59
Neutropénies auto immunes de l’adulte DES Hématologie - Mars 2017 - Flore Sicre

Neutropénies auto immunes de l’adulte
DES Hématologie
-
Mars 2017
-
Flore Sicre

Définition ?
• Neutropénie avec anticorps-anti granuleux
= « Primary autoimmune neutropenia » Berliner, Blood 2014 Akhtari, Auto-immunity review 2009
Ou
• Neutropénies de mécanismes immunologiques

Définition ?
• Neutropénie avec anticorps-anti granuleux
= « Primary autoimmune neutropenia » Berliner, Blood 2014 Akhtari, Auto-immunity review 2009
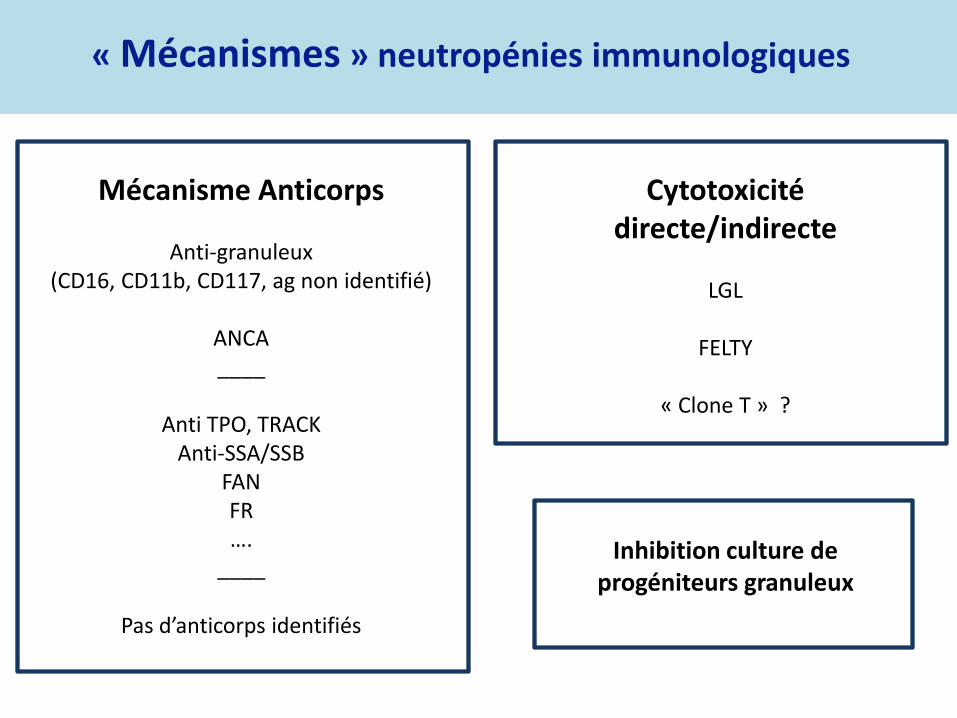
« Mécanismes » neutropénies immunologiques
Mécanisme Anticorps
Anti-granuleux (CD16, CD11b, CD117, ag non identifié)
ANCA ____
Anti TPO, TRACK
Anti-SSA/SSB FAN FR ….
____
Pas d’anticorps identifiés
Cytotoxicité directe/indirecte
LGL
FELTY
« Clone T » ?
Inhibition culture de progéniteurs granuleux
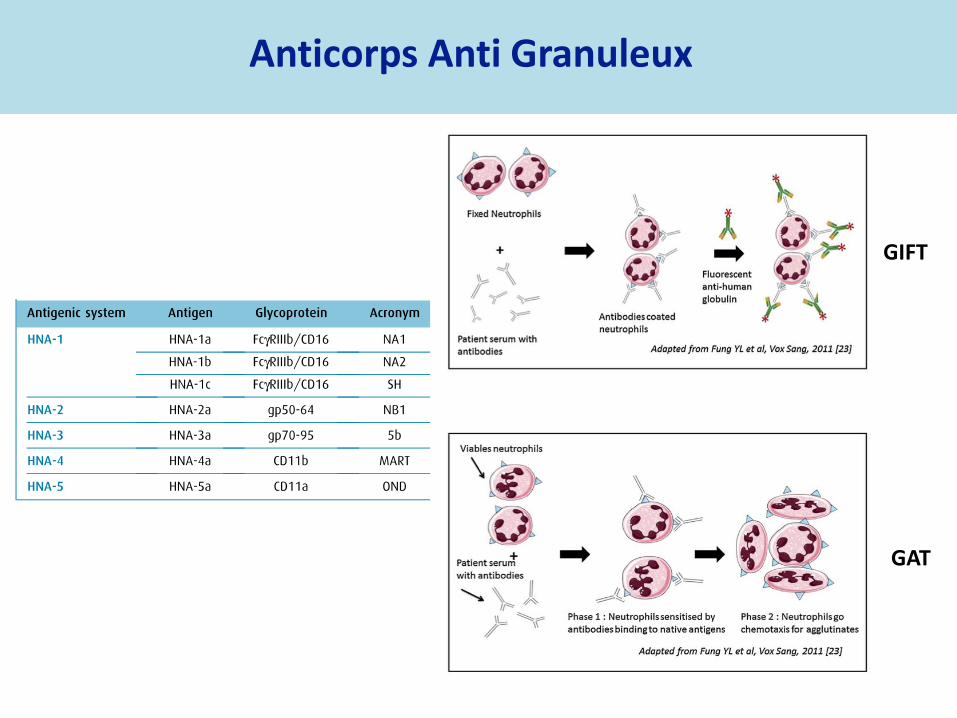
Anticorps Anti Granuleux
GAT
GIFT

MAIGA
Anticorps Anti Granuleux

Difficultés techniques
GIFT : PNN pts GAT : PNN donneur phénotypés
Faux positifs
Anti HLA I Complexes immuns
GCSF Grossesse
Faux négatifs
Faible sensibilité (titre/affinité)
MAIGA
Test + mais Ag non identifié
Anticorps Anti Granuleux

Test d’Inhibition Culture Progéniteurs Granuleux
Myélogramme Hypoplasie granuleuse/ blocage maturation
Culture progéniteurs granuleux MO patient / MO contrôle +
sérum du patient / sérum contrôle AB
Inhibition de la pousse des granuleux par le sérum du patient
Transplantation 2014
Am J Med 1998

Mécanisme immun suspecté mais non identifié
Mère avec une neutropénie chronique sans anticorps identifiés Nourrisson avec neutropénie néonatale transitoire
d’évolution spontanément favorable en 3 à 6 mois
Tests d’inhibition de la culture de progéniteurs granuleux positif sans anticorps identifiés

Identification d‘auto-anticorps & Rôle réel de ces derniers ?
Présence chez certains patients d’anticorps anti granuleux et
d’un clone T ou d’autres auto-anticorps
• Rôle réel dans la survenue de la neutropénie ?
• Marqueurs de dysimmunité

Neutropénies immunologiques
Secondaires
Hémopathies lymphoïdes Connectivites (LES, GSG…)
LGL Déficits immunitaires (DICV, ALPS,
CID) Infections virales
Médicamenteuses
Transplantation
Primitives
« Neutropénies auto-immunes »
« Neutropénies idiopathiques »
« Neutropénies avec clone T »

Epidémiologie
• Fréquence neutropénies ?
Etude Danoise (NFS prescrites par les MG sur 20% population - > 378 000
pts sur 5,5 ans), prévalence neutropénie - Aigue < 1.8 G/L : 2 % - Aigue <1.5 G/L : 0,9 % - Chroniques < 1.8 G/L : 0,12 % - Chroniques < 1.5 G/L : 0,06 %
Andersen, J Intern Med 2016

Epidémiologie
• Fréquence neutropénies ?
Etude Danoise (NFS prescrites par les MG sur 20% population - > 378 000
pts sur 5,5 ans), prévalence neutropénie - Aigue < 1.8 G/L : 2 % - Aigue <1.5 G/L : 0,9 % - Chroniques < 1.8 G/L : 0,12 % - Chroniques < 1.5 G/L : 0,06 %
Etude US (<1.5 G/L) : - « Whites » : 0.8 % - « Afro-americans » : 4.5 % - « Mexican- americans »: 0.38 %
Etude Moyen Orient - « Arabs » : 10.7 % - « Arabs bedouins » : 20 % - Ouganda : 30 %
Andersen, J Intern Med 2016
Hsieh, Ann Intern Med 2007
Denic, BMC Blood disorders , 2009

Epidémiologie
• Facteurs épidémiologiques influençant PNN ?
Etude US : - Ethnie - Age > 18 ans - Sexe masculin - Tabac (ns)
Hsieh, Ann Intern Med 2007

Epidémiologie
• Association entre neutropénie et survenue d’une pathologie ?
Etude Danoise, survenue pathologie dans les 4 ans : maladies auto immunes*, infections virales, hémopathies
Infections virales : VIH +++, HCV, HBV Hémopathies : LAM, MDS
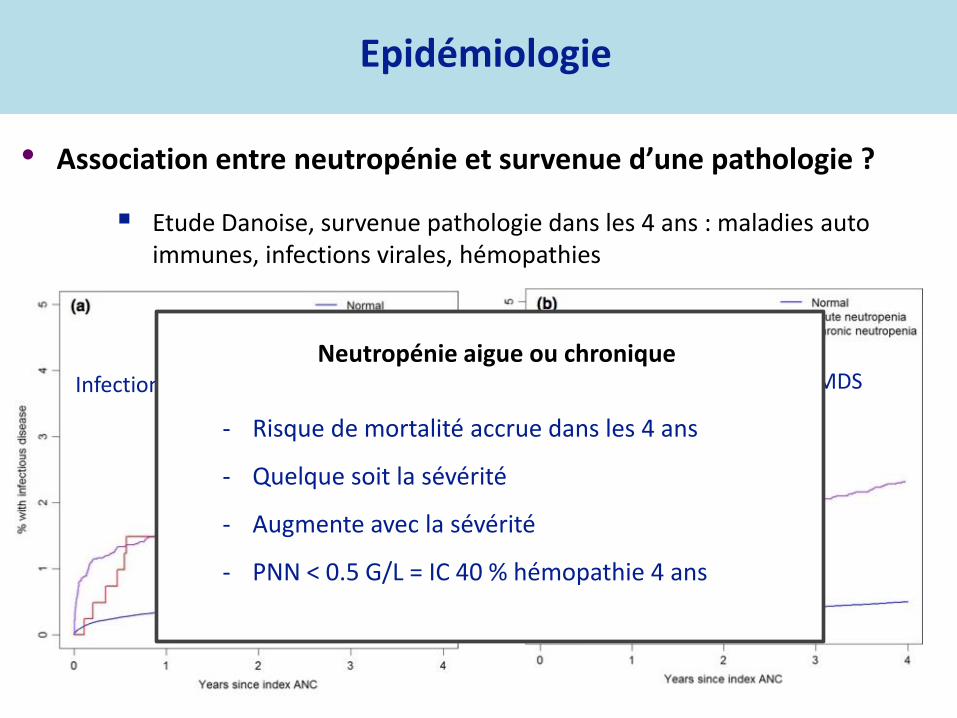
Epidémiologie
• Association entre neutropénie et survenue d’une pathologie ?
Etude Danoise, survenue pathologie dans les 4 ans : maladies auto immunes, infections virales, hémopathies
Infections virales : VIH +++, HCV, HBV Hémopathies : LAM, MDS Neutropénie aigue ou chronique
- Risque de mortalité accrue dans les 4 ans
- Quelque soit la sévérité
- Augmente avec la sévérité
- PNN < 0.5 G/L = IC 40 % hémopathie 4 ans

Epidémiologie
• Association entre neutropénie et survenue d’une pathologie ?
Etude Danoise, survenue pathologie dans les 4 ans : maladies auto immunes, infections virales, hémopathies
Infections virales : VIH +++, HCV, HBV Hémopathies : LAM, MDS
Neutropénie immunologique
1ère étape = diagnostic différentiel

