Page 1
no-f173 ?68 PROJECTED NAMPONER REQUIREMENTS: IOENTIFYINO STAFFINO 1/2
no-a'? REQUIREMENTS FOR OP.. (U)
AIR FORCE INST OF TECH
IRIOHT-PRTTERSON SF3 OH R HILLIAMS SEP 86
, NcLlLRSSIFIED FIT/C/N - 9 6-19F/ 65 NL
Page 2
IIIIIIII1
11111"----5I;,I'__ 1111J.6
I-P
p%
'4...
4.. •. •. =
I liii IIII"lNAIIONALRURILAU 0 "SADRS16-
I
HHi 1.1- iIIII-.8
1 1 1 1 . 5 1 1 1 . - .
.'q .)
4... *. . .
.. ,:.;.
-. 4
Page 3
A.- SECURITY CLASSIFICATION OF THIS PAGE (Wh'Ien Data Filtered),
PAGE READ INSTRUCTIONSREPORT DOCUMENTATION PAE EFORE COMPLETING FORM
I.~~2 GOVTR ACCERESSION NO. 3. RECIPIENT'S CATALOG NUMBER
k A AFIT/C1/NR 86-f
4. TITLE (and Su.btitleo) S. TYPE OF REPORT & PERIOD COVERED
Projected Manpower Requirements: Identif ynqTHESIS/W V~1pJNStaffing Requirements for Operating the Neu
% Composite Medical Facility at the USAF Medi qOERFORMING OR G. REPORT NUMBER
Center, Wright-Patterson AFB Ohio%1 "7. AUTHOR(.) B. CON TRACT OR GRANT NUMBER(s) .. a
Raymond Williams, III
9. PERFORMING ORGANIZATION NAME AND ADDRESS 10. PROGRAM ELEMENT PROJECT, TASKAREA & WORK UNIT'NUMBERS
1%AFIT STUDENT AT: Xavier University
V) It. CONTROLLING OFFICE NAME AND ADDRESS 12. REPORT DATE
N 198613. NUMBER OF PAGES
109v:14. MONITORI, AGENCY NAME a ADORESS(iI differentI froms Controling,~ Office) IS. SECURITY CLASS. (of (hi. ,rOe
I UNCLASS
- I. DEC LASSIFICATION /DOWNGADNSCHEDULE
I6. DISTRIBUTION STATEMENT (of thirs R~eport)
APPROVED FOR PUBLIC RELEASE; DISTRIBUTION UNI.IMITED
17. DISTRIB3UTION STATEMENT (of (lie abstract entered in Blockr 20, It different from, Report)
l8. SUPPLEMENTARY NOTES
APPRVEDFOR PUBLIC RELEASE: IAW AFR 190-1 7W0LVD fr Research and
Professional DevelopmentAFIT/NR
9. KEY WORDS (Con~tinue or. reverse si de it neceo. ery an.d Idlentify by block. nu~mber)
ATTACHED .
L&J
.3 DD 1 1473 EDITION1 OF I NOV 15 IS OBSOLETE
SECURITY CLASSIFICATION OF THIS PAGE (11hen Datle Ewseredl
% %I
Page 4
DISCLAIMER NOTICEN:.
THIS DOCUMENT I&BEST QUALITYPRACTICABLE. THE COPY FURNISHEDTO DTIC CONTAINED A SIGNIFICANTNUMBER OF PAGES WHICH DO NOTREPRODUCE LEGIBLY.
.6, . °5.= . .
; ,K•.i..::.§.:.K-:. :-> .*.*,
Page 5
I
XAVIER UNIVERSITY
I .*
PROJECTED MANPOWER REQUIREMENTS:
IDENTIFYING STAFFING REQUIREMENTS
FOR OPERATING THE NEW COMPOSITE MEDICAL FACILITY
AT THE USAF MEDICAL CENTER, WRIGHT-PATTERSON
WRIGHT-PATTERSON AIR FORCE BASE, OHIO /
A Thesis Submitted to
The Faculty of the Graduate Program-ii
In Hospital and Health Administration . 0
In Partial Fulfillment of the Requirements for a
Master's Degree in Hospital and Health Administration
By -.
Raymond Williams, III
Captain, USAF, MSC
United States Air Force Medical Center, Wright-Patterson
Wright-Patterso r AFB, Ohio
September 1936
86 11 4 097 -
-. . %. .'- *%* .. .~*%~~ - * \~~,- - -.-%. %. . ..-
Page 6
I TABLE OF CONTENTSLIST OF TABLES........................ . .. ... . .. .. . . ...
z.CHAPTER W
I INTRODUCTION.................... . . .... . .. .. ... 1
I I REVIEW OF RELATED WORK......................4
I II THE USAF MEDICAL CENTER, WRIG4T-PATTERSON-PAST AND PRESENT.......................16
External Environment and Mission Assessment ... 16Internal Organization and Management
Climate Assessment...................24
IV OPERATIONS RESEARCH.......................28
V THE USAF ME DI CAL C ENTER , W RIGHT- PATTERSON- 19 88. 33
Data Summary.............................33Description and Discussin..................36
V I ANALYSIS OF FINDINGS -- INTERPRETATION.........41%
Linear Forecasting..........................41Financial Impact.......................44
VII CONCLUSION AND RECOMMENDATION................46
APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . 4
* SELECTED BIBLIOGRAPHY...........................105
* ABSTRACT...................................108
S,
Distributitll/
Dist Cp~~.i
Page 7
LIST OF TABLES
T ABLE
-1 SUMMARY TOTALS OF MANPOWER MEASUREMENTS..........34
2 DEPARTMENTS and DIRECTORATES SURVEYED............35
3 LINEAR PROGRAM FORECASTING ............. 4
~4 FINANCIAL IMPACT OF MANPOWER CHANGES.............45
K,,
Page 8
, ,%
CHAPTER I %
INTRODUCTION
Today, health care finds itself in a highly competitive
environment. This is principally a result of the federal
government's implementation of the prospective payment system for
Medicare hospitalization reimbursement. Other payors, be they
commercial insurers or employers with large self-insured health
benefit programs, have placed external pressures on the health
care industry to reduce costs. These pressures have caused
hospitals to concentrate on efficiencies and productivity efforts
within their traditional concept of operations to combat
declining occupancy rates and shrinking lengths of stay. The
initial successes of for-profit hospitals and the entry into the
market place of a variety of alternative health care delivery
systems have produced even greater incentives for hospitals to
deliver health care services at a more reasonable price--one
which purchasers of health care are willing to pay. -.
Concurrent with the competitive pricing environment is
the equally challenging demand to deliver quality health care
*"" measured by advanced medical technology and competent medical.
. staff. Not only does the public expect quality health care at a
fair price; they also expect health care services to be delivered
in a friendly, compassionate manner with amenities conveying
cmfort and quality.
Expectations for the military health care delivery systems
... .. .-S.'. ,
'S . a%.%."..".", . .- -"-" ""- '- -Z -- t_ - ' ' "-a- -.- - -. . . . . .
Page 9
wrur- .7 VK.i
are equally high. As each service manages its own health care
system, military medicine is under close scrutiny to provide
health care in an equally cost conscious manner and is often.-.
measured for quality using esthetic appearance, technological
capabilities, and the qualifications of medical staff as -"
indicators. Changes in medical technology, military missions and
medical practices have exerted enormous pressures on existing
military medical facilities to support sustained high levels of
care at reasonable costs. The greatest long term issue facing
the military medical services, aside from its wartime readiness
posture, has been a need to deliver quality care.
In response to these pressures, the United States Air
Force (USAF) Medical Service commenced a multimillion dollar
renovation and alteration of its medical center at
Wright-Patterson Air Force Base (AFB) located near Dayton, Ohio
in 1982. This medical Military Construction Program (MCP) was
designed to double the size of the institution and to provide a
facility capable of delivering the leading edge in military
medicine .
Due to past budgetary constraints, manpower planning for
the Wright-Patterson facility has been hindered in developing
staffing forecasts for operating the new composite medical ". -. -.
facility once construction is completed in 1983. Thus, the
purpose of this study is to answer the question of what staffing
requirements are needed to deliver outpatient and inpatient
2* -.. " .. °
% %
-*-.... -n7.
Page 10
health care in the new facility. In doing so, this management
study will focus on reviewing current literature dealing with
I:
manpower planning and forecasting, on discussing the external and
internal environment that this USAF medical center faces today,
on discussing alternative solutions to the staffing problems I... !
confronting the medical Penter as well as the methodology used to
determine a staffing projection, and finally, a presentation of
the recommended manpower requirements for the completed health
care institution.
..-1-[
.-. .
_ .I.m.
. I- %b.,u a
-I4"<
,.- -.3,
r - - ~ .... '.** /--.. ,
Page 11
CHAPTER II ,
REVIEW OF RELATED WORKI
Whether examining the manpower requirements for an entire
multi-institutional system or a single hospital, hcalth care
executives have continuously sought ways to provide the optimum
human resources for delivering patient care. Regardless of the
economic environment that health care finds itself in, the
challenge for management remains to achieve the optimum staffing
levels necessary for effective daily operations (Pakchar, 1983).
Today, increases in competition among civilian hospitals
have caused many institutions to assess manpower requirements
seeking ways to reduce costs, yet deliver quality health care,
build morale, and improve productivity. Assessing the
organization to determine the adequacy of staffing authorizations
is a key element in the review process. This assessment must
consider both skill and knowledge levels of required staff and
associated labor costs (Arni, 1983).'-.
The Joint Commission on the Accreditation of Hospitals
(JCAH) places great emphasis on the staffing issue, too. Today,
the JCAH accreditation process examines staff to assure it is,
"commensurate with the anticipated needs of patients and the
scope and complexities of services offered." As a furdamental . .-
standard, appropriate staffing is a key requirement in the
accreditation decision process for the JCAH (1936, p. 1,2). " -
Since health care is experiencing dynamio changes in the
'4 o T:• Li#
"I",%
~~~~~~~~~~ -...................................
Page 12
competitive marketplace, there is a strong impetus for justifying
enhanced, definitive approaches to medical manpower planning. To
bring about changes in manpower requirements, executive
management must use planning approaches that meet the challenge
for innovation, yet utilize sound business practices. According
to Lyons (1979), management should concentrate on:
o Examining current manpower authorizations to identify
a staffing mix in terms of work experience and qualifications.
o Examining strategic plans which need human resources
to successfully attain goals and objectives.
o Identifying human resource requirements to meet
business strategies.
o Developing a manpower plan to meet those business
intentions.
Pakchar (1933) adds that a practical manpower plan should span
the entire period of projected growth, often five to ten years.
To provide a more definitive structure in manpower
planning, health care institutions are viewing human resource
management via the systems approach to management. Since a
system is a linking of interrelated and interdependent components
having a facilitating effect on the carrying out of a process, .-.
the system in health care is the medical institution and the 4
subsystem of the institution is human resource management.
Torrez (1983) illustrated the systems approach to
staffing using a 500-bed acute care teaching hospital as a model
5
%o Ut. 4. .
Page 13
-° . ° .- "
(Appendix A.) Under this conceptual approach, the institution
can be also viewed as a sccio-technical system with a flow and
process consisting of services, facilities, technology, manpower,
and resources. Bearing in mind that a process is an identifiable
NO flow of events moving toward some goal, manpower planning becomes
the process and staff, then, becomes an input into the process of
delivering health care. Under closer examination, Torrez (1983)
* maintains that the patient acuity system is another process
utilizing the quality and quantity of staff to mneet patient care
needs. Thus, manpower planning requires an ever constant vigil
and should be managed as a dynamic process.
Regardless of approach, more and more managers arer
looking for ways to optimize the use of their most important
resource -- people. Since the operating costs of hospitals are
dominated by salaries, wages and benefits; managers are looking
to comprehensive human resource management as a system for
solving the impact staffing has on the cost of care. Solutions
a_ to these challenges have used projections based on historical
data, on comparative statistical data, on models and simulations,
or or professional advice (Mackley, 1984). Pakchar (1983) points .
W -to significant problems associated with using unaltered
historical data exclusively to, predict future manpower needs in
the changing environment health care institutions operate in
today. However, historical data can be quite useful when ccupled
w h s. u... i'" ~with staff involvement in determining future staffing levels. "..'
i%
..
* . . .,
Page 14
But, these activities should be based on professional judgment
and provide management with sound justification for manpower
authorization adjustments (Fawcett, 1935).
The mc t frequently used method for predicting future
manpower requirements is based on this collective opinion of
in-house professionals and practitioners. While it is basically
a means for management to synthesize all information available
into a qualitative, yet nonquantitative form; it should not be
discounted due to its subjectivity. The implicit views and
judgments by individuals with experience and insight into the
realities of daily operations are invaluable in attaining -e
productive and efficient responses to health care demands
(Dr andell, 1915).
One technique offered to incorporate this collective
opinion into the planning process is manpower value planning
(MVP). As a management process to enhance effectiveness and as
an approach to justifying manpower, MVP utilizes nominal group
decision making to determine the optimum investment in human
resources for each of the functions (Fifield, 1974). 'n...
In the face of prospective pricing and other economic,
pressures, hospital departments are turning to tools, such as
MVP, to manage staff allocation and the costs associated with
staff. The key strategy is to minimize salary, wage and benefit
crsts while maximizing the productivity of the enormous number of
health care personnel required to deliver health care services. "
m o - -,-*
* . - -- ... . . . .. . . . . . .
Page 15
An outgrowth of collective opinion methodologies has been
the implementation of flexible staffing policies for health care
institutions. Since departments are differentiated by the impact
which patient census or visits have on specific department-e
workloads, not all departments are suited for flexible staffing
either. However, flexible staffing has proven to be extremely
h i w c sv ls e geffective in reducing the cost impact of the one area in
hospitals which accounts for over half the salaries, wages and .'
benefits paid--Nursing Services. Nursing Services has turned to
flexible staffing techniques which can be combined to meet
individual hospital staffing needs. In general terms, a core
staff of full-time and part-time nurses identified to meet
anticipated work is augmented by a flexible staff when workload
exceeds expectations. The flexible staff approach allows such
techniques as float pools and squads and incidental staff to
minimize the impact Nursing Services has on the hospital budget
(Herzog, 1935). Bracken (1985) comments that commitment by
executive management and by the hospital staff is essential for
successful incorporation of adaptive, or flexible, staffing.
Historically, consultants have been hired to provide the
technical service for developing a manpower plan using new '
methods, such as flexible staffing. As shown above, that role is
shifting to the hospital's staff. Consultants are now being used
to manage the process, development and design of manpower
,. *%*,
programs using the expertise of practitioners (Bracken, 1985).
4. F . ,
A :*.* - -
Page 16
Other functional areas within the health care institution
also use flexible staffing. Staffs are increased or decreased
whenever significant changes in workload are projected.
Projection of that workload can then become the basis for tying
* workload and staffing requirements together, as in the case of
* the clinical laboratory. One 360-bed hospital plans to use its
* historical data on the number of tests performed per patient
census to set laboratory staffing levels. They stress that
historical data is valuable only if it is used prospectively
As might be expected, most industries are using automated
-tsystems to expedite the processing of vast amounts of data and to
compute manpower requirements using a variety of staffing
methodologies. With the rapid growth in management information
* systems in all industries, including health care, executives are
* looking to decision support systems (DSS) to assist them in
* containing rising personnel costs. Nutt (198'4), in his study of
*staffing models in hospitals, suggests that decision models must
be developed by individual institutions. His rationale was based
*on the diversity of decision making criteria used by health care
executives and or the variety of, and in the incompatibility of,
- medical information management system designs in individual
* health care institutions. Also, he concluded that "the lack of
* overall norms poses a potentially serious problem for
cost-containment efforts in health care delivery organizations"
9
Page 17
'd.T- 7F''
(Nutt, 1984, p. 1013).
While much is written about changes to staffing
methodologies for hospitals seeking improved efficiencies in the
highly competitive environment, little is said about how manpower .
standards are developed for new institutions. Shaw (1983) ;
attempted to provide some insight into approaching this challenge
by briefly describing a plan to staff a new psychiatric facility
in Michigan. Through the apparent use of local labor management
standards, Havenwyck Hospital management established manpower
requirements developed internally for each department based on
fixed and variable hours projected to change with patient census.
Starting with higher full-time equivalents (FTEs) and working
towards a goal of designated lower FTEs, a staffing plan was
prepared for the first 245 days of operation linking the FTEs to -'
average daily census. The manpower plan then became the basis
for staff recruitment activities to meet the expected demand when
the new hospital opened.
Parkland Memorial Hospital in Dallas, Texas faced a
similar challenge as a result of an $80 million building program.
They approached the problem of determining staffing requirements
for their new facility by creating a master staffing model. The
model was created through the use of commercially developed
productivity standards applied to data collected from hospital
staff interviews. This resulted in the identification of local
staffing standards driven by workload factors to determine FTEs
.d-..
10
. -.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~~* °°... ............... . . . . . . . . . . . . . . . . . - . . . , . . .
• ° oo .o , " ° .° "o° '° ." 2 . ° . .* ° . .'°..".**.-. °..°.*p . .°° ° " " " , *.'°.. ° o . . : ' '-' "
:." -' ''• ." -°- . . .
Page 18
(E~wing-Juu.l, 1985).
Since Nursing Services comprise a majority of a
hospital's staff, there have been numerous studies conducted in
England to develop effective staffing methodologies. The British
interest in medical manpower planning seems to be caused by the O
* cost-containment efforts of their government in dealing with the
budgetary constraints imposed by their National Health Service.
* Many of these methodologies use some form of workload method
combined with a patient acuity system. Their aim is to identify
historical data on the kinds of patients treated and the nursing
hours neede-~ to treat specific sevenities of illness or injury..4i
There seems to be a polarization of opinions as to whether the
Aberdeen Nurse Staffing Formula, a patient dependency-based
method, or the Telford System, a consultative approach, is best
for manpower planning (Mackley , 1984) Because problems have
been attributed to these approaches, Fawcett (1985) proposes a
three-tier approach which uses professional judgment, a quality
monitoring instrument to substantiate this judgment and to
* maintain standards and a simple dependency rating to provide
*current information or workload changes. e
Although the American federal government has yet to
invo~lve itself in providing national health insurance, there are
many aspects of medical manpower planning it is involved with.
*Th 3ur eau of Health Manpower, Department of Health and Human
a' Services, contracted with the University of Florida to develop
Page 19
-7%
design and operational guidelines for manpower in health
maintenance organizations (HMOs) or prepaid group practices
(PGPs). Specifically, this initiative sought to provide a system
for forecasting manpower requirements for ambulatory care
services in adult medicine, pediatrics and obstetrics/gynecology.
Four models were developed to facilitate planning for these
delivery systems, which were, at the time, receiving considerable
attention as the government sought ways to encourage cost
containment on a national level (Develo.ment of Design and
O_* eational Guidelines for Optimum Man.power in HMO/PGP Settings:
Volume I A.plica of Staffin. Models, 1977).
On the other end of the spectrum, the Veterans' '.,
Administration (VA) has been developing staffing methodologies
for their own hospitals for a quarter of century. Illustrating
the complexities and changes in managing human resources for
health care systems, the VA recently announced new guidelines for
what they consider to be appropriate staffing. These guidelines
are to be used by executive management in making decisions about
manpower authorizations and workload changes. Additionally, the
guidelines are intended to develop data bases which will support
budgetary requests to Congress. Issues still to be addressed by ...
the VA include development of guidelines for physicians and
nurses. The VA has contracted with the ,ational Academy of
Sciences to develop physician staffing guidelines. This approach
was taken to prevent the "backlash" of criticism expected with
12
V.
. . . . . . . . .* o * .. . . . . . . . . . . . . . . . . . . .. . . . . . .
Page 20
JVg
attempting to quantify standards for physicians. The nursingprofession presents equally difficult challenges for the VA when
developing measured task-oriented standards. To complicate this
process, the VA is being pressured by Congress to link staffing
with diagnosis-related groups or to centrally manage medical
manpower (US Medicine, 193 4)-
The Department of Defense (DOD) uses a variety of
quantitative approaches to determine manpower requirements.
