110 Lecture 5: Immune response and inflammation Immunity The term immunity refers to the resistance exhibited by the host towards infection caused by micro organisms and their products(toxins) as well as any abnormal cells that might arise within the body itself. This is based on the property of self and non self recognition. That means immunity is carried out by the process of recognition and getting rid of non self or materials that enter the body. Immune response is the reaction of the body against any foreign antigen. 1 st line of Defense The first line of defense against invading microorganisms involves the physical barriers presented by the skin on the body surfaces and the mucous membranes that protect openings into the body. These mucous membranes are covered by secretions such as stick mucus that can trap invading organisms. Digestive enzymes such as lysozymes are often found within mucous membrane secretions and provide a chemical barrier to infections. 2 nd line of Defense Organisms that are able to penetrate this first line of defense must now face : circulating Phagocytic white blood cells, antimicrobial substances and natural killer cells , • all of which attack invading organisms in a nonspecific manner. • In addition, the entry of these foreign organisms into the body will trigger a significant inflammatory response and possibly fever, both of which are also protective. 3 rd line of Defense In addition to the above nonspecific defense mechanisms, specialized cells called lymphocytes and antimicrobial proteins called antibodies can attack foreign organisms in a highly specific manner.
Transcript
110
Lecture 5: Immune response and inflammation
Immunity
The term immunity refers to the resistance exhibited by the host towards infection caused by micro organisms and their products(toxins) as well as any abnormal cells that might arise within the body itself.
This is based on the property of self and non self recognition. That means immunity is carried out by the process of recognition and getting rid of non self or materials that enter the body.
Immune response is the reaction of the body against any foreign antigen.
1st line of Defense
The first line of defense against invading microorganisms involves the physical barriers presented by the skin on the body surfaces and the mucous membranes that protect openings into the body.
These mucous membranes are covered by secretions such as stick mucus that can trap invading organisms.
Digestive enzymes such as lysozymes are often found within mucous membrane secretions and provide a chemical barrier to infections.
2nd line of Defense
Organisms that are able to penetrate this first line of defense must now face : circulating Phagocytic white blood cells,
antimicrobial substances and
natural killer cells ,
• all of which attack invading organisms in a nonspecific manner.
• In addition, the entry of these foreign organisms into the body will trigger a significant inflammatory response and possibly fever, both of which are also protective.
3rd line of Defense
In addition to the above nonspecific defense mechanisms, specialized cells called lymphocytes and antimicrobial proteins called antibodies can attack foreign organisms in a highly specific manner.
111
Summary: Immune System Defense against Infection
1. Physical and Chemical Barriers (Innate Immunity)
2. Nonspecific Resistance (Innate Immunity)
3. Specific Resistance (Acquired Immunity)
112
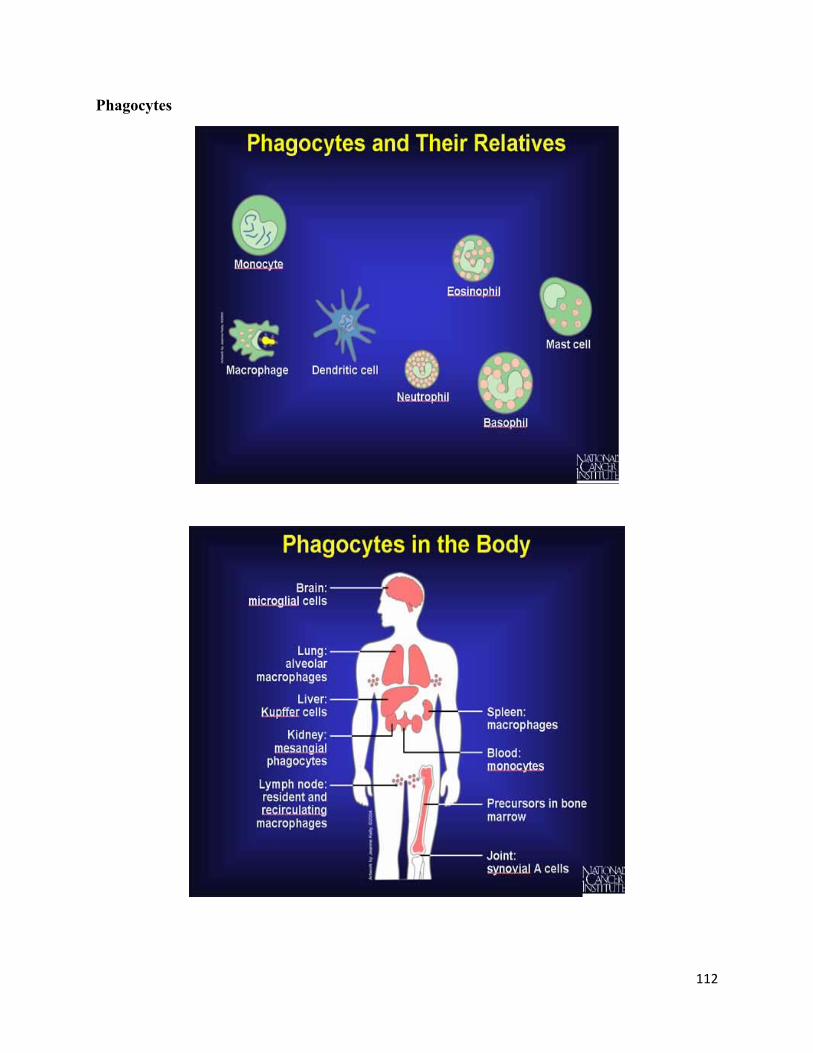
Phagocytes
113
Key tasks of the immune system
1) Recognition:
Discrimination between Ag from self and nonself is fundamental for function and evolution of immune system .
Self fanaticism
Reacting against foreign Ag simply because it is foreign
Not based on beneficial or harmful effects of Ag
2) Effector functions – contain the infection and eliminate it completely– Antibodies– Cytotoxic lymphocytes
3) Regulation – Homeostasis or equilibrium must be established by shutting down the system when it's no longer needed
Ag ➔ immune response ➔ proliferation of specific molecules that will not be useful after their job is finished
Infection ➔ response ➔ cure.
Deregulation of the immune system has severe consequences
Immune response to self Ag ➔ Autoimmunity
4) Memory – generate an immediate and strong secondary response to protect the individual against recurring disease due to the same pathogen
Lymphatic System
A complex network of lymphoid organs, lymph nodes, lymph ducts, lymphatic tissues, lymph capillaries and lymph vessels that produce and transport lymph fluid from tissues to the circulatory system
The lymphatic system has three interrelated functions: 1. fight infection (production of immune cells such as lymphocytes)
2. carry lipids absorbed from the GI tract to the bloodstream
3. return fluids and plasma proteins that escaped from the bloodstream back to the bloodstream
114
Lymphoid Organs & Tissues
Mature B and T lymphocytes exit the primary lymphoid organs and are transported via the bloodstream to the secondary lymphoid organs, where they become activated by contact with foreign materials (antigens).
