RFP: Vermont Adult Consumer Survey 2014-2015 Page 1 of 83 Request for Proposals Vermont Consumer Survey of Adults with Developmental Disabilities Receiving Services Developmental Disabilities Services Division Department of Disabilities, Aging and Independent Living Vermont Agency of Human Services Mailing address: 103 South Main Street, Waterbury, VT 05671-1601 Physical address: 94 Harvest Lane, Williston, VT Contact: June Bascom Voice: (802) 871-3050 Fax: (802) 871-3052 E-mail: [email protected]DEADLINE FOR SUBMISSIONS OF PROPOSALS: Significant dates : September 23, Bid document posted on Electronic Bulletin Board/Vermont Bid Opportunities Website October 20, 2014 Deadline for submission of proposals October 21, 2014 Target date for selecting contractor October 21, 2014 Target date for notification to bidders of December 8, 2014 Target date for beginning of contract – contingent upon contract being Contents : A. Introduction B. Purpose of Request C. Specification of Work to be Performed D. Contract Specification
Transcript
RFP: Vermont Adult Consumer Survey 2014-2015 Page 1 of 83
Request for Proposals
Vermont Consumer Survey ofAdults with Developmental Disabilities Receiving
Services
Developmental Disabilities Services Division Department of Disabilities, Aging and Independent Living
Vermont Agency of Human ServicesMailing address: 103 South Main Street, Waterbury, VT 05671-1601
September 23, 2014Bid document posted on Electronic Bulletin Board/Vermont Bid Opportunities Website
October 20, 2014 Deadline for submission of proposalsOctober 21, 2014 Target date for selecting contractorOctober 21, 2014 Target date for notification to bidders of selection of contractor
December 8, 2014Target date for beginning of contract – contingent upon contract being signed by all parties
Contents:A. IntroductionB. Purpose of RequestC. Specification of Work to be PerformedD. Contract SpecificationE. Proposal Submission RequirementsF. Selection Criteria
Attachment 1: 2014-2015 National Core Indicators Adult Consumer Survey Attachment 2: Customary State of Vermont Contract Provisions
This Request for Proposal (RFP) is available in alternate formats upon request.
RFP: Vermont Adult Consumer Survey 2014-2015 Page 2 of 83
A. INTRODUCTION
The Department of Disabilities, Aging and Independent Living (DAIL, or the State) manages services and supports in Vermont for people with developmental disabilities (DD). As part of the quality assurance process DAIL conducts consumer survey interviews of adults (age 18 and over) receiving DD services. In SFY 2015, DAIL joined National Core Indicators (NCI) and will be using the NCI Adult Consumer Survey (ACS) to compare the survey results of service recipients in Vermont with the other NCI states who conduct the same survey. In future years, this will include comparisons of current consumer perceptions to previous consumer perceptions.
The State seeks a contractor to conduct a consumer satisfaction survey of adults receiving developmental disabilities services. This survey shall be conducted between January 2015 and June 2015.
B. Purpose of Request
The State seeks to compare current consumer perceptions of developmental disabilities services with the results of the same National Core Indicator survey conducted by other states.Subsequent surveys will also provide an opportunity to gauge consumer perception and to monitor for changes over time.
C. Specification of Work to be Performed
The contractor will collaborate with the State and developmental disabilities (DD) services providers (agencies) in Vermont to arrange for and conduct in-person interviews with a statistically significant sample of adults (age 18 and older and no longer in high school), living in Vermont and receiving home and community-based DD services. Individuals to be interviewed must have been in services for a minimum one year and must be receiving at least one paid service in addition to service coordination in order to participate in the survey.
The Contractor (and any surveyors arranged by contractor) will attend a mandatory one-day in- person training in Vermont provided by Human Services Research Institute (HSRI) staff on setting up and conduct interviews. The Contractor will also be required to participate in a webinar conducted by HSRI on how to use the ODESA (on-line database) for reporting data. There will be no cost to participate the training or webinar. Any staff/subcontractors will need to be prior- approved by the State. The Contractor may use more than one surveyor but all surveyors must participate in the in-person one-day training and pass the required DAIL background check prior to conducting interviews. Costs of the background check for the contractor will be paid for by the State. The Contractor will be responsible for paying for the background check for other surveyors, if any. If it is necessary to bring in additional surveyors later in the process, the State will provide HSRI training materials in lieu of the in-person training. The Contractor must also sign a HIPAA Agreement as part of the contract.
RFP: Vermont Adult Consumer Survey 2014-2015 Page 3 of 83
The survey tools are provided by NCI (see Attachment 1) and cannot be altered by the Contractor. Additional questions may be added to the survey tool by the State (not to exceed 25 additional questions between the Background Information and Interview survey).
Timeline
- November – Agency Lists prepared by State- December – Pre-Survey Information and Background Information obtained- January – Interviews set up- January – June – Conduct interviews and enter data- June 30th – All data entry completed
Tasks
Select survey sample :1. The State shall identify the names of the individuals and their respective agency that will
make up a statewide representative valid sample of consumers. The initial draw will include an estimated 450 – 600 names. The sample must result in a total of 325 completed surveys. The State will provide the Contractor an initial list of 450 – 600 names by agency. It is anticipate that not all the individual’s included in the list will need to be contacted by the Contractor before 325 completed surveys have been accomplished. If, however, additional names need to be added to the list, the State will provide that information.
Gather preliminary survey information :2. The Contractor shall meet with each agency contact person to review the Pre Survey Form
(i.e., information to help the surveyor) and Background Information (e.g., demographics). The contractor shall send the Pre Survey Form and Background Information to the agency contact person. Agency staff will complete both the Pre-Survey Form and Background Information for each individual participating in an interview and provide a hard copy of the data to the Contractor prior to the interview.
3. The Contractor shall enter Background Information onto ODESA. If there is missing Background Information, the Contractor shall try to obtain this information during the interview. The Contractor shall use information from the Pre Survey Forms to inform the interviews.
RFP: Vermont Adult Consumer Survey 2014-2015 Page 4 of 83
Conduct survey interviews :4. The Contractor shall work with the agency contact person to contact individuals from the
sample and arrange for a time and place to conduct face-to-face interviews. Agency staff will set up the interviews in locations that are comfortable for the individual and ideally have internet access.
5. The Contractor shall conduct the face-to-face interviews using a laptop or iPad/tablet to enter survey data into ODESA at the time of the interview when internet connection is available. There may be times when this cannot be done during the interview (e.g., no internet connection), in which case data will be recorded on paper and later entered into ODESA.
6. As part of the survey process, the Contractor shall let each individual know that participating in the interview is voluntary, services are not contingent on participation, and not all questions must be answered. The Contractor will verify that each individual participating gives his or her consent to the interview.
7. Prior to the interview, the agency contact person, along with the individual and his/her support staff, determines if the individual needs to have a proxy available to help answer questions in Section 2 of the survey tool. A proxy may not be the individual’s services coordinator/case manager. During the interview, the Contractor works with each individual to determine which, if any, questions the individual is unable to answer and if they would like to have a proxy answer the questions. If a proxy is needed but is not present, the surveyor may contact a proxy at a later date to obtain answers to those questions in Section 2 that were not answered by the individual. This can be done by telephone.
8. The Contractor must assure that only the individual being interviewed may answer questions in Section 1 of the survey tool.
9. The Contractor shall complete the Interviewer Feedback form for each interview.10. The contractor must ensure validity of all surveyors through inter-rater reliability between
surveyors. Mock interviews and shadowing a certain percentage of actual interviews are acceptable methods for checking reliability.
11. The Contractor shall conduct interviews starting in January and must have them completed by the end of June. Interviews may take, on average, 45 – 60 minutes each plus additional time before and after the interview.
12. All surveys must be completed and data entered and submitted into ODESA no later than June 30, 2015.
RFP: Vermont Adult Consumer Survey 2014-2015 Page 5 of 83
Outcome Measures :
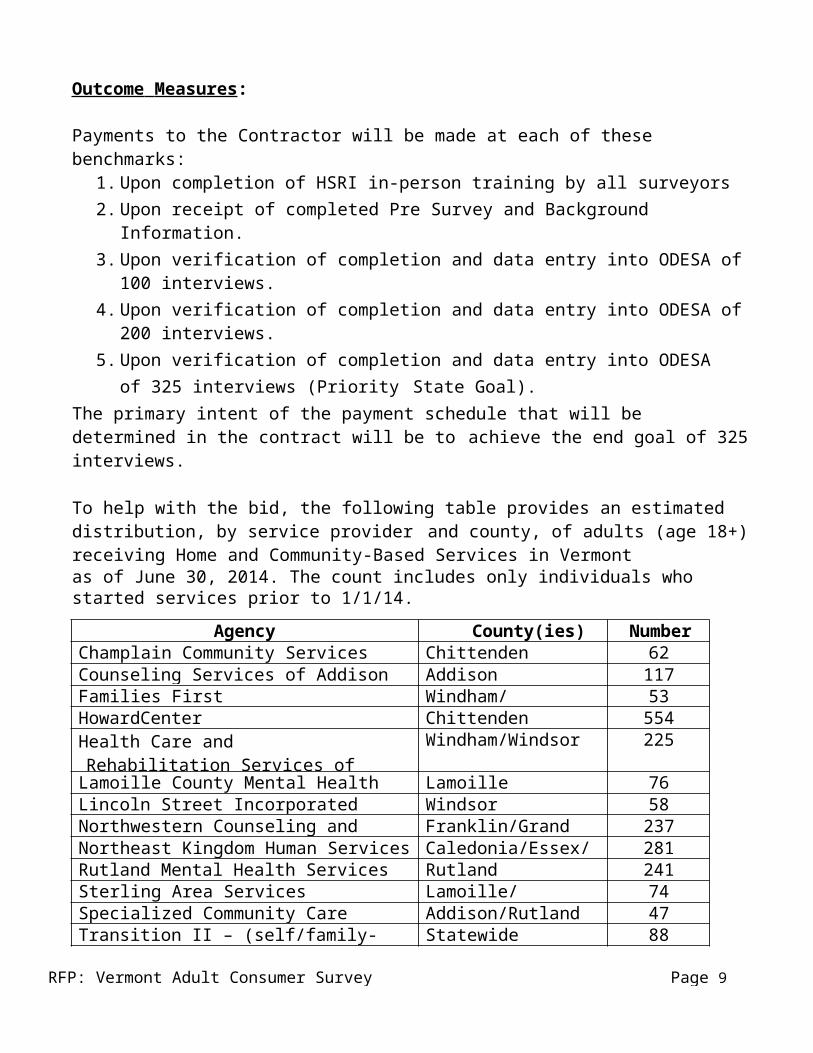
Payments to the Contractor will be made at each of these benchmarks:1. Upon completion of HSRI in-person training by all surveyors2. Upon receipt of completed Pre Survey and Background Information.3. Upon verification of completion and data entry into ODESA of 100 interviews.4. Upon verification of completion and data entry into ODESA of 200 interviews.5. Upon verification of completion and data entry into ODESA of 325 interviews (Priority
State Goal).The primary intent of the payment schedule that will be determined in the contract will be to achieve the end goal of 325 interviews.
To help with the bid, the following table provides an estimated distribution, by service provider and county, of adults (age 18+) receiving Home and Community-Based Services in Vermontas of June 30, 2014. The count includes only individuals who started services prior to 1/1/14.
Agency County(ies) NumberChamplain Community Services Chittenden 62Counseling Services of Addison County Addison 117Families First Windham/Bennington 53HowardCenter Chittenden 554Health Care and Rehabilitation Services of Southeast Vermont
Windham/Windsor 225
Lamoille County Mental Health Services Lamoille 76Lincoln Street Incorporated Windsor 58Northwestern Counseling and Support Services Franklin/Grand Isle 237Northeast Kingdom Human Services Caledonia/Essex/Orleans 281Rutland Mental Health Services Rutland 241Sterling Area Services Lamoille/Washington 74Specialized Community Care Addison/Rutland 47Transition II – (self/family-managed) Statewide 88United Counseling Service Bennington 129Upper Valley Services Orange/Washington 188Washington County Mental Health Services Washington 228
D. Contract Specification
The contract format will be the State of Vermont Standard Contract for Personal Services, with relevant attachments, describing the tasks to be performed. The Contractor is expected to comply with the customary State contract provisions (current provisions appear in Attachment 2).
RFP: Vermont Adult Consumer Survey 2014-2015 Page 6 of 83
The State of Vermont assumes no responsibility and no liability for costs incurred by respondents in responding to the RFP or in responding to any further requests for interviews, additional data, etc. prior to the issuance of a contract. The State reserves the right to waive portions of this RFP, to waive any informalities in proposals, to reject any or all proposals and/or to negotiate terms and conditions of the awarded contract. The State reserves the right to negotiate specific terms and provisions of the proposal. The contract, if approved, may be renewed by amending the contract up to a period not to exceed two years, for an aggregate maximum of three years.
E. Proposal Submission Requirements
Interested bidders must submit a proposal, which must include the following:
1. Describe the qualifications and experience of the Bidder and any staff/subcontractors; the availability of personnel; knowledge of survey accommodations and techniques for interviewing individuals with developmental disabilities; and relevant expertise and specific previous experience in successfully completing similar types of surveys. Bidders may attach previous work products as attachments or links (not subject to the page limit).
2. Provide two professional references that verify the Contractor’s capacity (skills and experience) to manage this project successfully.
3. Provide itemized price quotation for the successful completion of each Outcome Measure listed below. The quote for each measure must be inclusive of all costs, including but not limited to Contractor’s and any staff/subcontractor’s time and expenses (e.g., travel, supplies, technology, copies, telephone, etc.). (Note: secondary administrative overhead calculated into the costs must be limited to no more than 15%.)
a. Completed HSRI in-person training by all surveyors: $ b. Completed Pre Survey Forms: $ c. Completion and data entry of 100 interviews: $ d. Completion and data entry of 200 interviews: $ e. Priority State Goal: Completion and data entry
of 325 interviews: $ Total: $
The actual payment schedule will be determined in the contract.
Proposals may not exceed fifteen (15) pages. Individual resumes may be submitted as attachments to the proposal (not subject to the page limit).
RFP: Vermont Adult Consumer Survey 2014-2015 Page 7 of 83
Proposals must be submitted to: June Bascom
Developmental Disabilities Services DivisionMailing address: 103 South Main Street, Waterbury, VT 05671-
Completed proposals must be received by 5:00 PM on Monday, October 20, 2014. If a proposal is submitted by email, it must be submitted in pdf format and must include the signature of the individual who is authorized to submit the proposal on behalf of the bidder. It is the bidder’s responsibility to ensure that a submission (including electronic submission) is received by the State before the stated deadline. Bidders are encouraged to confirm that a proposal has been received by the State before the deadline, including the use of an electronic received message. The State shall not be responsible for any submission (including any electronic submission) that is not received by the deadline, regardless of cause (including but not limited to the failure of electronic communication). Bidders are expected to keep an original paper copy of proposals at their primary place of business, which must be available for review by State staff.
F. Selection CriteriaDAIL anticipates selecting a Contractor under the terms of this RFP. The Contractor that is judged to best meet the criteria of the RFP will be awarded the contract. The selection of a Contractor will be made using the following criteria:
1. Qualifications and experience of the Contractor and any staff/subcontractors; the availability of personnel; knowledge of survey accommodations and techniques for interviewing individuals with developmental disabilities; and relevant expertise and specific previous experience in successfully completing similar types of surveys. (40%)
2. Strength of two professional references that verify the Contractor’s capacity (skills and experience) to manage this project successfully (20%)
3. Proposed Reimbursement (40%)
DAIL reserves the right to reject any or all proposals. Bidders that submit a proposal will be notified of the results of the selection process.
Form and Background Information) – National Core Indicators (does not include up to 20 additional questions in the Background Information and Interview survey.
Attachment 2: State of Vermont Customary State Contract Provisions (current version as of the release of this RFP).
RFP: Vermont Adult Consumer Survey 2014-2015 Page 8 of 83
ATTACHMENT 1
2014 – 2015 NATIONAL CORE INDICATORS ADULT CONSUMER
Description of NCI:This survey was developed in conjunction with the National Core Indicators (NCI), an effort that began in 1997 and is co-sponsored by the National Association of State Directors of Developmental Disabilities Services (NASDDDS) and the Human Services Research Institute (HSRI). The purpose of NCI is to identify and measure core indicators of performance of state developmental disabilities service systems. Currently, 40 States, the District of Columbia, and 22 sub-state entities participate in NCI. This survey is intended to measure performance indicators originally identified by the NCI Operations Committee, which is made up of representatives from the participating states. For more information, go to www.nationalcoreindicators.org.
Organization of Survey:The survey consists of five parts.
The Pre-Survey Form requests information that may be useful for scheduling and conducting the face-to-face surveys. This information is not analyzed by HSRI and cannot be placed into the Online Data Entry Survey Application (ODESA).
The Background Information section consists of information that will be analyzed in conjunction with the face-to-face survey responses. This information must be collected for all individuals surveyed. Most states collect this information from case manager or system records, however, some states use surveyors to collect some of this information directly from the individual, guardian, or family. The state will specify which elements need to be obtained directly by the surveyor.
Section I contains questions that may only be answered by face-to-face meetings with the person receiving services and supports. These are subjective, "satisfaction" related questions that may not be answered by anyone else.
Section II contains questions that may be answered by the individual or someone who knows the person well (proxy respondent), such as a family member, friend, staff person, guardian or advocate. Service coordinators or case managers are not allowed to be Section II respondents. If the individual is answering, the questions need to be asked face-to face. If a proxy respondent answers, questions need to be asked face-to-face if all possible. Only when necessary, questions for proxy respondents may be asked over the phone.
The Surveyor Feedback Sheet is the last page of the survey. Please fill out one sheet for each survey you complete.
Pre-Survey Form
Page 11 of 83NCI Adult Consumer Survey 2014-15
Pre-Survey FormThe Pre-Survey Form is intended to provide surveyors with the information they will need to schedule and conduct the face-to-face surveys. The state should review this form and decide what information will be provided to surveyors in advance (e.g., name, phone number, communication needs, etc.), how the information will be gathered (e.g., service coordinators, databases, surveyors etc.), and determine the administrative procedures (including informed consent) that must be followed when arranging the face-to-face surveys.