Drandell (1975) used a quantitative technique to determine
manpower requirements for a federal agency outside health care.
In examining the staff authorizations necessary for contract
administration at the Defense Contract Administration Services
Region in Los Angeles, California, exponential smoothing and
regression analysis were used in dealing with fiscal year time
periods and manpower projections. lie noted, that due to the
differences between actual and predictive behavior, quantitative
analysis could not stand alone as a method for determining
manpower requirements. Drandell concluded that "elements of a
subjective nature which could not be determined from an analysis
of past history must be included in any final forecasting
procedure" ( 1913, p. 515).
Presently, the USAF Medical Service incorporates manpower
engineering standards based on historical workload to staff its
i medical facilities. These stindards provide statistical formula
for identifying the manpower authorizations appropriate to a
- . . -
- .-4
13"-"-
- " ,*.*o.•. A . ° c. . .•• . . -.. . . . .. • . . . . . . . . . . . . . U. .. . . . . . . . . .* * ~ .;,-
Page 21
- ., .- ., .,- - / , 1
given functional work area. These manpower standards are then
adjusted based on annual historical workload for that given
functional area. Thus, the system adjusts manpower
authorizations based on increases or decreases in workload (Air
Force Regulation 26-1, 1933). However, there are no adjustments
for changes brought about by new physical capabilities.
Since this manpower management technique is retrospective
in nature, Air Force standards will not necessarily focus on
future operating requirements. To prospectively plan military
health care provider manpower requirements, the Medical Service
will commence using a model called the Provider Requirements ,
Integrated Specialty Model (PRISM). Health care providers are
defined under this modeling program as physicians, physician
assistants, podiatrists, optometrists, nurse practitioners, nurse
midwives, nurse anesthetists, psychologists, social workers,
physical therapists, and occupational therapists. Support people
such as registered nurses or technicians are not currently
incorporated into the model.
The PRISM model has three components. Two of these
components, PRISM I and III, will be the basis for future
manpower projectionrs included in The Pr,_sident's annual budget
submission tc Congress. The final component, PRISM II, is a
decision support system used to plan medical care provider
requirements for each of the USAF medical treatment facilities
throughout the world.
1 4
.4, d
-... .-
Page 22
* A 3.3.3 S - - .. -. 5 ~.~~.5... . ~ ~ ~
Although the most recent application of the PRISM model .*
was to interface medical manpower requirements with Air Force
medical facility design or modification projects, this advanced
manpower planning tool was implemented well after the new4
composite medical facility was begun at Wright-Patterson Air
* Force Base, Ohio (Tufte, 198~4).
-J44
.5
54
5.
'S
S.., I.
'S
~55
'5 5%* %
55 %% ~.
4.
- 154. '1
S. -S..--
5? -o
'5~~~
. S S S ~ SS,..--5-.*-*
- - . . - . .5..-. -S... S*~~*~S5*5 -5----
~ -. -. -. ~ p ~ -.
Page 23
-77- - - -
CHAPTER III
THE USAF MEDICAL CENTER, WRIGHT-PATTERSON - PAST AID PRESENT
The United States Air Force Medical Center, N
Wright-Patterson located at Wright-Patterson Air Force Base is a
352-bed health care institution on the outskirts of Dayton, Ohio.
Providing comprehensive inpatient and outpatient care for
thousands of military personnel, it will become the second
largest hospital in the Air Force when a $113.4 million
renovation and expansion project is completed in 1988. The work
will more than double the size of the medical center, from
297,000 square feet to a 657,000 square foot composite medical
facility (Hale, 1985).
External Environment and Mission Assessment
T o provide a valid assessment of the Wright-Patter son €-.A - -"W .-
Medical Center, this study will focus on the mission, goals, and
objectives of the USAF Medical Center, Wright-Patterson. Also -..
addressed will be the background and scope of the MCP; the 1%
catchment area for the Medical Center; the population served and
the range of services provided by this military medical
institution; the array of agencies and institutions with which,
the Medical Center interacts, and any significant changes over
time regarding these factors.
Goal1 s a n d Ob ectives. '
The goals and the mission of the USAF Medical Center,
Wright-Patterson, are primarily established by higher
16 ,a .'.<
, .-
% % . . A . 9 .. ' ___ ____ ___ ____ ____ ___ ____ ___ ____ ___ ____ ____ ___ ____ _"_-.__ ___
Page 24
7. 7, -777..
headquarters. The mission statement prescribes that the
right-Patterson Medical Center provide the medical support
necessary to ensure maximum wartime readiness, combat casualty
care capability, and to the greatest extent possible, a peacetime
health care system for all eligible beneficiaries. This mission .
includes medical and dental care, environmental health services,
occupational medicine, and bioenvironmental engineering services
for all personnel assigned, attached or supported by the Medical
Center. This Medical Center operates as a military consultant .-
center, as a direct referral hospital and as an area medical
center for specific Air Force and DOD regions. This institution
also provides training programs for medical, dental, chief nurse,
and administrative residencies; for clinical psychology,
cardiopulmonary and radiology specialties; and for nurse
internships, a physician assistant orthopedic specialty, and
medical laboratory training. Other services include hyperbaric
medicine, alcohol and drug treatment, and radioisotope services
(Air Force Logistics Command R eulation 26-2, 1985).
As for the goals of the Medical Center, they are
primarily directed by the USAF Surgeon General and the Air Fo-rce
L.ogistics Command Surgeon (AFLC), both comparable positions to
corporate executive management acting as the Medical Center's
goverring body. These established goals are:
o To continue initiatives to prepare to equip Air Force
Medical Service personnel and resources for immediate employment
17
,< ..... ,,..- . - . .v ... ,,-..',. -... ..-. , . .. -. .. ... ,--,. ,..-. . .- • . -:. -.;... . . . . . ..'-.--.. .-.-. .-. ...-.. '. .-.. . . .". .-.. .-.. . . .--
Page 25
. . . ,. - 4~ -- ~ *J ~ ** ** b °- - - --. ",:-.-i
worldwide to support Air Force operational requirements, during
both peacetime and wartime.
o To implement new programs and enhance others to ensure .
provision of the best medical care possible. ,;. Y.
o To develop more effective and efficient ways of. ... P .1'p. .
conducting a comprehensive medical program in the face of
day-to-day fiscal constraints.
0 To improve patient perceptions as to the
accessibility, availability and quality of medical care provided
by Air Force medical organizations.
o To develop higher standards of personal conduct and
integrity for Air Force Medical Service personnel in the areas of
responsibility, leadership, accountability, and officership.
The executive management of the Wright-Patterson Medical
Center incorporates these goals in the local strategic plan and
recognizes that the MCP is an important resource allocation aimed
at facilitating the attainment of these goals.
The present medical facility was built to provide total
medical and dertal care for active duty and retired military
personnel and their dependents within a specified Air Force
regionr. Today, the Wright-Patterson facility provides care for
approximately 12 ,500 Air Force, Army and Navy personnel and
45,?D0 dependents rf active duty or retired personnel in the
immediate Dayton area. The Medical Center also accepts cases
referred from Air Fcrce bases in the northeastern and '
d
- - 4,
_.... , #- . _.._.... .. ..-.....- - - -
........ .
Page 26
north-central United States. Finally, this tertiary care medical
treatment facility serves a DOD regional population of almost
400,000 eligible beneficiaries (The Big Picture Management ---
Summary, 1985).
Tc provide enhanced care for this large geographical
region (Appendix B), a construction project for this Medical
Center was started in 1982. It was designed to provide necessary
alterations, renovations anJ additions to the main facility,
built in the early 1950s, and tr, consolidate numerous other
medical departments geographically separated from the main
facility. This $113 million-plus project was designed in the
1970S to reflect the advances in medical, surgical and dental
inpatient and outpatient practices; to affect the changes in
applicable technology; and to meet the growth in eligible
military patient pcpulation.
Prior to construction starting, the main facility
ercompassed 297,345 square feet of area, 350 nursing beds, a
28-chair dental clinic and outpatient and ancillary services.
The old facility was extremely overcrowded and additional mission
requirements forced the conversion of cer tain spaces to other "
than their originally intended use. A total mix of outpatient
and inpatient care could be frurd or every flor. Office or
examination space for varirus specialties had taken over patient
rooms The location of key ancillary departments, such as
" cardiac catheterization and radiation therapy, forced the
. •. .d
* **% . ... . ....... ....-............... ......... *- . . . ,,.,:. -,:,-i . .i: i,.......... . "
Page 27
._T7., % .-. . .,. % % % j . ; ,<r.-. - .,-. .7.-- :...- - - .- ,.7. 1 " -. -. -:" --" ." . "- .' " " -" " " "
movement of inpatients to all parts of the facility including the
nonpatient areas of the basement. To facilitat, the use of space
within the Medical Center, several departments and clinics were
relocated to remote locations. These moves further compourded
the effective management of all Medical Center activities
(Sherlock, Smith and Adams, Inc., 1931).
The chief aim of the new construction is to bring all the
base medical facilities under ore roof (Appendix C). Trends
toward outpatient care, advanced treatment and ancillary
services, and developments toward major medical training programs
at the hospital created a need for more space and improved
facilities. The new facility and accompanying modernizations in
medical equipment technology will result in improved or new
medical capabilities. Laser surgery for cataracts, cardiac
catheterization, expanded special care units, and radiotherapy
are a few services which will benefit from the new construction.
A new computed axial tomography (CT) scanner, a linear
accelerator and new special procedure and angiography rooms will
accompany this growth.
The new composite medical facility is significantly " -
larger than the present structure, has a different design and is
intended to accommodate up to almost 10,000 annual admissions and
outpatient visits exceeding 400,000. The difference in design
will affect the staffing requirements for the facility. For
example, whereas the old hospital has orly 5 operating rooms, the
20 : -
IIII
/
.aE .t •
* 4 I
Page 28
S%
4 .. • p
new building has 12 operating rooms, including 2 large rooms for
orthopedic surgery and 1 large room specialized for neurosurgery.
Also, included are 3 ambulatory operating rooms. . ?..
The expanded facilities at the Medical Center will
consist of 2 major three-story additions flanking the south wing -.*
of the existing hospital. Circular 136-foot diameter turrets in
each addition will house the wheel-shaped intensive care and
cardiac care units and mechanical operations room. The newhyperbaric pressure chamber, which accommodates 18 persons, is
the only one of its kind for patient treatment in the DOD. The
bottom floor of the southeast addition provides facilities for
mental health, the flight surgeon's office, hyperbaric chamber,
and occupational and physical therapy. A 43-chair dental clinic,
professional training facilities including a 245-seat auditorium,
and a complete renovation of the interior of the existing
structure to ensure compliance with appropriate building codes
and accreditation standards are also included in the
construction. Other improvements will include the implementation
of central processing and distribution, advanced management
information systems and state-of-the-art communication systems.
As for the southwest addition, it includes an emergency
treatment area, records office, outpatient pharmacy and a
crng meration of clinics. A new 185-space parking lot has
already been constructed near the clinic entrance. The thorough
rerovation of the interior and exterior of the Medical Center
21
- --- -. -- *-w..
Page 29
will present a new image of military medicine for the local
community. The new composite medical facility will represent the
latest in medical facility improvements at Wright-Patterson Air
Force Base since the first hospital building at Wright Field was
completed in October 1917 (Hale, 1985). Indeed, this tertiary
care facility will stand well with the major renovations of
Dayton community hospitals.
The Wright-Patterson Medical Center interacts with a widearray of agencies and institutions in both the delivery of health"
care and in functioning as an organization within the Air Force
community. Appendix D provides a list of these organizations on
Wright-Patterson Air Force Base.
As for the MCP itself, the AFLC Command Surgeon's Office,
the USAF Surgeon General's Office, and the DOD played key roles
in the strategic process related to enhancing the
Wright-Patterson facility.
The approval and appropriations process for all capital .-
expenditures within the DOD and for the Wright-Patterson project
were under close scrutiny from Congress, even in the earlier
.'ears of the 60s and 70s, and can best be characterized as a
period cf austerity. As with most programs competing for limited
dollars, the Wright-Patterson project advocates were forced to
make concessions to gain the ultimate approval and funding
necessary to build a new facility. Perhaps the greatest
concession was that concerning additional manpower requirements
22 . ._
'. . . .. . . . -. . -. -. , -. -*l . -. *, . - N , . * . * *'* - * . . . - .. , •>* . . , * . . ." . . . - .
Page 30
. r..e
for providing health care, as envisioned in this new composite
medical facility. As a result, no requests for manpower to '
support the expanded and renovated Medical Center were submitted.
Whether those concessions were correct or not is not an
issue as far as this study is concerned. Never-the-less, the
changes in health care technology and treatment have significant
impact on the delivery of care in the new composite medical
treatment facility. It is obvious to the Medical Center's
management and staff that additional personnel are needed at all
levels if the accessibility, availability and quality of care are
to be maintained while minimizing cost increases. These concerns
become the basis for studying the manpower requirements for the
future occupancy of this altered and renovated military medical
, %*institution. 4
On a national level, there has been great interest shown
recently in reducing the cost of 'are in the military health care
systems. During the budget review cycle in the fall of 1984,-%--
congressional concern for cost containment was high. While the . .
military system of operations is under continual review from
within, the Congress felt it was time for an independent revi ew
by a panel of civilians, focusing on the military medical
construction program (MCP). Consequently, the Assistant
Secretary of Defense (Health Affairs) established such a panel,
the Blue Ribbon Panel on Sizing DOD Medical Treatment Facilities.
The panel reviewed the criteria for sizing and staffing military
23..-
............................................ -- ...-. . -".......'.. ..-..... ..-- '''- "
.. . . . . . .. . . . . ... .... ,. , • - . . .-.-. ... . . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . ... ,'- . .... ,.,_..,.. ....... , -, ,.... ....- .-... -,.' .... '.. .-...-... .-. o.,_.-,"-, ,.. .- _._-,, ,_,.- -
Page 31
hospitals and recommended numerous actions for improving
V management policies and medical capabilities. ___
In a strong showing of support for the panel, the .
Assistant Secretary of Defense (Health Affairs) was directed to
implement the recommendations of the Blue Ribbon Panel without
delay . One of the recommendations was to finalize an analytical
methodology for sizing and staffing medical facilities under
peacetime and wartime conditions (Cerha, 1985). Initiatives of
this nature are indicative of the external pressures being
exerted to enhance productivity within the military system and to
place controls which foster cost effective medical treatment
facility construction programs.
Other external pressures impact the Wright-Patterson
facility, too. Colonel Bruce D. Wilhelm, USAF, MSC, current
Medical Center Administrator, articulated the changes he's seen
recently in a February 1986 interview. He pointed to increased
JCAH requirements, increased quality assurance and risk r. management requirements, changes in nursing management concepts,
" public concerns with the quality of military medicine, and the
* increasing numbers of patients seeking care as some of the
factors challenging Wright-Patterson, today.
The Internal Organization and Management Climate Assessment
This aspect of the assessment will describe and evaluate
the institution's organizational structure with emphasis n
understanding the operations, management style and climate of the
24
%' %
~--------------. *. -- .r.. .,
_,, ,_~j _-. ,-./_• , , _ _. _X.' / , ¢, '.- 'JW. '. -.'." _. - . ....AL:._ b "L ':. A X: :'' :' :-.
Page 32
.• . .
organization and significant developments and changes in these -'.,
factors over time as influenced by the MCP.
As might be expected for a military organization, the
Wright-Patterson Medical Center is organized under a functional
structure (Appendix E). Such a structure is mandated by
Headquarters USAF and facil itates standardization and control for
all Air Force organizations (Air Force Regulation 168-4, 1985).
This specific structure has proven successful over the years
providing the military medical organizations with an approach to
span of control and unity of command that is both efficient and
effective. The USAF Medical Service is charged with keeping the
force healthy and, in instances of disease or injury, returning
the military member to duty promptly. The importance chain of
command plays in execution dictates a structure responsive to '1
quick and effective vertical communication.
The basic division of the military health care system
into administration and professional services clearly delineates
control. Administration provides management and leadership for
the organization. The professional component is responsible for-. %.,_
providing health care services through hospital, dental, .--
aeromedical and other professional activities. Unity of command
is also clearly defined under this functional design. For the
most part, lines of authority are vertical. With the
commencement of construction at Wright-Patterson, the local
administration has added the Development Directorate to improve -
25
,,* ?I- -
,.-°,
. . 2 * . .. ; ;/ . ? . 2 : - -e". _.,., . .¢: .¢¢.,.m:,' r 4.4-,
Page 33
control, conflict management resolution, and communication in
matters dealing with the renovation and alteration of the
existing facility.
As for the management style at the Medical Center, it is
principally influenced by the primary mission of the
military--defense of the country. For this reason, management
4. style, even in the military medical institution, is subtly
attuned to task orientation. Nevertheless, senior health care
executives embrace innovative leadership and managerial
philosophies in practice in the private sector. The application
of such strategies and tactics are employed when the operational
aspect of military health care allows participatory management
and other people-oriented activities.
The major impact of operating a tertiary care facility,
simultaneous with the enormous complexities of the renovation and
* alteration of the facility, has placed great stress on
management, medical staff and patients alike. Construction has
been ongoing at Wright-Patterson for over four years, row.
During this period, numerous inconveniences caused by interim
moves of departments and the physical distractions caused by
construction have challenged everyone. A sensitivity to personal
concerns, and a desire for operating in a positive climate, have
been of major import to senior management. Success in truly
creating a positive working environment has been tempered by
increasing workload5 supported by financial and human resources
26
4el
Page 34
constrained by budgetary limitations. Due to concerns for such
limitations, executive management is committed to~ strategic
activities aimed at improving resource availability. One such
initiative is this management study.
I..4
p.27
Page 35
CHAPTER IV
OPERATIONS RESEARCH
The USAF Medical Center, Wright-Patterson, is
experiencing significant changes in its delivery of health care
due to this major construction project. As stated previously,
executive management seeks to determine what manning requirements
are necessary to operate this new structure effectively and
efficiently. This study examined historical and solicited data
to ascertain if changes to manpower authorizations are needed.
And if changes are needed, what those changes should be.
The methodology incorporated in this study involved the ,
use of nonreactive and reactive measures to arrive at a solution
to determining these future manpower needs.
Data Collection
A variety of historical records in the Medical Resource
Management Office at the Wright-Patterson facility provided ample
data for conducting this study. They are:
o A summary of historical manpower authorizations for
this institution since 1979 (Facts and Figures of Comparati ve
Manag.ement Data, 1 980-1 981; Manaement Summary, 1981; The Big.
Picture Management Summary, 1982-1984).
o Current authorized manpower for FY 86 and projected
accomplished by the Medical Center (Extended Unit Manpower.
Documen t , 1986).
28
.. ...... ............. .......
Page 36
o Projected manpower requirements using PRISM estimates
for FY 88 (HQ AFLC/S'3A, 1986).
o Pro jected manpower requirements developed by the USAF
Health Facilities Division in conjunction with the MCP design
study (Preliminary Stud : Composite Medical Facility/Dental
Clinic Addition-Alteration, 1934).
o A previous manpower projection based on the Military
Construction Program (MCP) developed by the Medical Resource
Management Office at Wright-Patterson (FY35-89 Medical Program
Objective Memorandum, 1982).
As for the reactive measure, a more current manpower
projection based on the MCP was required. Since Fawcett (1985)
and Fifield (1974) proposed the use of professional judgment,
coupled with historical Jata, in developing manpower forecasts, a
needs assessment was developed to collect department or
directorate specific manpower requirements (Appendix F). The
survey provided each function with its FY 86 manpower
authorizations. Based on this information and based on the
changes to the physical environment resulting from the MCP, the
departments and directorates were asked to forecast a reasonab'le
expectation of their manpower needs for FY 88. Any forecasted
increase or decrease had to be supported by a detailed, realistic
justification.
Evaluation and Presentation of Data.
Most cf the norreactive data was determined to be valid
2929 ""
i- .. *.. .- * _ & ~ *- -r- * g- ..-- ; . aJ
Page 37
and reliable. The data extracted from official USAF management
summaries and manpower documents, by its very nature, should
stand on its own merit. The basis for development of these
documents is through statistically valid and reliable management
engineering standards.