Peyer’s patches are mucosa-associated lymphoid tissues of the small intestine
Types of Immunity
Immune system responses to pathogens have been classified as either Innate (non-specific) or Adaptive (specific)
Innate/Natural : (nonspecific) defenses Non-specific cellular, molecular, and physical elements to prevent or neutralize
infection
Immediate response
No memory
Adaptive/Acquired : (specific) defenses Specific response to epitope on Ag
Slow (3-5 day) response
Memory of prior exposure
115
116
Cells of the Immune System
Stem Cells develop into myeloid progenitor cells while others become lymphoid progenitor cells.
The myeloid progenitors develop into the cells that respond early and nonspecifically to infection.
Monocytes turn into Macrophages in body tissues and gobble up foreign invaders.
Neutrophils engulf bacteria upon contact and send out warning signals.
Granule-containing cells such as eosinophils attack parasites, while basophils release granules containing histamine and other allergy-related molecules.
Lymphoid precursors develop into lymphocytes. Lymphocytes respond later in infection. They mount a more specifically tailored attack after antigen-presenting cells such as dendritic cells (or macrophages) display their catch in the form of antigen fragments.
The B cell turns into a plasma cell that produces and releases into the bloodstream thousands of specific antibodies.
The T cells coordinate the entire immune response and eliminate the viruses hiding in infected cells.
117
Summary: Cells of the Immune System
Lymphocytes o B cells
o T helper cells (TH)
o Cytotoxic T cells (Tc)
o Natural Killer (NK) cells
Megakaryocytes o Platelets
PMNs o Neutrophil
o Basophil & Mast cells
o Eosinophil
Monocytes o Dendritic cells
o Macrophages
Polymorphonuclear leukocytes (PMNs)
The granulocytes are called as Polymorphonuclear leukocytes (PMNs, PML) because of the shape of the nucleus, which is usually lobed into three segments.
PMNs include neutrophils, basophils and eosinophils.
The term polymorphonuclear leukocyte often refers specifically to neutrophil granulocytes (the most abundant of the granulocytes)
118
Components of the immune system
Antigens
Major histocompatibility complex (MHC)
MHC I
MHC II
Monocytes and macrophages
Lymphocytes
T lymphocytes (T cells)
Helper T cells
Cytotoxic T cells
B lymphocytes (B cells)
Antibodies
Natural killer cells
Cytokines
Complement proteins
119
Antigens
An Antigen is any substance that can induce an immune response, usually foreign material but may be our own tissues. ( Antibody Generators)
Specific molecules on bacteria, viruses, pollen, plants, insect venom and transplant tissue can all act as antigens.
The specific region of the antigen molecule that initiates the immune response is called the epitope.
Most powerful antigens are large and complex macromolecules and are most often proteins and polysaccharides.
haptens are small-molecular-weight molecules such as drugs, that aren't antigenic by themselves , that can only trigger an immune response if bound to larger antigenic macromolecules called carriers
Antigen & Self antigen
Antigen was originally a substance(usually proteins or polysaccharides) that binds specifically to the antibody, but the term now also refers to any molecule or molecular fragment that can be recognized by highly variable antigen receptors (B-cell receptor or T-cell receptor) of the adaptive immune system.
Self antigens are antigens present on SELF tissue that would normally not provoke an immune response unless in a diseased state.
A foreign antigen is an antigen that is present on nonself /foreign tissue. Examples of foreign antigens are components of microorganisms, foreign proteins and toxins. Usually these foreign antigens will provoke antibody production by the body because they are recognized as nonself.
Autoimmune diseases happen when the body attacks its self antigens with antibodies made against it.
120
An example of self antigen is the Rhesus antigen on red blood cells. People who are Rhesus positive will not produce anti-rhesus antibodies because the rhesus antigen is a self antigen which is present on their red blood cells.
A Rhesus negative person, their red blood cells do not have rhesus antigens, and therefore when they receive transfusions of Rhesus +ve blood, their immune systems recognizes the rhesus antigen as foreign and attacks the foreign red blood cells.
Major histocompatibility complex (MHC)
A group of unique glycoproteins found on the surface of cells.
MHC is a collection of human genes on chromosome 6 that encode proteins that function in cells to transport antigens from within the cell to the cell surface.
Each individual possesses cell surface antigens that are unique to that individual.
These antigens, the MHC proteins, serve as a sort of cellular fingerprint.
MHC was originally called human leukocyte antigen (HLA) because it was first identified on the surface of human white blood cell (leukocytes).
Two distinct types of MHC are found on cells: MHC I and MHC II.
MHC proteins have two functions:
(1) they present self-antigens to T cells, and
(2) they bind foreign antigens and present these to T cells.
T-cells may recognize this complex using their T-cell receptor (TCR).
There are two groups of MHC proteins:
MHC I and MHC II.
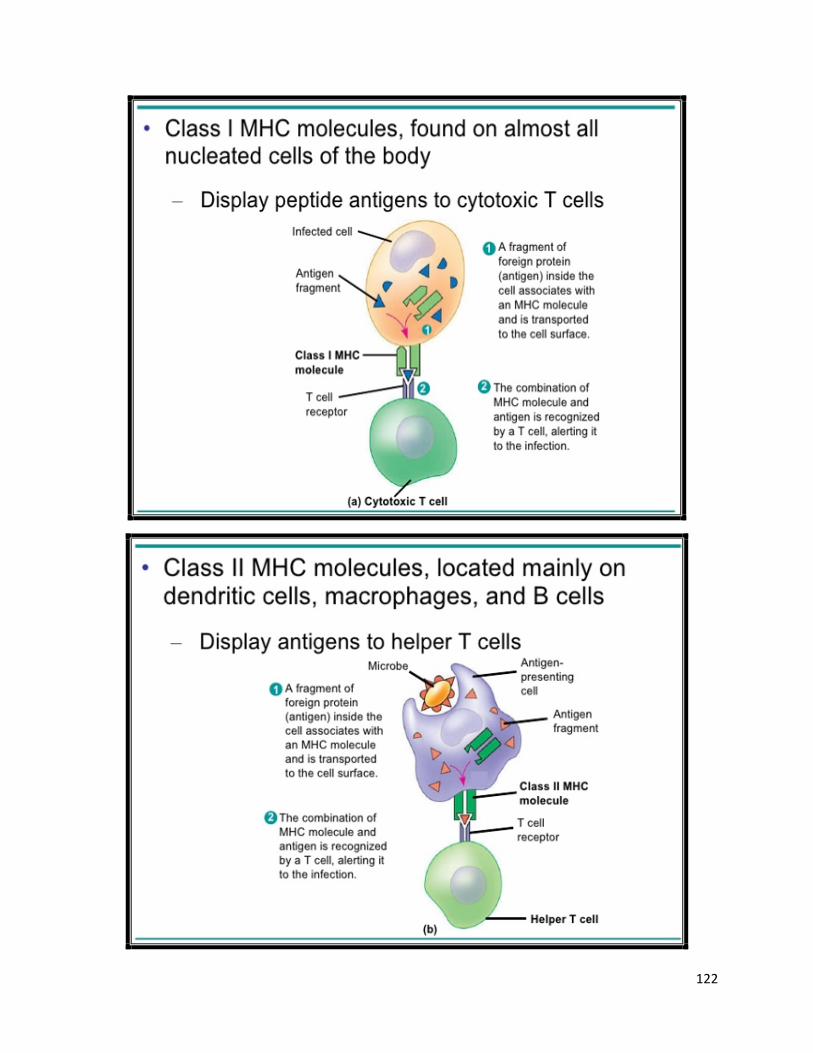
The MHC I proteins are found on nearly all cells of the body except the RBC
The MHC II proteins are found only on the surface of macrophages and B cells.
