20
CLICK TO EDIT MASTER PROGRAMME TITLE CLICK TO EDIT MASTER PROGRAMME TITLE Neonatal Sepsis Mike Sharland, Sally Ellis and Neonatal Sepsis team

CLICK TO EDIT MASTER PROGRAMME TITLECLICK TO EDIT MASTER PROGRAMME TITLE
Neonatal SepsisMike Sharland, Sally Ellis and
Neonatal Sepsis team

Disease burden
• Maternal and child deaths have halved worldwide over the past two decades
• Neonatal mortality remains high with 2.9 million deaths estimated in newborns (<28 days) every year
• Nearly a quarter(23%) of deaths are due to infectious causes
Sepsis
Prematurity
Asphyxia
• To achieve the SDGs, a high proportion of neonatal deathsneeds to be prevented and the outcome of neonates withsepsis must significantly improved
Number of neonatal lives saved annually, and from asphyxia, sepsis and prematurity. Arnesen L, BMC
Public Health. 2016

• SBIs in neonates account for about 3% ofall disability-adjusted life years (DALY),and infection-attributable deathscontribute largely to the global burden ofdisease
• The first pooled estimate of incidencerisk in LMICs was 7.6%, with 6.9 millioncases of pSBI estimated among neonatesin 2012 (Seale AC, Lancet Infect Dis 2014)
• Overall, case-fatality risk associated withpSBI was 9.8%
Global burden of neonatal sepsis
Clinical diagnosis of Severe Bacterial Infections (SBIs) is often challenging in neonates, since symptoms and signs can be non-specific and difficult to detect
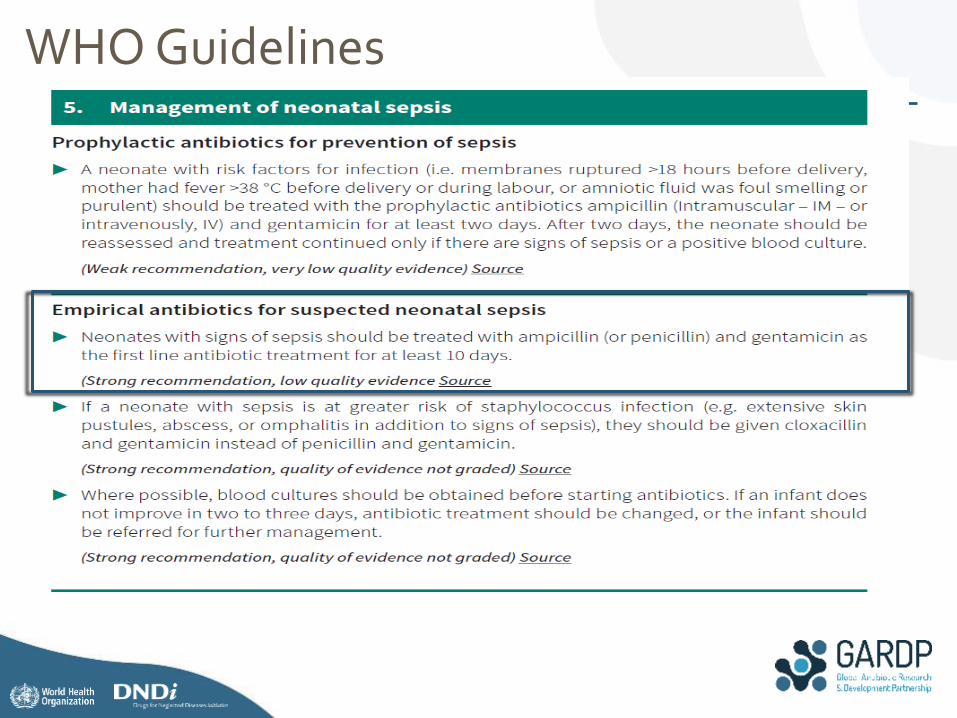
WHO Guidelines