The projected manpower projections provided by the Health
Facilities Division were not used due to the generic nature of
descriptive data and the vagueness of specific position
descriptions. This was further complicated by the fact that the
basis for the decision criteria for this projection could not be
determined. S
As for the 1983 projection, this reactive measure was an
abbreviated study designed to determine manpower requirements for
the new composite medical facility. Due to changes in health
care practices and technology, due to the cursory nature of the
aforementioned study and due to manpower management's questioning
the validity and reliability of these forecasts; it has been 54
excluded from this study. - .
The needs assessment survey was the other reactive
measure used in the study. It was considered an appropriate
instrument using manpower forecasts generated from historical
workload which were modified by the professional judgment of the
Medical Center staff. However, these changes were only
considered valid if they were accepted by executive management.
All recommended changes for the medical departments were reviewed
IA.
30
W
% ,
Page 38
by the Chief of Hospital Services to assures a strategic fit in
the multidisciplinary structure of the professional services. . %VI"
Following that review, all changes were then resubmitted to the
ancillary and support services. This action was taken to .
preclude these functions from being subjected to new workloads by
the clinical departments which had not been addressed previously
in the survey. Once those reviews were concluded, the entire
proposal was submitted to the Medical Center Administrator and
Commander for their review and comments. They were presented
with the data from the reactive and non-reactive measures for .
comparative purposes (Appendix G).
Alternative Solutions.
The problem posed in the study was to determine what
manpower changes, if any, were required at the Wright-Patterson Ifacility to operate the new composite institution. The
alternative solutions to the problem are: .. t
o No change to current manpower authorizations (use
projected manpower for FY 88 based on current workload).
o Use PRISM authorizations.
C Use previous manpower projection based on the MCP..
o Use current manpower projection based on the MCP
(June 1986 survey data.)
o Use a combination of the above solutions. - - n
An aly si s.
Once the data from all measures was accumulated, a
31
-- .--
p °..'..
1 - _ -. . "
;". ., .. ..-
Page 39
comparative analysis was performed. Specifically, the
recommendations of the Medical Center's departments and
directorates were compared with the current and projected
manpower authorizations based on historical workload and the
projections suggested under PRISM applications.
The application of a quantitative technique was used to
compare historical manpower authorizations since 1979 with the
recommendations made by the departments and directorates. The
use of a linear program forecast provided a basis for determining
internal validity. It is a generally accepted fact that there is
a casual relationship between patient-driven workload and
staffing requirements. That is, as workload changes, so does
manpower requirements proportionally. As stated earlier in this
study, one reason for the construction project at
Wright-Patterson was to provide a facility which meets the
demands of an increasing patient population. -*.
Finally, any changes to the overall manpower requirements
were examined fcr the financial impact on the Medical Center's
budget for FY 83. These manpower changes were converted to
salary and benefit costs extracted from current USAF Medical ,
Expense and Performance Report data.
32
,'-;'
. ... .... ., -,'..;''..;''2;.'."".._''_''_..-.""."'.- "_ h ¢' ;'-:' ',. , - - - ".. .. . ... "-"-"" - "" .. ..... .. . ... ..... 4
Page 40
-..'-.
-7.-.- IF
CHAPTER V .-"-
future manpower requirements on historical workload and its
I
application to manpower engineering standards. The manpower
planning system based on these standards is, then, applied to all
medical treatment facilities Air Force wide. Thus, this study
used the FY 86 authorized manpower requirements for the
Wright-Patterson medical facility as a baseline for forecasting
future needs. Appendix G represents in indepth examination of
this baseline authorization with alternative solutions proposed
in the study. Each department and directorate is represented
with a specific listing of all personnel requirements broken into
the three categories of employees (officer, enlisted and civilian
personnel).
Data Summary
Since the military construction project was undertaken,
in part, to meet the growing demands of an increasing patient
population; the FY 86 manpower authorizations presented an
appropriate staffing level to compare with future needs. Table 1
is a summary of the total personnel requirements identified in
Appendix G. As shown by Table 1, FY 88 staffing requirements ,.
based on historical workload are projected to grow by 2 percent
(comparing FY 86 total authorizations of 1411 with FY 83 needs of .'S
1445.) These two manpower planning instruments represent the
33
• 0.) ' .
I
Page 41
.,,__ .-. ~i.Z ..-.. r- . ..- ,., ---. ' '."r -. 7' .. ."
" ... -.-
current method which the USAF uses in identifying manpower needs.
However, this projection does not take into consideration the
changes in treatment capability brought about by the MCP.
Another manpower system for developing manpower
requirements is PRISM. Although rot fully incorporated into the
manpower allocation process at present, PRISM does provide
manpcwer requirements fcrecasted for USAF health care providers
based on productivity standards and forecasted patient demands.
Table 1Summary Tctals of Manpower Measurementsfor Current and Forecasted RequirementsUSAF Medical Center, Wright-Patterson
Wright-Patterson AFB, Ohio
Unit Manpower Doc Adjusted Adjusted NeedsFY 36 FY 38 FY 83 FY 88 Assessme.._i_,Authorized: Authorized: PRISM I PRISM III Survey "
GRAND TOTAL: 1L411 1445 1456 1433 1652
over FY 35 .00 .02 .03 .05 .17
r. -'"'; 4-----------------------------------------------------------------------------------.
Again, the manpower requirements for providers projected for FY
83 using PRISM are higher that FY 86 levels. PRISM manpower ".-.
prcjections used were those identified as PRISM I requirements,
cr those requirements adjusted due to projected congressional
budgetary corstraints, and PRISM III, or unconstrained
requirements. To provide a more plausible comparison, the PRISM
I ard PRISM III projections were combined with the norprovider
prcjections cf the FY 33 historical workload-driven projections.
. . .43
rr
Page 42
~~~~~~.. ... ................................. iCii
'* %
Those combinations are identified as Adjusted FY 88 PRISM I and
PRISM III in Appendix G and in Table 1. Total requirements under, .
an adjusted PRISM forecast were 1456 and 148 3 (for PRISM I and
III, respectively) and are 3 and 5 percent higher than the FY 85 ... ,.
euthorization level. Again, these projection do not consider the '
added variable cf the major change to facility capacity brought "
about by construction. -'-
To account for the physical impact of the new composite _
medical facility, a needs assessment was conducted with all
departments and directorates in the USAF Medical Center,
Wright-Patterson as illustrated in Table 2. I
d----
Table 2Departments and Directorates Surveyedfor Forecasted Manpower Requirements ;.
USAF Medical Center, Wright-Patterson
Wright-Patterson AFB, Ohio
Aerospace Medicine Department Medical Education and TrainingBinervironmental Engineering Medical Information SystemsDental Service Medical Legal AdvisorDepartment of Medicine Medical Logistics ManagementDepartment of Nursing Mental Health DepartmentDepartment of Nuclear Medicine DepartmentObstetrics/Gynecology (OB/GYN) Nutritional Medicine DepartmentDepartment of Radiology Orthopedic DepartmentDepartment of Surgery Pathology Department I .,_1Development Directrrate Patient Affairs
Directorate of Pediatric DepartmentHospital Services Personnel and Administrative
Directorate, Resource ServicesManagement Office Pharmacy Department
Emergency Medicine Physical Therapy DepartmentFacilities Management Physiolo gical TrainingHyperbaric Medicine Primary Care
Medical Command Administratirn
o.2
........................................
- -'- - - - - - - -- -. - - - - - -. -. - --------
%.
I-.-A
Page 43
Thirty of the thirty-one surveys were returned for a
ninety-seven percent return rate. Twenty-one departments
responded that changes to their manpower requirements were
needed. Nine indicated that no changes to their manpower needs
were necessary. The overall effect of the survey was to increase
manpower requirements to 1652 authorizations, or a 17 percent
increase over the FY 85 baseline.
Description and Discussion
This study has already provided ample discussion on
current Air Force manpower standards and the new manpower
modeling program for health care providers. The needs assessment
survey identified numerous increases in manpower requirements,
which the departments and directorates felt were needed. While
these changes were broad based, some bear discussion:
o Medical Command was recommended to increase with the
addition of a Vice Commander and Executive Officer to the Medical
Center Commander. These two positions are needed to improve
continuity of executive health management as a result of the
complex technologies, increased physical capability and
increasing staff size of this Medical Center.
o Medical Information Systems requires a 54 percent
.5 increase in staff at management and technician levels to meet the
tremendous growth in advanced health information systems since q
the commencement of the ACP .
r, The Development Directorate, resprsible for
0..6
.. . .*6 .*.--.
., . . . . .. .. . . .. *.-, .. .. ... *.. - - - .,"' - ._-". .4 ..- ".- ,"'-- -:- -
Page 44
V"7717 77 .
construction liaison, will be disassembled upon completion of the
MCP and the manpower authorizations returned to HQ USAF.
o T he Medi cal Logi stic s Man agement D irec tor ate requested
38 additional enlisted and civilian positions. These increases
j are needed to provide technical logistics support for the Central
Processing and Distribution function incorporated in the new
facility's design. Further increases are needed to meet
logistical and biomedical maintenance management demands caused
* by the numerous systems and technologies delivered in the new
health care facility.
0 Facilities Management requested four more civilian and
* enlisted authorizations to manage a facility which has doubled in
- size as a result of the construction project. Not included in
these increases are additional requirements for facilities
support and housekeeping. Technical facilities support is
-, provided by personnel assigned to the base civil engineering
function but attached to the Medical Center. This relationship
* should be considered similar to contracted support. Facilities
* support staff is projected to increase from 17 positions to 43
upon MCP completion. As for housekeeping, this service is
*provided by commercial contract. Presently, the housekeeping
* contractor employs 70 people and expects that to grow to over
o The Department of Radiology has requested 17
additional authorizations. Both professional and technician
37
Page 45
%'
levels should be increased to meet the clinical demands of all
medical departments, to support modernized and new equipment
technologies acquired in conjunction with the MCP and to meet
increased patient care demand levels. New capabilities exist
with the addition of a new special procedures suite, a new CT
scanner, a new breast ultrasound unit, and two new
angiographic/interveniol radiologic suites.
0 The Radiation Therapy Department requires six more
authorizations to support a dual-energy linear accelerator,
simulator, hyperthermic facility, and specialized computer
equipment.
o The Clinical Laboratory Department requires five
additional technicians to accommodate facilities now provided on
two floors. Previous tasks which could use shared technician
resources are now geographically separated requiring additional
manpower for support.
o Pharmacy Services requested increases of four
pharmacists and eight technicians. Increases in patient visits
coupled with the design of significantly separated inpatient and
outpatient pharmacies necessitates these manpower increases.
Co The Department of Medicine requested numerous
increases in their manpower authorizations. Internal Medicine
was requested to increase by eleven internists to support
teaching and referral loads as well as supporting the projected
ircreases in intensive care and neo-natal beds. Technician
38
A.. '-...-.
".............: , .-..- .................................................. .... ....... ..... ..... ...... ...... ..... ........ 1>
Page 46
--------. ,- -
increases were also requested inspotof the new
gastrointestinal laboratory, the special hemodialysis laboratory,
and the expanded clinical services. Cardiopulmonary Services
were also requested to expand to meet new demands to support
major referrals from the physiology laboratory, the new neo-natal
intensive care unit, the expanded 24 bed intensive care unit
(ICU), expanded surgical capabilities, and expanded noninvasive
and cardiac catheterization laboratories. Increases in the
Neurology Service were also forecasted to accommodate increases
in patient demand. A third dermatologist and supporting
technicians were requested to support additional training
requirements and commitments to the Verterans Administration ,.-
Medical Center and Wright State University in Dayton. Two
additional allergists will be required to support the regional
mixing laboratory and consultative requirements for DOD Region
Six. Five technicians plus one physician will also be needed to
support the mixing laboratory and immunization requirements.
o The Department of Ophthalmology requires increases nf
one optometrist and six technicians. These increases are needed
to support new capabilities in laser surgery, supr athreshold and
full threshold perimetry, slit lamp photography, and improved
fluorescein angiography and fundus photography. Two
ophthalmology examination lanes and a dedicated ophthalmology
minor surgery room have also been added.
0 The remaining increases in personnel are needed to
39 -
V.
Page 47
meet the overall expanded capabilities throughout the Medical
Center caused by the doubling in square footage and the
enhancements in facility and equipment technology brought about
by construction. Of significance is the increase in medical
technologists and support personnel in the subspecialties areas,
such as cardiology and internal medicine.
As shown above, the manpower requirements from the needs
assessment survey identify manpower projections above the FY 36
and FY 88 authorization levels. Further, the results of the
survey also revealed levels which generally exceeded those of
both PRISM projections. The forecasts from the needs assessment
differ significantly from the other forecasts as it takes into
consideration the new capabilities offered by the completed
composite medical facility.
-- --
4'~ .J 4
V
6p- 1
44
4.-. %
".qy
400
-. .
.. .................................................. ...... ...--.-........ .... .............-.-........-.-........ ...... .. 1..... -.
Page 48
CHAPTER VI ,
ANALYSIS OF FINDINGS -- INTERPRETATION
In examining the issue of whether changes were needed at
the Wright-Patterson Medical Center, five options were
corsidered. Those alternatives ranged from doing nothing at all
to using a combination of manpower projections to arrive at the
best proposal for the expanded Wright-Patterson facility. The
needs assessment survey revealed numerous manpower requirements
that were not presently being met by other manpower projection -
techniques. The over riding factor causing this disparity was
that these systems did not take into consideration the military 4construction project underway at Wright-Patterson.
The results of the needs assessment survey suggest that
changes are needed in the manpower authorizations for the 4
Wright-Patterson Medical Center in FY 83. Considering the scope
of this construction project and the significant upgrading of the
physical capabilities of the medical structure and its
accompanying technology; the results of the survey were not
surprising. However, it was felt that a comparison of projected .
growth based or historical workload with the results of the
survey would provide a quantitative viewpoint of what the future
had in store for the Medical Center.
Linear Forecast
A linear program was performed using summary historical
data relating to total manpower authorizations. Appendix H is a
44 1
AL 20:.
Page 49
-, • .w~ y y .-- \ .
linear presentation of the growth of manpower authorizations at
the Wright-Patterson facility since 1979 (Facts and Figures of
Com2arative Management Data, 1980-1981 and The Big Picture
M4anagement Summar., 1982-1984). This graphically shows that
management would expect a growth in manpower authorizations to
occur without the added variable of the MC?. Table 3 provides a
summary of the forecasting technique as it applies to the
Wright-Patterson study. Applying this technique revealed that
the Wright-Patterson facility should realize a three percent
growth in manpower authorizations, or an increase from 1411 to tal
authorizations in FY 86 to 1460 authorizations in FY 83.
Comparing this linear forecast with the other growth projectiors,
a similar pattern is seen: historical workload projections
(1445), PRISM I adjusted projections (1456), and PRISM III
adjusted projections (1483).
As for the projections arrived at by the needs assessment
survey, they were well above the linear forecast (1652
requirements). But as stated previously, the linear forecast and
workload-related or productivity-related projections did not
consider the change in capacities for the Wright-Patterson
facility brought about by the MCP. Therefore, the projections
identified in the needs assessment survey must be considered for
meeting the future needs of the USAF Medical Center,
Wright-Patterson. Although the survey is
42- - -,"
S '* 5 5 ' S S - ,"-:-? ..-. ".5-
,- -.....-. ,~ ..
.# ..• ..o4, °>"- .° ° .. .- . .5. " *
Page 50
VA-Table 3
Linear Program ForecastingAuthorized Manpower
USAF Medical Center, Wright-Patterson- Wright-Patterson AFB, Ohio
1% ~~----------- --- -- -- --- -- --- ---- ----- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- ----N r F Y Total Auth
-------------------------------------------------------------------------------------
Historical Data: 1 1979 1216 1216.03 1 .002 1980 1201 2401 .92 4 .003 1931 121 3 3639 .05 9 .004 1982 1272 5089 .25 16 .005 1933 1302 6512.31 25 .006 1984 1327 7959 .49 36 .007 1985 1375 9623.74 49 .008 1 986 1 41 1 1 1283 .00 64 .00%
Totals: 36 10317 47729.79 204 .00
L in e ar 9 1 987 1 429 i.-
Projections 1 0 1938 1460(see equations)
L inear Equations:
a =(sumY)(sumX^2) - (sumX)(sumXY) 1.150e3 = 1150
N s um X 2) s (u mX) 2
b N(sumXY) - (sumX)(sumY) - 31 .01I: N(sumX^2) - (SumX)^2
y =a + bx, where y = 1150 + 31 Olx
no nquantitati ve technique , Dr andell (1975) clearly stated it
suld ntbe discounted. The implicit views and judgments of
the departments and directorates coupled with their explicit
justifications for additional staff are aimed at dealing with the
realities of providing health care in the military environment.
These increases are deemed necessary to reach the optimum
43
Page 51
pcapability of providing the clinical, ancillary, and support
Iservices intended by the design of the facility, dictated by
current clinical and medical management practices, and
commensurate with the educational philosophy of the institution.
Financial Impact
As with the private sector of the health care industry,
personnel costs in the military health care delivery system
impose major financial demands on the budget. Until recently,
only the civilian portion of persornel costs was considered by
Air Force medical facilities in their appropriated budget.
Congressional concern over the rising costs of health care in all
6sectors of the federal budget has brought about major changes in
the military medical financial management systems. Today, Air
Force medical facilities, like Wright-Patterson, are operating
A under the Medical Expense and Performance Reporting System
( MEPRs), designed to accurately ascertain operating costs and
performance levels. Using MEPR data, annual salary costs can be
ascertained and applied against the manpower forecasts of the
needs assessment survey , as shown in Table 4~ (Medical Expense and -.- ,*
Performance Reot 1986 and Unit Strength Summary Repor t, 1986).
I44
a~
1. ..
Page 52
Table 4 4.,
Financial Impact of Manpower ChangesResulting from Needs Assessment SurveyUSAF Medical Center, Wright-Patterson
Wright-Patterson AFB, Ohio
Personnel Personnel Annual Salaries Total -_-
Category: Totals: Per Employee: Salaries:
Officers 42 $55,378.27 $2,325,887.34 "-.'3-Enlisted 97 21 ,800 .51 2 ,114 ,649 .47Civilians 68 22,164.00 1,507,152.00
Total 207 5,947,683.81
The difference between the FY 86 authorizations and those
projections suggested by the needs assessment survey is 207
manpower requirements and equates to an additional $6,000,000 in
annual salary and benefits for the Wright-Patterson Medical
Center. There will be difficulties in relating the financial
impact of these increases with the USAF Medical Service budget
system. At present, military personnel costs are not included in
this financial management system. As for the projected increases
in civilian payroll costs, the benefit oortion of these costs are
not included in the accrued expenses for civilian payroll as
identified in this same system.
45.
. . . . . .. . .~ ~~. . . . . . . . .. .* . . . • . . , . _ ." .
Page 53
- . ,-- --- -. ~ - -.-.- - -..
CHAPTER VII
CONCLUSION AND RECOMMENDATIONS
The intent of this study was to determine the future
staffing requirements for the USAF Medical Center,
Wright-Patterson once the $113 million-plus medical military
construction project (MCP) was completed. This project broke
ground in 1982 and is scheduled for completion in 1983 Th e MCP
represents a meaningful enhancement to this tertiary care
facility by renovating, altering, and expanding the physical
structure and associated technology appropriate for the
comprehensive health care delivered in today's military medical
faci ities.
Inr view of DOD, congressional, and local management
concerns for medical facility staffing, this study was
commissioned to ascertain what changes, if any, were needed to
the staff at Wright-Patterson. Present and future manpower
methodologies for the USAF Medical Service do not address the
growth of manpower requirements driven by major construction .j ."projects. Consequently, a needs assessment survey was conducted .*
with the departments and directorates operating at the USAF
Medical Center, Wright-Patterson. This survey combined the
validity of historical manpower standards with the professional
judgment of the local staff in developing future staffing
requirements. This study determined that the Wright-Patterson
Medical Center's manpower requirements will grow by 207 pcsitiors
%, %*,
46
. 5 .INV
-'-,--
. .I. " . ' . . - . - . - . - ' , . - - ' .' . - . . " . , . - . - - . ' " . . . . . . . , - , . . - , . . , . . - . - , . . . . - ' . ' .% p w .
