47
Salivary Gland Tumors Slide Seminar Arghavan Etebarian DDS, MSc February 2021

Salivary Gland Tumors Slide Seminar
Arghavan Etebarian DDS, MSc
February 2021

Case 1 –video 1 attached
A 15 yrs. old young lady
with a parotid mass
https://www.dropbox.com/s/l9tqx9ya6wgmmeq/1.mp4?dl=0
To see video #1, please find the attached video or, click
the below link to open it in the browser:
What is your diagnosis?
• A. Cystadenocarcinoma
• B. Metastatic squamous cell carcinoma
• C. Mucoepidermoid carcinoma
• D. Low grade salivary duct carcinoma
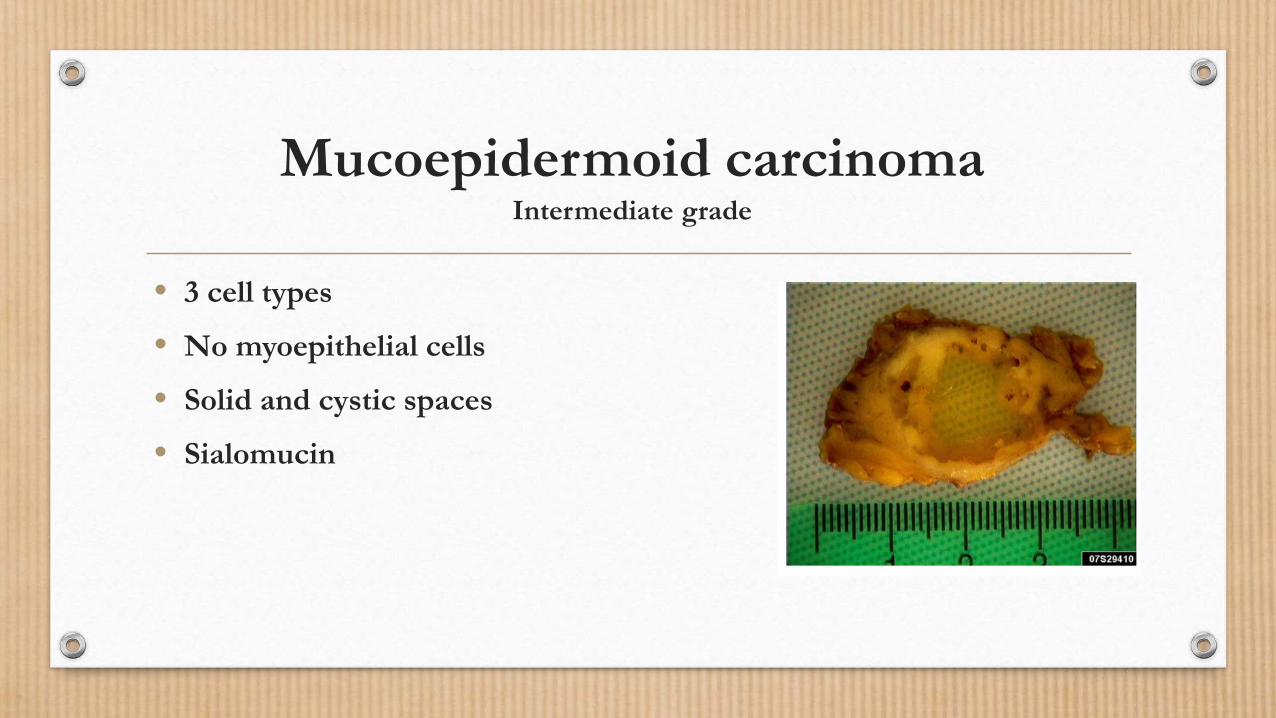
Mucoepidermoid carcinomaIntermediate grade
• 3 cell types
• No myoepithelial cells
• Solid and cystic spaces
• Sialomucin

