Role of ATG in Role of ATG in Allogeneic HSCT Allogeneic HSCT ZiYi Lim ZiYi Lim National University Cancer National University Cancer Institute Institute Singapore Singapore 3 3 rd rd BTG – Hong Kong BTG – Hong Kong 24 24 th th Feb 2012 Feb 2012
Transcript
Role of ATG in Allogeneic Role of ATG in Allogeneic HSCTHSCT
ZiYi LimZiYi LimNational University Cancer InstituteNational University Cancer Institute
SingaporeSingapore
33rdrd BTG – Hong Kong BTG – Hong Kong2424thth Feb 2012 Feb 2012
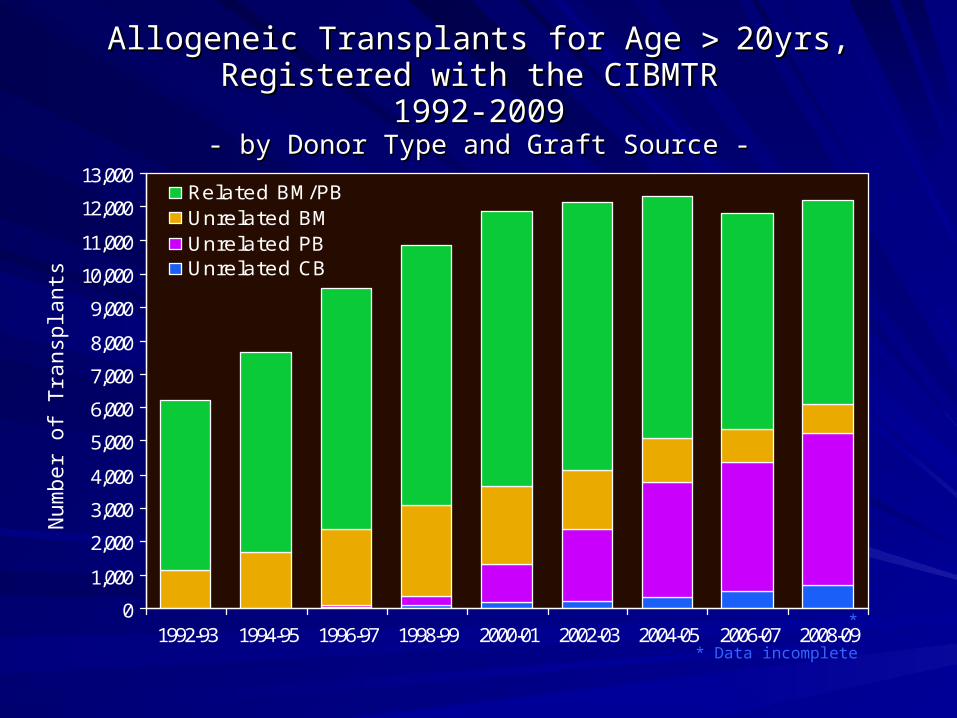
Allogeneic Transplants for Age Allogeneic Transplants for Age 20yrs,20yrs,Registered with the CIBMTR Registered with the CIBMTR
1992-20091992-2009- by Donor Type and Graft Source -- by Donor Type and Graft Source -
• Ground rat spleens Ground rat spleens > injected into > injected into guinea pigsguinea pigs
• Hyperimmune Hyperimmune serum > serum > agglutinate and agglutinate and destroy rat destroy rat leukocytesleukocytes
Father of ATG?