Epidémiologie Neutropénies Immunologiques Primitives
Dale D, Supportive Cancer Therapy 2005
Registre 35 pays 1163 patients Non exhaustif < 0.5 G/L > 3 mois

Epidémiologie Neutropénies Immunologiques Primitives
Registre Français
1993-2014
2134 patients (tout patient signalé)
Sévère Modérée sympto
> 3 mois FU > 1 an
178 pts
Primitive
114
797 constitutionnelles

Neutropénie Isolée de l’adulte : quel bilan ?
Faut il explorer tous les patients adressés pour une neutropénie ?
Qui explorer ? Neutropénies bénignes ou ethniques

Neutropénie Isolée de l’adulte : quel bilan ?
Faut il explorer tous les patients adressés pour une neutropénie ?
Qui explorer ? Neutropénies bénignes ou ethniques
NFS antérieure normale, durée d’évolution ?
Origine ethnique pour les neutropénies modérées
Antécédents personnels & familiaux
Reste de l’hémogramme : monocytopénie, lymphopénie
Manifestations cliniques : aphtose, infections…
Signes cliniques associées

Neutropénie Ethnique ou Bénigne
≠ neutropénie constitutionnelle
= variation de la normale
Asymptomatique
Pas de test biologique ayant VPP/VPN suffisante
Faisceau d’argument (origine ethnique, NFS antérieures, recul)

Neutropénie Ethnique & Duffy
Reduced Neutrophil Count in People of African DescentIs Due To a Regulatory Variant in the Duffy AntigenReceptor for Chemokines Gene
David Reich1,2*, Michael A. Nalls3,4, W. H. Linda Kao5, Ermeg L. Akylbekova6, Art i Tandon1,2, Nick
Patterson2, James Mullikin7, Wen-Chi Hsueh8, Ching-Yu Cheng5,9, Josef Coresh5, Eric Boerwinkle10, Man
Li5, Alicja Waliszewska2,11, Julie Neubauer2, Rongling Li12, Tennille S. Leak13, Lynet te Ekunwe6, Joe C.
Files14, Cheryl L. Hardy14, Joseph M. Zmuda13, Herman A. Taylor15,16,17, Elad Ziv18,19,20, Tamara B.
Harris4, James G. Wilson21,22*
1 Department of Genetics, Harvard Medical School, Boston, Massachusetts, United States of America, 2 Broad Institute of Harvard and MIT, Cambridge, Massachusetts,
United States of America, 3 Laboratory of Neurogenetics, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
4 Laboratory of Epidemiology, Demography and Biometry, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
5 Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America, 6 Jackson Heart Study Analysis Group,
Jackson State University, Jackson, Mississippi, United States of America, 7 Comparative Genomics Unit, Genome Technology Branch, National Human Genome Research
Institute, Rockville, Maryland, United States of America, 8 Division of Medical Genetics, Department of Medicine, Department of Epidemiology and Biostatistics, Institute
for Human Genetics, University of California San Francisco, San Francisco, California, United States of America, 9 Inherited Disease Research Branch, National Human
Genome Research Institute, Baltimore, Maryland, United States of America, 10 Human Genetics Center, University of Texas Health Science Center at Houston, Houston,
Texas, United States of America, 11 Laboratory of Molecular Immunology, Center for Neurologic Disease, Brigham and Women’s Hospital, Boston, Massachusetts, United
States of America, 12 Department of Preventive Medicine, Center for Genomics and Bioinformatics, University of Tennessee Health Science Center, Memphis, Tennessee,
United States of America, 13 Department of Epidemiology, Graduate School of Public Health, University of Pittsburgh, Pittsburgh, Pennsylvania, United States of America,
14 Department of Medicine, Division of Hematology, University of Mississippi Medical Center, Jackson, Mississippi, United States of America, 15 Jackson State University,
Jackson, Mississippi, United States of America, 16 Tougaloo College, Jackson, Mississippi, United States of America, 17 University of Mississippi Medical Center, Jackson,
Mississippi, United States of America, 18 Division of General Internal Medicine, Department of Medicine, University of California San Francisco, San Francisco, California,
United States of America, 19 Department of Epidemiology and Biostatistics, Institute for Human Genetics, University of California San Francisco, San Francisco, California,
United States of America, 20 Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America,
21 V.A. Medical Center, Jackson, Mississippi, United States of America, 22 University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Persistently low white blood cell count (WBC) and neutrophil count is a well-described phenomenon in persons of Africanancestry, whose etiology remains unknown. We recently used admixture mapping to identify an approximately 1-megabaseregion on chromosome 1, where ancestry status (African or European) almost entirely accounted for the difference in WBCbetween African Americans and European Americans. To identify the specific genetic change responsible for thisassociation, we analyzed genotype and phenotype data from 6,005 African Americans from the Jackson Heart Study (JHS),the Health, Aging and Body Composition (Health ABC) Study, and the Atherosclerosis Risk in Communities (ARIC) Study. Wedemonstrate that the causal variant must be at least 91% different in frequency between West Africans and EuropeanAmericans. An excellent candidate is the Duffy Null polymorphism (SNP rs2814778 at chromosome 1q23.2), which is theonly polymorphism in the region known to be so differentiated in frequency and is already known to protect againstPlasmodium vivax malaria. We confirm that rs2814778 ispredictive of WBCand neutrophil count in African Americans abovebeyond the previously described admixture association (P= 3.86 102 5), establishing a novel phenotype for this geneticvariant.
Citat ion: Reich D, Nalls MA, Kao WHL, Akylbekova EL, Tandon A, et al. (2009) Reduced Neutrophil Count in People of African Descent Is Due To a RegulatoryVariant in the Duffy Antigen Receptor for Chemokines Gene. PLoS Genet 5(1): e1000360. doi:10.1371/journal.pgen.1000360
Editor: Peter M. Visscher, Queensland Institute of Medical Research, Australia
Received September 3, 2008; Accepted December 30, 2008; Published January 30, 2009
This is an open-access article distributed under the terms of the Creative Commons Public Domain declaration which stipulates that, once placed in the publicdomain, this work may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose.
Funding: Research support for JHSwas provided by R01-HL-084107 (JGW) from the National Heart, Lung, and Blood Institute and contracts N01-HC-95170, N01-HC-95171, and N01-HC-95172 from the National Heart, Lung, and Blood Institute and the National Center on Minority Health and Health Disparities. Researchsupport for Health ABC was provided by the Intramural Research Program of the National Institute on Aging, and contracts N01-AG-6-2101, N01-AG-6-2103, andN01-AG-6-2106. The Atherosclerosis Risk in Communities Study is a collaborative study supported by National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. Support for the ARIC admixture mapping studies wasprovided by R21DK073482 and K01DK067207 (WHLK). Genotyping for both the JHS and Health ABC was supported by grant U54 RR020278 from the NationalCenter for Research Resources to the Broad Institute of Harvard and MIT; a subsidy from this grant covered half the cost of Health ABC genotyping. DR wassupported by a Burroughs Wellcome Career Development Award in the Biomedical Sciences, and methodological and statistical analysis was supported by grantU01-HG004168.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected] (DR); [email protected] (JGW)
PLoS Genetics | www.plosgenetics.org 1 January 2009 | Volume 5 | Issue 1 | e1000360
Reduced Neutrophil Count in People of African DescentIs Due To a Regulatory Variant in the Duffy AntigenReceptor for Chemokines Gene
David Reich1,2*, Michael A. Nalls3,4, W. H. Linda Kao5, Ermeg L. Akylbekova6, Art i Tandon1,2, Nick
Patterson2, James Mullikin7, Wen-Chi Hsueh8, Ching-Yu Cheng5,9, Josef Coresh5, Eric Boerwinkle10, Man
Li5, Alicja Waliszewska2,11, Julie Neubauer2, Rongling Li12, Tennille S. Leak13, Lynette Ekunwe6, Joe C.
Files14, Cheryl L. Hardy14, Joseph M. Zmuda13, Herman A. Taylor15,16,17, Elad Ziv18,19,20, Tamara B.
Harris4, James G. Wilson21,22*
1 Department of Genetics, Harvard Medical School, Boston, Massachusetts, United States of America, 2 Broad Institute of Harvard and MIT, Cambridge, Massachusetts,
United States of America, 3 Laboratory of Neurogenetics, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
4 Laboratory of Epidemiology, Demography and Biometry, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
5 Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America, 6 Jackson Heart Study Analysis Group,
Jackson State University, Jackson, Mississippi, United States of America, 7 Comparative Genomics Unit, Genome Technology Branch, National Human Genome Research
Institute, Rockville, Maryland, United States of America, 8 Division of Medical Genetics, Department of Medicine, Department of Epidemiology and Biostatistics, Institute
for Human Genetics, University of California San Francisco, San Francisco, California, United States of America, 9 Inherited Disease Research Branch, National Human
Genome Research Institute, Baltimore, Maryland, United States of America, 10 Human Genetics Center, University of Texas Health Science Center at Houston, Houston,
Texas, United States of America, 11 Laboratory of Molecular Immunology, Center for Neurologic Disease, Brigham and Women’s Hospital, Boston, Massachusetts, United
States of America, 12 Department of Preventive Medicine, Center for Genomics and Bioinformatics, University of Tennessee Health Science Center, Memphis, Tennessee,
United States of America, 13 Department of Epidemiology, Graduate School of Public Health, University of Pittsburgh, Pittsburgh, Pennsylvania, United States of America,
14 Department of Medicine, Division of Hematology, University of Mississippi Medical Center, Jackson, Mississippi, United States of America, 15 Jackson State University,
Jackson, Mississippi, United States of America, 16 Tougaloo College, Jackson, Mississippi, United States of America, 17 University of Mississippi Medical Center, Jackson,
Mississippi, United States of America, 18 Division of General Internal Medicine, Department of Medicine, University of California San Francisco, San Francisco, California,
United States of America, 19 Department of Epidemiology and Biostatistics, Institute for Human Genetics, University of California San Francisco, San Francisco, California,
United States of America, 20 Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America,
21 V.A. Medical Center, Jackson, Mississippi, United States of America, 22 University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abstract
Persistently low white blood cell count (WBC) and neutrophil count is a well-described phenomenon in persons of Africanancestry, whose etiology remains unknown. We recently used admixture mapping to identify an approximately 1-megabaseregion on chromosome 1, where ancestry status (African or European) almost entirely accounted for the difference in WBCbetween African Americans and European Americans. To identify the specific genetic change responsible for thisassociation, we analyzed genotype and phenotype data from 6,005 African Americans from the Jackson Heart Study (JHS),the Health, Aging and Body Composition (Health ABC) Study, and the Atherosclerosis Risk in Communities (ARIC) Study. Wedemonstrate that the causal variant must be at least 91% different in frequency between West Africans and EuropeanAmericans. An excellent candidate is the Duffy Null polymorphism (SNP rs2814778 at chromosome 1q23.2), which is theonly polymorphism in the region known to be so differentiated in frequency and is already known to protect againstPlasmodium vivax malaria. We confirm that rs2814778 ispredictive of WBCand neutrophil count in African Americans abovebeyond the previously described admixture association (P= 3.86 102 5), establishing a novel phenotype for this geneticvariant.
Citation: Reich D, Nalls MA, Kao WHL, Akylbekova EL, Tandon A, et al. (2009) Reduced Neutrophil Count in People of African Descent Is Due To a RegulatoryVariant in the Duffy Antigen Receptor for Chemokines Gene. PLoS Genet 5(1): e1000360. doi:10.1371/journal.pgen.1000360
Editor: Peter M. Visscher, Queensland Institute of Medical Research, Australia
Received September 3, 2008; Accepted December 30, 2008; Published January 30, 2009
This is an open-access article distributed under the terms of the Creative Commons Public Domain declaration which stipulates that, once placed in the publicdomain, this work may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose.
Funding: Research support for JHSwas provided by R01-HL-084107 (JGW) from the National Heart, Lung, and Blood Institute and contracts N01-HC-95170, N01-HC-95171, and N01-HC-95172 from the National Heart, Lung, and Blood Institute and the National Center on Minority Health and Health Disparities. Researchsupport for Health ABCwas provided by the Intramural Research Program of the National Institute on Aging, and contracts N01-AG-6-2101, N01-AG-6-2103, andN01-AG-6-2106. The Atherosclerosis Risk in Communities Study is a collaborative study supported by National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. Support for the ARIC admixture mapping studies wasprovided by R21DK073482 and K01DK067207 (WHLK). Genotyping for both the JHS and Health ABC was supported by grant U54 RR020278 from the NationalCenter for Research Resources to the Broad Institute of Harvard and MIT; a subsidy from this grant covered half the cost of Health ABC genotyping. DR wassupported by a Burroughs Wellcome Career Development Award in the Biomedical Sciences, and methodological and statistical analysis was supported by grantU01-HG004168.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected] (DR); [email protected] (JGW)
PLoS Genetics | www.plosgenetics.org 1 January 2009 | Volume 5 | Issue 1 | e1000360
Reduced Neutrophil Count in People of African DescentIs Due To a Regulatory Variant in the Duffy AntigenReceptor for Chemokines Gene
David Reich1,2*, Michael A. Nalls3,4, W. H. Linda Kao5, Ermeg L. Akylbekova6, Art i Tandon1,2, Nick
Patterson2, James Mullikin7, Wen-Chi Hsueh8, Ching-Yu Cheng5,9, Josef Coresh5, Eric Boerwinkle10, Man
Li5, Alicja Waliszewska2,11, Julie Neubauer2, Rongling Li12, Tennille S. Leak13, Lynette Ekunwe6, Joe C.
Files14, Cheryl L. Hardy14, Joseph M. Zmuda13, Herman A. Taylor15,16,17, Elad Ziv18,19,20, Tamara B.
Harris4, James G. Wilson21,22*
1 Department of Genetics, Harvard Medical School, Boston, Massachusetts, United States of America, 2 Broad Institute of Harvard and MIT, Cambridge, Massachusetts,
United States of America, 3 Laboratory of Neurogenetics, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
4 Laboratory of Epidemiology, Demography and Biometry, Intramural Research Program, National Institute on Aging, Bethesda, Maryland, United States of America,
5 Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America, 6 Jackson Heart Study Analysis Group,
Jackson State University, Jackson, Mississippi, United States of America, 7 Comparative Genomics Unit, Genome Technology Branch, National Human Genome Research
Institute, Rockville, Maryland, United States of America, 8 Division of Medical Genetics, Department of Medicine, Department of Epidemiology and Biostatistics, Institute
for Human Genetics, University of California San Francisco, San Francisco, California, United States of America, 9 Inherited Disease Research Branch, National Human
Genome Research Institute, Baltimore, Maryland, United States of America, 10 Human Genetics Center, University of Texas Health Science Center at Houston, Houston,
Texas, United States of America, 11 Laboratory of Molecular Immunology, Center for Neurologic Disease, Brigham and Women’s Hospital, Boston, Massachusetts, United
States of America, 12 Department of Preventive Medicine, Center for Genomics and Bioinformatics, University of Tennessee Health Science Center, Memphis, Tennessee,
United States of America, 13 Department of Epidemiology, Graduate School of Public Health, University of Pittsburgh, Pittsburgh, Pennsylvania, United States of America,
14 Department of Medicine, Division of Hematology, University of Mississippi Medical Center, Jackson, Mississippi, United States of America, 15 Jackson State University,
Jackson, Mississippi, United States of America, 16 Tougaloo College, Jackson, Mississippi, United States of America, 17 University of Mississippi Medical Center, Jackson,
Mississippi, United States of America, 18 Division of General Internal Medicine, Department of Medicine, University of California San Francisco, San Francisco, California,
United States of America, 19 Department of Epidemiology and Biostatistics, Institute for Human Genetics, University of California San Francisco, San Francisco, California,
United States of America, 20 Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America,
21 V.A. Medical Center, Jackson, Mississippi, United States of America, 22 University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Persistently low white blood cell count (WBC) and neutrophil count is a well-described phenomenon in persons of Africanancestry, whose etiology remains unknown. We recently used admixture mapping to identify an approximately 1-megabaseregion on chromosome 1, where ancestry status (African or European) almost entirely accounted for the difference in WBCbetween African Americans and European Americans. To identify the specific genetic change responsible for thisassociation, we analyzed genotype and phenotype data from 6,005 African Americans from the Jackson Heart Study (JHS),the Health, Aging and Body Composition (Health ABC) Study, and the Atherosclerosis Risk in Communities (ARIC) Study. Wedemonstrate that the causal variant must be at least 91% different in frequency between West Africans and EuropeanAmericans. An excellent candidate is the Duffy Null polymorphism (SNP rs2814778 at chromosome 1q23.2), which is theonly polymorphism in the region known to be so differentiated in frequency and is already known to protect againstPlasmodium vivax malaria. We confirm that rs2814778 ispredictive of WBCand neutrophil count in African Americans abovebeyond the previously described admixture association (P= 3.86 102 5), establishing a novel phenotype for this geneticvariant.
Citation: Reich D, Nalls MA, Kao WHL, Akylbekova EL, Tandon A, et al. (2009) Reduced Neutrophil Count in People of African Descent Is Due To a RegulatoryVariant in the Duffy Antigen Receptor for Chemokines Gene. PLoS Genet 5(1): e1000360. doi:10.1371/journal.pgen.1000360
Editor: Peter M. Visscher, Queensland Institute of Medical Research, Australia
Received September 3, 2008; Accepted December 30, 2008; Published January 30, 2009
This is an open-access article distributed under the terms of the Creative Commons Public Domain declaration which stipulates that, once placed in the publicdomain, this work may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose.
Funding: Research support for JHSwas provided by R01-HL-084107 (JGW) from the National Heart, Lung, and Blood Institute and contracts N01-HC-95170, N01-HC-95171, and N01-HC-95172 from the National Heart, Lung, and Blood Institute and the National Center on Minority Health and Health Disparities. Researchsupport for Health ABCwas provided by the Intramural Research Program of the National Institute on Aging, and contracts N01-AG-6-2101, N01-AG-6-2103, andN01-AG-6-2106. The Atherosclerosis Risk in CommunitiesStudy is a collaborative study supported by National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. Support for the ARIC admixture mapping studies wasprovided by R21DK073482 and K01DK067207 (WHLK). Genotyping for both the JHSand Health ABC was supported by grant U54 RR020278 from the NationalCenter for Research Resources to the Broad Institute of Harvard and MIT; a subsidy from this grant covered half the cost of Health ABC genotyping. DR wassupported by a Burroughs Wellcome Career Development Award in the Biomedical Sciences, and methodological and statistical analysis was supported by grantU01-HG004168.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected] (DR); [email protected] (JGW)
PLoS Genetics | www.plosgenetics.org 1 January 2009 | Volume 5 | Issue 1 | e1000360
Phénotype duffy null/null = absence d’expression DARC sur GR (≠ ¢ endotheliales) Récepteur chemokine (CXC et CC) : CXCL8 et RANTES (CCL5) Recrutement des neutrophiles Mécanisme ? Absence de transduction du signal Régulateur des chemokines circulantes
Autres arguments - Phénotype duffy null/null associé à la R Plasmodium vivax - Zones géographiques neutropénies ethniques / paludisme - Phénotype fréquent au sein de la pop juive yéménite
Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lett re3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamat ini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinor i Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108
Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lettre3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamatini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinori Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108
Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lettre3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamat ini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinor i Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108