PAS + Mucicarmine

Cystic low grade MEC

Intermediate cells and foci of epidermoid cells

Epidermoid cells with no keratinization
HMWCK +
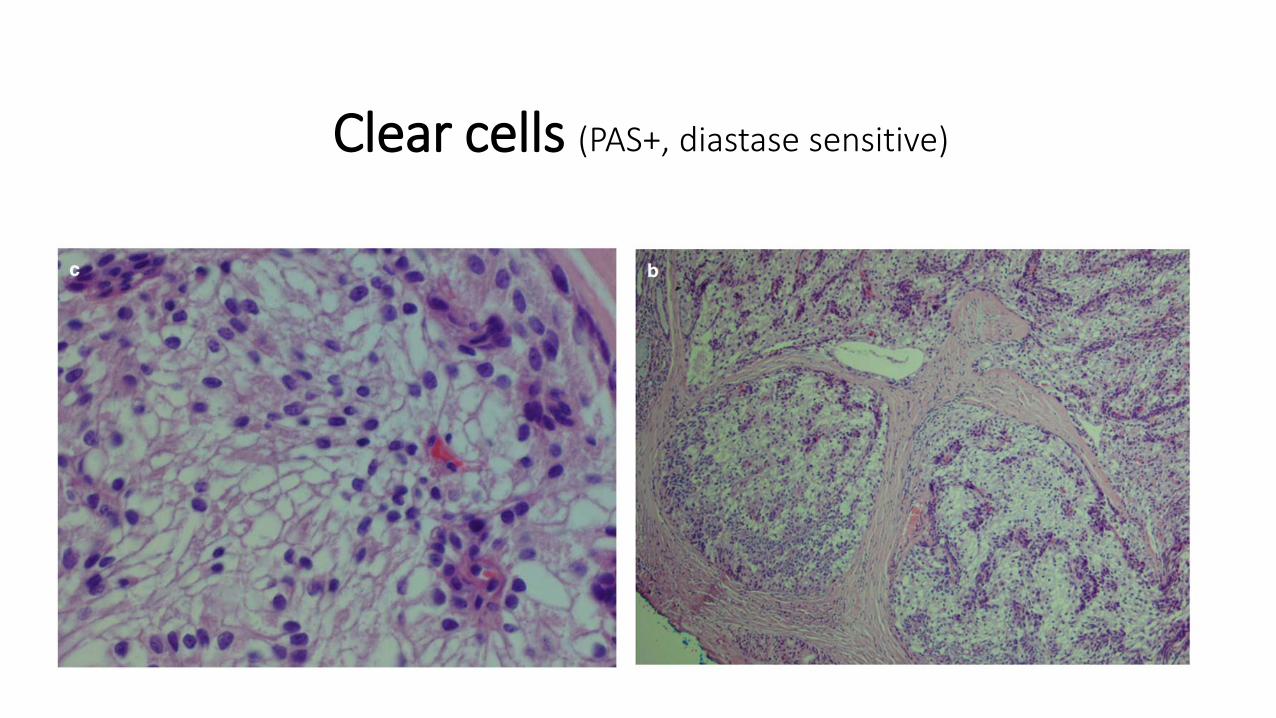
Clear cells (PAS+, diastase sensitive)