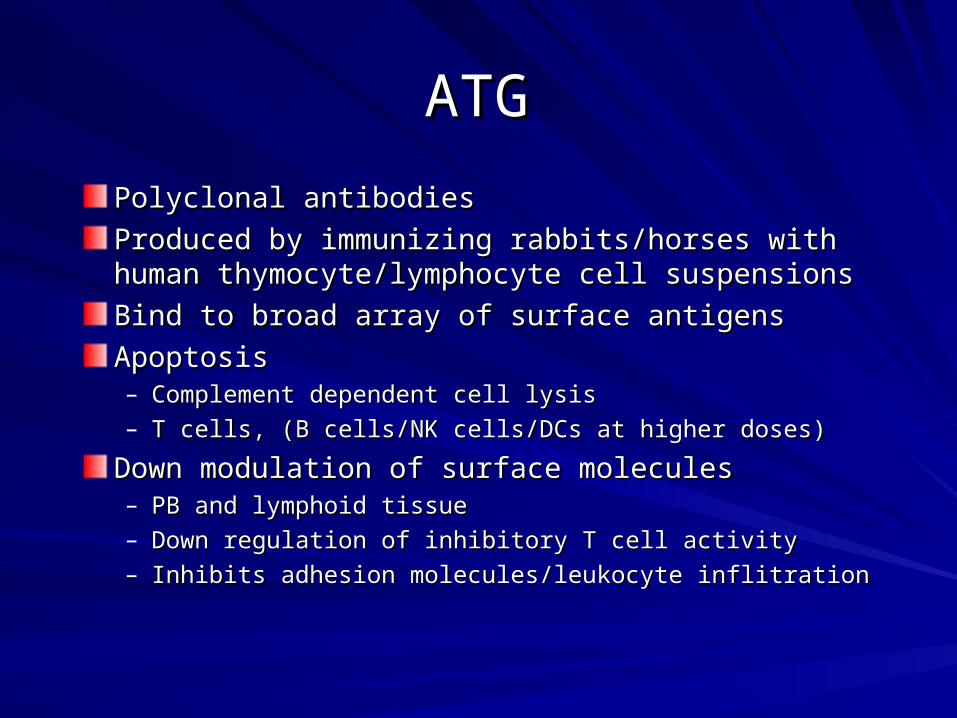
ATGATG
Polyclonal antibodiesPolyclonal antibodies
Produced by immunizing rabbits/horses with human Produced by immunizing rabbits/horses with human thymocyte/lymphocyte cell suspensionsthymocyte/lymphocyte cell suspensions
Bind to broad array of surface antigensBind to broad array of surface antigens
ApoptosisApoptosis– Complement dependent cell lysisComplement dependent cell lysis– T cells, (B cells/NK cells/DCs at higher doses)T cells, (B cells/NK cells/DCs at higher doses)
Down modulation of surface moleculesDown modulation of surface molecules– PB and lymphoid tissuePB and lymphoid tissue– Down regulation of inhibitory T cell activityDown regulation of inhibitory T cell activity– Inhibits adhesion molecules/leukocyte inflitrationInhibits adhesion molecules/leukocyte inflitration
Different sources and immunogens used Different sources and immunogens used Multiple target antigens: immune response, Multiple target antigens: immune response,