It is strongly suggested that as many Pre-Survey items as possible be filled out and reviewed before starting the face-to-face survey. Experience has shown that using familiar names and terms helps the respondent understand the questions being asked and facilitates the survey process. Surveyors can use the Pre-Survey items to fill in blanks in Sections I and II of the survey form where indicated with a symbol. Doing this prior to the face-to- face survey helps the conversation flow more smoothly.
None of the Pre-Survey information is submitted to HSRI. Actual procedures for using the Pre-Survey Form should be determined by the state’s NCI coordinator and communicated to surveyors during training. These procedures should also be communicated to HSRI.
Additional instructions regarding your state’s specific administrative procedures may be noted below:
Pre-Survey Form
Page 12 of 83NCI Adult Consumer Survey 2014-15
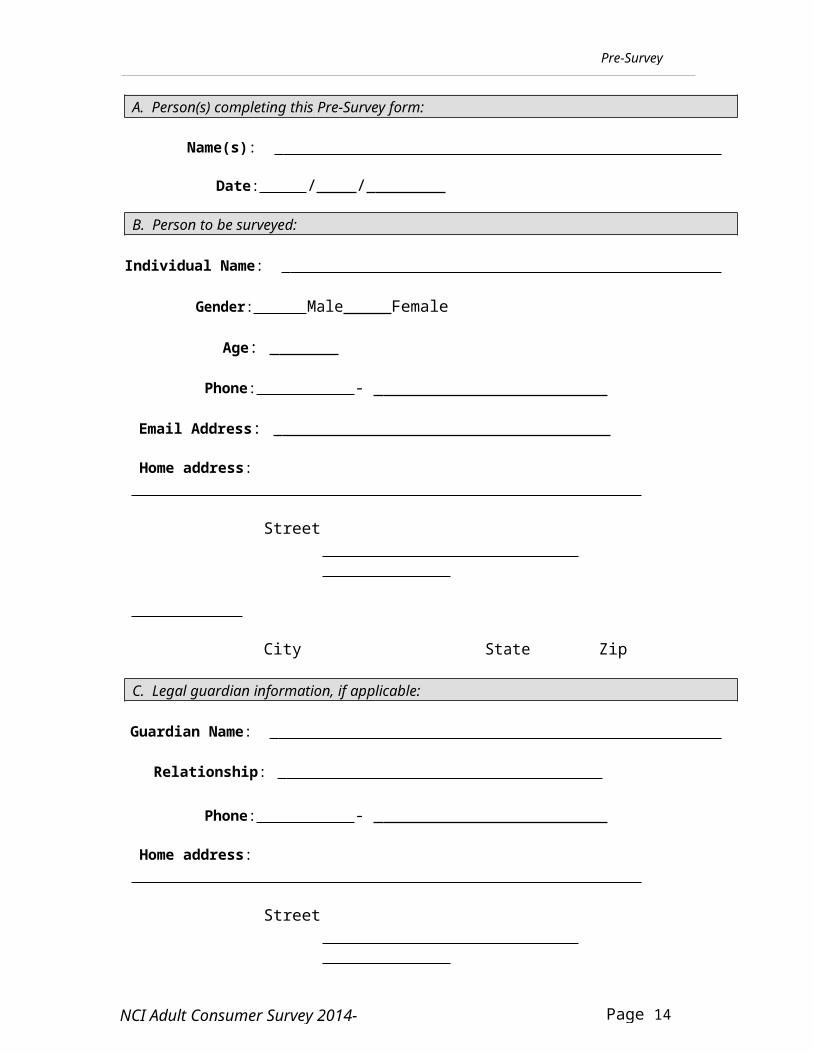
A. Person(s) completing this Pre-Survey form:
Name(s):
Date: / /
B. Person to be surveyed:
Individual Name:
Gender: Male Female
Age:
Phone: -
Email Address:
Home address:
Street
City State Zip
C. Legal guardian information, if applicable:
Guardian Name:
Relationship:
Phone: -
Home address:
Street
City State Zip
E-mail:
Pre-Survey Form
Page 13 of 83NCI Adult Consumer Survey 2014-15
D. Consent Requirements and Procedures
Each state will follow its own specific consent requirements. However, at a minimum, the surveyor needs to obtain verbal consent from the individual (or his/her legal guardian, if applicable) before the face-to-face survey takes place.
Note: The consent questions at the bottom of page 25 must be answered.
PS-1. Contact… Who should the surveyor call to arrange a face-to-face survey with this person (individual, parent/guardian, day or residential program staff, etc.)?
Name: Relationship:
Phone #1:
Phone #2:
E-mail address:
Note… We would like to conduct the face-to-face survey with persons alone, when appropriate. However, some persons may feel uncomfortable with strangers, may have community protection issues, or may have medical or behavioral challenges that require supervision by designated caregivers.
Do you recommend that a caregiver be present while this person is surveyed?
Yes No
If yes, please explain:
Pre-Survey Form
Page 14 of 83NCI Adult Consumer Survey 2014-15
PS-2. Accommodations… Does this person need any accommodations? (Examples: Communication - e.g., interpreter if the primary language is something other than English, sign language, communication device, voice amplifier, someone familiar with the person’s communication style; Accessibility - e.g., transportation, space issues; Other - e.g., medical, allergies). Please explain what arrangements are needed for the face-to-face survey.
PS-3. Case manager/service coordinator… What is the name and contactinformation of this person's case manager/service coordinator?
Name: Phone:
Cell Phone:
E-mail address:
PS-4. Person who can provide information about this individual’s employment… Please indicate the person (e.g., Job Coach, Case Manager) who can provide the most accurate information about this person’s employment, such as hours worked and wages earned. This information is needed for questions BI-37 through BI-47 in the Background Information section.
Name: Relationship:
Phone:
E-mail address:
PS-5. Proxy Respondents… If you believe this person may be unable or unwilling to complete Section II of the survey, please indicate the name(s) and number(s) of others who know the him or her well and could respond on his/her behalf. Family members, guardians, friends, and staff may respond; case managers/service coordinators may not respond.
Name: Relationship:
Phone: E-mail address:
Name:
Relationship:
Phone: E- mail
Pre-Survey Form
Page 15 of 83NCI Adult Consumer Survey 2014-15
address:
Pre-Survey Form
Page 16 of 83NCI Adult Consumer Survey 2014-15
PS-6. Living Arrangement… Please indicate who this person lives with.
lives alone
lives with parent/relatives
lives in large residential care facility lives in shared house or apartment
lives with partner, spouse, and/or children
If applicable, provide first names of roommates or housemates:
PS-7. Support Staff… If there are any people who are paid to provide supports in this person’s home, or at work or day program, please indicate their first names. If there are several workers, please list the primary staff who spend the most time with this person.
Support Staff:
PS-8. Employment … If applicable, please indicate the name(s) of this person’s paid community job(s). A community job refers to paid work- either competitive or supported employment. Examples include both individual and group employment, such as a work crew or enclave. It does not include work done in a facility-based setting (e.g., sheltered workshop) or volunteer work. Use the term or abbreviation the person is most familiar with.
Place of work:
PS-9. Day Program/Other Regularly Scheduled Daily Activities… If applicable, please indicate this person’s day program or what they do as a regularly scheduled daily activity (examples include attending a sheltered workshop, volunteering or attending a senior program). Note: this does not include a paid job in the community (see PS-8). Use the term or abbreviation person is most familiar with.
Day Program/Other Activity:
Pre-Survey Form
Page 17 of 83NCI Adult Consumer Survey 2014-15
PS-10. Self-Advocacy Organization… What self-advocacy groups are active and well- known in the person's area? (Examples: People First, Self-Advocates Becoming Empowered, Speaking for Ourselves.)
PS-11. Self-directed supports… Is this person currently using a self- directed/participant-directed supports option? These options offer individuals (and their representatives) the opportunity to manage some or all of their services. For example, they may hire & fire their own support workers and/or have control over their budget or services.
Yes No
If yes, please provide additional information:
What is the term used to describe the participant-directed budget (e.g.,individual budget,
DDS budget, etc.)? Please note the term that would be most familiar to the person.
What is the name of the financial management service (also called fiscalagent, fiscal
intermediary, intermediary service organization, etc.) that manages the budget? Please note the term that would be most familiar to the person.
Does this person employ his/her own staff?
Yes No
Background Information
BI-1.Survey Code: (Unique Survey Code)
Note: This code should be provided by the state project coordinator and is for dataanalysis purposes only. A unique survey code should be assigned to each person. Do NOT use a number that could possibly identify the person (for example, do NOT use social security numbers). This code does not have to be limited to the amount of spaces above.BI-2.Region or County: {if applicable}
IMPORTANT: Background Information (BI) item numbers that are highlighted represent critical items for data analysis purposes. Please make every effort to provide this information so that your state’s data can be fully analyzed.
Page 18 of 83NCI Adult Consumer Survey 2014-15
BACKGROUND INFORMATION
The questions in this section are usually answered by reference to agency records or computer system reference (dependent upon availability by state). It is suggested that this section be completed along with the pre-survey form by the appropriate agency staff member, such as a case manager/service coordinator. Some items may be completed by the individual receiving services, a residential staff person or family member as necessary.
PERSONAL
BI-3. Date of birth:(mm/dd/yyyy) / /
BI-4. Gender: 1 Male 2 Female
BI-5. Is this person Spanish/Hispanic/Latino? (Note: based on U.S. Census Bureau definitions, ethnicity is considered to be a separate question from race.)
1 No, not Spanish/Hispanic/Latino 2 Yes (Mexican, Mexican American, Chicano, Puerto Rican,
Cuban, or Other Spanish/Hispanic/Latino) 3 Don’t know
Background Information
Page 19 of 83NCI Adult Consumer Survey 2014-15
BI-6. What is this person's race? (Check ONE or MORE races to indicate what this person considers himself/herself to be)
1 American Indian or Alaska Native 2 Asian (Asian Indian, Chinese, Filipino, Japanese, Korean,
Vietnamese or Other Asian) 3 Black or African-American 4 Pacific Islander (Native Hawaiian, Guamanian or Chamorro,
Samoan, or Other Pacific Islander) 5 White 6 Other race not listed 7 Don’t know
BI-7. Does this person have a legal/court-appointed guardian? (Check ONE)
1 No, person is independent of guardianship (legally competent or presumed competent)
BI-8. Marital status: (Check ONE) 1 Single, never married 2 Married 3 Single, married in past 4 Don’t know
BI-9. Is this person diagnosed with an intellectual disability (ID)? 1 No code BI-9a as NOT APPLICABLE 2 Yes 3 Don’t Know code BI-9a as NOT APPLICABLE
BI-9a. If BI-9 is answered ‘yes’, what level of ID? 0 NOT APPLICABLE – no ID diagnosis 1 Mild ID 2 Moderate ID 3 Severe ID 4 Profound ID 5 Unspecified level of ID 6 ID level unknown
Background Information
Page 20 of 83NCI Adult Consumer Survey 2014-15
BI-10. What other disabilities are noted in this person’s record? (Check one column for each disability)
Pervasive Developmental Disorder) 1 2 3 Cerebral Palsy 1 2 3 Brain Injury 1 2 3 Seizure Disorder/Neurological Problem 1 2 3 Chemical Dependency 1 2 3 Down Syndrome 1 2 3 Prader-Willi Syndrome 1 2 3 Other disabilities not listed 1 2 3 No other disabilities other than ID
BI-10a. What health conditions are noted in this person’s record?(Check one column for each health
condition) No Yes Don’tKnow
1 2 3 Cardiovascular Disease (e.g., Coronary Heart Disease, Angina) 1 2 3 Diabetes (including Type I and Type II) 1 2 3 Cancer (e.g., Breast, Prostate, Colon, Lung, etc.) 1 2 3 High Blood Pressure 1 2 3 High Cholesterol 1 2 3 Dysphasia 1 2 3 Pressure Ulcers 1 2 3 Limited or No Vision- Legally Blind 1 2 3 Hearing Loss- Severe or Profound 1 2 3 Alzheimer’s Disease or other Dementia 1 2 3 Other health conditions not listed
BI-11. What is this person’s primary language? (What language does s/he best understand?) 1 English 2 Other
Background Information
Page 21 of 83NCI Adult Consumer Survey 2014-15
BI-12. What is this person’s primary means of expression? (Check ONE –most frequently used)
1 Spoken 2 Gestures/body language 3 Sign language or finger spelling 4 Communication aid/device 5 Other 6 Don’t know
BI-13. How would you describe this person’s mobility? (Check ONE) 1 Moves self around environment without aids 2 Moves self around environment with aids or uses wheelchair independently 3 Non-ambulatory, always needs assistance to move around environment 4 Don’t know
HEALTH
BI-14. Overall, how would you describe this person’s health? 1 Excellent 2 Very good 3 Fairly good 4 Poor 5 Don’t know
BI-15. Does this person have a primary care doctor? 1 No 2 Yes 3 Don’t know
BI-16. When was his/her last complete annual physical exam? (We are referring to a routine exam, not a visit for a specific problem or illness.) (Check ONE) 1 In the past year (anytime less than 12 months ago) 2 One year ago or more 3 Don't know
BI-17. When was his/her last dentist visit? (Check ONE) 1 Within the last six months (anytime less than 6 months ago) 2 Within the past year (6 months but less than 12 months ago) 3 One year ago or more 4 Don't know
Background Information
Page 22 of 83NCI Adult Consumer Survey 2014-15
BI-18. When was the last time this person had an eye examination/vision screening? 1 Within the past year (anytime less than 12 months ago) 2 Within the past 2 years (1 year but less than 2 years ago) 3 Within the past 3 years (2 years but less than 3 years ago) 4 Within the past 5 years (3 years but less than 5 years ago) 5 5 or more years ago 6 Has never had a vision screening 7 Don’t know
BI-19. When was the last time this person had a hearing test? 1 Within the past 5 years (anytime less than 5 years ago) 2 5 years ago or more 3 Has never had a hearing test 4 Don’t know
BI-20. During the past 12 months, has this person had a flu vaccination? 1 No 2 Yes 3 Don’t know
BI-21. Has this person ever had a vaccination for pneumonia? 1 No 2 Yes 3 Don’t know
BI-22. How much does this person weigh? lbs.
BI-23. How tall is this person? feet inches
BI-24. Does this person routinely engage in any moderate physical activity? (Moderate physical activity is an activity that causes some increase in breathing or heart rate. Examples include, but are not limited to, brisk walking, swimming, bicycling, cleaning, and gardening.) (Check ONE) 1 No 2 Yes 3 Don’t know
Background Information
Page 23 of 83NCI Adult Consumer Survey 2014-15
BI-24a. If yes, does the moderate physical activity last 30 minutes or more? (Check ONE) 0 NOT APPLICABLE – does not do activity 1 No 2 Yes 3 Don’t know
BI-24b. If yes, how many times per week? (Check ONE) 0 NOT APPLICABLE – does not do activity for at least 30 minutes 1 Five times or more per week 2 Three to four times per week 3 One to two times per week 4 Don’t know
BI-25. Does this person smoke or chew tobacco? 1 No 2 Yes 3 Don’t know
BI-26. If female, when was her last Pap test screening? A Pap test is a test used to check women for cancer of the cervix. (Check ONE) (Will be reported for females age 18 and over) 0 NOT APPLICABLE – INDIVIDUAL IS MALE 1 Within the past year (anytime less than 12 months ago) 2 Within the past 2 years (1 year but less than 2 years ago) 3 Within the past 3 years (2 years but less than 3 years ago) 4 Within the past 5 years (3 years but less than 5 years ago) 5 5 or more years ago 6 Has never had a Pap test 7 Don’t know
BI-27. If female, when was her last mammogram? A mammogram is an x-ray of each breast to check for breast cancer. (Check ONE) (Will be reported for females age 40 and over) 0 NOT APPLICABLE – INDIVIDUAL IS MALE or FEMALE IS UNDER 40 1 Within the past year (anytime less than 12 months ago) 2 Within the past 2 years (1 year but less than 2 years ago) 3 Within the past 3 years (2 years but less than 3 years ago) 4 Within the past 5 years (3 years but less than 5 years ago) 5 5 or more years ago 6 Has never had a mammogram 7 Don’t know
Background Information
Page 24 of 83NCI Adult Consumer Survey 2014-15
BI-28. When was the last time this person had a screening for colorectal cancer (either sigmoidoscopy or colonoscopy)? (Check ONE) (Will be reported for all adults age 50 and over) 0 NOT APPLICABLE – INDIVIDUAL IS UNDER 50 1 Within the past year (anytime less than 12 months ago) 2 Within the past 2 years (1 year but less than 2 years ago) 3 Within the past 3 years (2 years but less than 3 years ago) 4 Within the past 5 years (3 years but less than 5 years ago) 5 5 or more years ago 6 Has never had a screening for colorectal cancer 7 Don’t know
BI-29. How often does this person require medical care? (Check ONE) (Medical care refers to care that must be performed or delegated by a nurse or physician. Do not include medication administration.) 1 Less frequently than once/month 2 At least once/month, but not once a week 3 At least once/week, or more frequently 4 Don’t know
BI-30. If this person has seizures, how often do they occur? (Check ONE) 0 NOT APPLICABLE -- does not have seizures 1 Seizures are controlled 2 Less frequently than once/month 3 At least once/month, but not once a week 4 At least once/week, or more frequently 5 Don’t know
BI-31. Does this person currently take medications to treat mood disorders, anxiety, and/or psychotic disorders?[Medications for mood disorders- includes any drug prescribed to elevate or stabilize mood (reduce mood swings), e.g., to treat depression, mania, or bipolar disorder.][Medications for anxiety- includes any drug prescribed to treat anxiety disorders (including obsessive disorders and panic disorders) or to reduce anxiety symptoms.][Medications for psychotic disorders- includes any drug (e.g., anti-psychotic or “neuroleptic”) used to treat psychotic disorders such as schizophrenia or psychotic symptoms such as hallucinations.] 1 No 2 Yes 3 Don’t know
Background Information
Page 25 of 83NCI Adult Consumer Survey 2014-15
BI-31a. If ‘Yes’ to BI-31, how many medications to treat mood disorders, anxiety, and/or psychotic disorders does this person take? 0 NOT APPLICABLE – does not take medications for these disorders 1 1-2 medications 2 3-4 medications 3 5-10 medications 4 11 or more medications 5 Don’t’ know
BI-31b. Does this person currently take medications for behavioral challenges?[Medications for behavioral challenges- includes any drug prescribed for a behavior modification purpose (e.g. such as a stimulant, sedative, or beta-blocker), e.g., to treat ADHD, aggression, self- injurious behavior, etc.]