The MHC I Serve as:
markers of “self” for the immune system. Identify cells as being normal and belonging in the body.
Foreign organisms like viruses will often express some of their foreign antigens on the MHC I of the cells they infect. This change in MHC I signals cells of the immune system that a particular cell has been infected and is no longer “normal.”
The MHC II Can be used by immune cells to present foreign antigens to other immune cells.
121
MHC I & MHC II
The MHC I molecules bind and present antigens only to cytotoxic T cells.
The MHC II molecules bind and present antigens only to helper T cells (both Th1 and Th2 types).
An antigen-presenting cell (APC) or accessory cell is a Cell that displays foreign antigen complex with (MHC) on its surface.
MHC molecules is the general name given to the highly polymorphic glycoproteins encoded by MHC class I and MHC class II genes, which are involved in the presentation of peptide antigens to T cells. They are also known as histocompatibility antigens.
122
123
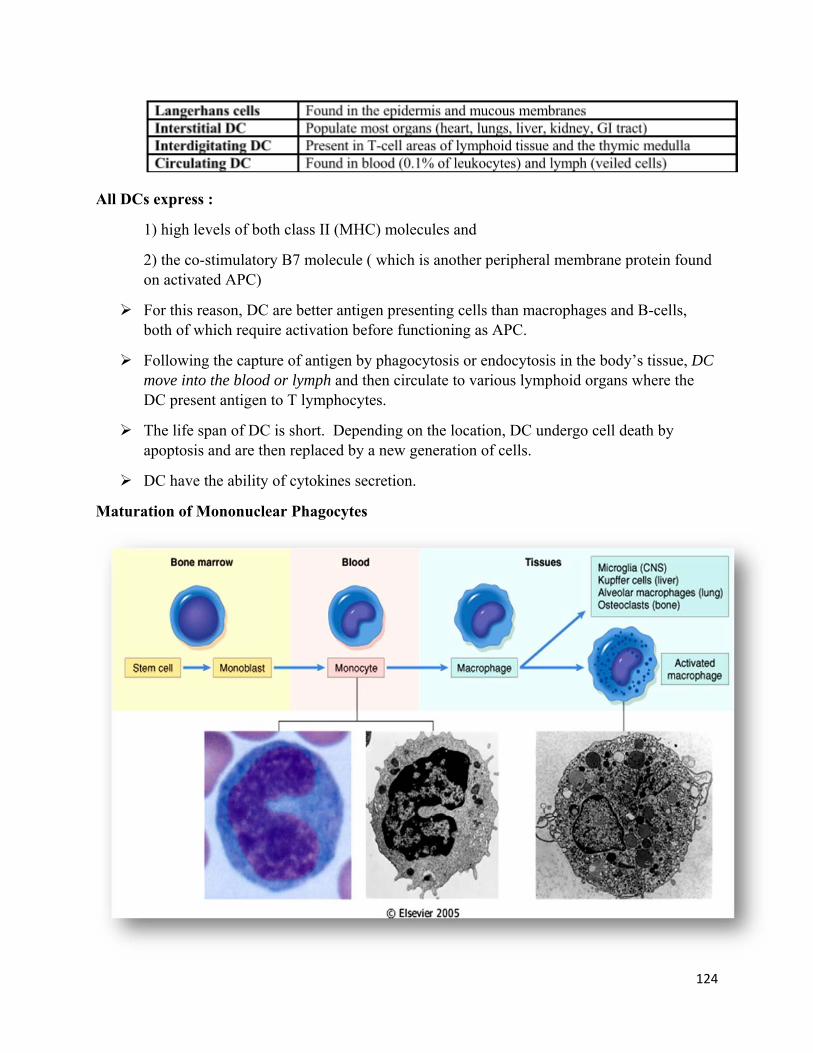
Monocytes
Monocytes are produced in the bone marrow , circulate in the blood and enter injured tissue across capillary membranes that become permeable as part of the inflammatory reaction.
Monocytes are not phagocytic, but after several hours in the tissue area, they change shape and mature into macrophages.
Macrophages
Macrophages are large cells capable of ingesting large quantities of cell debris and bacteria. Macrophages can phagocytize lysed red blood cells and other white blood cells.
Some macrophage cells colonize tissues such as skin, lymph nodes, and lungs for months or years. These cells are readily available to scavenge microorganisms that may enter the body through those routes.
There are different names for the Macrophages that have immigrated to the tissues: such as the liver sinuses (Kupffer cells), pulmonary alveoli, splenic sinuses, peritoneal lining, lymph nodes, skin (Langerhans cells), joints (synovial A cells), brain (microglia), and epithelium (e.g., renal glomeruli).
When macrophages engulf a foreign organism or particle, they take the antigenic portion of what they have digested and present it on their own cell surface using their MHC II. Macrophages that exhibit foreign antigens on the MHC II are called antigen-presenting cells (APC).
The antigen presented on the surface of the macrophages may be recognized by specific lymphocytes called helper T cells that, in turn, will activate other lymphocytes to attack and destroy any foreign organisms displaying that particular antigen.
Macrophages also produce cytokines such as interleukin-1 (IL-1) that enhance the inflammatory reaction.
The monocyte-macrophage cell system is called the mononuclear phagocytotic system (MPS) or the reticuloendothelial system (RES)
Circulating monocytes account for approximately 3 to 7% of white blood cells in adults.
Macrophages can recognize relatively nonspecific carbohydrate components on the surface of bacteria and thereupon phagocytize and digest them.
The three major type of antigen presenting cells (APC) 1. Macrophages
2. B Lymphocyte
3. Dendritic cells (DCs) are: stellate or tree-like cells (Greek, dendron, tree) that are found in lymphoid organs, and at the interfaces between our bodies and the environment.
124
All DCs express :
1) high levels of both class II (MHC) molecules and
2) the co-stimulatory B7 molecule ( which is another peripheral membrane protein found on activated APC)
For this reason, DC are better antigen presenting cells than macrophages and B-cells, both of which require activation before functioning as APC.