Neutropénie Ethnique & autres polymorphismes
rs4065321 : 17q12, gène CSF3, R-GCSF • 1 étude européenne • 2 études japonaise GB/PNN plus bas
210 VOLUME 42 | NUMBER 3 | MARCH 2010 NATURE GENETICS
ARTI CLES
The recent progress in genome-wide association studies (GWAS) has
led to the identification of many loci associated with common diseases
as well as with quantitative traits. We report here a GWAS for a range
of hematological and biochemical traits. We used genome-wide SNP
data from ten cohorts including a total of ~14,700 Japanese individuals.
The genotypes were originally obtained as part of the BioBank Japan
project for ongoing GWAS. An advantage of our sample is that the
structure of the Japanese population has been extensively studied1.
Furthermore, individual data for factors that may confound the results
of the association studies were available, and we were able to adjust for
these factors.
RESULTS
The GWAS results are summarized in Table 1 (hematological traits)
and Table 2 (biochemical traits). Quantile-quantile (Q-Q) plots
are shown in Supplementary Figure 1 and Manhattan plots are
shown in Supplementary Figure 2. Regional plots are shown in
Supplementary Figure 3.
White blood cell count
GWAS for white blood cell count (WBC) revealed four newly associ-
ated loci, including rs4895441 in the HBS1L-MYB locus (P = 1.67 ×
10−9), rs3094212 in CDSN-PSORS1C1 in the human MHC region
(P = 6.76 × 10−9), rs445 in CDK6 (P = 2.44 × 10−8) and rs12313946
in the RAP1B-NUP107-SLC35E3-MDM2 locus (Table 1). We also
confirmed the previously reported association of WBC with rs4065321
in the GSDM1-PSMD3-CSF3-MED24-THRA locus2 (P = 2.94 ×
10−14), which includes the CSF3 gene, encoding granulocyte colony-
stimulating factor (Table 1).
Variants in the HBS1L-MYB region were initially reported to be
associated with fetal hemoglobin (HbF) levels in adults3. Subsequently,
variants in the HBS1L-MYB locus were reported to be associated with
red blood cell, platelet and monocyte counts4. In our study, we repli-
cated this association with WBC in a larger data set.
The WBC-associated SNP with the third-lowest P-value, rs3094212,
is located in the human MHC region in 6p21. The fourth-lowest
P-value was observed for rs445 in CDK6 (Table 1). CDK6 encodes
cyclin-dependent kinase-6, which is a regulator of cell cycle progres-
sion. The SNP with the fifth-lowest P-value was rs12313946, which is
located in a linkage disequilibrium (LD) block that includes RAP1B,
NUP107, SLC35E3 and MDM2 (Supplementary Fig. 3a).
Red blood cell traits
We performed GWAS for the following six erythrocyte-related traits:
red blood cell count (RBC), hemoglobin concentration (Hb), hemato-
crit (Ht), mean corpuscular volume (MCV), mean corpuscular
hemoglobin (MCH) and mean corpuscular hemoglobin concentra-
tion (MCHC). In total, we found 8 RBC loci, 2 Hb loci, 2 Ht loci,
15 MCV loci, 15 MCH loci and 7 MCHC loci (Table 1). We confirmed
the previously reported associations of erythrocyte-related traits with
the following ten loci2,4–7: HBS1L-MYB, TMPRSS6, PDGFRA-HK1,
CCND3, RCL1, MARCH8, CITED2, TFRC-ZDHHC19, CD164 and
HBA2-HBA1-LUC7L-ITFG3-RGS11 (Table 1). We also found some
associations between these loci and erythrocyte-related traits that, to
our knowledge, have not been reported previously, including PDGFRA-
HK1 with RBC and MCH, CCND3 with RBC, CD164 with RBC and
MCH, PRKCE with RBC, MARCH8 with MCH, and TYMP with MCH.
Regional plots for these loci are shown in Supplementary Figure 3b.
Genome-wide association study of hematological and biochemical traits in a Japanese population
Yoichiro Kamatani1,2, Koichi Matsuda1, Yukinori Okada3, Michiaki Kubo4, Naoya Hosono4, Yataro Daigo1,2,
Yusuke Nakamura1,5 & Naoyuki Kamatani3
We report genome-wide association studies for hematological and biochemical traits from ~14,700 Japanese individuals. We
identified 60 associations for 8 hematological traits and 29 associations for 12 biochemical traits at genome-wide significance
levels (P < 5 × 10–8). Of these, 46 associations were new to this study and 43 replicated previous reports. We compared these
associated loci with those reported in similar GWAS in European populations. When the minor allele frequency was >10% in
the Japanese population, 32 (94.1%) and 31 (91.2%) of the 34 hematological loci previously reported to be associated in a
European population were replicated with P-values less than 0.05 and 0.01, respectively, and 31 (73.8%) and 27 (64.3%) of the
42 European biochemical loci were replicated.
1Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science and 2Department of Medical Genome Sciences, Graduate School of Frontier
Sciences; the University of Tokyo, Tokyo, Japan. 3Laboratory for Statistical Analysis, 4Laboratory for Genotyping Development and 5Center for Genomic Medicine,
RIKEN, Kanagawa, Japan. Correspondence should be addressed to N.K. ([email protected]).
Received 25 August 2009; accepted 22 December 2009; published online 7 February 2010; doi:10.1038/ng.53 1
© 2
010
Na
ture
Am
eri
ca
, In
c. A
ll r
igh
ts r
es
erv
ed
.
210 VOLUME 42 | NUMBER 3 | MARCH 2010 NATURE GENETICS
ARTI CLES
The recent progress in genome-wide association studies (GWAS) has
led to the identification of many loci associated with common diseases
as well as with quantitative traits. We report here a GWAS for a range
of hematological and biochemical traits. We used genome-wide SNP
data from ten cohorts including a total of ~14,700 Japanese individuals.
The genotypes were originally obtained as part of the BioBank Japan
project for ongoing GWAS. An advantage of our sample is that the
structure of the Japanese population has been extensively studied1.
Furthermore, individual data for factors that may confound the results
of the association studies were available, and we were able to adjust for
these factors.
RESULTS
The GWAS results are summarized in Table 1 (hematological traits)
and Table 2 (biochemical traits). Quantile-quantile (Q-Q) plots
are shown in Supplementary Figure 1 and Manhattan plots are
shown in Supplementary Figure 2. Regional plots are shown in
Supplementary Figure 3.
White blood cell count
GWAS for white blood cell count (WBC) revealed four newly associ-
ated loci, including rs4895441 in the HBS1L-MYB locus (P = 1.67 ×
10−9), rs3094212 in CDSN-PSORS1C1 in the human MHC region
(P = 6.76 × 10−9), rs445 in CDK6 (P = 2.44 × 10−8) and rs12313946
in the RAP1B-NUP107-SLC35E3-MDM2 locus (Table 1). We also
confirmed the previously reported association of WBC with rs4065321
in the GSDM1-PSMD3-CSF3-MED24-THRA locus2 (P = 2.94 ×
10−14), which includes the CSF3 gene, encoding granulocyte colony-
stimulating factor (Table 1).
Variants in the HBS1L-MYB region were initially reported to be
associated with fetal hemoglobin (HbF) levels in adults3. Subsequently,
variants in the HBS1L-MYB locus were reported to be associated with
red blood cell, platelet and monocyte counts4. In our study, we repli-
cated this association with WBC in a larger data set.
The WBC-associated SNP with the third-lowest P-value, rs3094212,
is located in the human MHC region in 6p21. The fourth-lowest
P-value was observed for rs445 in CDK6 (Table 1). CDK6 encodes
cyclin-dependent kinase-6, which is a regulator of cell cycle progres-
sion. The SNP with the fifth-lowest P-value was rs12313946, which is
located in a linkage disequilibrium (LD) block that includes RAP1B,
NUP107, SLC35E3 and MDM2 (Supplementary Fig. 3a).
Red blood cell traits
We performed GWAS for the following six erythrocyte-related traits:
red blood cell count (RBC), hemoglobin concentration (Hb), hemato-
crit (Ht), mean corpuscular volume (MCV), mean corpuscular
hemoglobin (MCH) and mean corpuscular hemoglobin concentra-
tion (MCHC). In total, we found 8 RBC loci, 2 Hb loci, 2 Ht loci,
15 MCV loci, 15 MCH loci and 7 MCHC loci (Table 1). We confirmed
the previously reported associations of erythrocyte-related traits with
the following ten loci2,4–7: HBS1L-MYB, TMPRSS6, PDGFRA-HK1,
CCND3, RCL1, MARCH8, CITED2, TFRC-ZDHHC19, CD164 and
HBA2-HBA1-LUC7L-ITFG3-RGS11 (Table 1). We also found some
associations between these loci and erythrocyte-related traits that, to
our knowledge, have not been reported previously, including PDGFRA-
HK1 with RBC and MCH, CCND3 with RBC, CD164 with RBC and
MCH, PRKCE with RBC, MARCH8 with MCH, and TYMP with MCH.
Regional plots for these loci are shown in Supplementary Figure 3b.
Genome-wide association study of hematological and biochemical traits in a Japanese population
Yoichiro Kamatani1,2, Koichi Matsuda1, Yukinori Okada3, Michiaki Kubo4, Naoya Hosono4, Yataro Daigo1,2,
Yusuke Nakamura1,5 & Naoyuki Kamatani3
We report genome-wide association studies for hematological and biochemical traits from ~14,700 Japanese individuals. We
identified 60 associations for 8 hematological traits and 29 associations for 12 biochemical traits at genome-wide significance
levels (P < 5 × 10–8). Of these, 46 associations were new to this study and 43 replicated previous reports. We compared these
associated loci with those reported in similar GWAS in European populations. When the minor allele frequency was >10% in
the Japanese population, 32 (94.1%) and 31 (91.2%) of the 34 hematological loci previously reported to be associated in a
European population were replicated with P-values less than 0.05 and 0.01, respectively, and 31 (73.8%) and 27 (64.3%) of the
42 European biochemical loci were replicated.
1Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science and 2Department of Medical Genome Sciences, Graduate School of Frontier
Sciences; the University of Tokyo, Tokyo, Japan. 3Laboratory for Statistical Analysis, 4Laboratory for Genotyping Development and 5Center for Genomic Medicine,
RIKEN, Kanagawa, Japan. Correspondence should be addressed to N.K. ([email protected]).
Received 25 August 2009; accepted 22 December 2009; published online 7 February 2010; doi:10.1038/ng.531
© 2
010
Na
ture
Am
eri
ca
, In
c. A
ll r
igh
ts r
es
erv
ed
.
210 VOLUME 42 | NUMBER 3 | MARCH 2010 NATURE GENETICS
ARTI CLES
The recent progress in genome-wide association studies (GWAS) has
led to the identification of many loci associated with common diseases
as well as with quantitative traits. We report here a GWAS for a range
of hematological and biochemical traits. We used genome-wide SNP
data from ten cohorts including a total of ~14,700 Japanese individuals.
The genotypes were originally obtained as part of the BioBank Japan
project for ongoing GWAS. An advantage of our sample is that the
structure of the Japanese population has been extensively studied1.
Furthermore, individual data for factors that may confound the results
of the association studies were available, and we were able to adjust for
these factors.
RESULTS
The GWAS results are summarized in Table 1 (hematological traits)
and Table 2 (biochemical traits). Quantile-quantile (Q-Q) plots
are shown in Supplementary Figure 1 and Manhattan plots are
shown in Supplementary Figure 2. Regional plots are shown in
Supplementary Figure 3.
White blood cell count
GWAS for white blood cell count (WBC) revealed four newly associ-
ated loci, including rs4895441 in the HBS1L-MYB locus (P = 1.67 ×
10−9), rs3094212 in CDSN-PSORS1C1 in the human MHC region
(P = 6.76 × 10−9), rs445 in CDK6 (P = 2.44 × 10−8) and rs12313946
in the RAP1B-NUP107-SLC35E3-MDM2 locus (Table 1). We also
confirmed the previously reported association of WBC with rs4065321
in the GSDM1-PSMD3-CSF3-MED24-THRA locus2 (P = 2.94 ×
10−14), which includes the CSF3 gene, encoding granulocyte colony-
stimulating factor (Table 1).
Variants in the HBS1L-MYB region were initially reported to be
associated with fetal hemoglobin (HbF) levels in adults3. Subsequently,
variants in the HBS1L-MYB locus were reported to be associated with
red blood cell, platelet and monocyte counts4. In our study, we repli-
cated this association with WBC in a larger data set.
The WBC-associated SNP with the third-lowest P-value, rs3094212,
is located in the human MHC region in 6p21. The fourth-lowest
P-value was observed for rs445 in CDK6 (Table 1). CDK6 encodes
cyclin-dependent kinase-6, which is a regulator of cell cycle progres-
sion. The SNP with the fifth-lowest P-value was rs12313946, which is
located in a linkage disequilibrium (LD) block that includes RAP1B,
NUP107, SLC35E3 and MDM2 (Supplementary Fig. 3a).
Red blood cell traits
We performed GWAS for the following six erythrocyte-related traits:
red blood cell count (RBC), hemoglobin concentration (Hb), hemato-
crit (Ht), mean corpuscular volume (MCV), mean corpuscular
hemoglobin (MCH) and mean corpuscular hemoglobin concentra-