Page 54
7.~~~~~~, T..'7' : .717 .
in 1983, reaching a total requirement of 1652 positions. This
growth will result in the total salary and benefit costs
increasing by approximately $6 million in 1988.d .
The following recommendations are made to implement the
new Wright-Patterson staffing requirements within the Air Force
manpower planning system:
1. Executive management should incorporate the results
of this study as appropriate goals and objectives in the USAF
Medical Center, Wright-Patterson Strategic Plan. As part of the
strategic management process, executive management may wish the
Medical Center Methods Improvement Committee and the Financial
Working Group to review, comment, and recommend a course of
action appropriate to the intent of the study to the Medical.I
Center Executive Committee.
2. The local Air Force Management Engineering Team
should review and comment on the results of this study. Such
action would provide the basis and support for future management
actions aimed at increasing the staff at the Medical Center.
3. Based on the guidance provi ded by the local
management engineering team, the Medical Center management should
initiate authorization requests for manpower allocations and the
necessary budgetary increases in the FY 83 Medical Center to
implement the recommended changes. This action may be best
accomplished through the submission of a program objective
memcrandum (POM) tr the Office of the Command Surgenr,
4~7"° " -S.
~-. ~ J -- --- ~ - .-- -.- - - - ---- 5' % ~ * %* *" %%
Page 55
W ,
Headquarters Air Force Logistics Command. The POM submission
would introduce the unfunded requirements of the Medical Center's t
manning needs into the five year DOD budgetary and planning
system. Due to the e3rly concessions made in obtaining the MCP
approval and due to the questionable validity of the past . I
manpower planning submission for this MCP, executive management
should seek an elevation of the future manpower needs within the
overall major command requirements for FY 38.
r. In summary, all aspects of the health care industry are
feeling the effects of competition fcr limited dollars needed to
deliver quality care. The Air Force health care delivery system,
just as the private sector, is constantly striving to enhance the
quality of care it provides. A key component in attaining that
goal is providing the optimum human resources necessary to
deliver quality health care. This study has determined that
increases in staffing are needed at the USAF Medical Center, -
Wright-Patterson to support the overall USAF Medical Service goal
of enhancing current programs to ensure the provision of the best
medical care possible.
48
..-.. ..- ,... .
-. ." j
Page 56
4--..p 'V
4%d p .p
4. ,~
,4,~ ...
.4.
.4. ..4.
.4.2
V
APPENDIX A
'5
5.4
'p.
/
4..
*45,
SW
.4...4..J5
S.
S.' S
S.5
5-
5..-..-
------
~ ~ S -*5~ .. ~...-\.-..-i....-'...K.-...5---. * ~. ~ - -. * S..-' ~ *~****
Page 57
-~ - . -- ~. ~ * - * -
JU-p.
cp
ItC
7i c
2 C 5
. c E ~ _ _
4 1. 4
w. &*..* .. . . .. 3t
49.
Page 58
~-. .~.. -.~
.~ -
V -
V
~
, *~4
4 ~ ~*
APPENI.~IX B
I
i
-. a* f.'1
.1 p
Page 59
CO ~ %%
E-4-
di4
z EcrO
3:J
0S
WI(oz)
..
u. .9c
E. r
00
cr2n
UP.
1..
0" "*
5~*5 5S*** * 5
Page 60
7. 7.. W. .- .- -- I. -
71
Page 62
S.*-.,, .-.
~r~
'A -
- I
9"' .' '.'.
A- ,.,
A,'% '
'% '% -
A.ll
J*"; *-'
itA'
'
Page 63
T-7-, IV wve . - ,'W. .
ceeCL..
C.L*J LL)* . .
-i Inc
0 0 U
LI-.
(11 ce w CL V~0 0 o
>.L.J LPn 0 CD-
0.0 CD I-cL
CL. LL) Z- C) C.- t-)
cr LLI LiiUJ
ce LL. C Li. 0 c
LL C) i 0 mc O
It. LL : k
L 0 Iii JL L L C
-cc1 S-c L/
LiiI , CA0 = ii --. -
CDc
3. Li. C.
-w C5I w/ 0 0'C 0:
L) Lii t/- C) Lii
U-~ 7-7
LL. re w r . U
52Ln"
C14 rr L.
*5 '* ' ~ 4.. **.*p..*n....*.*4....* .. .*.4.... .. .-- 4.~*-.52 *5
* ________ l
Page 64
% I
~>
E- >
* _ :o
z ::)
* .4
zz Q0--d <
Cf "" 53
~N
Page 65
LJJ
-L C'A
LL. Lo 0 r 0 LLL. ~ ~ r ul -C .
LL)
LL CJ - L
L' 0 -J i
C3
CD
- -
00 "
544
"I 7z
Page 66
-..
E - 4. ..~
crxi
< )-
c L J cy UJ
w >- C) S
LLIj c~ L L J L) (D
:C: -. C) -i )
c <~ * - >- M0 U
554
Ad
Page 67
.4-
0 P4 H .. 0 04
C0 Q40
L- .) Z.) 0 0 -z 0 % ,
- 4- 3 -
H) Ul~~- cn E-4 C. ) U C
H~ ~ ~ ~ j C. 4 -c<' kH 4
C/3 H ) H H E- 'o H H
u >) HE-4 CA H HH
C44 rZ Ci ri. H 0 H
E -En z H %I %
0 H -4 E -
Ht C-4
Orz
-Z 1-4 C4- I-
P 41
C4 C
zz
C.CO
Zz V..-
-ad w C) C
ad Cw .) C4) CllC 4-4 Z -40
0 H C. R2. , C C)-
He u Ol Ol C-
ce A ZC: Ge .44 0 0 H
C.) 0 w- -W Ci4
4-cd H 0) E-4 HV
-4.a CHc1 Z4 Z 3' t
- E-4 4- x:DJ
H E
Z- E- 4 -4 0If
E- 0 - E-4 L) E-4 H ' o -
[- F41 ;z~ ) '4 H - -
C14 E,() O 1 4 4 ~ (. ) ~ C~~ -4 0 En rn % .n5-
(4*4r-co Ln tf) c r- M... .,
56
Page 68
i'4 E
44.~ T.a..T
-aa
C, C
F-4 z0X
-. Al
O-4 IU -) --
C) FH Z En 4 0419= U3 0C-
a4 04
~ H ~ aCD ~ W4 E-44', w u' C, 0C-
>- 0-- CLI
H ~ ~ ~ ~ 0 .-4 r.4fl Ii 41 ~ - a
'E-4
U) w * -E-4cn Ww
'4.n
Jlba
R5
Page 69
F-LL
F4 04 PA P
uA u C-1
E-4 w H H C
C-. Ci2 c L
% CA
Page 70
w -r~rrr r C - r- -rr-7.--~r r ~ -rr -%
E-4 4
z 0 zz ~ ~ ~ 0 40 t C
04 CI 04 04 0n E-4 E- 04
H- C-4 C' H H z H- .4 - ( H
r.4 44 C., C) -4 -
E-
f--4H H- H-
H En p 0 E-4 0E ~-4 0 H E ~ O 0 r.-4 E-41"- r, IN '4 H o C14 o 1 - C4 r- en 0D C4 U')
co -4 C1 (4 H- H4 H4 H aN H4 H H c*
59'
f 41' d,,c ' "-.7. '
Page 71
4>
0 0 Z
0Z ,-4 0 r 5..
Ui > E- 04 PE 0E- 1 4-4 z U -
En (n4~~ En
u~ 00.1
cm. c) .
ir l) 0 0 0 H- C0 > i
0
.5~~~ w~~HU i i
H Z 9z E-
u 0 E_4 E-ad En (n
0 E-4 4
C- z .
ad IV.
E- 0 u1 0
60
% % .*.%
Page 72
PC-
1'O cnp
4. .
4..)
C.)
.5,
C4 >b~,Cl1) a.
/ C'.
S.0
UJ d 1 .
IL4*
S2.
CL C/)
>d Qvo-~
XX l
co.a
6 Ie .c
AC
z Z.
Page 73
* ." - -. ;
AP PENDIX0'.'- tQ
I'
L.4 ... ',
' -. " rP.-. 4
/ 8 " %4
Page 74
-U
0 r -ii 0U 3:~~--- 1 6
U co6
4A U~j IX-
u t-* *b
R t
"p. -- - ILU mL4. %I-.
V !I
2 L-0- L. Lr JL- - _
L -
0V3 Io A a
_ F-iTil LT
62I0 ~ -
Page 75
-J " I, . .- , . ,,- .-- , - . 4 .. -.
°S. -o
p . o°",
APPENDIX F" "
5.
% . -.
S %...q,..:..:.-
.:-"5,o°°:
"IN . .
L." " .a . '' '"'" " " "" " %
" " "," - " " " . . ,' ". ". , ." ," ' " " - " - - ". " 'S .
Page 76
SG A- R
Manpower Requirements Resulting from the Medical Military
Construction Program
See Distribution
1. I'm pleased to advise you that we are initiating acomprehensive review of our Medical Center manpower program inanticipation of our occupancy of all areas renovated, al1te r ed or
added to by the medical Military Construction Program (MCP)Iproject. Specifically, we want to examine what manning isnecessary to operate your directorate or department in this new t2environment. 'That is, do we need to change the number ofpersonnel authorizations required to operate your functional areaat its optimum capacity?
2. Since our last manpower projection based on this MCP, we havecollectively experienced numerous changes to those factorspinfluencing our methods of delivering care. Some examples ofthese changes are improvements in health care practices, newIrequirements in quality assurance, medical readiness, changes intechnology, and new mission requirements. These issues may havealready been addressed by specific manpower additives or byworkload adjustments.
3.- Now that we are well past the halfway point with thisconstruction project, I have asked Capt Ray Williams to conduct amanpower management study. Capt Williams, a 10-year veteranMedical Service Corps officer completing an AF-sponsored master's%p degree in hospital and health administration, is assigned to us9as an administrative resident through the summer. ~'%
4 . One aspect of Capt Williams' study of our manningLi requirements necessitates your valuable input. Request youdetermine your future manpower needs based only on the changes inwork environment you'll experience as a result of the MCP.Fiscal Year 1983 has been chosen since this point in time shoulIdsignify completion of construction. It should also mark thepoint, for forecasting purposes, that your workload will beeffected by providing care in a new physical environment. We >~
have provided a manpower authorization document in Attachment 1,which will become the 1986 basis for your submission. Based o nthis information and the changes you will experience in thephysical capacity of your work environment resulting from theMCP , you should be able to forecast a reasonable expectation of
% your manpower needs for FY83. Any increase or decrease in yourforecast must be supported with detailed, realistic
Qf63
d- - 76.
Page 77
justifications supported by changes in your facility's capacityand by new equipment provided under the MCP.
5. We realize the impact this request has upon your alreadyhectic schedule. However, I'm sure you'll agree that the futurebenefits to your staff and to your patients warrant a top-notcheffort. We have provided for your review a sample forecast inAttachment 2. We ask you to respond with your projected manpowerand justification in the format illustrated in Attachment 3. kYour response should reach SGM not later than 15 May 1986.Negative replies are required.
6. Questions or clarifications may be addressed with Capt ...
Williams, ext 79883, or Capt Underwood, ext 79120.
BRUCE D. WILHELM 3 AtchColonel, USAF, MSC 1 ManpowerAdministr ator Authorization
Document2. Sample Response3. Response Format
I e
<<.
64 . -,,"7614 L
I-... . . . . . . . . .. . . . . . . . -,-. . . . . . . . . . . . . . . . . . .
. .. .'s',%,
Page 78
.' .
- SAMPLE-FY88 MANPOWER FORECAST
Functional Account Code (FAC): 5110
Function Title: Medical Logistics Management Directorate
Prepared by (Name, office symbol, extension):
Major Gruendell, SGL, '77195
FY86 FY88 Forecast
Number Number
AFSC AFSC Title Cat Authorized Required Difference
9016 Chief, Med Log Off 1 1 09025 Chief, MEMO Off 1 1 091500 Super, Med Log Enl 1 1 0 ".
91570 Med Mat Supervisor Enl 5 5 0C i v 1 1 0 A""Q
91550 Med Mat Specialist E+ n1 8 8 0Civ 1 1 16 +5 .. _
91530 Med Mat Apprentice En1 6 16 +1090650 Clerk Stenographic Civ 1 1 0
Justification for change in manpower (be specific):
As a result of the FY32 Military Construction Program (MCP), theMedical Logistics Management Directorate will operate the newlyinstituted function, the Central Processing and Distribution (CP-D) Division. The function of CPD is to provide materielprocurement, sterilization, processing, decontamination, storage,distribution, and transportation in support of all inpatientmedical functions at the USAF Medical Center, Wright-PatterSon.Primary missions will be to provide automatic resupply ofroutinely used medical supply items and to provide an asepticallymanaged system that processes medical instruments. Approximately60 medical center accounts will be supported by this new conceptin logistics support.
Tr, accomplish this 24 hours-a-day, 7 days-a-week mission, anelaborate specially designed system of exchange carts, storagemedia, decontamination, and sterilization equipment, andautomated information management systems will be used to carryout the policies and procedures prescribed by AFM 67-1, Vol V,
65
. . . . .
Page 79
'.,.- .
Chap 10. Presently, medical items are issued from MedicalLogistics to the using activities during normal duty hours,
Monday through Friday. Ordering and storage of routinely usedmedical supply items require the daily involvement of health careproviders and technicians often resulting in stock outages orexcessive on-hand inventories. CPD is designed to reduce supplymismanagement or maldistribution and to free providers andtechnicians enabling greater involvement in direct patient care.CPD requires the assignment of 20 additional medical materielspecialists to perform required duties.
Approved by: Date: 14 April 1986
Dir ectorate/Departmen t Chairperson
66-
-CO
S °°
F .
* ., °,.
" ~~66 ''- :
.." 5-% .. % . . . .. 5,*-.
Page 80
FY88 MANPOWER FORECAST
Functional Account Code (FAC):
Function T itle:
Prepared by (Name, office symbol, extension):
FY86 FY83 Forecast------------------------------------------------------------ -----------------------
Number NumberAFSC AFSC Title Cat Authorized Required D if fe re n ce
Justification for change in manpower (be specific):
Approved by: Da te:
Directorate/Department Chairperson
67
Page 81
DISTRIBUTION LIST .'*
SG3 B SG HN ISGD SG HASG E S' HBSGF SG HC 4.1
SGG SG HESG I SGHGkISG J SG HHSG K SGH I
-. SO5GM SGSOHI iMSG P SOu HOSG Q SG HPS G R SG HR
SG A 1 SG HS
INFORMATION
SG SrGA- 2SG A SGMM
IkVI
V68
Page 82
.%-C -
** .-
P* "%' "A.
VP.o*.,, ."
APPENDIX G"I...,
"/ .-TM-
i.i5 ty: i
.. J9.
Page 83
-- >--- - - -- -C,0 0 0
w- 43 0
3/) 1"o. 7:
a1 > 0 00000-- 0N'C - tz3'.J -.- 0-- C: 0mo C 0000 C)C3C
b4.- - ------ - In vMn
m 1 1>
0 -I --
4~L C.
-> -..
3. -
0 03
10 ( 1 - - - - ,C4f"CIcmI, o
IC-)
-- 1 1- 031' I - nn n I
cn0. 10 . . -,W*I )a ,CC 3 C
-33 l3 /
(A ) n I 4
'1: 103..V c la> E E
V 'o CL
,c -C 3. I 3o 0 0- 0- '3C3 0 - ~ . -b N c . :1 -.I M In V)0 .- 0 ,.4IVI
-- C 0 I0
IL I 17C4 u >. u 303"0 33 X -') I
1 1-FF m MC. v 0C j~~.C C~ -a w , m v-U 00 C-C33C -r CCCC uJIM3M
-- AD.~I 0 0 ~ . C ~ -0 0 0. IL l . )0 ' 3 t).3-.v , w ,r-
I 01 00 0It
t3 CO.. t~ U, C) 103. CD N -I= n - ,~~3.3~I In In3~34- In 434 CO
3 V3/)--30.3)c/~4,'3-693
Page 84
-- I > I --
12 I - 1 1- S~ .I 1 0
co '
-- hgI 0 --
V 50
:1 ~~C - ---s --- 0-- j Cl M j(
I.' o
I- 1 ) I
0~~
mE ~ ~ 2: 0000:X120 12* L..fl.I
N ~ ~~~~~~ ~ In0 0 0 0 C )C30 0 C ) C , 0-
10 Im \0. 100 0 0.-00 0C
-m a,-~I0 3,0 m- M
1>1 (>
En I' m u4 cv-I-C I - a 00 3 LCL - C C .- u w 0 (
0 4) V) V)- I Uno 00
-- 1 w -1 1 -
>- 0. -) - " , '
r w -Z- I
-IJ
n U In 0 10 00 0000 tCo o o M'n0M 000000
oo m ,o
4) .~*) 70
n ON o.ft C 4
Page 85
10 IN 4O
- 4>l .0 M- - -ar --444 I r"..
I- -_uI~ - --OF > I --
CJ Ng N. tn - -
IC'j
o 0- C3 0 c 0 c. C 00 a o4
:3 .. I I - \ Q t- -h0 I I --
v w I I
a)/I >
0- ( a to I CV0t--C
* I>I
-- 101 Li- n ,
-- ~~~~n C, M I - N N 4 0 N ',"
(I d) I .4
4. N u(4 010I 01-- r44E4 10 c0,-2I
m- u t- I0-U '-c M Ch0 1a O 1 (1M Y 44 ) m 0 ~ N N
- ) V) CM Y)0E/0-00 0 tn0V0GI0m 0 0 0000000000 0 00000000
-- 4 10 0 0
01 -I-l -4 0 P 1 0 d )0 I 1IU1 7 :'- r X Zr ).( ,0
x-4 3L 3cl -vl um a *cd )r YCt
to %-144 (4. q o -q 4
-- 1 0 1 a l d l v T o - W-t .4 1
At M tn t-N N m-- M M0 r t -Nn m t-0 4 -n' --
C3 1 4 3 --
* -- 4- I I -- N~mU '71
Page 86
k --j o,-.---;.' -I A N ~-'-4. - -. .- .- - - -r-
4) m c cm 0cm IN*. ('
1>1 CVC % 1 I
--~~~r n1> IN-N ,
-- c - -- -IN N O1 rj In
OD x > La
100 7-*
t- l-d -V
I Q M \IVCJ <4 ~U -- ~00 000 0000 000 000 000 0 00 000 000 000
-'I I
1,n C,%L6*O~:Im -N.-uN--NO 0
31~
C - C- 4'1E
p1
' --
.3 D ~ M Dn0C ; DC >nC >0c In0(DC C )0nC ,n0nIIn zL4 . 0 -- I nL Amm- -u ' nInI nI U U IN I n" n" ~ nI
, o 0 or I 0% 00O \ nN(JC 0 D U1 I ~ )0 001 01 0n C 01 -:31 NI 1CJC1NCj()C j(j Ci(I r jC\ ~ v(j011 0 00 C -
aI , ~ 1000m0000In00000000m0 0 000 M 0 000000 000 M3 %
N '
0- In-~I V)v'n E ,Ii 0 w - , 0 C)- id 14
II- w -w>CI ri-.- N~ CL' CLv w v 0 4 )w L LaC
0 >~ 6 r0-C .0 4). 14 1 ov00> 0103 0 L
_u M10 'a--1
I- ILI I --- 0I
-- 0 0 10 (DzC3 0. 4,r -4 -
> r Ic c .4 -t < r77
Cl. 06 l. I Cl 4 0.l 0) W W I'0'0'0 n0 1110 0
0>- CL I'I to, (3 wNN 12'aNwNw ICNN CNu t' 0000000 00 M:000
T3
IL0 41
10 j00 0 0
a 'a4 C,
17 N,,,, 1 1 .l 04 1 1 4,, 1 1 14>4 .1100
I~ ~ ~ ~ ~ ~ ~~~Al eet..O.. ~0 .0 ....... ,I 11I1/ 1.44
NI l0~ 0.4 4
1(1 V6l,1C1V44~14d. -> 0 0 0 4-I
Page 87
*-'--- .. .--. -- -4!U
-w..