adhesion and cell trafficking, heterogeneous adhesion and cell trafficking, heterogeneous cell pathwayscell pathways
Batch-to-batch variabilityBatch-to-batch variability Doses and duration of therapy vary Doses and duration of therapy vary
considerably and have not been systematically considerably and have not been systematically compared.compared.
Weiden PL, Doney K, Storb R, Thomas ED. Antihuman thymocyte globulin for prophylaxis of graft-versus-host disease. A randomized trial in patients with leukemia treated with HLA- identical sibling marrow grafts. Transplantation. 1979;27:227- 230.
Ramsay NKC, Kersey JH, Robinson LL, et al. A randomized study of the prevention of acute graft versus host disease. N Engl J Med. 1982;306:392-397
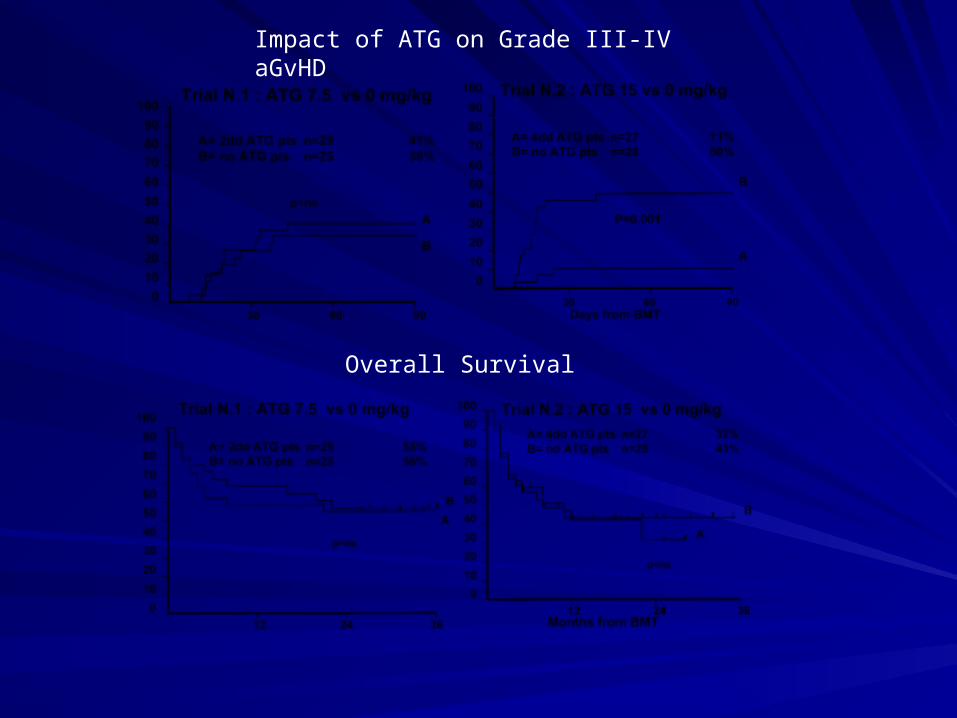
109 patients with haematological malignanciesAll received cyclophosphamide/TBI conditioning GvHD prophylaxis with CyA