tion (MCHC). In total, we found 8 RBC loci, 2 Hb loci, 2 Ht loci,
15 MCV loci, 15 MCH loci and 7 MCHC loci (Table 1). We confirmed
the previously reported associations of erythrocyte-related traits with
the following ten loci2,4–7: HBS1L-MYB, TMPRSS6, PDGFRA-HK1,
CCND3, RCL1, MARCH8, CITED2, TFRC-ZDHHC19, CD164 and
HBA2-HBA1-LUC7L-ITFG3-RGS11 (Table 1). We also found some
associations between these loci and erythrocyte-related traits that, to
our knowledge, have not been reported previously, including PDGFRA-
HK1 with RBC and MCH, CCND3 with RBC, CD164 with RBC and
MCH, PRKCE with RBC, MARCH8 with MCH, and TYMP with MCH.
Regional plots for these loci are shown in Supplementary Figure 3b.
Genome-wide association study of hematological and biochemical traits in a Japanese population
Yoichiro Kamatani1,2, Koichi Matsuda1, Yukinori Okada3, Michiaki Kubo4, Naoya Hosono4, Yataro Daigo1,2,
Yusuke Nakamura1,5 & Naoyuki Kamatani3
We report genome-wide association studies for hematological and biochemical traits from ~14,700 Japanese individuals. We
identified 60 associations for 8 hematological traits and 29 associations for 12 biochemical traits at genome-wide significance
levels (P < 5 × 10–8). Of these, 46 associations were new to this study and 43 replicated previous reports. We compared these
associated loci with those reported in similar GWAS in European populations. When the minor allele frequency was >10% in
the Japanese population, 32 (94.1%) and 31 (91.2%) of the 34 hematological loci previously reported to be associated in a
European population were replicated with P-values less than 0.05 and 0.01, respectively, and 31 (73.8%) and 27 (64.3%) of the
42 European biochemical loci were replicated.
1Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science and 2Department of Medical Genome Sciences, Graduate School of Frontier
Sciences; the University of Tokyo, Tokyo, Japan. 3Laboratory for Statistical Analysis, 4Laboratory for Genotyping Development and 5Center for Genomic Medicine,
RIKEN, Kanagawa, Japan. Correspondence should be addressed to N.K. ([email protected]).
Received 25 August 2009; accepted 22 December 2009; published online 7 February 2010; doi:10.1038/ng.531
© 2
010
Na
ture
Am
eri
ca, In
c. A
ll r
igh
ts r
es
erv
ed
.
rs9131 : 4 q13, CXL2 Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lett re3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamat ini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinor i Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108
Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lettre3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamatini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinori Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108
Genome-Wide Association Study of White Blood CellCount in 16,388 African Americans: the ContinentalOrigins and Genetic Epidemiology Network (COGENT)
Alexander P. Reiner1,2. * , Guillaume Lettre3,4. , Michael A. Nalls5. , Santhi K. Ganesh6. , Rasika Mathias7. ,
Melissa A. Aust in2,8. , Eric Dean9. , Sampath Arepalli5, Angela Brit ton5, Zhao Chen10, David Couper11, J.
David Curb12, Charles B. Eaton13, Myriam Fornage14, Struan F. A. Grant15, Tamara B. Harris16, Dena
Hernandez5, Naoyuki Kamat ini17, Brendan J. Keat ing15, Michiak i Kubo18, Andrea LaCroix1,2, Leslie A.
Lange19, Simin Liu20, Kurt Lohman21, Yan Meng22, Emile R. Mohler III23, Solomon Musani24, Yusuke
Nakamura25, Christopher J. O’Donnell26,27, Yukinor i Okada17, Cameron D. Palmer22, George J.
Papanicolaou26, Kushang V. Patel16, Andrew B. Singleton5, Atsushi Takahashi17, Hua Tang28, Herman A.
Taylor Jr.29,30, Kent Taylor31, Cynthia Thomson32, Lisa R. Yanek7, Lingyao Yang33, Elad Ziv9, Alan B.
Zonderman34, Aaron R. Folsom35" , Michele K. Evans36" , Yongmei Liu21" , Diane M. Becker7" , Beverly M.
Snively33" , James G. Wilson37" *
1 Department of Epidemiology, University of Washington, Seattle, Washington, United States of America, 2 Division of Public Health Sciences, Fred Hutchinson Cancer
Research Center, Seattle, Washington, United States of America, 3 Montreal Heart Institute, Montreal, Canada, 4 Departement de Medecine, Universite de Montreal,
Montreal, Canada, 5 Laboratory of Neurogenetics, National Institute on Aging, National Institutes of Health, Bethesda, Maryland, United States of America, 6 Division of
Cardiovascular Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, United States of America, 7 Department of Medicine, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, United States of America, 8 Department of Epidemiology and Institute for Public Health Genetics, School of
Public Health, University of Washington, Seattle, Washington, United States of America, 9 Department of Medicine, University of California San Francisco, San Francisco,
California, United States of America, 10 Division of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson,
Arizona, United States of America, 11 Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, United States of
America, 12 Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, Hawaii, United States of America, 13 Center for Primary
Care and Prevention, Alpert Medical School of Brown University, Providence, Rhode Island, United States of America, 14 Houston Institute of Molecular Medicine,
University of Texas, Houston, Texas, United States of America, 15 Center for Applied Genomics, Division of Human Genetics, Children’s Hospital of Philadelphia Research
Institute, Philadelphia, Pennsylvania, United States of America, 16 Laboratory for Epidemiology, Demography, and Biometry, National Institute on Aging, National
Institutes of Health, Baltimore, Maryland, United States of America, 17 Laboratory for Statistical Analysis, Center for Genomic Medicine (CGM), Institute of Physical and
Chemical Research (RIKEN), Yokohama, Japan, 18 Laboratory for Genotyping Development, CGM, RIKEN, Yokohama, Japan, 19 Department of Genetics, University of
North Carolina, Chapel Hill, North Carolina, United States of America, 20 Departments of Epidemiology and Medicine, University of California Los Angeles, Los Angeles,
California, United States of America, 21 Center for Human Genomics, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest
University School of Medicine, Winston-Salem, North Carolina, United States of America, 22 Program in Medical and Population Genetics, Broad Institute, Cambridge,
Massachusetts, United States of America, 23 Cardiovascular Division, Vascular Medicine Section, Department of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, Pennsylvania, United States of America, 24 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States of America,
25 Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, University of Tokyo, Tokyo, Japan, 26 National Heart, Lung, and Blood Institute
(NHLBI), Division of Cardiovascular Sciences, Bethesda, Maryland, United States of America, 27 NHLBI’s Framingham Heart Study, Framingham, Massachusetts, United
States of America, 28 Department of Genetics, Stanford University School of Medicine, Stanford, California, United States of America, 29 Jackson State University,
Tougaloo College, Jackson, Mississippi, United States of America, 30 Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi, United States
of America, 31 Medical Genetics Institute, Cedars-Sinai Medical Center, Los Angeles, California, United States of America, 32 Nutritional Sciences, Arizona Cancer Center,
University of Arizona, Tucson, Arizona, United States of America, 33 Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of
Medicine, Winston-Salem, North Carolina, United States of America, 34 Laboratory of Personality and Cognition, National Institute on Aging, National Institutes of Health,
Baltimore, Maryland, United States of America, 35 Division of Epidemiology and Community Health, University of Minnesota, Minneapolis, Minnesota, United States of
America, 36 Health Disparities Research Section, Clinical Research Branch, National Institute on Aging, National Institutes of Health, Baltimore, Maryland, United States of
America, 37 Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi, United States of America
Abst ract
Total white blood cell (WBC) and neutrophil counts are lower among individuals of African descent due to the commonAfrican-derived ‘‘null’’ variant of the Duffy Antigen Receptor for Chemokines (DARC) gene. Additional common geneticpolymorphisms were recently associated with total WBC and WBC sub-type levels in European and Japanese populations.No additional loci that account for WBC variability have been identified in African Americans. In order to address this, weperformed a large genome-wide association study (GWAS) of total WBCand cell subtype counts in 16,388 African-Americanparticipants from 7 population-based cohorts available in the Continental Origins and Genetic Epidemiology Network.In addition to the DARC locus on chromosome 1q23, we identified two other regions (chromosomes 4q13 and 16q22)
PLoS Genetics | www.plosgenetics.org 1 June 2011 | Volume 7 | Issue 6 | e1002108
rs12149261 and every other typed SNP in the genome. There
was reduced local LD within the chromosome 16 duplicated
region, relative to the surrounding chromosome 16 SNP (FigureS5). Three SNPshad r-squared valuesof . 0.20 with rs12149261:
one located 20 kb away on chromosome 16 in the HYDIN gene
(rs1774524; r2= 0.27), and two located on chromosome 1 at, 120 Mb near the HYDIN paralogue (rs12087334 and
rs4659245; r2= 0.25 and 0.22, respectively). Moreover, com-bined analysis of the 4 cohorts typed on the Affymetrix GWA
platform showed that the chromosome 16q22 association signalat rs12149261 (P= 2.126 102 18) was completely abolished after
conditioning on chromosome 1 DARC rs2814778 (P= 0.36).
While defects in theHYDIN gene result in hydrocephalus[19,20],this genomic region has not previously been associated with
WBC. Together, these results demonstrate that the chromosome
16 HYDIN association finding is most likely a probe cross-hybridization artifact due to inter-chromosomal sequence simi-
larity with the duplicated segment on chromosome 1q21 near the
DARC region and that the polymorphisms associated with WBC
in the studies using the Affymetrix arrays actually map to the
chromosome 1 region.
Discovery of a novel CXCL2 association finding on
chromosome 4q13 and replication in other ethnic
populations
A novel SNP association on chromosome 4q13 was identified
in our African-American WBC discovery GWAS. The lead SNP
rs9131 is located in the 39 UTR of the CXCL2 gene, which
encodes a macrophage-derived chemotactic cytokine for
polymorphonuclear leukocytes. In African Americans, the
minor T allele (MAF= 23%) was associated with lower WBC.
Several additional SNPs in the chromosome 4 chemokine gene
cluster had P-values ranging from 102 5 to 102 7, including
rs2367291 located upstream of CXCL1 (Figure 3A) Further
adjustment for rs9131, however, abolished these associations
(data not shown). Based on HapMap phase 2 and 1000 genomes
data, rs9131 is in perfect LD with 7 other inter-genic SNPs in
Figure 2. Manhattan plot of meta-analysis P-values in GWAS for total WBC count. Horizontal axis indicates chromosomal position. Verticalaxis indicates 2 log10 P-values from inverse variance-weighted fixed effects meta-analysis. The red horizontal line indicates the genome-widesignificance threshold of P= 2.56 102 8. Association signals are present at 1q23, 4q13, and 16q22. The P-values for the broad chromosome 1 signal aretruncated at 102 20. This region spans nearly 90 Mb on both arms of chromosome 1 and results artifactually in two apparently distinct peaks becauseof the lack of genotyped or imputed SNPs around the centromere.doi:10.1371/journal.pgen.1002108.g002
Table 3. Meta-analysis results of genome-wide significant SNPs for white blood cell count subtypes.
Cell type Chromosome 1q23 DARC rs2814778 T allele Chromosome 4q13 CXCL2 rs9131 T allele
N Effect size (Standard Error) P-value N Effect size (Standard Error) P-value
Neutrophils 5609 +0.305 (0.009) 1.06 102 237 7353 2 0.038 (0.008) 1.56 102 6
Lymphocytes 5642 +0.020 (0.007) 3.86 102 3 7390 +0.010 (0.005) 0.06
Monocytes 5593 +0.048 (0.004) 6.06 102 27 7330 2 0.004 (0.004) 0.23
Eosinophils 5411 +0.012 (0.003) 8.66 102 5 6402 2 0.0005 (0.003) 0.85
Basophils 5104 +0.002 (0.0008) 3.56 102 3 6052 2 0.0007 (0.0007) 0.27
Effect size represents the effect of a minor allele on natural log-transformed white blood cell count.
doi:10.1371/journal.pgen.1002108.t003
GWAS of WBC in African Americans
PLoS Genetics | www.plosgenetics.org 5 June 2011 | Volume 7 | Issue 6 | e1002108