• Hospitalised neonates and infants are at high-risk of developing MDR healthcare-associated infections
• Very high rates of AMR reported in both resource-rich and resource-poor countries
Pathogen
WHO Regions
EURO EMRO AFRO PAHO WPRO SEARO
A^ G^^ A G A G A G A G A G
E. coli 35.5% 86.5% -* - 7.1% 57.1% - - - - 3.1% 16.7%
K. pneumoniae - 73.8% - - 0% 45.5% - - - - 6.2% 31.2%
P. aeruginosa - 85.7% - - - - - - - - 85% 80.6%
S. aureus** 83% - - - - -
^A: ampicillin; ^^G: Gentamicin; *No regional data available; **Percentage of methicillin-susceptibility
Sensitivity to the individual components of WHO first-line neonatal sepsis regimen
• Pooled data demonstrate that over 40% of sepsis in neonates was due to pathogensthat were resistant to the currently recommended WHO regimen (ampicillin andgentamicin)
Global AMR in neonatal sepsis
• Based on the first estimate of neonatal deaths due to AMR, 214,000 neonatal sepsisdeaths due to MDR pathogens have been predicted every year globally (Laxminarayan R,2016)
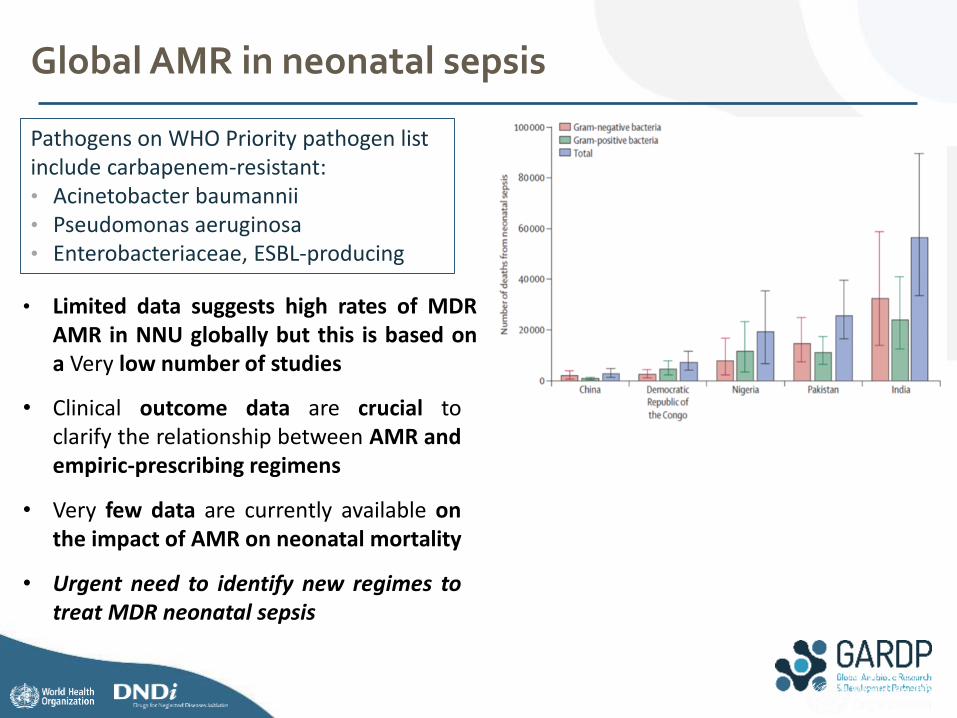
• Limited data suggests high rates of MDRAMR in NNU globally but this is based ona Very low number of studies
• Clinical outcome data are crucial toclarify the relationship between AMR andempiric-prescribing regimens
• Very few data are currently available onthe impact of AMR on neonatal mortality
• Urgent need to identify new regimes totreat MDR neonatal sepsis
Global AMR in neonatal sepsis
Pathogens on WHO Priority pathogen list include carbapenem-resistant:• Acinetobacter baumannii• Pseudomonas aeruginosa• Enterobacteriaceae, ESBL-producing

• 14 779 neonates admitted to NICU
• 59·9% (8111) were low birthweight, and 44·2% (5989,) were preterm.
• 1980 episodes of sepsis in 1934 neonates = incidence of 14·3% (95% CI 13·8–14·9)
• culture-positive sepsis was 6·2% (5·8–6·6) of NICU admissions.
• Common isolates: Acinetobacter spp, Klebsiella spp, E coli, Pseudomonas spp,
• Most isolated pathogens showed a high degree of resistance, including to extended-spectrumcephalosporins and carbapenems
Neonatal sepsis on 3 hospitals in Delhi (DeNIS)