2 trials:
Trial A: ATG (3.75 mg/kg x D-4,-3) vs no ATG
Trial B: ATG (3.75 mg/kg x D-5 to -2) vs no ATG
Impact of ATG on Grade III-IV aGvHD
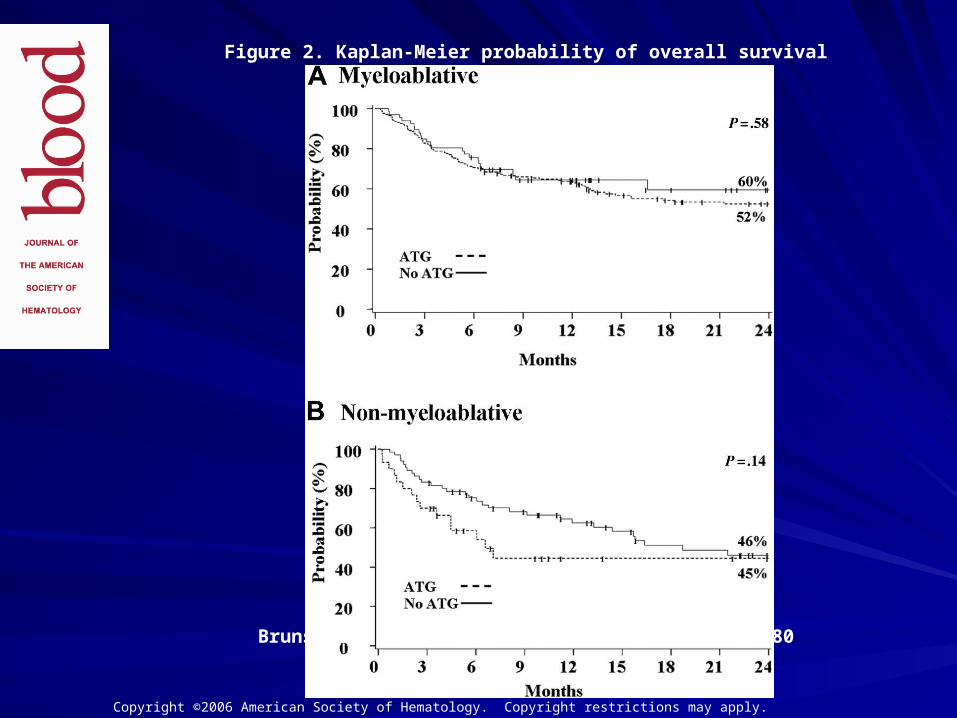
Overall Survival
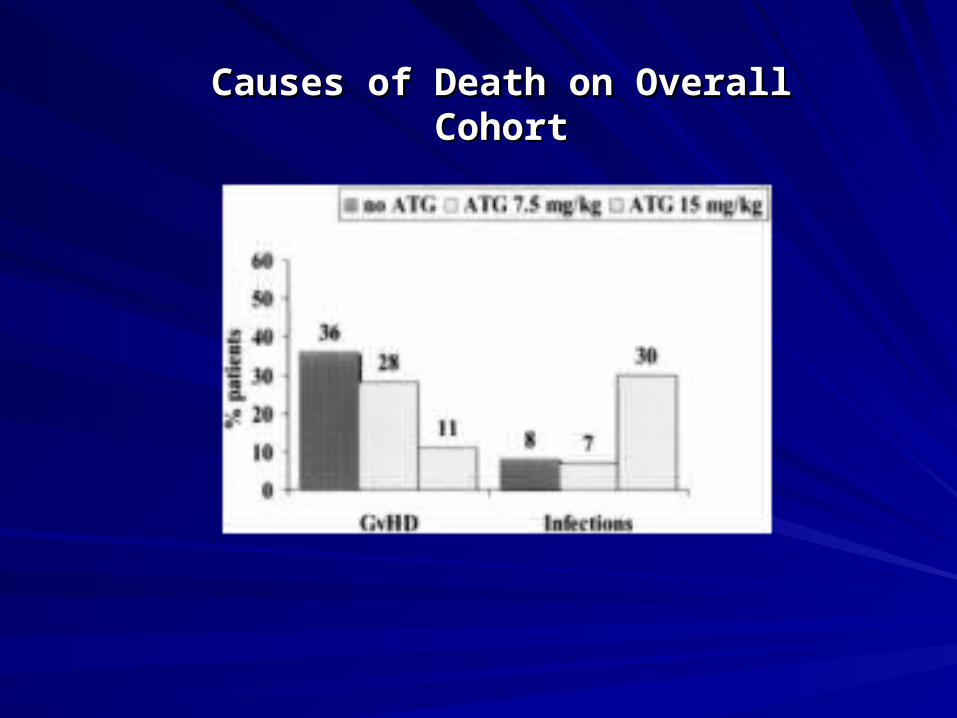
Causes of Death on Overall CohortCauses of Death on Overall Cohort
Update of original Italian randomised study
75 patients surviving more than 100 days (ATG 38 vs non ATG 37)
Median follow-up 5.7 years
Assessment of long-term risk of chronic GVHD chronic lung dysfunction quality of life
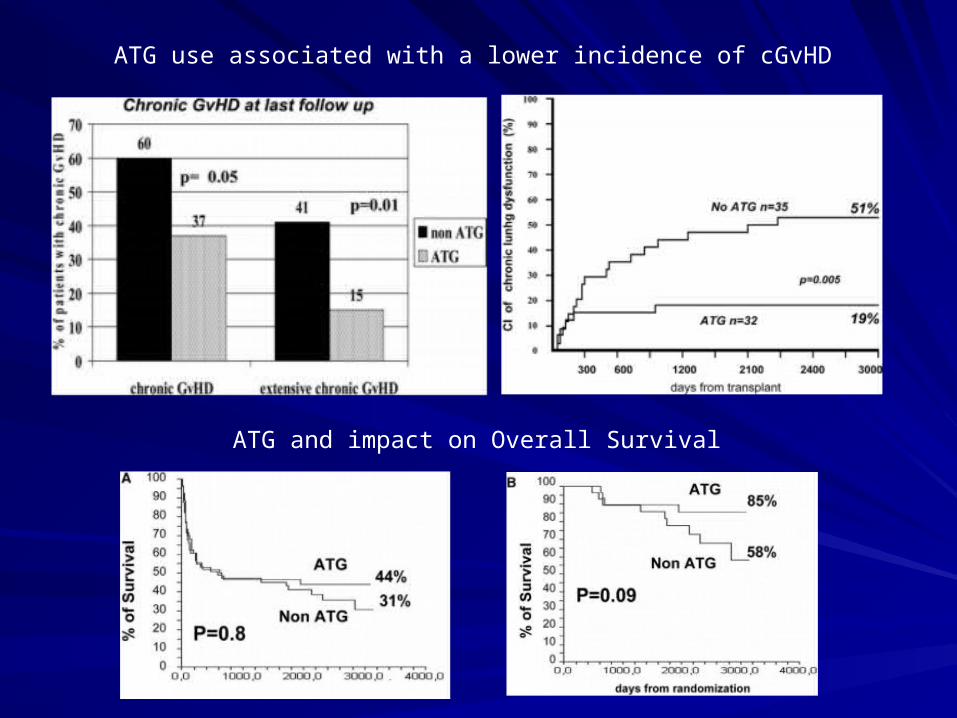
ATG use associated with a lower incidence of cGvHD
ATG and impact on Overall Survival
Use of ATG Use of ATG
in in
Related Adult Donor HSCTRelated Adult Donor HSCT
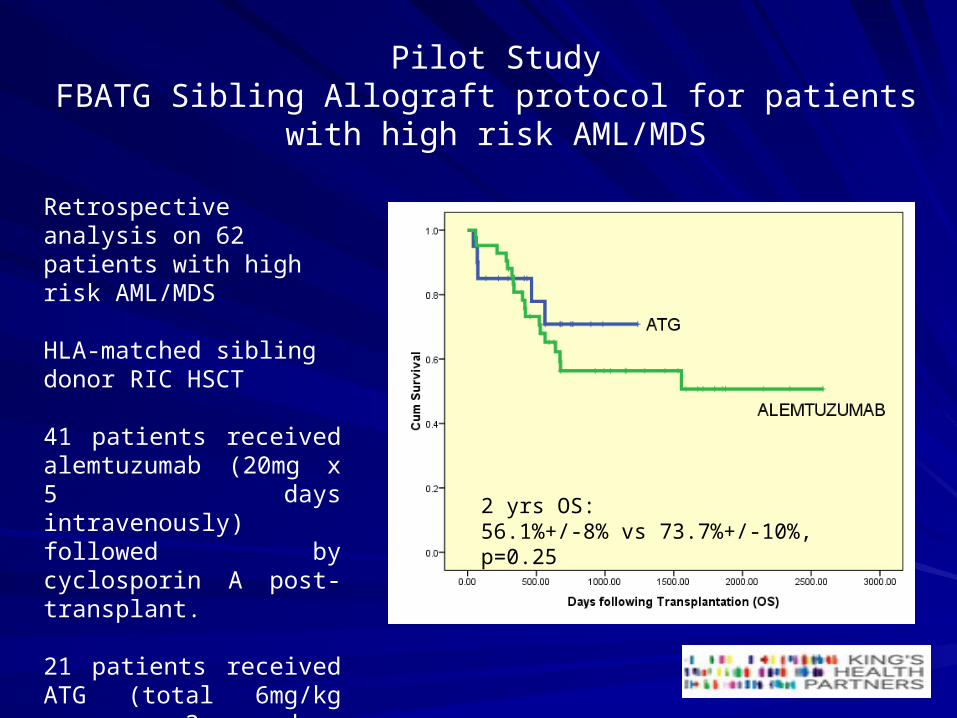
Pilot StudyFBATG Sibling Allograft protocol for patients
with high risk AML/MDS