Neutropénie Ethnique & autres polymorphismes
CXCL2=MIP2α
• Sécrétée ds les tissus peripheriques (infection, inflammation) : chimiotactisme
• R= CXCR2
• Souris : IV -> polynucléose (idem GCSF)
• Migration PNN : moelle -> sang peripherique
The Journal of Clinical Investigation http:/ /www.jci.org Volume 120 Number 7 July 2010
of neutrophils in the blood were from Cxcr2–/– cells (P < 0.0001).
Of note, the number of neutrophils in the spleen, another reser-
voir for neutrophils, was comparable between Cxcr2–/– and WT
cells (Figure 1C). Neutrophil trafficking from the bone marrow
was estimated by calculating the percentage of neutrophils in the
blood relative to the total number of neutrophils in the blood,
bone marrow, and spleen (neutrophil distribution index; NDI;
ref. 5). Consistent with previous studies (22, 38), under basal
conditions, 1.84% ± 0.32% of WT neutrophils were present in the
blood (Figure 1D). In contrast, the percentage of Cxcr2–/– neutro-
phils in the blood was 0.57% ± 0.18% (P = 0.02). No perturbation
in other hematopoietic lineages was observed (Figure 1E), which
indicates that the observed differences in neutrophil chimerism
are not caused by altered engraftment of Cxcr2–/– hematopoietic
stem cells. Consistent with this observation, the number and
cytokine responsiveness of myeloid progenitors in the bone mar-
row were comparable between WT and Cxcr2–/– cells (Figure 1F).
Myelokathexis is characterized by the accumulation of mature,
often hypersegmented or dysplastic, neutrophils in the bone mar-
row (10). Consistent with this phenotype, we observed that the
percentage of Gr-1hiSSChi cells — representing the most mature
neutrophils (39) — relative to the total Gr-1+ myeloid cell popula-
tion was higher for Cxcr2–/– than WT cells (Figure 2, A and B). To
confirm this finding, Cxcr2–/– and WT Gr-1+ myeloid cells were
m
m
m
Downloaded from http://www.jci.org on March 16, 2015. http://dx.doi.org/10.1172/JCI41649
The Journal of Clinical Investigation http:/ /www.jci.org Volume 120 Number 7 July 2010
of neutrophils in the blood were from Cxcr2–/– cells (P < 0.0001).
Of note, the number of neutrophils in the spleen, another reser-
voir for neutrophils, was comparable between Cxcr2–/– and WT
cells (Figure 1C). Neutrophil trafficking from the bone marrow
was estimated by calculating the percentage of neutrophils in the
blood relative to the total number of neutrophils in the blood,
bone marrow, and spleen (neutrophil distribution index; NDI;
ref. 5). Consistent with previous studies (22, 38), under basal
conditions, 1.84% ± 0.32% of WT neutrophils were present in the
blood (Figure 1D). In contrast, the percentage of Cxcr2–/– neutro-
phils in the blood was 0.57% ± 0.18% (P = 0.02). No perturbation
in other hematopoietic lineages was observed (Figure 1E), which
indicates that the observed differences in neutrophil chimerism
are not caused by altered engraftment of Cxcr2–/– hematopoietic
stem cells. Consistent with this observation, the number and
cytokine responsiveness of myeloid progenitors in the bone mar-
row were comparable between WT and Cxcr2–/– cells (Figure 1F).
Myelokathexis is characterized by the accumulation of mature,
often hypersegmented or dysplastic, neutrophils in the bone mar-
row (10). Consistent with this phenotype, we observed that the
percentage of Gr-1hiSSChi cells — representing the most mature
neutrophils (39) — relative to the total Gr-1+ myeloid cell popula-
tion was higher for Cxcr2–/– than WT cells (Figure 2, A and B). To
confirm this finding, Cxcr2–/– and WT Gr-1+ myeloid cells were
m
m
m
Downloaded from http://www.jci.org on March 16, 2015. http://dx.doi.org/10.1172/JCI41649