'hT'4 4 ' ! ~ .0
o2
ru. m e
* - ~ Ij (% M--- 4---.N
V- 4,. In t- In C4 Iv I
it - I e- /- 0 1 -- %6-P. I~g 4.. .I.IgCI
Wg~.l N (n0 %
.4A 034 -0 Io 4.1-- k.0. C, "
z 14,04
-- NV (1 --x I C
0- 000 0( 00 00 0 -- . -400.
--Z ((Eco ~ l'I- . ~
C. 11 M -- 0 00000a - C t
- 0 X, I1 I -
.0 U I I -
t, C, C, 1-
-- ~c N I - -
QLO I-4.0- ' M(4 C00. 00 oC o nt r -c)t
L, cj i -- C 1
co 0. 441 co M1 - 1 m
00 C03 a a4 00 00 00000000 oonooo
14 IO 1 \0 10 10 0 0 1N 10 1010 10 100 10 100 .0.04. I 0 ,100C0 0 0 0 0 0 0000C0 00000
ti0 0 0 -0 40(
I 20 C-v .- 4.) .4)- 4,00 .-4)~ ~ &I II M, M4 bo M4 v4 . 4 4 4 44 0 0 M . * 3.
4 ~ ~ ~ " c 0 01 -.4 c . ~ . ~4 0 0 .~ 0. 4,- &Z ~ 0 w w. 0....- 4 -z -4
CL. I .3 'o C t C~ " v ~ cu 4, tnE I V tI~~CCC~~~~4,4,~~ 0, , C . ~ C 42 ~ ; 4 4 4 --It; a, *.cmJ- .4404 *. ~., 4. 44. *44- .
L? TI---2Co ~ ~ ~ ~ ~ ~ ~ ~ l EI p-L 22o.-~4-..4...4
V)0 2 ,-.-4..4 ~ ..-
w 0.4. 4, 043. v c% 0 llo )44.* X-. 0: X -- .0I 0 jx - - cit
-r- -f- - oJ-CO NIm n% t,-m , N-r ID 4 '0- 0100 "1
73
~j * ~ ~%
Page 88
C',.
01 AI - -CJ- --N - - .-- -
tn 4)t-t -c
-,- -.. -N - - - -
IM I
., C, 0
> -- -)~ - -, -I - -~ -- - "LO -
-- - -
4 %-
0. .n0
5 -= 0 0 0 0 0 0 0 0 0 I V OnO O O O Io O On oI n oI n 0 0
*1*41
4.J C4
.4I CL 1'
to 00w > -INm t
40 00001 0;161i~ 06 -L r 0: 'a00e0MO00006000> >j .1a. 0' 0' --
CL 1 0 1c In1
C6 C) LI3r
I
0 0 tn 0- 0
0g IC I >
o- m-4 m r. **
0 ILI I'.-.C )
c- m. 4, wI , C
lu
I - tn --- --tn 'oo t. m 0000 m 000o0I'D
IN Nr.,,~ (\l-jff~fU Pi~.gs-,,,~0rr,-.lr.- U m~ Ini r
74 0
Oft Al
Page 89
w ~ ~ en.r - nM - - - - -
vi w
M (M -- - - - - - - N
C'3 - -- - - 0 C) C) 0 0co Ia -
:: 0 V I I - 'Ln M \0 ' , , C
N' CICJ- - N
00 4 r I-4 cv\ m -C
-- 1 Ln M -~ --- 0(7 0
ID
m I .1
1 03 to
C) *0 I_ , -- t- _NnU nL oI
r- -- .- L~ 0 --- c ~ j
-11 I
-- bI I3 -- 00 00 -L Oo O O oXO 0 0000o0 w
0-4 Int n11I
> -c c 10 -. -. o Im 1 m -c1
-0 I -a'
c -- a)L~ , -- 000 o 1
0 vI l 10 1 Qv'
C3. 1 -
N- tiO a -c 3--i 0t- omC -. ,1-00C l oI n0In Ln LA -- % Ln1 01 01 00 ' . -c f - o, 7 ,m O Y
1>1 75
Page 90
P.. -,P 7.P. -F " ) .
(NJ~~. - -If
M - -- -. CD 0O
-- V) WI -- 0D nj0NC~--. 2 I I IX.-CJ (I
(/c w
-- 022 0 C) 0 0C) C)0 -0000 -t- NC3- CO o N oJ(-CcJ N
.0 V) 1''-- O 0 -
CL. > a
i-i V)0 o 0 C )1 ''
I -- 000 00 00 0 o .000 m ( C 50 71 NO O OO O n 00000C 0 C , DC I,
-- 4 b.0. N (\ -
r- ii coN 00.-0.-- ( n
-- ~( 0 I - NN0r -2 U-1I .
m-I I - r-a' 0~0 00 0 -0,Io (\
.0 C II , . nu-- ~~~~C In t- In-0 00 0 .n -000 .n u00 00 0 0 0 00
- -,o0 N 'o' nI I D nI -- -I,1
1-a' (XC o )-- 14.0. In x
*~ -- 2 r I -
III4.. m. - N .. 1 0v . 0
V- TI T) a- 'a- N 1-0U 0 T m( DC0 (1U m71V7
--. a, M II m- N w.r -.- 0.wm mI) I I I
CL 0 I lev ZX 3 ClC
r4 U I 0 -- M n t- 1 I-01
d
In0InM I
-- 0 VI 0176 ,- V. "1 7 ,
Page 91
7..4 77V.7TW
1.1i
> I ri r
41 - 44 N I - N -~ - .--
1c 4, 0 4
-00 141640J (D0C 000C
0 O I- ;/i
cm C4- CM- -
n, o'j '-'o-. ci
co IC
N -- J 4',- -.J- -
co -'M ell' I~ =t ~ MI n
-41IV
-- -- 0 \0'0 00000000- CC,) tI tr ' i - I~
In In In -- 0 0I0 If,0 In 11IN ' - - - - -
44-O-I In--L nn
b~~ e '0 I
IV4 II aILCLt- -1 '0I n .I
M m
013 v-o-01 41l
'I L- rN mONIeL.- -(C -W hOb O
1- 0m' 0 m 0
*l C, 101 >
ILI 1 ) -- 0 0 00 0 .- o M -- ~ ~ o o .0 00 00 0wCL 0.r)muV . MII 1)- 1 7 omV
m- 4040 1- In -.0 t-- n 7 ; 4In4 In InI nI ' o' D'
-- t..~l I77
Page 92
- > 10 -- - - -M n -
0 1>1 0 -
-M - - - -
- 3 00) - - -- - -.1-i-i- - -,
- - >)4)4I=IIn
CO' '1 LA .
=I z* '. I0 1 ---- - - - -
.cL CL 1 01 '4
-O Cy -,D-N
- .0 I -- - ' J 0.0 J--fI-l- - - - -- -0,n n
Ip. - -W - - -
> LOI
_-r mL.Q -D - -- -' -- - -y (i -
I M .0
n* nZ -1 0
-- u IiQ vu i I Q-.' X -OLiw- w) '4I1 - ) w
IL 111 0,-,I.J m '
I V W0 -- 0 I -- 0~O ~ o o O O o 0 00 00a0 0 0 a 0 LXa) 00>
10 n 0sn 3F
-1 LL- I- c- 0 1-- % (
IID i n' A F- - - - - - - I . w m '
-- '0LL -- '. m mMM>"'7 4 L Mr
10 T) '0 It It. _n _I u-i ->* I .1 C .1 1.1 1)- 1 1-
W- Lt. I0 4)d X a )0 09 11c n ;- : - -I - .
41- Oi- Ini Ii., -
CM~i -n 0 t
I a 0I : 1 nm CD 0
N~. IN t-. N N C" N n, tfi N IN N N N-"I (NJ N lU N n)r"I N n. "A cm
* '- C73
Page 93
U 11
,.-:..-.
I _ 4 p
-- In I
.1 I m I
o o 0o I ',
- I
-_ --- : ---- ---- ----- ----.-. ----
cl 1>
-- 10 101
o /..-- 0% IC
-- - - - - --. - o -
I-31 I
ao ' I In '-Idn .n nI n I nI n n oIn' o'
I It,/-" I
o%., 41 I 1 m "t "0
I., .-- I I
J, w - C) c) c5 o c. . . . .o 0-. kC 5C I,. o ,o o o C o -o .l0 o n 0 c
L I-
-- t 101a r - r rm : 3 3 : 1:
I- n4 o n I -- oC
- ----------- - - - -/
14. - I d I 0o 0 o 0000000C 0 v > >
I 1 1 o -1. m mm m m
III - .. - - IIn M. ck, a.D
d, 4) :.1. .
nj ;3 In WoCII I
A, -- , 04.0 MIN n nII nI
4Oft
3 I '.-.
-- 13-~I %
Page 94
, , ,L , _
'0 ~ ~ ~ ~ ~ ~ ~ ~ , - 0N- n.-t 0 o , ODI
"d-- I W --
:I-- , 14, -- - -
e'-- 44 I I -
V) all 0 ' j-'""
-"- - -444414.4 -- " . ,
-g wI --1'1
4' ,- -4 .
-- I. -- -- - - -
-- I --
444- 1 -- - - - -
'0 0) ¢0 0. C) 0 C)0MC )0 , 0000000 3000C ) )C ) ,C
100. 0 -- I 7 1 11 - 7
w I > I L
1" ol .. 't "0 rV m , 0 t1
-- -- -. - - --- - - - - - - -
CL 41 1
e- f -- t- t -- + -f- e-- t- t--/ ) / ts- T-- E--- t-- I, f- I-N ti "I tQ (N' (N) op oI m,~ N (I
i~
80 0
al4 11 IV n.1
--'I.
71 ~ mInI V n-
_3 71. . .n Z r Z -C 3 3 -. Z .n . .......3.n.- .. - .. s , W. -.. o..r...-..r - C. . u. -, .. ". (-- 1 .., ..0--- .-< .
,v-.'n
--- - -I1 I 1- " , - - O \ 11 1 W 0 a W dO '
,, IIC
em In0. IY -- "i U 0 nII \'D -0 '0 '0
-- "t1 in Ifo In -'0r 003- 10344 (4) '0a''f r-r-'I - -(r
4-Iso
Page 95
-. -t" ".' 4
"-2'
-. - -. ~ -- - - - - - - - - - - -
I I'. .:')*i., ,'4),
- - 1- -i 0 %4>. °,-_ P
-- v) 3 1 -- ,I , ,
-- ,. 4,4) .- m
Uy 4)4L I -
-- - - - - - - - - - - - - --- .-- - ---- --(Y~-1 4)'~d
..- I. od -- .:-- I -- oo o o o o o o o ooo o oooo oo o(oo o o o "
-.-I -: .:.. -
• -- '.4IO -- % lp.'
I' f -00000 0 a0 0 000a0 00)0 m aC)C C)n0 (,nD nci0 C C D0 000 ')0 00 0 0
-- ').Q --I9" . .
-- -o i -- -
-- g -- .
C, C, a) C-.4 0 DC 0aC DC )I= M = ) )nC 7,0C 30C
*-- 14.2 WI -- -o o o oo
*-- Ini-) ( I --
LI, C '.
ON, L 3 1 % %
-- ) L" -- - - - - - -o-oo o - - o - o - -o - - -o o -o c - -o o o - -i-
- - - - -
,...
-- 0 0 4)s I I --0 0 0 - - - - - -O O-O-OO O-O-O -O- O-O-
... "
t-- cl_ (V t- t- .t.- t-. t_- - r - t- t , - I- t- t-- t- - .t- t -- I -t- t C .- t - 4 .' r-C-
, I I ., o 0 C-5 C7. 7 ' O O O O m 1 Y 0 O m 0 a m m O O c-
0- V) i- dIM 0
- . . . - - - - . . . . -
, L, > -.
CL :) w 0v0 0 j~ :3- )- - - ------ -- - -0
*j In S . 0 IN In I, n0*~~C 4)1 C 0n r ~ ~ O 0
It 0-4) - - - -- -
Page 96
- ~ ~ ~ ~ ~ ~ ~ --- -, - - - - -co 'A. , ' f
C3,~~* 411 1-
-- -- - - - - - - - - -- - --
Lin In CY
--r 100 -jI'
-- - - -- -~) -fU -r)' O - .' - - --
-- - - - -
-- -ial - - -- - -
ItI
PI I-n *l-(JM n i w' n
m0/) I1Cma 11 a ,n
-- ~ I do 10:,~. ur
-. 4)10 V--
~IIn
>> > > ,J > 0i m
10 101
0 I
-- I)..-J It V)0 C% I Ir cm-I n r ,t. n-
'0 -. I-A
Page 97
S .. ,
* ,, . 4
. In
-- gI -- " ' Mt
I-I -I-- z 1. {) 01 -- - - =
-- co g: W -- - - - - -- - - - - -- -- -- - -
* -- fl.)V WI -
-- ~C 0~ - D 0 0 O O O C) , 0 0 (0 0 0 C50 C) 0 C (D O 10 0 C5 0- Ic 0 O C, O 0 OD 0 ) O 0 0 0 0 """"'
.. - - I n4 I
-- u-~) ~ --
0-- 1 I -- - - - - - - -
I*'-. I-- .- I0I -- OO O (7O OOO O O O O OOO OO O O OO O O ""
-- - -.. - -- - - r- -,--j m o - - - - -.-- -
-- ,0 - -I -- - ---
-- 7 ,1 --
" °
.. ... .> Z
*no oo o- -- o 4-oo Iz ID 10000000000000000 0n0o In o0n0In0a0o0 00G 0
It 44%4I I~ mI jc
._ _ n m;o _
In n 'A( InI-- t..-I....
1,_ In In 1) 1,' ' In II -,
-M 1>1 1- M- Mu 1 , I M , m T 0* 0 Cm0 -- -
I' -- - - - - - - - -
j IN N- -jr,
S 3I 4.-
,
-- 4.........0I -
,- * 4)4 j 1o o o > o '. J o J ('1 2> .% > > > > ) o . 0 "p' - '-
_ L L U -J r.. U -.9 U U , u u u u u (J [) ) .- ) q lC - -"E F " ' < ' '
*' ," " .
. . . . . . . . . . .. . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. .: -% '
* .0.
.1 .. . ."-",.",. "". ,."" I4'.'1 'U' -- "'.-" ." -"-"-" " " ." / - '" ."" ''. ,-,.. .. . - -4. . . . . . . .. . . . , , ... " " % " , " - " - ". - - '" ', - '"",-,'-,. I .. I,,- K . a.je W ,., L , -,L , -W ,- '-
."a.- - ', L .. " 101 _ -2 " J-''" - e ._ ° .. * -I' .'I [LL ,K'a.J ' m a ' ' .
". .
Page 98
CY C '
tn I
I',
Ind~
-- I lo - a~0 -
...
.o 'D
In 0 1 1 -
U,
1• -
-- c a I I --
__ i- -.
:.
-- i.. __~J -
-- "4J> I o
-- I I -
o
a
-- __0 --
,
--- I tn -- I
,%.
.*.
-.- .. .. . . .. . . .. . . .. . .
M Q
0-I
-- >-~at
Page 99
AD-8173 760 PROJECTED NRNPONER REQUIREMENTS: IDENTIFYING STRFFING 2/2REQUIREMENTS FOR OP..(U) RIR FORCE INST OF TECHIRIGHT-PRTTERSON RFB OH R NILLIRS SEP 86
UNCLASSIFIED FIT/C I/NR-86-193T F/G 65 L
I flfflf1f11..1....f
Page 100
. . . . . . . . . . .-.... ' -. -. . .- , .--..- " -. -r- ,- '. <, , % :
.4%
--9!
N.,
1.8.
11111_25 11111
I -- -_.,
..
..-..-
MICROCOPY RESOLUTION TEST CHARTNABiONAT NARTAU Of STANDARDS 1963-A
Page 101
~J, %..
*101
>- cm, MIwi---
IC f.-
.0 -t
n oa D 00-- -- M-~ - -
-~~~n M-.0.IC
0 0000000 C )0C)0 0 0 0 00 0 0 0 0 oo 000000000 --------
cot I
LaN N
im IJ
CO d, Ie. 44.e. -a ~ -4m I
43 N~ N> N N~ n ~ ' nt nnLL ~-- 0 014.,04(1,C C \m la (\0 - n o o
V I1
o m 1.-lI41 .00 UC
CL a- C) I I 3W t u 4 1
-- 1 0 10
U- 0. 4)1 m 0
L LI C 14C
CY II en '0!5m ~ ~ ~ ~ Ia al N im 'ai 'aj 'a 'a -a 0 0 - -~ 0 0t 0t 0n 0 0n 0 000> > 5- 0 0'0'
J-en *~ al--4-u~-ufl~~cl.r~nr~-.-Ifr--fl0fl'4c44cfC055Ce
I If I NNNIOU~fOOUOIS~aSIPfI' en.)N04',a'a ~ 0~4ennen).e
Page 102
*l r., '--
rP %
I-- r I0 -
> I- 4, - (V N- N m m M
I (AI
0 1 14m N (M(JC
0~~C Vt 't1.I C
-- W- 1 0
00 1 - - - -- - - - - - - -0000
Int
I to- -- -t0 - - - - - D
-- ~~~~t In In-.-ni--m~ 4, m-~-t Int4mn jN - - n jn 0NN( 'NM
n- I I"I -- m -- - NNN m 00007 mo , 00 )00 C , 0 )nn00C)C l
.0 :1... 10 w -- oQ :I
-- co -0. 0-.- m (x w 4) M 040000 v 0 000000000 0 0
V, 06 tr -. w0 .a 0 o r tnnt
-- cI~ I w -- mmmm
4) 1* > N 1 n 30 00
1 4, - I -- ttt";.d) 10 t-t.- c ZC cc v0e 1 -- 0 M ,a
CI I I -uI -
N n --- I 0 -o -- -yl-0U,' on 'm ~ In 'n r-c 0 ' r
* I..) !>.e teC\e
Page 103
0 * - - .v
a- nN-j-
-- -1~I-J --- j j)C
"0 1 1 r.- (1m- n OC, I
n' -0 0l J t-m--- n -r ~-- I - ---
*0 -- -'- -. - -.. - - --
(V -- -o -t.- nI -r-t N
-- n,- I I -
I I ,
-- -~. - -- - a -
-- 101 -- ')
-- lf ,o0 7, 0 0 O-N M-NC-.' -
-- ) oto I,.l F-0 u04/ "o -~ - 0
41 m.- "' I'-
3
M. MI d) 0 . MI-n L)iV)_ 0 N N 1. N
-- n 0CLc>' c .. I. I..-Q>'
IV I -.- mI
C,~ 0~.~ TI" a
E- wo I-,J u-Ln-
v 4, v 1~ N N -,4 ,4
n) 0 ll 1- I I" k -- O N 0 I - n ot M r) ' - M 7 n(1-
0-0 0I I -- N-- -
o 4, I-.~37
4 ~ e Ali-I
Page 104
-- -l 0 UN
> I-v--- ------
,,0 0- 1 - -- - -. -p -
IVV
-- 0 - -: --- - -CO -I'
ILI >,1 , W --
-- V.4D, - -- -
(0 4,1. 1- ICL ( 1)~I -
- -c 0II - .- 0 ~ '
-C co In%
0, -- , C (-( 0 n- a-0 -knn (0nm',,m 0C( 0n
0.. .4 4...
En ..,-0.0 x -- I WNM0 h
14 0
10 01 -- .m 0 .0 - 0 0 - - - - - - - - - - 0 0 0 0 0 0 0 0
.I -n> > m -
-- 10 -- m=-- I M M. m 0 o X >
I,. I .
t- 0 ~ >-. CO ON- M O M - 3'
-~L..4.I~l -
Page 105
et. U~ - C. (VC~- ' 3
(DI
C4~~~ - - - .- -
) u - .. .- -- n -
h4 00 (n --
-, ID 0 -- u0.~ CD0 t- r i0C5or 0clC 0N N n
rj tn -- t- > n n
0 --Iu -- - 4
n1 . - 3 c .