Antibiotics for use in children / neonates
New Antibiotics (2013)11 newly approved antibiotics, 31 clinical trials enrolling children in Europe BUT• trials often included adults and children but did not provide a subset analysis for children,
limiting the relevance of their findings. • prematurely terminated or apparently active but not yet recruiting patients• Among paediatric-specific studies,
• 18 evaluate safety and efficacy of new compounds, • 4 are pharmacokinetic studies, but only 2 focus on neonates.
• For most antibiotics, despite adult phase 3 studies being completed, with specific concerns for particular drugs already noted, it will take another 3–5 years before adequate prescribing information becomes available for paediatricians.
Old antibiotics – Limited data• Only 6 of the antibiotics identified in the ECCMID review of 33 antibiotics have a
licensed neonatal indication and of these 6, only tobramycin and fosfomycin have significant MDRGN activity.
• Colistin – 2 pharmacokinetic studies in neonates 1 in 1967 and second in 2016 each with less than 10 patients

NeoAMR Program
WP1: Pre-selection of potential agents Advisory Role for study conduct
WP6: Project Management
Target PopulationWP 2: Clinical Observational study of
neonatal sepsis in target settings
Bacterial EpidemiologyWP3: Microbiological study of neonatal
sepsis in target settings
Therapeutic Options
WP4: Pharmacokinetic study(ies)
WP4: PK /PD modelling
WP4: Formulation
WP5: Clinical
Trial(s)
• Empiric
treatment
• Confirmed
MDR
resistant
treatment
Aim: By 2023,
deliver one
combination
treatment for the
empiric
management and
one combination
treatment targeted
for MDR cases

Primary objectives: Develop 1-2 new treatments within the 6 years. 1. An empirical treatment for babies with possible serious bacterial infection in areas
where drug-resistant Gram-negative (ESBL) pathogens are suspected (cf. TPP1) 2. A treatment for babies where MDR Gram-negative pathogens have been confirmed (e.g.
carbapenem-resistant K. pneumoniae, or Acinetobacter spp), cf. TPP2.
Secondary Objectives 1. To develop a global network of neonatal centers and relevant partners to design and conduct
studies (optimal use of off-patent/new antibiotics, and other strategies, for the effective prevention and management of MDR/XDR neonatal sepsis)
2. To determine the current phenotypic and genotypic resistance profiles of invasive and colonizing GN isolates from Neonatal Units participating in the project
3. To design and conduct PK, observational and interventional studies (efficacy and safety of novel regimens vs existing therapies)
4. To develop a conservation strategy for novel treatment regimens
Neonatal Sepsis Program
NeoAMR - A global consortium to develop two new treatments for neonatal sepsis

Prospective cohort study of empirical antibiotic treatment in neonatal sepsis and clinical outcome
AimCollect Routine clinical data for 28 days on:• Patients with Significant sepsis (2
clinical signs / laboratory finding)• Patients with microbiologically
confirmed MDR gram negative organisms in blood or CSF
• Collect opportunistic pharmacokinetic samples (blood, CSF) from patients with confirmed MDRGN sepsis in selected sites
Primary Objective• To prospectively characterise mortality rates in infants in NNU treated for clinical sepsisTrial Design• Prospective, multinational, multicentre, observational cohort study of the inpatient
management of neonatal sepsis in approximately 20 sites. • Enroling 200 infants per site gives >80% power to detect differences in mortality of 50% in
5% blood culture positives vs 10% in 95% blood culture negatives, as observed in DENIS