1 No 2 Yes 3 Don’t know
BI-31c. If ‘Yes’ to BI-31b, how many medications to treat behavioral disorders does this person take? 0 NOT APPLICABLE – does not take medications to treat behavioral disorders 1 1-2 medications 2 3-4 medications 3 5-10 medications 4 11 or more medications 5 Don’t’ know
BI-31d. Does this person have a behavior plan?A behavior plan is based on an assessment of an individual’s challenging behavior. The plan includes a description of the individual’s strengths, preferences and interests, the goal(s) related to diminishing/eliminating the behavior, and applicable information about the nature of the behavior and potential triggering events. The plan should describe the interventions and accommodations that will contribute to the goal(s). It should also include the ways in which progress will be monitored, the staff who will be responsible for the interventions, and the length of time that the plan will be in place.
1 No 2 Yes 3 Don’t know
Background Information
Page 26 of 83NCI Adult Consumer Survey 2014-15
BI-32. Does this person currently receive Medicare? 1 No 2 Yes 3 Don’t know
RESIDENCE
BI-33. How long has this person lived in his/her current home? 1 Less than 1 year 2 1-3 years 3 3-5 years 4 Over 5 years 5 Don’t know
BI-34. How would you characterize the place where this person lives?(Check ONE) 1 Intermediate Care Facility for persons with ID/DD
(ICF/ID)-1-3 residents with disabilities 2 Intermediate Care Facility for persons with ID/DD
(ICF/ID)-4-6 residents with disabilities 3 Intermediate Care Facility for persons with ID/DD
(ICF/ID)-7-15 residents with disabilities 4 Intermediate Care Facility for persons with ID/DD
(ICF/ID)-16 or more residents with disabilities 5 Other Specialized Institutional Facility 6 Group home- 1-3 people with disabilities; or agency-operated apartment. 7 Group Home- 4-6 people with disabilities 8 Group Home- 7-15 people with disabilities 9 Independent home or apartment, or shared with a roommate 10 Parent/relative’s home 11 Foster care or host home (round-the-clock services
provided in a single family residence where one or more people with a disability live with a person or family who furnishes services)
BI-34a. If this person lives in an Intermediate Care Facility for persons with ID/DD (ICF/ID), a specialized institutional facility or a group home, is it publicly or privately operated? (Check ONE) 1 Public 2 Private 3 Don’t know
BI-35. Who owns or leases the place where this person lives? (Check ONE) 1 Family, guardian, or friend 2 Foster care or host family 3 Private agency 4 State or County agency 5 Person rents home (name is on the lease) 6 Person owns home (name is on the title) 7 Don't know 8 Other
BI-36. What amount of paid support does this person receive at home?
(Include any paid support, regardless of funding source) (Check ONE) 1 24-hour on-site support or supervision (people living with or being available
in his/her home during all hours that s/he is home) 2 Daily on-site support (for a limited number of hours/day, not round-the-clock) 3 Scheduled, less frequent than daily support 4 As needed visitation and phone contact 5 None of the above 6 Don’t know
Background Information
Page 27 of 83NCI Adult Consumer Survey 2014-15
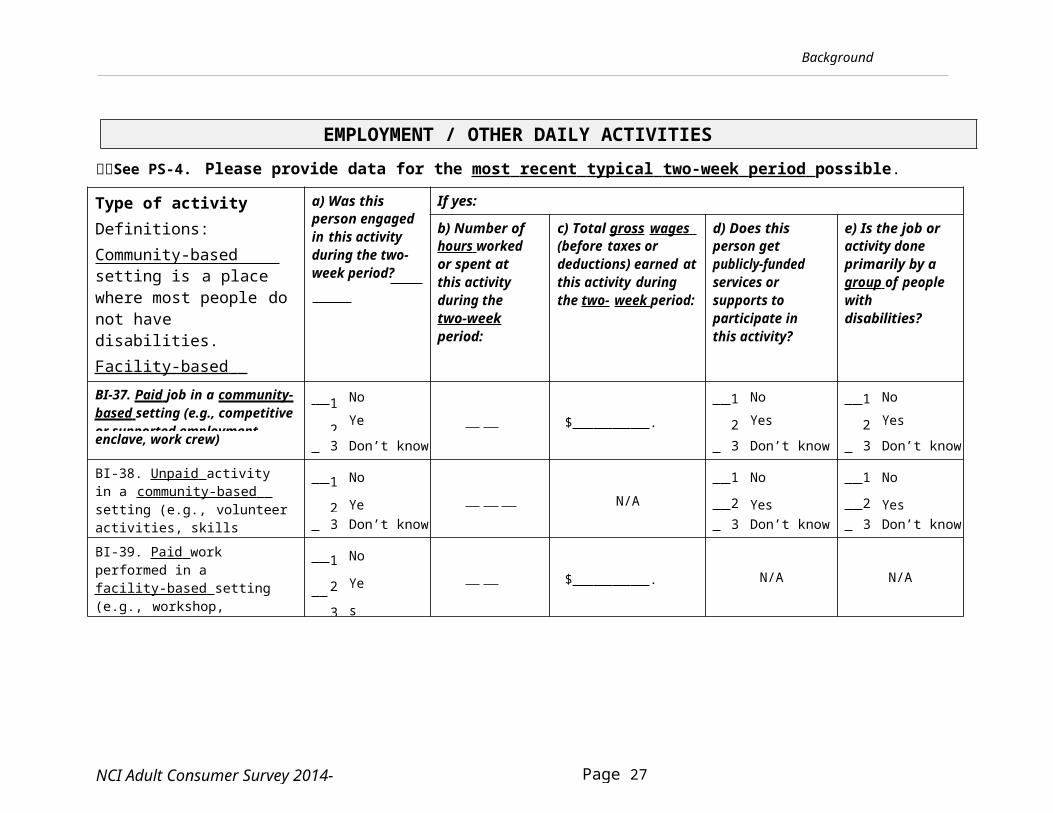
EMPLOYMENT / OTHER DAILY ACTIVITIESSee PS-4. Please provide data for the most recent typical two-week period possible.
Type of activityDefinitions:Community-based setting is a place where most people do not have disabilities.Facility-based setting is a place where most people do have disabilities.
a) Was this person engaged in this activity during the two- week period?
If yes:
b) Number of hours worked or spent at this activity during the two-week period:
c) Total gross wages (before taxes or deductions) earned at this activity during the two- week period:
d) Does this person get publicly-funded services or supports to participate in this activity?
e) Is the job or activity done primarily by a group of people with disabilities?
BI-37. Paid job in a community- based setting (e.g., competitive or supported employment,
BI-38. Unpaid activity in a community-based setting (e.g., volunteer activities, skills training)
1
2
No
Yes N/A 1
2
No
Yes
1
2
No
Yes
3 Don’t know 3 Don’t know 3 Don’t know
BI-39. Paid work performed in a facility-based setting (e.g., workshop, activity center)
1
2
3
No
Yes
Don’t know
$ . N/A N/A
Background Information
Page 28 of 83NCI Adult Consumer Survey 2014-15
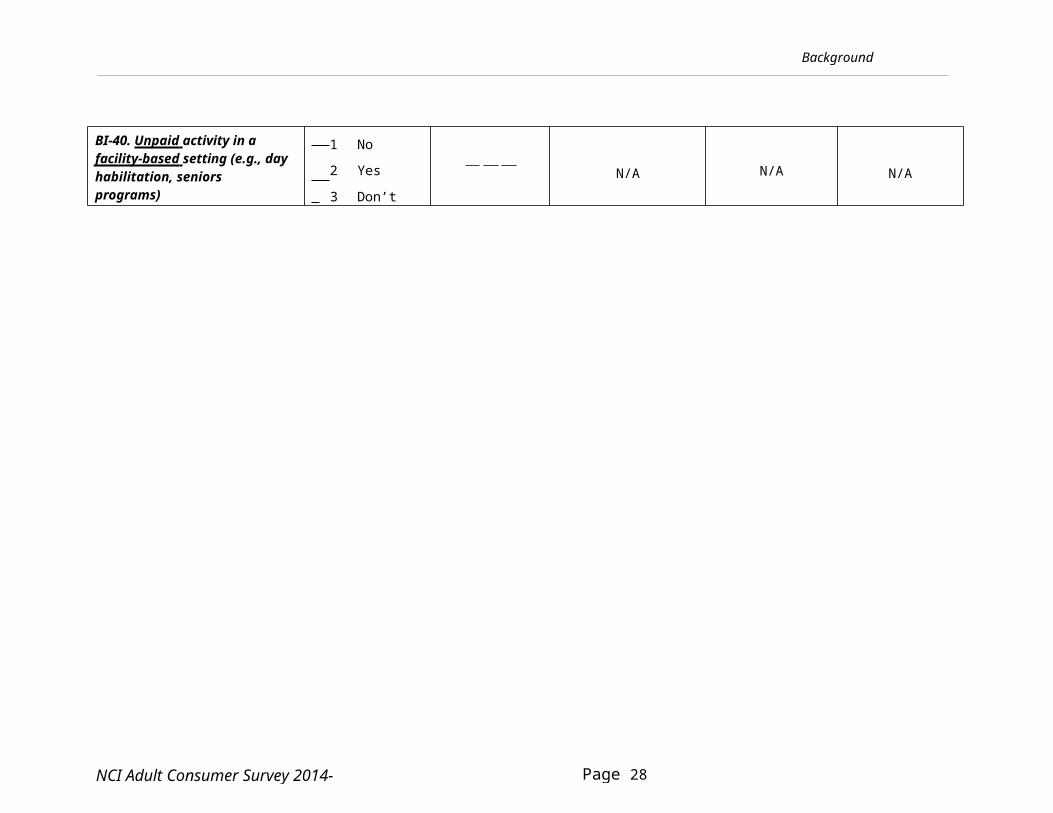
BI-40. Unpaid activity in a facility-based setting (e.g., day habilitation, seniors programs)
1 No
2 Yes
3 Don’t know
N/A N/A N/A
Background Information
Page 29 of 83NCI Adult Consumer Survey 2014-15
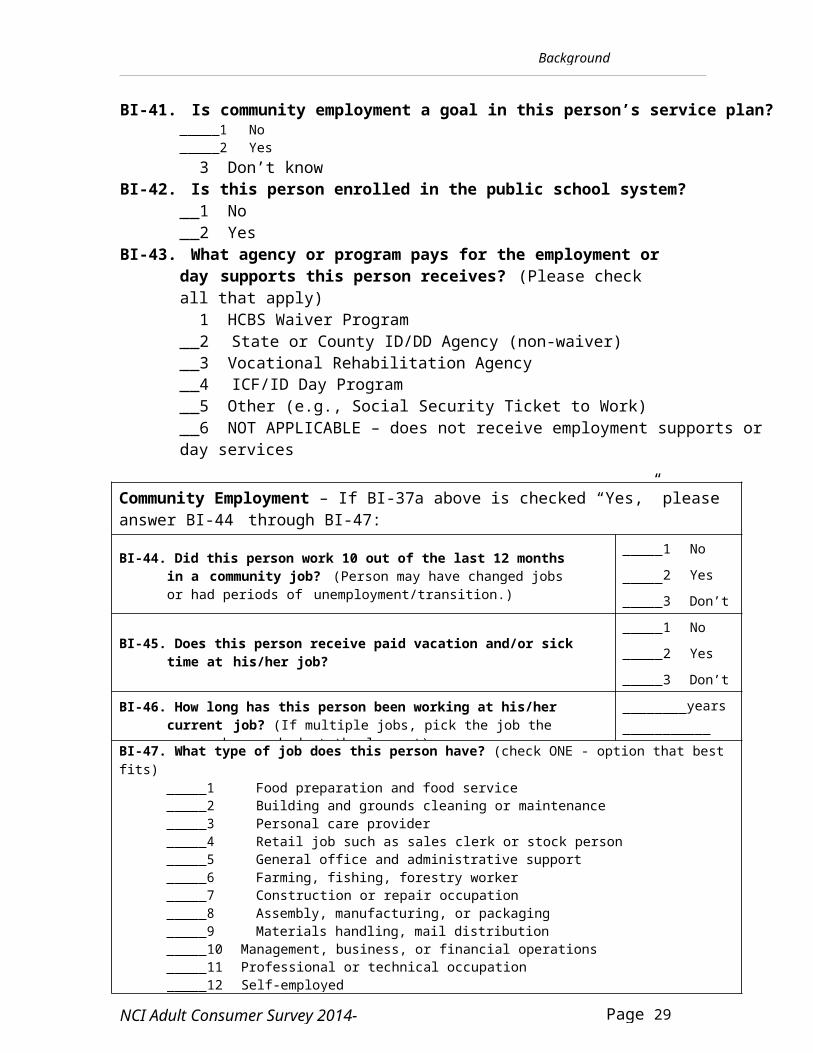
BI-41. Is community employment a goal in this person’s service plan? 1 No 2 Yes 3 Don’t know
BI-42. Is this person enrolled in the public school system? 1 No 2 Yes
BI-43. What agency or program pays for the employment or day supports this person receives? (Please check all that apply) 1 HCBS Waiver Program 2 State or County ID/DD Agency (non-waiver) 3 Vocational Rehabilitation Agency 4 ICF/ID Day Program 5 Other (e.g., Social Security Ticket to Work) 6 NOT APPLICABLE – does not receive employment supports or day services
Community Employment – If BI-37a above is checked “Yes,” please answer BI-44 through BI-47:
BI-44. Did this person work 10 out of the last 12 months in a community job? (Person may have changed jobs or had periods of unemployment/transition.)
1 No
2 Yes 3 Don’t Know
BI-45. Does this person receive paid vacation and/or sick time at his/her job?
1 No 2 Yes 3 Don’t Know
BI-46. How long has this person been working at his/her current job? (If multiple jobs, pick the job the person has worked at the longest).
years months
BI-47. What type of job does this person have? (check ONE - option that best fits) 1 Food preparation and food service 2 Building and grounds cleaning or maintenance 3 Personal care provider 4 Retail job such as sales clerk or stock person 5 General office and administrative support 6 Farming, fishing, forestry worker 7 Construction or repair occupation 8 Assembly, manufacturing, or packaging 9 Materials handling, mail distribution 10 Management, business, or financial operations 11 Professional or technical occupation 12 Self-employed 13 Other
Section I
Page 30 of 83NCI Adult Consumer Survey 2014-15
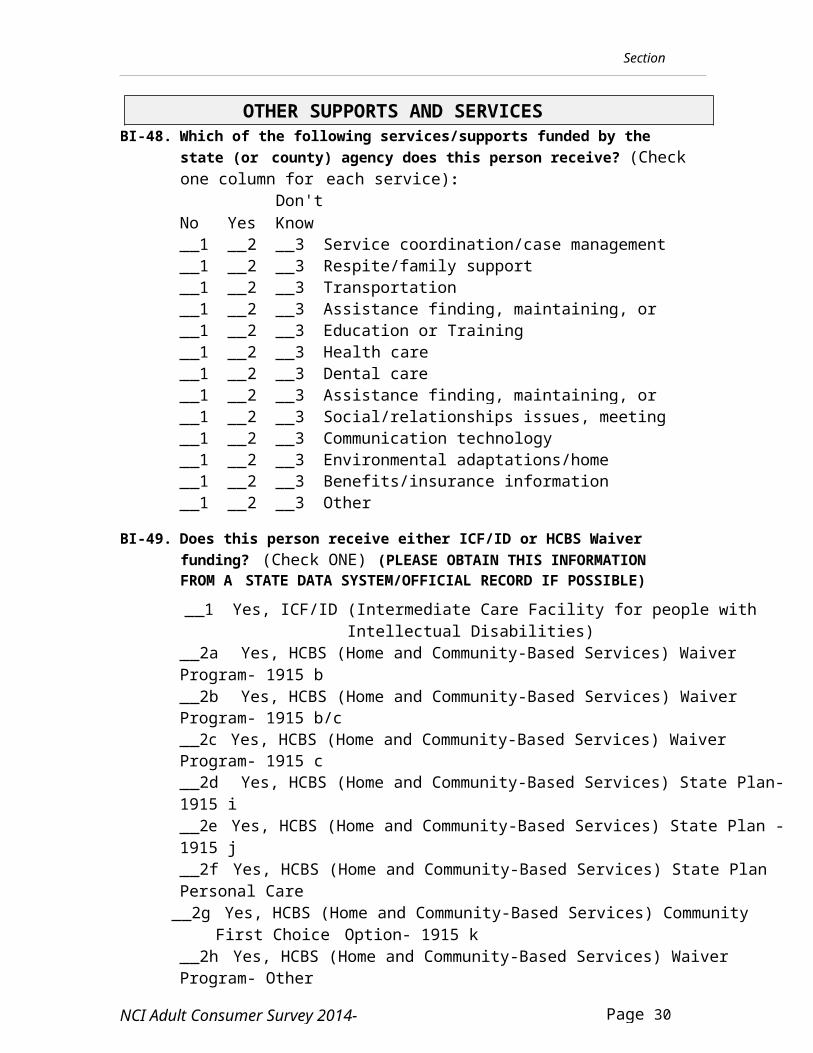
OTHER SUPPORTS AND SERVICESBI-48. Which of the following services/supports funded by the state
(or county) agency does this person receive? (Check one column for each service):
Don'tNo Yes Know 1 2 3 Service coordination/case management 1 2 3 Respite/family support 1 2 3 Transportation 1 2 3 Assistance finding, maintaining, or changing
jobs 1 2 3 Education or Training 1 2 3 Health care 1 2 3 Dental care 1 2 3 Assistance finding, maintaining, or changing
housing 1 2 3 Social/relationships issues, meeting people 1 2 3 Communication technology 1 2 3 Environmental adaptations/home
modifications 1 2 3 Benefits/insurance information 1 2 3 Other
BI-49. Does this person receive either ICF/ID or HCBS Waiver funding? (Check ONE) (PLEASE OBTAIN THIS INFORMATION FROM A STATE DATA SYSTEM/OFFICIAL RECORD IF POSSIBLE) 1 Yes, ICF/ID (Intermediate Care Facility for people with Intellectual
Disabilities) 2a Yes, HCBS (Home and Community-Based Services) Waiver Program- 1915 b 2b Yes, HCBS (Home and Community-Based Services) Waiver Program- 1915 b/c 2c Yes, HCBS (Home and Community-Based Services) Waiver Program- 1915 c 2d Yes, HCBS (Home and Community-Based Services) State Plan- 1915 i 2e Yes, HCBS (Home and Community-Based Services) State Plan - 1915 j 2f Yes, HCBS (Home and Community-Based Services) State Plan Personal Care
2g Yes, HCBS (Home and Community-Based Services) Community First Choice Option- 1915 k
2h Yes, HCBS (Home and Community-Based Services) Waiver Program- Other 2i Yes, HCBS (Home and Community-Based Services)- Other Plan or Option(including MFP)
Section I
Page 31 of 83NCI Adult Consumer Survey 2014-15
3 Don't know 4 No, receives other funding
Section I
Page 32 of 83NCI Adult Consumer Survey 2014-15
BI-50. Is this person currently using a self-directed supports option?“Self-directed” or “participant-directed” supports options offer individuals (and their representatives, including family members) the opportunity to manage some or all of their services. They may hire & fire their own support workers and/or control how their budget is spent. 1 No code BI-51 and 39-44 as NOT APPLICABLE 2 Yes 3 Don’t know code BI-51 and 39-44 as NOT APPLICABLE
BI-51. If yes, who employs this person’s support workers? 8 NOT APPLICABLE – not using self-directed/participant-directed supports 1 The person (or his/her representative) is the common-law
employer. A fiscal intermediary functions as the person’s agent to perform payroll and other responsibilities required by law.