-N - -4)0 - -- NO--
I In
(UU, 4)C )4
a- I " . -ZQ
T c2 4) t-1.l a . ) 3 - >wW2)( L
c n '-s- 0 .3 ,1: O I 0.v4
D- :3y I - 0 u u 0.000 0. O o) ~ o -000000000F,0
CL - m .4.. Y
tn 4)142 m----m0 0t 0t-0a- C) (\ ni 3 0- N-, - - .
(M O-f'U')r)njri NNr jNN NN 0, )NNC\'(\J lN m-- enIWIAd
-- ~ ~ r OftI--N
IN I~I .% A..
Page 106
a. a. 0.
-C 0 0 )~ )
.n (\ e
L, c
no a I" I -- O -- -. flC
m- x' o-' -_ N
4o) I I I --
I~ >' I~ m
I) > I I -- j
-j t-C~ d m-o
- - 11(O 11 -
lo~ - 0.
m m
z~a oica IC I
4) M u- I %,CL m Il o wCO
11, -).
C-CL~: ~ 'vNr~j (I (Ij ~j r N nC .v '
-9 4'!2
-
Page 107
%
e,
%
Ci C n
m In Cl
S.
.. .4,
.:.
::IN -v
.,.
10 It
C .1 2.Io.
--
) < w M
-.
-- a' "Io' I- %--
. ... ~ l I -. -.
-
...e--eN
L L..
.
>
I
7
E
....
I I0
.
=1,
t
fl~n'n 'n
I InI n 00r-
-- ;- l1-N
V f- cm 0 ( I m
--
N
g
- --.-..-
,,
1
- I,
10
.. ...II..- ,-. < . . .- . . . . . < . X . . .. " . - ¢ -
--.. . . . . . . . . . . . . ..- . .. .. . .. .- --......-.. ... ... ..-......-... -- :.. ..
-- -.-. ,-...op
Page 108
C.C*
-C-C -I)1
n I - C) \Int
-- 4)__ - - - - - - - C
4) 1 1 0 -- -N-l- n - - - ~ -)C-)-Cf r)
1- U) CD-C 0 H)0C 0 0 Ll o 0 0 I
I- InC rI N -- C)C-fOLr
04 ~ ~ ~ I 0-u -r -m LrCjoC -- r 3-r J
fn -I.) co nv ~ nI n0 0 o 7 l1) 00C
4)-)- -. IC.- I! 0. oN mC 7
- . -t I .1I 7 7 -- ) 0\ m m m0 C/CC C) 00 - - - - - - - -a ,0 o000\C) )C 1-
-I u o -- 0f C -- 4 4 )K I_ K 0
4) 'n n a-V-V
III n. M V) cI lI
1- 4)* CC- Ix a >P, E1-n Iv) m - " , _ _I - l" )1)
InCC .1Il VC L / I -m ,I Io e > w>I-) n )7
-C U-C)'I)z, C), Ix aC w 3 CrInm m m :3a ,4,4
'CIDIn InC] \C0 V XI---I -t-1 -t-
-- I -- z.z
CC,~~ *%I.-
Page 109
-7-77-74- 77. y J.2
M V ) ,, 1 0 1 C 3 C 3 - -. -' - -. -
too
- 4-
...'..'
CL..cli
->1 -. -- -
-- 101 -- 4'-- 4) . I Il -- -'%-- .14'
4-. .,-I 4-4-.4',
-- - 00 10 01 .. .. " I----- - 0 >1 Ii -- ~ ~ .-- 00 - - .
m4 0 0 1 O n4- In 11 n1 1 \ N)N (In00 In. 10mC -I n I n'
-- I n f- -t- J o lIn*"Ir
0 . " , -' 4...--0 - - 1 n ,-.- - :$ n -- I,
> o, a CL -( 0
-. C ,-4 )- C " -n 0.
-- bi o 0) In I -- .1-0 -),,
In >4 .I. I, I W o Q (--- '. uL0-.I0 --
(14 ()4 I: - a )a )V 11
> M --- oo 0 CL -o (I 0000 01 0 -) C>I> zCZ) I-I/ > (U U o> 0 L ) > m m d -( nI
-- i0 -- ,I-u0 W V- C . 1 -I 1 " P
1 -41 IL "0"x
--~ k.0. o -- • -Z 1>1 Z -- .1
-- II -- m 0 -,- r, toM-'-
93" - "
:+;-- ,-' t ","':-- J -'1) ,, I -.-, .. ' '.;l'-- - --- . .. J',, _% .% . > .' I., I ',." _. t. 'i ' " . . . .
Page 110
E I-
0 1 1 -
-- -),4 -W --- - - - - -
ul I --- t J tf
-- - - - - - -- - - - - - -- - -
o 4, CI'~ 0 C),0 D00 )0 I
4.n- ICI
-- - -' -/ - - - -
co )- 'n 14- Io %C 3n ) nj ,-- I In- n Lu4, 01
n, 1j Iin j ,'I r q 0 N
0-4 1 m -0 0 0 0 0-m0m0 0 0 00N0m0 0000 ')o )0 0
w0 v20 w I d
n-4 I 3: L Z 1
v t4 IV tfl w- CL. l L0
"- 11) F- 3-t )-" nIn" n I )"
In > V4) (n In In n
M 0 W4 - V ) d , M 1 0 C C , ' n W M
'I V) 0,n I L -- .-. 0 0 OooLr.
0 '41
Page 111
-S - - - - - - -
~~~?~ e) 11C C 9
I F,.
4C. ,l fl --. -n -O .- .9---. D
-- 0 ,0 1.- -- - -N
I > 7: en m e CD
-- 11411 W -- - 000t
>1 --- 0- - ..'.
c I C)
C,1 - - - -
-o Il I -- - en en- c , - - --
w1- IDI
-- J ,- 011gv I -- m n0 0, - -
t I Lo
- - - -.- - --- - - - ,
N L I-tI I
-- 4 I I -- N N
S..., .
m m m m -- - - - - In 0 0 o
.-
9 -- 4 e 0 n In In 1. I -
-- In -- I w ."n
g-, I-Aa. I
tn~ ~ c c- .",.
-- CL > > >--to m "a . . _
e 0 0 n 0 0 0
ji -- a~n rI -- Ijc-- - I -- In o oo ooo oooooo,95 , -N
.... I> 2 - - en-le-
-- enO ( 1t. , I--
"- ..
- " " " " " '-- I' ," ","m / '' ." ' ,'J' I "--""""'--: '"'.-. "" ": . "' - " ' -"- -L'* ---" 0 I' "I -;'-'-,.,',.'_.:,,: " " "'" " " ..
Page 112
.* *- .%,.,-,> - . . ,
Il -
Ic -.- m IX
o~~- o on z1- a. L
cO, m aI,
- -- -a . - - - - -
0oo N -
Ij n (I ou ( u ufj
c7 I'- Il I C
z . I o 7 m m mo,
* Cw ItVO
0
'II I)11 11
- - a e." T" W
*0.
0" " .
o .. . .o 00
I. C
*4I I
w W)7 m Iwww . 1
...,:..:.
M" " I
--
I I
71: 1- -1- 71-
-- In t- I,7 1' In t00 t N
IN, Ne In 10In 1
oft
,
- -. c I .I.. % .
~~00 I~~~ .- OO .,o~ocn
-, -- Im , I -- ~ -- ".":oe tt
I-. ,.:" "" "" " " " " "-- - .. .. -,.'. , ". '..,. '..' " I ..' .. . . ,I '- l l - - - _ . - , . , . ., - . . . . . . . . . . . . . .
Page 113
N- CD - V - r ot-a I u 0.
., >, -.. 1.ul V) 4
v 0 >.cn~ 111
CL.3
-'o *pI
- CO'n I - -0 0 ~ 0 . . 0 - .-~ 0-.--
C~~1 -~ -- -
- - -- - N~
w C I31 1 1 - ~ - .- -- I~ *
-- 1oC I 1 -- -* -
InI n0 CD 0 C) N0~N tl1 -C0 N03 C V0 C- N', 2,0 ''n00an m u1 .3 (Vn N 1- N-I I r- I nI nt nI N0 n-I n.
r- t- t- 10 tv ; 0MC
mC IL ILC L .
% j
Il WI O0qr j 0:
m.' cI ) , 0 M
~'I o
r- LL . I.' V 0C .7
v C c I r- N Nr E d W 1-1 QN 0 F20 00
E I I a N c - ,Ni
C). IL I > )M Ww- 0J w IJ -C<,v=
m. lol 1) - NL 0e-C)L~ t c o ) - ,l cIn II01 II.J Io1 , 01 0 r -t ,t 0m
/.M 5001 A3. 2: I '-. 97I
--~~~g r~.0II -
Page 114
7 77 -,-..'. *I.
1. " - 7
> I I ---.--
In 101 -
N. i m). Cl IV-I
- W .0 x I, --- m In -- -- - - - -- - - - -
- I m 1 0 .
C.~~C MJ- r-I I
nI n
-oIO .- _I-
.... -- 00000 oOooo oooOoOoOoooooooooo oooooooo
-IV
-- --- -
-- I t -- - ,m e N N
- - ---
mI ,j 1 1 m I n - M I j I - n A JO (\ I % n . )n NVJ t 17) t-- t - In I t In M V M I-- IL 0 a a-- f U (I -- I- I.',
-- z* " o --
cI. I II
- In I 0 0 0 0 4) 000I0I00 0000 0000 0000 00000I00
0-- 0 0 --
w- V) I) 0) ILIt - (V - V -I- I- "t Q' (V (V
% 10 11 0 0 0
In 0~: a 0 n---10>a V o - ----- ------ 4
I ,.-. -
-> A- m .... m m m m m m m m m m m m m m CIA n-
, " 0 o : _
> >- > I" Q~t~(~t Z- (- V t- -L. M' (V Q(Mc
-- ~ II w
-- 0 I In f - (M m I 0t C l 0I I 0 - j- r
-,. . VI. 0 . 9 @ • . " . .:'.,
4- N I •..
1\- It In10 I' -a-L ,I
--- - -, - - -0
.0" "." ."t-"0. 00 ".'f""-0'-O.0.0.',0"O.".f"" "0."'O.fl "..-."00_009-,
* m -Jt~ 33 mr~r,,rrr.'OP
Page 115
Irv m4 t.* f t- .0M-l
cn w-%,V-I%6.
1- r4 .l N t-Iri - 0
"w Iv -- - - jI
co I tIp
-- 041> Il t- Nt--
-4 nI
Ir -- - - N l-
c In IN1)1- - ~ ~ )
b4 % I - - -
"o IC
Io t- I
-- (\ nj0. 0 --
--- Ln l- I -I
lo -- lo- U I3 In o- N ooo. Oc 7
-- 0 414I4I -
w ID aI , c Lo-- 4)LI.I) ILI -
-- 0.In m .I.-.
F.. -' 0 --- v . o U ac -- N I -- R N=a< Lncc uWj-cZz ,IV
2: 7' n 7.. n In( n cI cAou
eC 0, 0> Ci UN a r- a\n I I- 'LNot 00'0 n In lfm- 'Ir- 1-1-3 C
.- . . . .l . .-. .
Page 116
I L:
.3 co V)4.'J- 4 4 4lU
0 I
I Di
-- -' 1 - --
njc '0 tI yr
%I Li- 0 - J4
I '-3 Ico .0 u c Nt10t1 0%0' D1 0 1 Y . . ).
%- .4I.J
m I
r- l . " - 0 1-- o- c0 .C 41 I.' "a"0 V=
>, - .4 .IWgI'ell u(T. I1 -411I
J4
. 0 c '-) I 1. 1
411141110 1wI I D Ma0L o t
r4 c1 0 t 1 4-W('nJ4 In-(*Z.44. C4 IiI
410
Page 117
----- - - -------------- - -
>4
PILI
cc I *' I
101 --
oo 2: -:
-- v ) -- I.... '.. 1-.-
,
-- IL I J --
.- . ,
it.J , -- -o -/ - - - - - - -
-. ~ ~ c loo 3
- .c ooooooaoc c:I ooooooooo oo ooo oo71 oo c3o o o In 17, '
-~4 % 4'
4..... .;
41.
r C Q- r:c:v. c c. .c
-- Q oo: o-0 0 G000 0o00 o0 O0 O 00000 oo C) 0 00 0 0 0 0 0- i,
I- " - . --
-- v' 0 -- w" 4)
So . .v
a~~- A.a o0o
m t -o r-IIn
- 1'1 oD-
-
-- , I I ----
i : ...... ' .-.- I
' /. _ I~ I I 414 . 1 --1 11 1
Page 118
r."
91 In 4) 1 1G 0 .. nI
I" O'
a. 0*
-- I I I -
V- .0 x I -w - - - --- - -t- na
.- Eni~j I -a-C M
.0 lii 0m ---- ---- I n.
.S-3 In3J In1-
w- -L..0 -- - --- I nn r '
I\ k-
-V 10 033 COT c !c -- o K o mI n IIn In In -- C t
I ~ ~ ~ ~ ~ ~ OC 0 0--- 0-- ' 0 (J U ta-a0 ac~~
-- 0Z I I4--000000 000 0 0 00 0 0 0 0 WCjCJOr a a,00 Q0
I~~1 1- 4c '.-
m -- o Mm 0mfu I I
I- L
v M- vg0 4 ) -1alll I 9L. 0, . I
2- -I.J - ----
-- 00 I I --.- ~~~0-------- --- 2 ~ a ~ -an co.--.~ ~ '~bae)C a: 3.- o-- 0a' o nma-~' i) J,
Page 119
t-~~~~- -. -A) L l
I La
.0 a
-C L a.j 1 0 1
a -- 00 0 0 0 0 r
a,* W-
- 0 --' a(DOJ00 a-
a0 a cm~ t 0 n IV
a a)
-- a a --- Mco 0000 0 0 O
L) -'Ca -
w: aLa 2: : >
e a q ea-- 1" aoa 0 000
0 0~~ 05 0C
Page 120
. - ..- - .-- -..-. - bs baja. A S
'.1 Xt~ -
PS .1--A.t-..5-..
~
5--'I.53g. J* -p5-?..
U S-S
'St
94
v 'yeN
S.
.5
p. ~
~at4
ci
-p. . S55*5
I..-
-p.
.5 -p..
-5
APPENDIX H'5.
2. S.
'S. *~
5-
'-S.?.
'5-
~55
'5 t'I.
5-p
5S'
-' -S ~ 5-
7 r
9-' 5,
a-
4-p.a-,'I'.
F.
j* C *.*
-~.t.. *r--J~'5 .55~ ~2~ J.- C
-C
**
Page 121
* x*%.% -.
I I I
* .J ..*.
I -.--.-.. ~ -
- - * ---I.1II
F I- o h 4.H
(1)L
~4~)p i ~--.<-.
cL.I I
i I
LJJL0~-4
S~ *
U. .~ ~~~1
L I
"p i I * '4............................................ L..-U ~ -.
___U)
U-V..
I I I
......................................... .\K I--
____ I tI..LLLLL! LLLLIJJ P~.d.
.LLLL. .LLLL. 4.1 14. UJ4... LLL.L J.A.LL. -.1 .LLL
-
I.-.
S13 ~
I
Page 122
%J;TED BIBLIOGRAPHY
Arti, M. A. "Solving the Staffing Problems in Hospitals."Sue r visoMana2enent, January 1 9 3 3.-
Barletta, J. M. "Using Projectional Analysis to reach YourStaffing Goals. MLO: Medical Laboratcry ObserverMarch 1984.
Bracken J. et al "A Strategy for Adaptive Staffing of Hospitalsunder Varying Environmental Conditions." Health CareManagement Review, Fall 1985 .
Cerha, D. A. "Blue Ribbon Panel on Sizing DOD Medical TreatmentFacilities." USAF Medical Ser vice Die st, Fall 1985.
Drandell, M. "A Composite Forecasting Methodology for ManpowerPlanning Utilizing Objective and Subjective Criteria."Academy of Management Journal, September 1975.
Ewing-Juul, K. et al. "Determining Staffing Requirements for aNew Facility." Innovative Ambulatory Care Systems ,American Hospital Association, 1985.
Fawcett, R. "Manpower Planning: Art or Science?" Nursing Mirror,January 2, 1985.
Fifield, Fred F. "Manpower Value Planning." Personnel Journal,April 1974.
Finnigan, S. A. "Alternative Staffing Methods and Cost-Effectiveness." National League of Nursin-Publications, 1983.
Herzog, T. P. "Flexible Staffing Matches Staff to Patient andHospital Needs." Hospital Manager, July-August 1985 .
Hale, T.C. "1987 Completion Date Eyed for Medical CenterProject." Construction Digest, 5 May 1935. '-,
Hanson, R. L. "The Synergy of Fiscal Systems and StaffingRequirements. " Texas Hospitals, March 1984 .
Joint Commission on Accreditation of Hospitals.Accreditation Manual for Hospitals, 1986. Chicago:Joint Commission on Accreditation of Hospitals, 1935.
Lyons, T.P. "Personnel Policy and Manpower Planning in Barking."Long Range Plannin, October 19T9 .
105
. -.
.. . . . .. . . . . .......
Page 123
4"
Mackley, B. "Manpower Planning. The Misappliance of Scierce."Nursinj Times, October 3-9, 1934.
Nutt, P. C. "Decision-Modeling Methods Used to Design DecisionSupport Systems for Staffing." Medical Care,November 1984. ---.
Pakchar, P. "Effective Manpower Planning." Personnel Journal,October 1983.
Shaw, I. C. "Staffing A New Hospital." Michigan Medicine,Sep'tember 1983 .
Sherlock, Smith and Adams, Inc. Economic Analysis USAF MedicalCenter Wright-Patterson AF, Ohio. Atlanta: Sherlock,Smith and Adamss,,I-c., 1931.
Torrez, M. R. Systems Approach to Staffing." Nursing .anaement,May 1983.
Tufte, Lt Col R. W. et al. "PRISM: Provider RequirementsIntegrated Specialty Model." USAF Medical ServiceDi&est, Winter 1984 .
"VA Develops Guidelines for Appropriate Staffing." US Medicine, ,.-'-..April 15, 1984.
US Air Force. Air Force Logistics Command Re&lation 26-2 .Wright-Patterson Air Force Base, Ohio: Headquarters AirForce Logistics Command, 1985.
US Air Force. Air Force Regulation 26-1, Manpower Policiesand Procedures. Washington D.C.: HeadquartersU. S. Air Force, 1985.
US Air Force. Air Force Regulation 168-4_ Administration ofMedical Activities. Washington D.C.: HeadquartersU. S. Air Force, 1985.
US Air Force. Directorate of Health Services Management,* Office of the SugeoL_ HQ Air Force Loi sties Cmmand-.
Wrjt-Patterson Air Force Base. Letter to USAF MedicalCenter,_Wrig t-Patterson Concerning the 6th AnnualPRISM I and PRISM III. Wright-Patterson Air Force Base, ' 'Ohio, I April 1986.
US Air Force. FY35-39 Medical Program 0 bjective Memorandum.USAF Medical Center, Wright-Patterson,Wright-Patterson Air Force Base, Ohio, October 1982:
1-36.
ij 106
.
%-
m
Page 124
F -7 7 -.
US Air Force. Man aement Summary.USAF Medical Center, Wright-Patterson,Wright-Patterson AFB, Ohio, 3rd uarter FY 1931.
US Air Force. The Big Picture Management Summary. ,.- yUSAF Medical Center, Wright-Patterson,Wright-Patterson Air Force Base, Ohio, 30 September 1932.
US Air Force. The Big Picture Management Summary.USAF Medical Center, Wright-Patterson,Wright-Patterson AFB, Ohio, 30 September 19a3.
US Air Force. The Big Picture Management Summary.USAF Medical Center, Wright-Patterson,Wright-Patterson AFB, Ohio, 30 September 1934.
