51%) of thesemasks containing UV eye shades. Forty-four (53%)horses had a positive outcome from face mask usewith 3 (4%) horses completely stopping headshak-ing, 13 (16%) showing marked improvement, and 28(34%) showing some improvement (Table 2). Anegative outcome was observed in 39 (47%) horseswith 32 (39%) showing no response and 7 (8%)horses becoming worse following face mask use (Ta-ble 2). Negative side effects were noted in 18 (22%)horses with “spookiness,” tripping due to diminishedvision and worsening of headshaking most fre-quently cited. The presence of UV eye shades didnot affect outcome or occurrence of adverse effects.
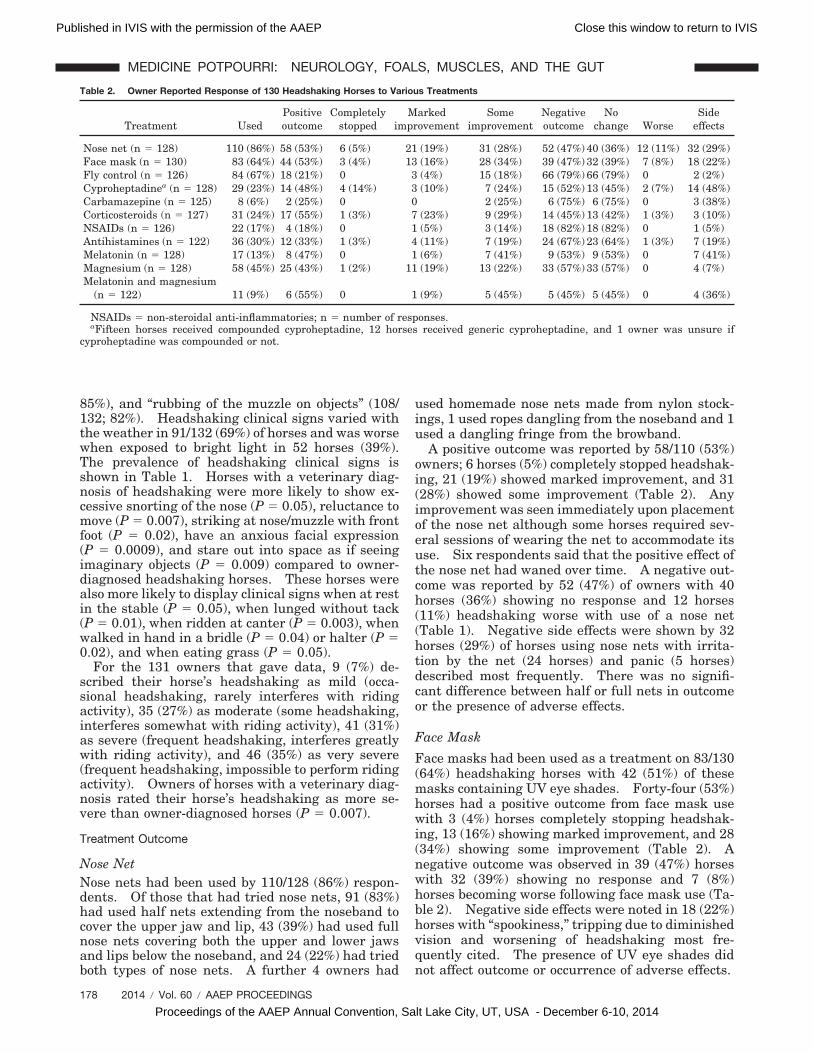
Table 2. Owner Reported Response of 130 Headshaking Horses to Various Treatments
NSAIDs � non-steroidal anti-inflammatories; n � number of responses.aFifteen horses received compounded cyproheptadine, 12 horses received generic cyproheptadine, and 1 owner was unsure if
cyproheptadine was compounded or not.
178 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Insect/Fly ControlInsect control had been used by 84/126 (67%) of own-ers in an attempt to decrease headshaking. Ofthese, 18 (21%) reported a positive outcome, with 3(4%) horses showing marked improvement and 15(18%) some improvement immediately upon use (Ta-ble 2). No horses displayed increased headshakingfollowing insect control measures. Two horses (2%)had negative side effects (skin irritation) followingtreatment.
CyproheptadineCyproheptadine treatment had been used by 29/128(23%) of owners to control their horses’ headshaking.Fifteen horses received compounded cyproheptadine,12 horses received generic cyproheptadine, and 1owner did not know if cyproheptadine was com-pounded. Six owners reported administering 0.3mg/kg, 2 owners stated 0.1 mg/kg, 15 owners did notknow the administered dose, and dosage was unableto be determined from information given by 6 own-ers using compounded product. Nineteen ownersreported administering cyproheptadine twice daily,2 owners once daily, and 8 owners did not reportfrequency of dosing.
Fourteen horses (48%) had a positive outcomewith cyproheptadine treatment: 4 (14%) stoppedheadshaking completely, 3 (10%) showed markedimprovement, and 7 (24%) showed some improve-ment (Table 2). Fifteen horses (52%) had a nega-tive outcome with 13 (45%) having no change and 2(7%) having worsening of headshaking. The me-dian (range) time to observe a positive responseoccurred 3 (2–14) days following initiation of ther-apy. Additionally, 1 owner reported that clinicalsigns resumed within 2 days of cyproheptadine with-drawal. Three owners described a transient effectsuch that headshaking recurred during administra-tion; 2 of these horses received generic cyprohepta-dine and 1 received compounded product. Oneadditional owner commented that cyproheptadinehad stopped working when changed to compoundedproduct. Adverse effects were reported in 14 (48%) ofhorses receiving cyproheptadine including lethargy,drowsiness, incoordination, colic, and irritability.