2 An “agency with choice” is the common-law employer of the support workers selected/recruited by the individual and performs necessary payroll and human resources functions. The person (or his/her representative) is the co-employer (managing employer).
3 Don’t know
BEHAVIORAL SUPPORT NEEDS
Analyses of project data show that the extent of behavioral support needs is significantly related to many of the questions on the survey. The requested information is used to "adjust" the data in order to make valid comparisons of performance across states. The responses will not be used to identify any individual.
The person conducting this survey may ask a family member or staff person on site to fill out the questions on the following page. This information may also be obtained from service coordinators or through record review. These questions rely upon the assessment of someone who knows the individual well. Please identify the level of support the person needs to manage any of the types of behavior listed below.
Does person need support to manage:
Level of Support Needed (Check ONE)
BI-52. Self-injurious behaviorRefers to attempts to cause harm toone’s own body, for example,
1 No support needed 2 Some support needed;
requires only occasional assistance or monitoring
Section I
Page 33 of 83NCI Adult Consumer Survey 2014-15
hitting or biting self, banging head, scratching or puncturing skin, ingesting inedible substances, or attempting suicide.
3 Extensive support needed; frequent or severe enough to require regular assistance
9 Don’t KnowBI-53. Disruptive behavior Refers to behavior that interferes with the activities of others, for example, by laughing or crying without apparent reason, yelling or screaming, cursing, or threatening violence.
1 No support needed 2 Some support needed;
requires only occasional assistance or monitoring
3 Extensive support needed; frequent or severe enough to require regular assistance
9 Don’t Know
BI-54. Destructive behavior Refers broadly to externally- directed, defiant behavior, for example, taking other people’s property, property destruction, stealing, or assaults and injuries to others.
1 No support needed 2 Some support needed;
requires only occasional assistance or monitoring
3 Extensive support needed; frequent or severe enough to require regular assistance
9 Don’t Know
BI-55. Whose responsibility was it to obtain the Background Information? (check all that apply)
1 Service coordinator/case manager 2 Other state staff 3 Contractor 4 Individual being surveyed 5 Family member 6 Provider staff 7 Other
Section I
Page 34 of 83NCI Adult Consumer Survey 2014-15
SECTION I: Face-to-face Survey With Person Receiving Services and Supports
General Instructions:
This section may only be completed by directly surveying the person receiving services and supports.
Prior to the survey, surveyors should use the pre-survey form to fill in the blanks throughout the survey. Using familiar names and terms during the survey will help ensure that the person understands the questions. Questions that refer to pre-survey information are indicated with a bell symbol:
Do not use responses from any other person to complete this section. If possible, the survey should be conducted in private. Others
may be present if the individual requests, or if another person is needed for interpretation purposes. If staff believe that a private survey may pose risks to surveyors, then staff should be present. If others are providing assistance, surveyors should emphasize that we are trying to find out the individual's perspective.
Be sure to read all instructions carefully. Help the person with any words that are not understood. You
may repeat or rephrase questions to improve understanding. Some questions have suggested rephrasing in italics - you do not need to limit yourself to these suggestions.
Do not read or show the list of response options to the individual. Let them answer in their own words and then code the most appropriate response.
Individuals may skip any question. If the person receiving services does not respond to a question or gives an unclear response, code the question as “9.”
If you have any questions concerning the intent of a survey question or need additional help in rephrasing a question, refer to the list of Core Indicators in your training packet.
A wide margin is provided for recording notes as necessary. Just be sure your response choices are clearly marked.
Please fill out the Surveyor Feedback Sheet after each interview.
Section I
Page 35 of 83NCI Adult Consumer Survey 2014-15
Take a few minutes to introduce yourself and make the person feel comfortable. Read or paraphrase the following introduction. Pause after each statement, making sure the respondent understands.
“Hi, my name is . I'm from , and I'm here to ask you some questions about where you live, where you work, your friends and family, and the people who help you. By answering these questions, you are helping us figure out how people in (State) are doing, and how to make supports and services better.”
“This is not a test, and there are no right or wrong answers to these questions. If you don't understand a question, let me know and I'll try to explain it. It's okay if you don't know how to answer. Whatever answers you give, you will not get into trouble and no one will be mad at you.”
“You don't have to answer any questions that you don't want to. Just tellme if you don't want to answer.”
“I'd like to know your opinions, how you feel about things. Whatever you tell me will be kept private, so you can be honest.”
Note: Before beginning Section I, make sure that the appropriate consent has been received from the individual or guardian (see questions below).
Consent Questions:
#CQ1. (Required)- Did the individual or legal guardian give consent toparticipate in this survey?
Yes No
If required in your state, please answer the following questions (otherwise leave blank).
#CQ2. Did individual/legal guardian give verbal consent for the surveyorto contact him/her?
Yes No
#CQ3. Is the signature of a legal guardian required for this individual toconsent to participation in this survey?
Yes No
#CQ4. If required, did individual/legal guardian give written consent to be surveyed?
Yes No
Section I
Page 36 of 83NCI Adult Consumer Survey 2014-15
EMPLOYMENT / OTHER DAILY ACTIVITIES
I’d like to start by asking you about what you do during theday – if you have a job or other place that you go to.
1) Do you have a paid job in the community?A community job refers to paid work - either competitive or supported employment (includes both individual and group employment, such as a work crew or enclave). It does not include work done in facility-based settings like sheltered workshops. It also does not include volunteer work.
PS-8 (Do you work at ?)
2 Yes code Question 2 as NOT APPLICABLE 0 No ask Question 2 9 Don’t know, no response, unclear response
2) If No, ask: Would you like to have a job in the community?
8 NOT APPLICABLE – has job in the community 2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
If person does not have a job in the community, code Questions 3-4 as NOT APPLICABLE.
3) Do you like working there?
8 NOT APPLICABLE – no job in the community 2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
Section I
Page 37 of 83NCI Adult Consumer Survey 2014-15
4) Would you like to work somewhere else? (Would you like a different job instead of this one?)
8 NOT APPLICABLE – no job in the community 2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
5) Do you go to a day program or do some other regularly scheduled activity during the day? This does not include a job in the community. Examples of an “other regularly scheduled activity” could include volunteering, a sheltered workshop, or attending a senior program.
PS-9 (Do you go to ?)
2 Yes 0 No code Questions 6-7 as NOT APPLICABLE 9 Don’t know, no response, unclear response
6) Do you like going there/doing this activity?
8 NOT APPLICABLE – no day program or other activity 2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
7) Would you like to go somewhere else or do something else during the day?
8 NOT APPLICABLE – no day program or other activity 2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
Section I
Page 38 of 83NCI Adult Consumer Survey 2014-15
8) Do you do any volunteer work? Do not include instances where individual is made or forced to spend time ‘volunteering.’ Volunteer work is not paid.
2 Yes 0 No 9 Don’t know, no response, unclear response
HOMENow I'm going to ask you about where you live.
9) Do you like your home or where you live? (Do you like living here?)
2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
10) Would you like to live somewhere else?
2 Yes 1 In-between 0 No 9 Don’t know, no response, unclear response
11) Do you ever talk with your neighbors?
2 Yes, often (weekly or more) 1 Yes, but not often 0 No, or very rarely 9 Don’t know, no response, unclear response
Section I
Page 39 of 83NCI Adult Consumer Survey 2014-15
12) Do people let you know before they come into your home? (Do they ring the doorbell or knock first and wait for an answer?) Do not include people who live in the home.
2 Yes 1 Sometimes 0 No 9 Don’t know, no response, unclear response, or
people do not come into your home
13) Do people let you know before coming into your bedroom?
2 Yes 1 Sometimes 0 No 9 Don’t know, no response, unclear response, or
people do not come into your bedroom
14) Do you have enough privacy at home? (Can you have time to yourself?) If person lives alone, code Q14 as NOT APPLICABLE.Here we are looking at privacy (e.g. going in a room and closing the door), not the person's need for supervision (e.g. staying home alone).
8 NOT APPLICABLE - lives alone 2 Yes, has enough privacy 0 No, would like more privacy 9 Don’t know, no response, unclear response
SAFETYNow I’m going to ask you some personal questions about your safety. Remember, you do not have to answer any questions that you do not want to.15) Are you ever afraid or scared when you are at home?
2 [Yes] - most of the time 1 Sometimes 0 [No] - rarely 9 Don’t know, no response, unclear response
Section I
Page 40 of 83NCI Adult Consumer Survey 2014-15
16) Are you ever afraid or scared when you are out in your neighborhood?
2 [Yes] - most of the time 1 Sometimes 0 [No] - rarely 9 Don’t know, no response, unclear response
17) Are you ever afraid or scared at work or at your day program/other activity?
8 NOT APPLICABLE – no work or day program/activity 2 [Yes] - most of the time 1 Sometimes 0 [No] - rarely 9 Don’t know, no response, unclear response
18) If you ever feel afraid, is there someone you can talk to?Please ask question to all respondents.
2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
FRIENDS AND FAMILYNow I'm going to ask you about friends and family.
19) Do you have friends you like to talk to or do things with?If s/he answers "yes," ask who the friends are and try to determine if they are family, staff, roommates, co-workers, etc. You can use prompts such as: Can you tell me their names? Are these friends staff or your family?
2 Yes, has friends who are not staff or family 1 Yes, all friends are staff or family, or cannot determine 0 No, does not have friends 9 Don’t know, no response, unclear response
Section I
Page 41 of 83NCI Adult Consumer Survey 2014-15
20) Do you have a best friend, or someone you are really close to? (Is there someone you can talk to about personal things?) Can include staff or family member.
2 Yes 0 No 9 Don’t know, no response, unclear response
If the person responds "NO" TO BOTH QUESTIONS 19AND 20, code Question 21 as "NOT APPLICABLE."
21) Can you see your friends when you want to see them? (Can you make plans with your friends when you want to?)We are trying to determine if person gets support to see friends. Try to factor out situations where friends are not available – this is not the issue.
8 NOT APPLICABLE – does not have any friends 2 Yes, can see friends whenever s/he wants to 1 Sometimes can’t see friends (e.g., not enough staff or
transportation) 0 No, often unable to see friends 9 Don’t know, no response, unclear response
22) Can you go on a date if you want to?
8 NOT APPLICABLE – does not want to date 2 Yes, can date, or is married or living with partner 1 Yes, but there are some restrictions or rules about dating 0 No 9 Don’t know, no response, unclear response
23) Do you ever feel lonely? (Do you ever feel like you don’t have anyone to
talk to?)If s/he responds “yes,” probe to determine how often s/he feels lonely.
2 [Yes] – often feels lonely (more than half the time) 1 Sometimes (about half the time) 0 [No] – not often (less than half the time) 9 Don’t know, no response, unclear response
Section I
Page 42 of 83NCI Adult Consumer Survey 2014-15
24) Do you have family that you see?If the person lives with family, ask about other family members that do not live in the home.
2 Yes 0 No 9 Don’t know, no response, unclear response
25) Can you see your family when you want to? (Can you pick the times you see them? Does someone help you make plans to see them?)If family is not available or does not wish to have contact, code as NOT APPLICABLE. If the person has family but does not want to see them, code as 2.
8 NOT APPLICABLE – family not available, person does not have family or family does not wish to have contact
2 Yes, sees family whenever s/he wants to, or chooses not to see family
1 Sometimes 0 No 9 Don’t know, no response, unclear response
26) Can you help other people if you want to? (Can you show other people how to do things if you want to?)
2 Yes 1 Sometimes 0 No 9 Don’t know, no response, unclear response
SATISFACTION WITH SERVICES/SUPPORTSNow I’m going to ask you some questions about your services.
ASK QUESTIONS 27 and 30-32 ONLY IF PERSON HAS A CASEMANAGER/ SERVICE COORDINATOR. If person does not have a case manager/ service coordinator, code these questions as "NOT APPLICABLE".
Section I
Page 43 of 83NCI Adult Consumer Survey 2014-15
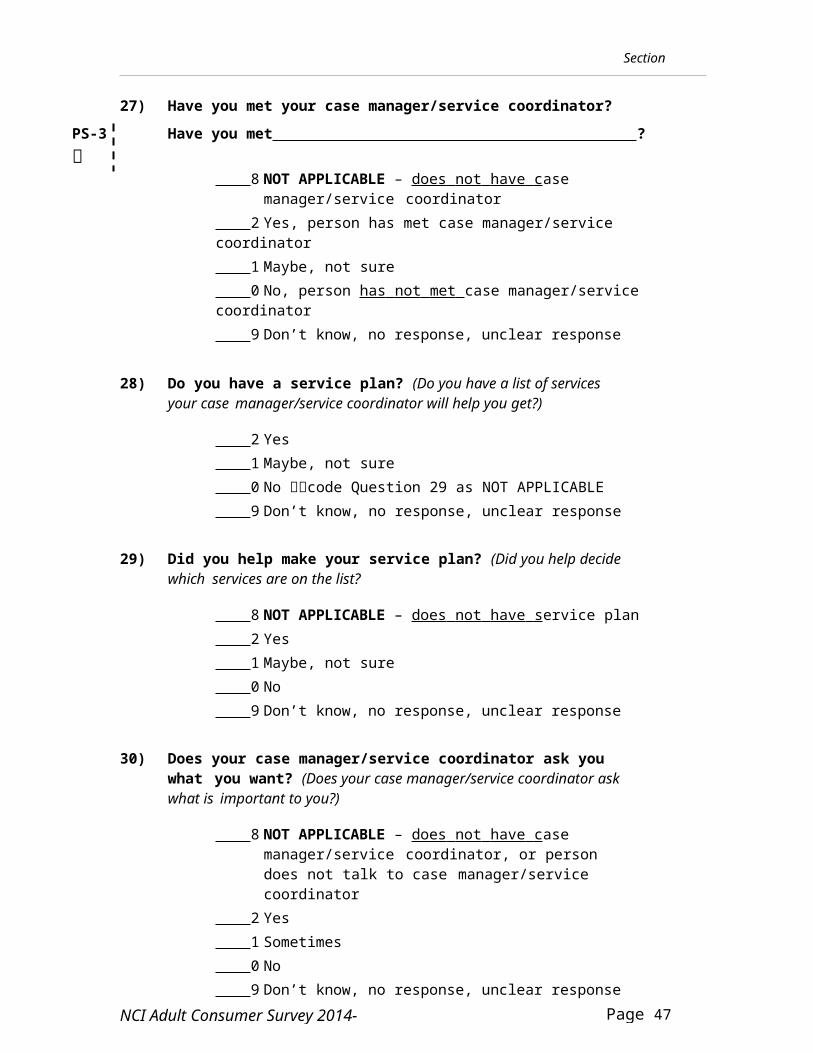
27) Have you met your case manager/service coordinator?PS-3 Have you met ?
8 NOT APPLICABLE – does not have case manager/service coordinator
2 Yes, person has met case manager/service coordinator 1 Maybe, not sure 0 No, person has not met case manager/service coordinator 9 Don’t know, no response, unclear response
28) Do you have a service plan? (Do you have a list of services your case manager/service coordinator will help you get?)
2 Yes 1 Maybe, not sure 0 No code Question 29 as NOT APPLICABLE 9 Don’t know, no response, unclear response
29) Did you help make your service plan? (Did you help decide which services are on the list?
8 NOT APPLICABLE – does not have service plan 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
30) Does your case manager/service coordinator ask you what you want? (Does your case manager/service coordinator ask what is important to you?)