US Air Force. The Big Picture Management Sumar[.USAF Medical Center, Wright-Patterson,Wright-Patterson AFB, Ohio, 30 September 1935.
US Air Force. Medical Expense and Performance Report,Salary Rank List. USAF Medical Center,Wright-Patterson, Wright-Patterson AFB, Ohio,
21 May 1986.
US Air Force. Unit Str ength-Sum Report.USAF Medical Center, Wright-Patterson,Wright-Patterson AFB, Ohio, 18 July 1986.
US Air Force. Resource Management Office UF Medical Cen ter.Wrijht-Patterson. Letter to Headquarters Air FcrceLogistics Command Surgeon's Office, Wright-Pattersn AirForce Base Concernin F 1936 Man er Program.Wright-Patterson AFB, Ohio, 11 December 19 3.
Wilhelm, Colonel Bruce D. USAF Medical Center, Wright-Patterson,Wright-Patterson Air Force Base, Ohio, Interview,6 February 1986.
Development of Desi _n and Operational Guidelines for OptimnumManpower in HMO/PGP Settin'-----------------_of Staffing Models, May 1917.
107
-.......... ,...... .
Page 125
ABSTRACT
All aspects of the health care industry are feeling the
effects of competition for limited dollars needed to deliver
quality care. The Air Force health care delivery system, just as
the private sector, is finding itself challenged to deliver
quality health care with the minimum human resources necessary to
deliver such services.
A study was conducted to determine the future staffing
requirements for the USAF Medical Center, Wright-Pattersor, once
a $113 million-plus medical military constructicr project (MCP)
was completed. The MCP was started in 1982, yet no significant
manpower planning actions had taken place to ascertain the human
resource requirements for operating the Medical Center once
construction was completed. The MCP represented a meaningful
enhancement to this tertiary care facility by renovating,
altering, and expanding the physical structure and associated
technology appropriate for the comprehensive health care
delivered in today's military medical facilities.
In view of DOD, congressional, and local manageme t .r,,
concerns for medical facility staffing, this study was
commissioned to ascertain what charges, if any, were needed to