Retrospective analysis on 62 patients with high risk AML/MDS
HLA-matched sibling donor RIC HSCT
41 patients received alemtuzumab (20mg x 5 days intravenously) followed by cyclosporin A post-transplant.
21 patients received ATG (total 6mg/kg over 3 days intravenously)
2 yrs OS: 56.1%+/-8% vs 73.7%+/-10%, p=0.25
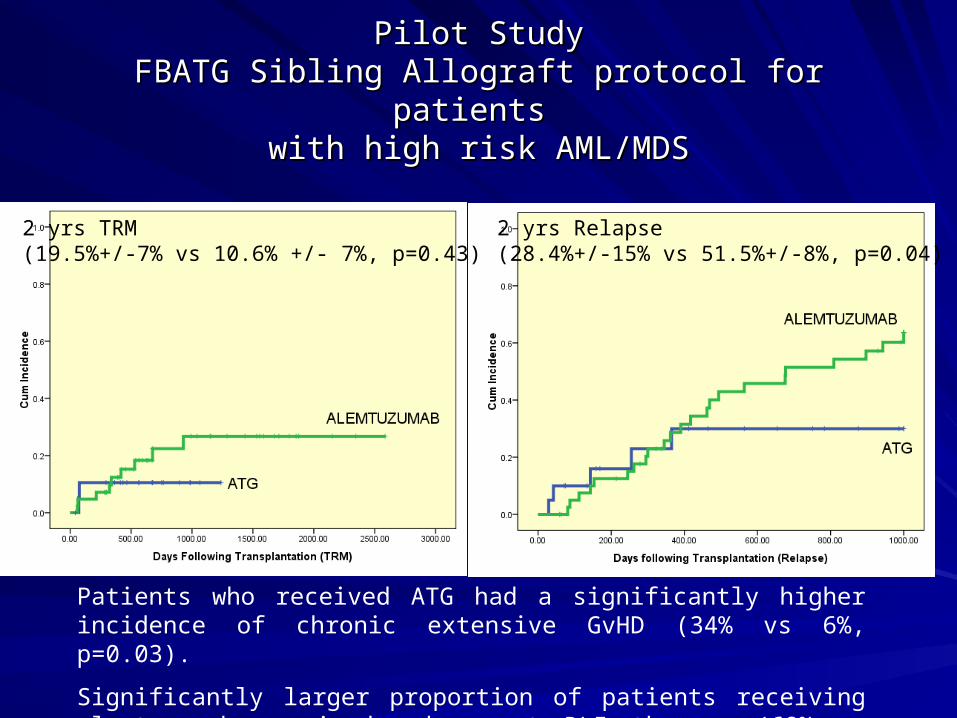
Pilot StudyPilot StudyFBATG Sibling Allograft protocol for patients FBATG Sibling Allograft protocol for patients
with high risk AML/MDSwith high risk AML/MDS
2 yrs TRM(19.5%+/-7% vs 10.6% +/- 7%, p=0.43)
2 yrs Relapse(28.4%+/-15% vs 51.5%+/-8%, p=0.04)
Patients who received ATG had a significantly higher incidence of chronic extensive GvHD (34% vs 6%, p=0.03).
Significantly larger proportion of patients receiving alemtuzumab required subsequent DLI therapy (68% vs 19%)
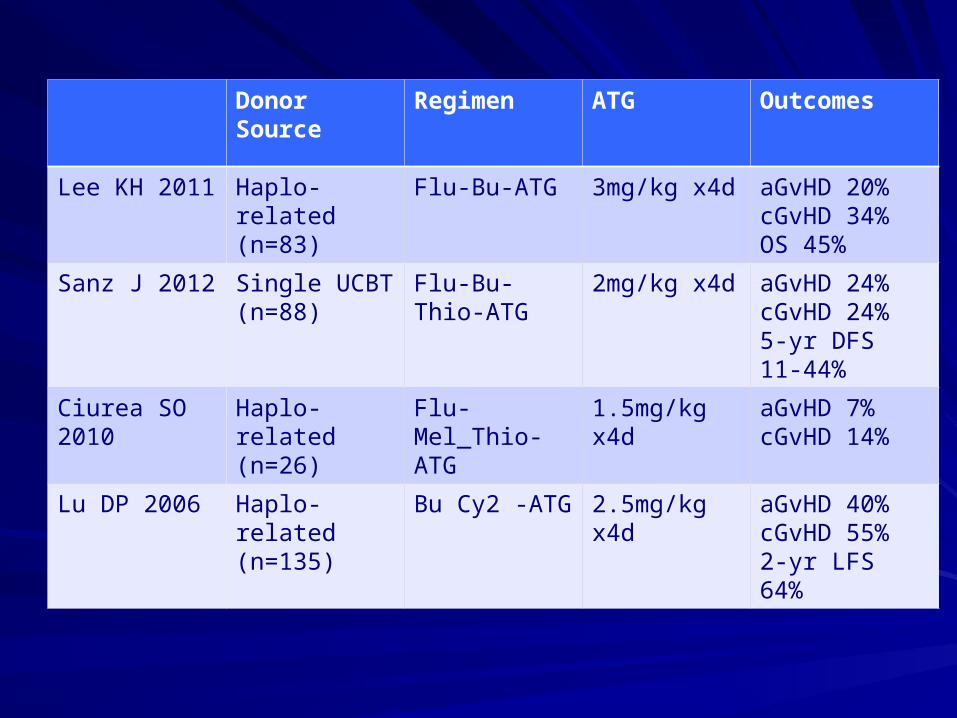
Use of ATG Use of ATG
in in
Alternative donor HSCTAlternative donor HSCT