Persistent ANC < 1.5 109/L
Isolated
• Familial history
• Clinical evaluation
Clinical & biological evaluation
- Myeloid and lymphoid malignancies
- Secondary immune neutropenia
- Large Granular Leukemia
- Primary immune deficiency
- HIV and HCV infections
Chronic Primary Neutropenia
Evaluate neutrophil antibodies
- Early onset
- Cyclic neutropenia
- Familial history of neutropenia
or myeloid malignancies
- Lymphoedema, warts,
pulmonary disease,
immunodeficiency or
monocytopenia
Suspect
&
Evaluate
Genetic disease
Chronic
Secondary
Neutropenia
Yes
No
Yes
No
Blood 2015
Ethnic neutropenia
- Moderate
- Ancient
- No symptoms
- Ethnical origin
=> surveillance
Neutropénies immunologiques secondaires
• Neutropénies médicamenteuses
• Neutropénies AI associées aux hémopathies lymphoïdes
• LLC
• LNH B bas grade
Schivdel, Ann Hematol 2013
Visco, Am J Hematol 2014
Rare Anti PNN ou chronic T cell lymphocytosis (Rustagi, BJH 1987) Complications infectieuses, pronostique sévère (EVANS)

Neutropénies & Maladies Auto-immunes
• Lupus érythémateux disséminé
• Syndrome de Goujerot Sjogren
• Thyroidite auto-immunes
• ANCA

Lupus érythémateux disséminé
• 3 études de prévalence
• Neutropénie modérée ++
• 25-40 % ( def PNN < 1.5-2.5 G/L)
• Neutropénie sévère < 4%
• Associée à l’évolutivité de la maladie
• Association aux infections controversée (TTT IS)
• Réponse GCSF
Linda, Sem Arth Rheum 2014

Neutropénie et Goujerot Sjogren
PNN < 1 G/L (10%) : 50% hospitalisation pour infection (vs 9%, p=0.002) Facteur prédictif majeur LNH

Neutropénies & thyroïdites auto immunes
• Association fréquente ++
• Chronologie variable
• Evolution dissociée
• Lien de causalité ?
• Cases reports ++
• Marqueur d’auto-immunité à rechercher +++
Neutropénie et ANCA
• Neutropénie sévère
• Mécanisme humoral ++
• Association à des vascularites à ANCA rares
• Formes le + souvent cutanées
Antineutrophil Cytoplasmic Antibodies, Autoimmune
Neutropenia, and Vasculitis
Peter C. Grayson, MD1, J. Mark Sloan, MD2, John L. Niles, MD3, Paul A. Monach, MD, PhD1,
and Peter A. Merkel, MD, MPH1
1Vasculitis Center, Section of Rheumatology and the Clinical Epidemiology Unit, Department of
Medicine, Boston University Medical Center, Boston, MA
2Section of Hematology/Oncology, Department of Medicine, Boston University Medical Center,
Boston, MA
3Renal Unit, Department of Medicine, Massachusetts General Hospital, Boston, MA
Abstract
Objectives—Reports of an association between antineutrophil cytoplasmic antibodies (ANCA)
and autoimmune neutropenia have rarely included cases of proven vasculitis. A case of ANCA-
associated vasculitis (AAV) with recurrent neutropenia is described and relevant literature on the
association between ANCA, neutropenia, and vasculitis is reviewed.
Methods—Longitudinal clinical assessments and laboratory findings are described in a patient
with AAV and recurrent episodes of profound neutropenia from December 2008 – October 2010.
A PubMed database search of the medical literature was performed for papers published from
1960 through October 2010 to identify all reported cases of ANCA and neutropenia.
Results—A 49 year-old man developed recurrent neutropenia, periodic fevers, arthritis, biopsy-
proven cutaneous vasculitis, sensorineural hearing loss, epididymitis, and positive tests for ANCA
with specificity for antibodies to both proteinase 3 and myeloperoxidase. Antineutrophil
membrane antibodies were detected during an acute neutropenic phase and were not detectable in
a post-recovery sample, whereas ANCA titers did not seem to correlate with neutropenia. An
association between ANCA and neutropenia has been reported in 74 cases from 24 studies in the
context of drug/toxin exposure, underlying autoimmune disease, or chronic neutropenia without
underlying autoimmune disease. In these cases, the presence of atypical ANCA patterns and other
antibodies were common; however, vasculitis was uncommon and when it occurred was usually
limited to the skin and in cases of underlying toxin exposure.
Conclusions—ANCA is associated with autoimmune neutropenia, but systemic vasculitis rarely
occurs in association with ANCA and neutropenia. The interaction between neutrophils and
ANCA may provide insight into understanding both autoimmune neutropenia and AAV.
© 2011 Elsevier Inc. All rights reserved
Corresponding Author: Peter C. Grayson MD Vasculitis Center, Section of Rheumatology Boston University School of Medicine 72East Concord Street Boston, MA 02118 [email protected] phone: 617-414-2508 Fax: 617-414-2510. Reprint Requests: Peter A.Merkel, MD, MPH Vasculitis Center, Section of Rheumatology Boston University School of Medicine 72 East Concord StreetBoston, MA 02118.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our
customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of
the resulting proof before it is published in its final citable form. Please note that during the production process errors may be
discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
COMPETING INTERESTS None
NIH Public AccessAuthor ManuscriptSemin Arthritis Rheum. Author manuscript; available in PMC 2012 December 1.
Published in final edited form as:
Semin Arthritis Rheum. 2011 December ; 41(3): 424–433. doi:10.1016/j.semarthrit.2011.02.003.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t
Grayson, Semin Arthritis and Rheum 2011
Original article
Antineutrophil cytoplasmic antibody-associated neutropenia
Paul Coppoa,1, David Gheza,1, Vincent Fuentesb, Djaouida Bengoufac, Eric Oksenhendlera,Bruno Triboutd, Jean-Pierre Clauvela, Kaiss Lassouedb,*
aService d’Immuno-Hematologie, Hopital Saint-Louis, ParisbService d’Immunologie, CHU d’Amiens, France
cLaboratoire d’Immunopathologie, Hopital Saint-Louis, ParisdService de Pathologie Vasculaire, CHU d’Amiens, France
Received 14 January 2004; received in revised form 1 July 2004; accepted 31 August 2004
Abstract
Background: Antineutrophil cytoplasmic antibodies (ANCA) can be associated with various disorders. However, their association with
neutropenia has never been reported.
Methods: Nine patients with chronic unexplained neutropenia and ANCA were studied. Clinical charts were extensively analyzed and all
patients underwent hematological and immunological investigations.
Results: All patients (6 women and 3 men) were Caucasian and had a mean age of 49 years (range 16–67 years). All presented with a
neutropenia below 1.5 109/L for more than 6 months. The neutropenia was b0.5 109/L in six cases and moderate in three. There was no
evidence of toxic- or drug-related neutropenia or of ahematological malignancy. Autoimmune anemiaand/or thrombocytopenia werepresent
in five patients. ANCA, with various specificities, were present in all patients. ANCA were associated with various other autoantibodies in
eight patients, including antisurface-neutrophil antibodies in three cases. Four of the six patients with severe neutropenia experienced
infections. Five patients were treated with hematopoietic growth factors, steroids, intravenous immunoglobulins, splenectomy, methotrexate
and/or cyclophosphamide, allowing the neutrophil count to be restored transiently or permanently.
Conclusions: A subset of patients with neutropenia of possible autoimmune origin may develop ANCA. Their detection would provide
strong evidence of an autoimmune mechanism. Neutropenia should be added to the list of ANCA-associated diseases.
D 2004 Elsevier B.V. All rights reserved.
Keywords: Neutropenia; Antineutrophil cytoplasmic antibodies; Autoimmunity
1. Introduction
Antineutrophil cytoplasmic antibodies (ANCA) are
autoantibodies that are directed against different neutrophil
antigens. When detected by immunofluorescence on etha-
nol-fixed human neutrophils, ANCA usually displays three
major patterns: cytoplasmic (cANCA), perinuclear
(pANCA), and atypical (xANCA). The main targets of
ANCA are either myeloperoxydase (MPO) or proteinase 3
(PR3) [1–4], but they may also be directed against
lactoferrin, elastase, cathepsin, lysozyme [5], bactericidal
permeability increasing protein (BPI), and azurocidin [6].
ANCA are observed in a large spectrum of diseases [7–19].
Their specificity can make them a helpful tool in the
diagnosis of primary systemic vasculitides [20]. Anti-PR3
antibodies (Abs) are strongly associated with Wegener’s
diseaseand, to a lesser extent, with microscopic polyarteritis
and necrotizing crescentic glomerulonephritis [7–9]. Anti-
MPO antibodies are often associated with systemic vascu-
litis but can also be found in various autoimmune disorders
and connective tissuediseaseswithout evidenceof vasculitis
[10,11,13,14,16–18]. Other specificity is not considered to
0953-6205/$ - see front matter D 2004 Elsevier B.V. All rights reserved.
doi:10.1016/j.ejim.2004.08.009
* Corresponding author. Service d’Immunologie, Faculte deMedecine,
3 rue des Louvels, F-80036 Amiens Cedex 1, France. Tel.: +33 3 22 82 79
06; fax: +33 3 22 82 79 07.
E-mail address: [email protected] (K. Lassoued).1 Contributed equally to this work.
European Journal of Internal Medicine 15 (2004) 451–459
www.elsevier.com/locate/ejim
Coppo Eur J Int Med 2011