the staff at Wright-Patterson. Pr esent and future manp¢ower
methodologies for the USAF Medical Service did not address the
growth of manpower requirements driven by major ccr.structiorn
projects. Consequently, a needs assessment survey was conducted
108
1 S -: '
.- - - - - - -- - - - - -. *..*.*p..................
.- .- . i~ d mii abm~. am.~rn m~im~am b~ %mhm
Page 126
with the departments and directorates operating at the USAF
Medical Center, Wright-Patterson. This survey combined the I
validity of historical manpower standards with the professional
judment of the local staff in developing future staffing". ,
requirements. This study determined that the Wright-Patterson
Medical Center's manpower requirements would grow by 207
positions in 1983, reaching a total requirement of 1652
positions. _
1 09
I1 I i
Page 127
A
17-yin
V
'-'-4
p. *p~.v ~'
~%.q
,- ,~s% ~.. '.~- .p.
________________________________________ .. h.k~ ~ ~ ~






























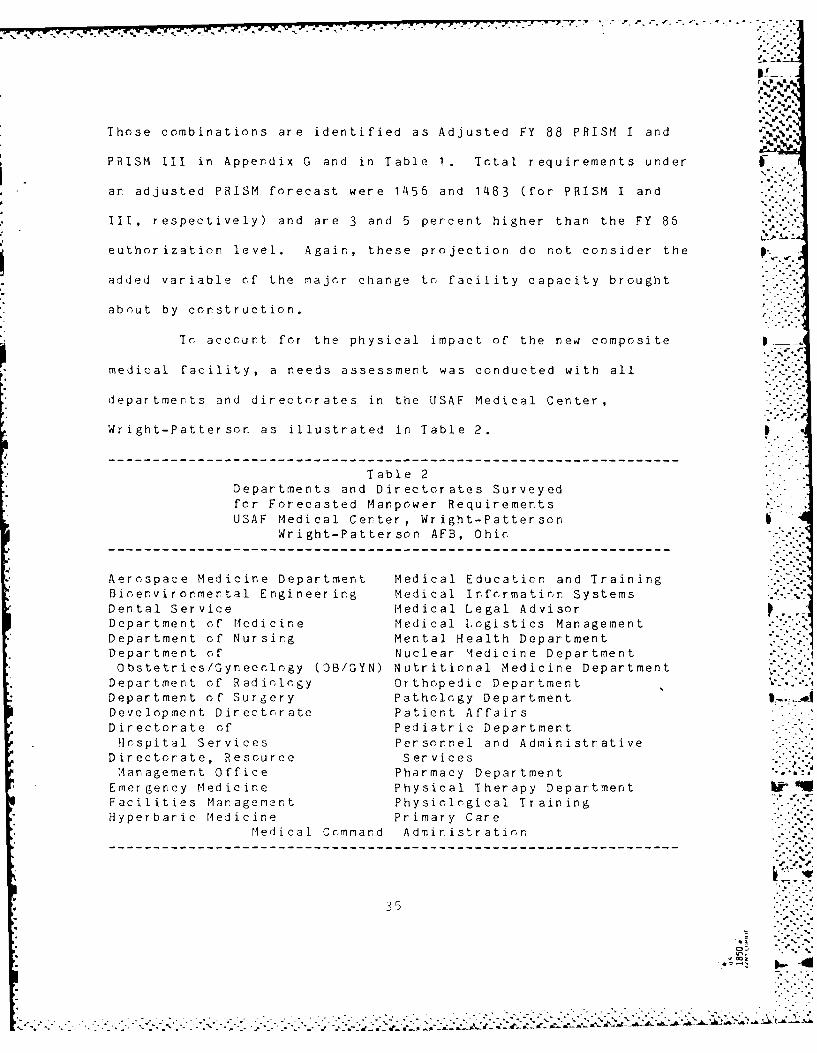





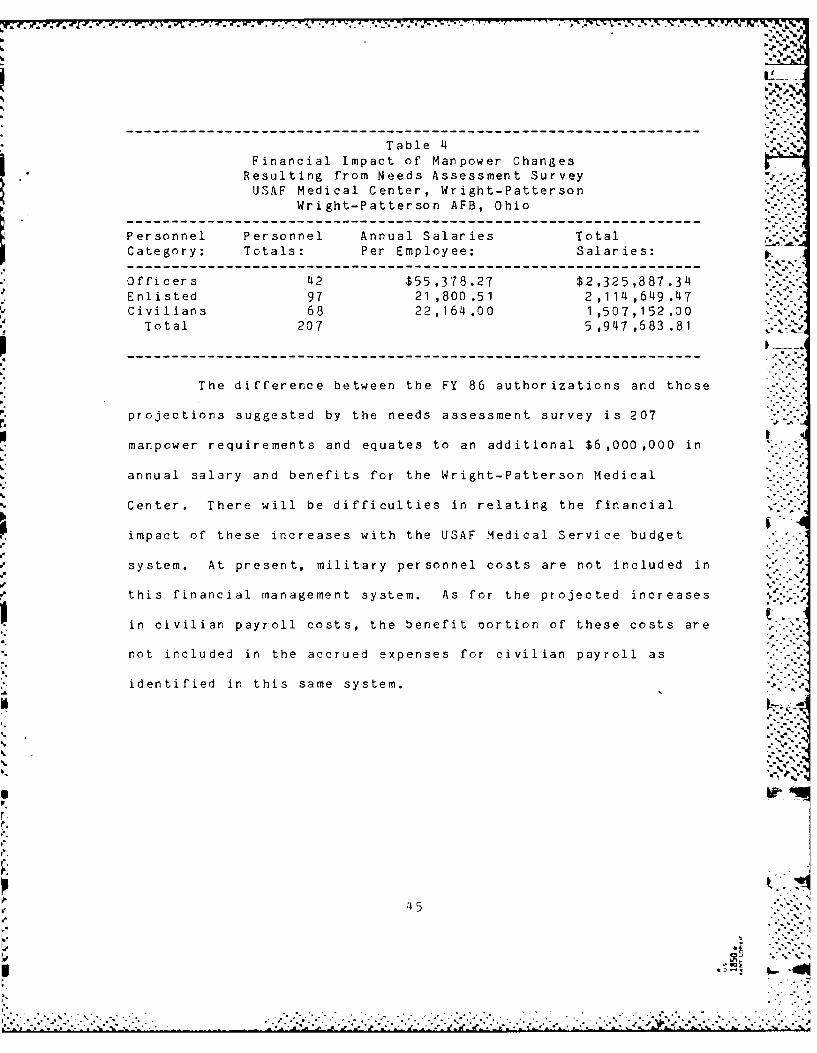


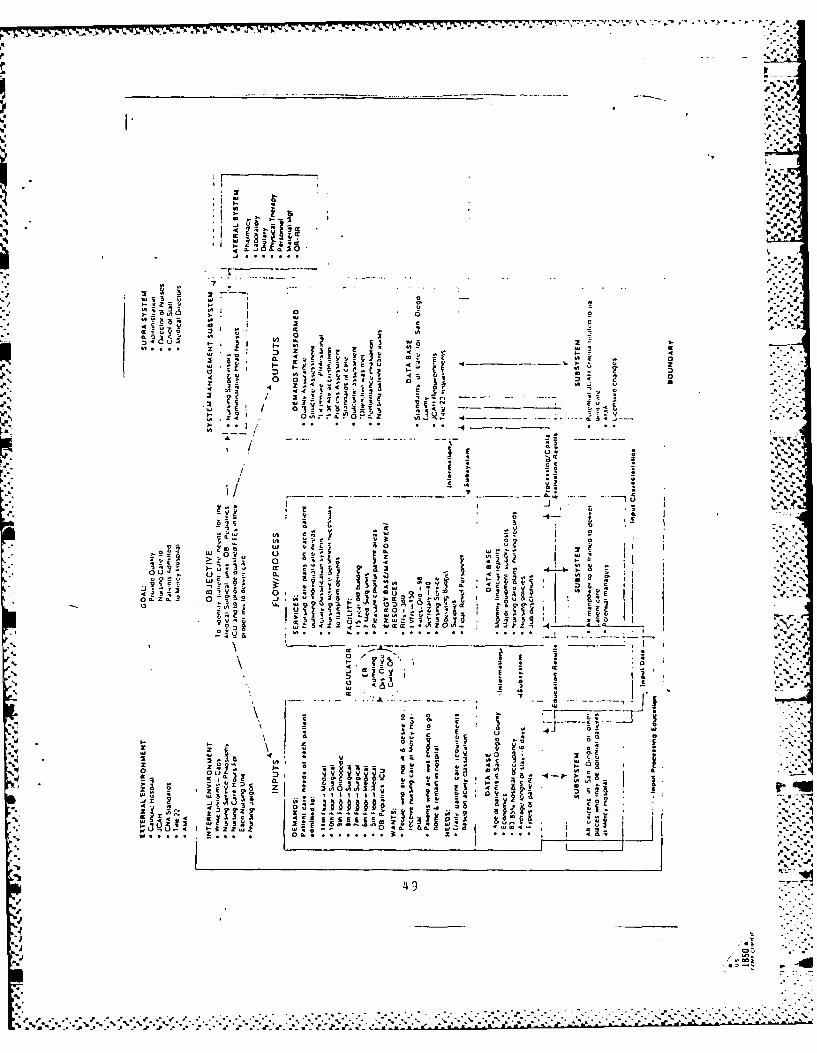



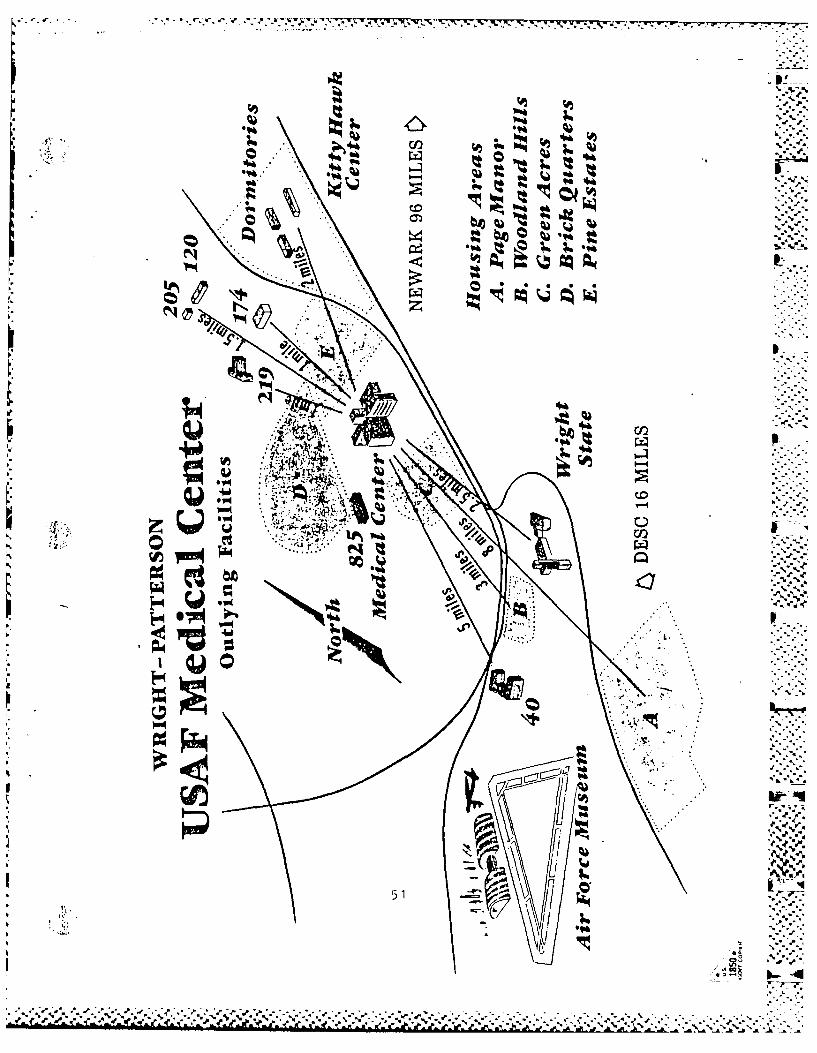

















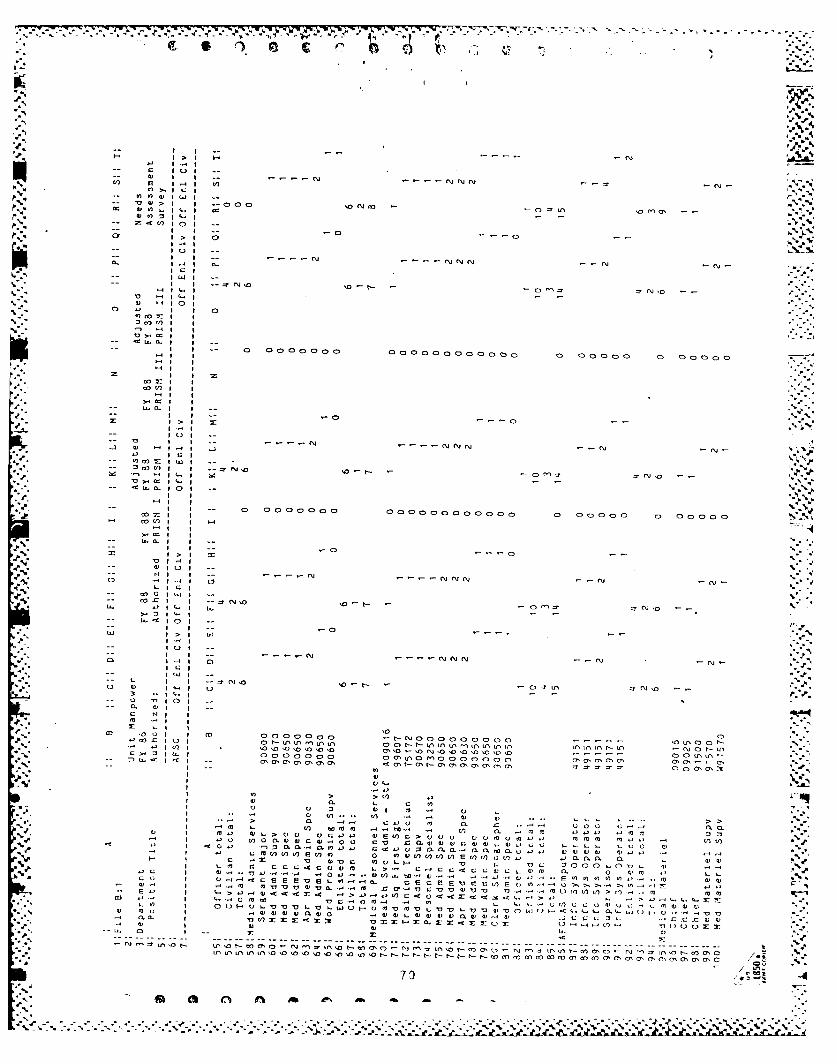



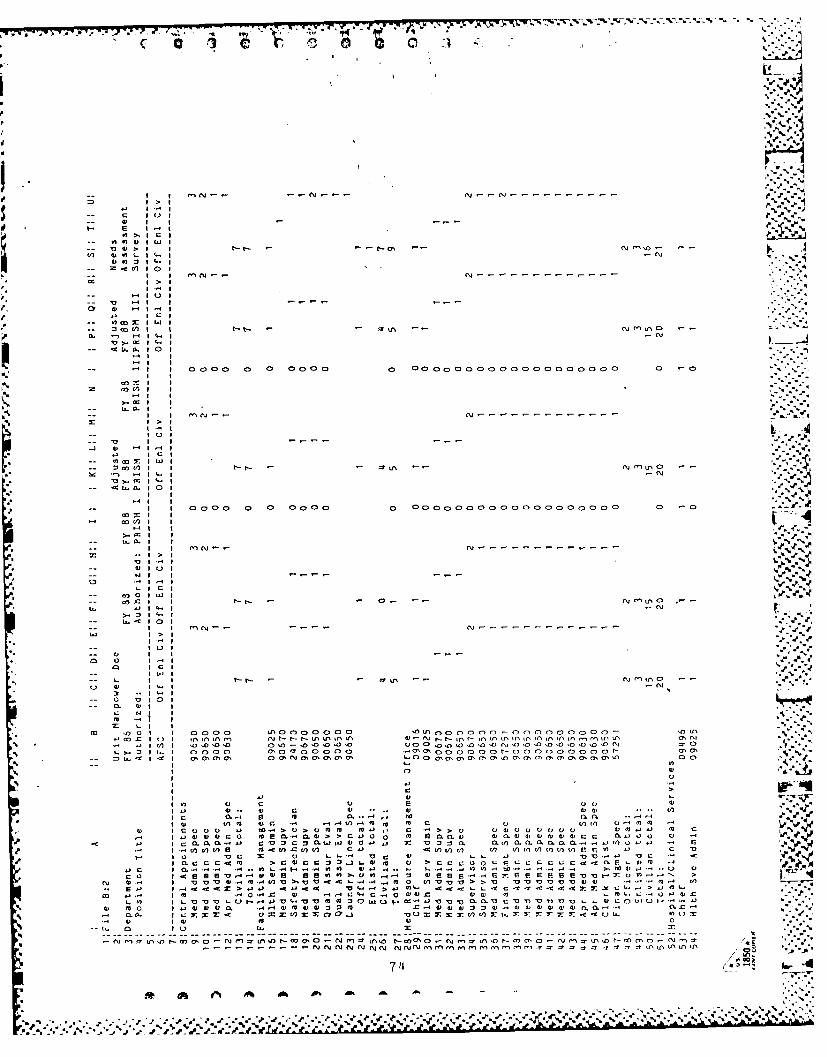

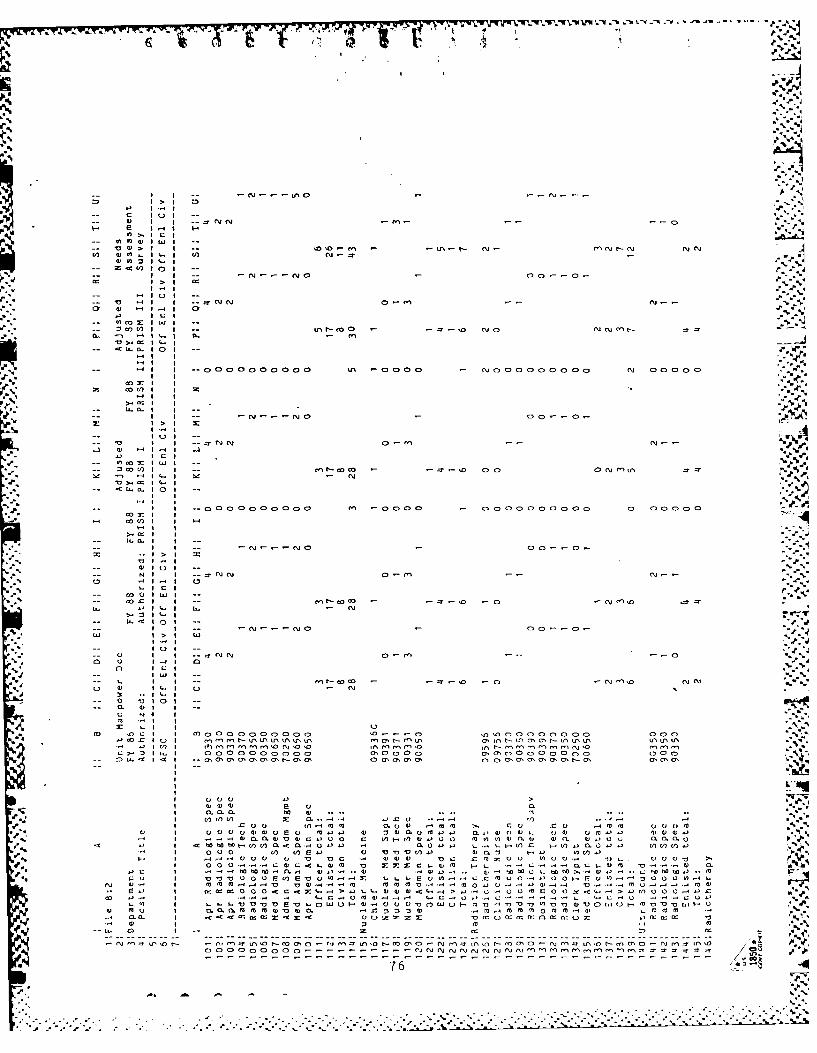
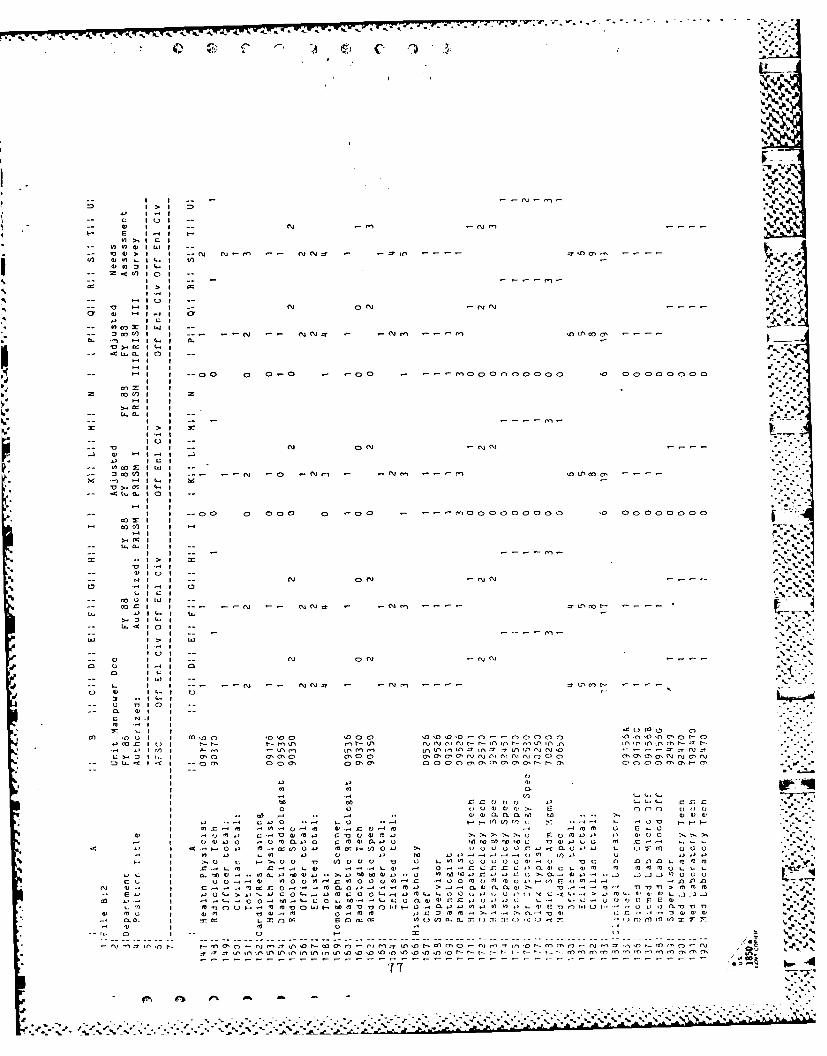
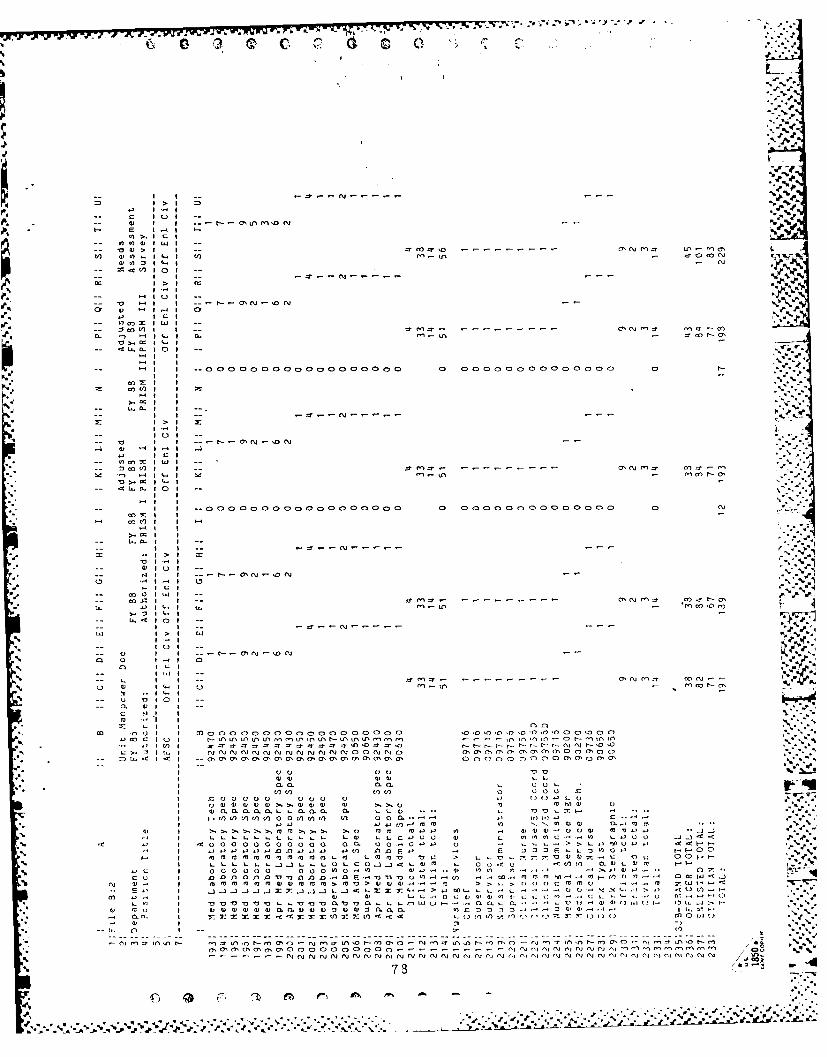




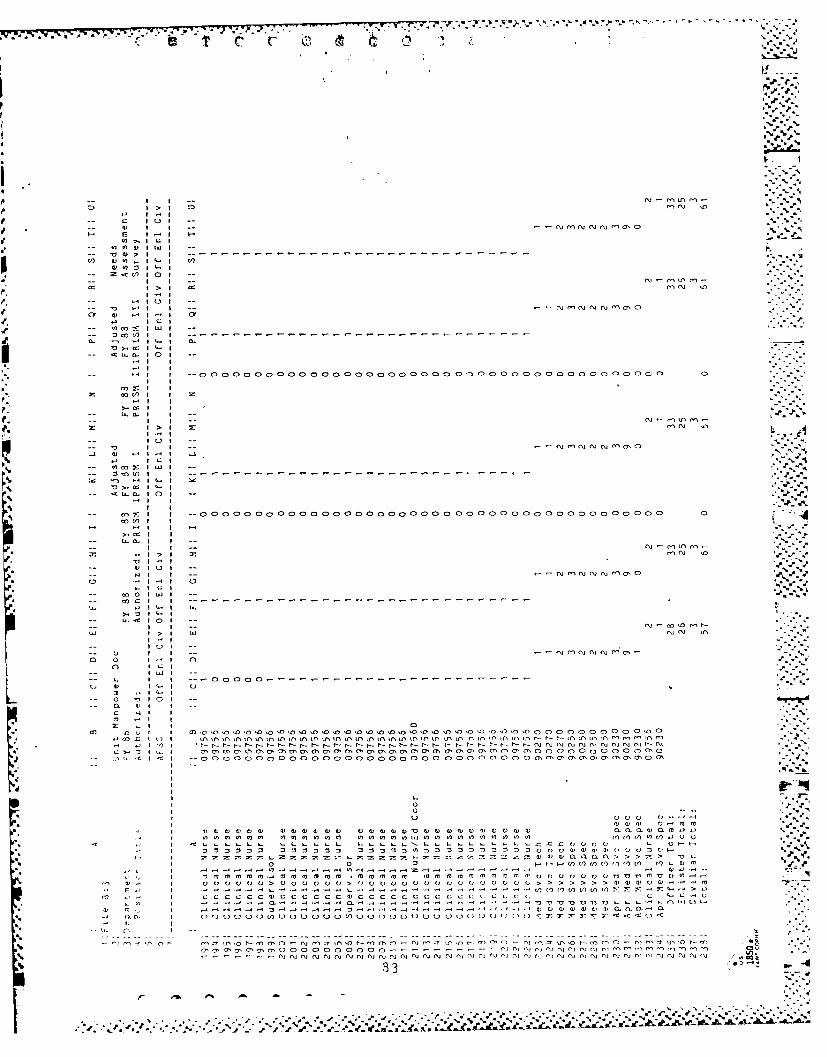



















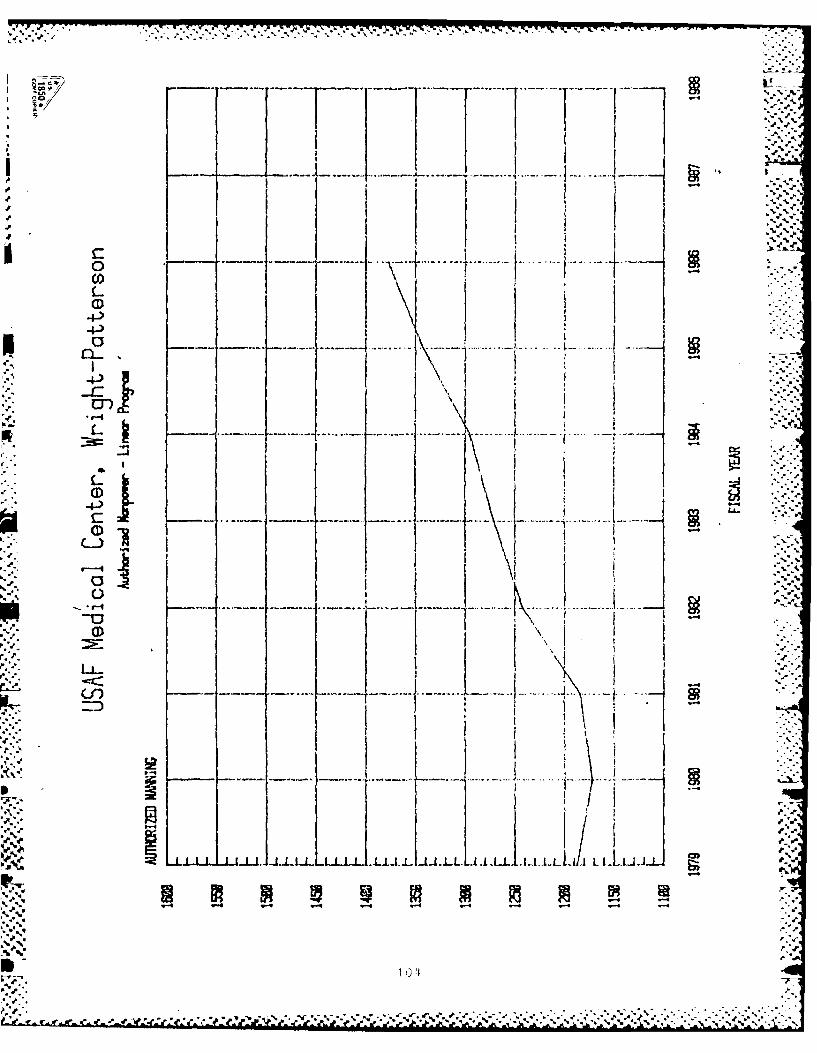



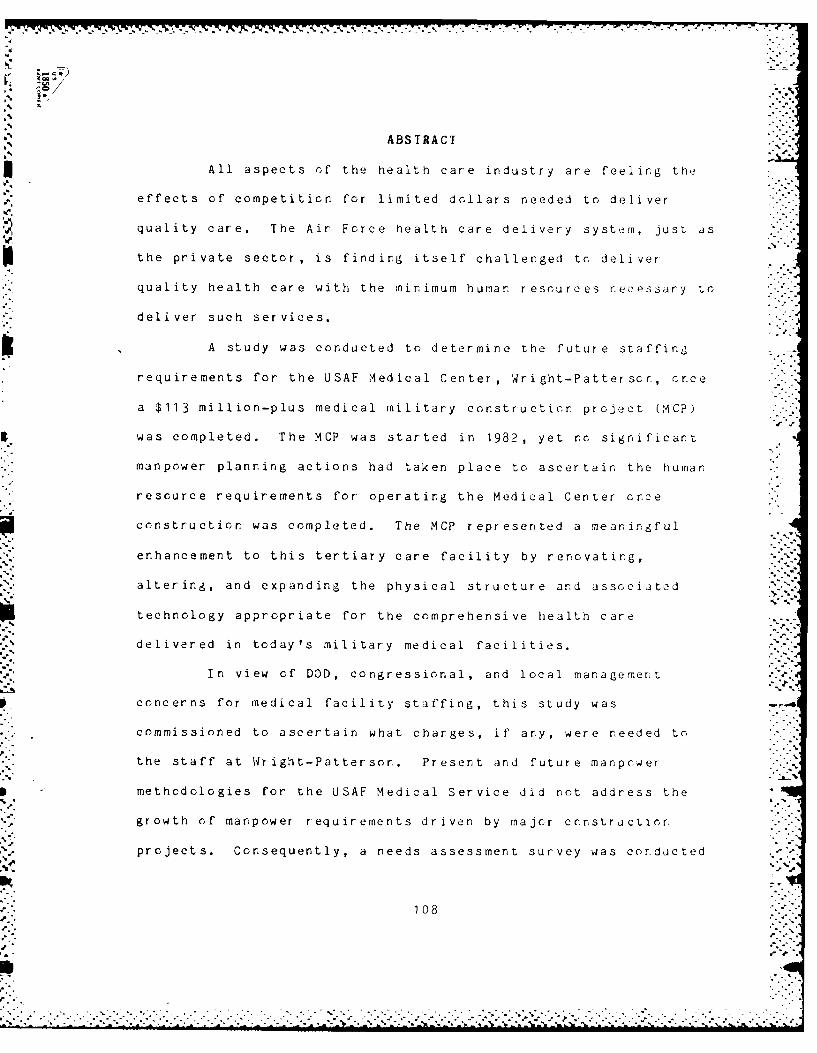
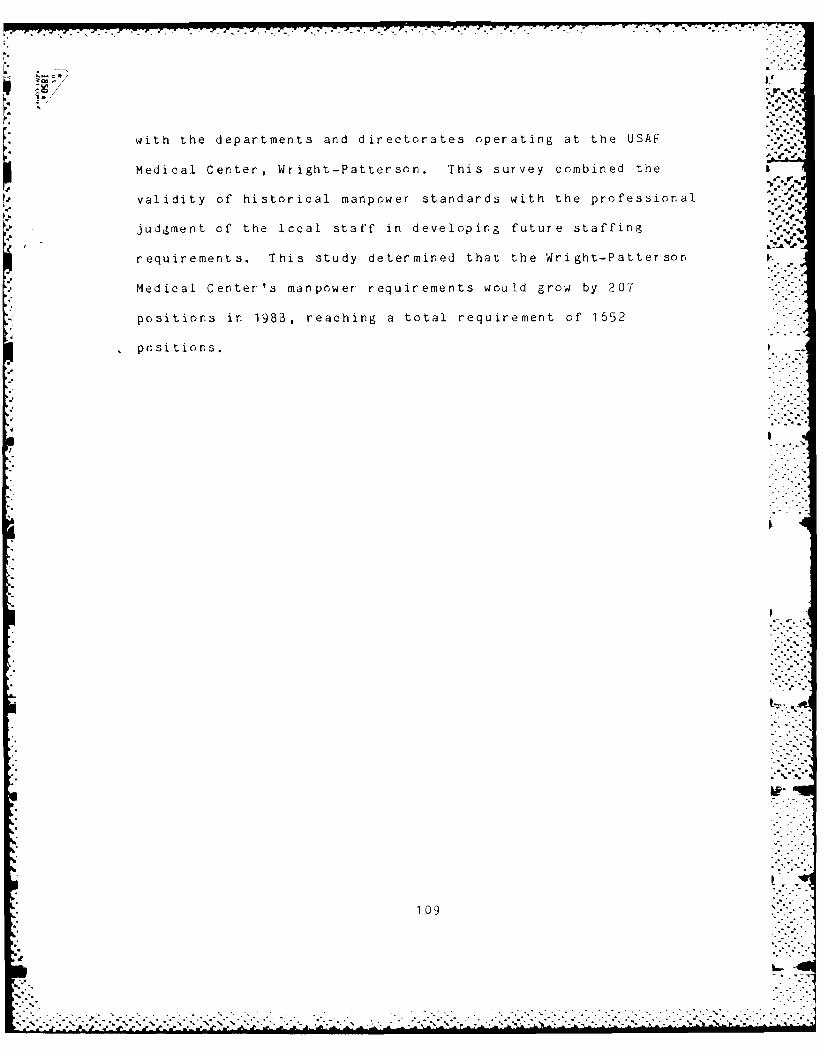





![· Web viewScience Batch F-3. Word: Spinal Column. العمود الفقري. Word ID: 601968. Strand: 3. Topic: [Human Body] [جسم الإنسان] Used: [SF3][SG3][SH3] Box 1:](https://static.documents.pub/doc/80x56/60f0b2351c8f1450e70bce5b/web-view-science-batch-f-3-word-spinal-column-word.jpg)








![€¦ · Web viewWord: Artery. شريان. Word ID: 602011. Strand: 3. Topic: [Circulatory System] [الجهاز الدوري] Used: [SF3][SG3][SH3] Box 1: Artery. The doctor helped](https://static.documents.pub/doc/80x56/61143d1c0832395e23220f06/web-view-word-artery-word-id-602011-strand-3-topic-circulatory.jpg)