Donor Source Regimen ATG Outcomes
Lee KH 2011 Haplo-related(n=83)
Flu-Bu-ATG 3mg/kg x4d aGvHD 20%cGvHD 34%OS 45%
Sanz J 2012 Single UCBT(n=88)
Flu-Bu-Thio-ATG
2mg/kg x4d aGvHD 24%cGvHD 24%5-yr DFS 11-44%
Ciurea SO 2010
Haplo-related(n=26)
Flu-Mel_Thio-ATG
1.5mg/kg x4d aGvHD 7%cGvHD 14%
Lu DP 2006 Haplo-related(n=135)
Bu Cy2 -ATG 2.5mg/kg x4d aGvHD 40%cGvHD 55%2-yr LFS 64%
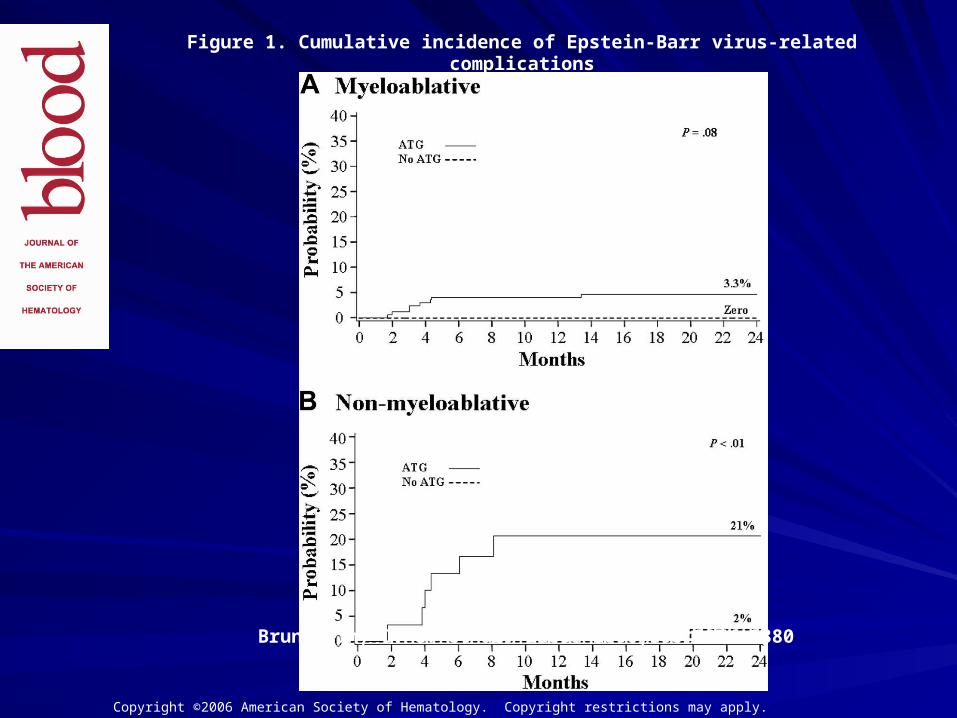
Marked increased risk of EBV-related Marked increased risk of EBV-related complications with addition of ATG to complications with addition of ATG to
nonmyeloablative conditioning prior to UCB nonmyeloablative conditioning prior to UCB transplantationtransplantation
Brunstein et al. Blood 2006; 108: 2874-2880Brunstein et al. Blood 2006; 108: 2874-2880
ProtocolProtocol
Standard: Cyclo+ Busulphan or TBI and Standard: Cyclo+ Busulphan or TBI and ALG in 174 (73%)ALG in 174 (73%)
ALG 15mg/kg bd x 3 daysALG 15mg/kg bd x 3 days
RIC: cyclo/fludarabine/TBI 200cG in 30 RIC: cyclo/fludarabine/TBI 200cG in 30 (32%) after 2002(32%) after 2002
Post Tx immune suppression: CSA/MMF Post Tx immune suppression: CSA/MMF (50%); CSA/MP (49%)(50%); CSA/MP (49%)
ResultsResults
15/335 developed EBV-related 15/335 developed EBV-related complications at median of D+133 (52-complications at median of D+133 (52-407)407)
4 viraemia; 11PTLD4 viraemia; 11PTLD
5/9 treated with rituximab responded to 5/9 treated with rituximab responded to treatment survivedtreatment survived







![ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS€¦ · CMV-seropositive recipients [R+] of an allogeneic haematopoietic stem cell transplant (HSCT). Consideration should be given to official](https://static.documents.pub/doc/80x56/5f961d40b205ea621347cdb0/annex-i-summary-of-product-characteristics-cmv-seropositive-recipients-r-of-an.jpg)