Following the capture of antigen by phagocytosis or endocytosis in the body’s tissue, DC move into the blood or lymph and then circulate to various lymphoid organs where the DC present antigen to T lymphocytes.
The life span of DC is short. Depending on the location, DC undergo cell death by apoptosis and are then replaced by a new generation of cells.
DC have the ability of cytokines secretion.
Maturation of Mononuclear Phagocytes
125
Lymphocytes
Lymphocytes are produced in the bone marrow and mature there or in other lymphoid tissues.
Make up 20 to 25% of all leukocytes.
Lymphocytes include the B and T lymphocytes;
T-cells can be killer, helper, or suppressor T-cells.
Natural killer (NK) cells destroy the invading cell;
Helper cells help B-cells secrete immunoglobulin;
Suppressor cells reduce AMI (Antibody-mediated immunity or humoral immunity)
B lymphocytes
B lymphocytes (B cells) mature in the bone marrow.
After maturation, a B cell circulates in the blood in an inactive state.
When B lymphocytes encounter a specific foreign antigen, to which it has been genetically programmed during fetal development to respond.
They bind to it and, under the influence of cytokines released by helper T cells, mature into plasma cells that produce antibodies.
A small subpopulation of activated B lymphocytes will differentiate
into memory B cells that persist in the body for long periods of time
and are capable of recognizing and rapidly responding to the same antigen if it encounters it at a later date.
B lymphocytes comprise the humoral immune system, meaning that they circulate in the blood (the humor).
Humoral Response (of the “Humors”) B Cells – mature in the bone marrow Migrate to the lymphatic system Activated by antigen Release antibodies into the blood while remaining in the lymph system Antibodies cover and coat pathogens, rendering them useless (مما يجعلها عديمة الفائدة) and
targeted for destruction. HUMORAL RESPONSE = B CELLS MAKE ANTIBODIES•
126
Memory B Cells
Some B lymphocytes do not become antibody-secreting plasma cells after antigenic stimulation, but rather become memory cells.
Memory cells circulate indefinitely in the blood and become active immediately upon repeat exposure to the antigen.
The first time a B lymphocyte is exposed to its antigen (the primary exposure), production of antibodies against the antigen can take 2 weeks to more than 1 year, although normally antibodies to an antigen are detectable in the blood within 3 to 6 months.
Because of memory cells, the next time the antigen is encountered, the antibody response occurs almost immediately.
T lymphocytes
T lymphocytes comprise the cellular immune system.
T cell produced in the bone marrow but mature in the thymus gland.
In the thymus the T cells develop surface receptors called T-cell receptors where they become ‘programmed’ for the antigen of their specific enemy.
Like a B cell, the mature T cell stays inactive until it encounters the specific antigen to which it has been programmed.
Recent evidence suggests that, despite the partial degeneration of the thymus that occurs at puberty, T cells continue to develop in the thymus throughout life.
Two distinct subsets of T lymphocytes are present: helper T cells and cytotoxic T cells.
127
Cell-Mediated Response:
T-Cells are made in the bone marrow, migrate to the thymus for maturation T-Cells remain in the lymph system waiting to be activated by an antigen. T-Cells respond to antigen when they bond to specific antigen called MHC proteins
(major histocompatibility complex proteins) on the surface of the antigen presenting cells.
T-cells do not recognize free antigen but do recognize antigens combined with an MHC protein
Once exposed to antigen, T lymphocyte proliferate and release large number of activated, specifically reacting T cell
Whole activated T cells are formed and release into the lymph and circulated throughout the body and move to the site of infection.
Cytotoxic T-cells (CD8) directly kill infected cells Helper T-cells (CD4) “train” macrophages & stimulate B-cells to do their job better Some T-cells form memory cells after the infection is over. MHC: Cell surface molecule that present antigen to T Cell CELL-MEDIATED RESPONSE = T CELLS KILL BAD CELLS
T cells
T cells can be divided into two major classes based on cell surface proteins called CD proteins
One class of T cells has CD4 and the other CD8
About one third of all T cells are CD8 and the other two third have CD4
Activated CD8 cells become cytotoxic T cells
Activated CD4 become Helper T cells
CD8 bind to the class I MHC proteins
CD4 bind to class II MHC proteins
128
T-Lymphocyte Response to an Antigen
Many different kinds of T cells are produced which recognize, attach and destroy infected, mutant or ‘foreign’ cells.
When a T lymphocyte binds to an immunogenic antigen, it is stimulated to mature and reproduce , however they do not produce antibodies like B cells.
This reproduction results in up to four subtypes of T cells capable of acting in response to the antigen:
o Helper T cells
o Cytotoxic T cells
o Regulatory T cells
o Memory T cells
Helper T cells
Express a unique protein group on their surface called CD4.
CD stands for “cluster of differentiation” and is a means of specifically identifying different lymphocytes.
Helper T-cells, Th (as the name would suggest, help other cells of the immune system).
Helper T cells are activated when they encounter foreign antigens presented on the surface of antigen-presenting cells such as macrophages.
Helper T cells, once activated, helper T cells secrete peptides, called cytokines, which act as cell messengers to coordinate the response of cytotoxic T cells and B cells.
There are two general categories of helper T (Th) cells:
o Th1 cells
o Th2 cells.
Th1 cells & Th2 cells
Th1 cells
release cytokines that are pro-inflammatory, in that they draw neutrophils and monocytes to the area of injury or infection and stimulate macrophage phagocytosis.
increase production of prostaglandins, leading to increased blood flow and interstitial edema, and induce systemic symptoms of inflammation, including fever.
129
Release cytokines (interlukin) which can stimulate cytotoxic T cells (Tc) and favor their production and induce cell-mediated immune responses.
Th2 cells
generally secrete anti-inflammatory cytokines, which put the brakes on potentially dangerous inflammatory reactions.
interact with B lymphocytes to stimulate their differentiation (to Plasma cells) and production of antibodies.
Normally, Th1 and Th2 immune responses are in balance with each other.
Cytotoxic T cells (Tc)
Express CD8 protein on their cell surface.
Cytotoxic T cells are “activated” by cytokines from helper T cells.
Activated cytotoxic T cells recognize and bind to foreign antigen presented on MHC I of infected cells.
Cytotoxic T cells directly destroy any infected host cells they encounter by releasing cytotoxic cytokines, cytolytic enzymes and proteins called perforins that perforate and destroy the infected cell.
Tc cells cannot kill isolated virus particles, as they need the viral antigen before they become activated.
Once the Th and Tc cells are activated, they divide many times, where some of the cells become effector Tc cells, and others as memory cells, where they migrate to the lymph nodes to be activated quickly upon a second invasion.
Cytotoxic cells & Helper T cells
Antigen presentation stimulates T cells to become either "cytotoxic" CD8+ cells or "helper" CD4+ cells.
Cytotoxic cells directly attack other cells carrying certain foreign or abnormal molecules on their surfaces.
Helper T cells (Th), coordinate immune responses by communicating with other cells.