Indication Empiric treatment of neonatal sepsis, including meningitis (premature and term, early and late onset)
Patient Population Neonates with pSBI in settings of high prevalence of resistance to first line WHO empiric therapy
Route of Administration i.v. (intravenous), 30-120 min infusions Dosing Schedule 2-4 x daily Efficacy Comparable clinical activity to ampicillin/gentamicin or
ceftriaxone/gentamicin in claimed indicationClinical activity in pathogens resistant to ampicillin/gentamicin or ceftriaxone/gentamicin
Treatment duration 5-28 daysSafety / Tolerability Low propensity for resistance development, large therapeutic window
concerning hepatotoxicity, nephro- and CNS-toxicity, no QT-prolongation
TPP1
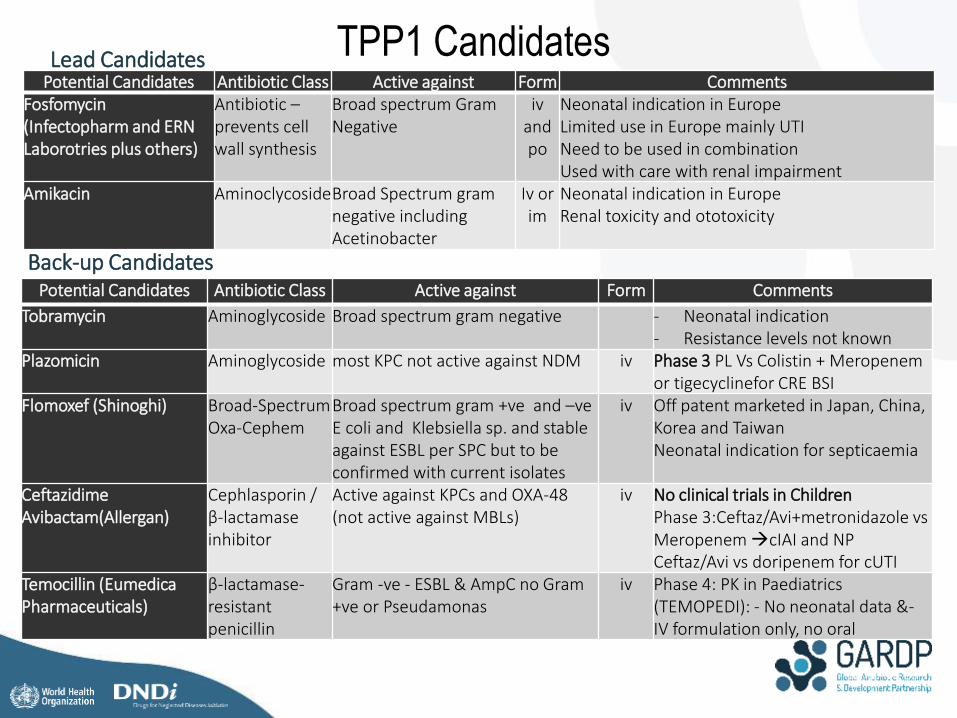
TPP1 Candidates Potential Candidates Antibiotic Class Active against Form Comments
Fosfomycin(Infectopharm and ERN Laborotries plus others)
Antibiotic –prevents cell wall synthesis
Broad spectrum Gram Negative
iv and po
Neonatal indication in EuropeLimited use in Europe mainly UTINeed to be used in combinationUsed with care with renal impairment
Amikacin AminoclycosideBroad Spectrum gram negative including Acetinobacter
Iv or im
Neonatal indication in EuropeRenal toxicity and ototoxicity
Lead Candidates
Potential Candidates Antibiotic Class Active against Form Comments
Tobramycin Aminoglycoside Broad spectrum gram negative - Neonatal indication- Resistance levels not known
Plazomicin Aminoglycoside most KPC not active against NDM iv Phase 3 PL Vs Colistin + Meropenem or tigecyclinefor CRE BSI
Flomoxef (Shinoghi) Broad-Spectrum Oxa-Cephem
Broad spectrum gram +ve and –veE coli and Klebsiella sp. and stable against ESBL per SPC but to beconfirmed with current isolates
iv Off patent marketed in Japan, China, Korea and TaiwanNeonatal indication for septicaemia
Ceftazidime Avibactam(Allergan)
Cephlasporin / β-lactamase inhibitor
Active against KPCs and OXA-48 (not active against MBLs)
iv No clinical trials in ChildrenPhase 3:Ceftaz/Avi+metronidazole vs Meropenem cIAI and NP Ceftaz/Avi vs doripenem for cUTI
Temocillin (EumedicaPharmaceuticals)
β-lactamase-resistant penicillin
Gram -ve - ESBL & AmpC no Gram +ve or Pseudamonas
iv Phase 4: PK in Paediatrics (TEMOPEDI): - No neonatal data &-IV formulation only, no oral
Back-up Candidates
Fosfomycin
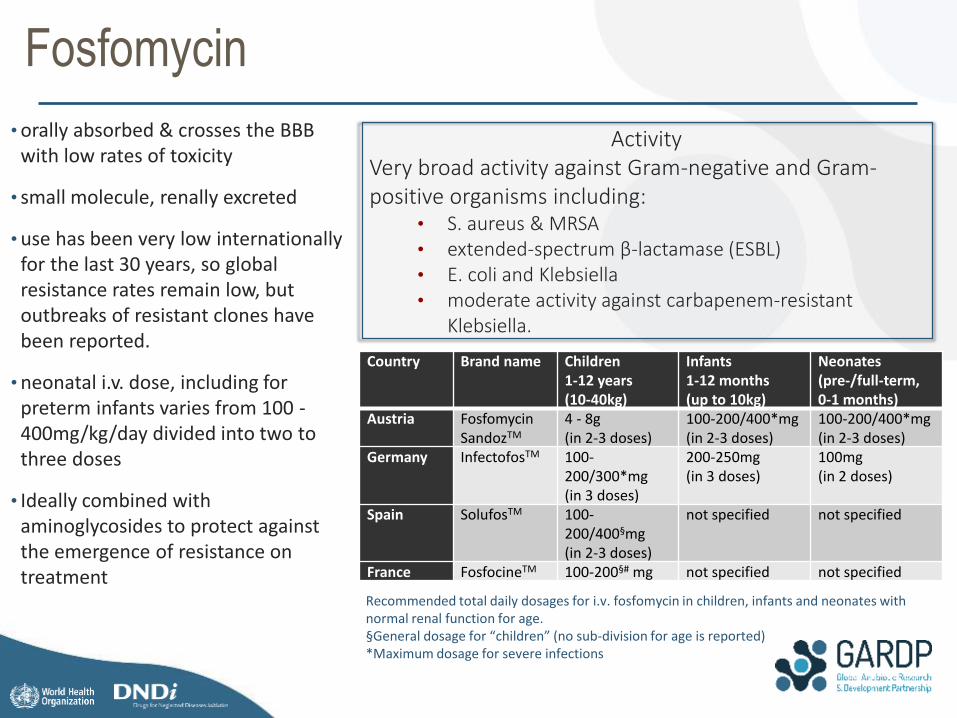
•orally absorbed & crosses the BBB with low rates of toxicity
• small molecule, renally excreted
•use has been very low internationally for the last 30 years, so global resistance rates remain low, but outbreaks of resistant clones have been reported.
•neonatal i.v. dose, including for preterm infants varies from 100 -400mg/kg/day divided into two to three doses
• Ideally combined with aminoglycosides to protect against the emergence of resistance on treatment
Country Brand name Children1-12 years(10-40kg)
Infants1-12 months(up to 10kg)
Neonates(pre-/full-term,0-1 months)
Austria FosfomycinSandozTM
4 - 8g(in 2-3 doses)
100-200/400*mg(in 2-3 doses)
100-200/400*mg(in 2-3 doses)
Germany InfectofosTM 100-200/300*mg(in 3 doses)
200-250mg(in 3 doses)
100mg(in 2 doses)
Spain SolufosTM 100-200/400§mg(in 2-3 doses)
not specified not specified
France FosfocineTM 100-200§# mg not specified not specified
Recommended total daily dosages for i.v. fosfomycin in children, infants and neonates with normal renal function for age.§General dosage for “children” (no sub-division for age is reported)*Maximum dosage for severe infections
ActivityVery broad activity against Gram-negative and Gram-positive organisms including:
• S. aureus & MRSA• extended-spectrum β-lactamase (ESBL) • E. coli and Klebsiella• moderate activity against carbapenem-resistant
Klebsiella.