Lympho-proliférations LGL T & NK
• Caractérisation phénotypique (CMF) :
• LGL T : TCRαβ, CD3+ CD8+ CD4- CD57+.
• LGL NK : CD3-CD8+CD57+CD16+
• Clone T : LGL T, syndrome de Felty
OMS 2008
leucémies à LGL T
lymphoproliférations chroniques NK
Excès de LGL, > 6 mois, sans autre étiologie
Critères diagnostiques n’incluent ni clonalité, ni seuil
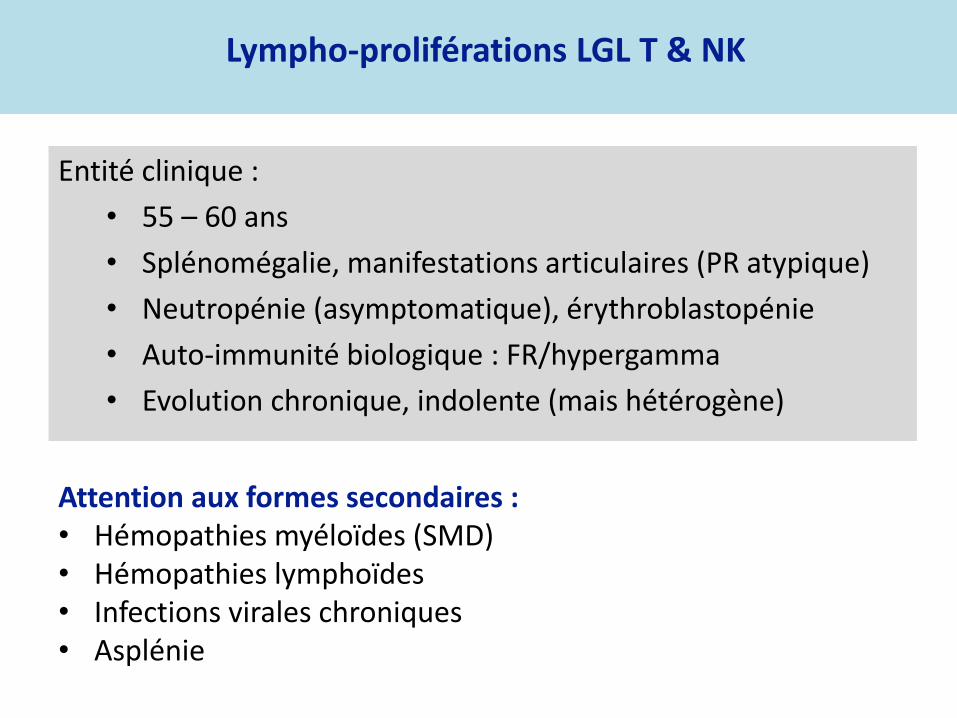
Entité clinique :
• 55 – 60 ans
• Splénomégalie, manifestations articulaires (PR atypique)
• Neutropénie (asymptomatique), érythroblastopénie
• Auto-immunité biologique : FR/hypergamma
• Evolution chronique, indolente (mais hétérogène)
Lympho-proliférations LGL T & NK
Attention aux formes secondaires : • Hémopathies myéloïdes (SMD) • Hémopathies lymphoïdes • Infections virales chroniques • Asplénie

Lympho-proliférations LGL T & NK
Dinmohamed AG
1ère étude prévalence non biaisée Registre des cancer aux Pays Bas = Exhaustivité > 95%
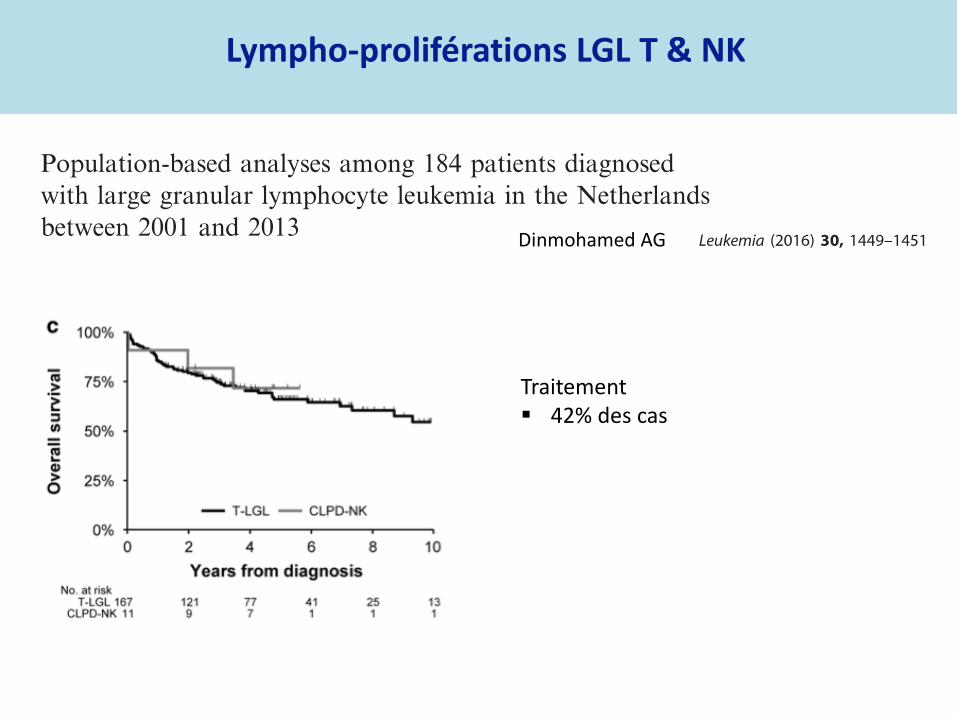
Lympho-proliférations LGL T & NK
Dinmohamed AG
Traitement 42% des cas

Lympho-proliférations LGL T & NK
Dinmohamed AG
Traitement 42% des cas Equivalent à prévalence de 1600 cas en France sur 20 ans

Somatic STAT3 Mutations in Large Granular Lymphocytic
Leukemia
Hanna L.M. Koskela, M.D., Samuli Eldfors, M.Sc., Pekka Ellonen, B.Sc., Arjan J. van
Adrichem, M.Sc., Heikki Kuusanmäki, B.Sc., Emma I. Andersson, B.Sc., Sonja Lagström,
M.Sc., Michael J. Clemente, M.Sc., Thomas Olson, B.Sc., Sari E. Jalkanen, M.Sc., Muntasir
Mamun Majumder, M.Sc., Henrikki Almusa, M.Sc., Henrik Edgren, M.Sc., Maija Lepistö,
M.Sc., Pirkko Mattila, Ph.D., Kathryn Guinta, B.Sc., Pirjo Koistinen, M.D., Ph.D., Taru
Kuittinen, M.D., Ph.D., Kati Penttinen, B.M., Alun Parsons, M.Sc., Jonathan Knowles, Ph.D.,
Janna Saarela, M.D. Ph.D., Krister Wennerberg, Ph.D., Olli Kallioniemi, M.D., Ph.D., Kimmo
Porkka, M.D., Ph.D., Thomas P. Loughran Jr., M.D., Caroline A. Heckman, Ph.D., Jaroslaw
P. Maciejewski, M.D., Ph.D., and Satu Mustjoki, M.D., Ph.D.
Hematology Research Unit Helsinki, Department of Medicine, University of Helsinki and Helsinki
University Central Hospital (H.L.M.K., E.I.A., S.E.J., K. Penttinen, K. Porkka, S.M.), the Institute
for Molecular Medicine Finland (S.E., P.E., A.J.A., H.K., S.L., M.M.M., H.A., H.E., M.L., P.M.,
A.P., J.K., J.S., K.W., O.K., C.A.H.), and the Haartman Institute (P.M.), University of Helsinki,
Helsinki; the Department of Medicine, Oulu University Hospital and University of Oulu, Oulu
(P.K.); and the Department of Medicine, Kuopio University Hospital, Kuopio (T.K.) — all in
Finland; the Department of Translational Hematology and Oncology Research, Taussig Cancer
Institute, Cleveland Clinic, Cleveland (M.J.C., K.G., J.P.M.); and Penn State Hershey Cancer
Institute, Pennsylvania State College of Medicine, Hershey (T.O., T.P.L.).
Abstract
BACKGROUND—T-cell large granular lymphocytic leukemia is a rare lymphoproliferative
disorder characterized by the expansion of clonal CD3+CD8+ cytotoxic T lymphocytes (CTLs)
and often associated with autoimmune disorders and immune-mediated cytopenias.
METHODS—We used next-generation exome sequencing to identify somatic mutations in CTLs
from an index patient with large granular lymphocytic leukemia. Targeted resequencing was
performed in a well-characterized cohort of 76 patients with this disorder, characterized by clonal
T-cell–receptor rearrangements and increased numbers of large granular lymphocytes.
RESULTS—Mutations in the signal transducer and activator of transcription 3 gene ( STAT3)
were found in 31 of 77 patients (40%) with large granular lymphocytic leukemia. Among these 31
patients, recurrent mutational hot spots included Y640F in 13 (17%), D661V in 7 (9%), D661Y in
7 (9%), and N647I in 3 (4%). All mutations were located in exon 21, encoding the Src homology 2
(SH2) domain, which mediates the dimerization and activation of STAT protein. The amino acid
changes resulted in a more hydrophobic protein surface and were associated with phosphorylation
of STAT3 and its localization in the nucleus. In vitro functional studies showed that the Y640F
and D661V mutations increased the transcriptional activity of STAT3. In the affected patients,
downstream target genes of the STAT3 pathway (IFNGR2, BCL2L1, and JAK2) were up-
Copyright © 2012 Massachusetts Medical Society.
Address reprint requests to Dr. Mustjoki at the Hematology Research Unit Helsinki, University of Helsinki and Helsinki UniversityCentral Hospital, P.O. Box 700, Haartmaninkatu 8, FIN-00029 Helsinki, Finland, or at [email protected]. Koskela, Loughran, Heckman, and Maciejewski and Mr. Eldfors contributed equally to this article.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
NIH Public AccessAuthor ManuscriptN Engl J Med. Author manuscript; available in PMC 2013 June 26.
Published in final edited form as:
N Engl J Med. 2012 May 17; 366(20): 1905–1913. doi:10.1056/NEJMoa1114885.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
t
Mutations gain de fonction STAT3 exon 21 40% LGL T Associée neutropénie et RA
NEJM 2012
213 pts STAT3* : 43% LGL T et 18% LGL NK 17% plusieurs mutations :
- Coexistence de plusieurs clones STAT3 mutations différentes - Coexistence de plusieurs mutations même clone
Pas d’association avec neutropénie Association > 1 mutation avec RA
Lympho-proliférations LGL T & NK

Phénotype biologique :
• Neutropénie, erythroblastopénie
• FR
• Hypergamma polyclonale
Pronostic : bon
• Formes clonales / tumorales
• Infections sévères rares
Traitements ? Edx, CsA, Mtx
Bareau B Haematologica 2010
Lympho-proliférations LGL T & NK

Neutropénies immunologiques & Déficit Immunitaires
• DICV • ALPS • CID
• IPEX / CD25 deficiency • Neutropénies sévères congénitales • Syndrome MonoMAC
Euroclass trial, Wehr Blood 2008

Explorations minimales
Frottis
Myélogramme + caryo, pas systématique mais toujours - si < 0,5 G/L (1 G/L pour certains) - Si infection(s) - Si autre anomalie même minime (thrombopénie, macrocytose…)
Phénotype lymphocytaire avec recherche de LGL T & NK et hémopathie
lymphoïde B
EPP : hypo ou hypergamma, pic
Sérologies hépatites B, C et VIH
FAN, FR, Anti SSA/SSB
BOM pour certains en cas de neutropénie profonde et myélo NC

Neutropénies secondaires
Sicre Blood 2015
Etude rétrospective (cohorte prospective) : 108 pts PNN < 0,5 ou < 1 G/L + spt FU médian 8.3 ans
Table S2: Causes of exclusion from the study
Patients excluded
All patients 123
Gender male 37 /123 (30%)
Exclusion reason
Pancytopenia 3 /123 (2.4%)
ANC > 0.5 109/L 39 /123 (31.7%)
Transitory neutropenia 1 (<1%)
Follow up < 1year or lack of data 22 /123 (17.9%)
Congenital neutropenia 14 /123 (11.4%)
Suspected* 11
Confirmed 3
MonoMAC syndrome 1
ELANE mutation 1
G6PC3 mutation 1
Large granular leukemia 14 /123 (11.4%)
Felty's syndrome 4 /123 (3.25%)
Sjogren's syndrome 11 (8.9%)
Systemic lupus erythematosus 2 (1.6%)
Myelodysplastic syndrome 8 (6.5%)
Others 5 (4.0%)
Others hematological malignancies 1
HCV infection 1
HIV infection 1
Drug toxicity 2
Footnotes: in the absence of genetic confirmation, congenital neutropenia was considered when the first
manifestations were reported during infancy (5 patients) and/or when an associated congenital organ dysfunction
(3 patients) was present, when neutropenia was diagnosed in a first degree relative (1 patient) or when an
immune deficiency was associated (2 patients).
Exclus 123 patients