CarbamazepineCarbamazepine therapy had been tried by 8/125owners (6%), 2 of which reported some improvementand the remaining 6 reported no change in head-shaking (Table 2). Improvement occurred withinseveral weeks in 1 horse and was not reported forthe other improved headshaker. One owner re-ported administration of 5 mg/kg 3 times daily, 6owners did not know the dosage administered, andthe dosage could not be extrapolated from the infor-mation given by 2 respondents. Five of thesehorses with an unknown dosage received carbamaz-epine twice daily and 1 three times daily. Adverseeffects of lethargy and drowsiness were reported in 3horses.
CorticosteroidsCorticosteroid therapy had been given to 31/127(31%) of headshakers. Of these, 9 received oralsteroids, 12 were administered injectable steroids, 6were given dexamethasone pulse therapy (DPT),and 2 horses received inhalational medication.A positive outcome was reported in 17/31 (55%) ofhorses of which 1 completely stopped headshaking, 7(23%) showed marked improvement, and 9 (29%)had some improvement (Table 2). Improvementwas most frequently described by owners (7/12) asoccurring a few days after treatment commenced.Three owners reported a transient improvementonly. A negative outcome was noted in 14 (45%) ofhorses with 13 (42%) having no change and onebecoming worse following therapy. Adverse effectswere observed in 3 horses (10%) and comprised 1each of increased appetite, lethargy, and mania (asdescribed by owner).
NSAIDsNSAID therapy had been used by 22/126 (17%) ofowners for treatment of their horses’ headshaking.Phenylbutazone was listed as the most frequentlyadministered NSAID (13/18 responses). Fourhorses (18%) improved with NSAID therapy with 1horse showing marked improvement and 3 horses(14%) showing some improvement whilst the re-maining 18 horses (82%) showed no change in head-shaking (Table 2). Hives were listed as an adverseeffect of treatment in one horse.
AntihistaminesAntihistamine treatment had been used in 36/122(30%) of headshaking horses. Most frequently useddrugs were chlorpheniramine (9 horses), hy-droxyzine hydrochloride (8 horses), loratadine ordesloratidine (8 horses), diphenhydramine (7horses), and pseudoephedrine hydrochloride pyril-amine maleate (3 horses). A positive outcome wasdescribed within a few days to a few weeks in 12(33%) of horses with 1 horse completely ceasingheadshaking, 4 horses (11%) showing marked im-provement, and 7 horses (19%) mildly improving(Table 2). A negative outcome was seen in 24 (67%)horses with no change in 23 (64%) and increasedheadshaking in 1 horse. Adverse effects were ob-served in 7 horses (19%) with drowsiness cited mostfrequently.
MelatoninMelatonin had been administered to 17/128 (13%) ofhorses, all of which were located in the U.S. exceptone in Canada and one in the Southern hemisphere.Dose range was 12 to 20 mg with 15 mg once dailycited most frequently (6 responses). Ten respon-dents reported giving melatonin at 5 PM/dusk, 1administered melatonin in the morning, and 1 gavemelatonin twice daily. Six horses started melato-nin therapy in winter, 6 in spring, and 5 in the
AAEP PROCEEDINGS � Vol. 60 � 2014 179
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
summer. Eight horses (47%) responded positivelyto melatonin within 1 to 4 weeks of therapy; markedimprovement was seen in 1 horse (the horse givenmelatonin in the morning) and some improvementin the remaining 7 (including the horse given mela-tonin twice daily) (Table 2). No change in head-shaking was reported in 9 (53%) of horses. Sevenhorses (41%) had a longer hair coat or did not shedtheir winter coat whilst on melatonin.
MagnesiumDietary supplementation with magnesium had beenused by 58/128 (45%) of owners as a headshakingtreatment. Magnesium oxide was the most com-mon formulation reported (26 responses) followed bymalate (7 responses). Doses of 5 to 40 g were re-ported. A positive outcome was reported in 25horses (43%) within 2 days to 4 weeks of initiatingtherapy; additionally 1 owner reported headshakingworsened within a couple of days of stopping mag-nesium supplementation. One horse completelystopped headshaking, 11 (19%) showed marked im-provement, and 13 (22%) showed mild improvement(Table 2). A negative outcome was noted in 33horses (57%) in which no change in headshakingwas observed. Two owners reported that theirhorse seemed calmer whilst on magnesium, whereas1 owner each reported nervousness and diarrhea asadverse effects.
Melatonin and MagnesiumOnly 11/122 (9%) owners had used melatonin andmagnesium combination therapy to treat theirhorses’ headshaking. Six horses (55%) respondedpositively with 5 horses (45%) showing some im-provement and 1 horse (10%) marked improvementin headshaking whereas 5 horses (45%) had nochange (Table 2). All respondents who gave data(n � 7) used a dosage of 15 to 20 mg melatonin(median 15 mg) at 5 PM and 5 to 40 g magnesium.Two owners initiated combination therapy in spring,5 in summer, and 4 in winter. Adverse effects wereobserved in 4 horses (36%), 3 of which did not shedtheir winter coat and 1 which gained weight andbecame lethargic approximately 1 month after ther-apy was initiated.
4. Discussion
Treatment of headshaking horses is challenging astherapies are largely directed towards managingclinical signs rather than treating the cause itself,which remains elusive. There are a plethora oftreatments recommended and utilized for manage-ment of headshaking; however, reported rates ofsuccess of such treatments are rare and often con-tain limited numbers of horses. This study de-scribes the owner-reported outcome of 11 treatmentsused in the management of idiopathic headshakingin 130 horses.
The demographics of the survey population andprevalence of clinical signs were similar to that de-
scribed in other headshaking studies.7,8 Somevariation in observed clinical signs existed betweenhorses diagnosed by owners and veterinarians, withthe latter group representing a more severely af-fected cohort, as previously reported.10 Ownershave proven reliable at using the clinical signs ofvertical headshaking, rubbing the nose on the tho-racic limb, and snorting for the diagnosis of idio-pathic headshaking.10 As vertical headshakingwas observed in over 90% of horses in this study, itis likely that owner-diagnosed horses were true id-iopathic headshakers; however, other causes ofheadshaking cannot be excluded. Likewise, detailsof the veterinary diagnostic procedure of the veteri-narian-diagnosed horses are also unknown. Infield situations, veterinarian diagnosis of headshak-ing, like owner assessment, is usually based on ob-servation and history. A single veterinary examhas limitations, and there is no diagnostic test forheadshaking. Idiopathic headshaking is a constel-lation of signs, which persist in the absence of arider, independent of tack, and apparent lack ofunderlying pathology (i.e., sinus mass, iris cyst,etc.).4,11,12 The authors, therefore, feel that veteri-nary diagnosis and owner assessment of clinicalsigns, which are the basis of any headshaking diag-nosis, are both equally valid.