Fosfomycin synopsis
Objectives
• assess the safety of IV fosfomycin with regard to possible elevation of sodium, calcium and creatinine at Day 2 and 7 in neonates
• estimate the PK of IV fosfomycin in neonates
• estimate the oral bioavailability of fosfomycin in neonates
Treatment
• Randomised to Amp/Gent (SoC) vs Amp/Gent plus a 7-day course of fosfomycin
• 48 hours (or more) IV fosfomycin, followed by up to 5 days of oral fosfomycin.
• Neonates will move to oral fosfomycin once they are tolerating oral feeds.
PK and Safety Sampling
• Two PK samples will be taken after the first IV and oral doses; the sampling times will be randomly allocated to one of three possible early and late time points
• Adverse events, blood sampling for electrolytes including sodium and kidney function at Day 2 and 7 to assess safety
• All SAEs reviewed by DSMB
Statistics
Sample size: 60 babies to get 45 with complete PK
Baseline Assessments including:Electrolytes, blood culture, Lumbar Puncture (if
indicated)
Randomisation
Standard of care aloneStandard of care + Fosfomycin
Early & Late PK sample after IV dose
Day 2: Electrolytes and CMP (48h) Electrolytes and CMP (48h)
Early and Late PK sample after IV dose
Day 7: Electrolytes
Start Ampicillin and GentamicinDay 1: Start Ampicillin and Gentamicin
Day 1 & 2: Start intravenous Fosfomycin
If tolerating oral meds / clinical improved:stop IV fosfomycin start Oral Fosfomycin Day 3-7
Day 7: Trough PK sample
Day 28: Follow-up
Day 7: Electrolytes
Day 28: Follow-up