8 NOT APPLICABLE – does not have case manager/service coordinator, or person does not talk to case manager/service coordinator
2 Yes 1 Sometimes 0 No 9 Don’t know, no response, unclear response
Section I
Page 44 of 83NCI Adult Consumer Survey 2014-15
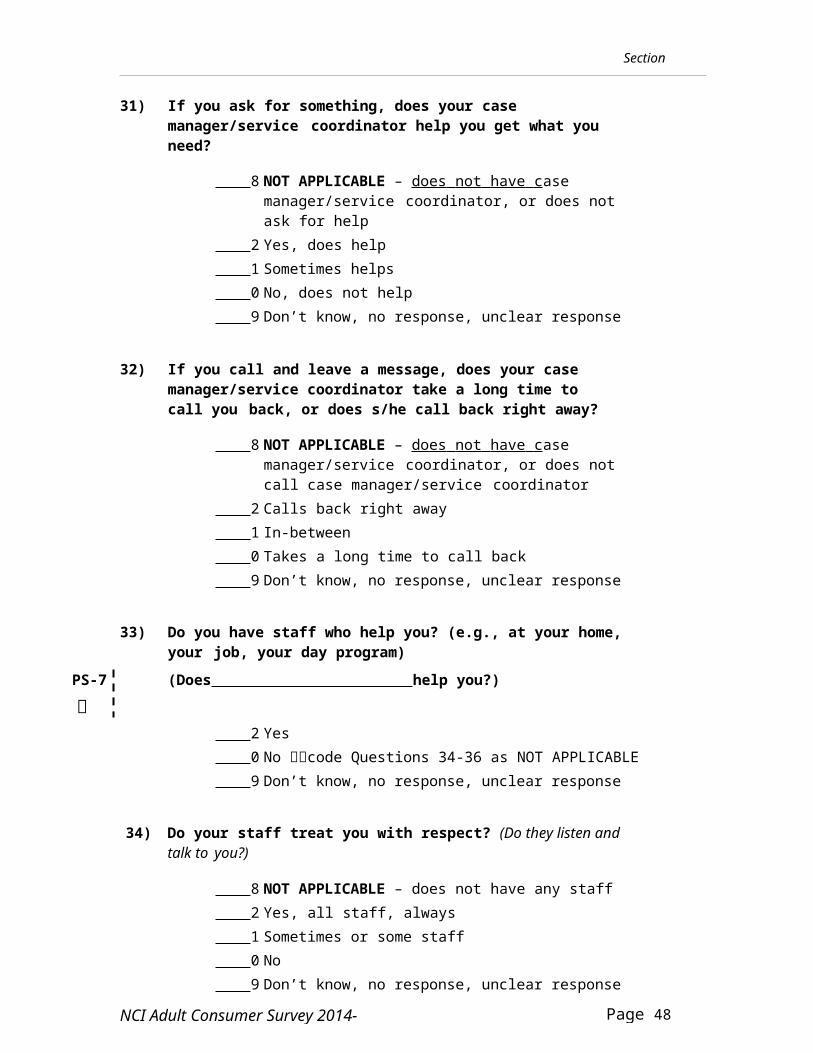
31) If you ask for something, does your case manager/service coordinator help you get what you need?
8 NOT APPLICABLE – does not have case manager/service coordinator, or does not ask for help
2 Yes, does help 1 Sometimes helps 0 No, does not help 9 Don’t know, no response, unclear response
32) If you call and leave a message, does your case manager/service coordinator take a long time to call you back, or does s/he call back right away?
8 NOT APPLICABLE – does not have case manager/service coordinator, or does not call case manager/service coordinator
2 Calls back right away 1 In-between 0 Takes a long time to call back 9 Don’t know, no response, unclear response
33) Do you have staff who help you? (e.g., at your home, your job, your day program)
PS-7 (Does help you?)
2 Yes 0 No code Questions 34-36 as NOT APPLICABLE 9 Don’t know, no response, unclear response
34) Do your staff treat you with respect? (Do they listen and talk to you?)
8 NOT APPLICABLE – does not have any staff 2 Yes, all staff, always 1 Sometimes or some staff 0 No 9 Don’t know, no response, unclear response
Section I
Page 45 of 83NCI Adult Consumer Survey 2014-15
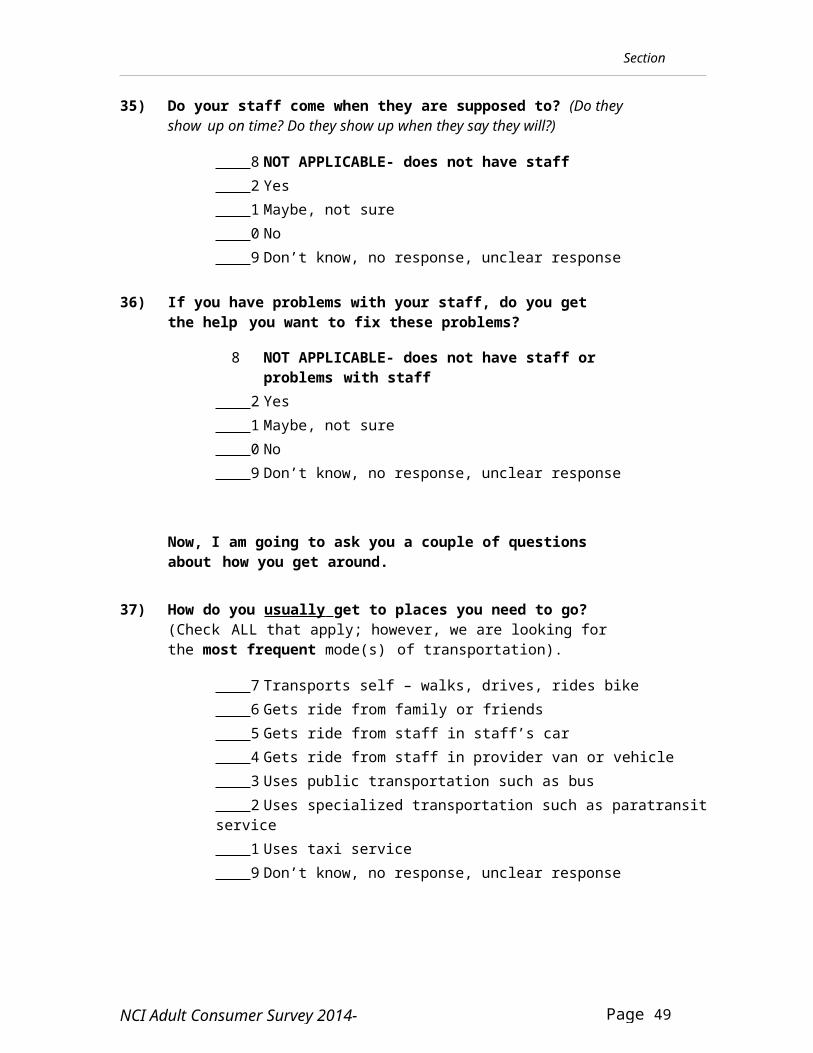
35) Do your staff come when they are supposed to? (Do they show up on time? Do they show up when they say they will?)
8 NOT APPLICABLE- does not have staff 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
36) If you have problems with your staff, do you get the help you want to fix these problems?
8 NOT APPLICABLE- does not have staff or problems with staff
2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
Now, I am going to ask you a couple of questions about how you get around.
37) How do you usually get to places you need to go? (Check ALL that apply; however, we are looking for the most frequent mode(s) of transportation).
7 Transports self – walks, drives, rides bike 6 Gets ride from family or friends 5 Gets ride from staff in staff’s car 4 Gets ride from staff in provider van or vehicle 3 Uses public transportation such as bus 2 Uses specialized transportation such as paratransit service 1 Uses taxi service 9 Don’t know, no response, unclear response
Section I
Page 46 of 83NCI Adult Consumer Survey 2014-15
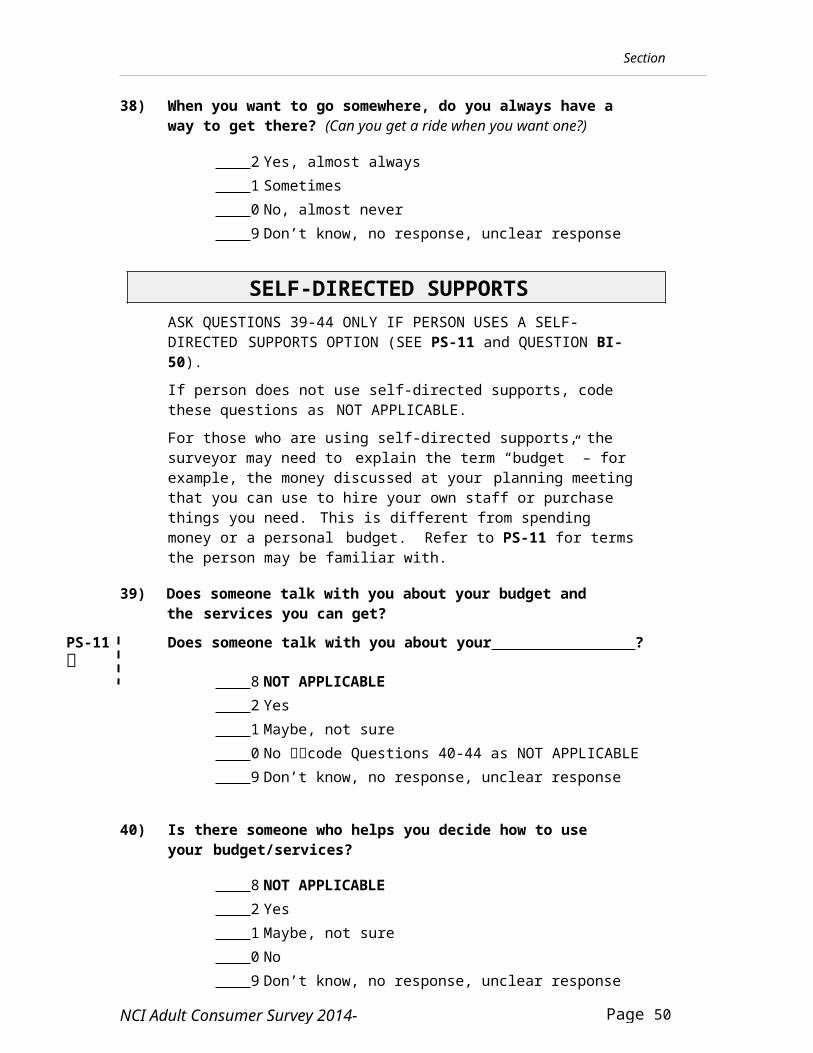
38) When you want to go somewhere, do you always have a way to get there? (Can you get a ride when you want one?)
2 Yes, almost always 1 Sometimes 0 No, almost never 9 Don’t know, no response, unclear response
SELF-DIRECTED SUPPORTSASK QUESTIONS 39-44 ONLY IF PERSON USES A SELF-DIRECTED SUPPORTS OPTION (SEE PS-11 and QUESTION BI-50).If person does not use self-directed supports, code these questions as NOT APPLICABLE.For those who are using self-directed supports, the surveyor may need to explain the term “budget” – for example, the money discussed at your planning meeting that you can use to hire your own staff or purchase things you need. This is different from spending money or a personal budget. Refer to PS-11 for terms the person may be familiar with.
39) Does someone talk with you about your budget and the services you can get?
PS-11 Does someone talk with you about your ?
8 NOT APPLICABLE 2 Yes 1 Maybe, not sure 0 No code Questions 40-44 as NOT APPLICABLE 9 Don’t know, no response, unclear response
40) Is there someone who helps you decide how to use your budget/services?
8 NOT APPLICABLE 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
Section I
Page 47 of 83NCI Adult Consumer Survey 2014-15
41) Can you make changes to your budget/services if you need to? (Can you decide to buy something different?)
8 NOT APPLICABLE 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
42) Do you want more help deciding how to use your budget/services, or do you have enough help?
8 NOT APPLICABLE 2 [Yes] – want more help 1 Maybe, not sure 0 [No] – have enough help 9 Don’t know, no response, unclear response
43) Do you get information about how much money is left in your budget/services?
PS-11 Do you get information from (financial management service)?
8 NOT APPLICABLE 2 Yes 1 Maybe, not sure 0 No code Question 44 as NOT APPLICABLE 9 Don’t know, no response, unclear response
44) If yes, is the information easy to understand?
8 NOT APPLICABLE 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response
Section I
Page 48 of 83NCI Adult Consumer Survey 2014-15
45) Surveyor : Could Section I be completed?
1 Yes, person answered independently or with some assistance
2 Yes, person answered using alternate/picture response format
3 No, person could not communicate sufficiently to complete this section
4 No, person was unwilling to participate 5 No, other reason
46) Surveyor : In your opinion, did the individual appear to understand most of the questions or not?
8 NOT APPLICABLE – did not complete Section I 2 Yes, appeared to understand most questions
(even if prompted) and could give an opinion 1 Not sure 0 No, appeared to have very little
understanding or comprehension
47) Surveyor : In your opinion, did the individual seem to answer the questions in a consistent manner? (Do you feel his/her responses were valid?)
8 NOT APPLICABLE – did not complete Section I 2 Yes, seemed to give consistent and valid responses 1 Not sure 0 No, did not seem to give consistent and valid responses
If you answered "yes" to questions 45-47, then determine now if s/he is willing to answer more questions. If the individual is not willing to continue, or if you believe comprehension or consistency was a problem and person does not have a proxy respondent, then say:
“Thank you for your help. It's been very nice talking to you. You've been very helpful.”
If the person is willing to continue or has a proxy respondent available, please continue to Section II.
Section II
Page 49 of 83NCI Adult Consumer Survey 2014-15
SECTION II: Survey with the Person Receiving Services or with Proxy Respondents
STOP - Please review Section 1 questions #45-47. Please make sure you have answered those questions before proceeding.
Ask the person receiving services the Section II questions if all possible. If the person is unwilling or unable to complete this section, other respondents may be surveyed (family, advocate, staff; however not the case manager or service coordinator). If the individual did not complete Section 1 or if you believe that s/he did not understand the questions and/or did not answer consistently, do not ask the individual the Section II questions…only ask the proxy respondent(s). Proxy respondents must be knowledgeable in the areas below (they should know the person well and have frequent contact with him/her). Use the alternate wording provided when questioning proxy respondents (e.g., ‘Did this person…?’).
For all questions, indicate who the respondent was; please check only one respondent for each question.
If both the individual and the proxy respondent contributed to the answer, and there is agreement between the two, check “individual” as the respondent.
If there is disagreement between the individual and the proxy respondent, you may need to ask follow up questions to determine the most valid response.
Ask the person if s/he wishes to continue with the questions, or if s/he would like to take a short break.
Section II
Page 50 of 83NCI Adult Consumer Survey 2014-15
COMMUNITY INCLUSIONIn this section, we are trying to find out if the person participates in integrated community activities (including people with and without disabilities). If the individual indicates they have only participated in a non-integrated activity (where only people with disabilities are participating) in the past month, then you should check ‘no’ as the response. If the person answers "yes," you may ask for an example to verify that the person understood the question and that the activity was indeed integrated.
48) In the past month, did you go shopping? (Examples: groceries, clothing) (Other respondent: In the past month, did this person go shopping?)
2 Yes 0 No 9 Don’t know, no response, unclear response
48a) If yes, how many times in the past month? times in past month
48b) If yes, who did you usually go with?(Check ALL that apply)
1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
49) In the past month, did you go out on errands or appointments?(Examples: bank, post office, hair dressers/barber)(Other respondent: In the past month, did this person go out on errands or appointments?)
2 Yes 0 No 9 Don’t know, no response, unclear response
Section II
Page 51 of 83NCI Adult Consumer Survey 2014-15
49a) If yes, how many times in the past month? times in past month
49b) If yes, who did you usually go with?(Check ALL that apply) 1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
50) In the past month, did you go out for entertainment? (Examples: movies, plays, concerts, attend sporting events)(Other respondent: In the past month, did this person go out for entertainment?)
2 Yes 0 No 9 Don’t know, no response, unclear response
50a) If yes, how many times in the past month? times in past month
50b) If yes, who did you usually go with?(Check ALL that apply)
1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
Section II
Page 52 of 83NCI Adult Consumer Survey 2014-15
51) In the past month, did you go out to a restaurant or coffee shop? (Other respondent: In the past month, did this person go out to a restaurant or coffee shop?)
2 Yes 0 No 9 Don’t know, no response, unclear response
51a) If yes, how many times in the past month? times in past month
51b) If yes, who did you usually go with?(Check ALL that apply) 1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
52) In the past month, did you go out to a religious service or spiritual practice? (Examples: church, synagogue, study or other place of worship)(Other respondent: In the past month, did this person go out to a religious service or spiritual practice?)
2 Yes 0 No 9 Don’t know, no response, unclear response
52a) If yes, how many times in the past month? times in past month
Section II
Page 53 of 83NCI Adult Consumer Survey 2014-15
52b) If yes, who did you usually go with?(Check ALL that apply) 1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
53) In the past month, did you go out for exercise? (Examples: jogging, swimming, riding bike, YMCA, gym/health club). Reminder: We’re looking for if the individual exercised in an integrated setting.(Other respondent: In the past month, did this person go out for exercise?)
2 Yes 0 No 9 Don’t know, no response, unclear response
53a) If yes, how many times in the past month? times in past month
53b) If yes, who did you usually go with?(Check ALL that apply) 1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
54) In the past year, did you go away on a vacation?(Other respondent: In the past year, did this person go away on a vacation?)
2 Yes 0 No 9 Don’t know, no response, unclear response
Section II
Page 54 of 83NCI Adult Consumer Survey 2014-15
54a) If yes, how many times in the past year? times in past year
54b) If yes, who did you usually go with?(Check ALL that apply) 1 Alone 2 Friends or family 3 House-mates or co-workers 4 Staff 5 Others not listed 9 Don’t know, no response, unclear response
Section II
Page 55 of 83NCI Adult Consumer Survey 2014-15
CHOICES
The intent of these questions is to determine the extent to which persons receiving services are involved in decision-making.
In this section, code “2” if this person played a major role in making the decision. The person may have consulted with others but ultimately made the decision for him/herself.