Nose nets were the most frequently used treat-ment for headshaking having been used by almost90% of respondents. Whereas some degree of im-provement was seen in over 50% (58/110) of horses,complete resolution of headshaking was rare andobserved in only 5%. These improvements arelower than that previously reported where use ofnose nets resulted in some decrease in clinical signsin 75% of 36 headshakers in the UK13 but greaterthan the 33% improvement reported in the U.S.7
Geographical location was not analyzed in this studydue to the heterogeneous nature of the data. Inthis study, nose nets resulted in one of the highestrates of positive outcome and, therefore, represent asimple first-line therapeutic option. Such physicaltreatments avoid competition medication regula-tions; indeed, the use of nose nets is now permittedin some equestrian disciplines. Adverse effects ofnose nets have not been previously reported, to theauthors’ knowledge, but were observed in approxi-mately 1⁄3 of horses and were reported for both typesof nose net. Owners should, therefore, be advisedof the possibility of irritation or panic upon theirapplication. The method by which nose nets reduceclinical signs of headshaking is unknown; however,it is postulated that they reduce aversive stimula-tion of hyperesthetic areas or, alternatively, the con-stant presence of the net might work by adjacentreceptor field inhibition or receptor adaptation of thecontact area.14 Interestingly, some owners re-ported a waning of clinical effect with time raisingthe possibility of habituation.
A positive treatment outcome of 53% (44/83) ofheadshaking horses with a face mask was similar to
180 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
that previously reported7,9 and equivalent to use of anose net in this study, although 20% fewer respon-dents had tried them. Again, adverse effects notpreviously reported such as “spookiness” and stum-bling due to presumed reduced vision were frequentand observed in over 1⁄5 of horses using face masks.Whereas observed less frequently than with use of anose net, these reported adverse effects were of amore disruptive nature.
A surprisingly large percentage of horses (21%;18/84) were reported to derive some benefit from theuse of fly control, in contrast to only 2% previouslydescribed.7 The current study population mayhave comprised more mildly affected horses than theaforementioned study,7 despite 2⁄3 of owners describ-ing their horse’s headshaking as “severe” or “verysevere.” It is likely that a positive outcome rate ofapproximately 20% is heavily influenced by re-sponse bias, as no treatment achieved lower than18% positive outcome. Such bias may have arisenfrom multiple sources including the difficulty in ob-jective assessment of headshaking and any treat-ment response, a proxy-placebo effect, thephenomena of spontaneous and seasonal remission,fluctuation of clinical signs, regression to the mean,any contemporaneous treatments, and recall bias.Whereas such bias limits interpretation of all ob-served responses to treatments, the variability inreported outcomes gives confidence that a genuinetreatment effect, above and beyond any bias, wasnoted for some treatments.
The positive response of over 50% (17/31) of head-shakers to corticosteroid therapy was also unex-pected given the documented aberrant trigeminalnerve activity5 and the failure of a recent blinded,clinical trial of pulsed high dose dexamethasonetherapy to have any effect on idiopathic headshak-ing.15 Whereas not a first-line treatment for neu-ropathic pain, corticosteroids have been shown toreduce spontaneous discharge in injured nerves andmight be useful as adjunct therapy.16 Althoughnerve injury is not suspected in idiopathic head-shaking, a reduced threshold for activation of thetrigeminal nerve has been documented5 and cortico-steroids might act to decrease such aberrant activ-ity. It is also possible that, in the respondingsubset of headshaking horses, there was a degree oflow grade inflammation or allergy contributing toclinical signs observed by owners. As prolonged,ongoing management of headshaking is usually re-quired, corticosteroids are unlikely to be useful as atherapeutic option due to the risk of serious adverseeffects such as laminitis.
One-third of owners reported general antihista-mine treatment improved their horse’s headshaking(12/36). Such improvement may suggest an aller-gic component to headshaking in these horses; how-ever, the reported effect may be largely due to biasas previously discussed. A positive response to cy-proheptadine treatment was observed in approxi-mately 50% of horses (14/29). Cyproheptadine is a
first generation antihistamine with additional anti-cholinergic, antiserotonergic, calcium channel block-ing, and local anesthetic activity,17 which is used totreat human vascular headaches. Previous reportsdescribing the response of headshaking to cyprohep-tadine treatment has varied widely, from no im-provement4,18 to 70%.7 Such variation in efficacy isdifficult to explain. The percentage of horses with aphotic component to their headshaking is variableacross these studies (none4; 39%, current study;60%7), which may be relevant in responsiveness tocyproheptadine. Inappropriate dosage may haveaffected treatment outcome with cyproheptadine inthe current study as, whereas only 2 owners re-ported using an inadequate dosage, many ownersreported they did not know or omitted administra-tion details. Adverse effects such as lethargy anddrowsiness were noted in almost 50% of horsestreated with cyproheptadine, which is likely to limitits use in ridden horses.
Carbamazepine, an anticonvulsant, which stabi-lizes voltage-gated sodium channels, had one of thelowest positive outcome rates of all treatments (25%;2/8) and, therefore, does not appear to be an effica-cious treatment for headshaking. Additionally,negative side effects were reported in 1⁄3 of treatedhorses. Although carbamazepine is the treatmentof choice for human trigeminal neuralgia,19 thepharmacokinetics of this drug in horses is unknown,which may explain its lack of effect. Additionally,recent trigeminal electrophysiological data suggeststhe etiopathogenesis of equine headshaking and hu-man trigeminal neuralgia may differ.5 NSAIDswere also poorly efficacious (22%; 4/22) as would beexpected in the treatment of a neuropathic condi-tion. The noted response in 4 horses may be due tothe aforementioned biases.