MDR Gram-negative - Current - Standard of carePotential Candidates Antibiotic Class Activity Form Dose
ColistemethateColistin(Generic)
Polymixin Broad spectrum Gram Negative including CRE
iv 50000-75000IU/Kg/day in 3 divided doses(up to 75000-120000 IU/Kg/day has been used in 3 divided doses)
ONGOING CLINICAL TRIALS• NCT02806141: Safety and Efficacy RCT on aerosolized + i.v. vs i.v. Colistin alone in VAP due to PDR
Acinetobacter Baumannii in neonates
o Estimated Enrollment: 204o Study start date: September 2016o Estimated Study Completion Date: December 2018
PK STUDIESAxline SG, Pediatrics 1967• Single i.m. 5 mg/kg dose in premature infants• 8 premature infants enrolled• Results: serum half-life did not decline with increasing postnatal age
Nakwan N, Pediatr Infect Dis J 2016• Single i.v. dose of colistimethate sodium in critically ill neonates• Equivalent to 1.1 and 2.6 mg/kg/day of colistin base (approximately 33,000–78,000 IU/d of CMS).• Prospective, open-label study conducted in NICU• 7 neonates enrolled (5 VAP, 2 MDR-GN BSIs)• Results: currently recommended dosage resulted in undectable levels in virtually all
babies….and this is the dose being used in SA..
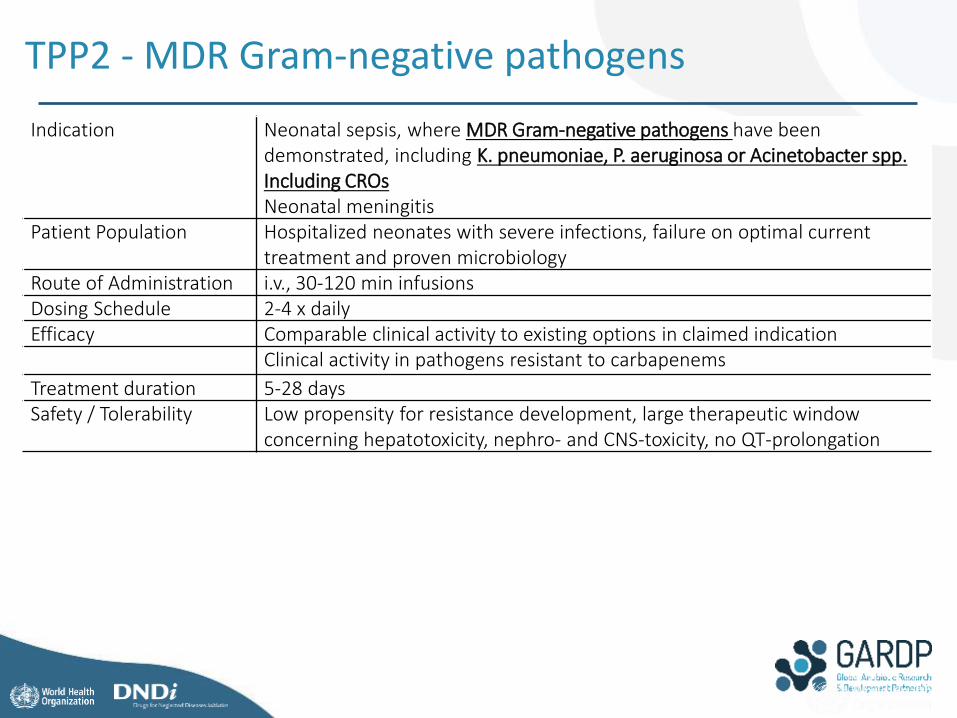
Indication Neonatal sepsis, where MDR Gram-negative pathogens have been demonstrated, including K. pneumoniae, P. aeruginosa or Acinetobacter spp. Including CROsNeonatal meningitis
Patient Population Hospitalized neonates with severe infections, failure on optimal current treatment and proven microbiology
Route of Administration i.v., 30-120 min infusions Dosing Schedule 2-4 x daily Efficacy Comparable clinical activity to existing options in claimed indication
Clinical activity in pathogens resistant to carbapenems
Treatment duration 5-28 daysSafety / Tolerability Low propensity for resistance development, large therapeutic window
concerning hepatotoxicity, nephro- and CNS-toxicity, no QT-prolongation
TPP2 - MDR Gram-negative pathogens