In most cases, T cells only recognize an antigen if it is carried on the surface of a cell by one of the body’s own MHC(major histocompatibility complex) molecules.
130
Regulatory T cells
Regulatory T cells act to suppress the host's immune response, a function which under some circumstances may increase the risk of infection, but under other circumstances may serve to protect the host against an overzealous immune system.
Regulatory T cells appear to suppress immune function via direct contact with B cells or other T cells, and/or by releasing anti-inflammatory cytokines.
A deficiency in regulatory T cells has been suggested to play a role in the development of autoimmune disease, while overactive regulatory T cells may protect tumor cells from immune attack.
Some evidence suggests that certain viruses, including the human immunodeficiency virus (HIV), exploit regulatory T cells' ability to dampen the body's antiviral response.
Regulatory T cells are characterized by C25 receptors on their cell membranes.
Natural killer (Nk) cells
It is a nonspecific type of lymphocyte .
Natural killer (Nk) cells have the same response as Tc cells.
NK cells distinguish infected cells and tumors from normal and uninfected cells by recognizing MHC I.
NK cells are activated in response to a family of cytokines called interferons.
Activated NK cells release cytotoxic (cell-killing) granules which then destroy the altered cells.
They were named "natural killer" because of the initial notion that they do not require prior activation in order to kill cells which are missing MHC class I.
131
B and T lymphocytes
In total, circulating lymphocytes account for approximately 30% of white blood cells in adults.
Approximately 75% of circulating blood lymphocytes are T lymphocytes and 10–15% are B lymphocytes;
the remainder are neither B nor T lymphocytes and are often referred to as "null cells."
Morphologically, B and T lymphocytes cannot be distinguished visually from each other under the microscope, but :
flow cytometry and immunophenotyping through recognition of cell surface markers and clusters of differentiation (CD markers) can distinguish between the two.
132
Antibody Structure
All antibodies are similar in appearance.
They consist of two long heavy chains called the Fc portion, and two small heads called the Fab portion.
The Fc portion is identical for all antibodies of a single class (e.g., IgG or IgM).
The Fab portion is specific for each antibody and contains the specific binding site for an antigen.
Binding of antigen to the Fab portion of the antibody activates the Fc portion, leading to destruction of the microorganism or other antigen-bearing cell.
Antibodies are y-shaped molecules composed of heavy chains and light chains, which are kept together by S-S bonds. The ends of the Y arms are the binding sites for an antigen.
133
Antibody Destruction of a Microorganism
Antibodies cause the destruction of bound antigen by a variety of mechanisms:
Antibodies typically interact with circulating antigens such as bacteria and toxic molecules, but are unable to penetrate living cells.
Antibodies work in different ways:
1. Neutralizing an Antigen
The antibody can bind to an antigen, forming an antigen-antibody complex. This forms a shield around the antigen, preventing its normal function. This is how toxins from bacteria can be neutralized or how a cell can prevent a viral antigen from binding to a body cell thereby preventing infection.
2. Activating Complement:
Complement is a group of plasma proteins made by the liver that normally are inactive in the body. An antigen-antibody complex triggers a series of reactions that activates these proteins. Some of the activated proteins can cluster together to form a pore or channel that inserts into a microbe's plasma membrane. This lyses (ruptures) the cell. Other complement proteins can cause chemotaxis and inflammation, both of which increase the number of white blood cells at the site of invasion.
3. Precipitating Antigens
Sometimes the antibodies can bind to the same free antigen to cross-link them. This causes the antigen to precipitate out of solution, making it easier for phagocytic cells to ingest them by phagocytosis (as describe above).
134
Also, the antigens within the cells walls of the bacteria can cross-link, causes the bacteria to clump together in a process called agglutination, again making it easier for phagocytic cells to ingest them by phagocytosis.
4. Facilitating Phagocytosis
The antigen-antibody complex signals phagocytic cells to attack. The complex also binds to the surface of macrophages to further facilitate phagocytosis.
Cytokines
Cyto = cell; kinos = movement
It often causes cell movement and activation.
Small proteins produced primarily by CD4+ T-cells (Th, or helper T-cells) and macrophages.
This group of molecules include:
Interleukins – something like 41 identified, known, communicate between leukocytes.
Interferons (INFs) - protect cells against viruses, stimulate macrophages and neutrophils to phagocytize bacteria, stimulate macrophages and NK cells to attack tumor cells, and stimulate Th1 cells, which drive cell-mediated reactions. Very high levels of gamma-IFN stimulates cytotoxic T-cells.
Interleukins (IL-1 to IL-17)
Inflammatory mediators
Stimulate proliferation and differentiation of T cells, B cells, macrophages and natural killer cells
“Chemotactic” factors for T cells and leukocytes
Interferons (α, β, γ)
Natural antiviral agents
Activate macrophages
Tumor necrosis factors (α and β)
Inflammatory mediators
Cytotoxic to tumor cells
Increase the activity of phagocytic cells
135
Transforming growth factor β
Produced by lymphocytes, macrophages and platelets
Chemotactic for macrophages
Stimulates the activity of fibroblasts for wound healing
Colony-stimulating factors
Produced by monocytes, fibroblasts and lymphocytes
Stimulate proliferation and growth of white blood cells and macrophages
Chemokines
are cytokines direct movement of cells around the body, from blood stream into tissues and to the appropriate location within each tissue.
share the ability to stimulate leukocyte movement (chemokinesis)
and directed movement to site of injury (chemotaxis)
and are particularly important in inflammation.
Immune response (summary)
The immune response primarily involves the interaction of antigens (foreign proteins), B lymphocytes, T lymphocytes, macrophages, cytokines, complement, and polymorphonuclear leukocytes.
Some immune active cells circulate constantly; others remain in the tissues and organs of the immune system, such as the thymus, lymph nodes, bone marrow, spleen, and tonsils.
B lymphocytes, mature in the bone marrow, work chiefly by secreting soluble substances called antibodies into the body's fluids, or humors. (This is known as humoral immunity.)
In the thymus, the T lymphocytes, in contrast, interact directly with their targets, attacking body cells that have been commandeered by viruses or warped malignancy. They do not need to become plasma cells and secrete antibody to destroy the antigen.(This is cellular immunity.)
The activated B cells differentiate into plasma cells, which secrete immunoglobulins (antibodies).
This response is regulated by T lymphocytes and their products — lymphokines, such as interleukin-2 (IL-2), IL-4, and IL-5, and interferon-8 — which determine which class of immunoglobulins a B cell will manufacture.
The lymph nodes, spleen, liver, and intestinal lymphoid tissue help remove and destroy circulating antigens in the blood and lymph.
136
Immune Response Summary (Humoral Vs Cell-mediated)
137
Immunoglobulins/Antibodies
• There are five specific immunoglobulins produced in response to an antigen: IgG, IgM, IgA, IgE, and IgD.
IgG
is the most common immunoglobulin and represents approximately 80% of all circulating antibodies.