Melatonin reduced headshaking in almost half(47%; 8/17) of horses in this study. The hypothesisfor melatonin treatment of headshaking is that alate afternoon (5 PM) dose of melatonin artificiallymanipulates photoperiod such that, biologically, thehorse remains in winter. Approximately 40% oftreated horses did not shed their coat due to thisphenomenon. Therapy is proposed to be most suc-cessful when melatonin is started before the onset ofspring for seasonal headshakers7and, therefore, ini-tiation of therapy when the horse was already head-shaking may have reduced efficacy. A positiveoutcome in the two horses given melatonin inappro-priately and the fact that suppression of the vernalincrease in gonadotropins did not reduce headshak-ing20 may question the proposed rationale. How-ever, melatonin is also able to modulate pain,including neuropathic pain, via various antinocice-ptive effects including activation of opioid receptors,inhibition of pro-inflammatory cytokine production,modulation of GABAA receptor function and actingas a free radical scavenger.21 Melatonin receptorshave been identified in the trigeminal ganglion andtrigeminal nucleus of mammals22 and interestingly,
AAEP PROCEEDINGS � Vol. 60 � 2014 181
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
melatonin has been shown to attenuate an induciblemodel of trigeminovascular nociception in rats.23
Melatonin might, therefore, act to reduce headshak-ing by mechanisms other than photoperiod manipu-lation. Only 13% of owners had used melatonintreatment, and all except one of these were based inNorth America, where the drug is cheaply availableas an “over the counter” product. Whereas melato-nin can be purchased with a veterinary prescriptionin other countries such as the UK, this does notappear to be occurring, most likely due to veterinar-ians being currently unaware of the protocol. Mel-atonin, as an endogenous hormone, also has theadvantage of having no restrictions for use in com-petition horses. Given that almost half of head-shakers improved with melatonin therapy, with onlywinter coat retention as an adverse effect, this treat-ment warrants further attention.
Magnesium supplementation had been used byalmost 50% of owners, with just under half of these(25/58) reporting an improvement in their horse’sheadshaking. Magnesium increases the activationthreshold of nerves such that a greater stimulus isrequired for depolarization.24 Magnesium, there-fore, appears a rational therapy given the reducedactivation threshold of the trigeminal nerve in head-shaking horses.5 Formulations of magnesium varyin their oral bioavailability with that of magnesiumoxide (the most frequently administered in thisstudy) reported to be questionable in the horse.25
Generally availability of magnesium in horses ishigh and feeding high percentages of roughage en-hances its absorption from the gastrointestinaltract.26 From this study, toxicity from daily mag-nesium supplementation of up to 40 g appears to berare, although it may be advisable to periodicallymeasure ionized magnesium concentrations. Mag-nesium may be another useful treatment for com-peting headshaking horses. Combiningmagnesium and melatonin therapy appeared to bebeneficial, resulting in an improved outcome thanuse of either treatment alone (55%; 6/11). Indeed,combined therapy had the highest overall positiveoutcome; however, this should be interpreted withcaution, as only 11 owners had used this treatment.
This study can be used to guide owners in themanagement of idiopathic headshaking. Owner-reported responses to treatment in 130 headshakinghorses suggest that nose nets, face masks, and mag-nesium supplementation are the most efficaciousnonmedical therapeutic options. Adverse effectssuch as facial irritation were reported in 1⁄3 of horseswith nose nets. Cyproheptadine, corticosteroids,and melatonin were the most successful pharmaceu-tical treatments in this study; however, the numberof horses using these therapies was low and, there-fore, these results should be interpreted with cau-tion. Of these pharmaceutical drugs, onlymelatonin is without significant adverse effects orallowed in competition horses. Veterinary diagno-sis of idiopathic headshaking is advised before com-
mencing any treatments. Further investigation ofthe pathophysiological mechanism underlying theaberrant trigeminal nerve activity in headshakinghorses is warranted in order to develop more suc-cessful therapeutic options.
Acknowledgments
Conflict of InterestThis study was funded by anonymous private dona-tion to the Equine and Comparative Neurology Re-search Group.
References and Footnotes1. Williams WL. Involuntary twitching of the head relieved by
trifacial neurectomy. J Comp Med Vet Arch 1897;18:426–428.2. Williams WL. Involuntary shaking of the head and its treat-
ment by trifacial neurectomy. Am Vet Rev 1899;23:321–326.3. Madigan JE, Kortz G, Murphy C, et al. Photic headshaking in
the horse: 7 cases. Equine Vet J 1995;27:306–311.4. Newton SA, Knottenbelt DC, Eldridge PR. Headshaking in
horses: Possible aetiopathogenesis suggested by the resultsof diagnostic tests and several treatment regimes used in 20cases. Equine Vet J 2000;32:208–216.
5. Aleman M, Williams DC, Brosnan RJ, et al. Sensory nerveconduction and somatosensory evoked potentials of the tri-geminal nerve in horses with idiopathic headshaking. J VetInt Med 2013;27:1571–1580.
6. Newton SA. The functional anatomy of the trigeminal nervein the horse [dissertation]. Liverpool, UK: University ofLiverpool; 2001.
7. Madigan JE, Bell SA. Owner survey of headshaking inhorses. J Am Vet Med Assoc 2001;219:334–337.
8. Mills DS, Cook S, Taylor K, et al. Analysis of the variationsin clinical signs shown by 254 cases of equine headshaking.Vet Rec 2002;150:236–240.
9. Mills DS, Cook S, Jones B. Reported response to treatmentamong 245 cases of equine headshaking. Vet Rec 2002;150:311–313.
10. Taylor K. An evaluation of equine headshaking syndromeand its management [dissertation]. Leicester, UK: DeMontfort University; 2004.