TPP2 Strategy
Short term Conduct opportunistic blood sampling in patients with confirmed multidrug resistant gram negative infections with CRO• Determining the feasibility of conducting neonatal PK in LMIC
setting with limited neonatal clinical trials experience as part of the observational study
Mid-term: • Design a randomised trial to evaluate optimally dosed polymyxin B compared to SOC (NeoPolyB) in neonates starting in Q4 2018.
Long term Evaluate the possibilities with partners to set up a master protocol / multi-arm stage study to evaluate pharmacokinetics of antibiotics or combinations of old and new antibiotics with activity against CRO/CRE. This could be established from 2019/2020.

TPP2 Lead Candidates
Potential Candidates Antibiotic Class Activity Form Comments
Polymixin B (Generic but limited use outside USA)
Polymixin Broad spectrum Gram Negative including CRE
iv Nephrotoxic – small therapeutic window
Plazomicin Aminoglycoside Active against most KPC not active against NDM
iv Phase 3 PL Vs Colistin + Meropenem or tigecyclinefor CRE BSI
Cefiderocol (S-649266) (Shionogi & Co. Ltd.)
Siderophore-β-lactam (cephalosporin)
Broad spectrum Gram-ve including CRE Acinetobacter & Pseudomonas aeruginosa,
iv Phase 3 (no CTs in children)
Biapenem/VaborbactamMeropenem/Vaborbactam (Carbavance, Rempex Pharmaceuticals Inc.)
Carbapenems + β-lactamase-inhibitor
Gram negative including Activity against KPC, CRE
iv Phase 1: currently recruiting children (0-18 yr) (NCT02687906)
Ceftazidime Avibactam(Allergan) Cephlasporin / β-lactamase inhibitor
Active against KPCs and OXA-48 (not active against MBLs)
iv Completed Phase 1Ceftaz/Avi+metronidazole vs Meropenem cIAI and NP Ceftaz/Avi vs doripenem for cUTI

CLICK TO EDIT MASTER PROGRAMME TITLECLICK TO EDIT MASTER PROGRAMME TITLE
www.gardp.org
Thank YouSt Georges, University of London Prof. Mike Sharland, Prof Paul Heath, Julia Bielicki, Laura Folgori, Grace LiPENTA Foundation Prof Carlo Giaquinto, Laura Mangiarini, Davide Bilardi, Daniele DonaUniversity of Antwerp Prof Herman Goossens, Tomislav Kostanyev














![Sepsis neonatal [autoguardado]](https://static.documents.pub/doc/80x56/58e75b911a28ab4a278b506b/sepsis-neonatal-autoguardado.jpg)