IgG is the main antibody that crosses the placenta from the mother to the fetus during pregnancy. It binds to receptors on placental trophoblasts, which results in transfer of the immunoglobulin across the placenta. As a result, the transferred maternal antibodies provide immunity to the fetus and newborn during the first months of life.
IgG has a half-life of approximately 21 days.
IgG is the major antibody produced in the secondary immune response
Levels of IgG increase slowly during the primary (first) exposure to an antigen,
IgM
IgM is the predominant antibody in the early (primary) immune response to most antigens.
IgM. Represents about 8% to 10% of the total serum Igs .
IgM is the first antibody that an immunologically committed B lymphocyte can produce.
It has a half-life of approximately 10 days.
IgM is the largest antibody in size.
IgA
is most concentrated in secretions such as saliva, vaginal mucus, breast milk, gastrointestinal (GI) and lung secretions, and semen.
IgA acts locally rather than through the systemic circulation. Maternal IgA passes to an infant during breastfeeding (as do IgG and IgM to a
lesser extent). IgE
is responsible for allergic reactions. It is also the antibody most stimulated during a parasitic infection.
IgD
exists in low concentration in the plasma. Its role in the immune response is not completely clear, although it appears to be
important for the maturation and differentiation of all B cells.
138
Immunological Memory
Antibody titre - the concentration of antibody in serum
Primary response - response to first contact with antigen; characterized by the appearance of IgM, followed by IgG.
Secondary (anamnestic or memory) response - subsequent contact with the same antigen by memory cells results in a much stronger and faster response - antibody titre is much higher, occurs much faster, and consists primarily of IgG.
139
Harmful Effects of the Immune System (Disorders of human immunity)
When the immune system responds inappropriately, Four basic categories of reactions may occur:
Hypersensitivity,
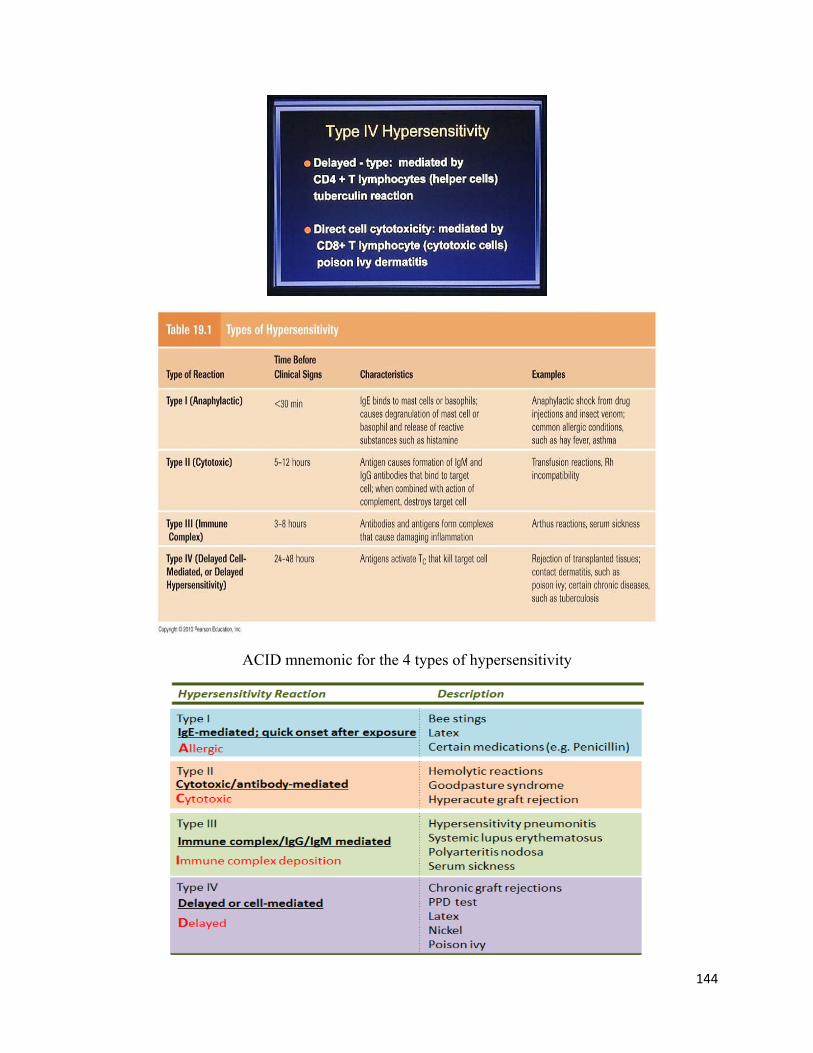
• Type I- immediate Ab-mediated hypersensitivity (mediated by IgE)
• Type II- cytotoxic Ab-mediated
• Type III- immune complex Ab-mediated
• Type IV- delayed-type cell-mediated
Autoimmune response (RA, SLE, celiac)
Immunodeficiencies (Genetic defect (SCID :Severe combined immunodeficiency) or acquired (AIDS)
Alloimmune response (Graft rejection :Immune response against transplanted organ)
The type of reaction is determined by the source of the antigen, such as environmental, self, or other person, to which the immune system is responding.
1) Hypersensitivity
Hypersensitivity refers to excessive, undesirable (damaging, discomfort-producing and sometimes fatal) reactions produced by the normal immune system.
Hypersensitivity reactions require a pre-sensitized (immune) state of the host ; occurs on second exposure to an antigen.
Allergy refers to the harmful effects resulting from a hypersensitivity to antigens, also called allergens.
Hypersensitivity reactions may be immediate, occurring within minutes to hours of re-exposure, or delayed, occurring several hours after re-exposure.
A delayed hypersensitivity reaction typically is most severe days after the re-exposure.
140
Hypersensitivity Types
Hypersensitivity Type I
Allergens activate T cells, which induce B-cell production of IgE, which binds to the Fc receptors on the surface of mast cells.
Repeated exposure to relatively large doses of the allergen is usually necessary to cause this response.
When enough IgE has been produced, the person is sensitized to the allergen.
At the next exposure to the same antigen, the antigen binds with the surface IgE, cross-links the Fc receptors, and causes mast cells to degranulate and release various mediators.
these mediators such as heparin, histamine, prostaglandins leukotrienes and cytokines
These effects result in the some of the classic associated signs and symptoms, such as hypotension, wheezing, swelling, urticaria , and rhinorrhea.
Examples of type I–mediated reactions include anaphylactic shock, allergic rhinitis, allergic asthma, and allergic drug reactions.
141
Hypersensitivity Type II
Cytotoxic reactions involve the binding of either IgG or IgM antibody to antigens covalently bound to cell membrane structures.
Antigen-antibody binding activates the complement cascade and results in destruction of the cell to which the antigen is bound.
Examples of tissue injury by this mechanism include:
Immune hemolytic anemia and
Rh hemolytic disease in the newborn.
Autoimmune hyperthyroidism
142
Hypersensitivity Type III
Immune complex-mediated reactions occur when immune complexes are formed by the binding of antigens to antibodies.