11. Lane JG, Mair TS. Observations on headshaking in thehorse. Equine Vet J 1987;19:331–336.
12. Berger JM, Bell SA, Bradford BJ, et al. Successful treat-ment of head shaking by use of infrared diode laser deflationand coagulation of corpora nigra cysts and behavioral modi-fication in a horse. J Am Vet Med Assoc 2008;233:1610–1612.
13. Mills DS, Taylor K. Field study of the efficacy of three typesof nose net for the treatment of headshaking in horses. VetRec 2003;152:41–44.
14. Raj SN, Meyer RA, Ringkamp M, et al. Peripheral neuralmechanisms of nociception. In: Wall PD, Melzack R, eds.Pain 4th ed. Edinburgh: Churchill Livingstone, 1999;11–57.
15. Tomlinson JE, Neff P, Boston RC, et al. Treatment ofidiopathic headshaking in the horse with pulsed high dosedexamethasone. J Vet Intern Med 2013;27:1551–1554.
16. Watanabe S, Bruera E. Corticosteroids as adjuvant analge-sics. J Pain Symptom Manage 1991;9:442–445.
17. Lowe DA, Matthews EK, Richardson BP. The calcium an-tagonistic effects of cyproheptadine on contraction, mem-brane electrical events and calcium influx in the guinea-pigtaenia coli. Br J Pharmacol 1981;74:651–663.
18. Mair TS. Assessment of bilateral infra-orbital nerve block-ade and bilateral infra-orbital neurectomy in the investiga-tion and treatment of idiopathic headshaking. Equine Vet J1999;31:262–264.
19. Attal N, Cruccu G, Baron R, et al. EFNS guidelines on thepharmacological treatment of neuropathic pain: 2010 revi-sion. Eur J Neurol 2010;17:1113–1123.
182 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
20. Pickles KJ, Berger J, Davies R, et al. Use of a gonadotro-phin-releasing hormone vaccine in headshaking horses. VetRec 2011;168:19.
21. Ambriz-Tututi M, Rocha-Gonzalez HI, Cruz SL, et al. Mel-atonin: A hormone that modulates pain. Life Sci 2009;84:489–498.
22. Weaver DR, Rivkees SA, Reppert SM. Localization andcharacterization of melatonin receptors in rodent brain by invitro autoradiography. J Neurosci 1989;9:2581–2590.
23. Le Grand SM, Patumraj S, Phansuwan-Pujito P, et al.Melatonin inhibits cortical spreading depression-evoked tri-geminal nociception. Neuroreport 2006;6:1709–1713.
24. Fawcett WJ, Haxby EJ, Male DA. Magnesium: Physiologyand pharmacology. Br J Anaes 1999;83:302–20.
25. Harrington DD. Influence of magnesium deficiency on horsefoal tissue concentration of magnesium, calcium and phos-phorus. Br J Nutr 1975;34:45–57.
26. Kienzle E, Zorn N. Bioavailability of minerals in the horse,in Proceedings. 3rd Eur Equine Nutr Health Congress Bel-gium 2006.
aSurvey Monkey, Palo Alto, CA 94301-2580.bFacebook, Menlo Park, CA 94025.
AAEP PROCEEDINGS � Vol. 60 � 2014 183
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Review of the Discovery of the Basis for aSeasonal Pasture Myopathy/Atypical Myopathy
Seasonal pasture myopathy,1,2 atypical myop-athy,3,4 and atypical myoglobinuria5 are terms usedto describe an often-fatal form of rhabdomyolysisthat develops in unexercised horses kept on pas-tures. Although initial clinical signs resemblecolic, the apparent discomfort, trembling, tachycar-dia, short stiff stride, periods of recumbency, tachy-pnea, and myoglobinuria actually arise from severedegeneration of postural and respiratory muscles.5–7
The first reports date back to 1939 in Wales8 and1959 in Southern Ontario.9 Although described for75 years, the cause of this disorder has remained amystery until very recently. The purpose of thisreview is to highlight the sentinel findings that ledto the discovery of the toxin associated with cases ofseasonal pasture myopathy in European and NorthAmerican horses.
2. Epidemiology
Vital epidemiological information on a large numberof cases of pasture myopathy arose from the AtypicalMyopathy Alert Group (http://www.myopathieaty-pique.fr/en/amag-2/). Many hundreds of cases weredocumented in Denmark, France, Germany, Ire-
land, United Kingdom, Latvia, Luxembourg, Spain,Switzerland, The Netherlands, Austria, Czech Re-public, Italy, Norway, and Sweden.7,10–12 Fewercarefully researched cases were documented inNorth America.1,2,13 It became apparent that thenumber of outbreaks of pasture myopathy variedfrom year to year, were preceded by stormy weather,and occurred in pastures with trees in or aroundthem that also contained dead leaves, dead woodand wet areas. The clustering of cases to specificpastures where horses were housed for at least 12 ha day, the seasonal occurrence in fall or the subse-quent spring, the cessation of cases from Decemberto January, and the lack of gender or breed predi-lection suggested a toxin was present in pastures ona seasonal basis. The wide variety of plants thatcould be implicated in causing pasture myopathymade the search for potential toxins confounding.Potential etiologic agents initially under investi-gation included white snakeroot,1 clostridium tox-ins in soil,14,15 toxins in dead leaves,10,12 and thetar spot fungus growing on the leaves of Acerpseudoplatanus,16 the European sycamore maple.Studies from 1988 in the United Kingdom5 and
184 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
2010 in the Netherlands16 had identified the syc-amore maple as a consistent presence on affectedpastures. Information on the mechanism bywhich the toxin produced rhabdomyolysis was animportant missing piece of the puzzle.