Code “1” if the person had some input in making the decision but did not play a major role.
Code “0” if the person did not have input in making the decision. Choices made with spouses/partners should be coded as “2- person
madethe choice”.
Do not overuse the "NOT APPLICABLE" code here. It is not appropriate to use "8" to indicate NOT ALLOWED or NOT CAPABLE of making decisions in this area. For those cases, code “0”.
Read one of the following introductions to the respondent(s):For Individuals:I'm going to ask some questions now about some decisions you may have made or helped make. For each question, I'd like you to tell me if you made the choice yourself, if you had some say about it, or if someone else decided for you.For Proxy Respondents:I'm going to ask some questions now about decisions this person may have made. For each question, please indicate if s/he made the decision, if s/he had some input in making the decision, or if someone else made the decision for him/her.
55) Who chose (or picked) the place where you live? (Did you help pick the place where you live?)(Other respondent: Who chose the place where s/he lives? Did s/he have any input in making the decision?)If the person lives in their family home, please code Q55 as “8- NOTAPPLICABLE”
8 NOT APPLICABLE – person lives in the family home 2 Person made the choice 1 Person had some input 0 Someone else chose 9 Don’t know, no response, unclear response
56) Did you choose (or pick) the people you live with (or did you choose to live by yourself)? (Did anyone ask you who you’d liketo live with? Were you given choices, did you get to interview people?)PS-6 Did you choose to live with ?
(Other respondent – Did this person choose any of the people s/he lives with?Or: Did this person choose to live alone?)If the person lives in their family home, please code Q56 as “8- NOTAPPLICABLE”
8 NOT APPLICABLE – person lives in the family home 2 Yes, chose people s/he lives with, or chose to live alone 1 Chose some people or had some input 0 No, someone else chose 9 Don’t know, no response, unclear response
Section II
Page 57 of 83NCI Adult Consumer Survey 2014-15
57) Who decides your daily schedule (like when to get up, when to eat, when to go to sleep)?(Other respondent – Who decides this person’s daily schedule, like when to getup, when to eat, when to go to sleep?)
2 Person decides 1 Person has help deciding 0 Someone else decides 9 Don’t know, no response, unclear response
58) Who decides how you spend your free time (when you are not working, in school or at the day program)?(Other respondent – Who decides how this person spends his/her free time?)
Question 59 refers to choices made concerning paid work in the community.
59) Who chose (or picked) the place where you work? (Did youhelp make the choice?)
PS-8 Did you choose to work at ? (Other respondent: Who chose the place where s/he works?
Did s/he have any input in making the decision?)
8 NOT APPLICABLE – no job in the community 2 Person made the choice 1 Person had some input 0 Someone else chose 9 Don’t know, no response, unclear response
Question 60 refers to choices made concerning day programs or other regularly scheduled activities during the day. This does not include paid work in the community.
60) Who chose (or picked) where you go during the day? (Did youhelp make the choice?)
PS-9 Did you choose to go to ? (Other respondent: Who chose the place where s/he goes
during the day? Did s/he have any input in making the decision?)
8 NOT APPLICABLE – no day program or other activity 2 Person made the choice 1 Person had some input 0 Someone else chose 9 Don’t know, no response, unclear response
61) Do you choose what you buy with your spending money?Do not include things like rent or groceries.(Other respondent – Does this person choose how to spend his/her money?)
63) Do you choose (or pick) your staff? (Do you get to interview them?Did you get to meet different people or was someone assigned to you? Could yourequest someone different?)
PS-7
Did you choose to work with you?(Other respondent – Does this person choose his/her staff?)
8 NOT APPLICABLE - no staff 2 Yes, person choose staff 1 Staff are assigned but can be changed if
requested by person 0 No, someone else chose 9 Don’t know, no response, unclear response
RIGHTS
64) Do people read your mail or email without asking you first?(Other respondent – Does anyone read this person’s mail or email withoutpermission?)
8 NOT APPLICABLE - does not get mail/email 2 [Yes] – mail/email is read without permission 0 [No] – person reads own mail/email or others
read with permission 9 Don’t know, no response, unclear response
Section II
Page 61 of 83NCI Adult Consumer Survey 2014-15
65) Can you be alone with friends or visitors at your home, or does someone have to be with you? (Are there rules about having friends or visitors in your home?)
(Other respondent – can this person have privacy to be alone with friends when s/he wants to, or does someone else have to be present?)
8 NOT APPLICABLE – no friends or visitors, or no friends visit your home
2 Can be alone with friends or visitors 0 There are rules against being alone with friends or visitors 9 Don’t know, no response, unclear response
66) Are you allowed to use the phone and internet when you want to?If person is unable to use the phone or internet, or doesn’t have access, code as “NOT APPLICABLE.”
(Other respondent – is this person allowed to use the phone or internet when s/he wants to?)
8 NOT APPLICABLE - doesn’t have access or unable to usephone/internet
2 Yes, can use anytime, either independently or with assistance
0 No, there are rules/restrictions on use of phone/internet 9 Don’t know, no response, unclear response
Section II
Page 62 of 83NCI Adult Consumer Survey 2014-15
67) Have you ever participated in a self-advocacy group meeting, conference, or event? (A self-advocacy group is where people with disabilities meet together to talk about things in their lives that are important to them. Some groups include People First, Speaking for Ourselves, and Self-Advocates Becoming Empowered – SABE. Do not include human rights groups sponsored by provider agencies.)
PS-10 (Have you ever gone to a meeting or event?) (Other respondent – Has this person ever attended a self-
2 Yes code Question 68a as NOT APPLICABLE 1 Sometimes, or doesn’t get enough of the services needed 0 No 9 Don’t know, no response, unclear response
Section II
Page 63 of 83NCI Adult Consumer Survey 2014-15
68a) If additional services are needed, please note type of service or support below: (check all that apply):
0 NOT APPLICABLE - does not need additional services 1 Service coordination/case management 2 Respite/family support 3 Transportation 4 Assistance finding, maintaining, or changing jobs 5 Education or training 6 Health care 7 Dental care 8 Assistance finding, maintaining, or changing housing 9 Social/relationship issues, meeting people 10 Communication technology 11 Environmental adaptations/home modifications 12 Benefits/insurance information 13 Other
69) Do you feel your staff have the right training to meet your needs? (Other respondent – Does this person’s support staff have the right training to meeting his/her needs?)
8 NOT APPLICABLE- person does not have support staff 2 Yes 1 Maybe, not sure 0 No 9 Don’t know, no response, unclear response, or
respondent is staff
Section II
Page 64 of 83NCI Adult Consumer Survey 2014-15
70) Overall, how would you describe your health?(Other respondent: Overall, how would you describe this person’s health?)
Respondent: ( ) 1-individual ( ) 2-family/friend ( ) 3-staff ( ) 4-other 1 Excellent 2 Very good 3 Fairly good 4 Poor 9 Don’t know, no response, unclear response
71) Surveyor : Please indicate all respondents to Section II(check all that apply):
1 Person receiving services 2 Advocate, Parent, Guardian, Personal
Representative, Relative, Friend 3 Staff who provides supports where person lives 4 Staff who provides supports at a day or other
service location 5 Other
Interviewer Feedback
Page 65 of 83NCI Adult Consumer Survey 2014-15
SURVEYOR FEEDBACK SHEETInstructions to surveyors:
Please take a few minutes to complete a feedback sheet after each survey you complete. Please DO NOT INCLUDE any personally identifying information regarding yourself or the individual surveyed (e.g., names, addresses, phone numbers, etc.).Surveyor’s Initials or Code (optional): 1. How long did it take to complete the direct face-to-face survey(s)
(Sections I and II only)? Hours Minutes
2. How long did it take to complete the entire form, including phone-calls, collecting background information, arranging and conducting the face-to-face survey, travel time, etc.?
Hours Minutes3. Were there any questions that were problematic?
Yes NoIf yes, indicate the question number(s) below and describe the problem and any suggestions you have for improvement. REMEMBER: Please DO NOT INCLUDE any personally identifying information regarding yourself or the individual surveyed.
Question: Problem/Suggestions:
Interviewer Feedback
Page 66 of 83NCI Adult Consumer Survey 2014-15
Other Comments:
Additional Questions for Surveyor(s):
I-1. Where was the face-to-face survey held? (Check ALL that apply)
1 Person’s home 2 Person’s workplace 3 Provider agency (e.g., provider agency office; not a home or workplace) 4 Public place 5 Other
I-2. What is your job title/relationship to the State agency (or County agency if applicable)? (If there is more than one surveyor, check ALL that apply. If a surveyor has more than one role, select the principal role for the state agency.)
1 Quality Assurance staff 2 Case manager/service coordinator 3 Contractor or consultant 4 Person receiving services/self-advocate 5 Parent/family member/guardian of a person receiving services 6 Student 7 Interested citizen (not a family member or provider) 8 Other
I-3. Did you know/have you met the individual prior to conducting this survey?
1 No 2 Yes 3 Not sure
Interviewer Feedback
Page 67 of 83NCI Adult Consumer Survey 2014-15
I-4. How many surveyors conducted the survey with this person? (This includes “shadow surveyors” or other silent observers. This does not include translators.)
1 One 2 Two 3 Three 4 Four or more
I-5. Date of face-to-face survey:
(mm/dd/yyyy) / /
I-6. How was this survey administered? (check all that apply)
1 Paper 2 Laptop 3 Netbook 4 IPad 5 Smart phone (e.g., blackberry, palm pilot, IPhone) 6 Other
Page 67 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT 2
CUSTOMARY PROVISIONS FOR CONTRACTS AND GRANTS
STATE OF VERMONT Page 1 of
Page 68 of 83NCI Adult Consumer Survey 2014-15
CONTRACT FOR SERVICES Contract #
l. Parties. This is a contract for personal services between (Insert Department Name) (hereafter called "State"), and (Insert name of contractor) , with a principal place of business in (Address of Contractor) (hereafter called "Contractor"). The Contractor's form of business organization is a (type of business - e.g. LLC, PC, Inc., Individual, etc.). The Contractor's local address is (Insert alternative local address the Contractor). It is the Contractor's responsibility to contact the Vermont Department of Taxes to determine if, by law, the Contractor is required to have a Vermont Department of Taxes Business Account Number.
2. Subject Matter. The subject matter of this contract is personal services generally on the subject of management. Detailed services to be provided by the Contractor are described in Attachment A.
3. Maximum Amount. In consideration of the services to be performed by Contractor, the State agrees to pay Contractor, in accordance with the payment provisions specified in Attachment B, a sum not to exceed$(Insert maximum limiting amount of the contract).
4. Contract Term. The period of Contractor's performance shall begin on (Insert beginning effective Date) and end on (Insert expiration Date).
5. Prior Approvals. If approval by the Attorney General's Office or the Secretary of Administration is required, (under current law, bulletins, and interpretations), neither this contract nor any amendment to it is binding until it has been approved by either or both such persons.
Approval by the Attorney General's Office is required.
Approval by the Secretary of Administration (is/or is not) required.
6. Amendment. No changes, modifications, or amendments in the terms and conditions of this contract shall be effective unless reduced to writing, numbered and signed by the duly authorized representative of the State and Contractor.
7. Cancellation. This contract may be cancelled by either party by giving written notice at least(insert number of days) days in advance.
8. Attachments. This contract consists of (insert # pages, including attachments) pages including the following attachments, which are incorporated herein:Attachment A - Specifications of Work to be Performed Attachment B - Payment ProvisionsAttachment C - Customary State Contract provisions Attachment D - Modifications of Insurance Attachment E - Business Associate AgreementAttachment F - Customary Contract Provisions of the Agency of Human Services
STATE OF VERMONT Page 2 of
Page 69 of 83NCI Adult Consumer Survey 2014-15
CONTRACT FOR SERVICES
The order of precedence of documents shall be as follows: 1). This document2). Attachment D (if any) 3). Attachment C4). Attachment A5). Attachment B6). Attachment E (if any)7) Attachment F8) Other Attachments (if any)
WE THE UNDERSIGNED PARTIES AGREE TO BE BOUND BY THIS CONTRACT.
BY THE STATE OF VERMONT: BY THE CONTRACTOR:
Date:
Date:
Signature: Signature:
Name:
Name:
Title:
Agency/Dept.: Human Services / Title:
Phone: e-mail:Alternative Contact: (if any)
Revised AHS 7/21/08
ATTACHMENT A SPECIFICATIONS OF WORK TO BE PERFORMED
ATTACHMENT B PAYMENT PROVISIONS
The maximum dollar amount payable under this agreement is not intended as any form of a guaranteed amount. The Contractor will be paid for products or services specified in Attachment A, or services actually performed, up to the maximum allowable amount specified in this agreement. The payment schedule for delivered products, or rates for services performed, and any additional reimbursements, are included in this attachment. The following provisions specifying payments are:
Page 72 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT C: STANDARD STATE PROVISIONSFOR CONTRACTS AND GRANTS
1. Entire Agreement: This Agreement, whether in the form of a Contract, State Funded Grant, or Federally Funded Grant, represents the entire agreement between the parties on the subject matter. All prior agreements, representations, statements, negotiations, and understandings shall have no effect.
2. Applicable Law: This Agreement will be governed by the laws of the State of Vermont.
3. Definitions: For purposes of this Attachment, “Party” shall mean the Contractor, Grantee or Subrecipient, with whom the State of Vermont is executing this Agreement and consistent with the form of the Agreement.
4. Appropriations: If this Agreement extends into more than one fiscal year of the State (July 1 to June 30), and if appropriations are insufficient to support this Agreement, the State may cancel at the end of the fiscal year, or otherwise upon the expiration of existing appropriation authority. In the case that this Agreement is a Grant that is funded in whole or in part by federal funds, and in the event federal funds become unavailable or reduced, the State may suspend or cancel this Grant immediately, and the State shall have no obligation to pay Subrecipient from State revenues.
5. No Employee Benefits For Party: The Party understands that the State will not provide any individual retirement benefits, group life insurance, group health and dental insurance, vacation or sick leave, workers compensation or other benefits or services available to State employees, nor will the state withhold any state or federal taxes except as required under applicable tax laws, which shall be determined in advance of execution of the Agreement. The Party understands that all tax returns required by the Internal Revenue Code and the State of Vermont, including but not limited to income, withholding, sales and use, and rooms and meals, must be filed by the Party, and information as to Agreement income will be provided by the State of Vermont to the Internal Revenue Service and the Vermont Department of Taxes.
6. Independence, Liability: The Party will act in an independent capacity and not as officers or employees of the State.
The Party shall defend the State and its officers and employees against all claims or suits arising in whole or in part from any act or omission of the Party or of any agent of the Party. The State shall notify the Party in the event of any such claim or suit, and the Party shall immediately retain counsel and otherwise provide a complete defense against the entire claim or suit.
After a final judgment or settlement the Party may request recoupment of specific defense costs and may file suit in Washington Superior Court requesting recoupment. The Party shall be entitled to recoup costs only upon a showing that such costs were entirely unrelated to the defense of any claim arising from an act or omission of the Party.
The Party shall indemnify the State and its officers and employees in the event that the State, its officers or employees become legally obligated to pay any damages or losses arising from any act or omission of the Party.
7. Insurance: Before commencing work on this Agreement the Party must provide certificates of insurance to show that the following minimum coverages are in effect. It is the responsibility of the Party to maintain current
certificates of insurance on file with the state through the term of the Agreement. No warranty is made that the coverages and limits listed herein are adequate to cover and protect the interests of the Party for the Party’s
operations. These are solely minimums that have been established to protect the interests of the State.
Page 73 of 83NCI Adult Consumer Survey 2014-15
Workers Compensation: With respect to all operations performed, the Party shall carry workers’ compensation insurance in accordance with the laws of the State of Vermont.
General Liability and Property Damage: With respect to all operations performed under the contract, the Party shall carry general liability insurance having all major divisions of coverage including, but not limited to:
Premises - Operations Products and Completed Operations Personal Injury Liability Contractual Liability
The policy shall be on an occurrence form and limits shall not be less than:
$1,000,000 Per Occurrence $1,000,000 General Aggregate $1,000,000 Products/Completed Operations Aggregate $ 50,000 Fire/ Legal/Liability
Party shall name the State of Vermont and its officers and employees as additional insureds for liability arising out of this Agreement.
Automotive Liability: The Party shall carry automotive liability insurance covering all motor vehicles, including hired and non-owned coverage, used in connection with the Agreement. Limits of coverage shall not be less than: $1,000,000 combined single limit.
Party shall name the State of Vermont and its officers and employees as additional insureds for liability arising out of this Agreement.
Professional Liability: Before commencing work on this Agreement and throughout the term of this Agreement, the Party shall procure and maintain professional liability insurance for any and all services performed under this Agreement, with minimum coverage of $__N/A______ per occurrence, and$__N/A_______aggregate.
8. Reliance by the State on Representations: All payments by the State under this Agreement will be made in reliance upon the accuracy of all prior representations by the Party, including but not limited to bills, invoices, progress reports and other proofs of work.
9. Requirement to Have a Single Audit: In the case that this Agreement is a Grant that is funded in whole or in part by federal funds, the Subrecipient will complete the Subrecipient Annual Report annually within 45 days after its fiscal year end, informing the State of Vermont whether or not a Single Audit is required for the prior fiscal year. If a Single Audit is required, the Subrecipient will submit a copy of the audit report to the granting Party within 9 months. If a single audit is not required, only the Subrecipient Annual Report is required.
For fiscal years ending before December 25, 2015, a Single Audit is required if the subrecipient expends $500,000 or more in federal assistance during its fiscal year and must be conducted in accordance with OMB Circular A-133. For fiscal years ending on or after December 25, 2015, a Single Audit is required if the subrecipient expends $750,000 or more in federal assistance during its fiscal year and must be conducted in accordance with 2 CFR Chapter I, Chapter II, Part 200, Subpart F. The Subrecipient Annual Report is required to be submitted within 45 days, whether or not a Single Audit is required.