Complexes are usually cleared from the circulation by the phagocytic system.
However, deposition of these complexes in tissues or in vascular endothelium can produce immune complex-mediated tissue injury.
Such as Serum sickness, certain types of nephritis, and certain features of infective endocarditis.
143
Serum Sickness
generalized HS-III – circulating immune complexes
induced by injection of foreign proteins (antitoxin)
complex deposit in capillary beds
SS: vasculitis – rash, fever, joint pain, etc.
damage mechanism : C’ and neutrophils
diseases characterized by circulating complexes
o glomerulonephritis
o lupus (SLE), rheumatoid arthritis, chronic infections
Hypersensitivity Type IV
Unlike the other types, it is not antibody mediated but rather is a type of cell-mediated response.
144
ACID mnemonic for the 4 types of hypersensitivity
145
2) Autoimmune Diseases
Sometimes the immune system’s recognition apparatus breaks down.
It fails to properly distinguish between self and non-self, and the body begins to manufacture T cells and antibodies directed against self antigens in its own cells and tissues.
As a result, Autoimmune disorders can destroy healthy cells and body tissues, cause abnormal organ growth, and/or impair organ function.
Under normal circumstances, many T cells and antibodies react with “self” peptides ,produced throughout the body, and eliminate those cells that recognize self-antigens, preventing autoimmunity.
Misguided T cells and autoantibodies, as they are known, contribute to many autoimmune diseases.
For instance, T cells that attack certain kinds of cells in the pancreas contribute to a form of diabetes,
whereas an autoantibody known as rheumatoid factor is common in people with rheumatoid arthritis.
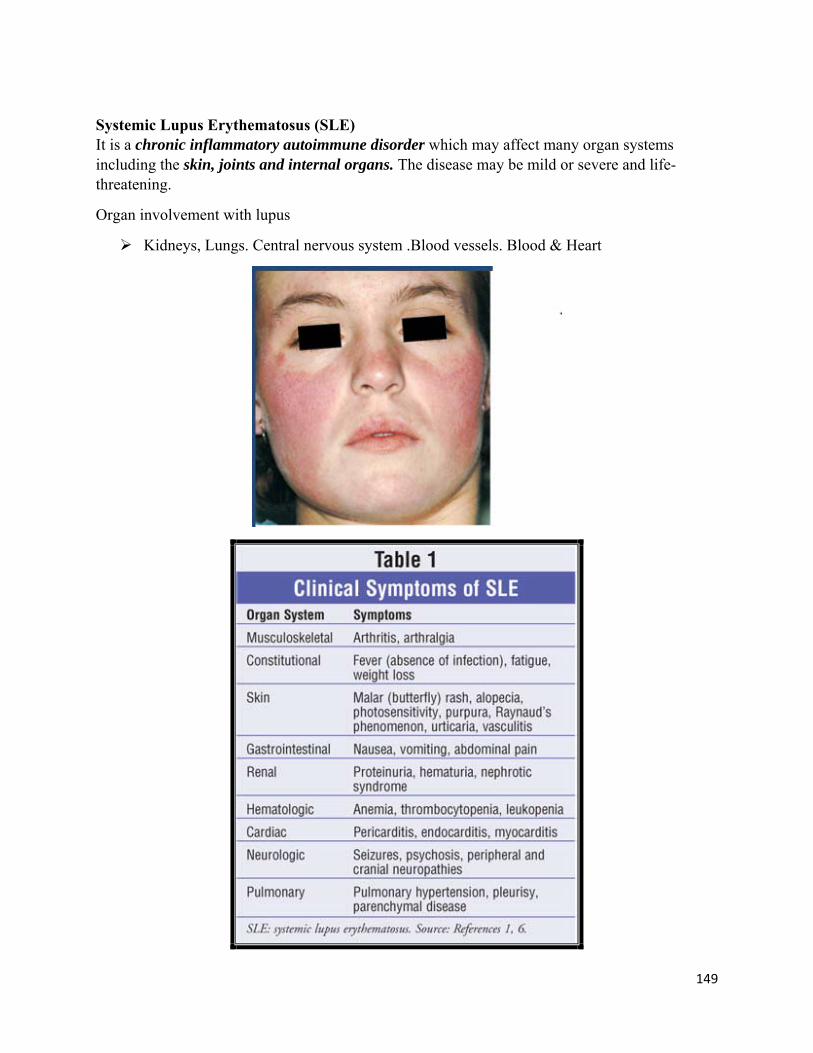
People with systemic lupus erythematosus (SLE) have antibodies to many types of their own cells and cell components.
SLE patients can develop a severe rash, serious kidney inflammation, and disorders of other important tissues and organs.
Autoimmune reactions are believed to result from a combination of factors, including drugs, viruses, genetic , hormonal, and environmental influences.
146
T cells (Misguided T) cells can attack insulin-producing cells of the pancreas contributing to an autoimmune form of diabetes mellitus.
while an autoantibody known as rheumatoid factor (RF)is common in persons with rheumatoid arthritis.
3)Immunodeficiencies
Immunodeficiencies occur when one or more of the components of the immune system are inactive.
The ability of the immune system to respond to pathogens is diminished in both the young and the elderly, with immune responses beginning to decline at around 50 years of age due to immunosenescence (تشيخ مناعي).
In developed countries, obesity, alcoholism, and drug use are common causes of poor immune function.
However, malnutrition is the most common cause of immunodeficiency in developing countries.
Diets lacking sufficient protein are associated with impaired cell-mediated immunity, complement activity, phagocyte function, IgA antibody concentrations, and cytokine production.
Deficiency of single nutrients such as iron; copper; zinc; selenium; vitamins A, C, E, and B6; and folic acid (vitamin B9) also reduces immune responses.
Additionally, the loss of the thymus at an early age through genetic mutation or surgical removal results in severe immunodeficiency and a high susceptibility to infection.
There are two main types of immune deficiencies: primary immune deficiencies and secondary immune deficiencies
Primary immune deficiencies are disorders that occur because part of the body's immune system does not function properly.
These disorders are caused by intrinsic or genetic defects in the immune system.
Some primary immune deficiencies are inherited.
o Individuals who have primary immune deficiencies are born with the disorders. Chronic granulomatous disease, where phagocytes have a reduced ability to destroy pathogens, is an example of an inherited.
Many individuals affected by primary immune deficiency diseases require life-long therapies, such as intravenous immune globulin infusions, antibiotic therapies, or bone marrow transplantations.
147
Chronic Granulomatous Disease
– Phagocytes(monocytes and neutrophils) fail to produce reactive oxygen intermediates (superoxides) and hydrogen peroxide that kill bacteria
Secondary immune deficiencies are caused by factors outside of the body, such as chemotherapy treatment, radiation therapy, malnutrition, HIV infection, and diabetes.
In addition, diseases, such as leukemia and multiple myeloma, cause cancerous immune cells to infiltrate the bone marrow, which is responsible for producing immune system cells.