Neutropénies immunologiques primitives
= Neutropénies « auto-immunes » primitives
+ Neutropénies chroniques idiopathiques
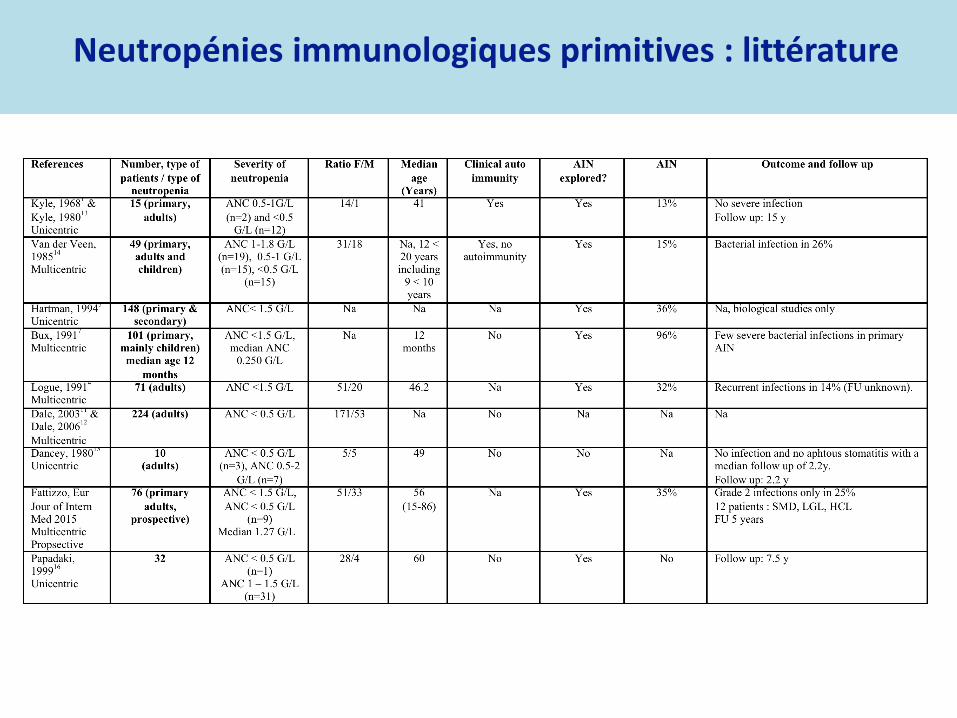
Neutropénies immunologiques primitives : littérature

Neutropénies immunologiques primitives : épidémiologie
Sicre Blood 2015
Etude rétrospective (cohorte prospective) : 108 pts PNN < 0,5 ou < 1 G/L + spt FU médian 8.3 ans

Neutropénies immunologiques primitives : épidémiologie
Sicre Blood 2015
Etude rétrospective (cohorte prospective) : 108 pts PNN < 0,5 ou < 1 G/L symptomatique FU médian 8.3 ans
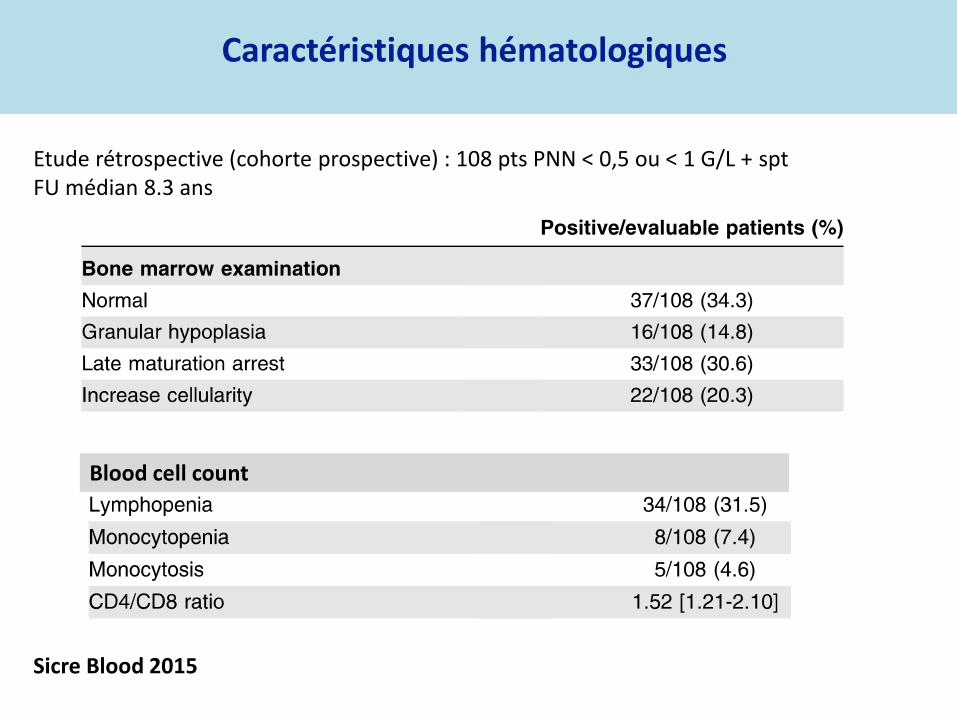
Caractéristiques hématologiques
Sicre Blood 2015
Etude rétrospective (cohorte prospective) : 108 pts PNN < 0,5 ou < 1 G/L + spt FU médian 8.3 ans
Blood cell count

Caractéristiques immunologiques
Sicre Blood 2015
Gammaglobulins

Complications infectieuses
Sicre Blood 2015

Complications infectieuses
Sicre Blood 2015
Table S4: Severe bacterial infections
Severe bacterial infections
Number of patients with severe bacterial infections
At least 1 27/108 (24.5%)
1 15/108 (13.9%)
2 7/108 (6.5%)
3 5/108 (4.6%)
Total number of severe bacterial infections 45
Abscess/cellulitis 24 (53%)
Pneumonia 7 (15%)
Tonsil phlegmon's 4 (9%)
Pyelonephritis 4 (9%)
Peritonitis 2
Adenitis 2
Osteitis 1
Arthritis 1
Septic shock 2
Intensive care unit admission 3
Table S4: Severe bacterial infections
Severe bacterial infections
Number of patients with severe bacterial infections
At least 1 27/108 (24.5%)
1 15/108 (13.9%)
2 7/108 (6.5%)
3 5/108 (4.6%)
Total number of severe bacterial infections 45
Abscess/cellulitis 24 (53%)
Pneumonia 7 (15%)
Tonsil phlegmon's 4 (9%)
Pyelonephritis 4 (9%)
Peritonitis 2
Adenitis 2
Osteitis 1
Arthritis 1
Septic shock 2
Intensive care unit admission 3
IC 3.7 % 1 y 21 % 5 & 10 y 39 % 20 y
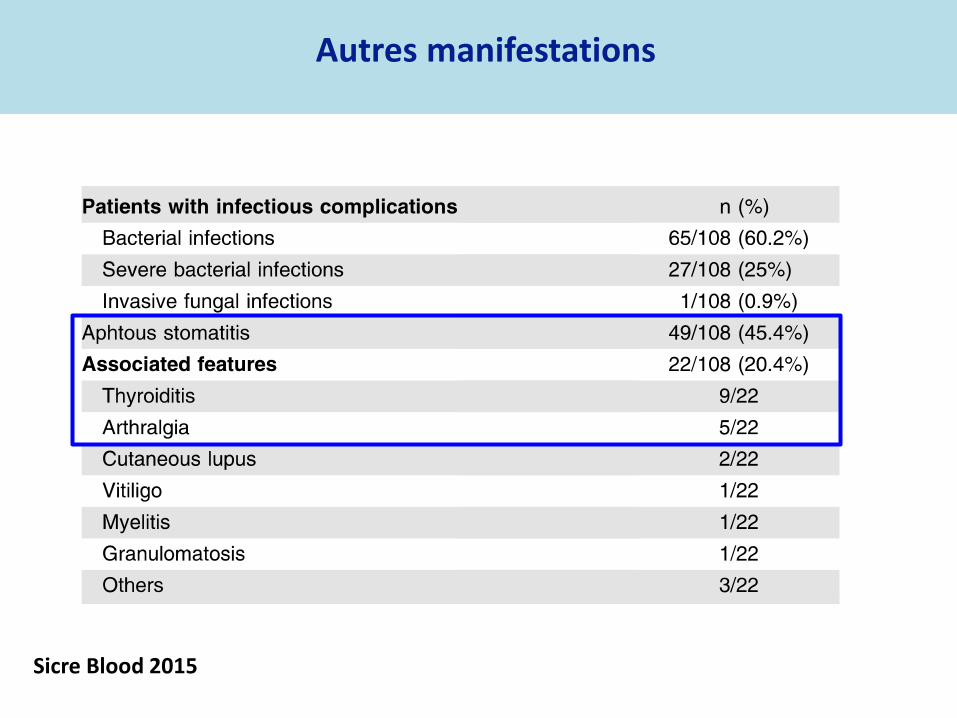
Autres manifestations
Sicre Blood 2015

Traitements
Sicre Blood 2015
Réponse 40%
Médiane 3 mois

Autres traitements
Evaluation difficile car hétérogénéité des indications - Echec (réfractaire = 4%) - Intolérance (céphalées, douleurs osseuses : fréquent -> baisser la dose) - Epargne du GCSF (peur de l’hémopathie secondaire)
Petites séries le plus souvent de réponses favorables… - Endoxan - Methotrexate - Ciclosporine - Campath - Rituximab - Corticoïdes : réponse fréquente mais cortico-dependnace forte dose - Splénectomie : échecs
Formes réfractaire au GCSF (> 15 jours, 5 à 10 μg/kg/j)
- 4 patientes consécutives - neutropénies très sévères, compliquées infections sévères - idiopathiques 3 / AI 1 - 3 sur 4 réponse rapide (7 à 15 jours), complète au Néoral
50% de réponse
Risque leucémique
Sicre Blood 2015
Cohorte française : Aucune évolution vers LAM / SMD
5 cas rapportés dans la littérature - 1 seul avait reçu du GCSF - 2 : histoire familiale d’hémopathie myéloïde (monoMAC,
SBDS, SMD familial ?)

Sicre Blood 2015
Persistent ANC <0.5 109/L or 0.5-1 109/L with symptoms
Normal hemoglobin level and platelet count
No spleen, liver or lymph nodes enlargement
Exclude drug induced neutropenia
• Familial history
• Clinical evaluation
Clinical & biological evaluation
- Myeloid and lymphoid malignancies
- Secondary immune neutropenia
- Large Granular Leukemia
- Primary immune deficiency
- HIV and HCV infections
Chronic Primary Neutropenia
Evaluate neutrophil antibodies
- Early onset
- Cyclic neutropenia
- Familial history of neutropenia
or myeloid malignancies
- Lymphoedema, warts,
pulmonary disease,
immunodeficiency or
monocytopenia
Suspect
&
Evaluate
Genetic disease
Chronic
Secondary
Neutropenia
Yes
No
Yes
No

Explorations complémentaires
Neutropénie chronique acquises sévère ou symptomatique :
o BOM si myélogramme de richesse diminuée
o Recherche d’anticorps anti-granuleux
o Bilan de thyroïdite auto immune
o Clone T (recherche)
o Adultes jeunes, pas de NFS antérieur normale, monocytopenie
ou lymphopénie : GATA2/SBDS


Risque leucémique
• Femme d’âge moyen • Marqueurs cliniques / biologiques d’auto-immunité >50% • Pas de « sous entité » clinique/pronostique identifiable Aspect médullaire Anticorps anti granuleux Auto immunité biologique Clone T
• Le plus souvent peu asymptomatique • Infections « neutropénique » peu fréquentes • Pas de symptômes = pas de traitement • 1ère ligne traitement = GCSF dose minimale efficace • Pas d’évolution vers SMD/LAM

Neutropénies Immunologiques de l’adulte
Registre Français
SCN J Donadieu
T Lamy B Beaupain L Croisille

