3. Pathophysiology
Serum biochemistry profiles of horses with pasturemyopathy provided little direction for toxin inves-tigation. Profiles revealed marked elevations inserum creatine kinase (CK) and aspartate transami-nase and a moderate elevation in gamma-glutamyltransferase activities. Electrolyte derangements(high potassium and phosphorus, low sodium, chlo-ride, and calcium), hyperglycemia, and lactic acidosiswere often present.1,7,13,17,18 Similarly, hematoxylinand eosin stains of formalin fixed muscle merelyconfirmed severe myodegeneration of postural andrespiratory muscles and inconsistent degenerationof cardiac muscle.4,5 Advances were made, how-ever, when special stains were applied to muscletissues and a lipid storage disorder was identifiedin postural and respiratory muscles of horses withpasture myopathy in both North America andEurope.1,3
A critical piece of the puzzle was contributed byWesterman et al. in 2008 that both narrowed the listof potential toxins causing pasture myopathy andled to a specific means to diagnose the condition.19
An acquired defect in the enzyme multiple acyl-coAdehydrogenase (MAD) that represents the first stepof �-oxidation of short and medium chain fatty acidsas well as branched chain amino acids was found inmuscle cells from Dutch horses with pasture myop-athy. A diagnosis of MAD deficiency could readily beestablished by measuring the backlog of byproducts oflipid (acylcarnitines) and amino acid metabolism (gly-cine conjugates) in the bloodstream or urine. Thespecific diagnostic indicators of MAD were high short(C2-C5) and medium chain (C6-C10) acylcarnitines,
variably high long chain (C14-C18) acylcarnitines, andmarked elevations in urine ethylmalonic and methyl-succinic acids and glycine conjugates ([iso]valeryl-,butyryl-, and hexanoylglylcine).19 Serum and urinesamples from horses in North America with pasturemyopathy were later found to also have a deficiencyof MAD.13 Thus, it seemed that the underlyingmechanism for pasture myopathy was the same inEurope and North America.
4. The Toxin
Combining epidemiologic and pathophysiologic in-formation, the responsible toxin would have to beseasonally associated with trees and capable ofblocking MAD in muscle cells. In 2012, we deter-mined that seeds from one particular tree in themidwestern U.S., Acer negundo (box elder, Manitobamaple) (Fig. 1A), were present in the fall on allinspected pastures where horses had succumbed topasture myopathy.2 The seeds of this tree (Fig. 1B)remain on the trees in the fall and are distributedonto the ground by high winds prior to an outbreak.2
The topographical distribution of Acer negundomatched previous cases of pasture myopathy diag-nosed in North America. A key connector was thefact that another tree within the same Sapinidaefamily, the Jamaican Ackee tree, produced a fruitthat when unripe contained a nonproteogenic aminoacid hypoglycin A, capable of causing an acquireddeficiency of MAD when ingested by humans.20
Subsequent studies found hypoglycin A in seedsfrom box elder trees growing in pastures where out-breaks of pasture myopathy had occurred.2 In ad-dition, the conjugated toxic metabolite of hypoglycinA, methylenecyclopropyl acetic acid (MCPA)-carni-tine, was found in the bloodstream and urine ofhorses with pasture myopathy in the midwesternU.S.2 Thus, hypoglycin A appeared to cause pas-ture myopathy in North America.
Fig. 1. A, Branches of a box elder tree (Acer negundo) laden with seeds in the late fall. B, One samara (husk) from the box elder treewith the seed removed (above and to the left) relative to the size of a razor blade (below).
AAEP PROCEEDINGS � Vol. 60 � 2014 185
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Acer negundo was an unlikely source of toxin inEurope as this tree is not native to Europe and itwas introduced largely as an ornamental varietal.A closely related tree, Acer pseudoplatanus, the syc-amore maple (Fig. 2A), had previously been identi-fied in European pastures where outbreaksoccurred. Hypoglcyin A was analyzed and identi-fied in seeds from Swiss sycamore trees (Fig. 2B)that were growing in pastures where horses haddied from pasture myopathy and blood samples fromaffected European horses were also found to containserum MCPA-carnitine.21
Thus, hypoglycin A present in seeds obtained inthe fall from box elder or sycamore maples is thelikely etiology for pasture myopathy in North Amer-ica and Europe. Storms increase the number ofseeds on pastures;2,10,11 snow cover in the winterprevents access to seeds on the ground and ingestionof germinating seeds in the early spring and canlead to emergence of new cases. Seed burdensshow annual variation, potentially explaining vari-ations in outbreaks from year to year.22 Toxin lev-els in seeds could vary from year to year as well, butthis has not been studied. Disruption of lipid me-tabolism in muscle cells leads to degeneration ofthose muscle cells most active at rest, postural andrespiratory muscles.
No studies have been performed in which hypo-glycin A or Acer species seeds have been fed tohorses to definitively prove the toxicity of Acer spe-cies seeds in horses. Thus, the number of seeds ahorse would need to eat to become ill is not known.Further, quantitative assays of hypoglycin A havenot been performed on seeds from other maple treesto determine their toxicity, nor have changes in hy-poglycin A concentrations been reported over thecourse of a year.
5. Diagnosis
A presumptive diagnosis of hypoglycin A-inducedpasture myopathy is based on the following:
1. Clinical signs of sudden rapidly progressivemuscular weakness and stiffness, myo-
globunuria, tachycardia, tachypnea, dyspnea,and recumbency, with death occurring in themajority of cases within 72 hours of the onset ofsigns. About 50% of horses will have cardiacdamage. Most horses retain a normal appe-tite; occasionally horses have signs of choke,cardiac arrhythmia, colon impactions, andhead swelling due to persistently low headposture.
2. Marked elevations in serum CK and aspartatetransaminase activities, hyperglycemia, elec-trolyte derangements, and acidosis.
3. A history of grazing pastures containing or sur-rounded by maple trees with seeds in the fall orearly spring.
A definitive diagnosis of hypoglycin A-induced my-opathy is based on characteristic changes in serumacylcarnitines and urine organic acids. These testsare most readily available and are routinely per-formed by human metabolic disease laboratoriessuch as the Baylor Institute of Metabolic Disease(http://www.baylorhealth.edu/Research/Institutes-Centers/IMD/Pages/Tests%20and%20Forms%2005–11.pdf). Normal equine values have beenpublished for reference ranges.13 Hypoglycin Aand MCPA-carnitine assays are not commerciallyavailable.