Secondary immune deficiency also occurs among critically ill patients and the elderly.
Secondary immune deficiencies usually resolve once the underlying illness is treated or the outside factor is eliminated.
For instance, immune deficiencies caused by chemotherapy or radiation therapy generally resolve once the treatment is completed.
4) Alloimmune reactions
Alloimmune reactions are directed at antigens (alloantigens) from the tissues of others of the same species.
Alloantigen is a part of an animal's self-recognition system. e.g., MHC (HLA) molecules.
This Alloantigen when injected to a member of the same species that does not have the alloantigen, it will be recognized as foreign. This means that:
The Recipient reacts to this Alloantigen which is found on the Donor cells to eliminate it.
148
Alloimmunity can occur :
o in the recipient after transfusions of fluids such as blood or plasma.
o in the recipient after allografts (grafts).
o in the fetus after maternal antibodies have passed through the placenta into the fetus, as in hemolytic disease of the newborn and fetomaternal alloimmune thrombocytopenia
This type of response is commonly associated with a type II hypersensitivity reaction.
Rheumatoid Arthritis
It is an autoimmune disease in which the body's immune system attacks itself.
It initially attacks the synovium, a connective tissue membrane that lines the cavity between joints and secretes a lubricating fluid.
The pattern of joints affected is usually symmetrical, involves the hands and other joints and is worse in the morning.
Rheumatoid arthritis is also a systemic disease, involving other body organs, whereas osteoarthritis is limited to the joints.
Over time, both forms of arthritis can be crippling.
149
Systemic Lupus Erythematosus (SLE) It is a chronic inflammatory autoimmune disorder which may affect many organ systems including the skin, joints and internal organs. The disease may be mild or severe and life-threatening.
Organ involvement with lupus
Kidneys, Lungs. Central nervous system .Blood vessels. Blood & Heart
150
Raynaud's phenomenon
Raynaud's phenomenon is characterized by blood vessel spasms in the fingers, toes, ears or nose, usually brought on by exposure to cold.
Raynaud's phenomenon and Raynaud's disease, a similar disorder, may be associated with autoimmune disorders such as rheumatoid arthritis, systemic lupus erythematosus and scleroderma.
The inflammatory reaction
Inflammation is a response of body tissues to injury or irritation.
It may be the result of tissue injury, infection, or allergic reaction.
Under normal circumstances inflammation is a protective response, the goal of which is to eliminate both the initial cause of injury, such as bacteria or toxins, and the consequences of such injury, such as dead cells and tissues.
Without inflammation, infections would go unchecked and wounds would never heal. In the context of infections, inflammation is part of a broader protective response that immunologists refer to as innate immunity.
Inflammatory conditions are named by adding the suffix -itis to the affected organ or system. For example, appendicitis refers to inflammation of the appendix, pericarditis to inflammation of the pericardium, and neuritis to inflammation of a nerve.
Inflammation is not a synonym for infection, even in cases where inflammation is caused by infection.
Although infection is caused by a microorganism, inflammation is one of the responses of the organism to the pathogen.
151
Inflammation
Advantages: o It causes destruction of microbes.
o Causes detoxification of toxins.
o Clears infections.
o Helps in healing process.
o Causes repair of damaged tissues.
Disadvantages: o Inflammatory responses are sometimes harmful as they cause: o Life threatening anaphylactic reactions to insects bites, drugs and other chronic
diseases like Rheumatoid arthritis, Atherosclerosis etc.
o Inflammation of peritoneum leads to fibrous bands that causes obstruction of intestines.
o Pericardial inflammation causes the formation of dense pericardium that impairs cardiac functions.
152
The inflammatory response may be divided into main two stages:
1. The vascular response stage and 2. The cellular response stage.
1. Vascular response
Rapid vasoconstriction of blood vessels occurs in the injured area and is followed by rapid vasodilatation.
An increase in capillary permeability occurs in the injured area leading to swelling and edema. The fluids that enter the injured area are useful for diluting out any bacterial toxins or irritants present in the tissue.
Phagocytic neutrophils are the first white blood cells to arrive in the injured area. Leukocytes are attracted to the injured area by certain bacterial substances as well as by cellular debris and cytokines (chemotaxis).
As fluid leaves the capillaries, the viscosity of blood increases and leukocytes precipitate to the walls of the capillary. This process is called margination. Leukocytes undergo a change in shape and squeeze through the now more permeable capillaries into the tissues. The movement of leukocytes through the capillary wall is called diapedesis.
Other white blood cells such as eosinophils and basophils also arrive at the injured area and release substances such as histamine that enhance the inflammatory reaction. Histamine is a powerful vasodilator that increases capillary permeability. Monocytes will also enter the inflamed tissues where they mature into phagocytic macrophages.
Cytokines such as interleukin and tumor necrosis factor are released to enhance the inflammatory and immune response.
Platelets
Platelets are not cells, but cytoplasmic fragments that develop from specialized cells in the bone marrow called megakaryocytes.
Like white blood cells, platelets are drawn to an area of inflammation.
Once the platelets arrive at the site of injury, they adhere to the vessel wall, forming aggregates or plugs.
Adhering to the vessel wall activates the platelets, causing them to release several biochemical mediators, including serotonin and histamine, which temporarily decrease blood flow and bleeding.
This vasoconstriction is short lived, however, and soon blood flow increases to deliver other white blood cells to the area.
If the injury is small, the platelet plug is usually sufficient to allow for healing.
Platelets circulate in the blood for about 10 days before they become non-functioning and are phagocytized by neutrophils and monocytes.
154
Acute inflammation
Acute inflammation is the body's immediate response to cell injury or cell death ,usually appearing within a few minutes or hours and ceasing upon the removal of the injurious stimulus.
The cardinal signs of inflammation include:
Rubor — The redness that occurs as a result of the increased blood flow to the inflamed area.
Tumor — Swelling of the inflamed tissue as a result of increased capillary permeability and fluid accumulation.
Calor — The increase in temperature (heat) that occurs in the inflamed area as a result of increased blood flow.
Dolor — Pain that occurs in the inflamed area as a result of stimulation of sensory neurons.
Functio laesa — Alteration or loss of function in the inflamed tissues. Outcomes of Acute Inflammation
1) 100% Resolution 2) Healing by Fibrosis (Scar) 3) Abscess formation 4) Progression to Chronic Inflammation
Inflammation of prolonged duration (weeks-months-years) in which active inflammation, tissue destruction, and tissue repair are simultaneously present.
Causes of Chronic Inflammation
Persistent injury or infection (ulcer, TB)
Prolonged toxic agent exposure (silica, lipids)
Autoimmune disease states (RA, SLE)
The body may encapsulate a pathogen that it can't destroy in order to isolate it.
An example of such a pathogen is mycobacteria, the cause of tuberculosis; encapsulated mycobacteria appear in X-rays as identifiable spots in the lungs.