Page 74 of 83NCI Adult Consumer Survey 2014-15
10. Records Available for Audit: The Party shall maintain all records pertaining to performance under this agreement. “Records” means any written or recorded information, regardless of physical form or characteristics, which is produced or acquired by the Party in the performance of this agreement. Records produced or acquired in a machine readable electronic format shall be maintained in that format. The records described shall be made available at reasonable times during the period of the Agreement and for three years thereafter or for any period required by law for inspection by any authorized representatives of the State or Federal Government. If any litigation, claim, or audit is started before the expiration of the three year period, the records shall be retained until all litigation, claims or audit findings involving the records have been resolved.
11. Fair Employment Practices and Americans with Disabilities Act: Party agrees to comply with the requirement of Title 21V.S.A. Chapter 5, Subchapter 6, relating to fair employment practices, to the full extent applicable. Party shall also ensure, to the full extent required by the Americans with Disabilities Act of 1990, as amended, that qualified individuals with disabilities receive equitable access to the services, programs, and activities provided by the Party under this Agreement. Party further agrees to include this provision in all subcontracts.
12. Set Off: The State may set off any sums which the Party owes the State against any sums due the Party under this Agreement; provided, however, that any set off of amounts due the State of Vermont as taxes shall be in accordance with the procedures more specifically provided hereinafter.
13. Taxes Due to the State:
a. Party understands and acknowledges responsibility, if applicable, for compliance with State tax laws, including income tax withholding for employees performing services within the State, payment of use tax on property used within the State, corporate and/or personal income tax on income earned within the State.
b. Party certifies under the pains and penalties of perjury that, as of the date the Agreement is signed, the Party is in good standing with respect to, or in full compliance with, a plan to pay any and all taxes due the State of Vermont.
c. Party understands that final payment under this Agreement may be withheld if the Commissioner of Taxes determines that the Party is not in good standing with respect to or in full compliance with a plan to pay any and all taxes due to the State of Vermont.
d. Party also understands the State may set off taxes (and related penalties, interest and fees) due to the State of Vermont, but only if the Party has failed to make an appeal within the time allowed by law, or an appeal has been taken and finally determined and the Party has no further legal recourse to contest the amounts due.
14. Child Support: (Applicable if the Party is a natural person, not a corporation or partnership.) Party states that, as of the date the Agreement is signed, he/she:
a. is not under any obligation to pay child support; orb. is under such an obligation and is in good standing with respect to that obligation; or c. has agreed to a payment plan with the Vermont Office of Child Support Services and is in full
compliance with that plan.
Party makes this statement with regard to support owed to any and all children residing in Vermont. In addition, if the Party is a resident of Vermont, Party makes this statement with regard to support owed to any and all children residing in any other state or territory of the United States.
15. Sub-Agreements: Party shall not assign, subcontract or subgrant the performance of this Agreement or any portion thereof to any other Party without the prior written approval of the State. Party also agrees to include in all subcontract or subgrant agreements a tax certification in accordance with paragraph 13 above.
Page 75 of 83NCI Adult Consumer Survey 2014-15
16. No Gifts or Gratuities: Party shall not give title or possession of any thing of substantial value (including property, currency, travel and/or education programs) to any officer or employee of the State during the term of this Agreement.
17. Copies: All written reports prepared under this Agreement will be printed using both sides of the paper.
18. Certification Regarding Debarment: Party certifies under pains and penalties of perjury that, as of the date that this Agreement is signed, neither Party nor Party’s principals (officers, directors, owners, or partners) are presently debarred, suspended, proposed for debarment, declared ineligible or excluded from participation in federal programs, or programs supported in whole or in part by federal funds.
Party further certifies under pains and penalties of perjury that, as of the date that this Agreement is signed, Party is not presently debarred, suspended, nor named on the State’s debarment list at: http://bgs.vermont.gov/purchasing/debarment
19. Certification Regarding Use of State Funds: In the case that Party is an employer and this Agreement is a State Funded Grant in excess of $1,001, Party certifies that none of these State funds will be used to interfere with or restrain the exercise of Party’s employee’s rights with respect to unionization.
(End of Standard Provisions)
State of Vermont – Attachment CRevised AHS – 9-3-2014
Page 79 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT DMODIFICATION OF CUSTOMARY PROVISIONS
OFATTACHMENT C OR ATTACHMENT F
1. The insurance requirements contained in Attachment C, Section 7 are hereby modified:
2. Requirements of other Sections in Attachment C are hereby modified:
3. Requirements of Sections in Attachment F are hereby modified:
4. Reasons for Modifications:
Approval:
Assistant Attorney General:
Date:
State of Vermont – Attachment D Revised AHS – 12-08-09
Page 80 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT E BUSINESS ASSOCIATE AGREEMENT
This Business Associate Agreement (“Agreement”) is entered into by and between the State of Vermont Agency of Human Services, operating by and through its [Insert Name of AHS Department, Office or Division](“Covered Entity”) and [Insert Name of Contractor/Grantee ] (“Business Associate”) as of This Agreement supplements and is made a part of the contract/grant to which it is attached.(“Effective Date”).
Covered Entity and Business Associate enter into this Agreement to comply with standards promulgated under the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), including the Standards for the Privacy of Individually Identifiable Health Information, at 45 CFR Parts 160 and 164 (“Privacy Rule”), and the Security Standards, at 45 CFR Parts 160 and 164 (“Security Rule”), as amended by Subtitle D of the Health Information Technology for Economic and Clinical Health Act (HITECH), and any associated federal rules and regulations.
The parties agree as follows:
1. Definitions . All capitalized terms used but not otherwise defined in this Agreement have the meanings set forth in 45 CFR Parts 160 and 164 as amended by HITECH and associated federal rules and regulations.
“Agent” means those person(s) who are agents(s) of the Business Associate, in accordance with the Federal common law of agency, as referenced in 45 CFR § 160.402(c).
“Breach” means the acquisition, access, use or disclosure of protected health information (PHI) which compromises the security or privacy of the PHI, except as excluded in the definition of Breach in 45 CFR § 164.402.
“Business Associate shall have the meaning given in 45 CFR § 160.103.
“Individual” includes a person who qualifies as a personal representative in accordance with 45 CFR § 164.502(g).
“Protected Health Information” or PHI shall have the meaning given in 45 CFR § 160.103, limited to the information created or received by Business Associate from or on behalf of Agency.“Security Incident” means any known successful or unsuccessful attempt by an authorized or unauthorized individual to inappropriately use, disclose, modify, access, or destroy any information or interference with system operations in an information system.
“Services” includes all work performed by the Business Associate for or on behalf of Covered Entity that requires the use and/or disclosure of protected health information to perform a business associate function described in 45 CFR §160.103 under the definition of Business Associate.
“Subcontractor” means a person or organization to whom a Business Associate delegates a function, activity or service, other than in the capacity of a member of the workforce of the Business Associate. For purposes of this Agreement, the term Subcontractor includes Subgrantees.
2. Identification and Disclosure of Privacy and Security Offices. Business Associate and Subcontractors shall provide, within ten (10) days of the execution of this agreement, written notice to the Covered Entity’s contract/grant manager the names and contact information of both the HIPAA Privacy Officer and HIPAA Security Officer. This information must be updated any time either of these contacts changes.
3. Permitted and Required Uses/Disclosures of PHI .
3.1 Except as limited in this Agreement, Business Associate may use or disclose PHI to perform Services, as specified in the underlying grant or contract with Covered Entity. The uses and disclosures of Business Associate are limited to the minimum necessary, to complete the tasks or to provide the services associated with the terms of the underlying agreement. Business Associate shall not use or disclose PHI in any manner that would constitute a violation of the Privacy Rule if used or disclosed by Covered Entity in that manner.
Page 81 of 83NCI Adult Consumer Survey 2014-15
Business Associate may not use or disclose PHI other than as permitted or required by this Agreement or as Required by Law.
3.2 Business Associate may make PHI available to its employees who need access to perform Services provided that Business Associate makes such employees aware of the use and disclosure restrictions in this Agreement and binds them to comply with such restrictions. Business Associate may only disclose PHI for the purposes authorized by this Agreement: (a) to its agents and Subcontractors in accordance with Sections 9 and 17 or, (b) as otherwise permitted by Section 3.
3.3 Business Associate shall be directly liable under HIPAA for impermissible uses and disclosures of the PHI it handles on behalf of Covered Entity, and for impermissible uses and disclosures, by Business Associate’s Subcontractor(s), of the PHI that Business Associate handles on behalf of Covered Entity and that it passes on to Subcontractors.
4. Business Activities . Business Associate may use PHI received in its capacity as a Business Associate to Covered Entity if necessary for Business Associate’s proper management and administration or to carry out its legal responsibilities. Business Associate may disclose PHI received in its capacity as Business Associate to Covered Entity for Business Associate’s proper management and administration or to carry out its legal responsibilities if a disclosure is Required by Law or if Business Associate obtains reasonable written assurances via a written agreement from the person to whom the information is to be disclosed that the PHI shall remain confidential and be used or further disclosed only as Required by Law or for the purpose for which it was disclosed to the person, and the Agreement requires the person or entity to notify Business Associate, within two (2) business days (who in turn will notify Covered Entity within two (2) business days after receiving notice of a Breach as specified in Section 6.1), in writing of any Breach of Unsecured PHI of which it is aware. Uses and disclosures of PHI for the purposes identified in Section 3 must be of the minimum amount of PHI necessary to accomplish such purposes.
5. Safeguards . Business Associate, its Agent(s) and Subcontractor(s) shall implement and use appropriate safeguards to prevent the use or disclosure of PHI other than as provided for by this Agreement. With respect to any PHI that is maintained in or transmitted by electronic media, Business Associate or its Subcontractor(s) shall comply with 45 CFR sections 164.308 (administrative safeguards), 164.310 (physical safeguards), 164.312 (technical safeguards) and 164.316 (policies and procedures and documentation requirements). Business Associate or its Agent(s) and Subcontractor(s) shall identify in writing upon request from Covered Entity all of the safeguards that it uses to prevent impermissible uses or disclosures of PHI.
6. Documenting and Reporting Breaches .
6.1 Business Associate shall report to Covered Entity any Breach of Unsecured PHI, including Breaches reported to it by a Subcontractor, as soon as it (or any of its employees or agents) becomes aware of any such Breach, and in no case later than two (2) business days after it (or any of its employees or agents) becomes aware of the Breach, except when a law enforcement official determines that a notification would impede a criminal investigation or cause damage to national security.
6.2 Business Associate shall provide Covered Entity with the names of the individuals whose Unsecured PHI has been, or is reasonably believed to have been, the subject of the Breach and any other available information that is required to be given to the affected individuals, as set forth in 45 CFR § 164.404(c), and, if requested by Covered Entity, information necessary for Covered Entity to investigate the impermissible use or disclosure. Business Associate shall continue to provide to Covered Entity information concerning the Breach as it becomes available to it. Business Associate shall require its Subcontractor(s) to agree to these same terms and conditions.
6.3 When Business Associate determines that an impermissible acquisition, use or disclosure of PHI by a member of its workforce is not a Breach, as that term is defined in 45 CFR § 164.402, and therefore does not necessitate notice to the impacted individual(s), it shall document its assessment of risk, conducted as set forth in 45 CFR § 402(2). When requested by Covered Entity, Business Associate shall make its risk assessments available to Covered Entity. It shall also provide Covered Entity with 1) the name of the person(s) making the assessment, 2) a brief summary of the facts, and 3) a brief statement of the reasons supporting the determination of low probability that the PHI had been compromised. When a breach is the responsibility of a member of its Subcontractor’s workforce, Business Associate shall either 1) conduct its own risk assessment and draft a summary of the event and assessment or 2) require its Subcontractor to conduct
Page 82 of 83NCI Adult Consumer Survey 2014-15
the assessment and draft a summary of the event. In either case, Business Associate shall make these assessments and reports available to Covered Entity.
6.4 Business Associate shall require, by contract, a Subcontractor to report to Business Associate and Covered Entity any Breach of which the Subcontractor becomes aware, no later than two (2) business days after becomes aware of the Breach.
7. Mitigation and Corrective Action. Business Associate shall mitigate, to the extent practicable, any harmful effect that is known to it of an impermissible use or disclosure of PHI, even if the impermissible use or disclosure does not constitute a Breach. Business Associate shall draft and carry out a plan of corrective action to address any incident of impermissible use or disclosure of PHI. If requested by Covered Entity, Business Associate shall make its mitigation and corrective action plans available to Covered Entity. Business Associate shall require a Subcontractor to agree to these same terms and conditions.
8. Providing Notice of Breaches .
8.1 If Covered Entity determines that an impermissible acquisition, access, use or disclosure of PHI for which one of Business Associate’s employees or agents was responsible constitutes a Breach as defined in 45 CFR§ 164.402, and if requested by Covered Entity, Business Associate shall provide notice to the individual(s) whose PHI has been the subject of the Breach. When requested to provide notice, Business Associate shall consult with Covered Entity about the timeliness, content and method of notice, and shall receive Covered Entity’s approval concerning these elements. The cost of notice and related remedies shall be borne by Business Associate.
8.2 If Covered Entity or Business Associate determines that an impermissible acquisition, access, use or disclosure of PHI by a Subcontractor of Business Associate constitutes a Breach as defined in 45 CFR § 164.402, and if requested by Covered Entity or Business Associate, Subcontractor shall provide notice to the individual(s) whose PHI has been the subject of the Breach. When Covered Entity requests that Business Associate or its Subcontractor provide notice, Business Associate shall either 1) consult with Covered Entity about the specifics of the notice as set forth in section 8.1, above, or 2) require, by contract, its Subcontractor to consult with Covered Entity about the specifics of the notice as set forth in section 8.1
8.3 The notice to affected individuals shall be provided as soon as reasonably possible and in no case later than 60 calendar days after Business Associate reported the Breach to Covered Entity.
8.4 The notice to affected individuals shall be written in plain language and shall include, to the extent possible, 1) a brief description of what happened, 2) a description of the types of Unsecured PHI that were involved in the Breach, 3) any steps individuals can take to protect themselves from potential harm resulting from the Breach, 4) a brief description of what the Business Associate is doing to investigate the Breach, to mitigate harm to individuals and to protect against further Breaches, and 5) contact procedures for individuals to ask questions or obtain additional information, as set forth in 45 CFR § 164.404(c).
8.5 Business Associate shall notify individuals of Breaches as specified in 45 CFR § 164.404(d) (methods of individual notice). In addition, when a Breach involves more than 500 residents of Vermont, Business Associate shall, if requested by Covered Entity, notify prominent media outlets serving Vermont, following the requirements set forth in 45 CFR § 164.406.
9. Agreements with Subcontractors . Business Associate shall enter into a Business Associate Agreement with any Subcontractor to whom it provides PHI received from Covered Entity or created or received by Business Associate on behalf of Covered Entity in which the Subcontractor agrees to the same restrictions and conditions that apply through this Agreement to Business Associate with respect to such PHI. Business Associate must enter into this Business Associate Agreement before any use by or disclosure of PHI to such agent. The written agreement must identify Covered Entity as a direct and intended third party beneficiary with the right to enforce any breach of the agreement concerning the use or disclosure of PHI. Business Associate shall provide a copy of the Business Associate Agreement it enters into with a subcontractor to Covered Entity upon request. Business associate may not make any disclosure of PHI to any Subcontractor without prior written consent of Covered Entity.
10. Access to PHI . Business Associate shall provide access to PHI in a Designated Record Set to Covered Entity or as directed by Covered Entity to an Individual to meet the requirements under 45 CFR § 164.524. Business
Page 83 of 83NCI Adult Consumer Survey 2014-15
Associate shall provide such access in the time and manner reasonably designated by Covered Entity. Within three(3) business days, Business Associate shall forward to Covered Entity for handling any request for access to PHI that Business Associate directly receives from an Individual.
11. Amendment of PHI . Business Associate shall make any amendments to PHI in a Designated Record Set that Covered Entity directs or agrees to pursuant to 45 CFR § 164.526, whether at the request of Covered Entity or an Individual. Business Associate shall make such amendments in the time and manner reasonably designated by Covered Entity. Within three (3) business days, Business Associate shall forward to Covered Entity for handling any request for amendment to PHI that Business Associate directly receives from an Individual.
12. Accounting of Disclosures . Business Associate shall document disclosures of PHI and all information related to such disclosures as would be required for Covered Entity to respond to a request by an Individual for an accounting of disclosures of PHI in accordance with 45 CFR § 164.528. Business Associate shall provide such information to Covered Entity or as directed by Covered Entity to an Individual, to permit Covered Entity to respond to an accounting request. Business Associate shall provide such information in the time and manner reasonably designated by Covered Entity. Within three (3) business days, Business Associate shall forward to Covered Entity for handling any accounting request that Business Associate directly receives from an Individual.
13. Books and Records . Subject to the attorney-client and other applicable legal privileges, Business Associate shall make its internal practices, books, and records (including policies and procedures and PHI) relating to the use and disclosure of PHI received from Covered Entity or created or received by Business Associate on behalf of Covered Entity available to the Secretary in the time and manner designated by the Secretary. Business Associate shall make the same information available to Covered Entity, upon Covered Entity’s request, in the time and manner reasonably designated by Covered Entity so that Covered Entity may determine whether Business Associate is in compliance with this Agreement.
14. Termination .
14.1 This Agreement commences on the Effective Date and shall remain in effect until terminated by Covered Entity or until all of the PHI provided by Covered Entity to Business Associate or created or received by Business Associate on behalf of Covered Entity is destroyed or returned to Covered Entity subject to Section 18.7.
14.2 If Business Associate breaches any material term of this Agreement, Covered Entity may either: (a) provide an opportunity for Business Associate to cure the breach and Covered Entity may terminate the contract or grant without liability or penalty if Business Associate does not cure the breach within the time specified by Covered Entity; or (b) immediately terminate the contract or grant without liability or penalty if Covered Entity believes that cure is not reasonably possible; or (c) if neither termination nor cure are feasible, Covered Entity shall report the breach to the Secretary. Covered Entity has the right to seek to cure any breach by Business Associate and this right, regardless of whether Covered Entity cures such breach, does not lessen any right or remedy available to Covered Entity at law, in equity, or under the contract or grant, nor does it lessen Business Associate’s responsibility for such breach or its duty to cure such breach.