6. Treatment
Early recognition of the disease is critical as themortality rate likely improves with early treatmentand prompt removal of horses from the source oftoxin. Since this condition can present as a succes-sion of cases, removal of all grazing animals fromthe pasture immediately is important along withchecking serum CK activities. Horses should berested in a warm dry environment and fed ad libi-tum hay and some grain to avoid a negative energybalance. Renal, respiratory, and cardiac functionshould be monitored by means of serum biochemis-try profiles, blood gases, and cardiac troponin. Ju-dicious use of nonsteroidal anti-inflammatory drugsis recommended, based on the status of dehydration
Fig. 2. A, Branches of the European sycamore maple (Acer pseudoplatanus) laden with seeds in the late fall. B, One samara (husk)from the sycamore tree with the seed (right) still present in the husk relative to the size of a razor blade (below).
186 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
and renal function. Intravenous fluids need to betailored to each horse’s electrolyte derangementsand severity of lactic acidosis at a rate that avoidsfluid overload, especially if the cardiovascular sys-tem is compromised. Nasal oxygen may benefithorses with tachypnea. Intravenous antioxidantssuch as dimethyl sulfoxide, vitamin C, vitamin Bcomplex (including riboflavin), and oral water dis-persible natural vitamin E may be beneficial for theoutcome.1,6 The mortality rate is about 75%.10
Horses that have recovered usually regain musclemass over time and return to their former level ofactivity.
7. Prevention
Minimizing a horse’s risk of exposure to box elder orEuropean sycamore seeds in the fall is the bestpreventive strategy. Nevertheless, it is importantto recognize that there are many older horses thathave been housed on pastures with large numbers ofAcer trees for years that have never become ill.Whether these horses avoid eating the seeds or havesome form of immunity is unclear. Horses partic-ularly at risk for pasture myopathy are those thatare young or new to overgrazed pasture with Acertrees, those turned out more than 12 h/day, andthose receiving little supplemental feed.2,10 Ide-ally, trees with heavy seed burdens should be re-moved from pastures. If this is not possible, turn-out of at-risk horses should be avoided in the fallwhen seed burdens are high or in the early spring.
8. Name Change for Atypical Myopathy and SeasonalPasture Myopathy
There are other potential causes for pasture-associ-ated myopathies in horses such as trematone toxinin white snakeroot and rayless goldenrod. Withadvances in defining the etiology of the most com-mon pasture myopathy, the terms Seasonal PastureMyopathy and Atypical Myopathy are now outdatedand nonspecific. A change to the name HypoglycinA Myopathy (H-AM) is proposed for those cases inwhich rhabdomyolysis develops in horses that arehoused in proximity to seed-bearing Acer negundo orAcer pseudoplatanus trees, especially when elevatedserum acylcarnitine or urine glycine conjugates con-centrations are confirmed to be present.
Acknowledgments
This research represents a collaborative effortamongst researchers at the University of Bern,Switzerland, the University of Liege, Belgium, In-stitute of Metabolic Disease, Baylor Research Insti-tute, Texas, Iowa State University, and theDepartment of Horticultural Sciences, University ofMinnesota.
Conflict of InterestThis research was funded by the University of Min-nesota Rapid Agricultural Response Fund.
References1. Finno CJ, Valberg SJ, Wunschmann A, et al. Seasonal pasture
myopathy in horses in the midwestern United States: 14 cases(1998–2005). J Am Vet Med Assoc 2006;229(7):1134–1141.
2. Valberg SJ, Sponseller BT, Hegeman AD, et al. Seasonalpasture myopathy/atypical myopathy in North America asso-ciated with ingestion of hypoglycin A within seeds of the boxelder tree. Equine Vet J 2013;45(4):419–426.
3. Cassart D, Baise E, Cherel Y, et al. Morphological altera-tions in oxidative muscles and mitochondrial structure asso-ciated with equine atypical myopathy. Equine Vet J 2007;39(1):26–32.
4. Votion DM, Linden A, Saegerman C, et al. History andclinical features of atypical myopathy in horses in Belgium(2000–2005). J Vet Intern Med 2007;21(6):1380–1391.
5. Whitwell KE, Harris P, Farrington PG. Atypical myoglobin-uria: an acute myopathy in grazing horses. Equine Vet J1988;20(5):357–363.
6. Finno CJ, Spier SJ. Prevention and treatment of equineatypical myopathy—an acute, highly fatal disease of un-known etiology. Vet J 2008;178(2):163–164.
7. van Galen G, Marcillaud PC, Saegerman C, et al. Europeanoutbreaks of atypical myopathy in grazing equids (2006–2009): spatiotemporal distribution, history and clinical fea-tures. Equine Vet J 2012;44(5):614–620.
8. Bowen JN, Craig JF. Myoglobinuria in horses. Vet Rec1942;35:354–355.
9. Pope DC, Heslop CH. An outbreak of myoglobinuria in lighthorses. Can Vet J 1960;1(4):171–174.
10. van Galen G, Saegerman C, Marcillaud PC, et al. Europeanoutbreaks of atypical myopathy in grazing horses (2006–2009): determination of indicators for risk and prognosticfactors. Equine Vet J 2012;44(5):621–625.
11. van Galen G, Amory H, Busschers E, et al. European out-break of atypical myopathy in the autumn 2009. J VetEmerg Crit Care (San Antonio) 2010;20(5):528–532.
12. Votion DM, Linden A, Delguste C, et al. Atypical myopathy ingrazing horses: A first exploratory data analysis. Vet J 2008.
13. Sponseller BT, Valberg SJ, Schultz NE, et al. Equine mul-tiple acyl-CoA dehydrogenase deficiency (MADD) associatedwith seasonal pasture myopathy in the midwestern UnitedStates. J Vet Intern Med 2012;26(4):1012–1018.
14. Gerber V, Straub R, Frey J. Equine botulism and acutepasture myodystrophy: new soil-borne emerging diseases inSwitzerland? Schweiz Arch Tierheilkd 2006;148(10):553–559.
15. Unger-Torroledo L, Straub R, Lehmann AD, et al. Lethaltoxin of Clostridium sordellii is associated with fatal equineatypical myopathy. Vet Microbiol 2010;144(3–4):487–492.
16. van der Kolk JH, Wijnberg ID, Westermann CM, et al.Equine acquired multiple acyl-CoA dehydrogenase deficiency(MADD) in 14 horses associated with ingestion of Mapleleaves (Acer pseudoplatanus) covered with European tar spot(Rhytisma acerinum). Mol Genet Metab 2010;101(2–3):289–291.
17. van Galen G, Cerri S, Porter S, et al. Traditional and quan-titative assessment of acid-base and shock variables in horseswith atypical myopathy. J Vet Intern Med 2013;27(1):186–193.
18. Votion DM, Serteyn D. Equine atypical myopathy: a re-view. Vet J 2008;178(2):185–190.
19. Westermann CM, Dorland L, Votion DM, et al. Acquiredmultiple Acyl-CoA dehydrogenase deficiency in 10 horseswith atypical myopathy. Neuromuscul Disord 2008;18(5):355–364.
20. Joskow R, Belson M, Vesper H, et al. Ackee fruit poisoning:an outbreak investigation in Haiti 2000–2001, and review ofthe literature. Clin Toxicol (Phila) 2006;44(3):267–273.
21. Unger L, Nicholson A, Jewitt EM, et al. Hypoglycin A con-centrations in seeds of Acer Pseudoplatanus trees growing onatypical myopathy-affected and control pastures. J Vet IntMed May 26, 2014. doi: 10.1111/jvim.12367.
22. Abrams MD. The red maple paradox. Bioscience 1988;48(5):355–364.
AAEP PROCEEDINGS � Vol. 60 � 2014 187
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Effect of a Dietary Supplement on Gastric UlcerSeverity
The objective of this study was to assess the effect ofa dietary supplement containing polar lipids (oatoil), soluble fiber (�-glucan), and amino acids (L-Glutamine and L-Threonine) on the developmentand treatment of squamous gastric ulceration inracing Thoroughbreds.
2. Materials and Methods
Sixty-seven Thoroughbreds in race training or pre-race training were recruited to the study on thebasis of having �grade 1 gastric ulceration (TheEquine Gastric Ulcer Council, 1999) on day 0 of thetrial. Of this group, 39 horses completed the trial,which involved repeat gastroscopy on day 30, 60,and 90. Each horse was randomly assigned to one oftwo treatment groups; omeprazoleb or the dietarysupplementa; treatments were administered accord-ing to label dosage for the duration of the trial.
3. Results and Discussion
Chi-squared tests were used to assess the differencebetween treatment groups in terms of the proportionof horses improving by 2 or more grades: sixteenhorses in each group improved by less than 2 grades orworsened (P � 0.53). McNemar’s tests were appliedto assess the effect of each treatment on gastric ulcerscore. There was no significant improvement on gas-tric ulcer score with either omeprazole (P � 0.38) orthe dietary supplement (P � 0.50) when a clinicallysignificant gastric ulcer score of �2 was used.
Acknowledgments
Conflict of InterestThis study was funded by Freedom Health LLC.
Footnotes
aSucceed™, Freedom Health LLC, Aurora, OH 44202.bGastroGard®, Merial Animal Health Ltd., Harlow, Essex, UK.
188 2014 � Vol. 60 � AAEP PROCEEDINGS
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Research Abstract
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
Effect of a Supplement on Non-Glandular GastricUlcer Scores and Gastric Juice pH
Frank M. Andrews, DVM, MS, DACVIM-LA; Pilar Camacho, DVM;Giavanna Gaymon, DVM; Patrick Loftin, DVM; Frank Garza, Jr., MS;Michael L. Keowen, BS; and Michael T. Kearney, PhD
SGU containing botanicals (herbs), coating agents,and natural antacids for horses with gastric ulcershas limited data available on its effectiveness.The purpose of this study was to evaluate the effectof SGU on nonglandular (NG) gastric ulcers scoresand gastric juice pH after omeprazole treatment install-confined horses.
2. Materials and Methods
This study was performed in racing-age stall-confined Thoroughbreds (n � 8) as a 42-day 2-period crossover design in which all horses receivedno treatment (untreated controls) or treatment(SGU pellets, 40 g, twice daily). In addition, fromdays 1 to 14 all horses were treated with omeprazolepasteb, and then treatment was discontin-ued. From days 28 to 35, all horses underwentintermittent feed-deprivation. During feed-depri-vation, all treated horses were fed SGU. From days
35 to 42, horses returned to their normal diet.Gastroscopy was performed on day �1, 14, 28, 35,and 42. Gastric juice pH was measured and NGgastric ulcer number (NGN) and severity (NGS)scores were assigned by a masked clinician (FMA).
3. Results
After 14 days, NGN and NGS scores significantlydecreased (P � 0.05) in both groups compared tothose on day �1. On days 28 and 35, NGN scoresremained significantly lower in the SGU-treatedhorses when compared to the untreated controls.By Day 42, NGN and NGS scores were not signifi-cantly different in either group. Gastric juice pHwas low and variable, except on day 14, when gastricjuice pH was significantly higher in both groups dueto omeprazole treatment.
4. Conclusions
SGU supplement fed to horses prevented gastriculcers from increasing in horses after omeprazole
AAEP PROCEEDINGS � Vol. 60 � 2014 189
MEDICINE POTPOURRI: NEUROLOGY, FOALS, MUSCLES, AND THE GUT
Research Abstract
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the AAEP Annual Convention, Salt Lake City, UT, USA - December 6-10, 2014
treatment, without increasing gastric juice pH.Supplementation with SGU aids in the protection ofthe NG stomach from the rebound acid effects afteromeprazole treatment is discontinued and in stall-confined horses undergoing intermittent feeding.
Acknowledgments
Conflict of InterestThis study was funded by Smart Pak Equine, LLC.,Equine Health Studies Program Equine Funds andthe LSU Foundation.