15. Return/Destruction of PHI .
15.1 Business Associate in connection with the expiration or termination of the contract or grant shall return or destroy, at the discretion of the Covered Entity, all PHI received from Covered Entity or created or received by Business Associate on behalf of Covered Entity pursuant to this contract or grant that Business Associate still maintains in any form or medium (including electronic) within thirty (30) days after such expiration or termination. Business Associate shall not retain any copies of the PHI. Business Associate shall certify in writing for Covered Entity (1) when all PHI has been returned or destroyed and (2) that Business Associate does not continue to maintain any PHI. Business Associate is to provide this certification during this thirty (30) day period.
15.2 Business Associate shall provide to Covered Entity notification of any conditions that Business Associate believes make the return or destruction of PHI infeasible. If Covered Entity agrees that return or destruction is infeasible, Business Associate shall extend the protections of this Agreement to such PHI and limit further uses and disclosures of such PHI to those purposes that make the return or destruction infeasible for so long as Business Associate maintains such PHI. This shall also apply to all Agents and Subcontractors
Page 84 of 83NCI Adult Consumer Survey 2014-15
of Business Associate.
16. Penalties and Training . Business Associate understands that: (a) there may be civil or criminal penalties for misuse or misappropriation of PHI and (b) violations of this Agreement may result in notification by Covered Entity to law enforcement officials and regulatory, accreditation, and licensure organizations. If requested by Covered Entity, Business Associate shall participate in training regarding the use, confidentiality, and security of PHI.
17. Security Rule Obligations . The following provisions of this section apply to the extent that Business Associate creates, receives, maintains or transmits Electronic PHI on behalf of Covered Entity.
17.1 Business Associate shall implement and use administrative, physical, and technical safeguards in compliance with 45 CFR sections 164.308, 164.310, and 164.312 with respect to the Electronic PHI that it creates, receives, maintains or transmits on behalf of Covered Entity. Business Associate shall identify in writing upon request from Covered Entity all of the safeguards that it uses to protect such Electronic PHI.
17.2 Business Associate shall ensure that any Agent and Subcontractor to whom it provides Electronic PHI agrees in a written agreement to implement and use administrative, physical, and technical safeguards that reasonably and appropriately protect the Confidentiality, Integrity and Availability of the Electronic PHI. Business Associate must enter into this written agreement before any use or disclosure of Electronic PHI by such Agent or Subcontractor. The written agreement must identify Covered Entity as a direct and intended third party beneficiary with the right to enforce any breach of the agreement concerning the use or disclosure of Electronic PHI. Business Associate shall provide a copy of the written agreement to Covered Entity upon request. Business Associate may not make any disclosure of Electronic PHI to any Agent or Subcontractor without the prior written consent of Covered Entity.
17.3 Business Associate shall report in writing to Covered Entity any Security Incident pertaining to such Electronic PHI (whether involving Business Associate or an Agent or Subcontractor). Business Associate shall provide this written report as soon as it becomes aware of any such Security Incident, and in no case later than two (2) business days after it becomes aware of the incident. Business Associate shall provide Covered Entity with the information necessary for Covered Entity to investigate any such Security Incident.
17.4 Business Associate shall comply with any reasonable policies and procedures Covered Entity implements to obtain compliance under the Security Rule.
18. Miscellaneous.
18.1 In the event of any conflict or inconsistency between the terms of this Agreement and the terms of the contract/grant, the terms of this Agreement shall govern with respect to its subject matter. Otherwise, the terms of the contract/grant continue in effect.
18.2 Business Associate shall cooperate with Covered Entity to amend this Agreement from time to time as is necessary for Covered Entity to comply with the Privacy Rule, the Security Rule, or any other standards promulgated under HIPAA.
18.3 Any ambiguity in this Agreement shall be resolved to permit Covered Entity to comply with the Privacy Rule, Security Rule, or any other standards promulgated under HIPAA.
18.4 In addition to applicable Vermont law, the parties shall rely on applicable federal law (e.g., HIPAA, the Privacy Rule and Security Rule, and the HIPAA omnibus final rule) in construing the meaning and effect of this Agreement.
18.5 As between Business Associate and Covered Entity, Covered Entity owns all PHI provided by Covered Entity to Business Associate or created or received by Business Associate on behalf of Covered Entity.
18.6 Business Associate shall abide by the terms and conditions of this Agreement with respect to all PHI it receives from Covered Entity or creates or receives on behalf of Covered Entity even if some of that information relates to specific services for which Business Associate may not be a “Business Associate” of Covered Entity under the Privacy Rule.
Page 85 of 83NCI Adult Consumer Survey 2014-15
18.7 Business Associate is prohibited from directly or indirectly receiving any remuneration in exchange for an individual’s PHI. Business Associate will refrain from marketing activities that would violate HIPAA, including specifically Section 13406 of the HITECH Act. Reports or data containing the PHI may not be sold without Agency’s or the affected individual’s written consent.
18.8 The provisions of this Agreement that by their terms encompass continuing rights or responsibilities shall survive the expiration or termination of this Agreement. For example: (a) the provisions of this Agreement shall continue to apply if Covered Entity determines that it would be infeasible for Business Associate to return or destroy PHI as provided in Section 14.2 and (b) the obligation of Business Associate to provide an accounting of disclosures as set forth in Section 11 survives the expiration or termination of this Agreement with respect to accounting requests, if any, made after such expiration or termination.
(Rev: 9/21/13)
Page 80 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT FAGENCY OF HUMAN SERVICES’ CUSTOMARY CONTRACT PROVISIONS
1. Agency of Human Services – Field Services Directors will share oversight with the department (or field office) that is a party to the contract for provider performance using outcomes, processes, terms and conditions agreed to under this contract.
2. 2-1-1 Data Base : The Contractor providing a health or human services within Vermont, or near the border that is readily accessible to residents of Vermont, will provide relevant descriptive information regarding its agency, programs and/or contact and will adhere to the "Inclusion/Exclusion" policy of Vermont's United Way/Vermont211. If included, the Contractor will provide accurate and up to date information to their data base as needed. The “Inclusion/Exclusion” policy can be found at www.vermont211.org
3. Medicaid Program Contractors :
Inspection of Records: Any contracts accessing payments for services through the Global Commitment to Health Waiver and Vermont Medicaid program must fulfill state and federal legal requirements to enable the Agency of Human Services (AHS), the United States Department of Health and Human Services (DHHS) and the Government Accounting Office (GAO) to:
Evaluate through inspection or other means the quality, appropriateness, and timeliness of services performed; and Inspect and audit any financial records of such Contractor or subcontractor.
Subcontracting for Medicaid Services: Having a subcontract does not terminate the Contractor, receiving funds under Vermont’s Medicaid program, from its responsibility to ensure that all activities under this agreement are carried out. Subcontracts must specify the activities and reporting responsibilities of the Contractor or subcontractor and provide for revoking delegation or imposing other sanctions if the Contractor or subcontractor’s performance is inadequate. The Contractor agrees to make available upon request to the Agency of Human Services; the Department of Vermont Health Access; the Department of Disabilities, Aging and Independent Living; and the Center for Medicare and Medicaid Services (CMS) all contracts and subcontracts between the Contractor and service providers.
Medicaid Notification of Termination Requirements: Any Contractor accessing payments for services under the Global Commitment to Health Waiver and Medicaid programs who terminates their practice will follow the Department of Vermont Health Access, Managed Care Organization enrollee notification requirements.
Encounter Data : Any Contractor accessing payments for services through the Global Commitment to Health Waiver and Vermont Medicaid programs must provide encounter data to the Agency of Human Services and/or its departments and ensure that it can be linked to enrollee eligibility files maintained by the State.
Federal Medicaid System Security Requirements Compliance : All contractors and subcontractors must provide a security plan, risk assessment, and security controls review document within three months of the start date of this agreement (and update it annually thereafter) to support audit compliance with 45CFR95.621 subpart F, ADP (Automated Data Processing) System Security Requirements and Review Process.
4. Non-discrimination Based on National Origin as evidenced by Limited English Proficiency . The Contractor agrees to comply with the non-discrimination requirements of Title VI of the Civil Rights Act of 1964, 42 USC Section 2000d, et seq., and with the federal guidelines promulgated pursuant to Executive Order 13166 of 2000, which require that contractors and subcontractors receiving federal funds must assure that persons with limited English proficiency can meaningfully access services. To the extent the Contractor provides assistance to individuals with limited English proficiency through the use of oral or written translation or interpretive services in compliance with this requirement, such individuals cannot be required to pay for such services.
5. Voter Registration . When designated by the Secretary of State, the Contractor agrees to become a voter
Page 81 of 83NCI Adult Consumer Survey 2014-15
registration agency as defined by 17 V.S.A. §2103 (41), and to comply with the requirements of state and federal law pertaining to such agencies.
6. Drug Free Workplace Act. The Contractor will assure a drug-free workplace in accordance with 45 CFR Part 76.
7. Privacy and Security Standards .
Protected Health Information: The Contractor shall maintain the privacy and security of all individually identifiable health information acquired by or provided to it as a part of the performance of this contract. The Contractor shall follow federal and state law relating to privacy and security of individually identifiable health information as applicable, including the Health Insurance Portability and Accountability Act (HIPAA) and its federal regulations.
Substance Abuse Treatment Information: The confidentiality of any alcohol and drug abuse treatment information acquired by or provided to the Contractor or subcontractor shall be maintained in compliance with any applicable state or federal laws or regulations and specifically set out in 42 CFR Part 2.
Other Confidential Consumer Information: The Contractor agrees to comply with the requirements of AHS Rule No. 08-048 concerning access to information. The Contractor agrees to comply with any applicable Vermont State Statute, including but not limited to 12 VSA §1612 and any applicable Board of Health confidentiality regulations. The Contractor shall ensure that all of its employees and subcontractors performing services under this agreement understand the sensitive nature of the information that they may have access to and sign an affirmation of understanding regarding the information’s confidential and non-public nature.Social Security numbers: The Contractor agrees to comply with all applicable Vermont State Statutes to assure protection and security of personal information, including protection from identity theft as outlined in Title 9, Vermont Statutes Annotated, Ch. 62.
8. Abuse Registry. The Contractor agrees not to employ any individual, use any volunteer, or otherwise provide reimbursement to any individual in the performance of services connected with this agreement, who provides care, custody, treatment, transportation, or supervision to children or vulnerable adults if there is a substantiation of abuse or neglect or exploitation against that individual. The Contractor will check the Adult Abuse Registry in the Department of Disabilities, Aging and Independent Living. Unless the Contractor holds a valid child care license or registration from the Division of Child Development, Department for Children and Families, the Contractor shall also check the Central Child Protection Registry. (See 33 V.S.A. §4919(a)(3) & 33 V.S.A. §6911(c)(3)).
9. Reporting of Abuse, Neglect, or Exploitation. Consistent with provisions of 33 V.S.A. §4913(a) and §6903, any agent or employee of a Contractor who, in the performance of services connected with this agreement, has contact with clients or is a caregiver and who has reasonable cause to believe that a child or vulnerable adult has been abused or neglected as defined in Chapter 49 or abused, neglected, or exploited as defined in Chapter 69 of Title 33 V.S.A. shall make a report involving children to the Commissioner of the Department for Children and Families within 24 hours or a report involving vulnerable adults to the Division of Licensing and Protection at the Department of Disabilities, Aging, and Independent Living within 48 hours. This requirement applies except in those instances where particular roles and functions are exempt from reporting under state and federal law. Reports involving children shall contain the information required by 33 V.S.A. §4914. Reports involving vulnerable adults shall contain the information required by 33 V.S.A. §6904. The Contractor will ensure that its agents or employees receive training on the reporting of abuse or neglect to children and abuse, neglect or exploitation of vulnerable adults.
10. Intellectual Property/Work Product Ownership. All data, technical information, materials first gathered, originated, developed, prepared, or obtained as a condition of this agreement and used in the performance of this agreement - including, but not limited to all reports, surveys, plans, charts, literature, brochures, mailings, recordings (video or audio), pictures, drawings, analyses, graphic representations, software computer programs
Page 82 of 83NCI Adult Consumer Survey 2014-15
and accompanying documentation and printouts, notes and memoranda, written procedures and documents, which are prepared for or obtained specifically for this agreement - or are a result of the services required under this grant - shall be considered "work for hire" and remain the property of the State of Vermont, regardless of the state of completion - unless otherwise specified in this agreement. Such items shall be delivered to the State of Vermont upon 30 days notice by the State. With respect to software computer programs and / or source codes first developed for the State, all the work shall be considered "work for hire,” i.e., the State, not the Contractor or subcontractor, shall have full and complete ownership of all software computer programs, documentation and/or source codes developed.The Contractor shall not sell or copyright a work product or item produced under this agreement without explicit permission from the State.
If the Contractor is operating a system or application on behalf of the State of Vermont, then the Contractor shall not make information entered into the system or application available for uses by any other party than the State of Vermont, without prior authorization by the State. Nothing herein shall entitle the State to pre-existing Contractor’s materials.
11. Security and Data Transfers. The State shall work with the Contractor to ensure compliance with all applicable State and Agency of Human Services' policies and standards, especially those related to privacy and security. The State will advise the Contractor of any new policies, procedures, or protocols developed during the term of this agreement as they are issued and will work with the Contractor to implement any required.The Contractor will ensure the physical and data security associated with computer equipment - including desktops, notebooks, and other portable devices - used in connection with this agreement. The Contractor will also assure that any media or mechanism used to store or transfer data to or from the State includes industry standard security mechanisms such as continually up-to-date malware protection and encryption. The Contractor will make every reasonable effort to ensure media or data files transferred to the State are virus and spyware free. At the conclusion of this agreement and after successful delivery of the data to the State, the Contractor shall securely delete data (including archival backups) from the Contractor's equipment that contains individually identifiable records, in accordance with standards adopted by the Agency of Human Services.
12. Computing and Communication: The Contractor shall select, in consultation with the Agency of Human Services’ Information Technology unit, one of the approved methods for secure access to the State’s systems and data, if required. Approved methods are based on the type of work performed by the Contractor as part of this agreement. Options include, but are not limited to:1. Contractor’s provision of certified computing equipment, peripherals and mobile devices, on a separate
Contractor’s network with separate internet access. The Agency of Human Services’ accounts may or may not be provided.
2. State supplied and managed equipment and accounts to access state applications and data, including State issued active directory accounts and application specific accounts, which follow the National Institutes of Standards and Technology (NIST) security and the Health Insurance Portability & Accountability Act (HIPAA) standards.
The State will not supply e-mail accounts to the Contractor.
13. Lobbying. No federal funds under this agreement may be used to influence or attempt to influence an officer or employee of any agency, a member of Congress, an officer or employee of Congress, or an employee of a member of Congress in connection with the awarding of any federal contract, continuation, renewal, amendments other than federal appropriated funds.
14. Non–discrimination. The Contractor will prohibit discrimination on the basis of age under the Age Discrimination Act of 1975, on the basis of handicap under section 504 of the Rehabilitation Act of 1973, on the basis of sex under Title IX of the Education Amendments of 1972, or on the basis of race, color or national origin under Title VI of the Civil Rights Act of 1964. No person shall on the grounds of sex (including, in the case of a
Page 83 of 83NCI Adult Consumer Survey 2014-15
woman, on the grounds that the woman is pregnant) or on the grounds of religion, be excluded from participation in, be denied the benefits of, or be subjected to discrimination, to include sexual harassment, under any program or activity supported by state and/or federal funds.The Contractor will also not refuse, withhold from or deny to any person the benefit of services, facilities, goods, privileges, advantages, or benefits of public accommodation on the basis of disability, race, creed, color, national origin, marital status, sex, sexual orientation or gender identity under Title 9 V.S.A. Chapter 139.
15. Environmental Tobacco Smoke. Public Law 103-227, also known as the Pro-children Act of 1994 (Act), requires that smoking not be permitted in any portion of any indoor facility owned or leased or contracted for by an entity and used routinely or regularly for the provision of health, child care, early childhood development services, education or library services to children under the age of 18, if the services are funded by federal programs either directly or through state or local governments, by federal grant, contract, loan or loan guarantee. The law also applies to children's services that are provided in indoor facilities that are constructed, operated, or maintained with such Federal funds.The law does not apply to children's services provided in private residences; portions of facilities used for inpatient drug or alcohol treatment; service providers whose sole source of applicable federal funds is Medicare or Medicaid; or facilities where Women, Infants, & Children (WIC) coupons are redeemed.Failure to comply with the provisions of the law may result in the imposition of a civil monetary penalty of up to$1,000 for each violation and/or the imposition of an administrative compliance order on the responsible entity. Contractors are prohibited from promoting the use of tobacco products for all clients. Facilities supported by state and federal funds are prohibited from making tobacco products available to minors.
Attachment F - Revised AHS -12/10/10
Page 84 of 83NCI Adult Consumer Survey 2014-15
ATTACHMENT G
MODIFICATIONS FOR ACADEMIC WORK PRODUCTS
1. Notwithstanding Attachment F, paragraph 10 is modified as follows:
The parties agree that ownership of all data, papers, reports, forms, or other material collected or produced by the Contractor, under this contract, (the "work product") shall belong to the Contractor. Upon a request made by the State, the Contractor shall provide, free of cost, copies of all such work product no later than 30 days from the date of the request. The State shall have a nonexclusive, nontransferable, irrevocable, royalty free paid-up license to use or have used the work product for or on behalf of the State during the pendency of the agreement and thereafter.The State may provide the work product to its contractors, grantees, community partners, and to other local, state, and federal governmental entities for their non-commercial use.
2. The parties also agree that the following clause will be included in all publications and any other material that are distributed in printed form or are posted or disseminated electronically.
Although this work product was funded in whole or in part with monies provided by or through the State of Vermont, the State does not necessarily endorse the researchers' findings and/or conclusions. The findings and/or conclusions may be inconsistent with the State's policies, programs, and objectives.