High grade MEC Cellular anaplasia
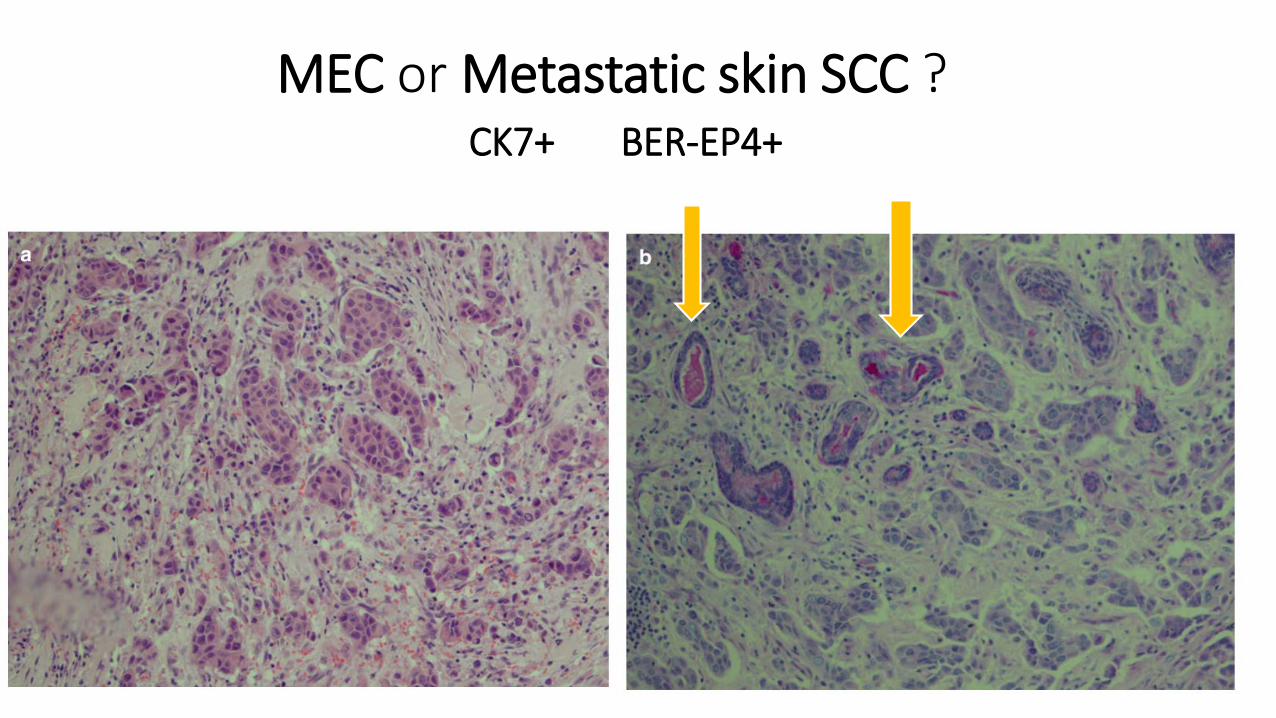
MEC or Metastatic skin SCC ? CK7+ BER-EP4+
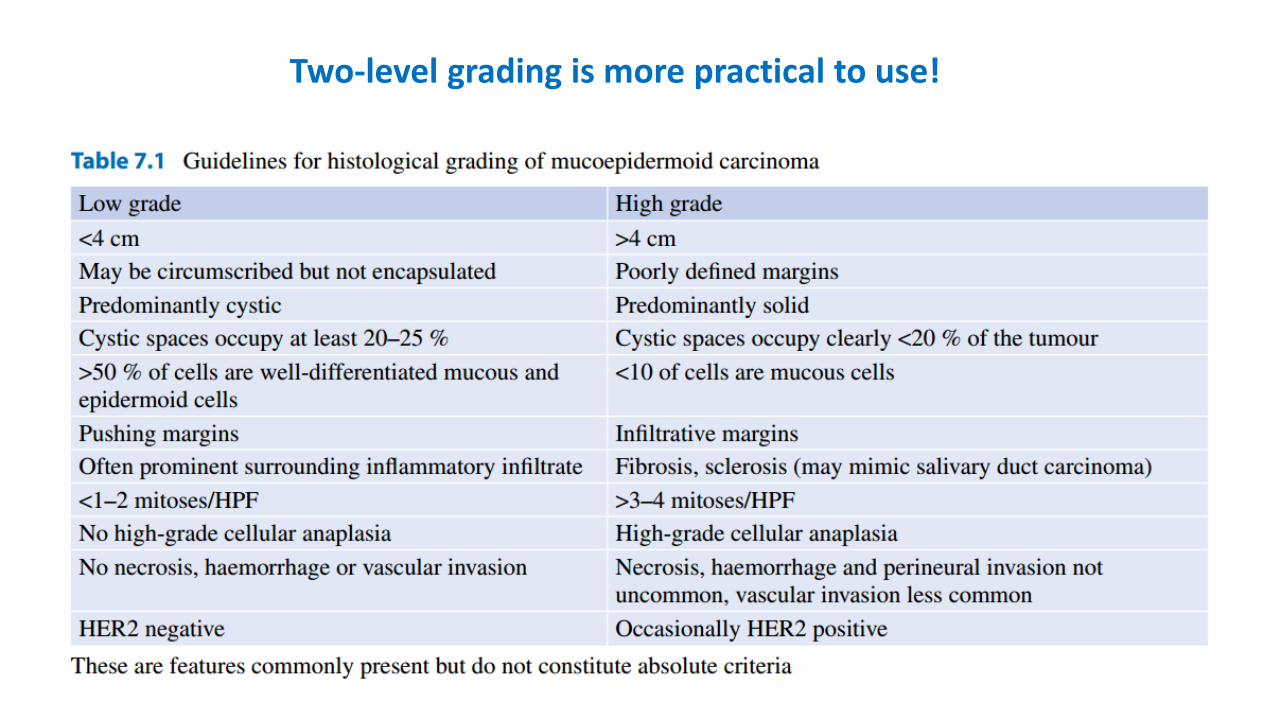
Two-level grading is more practical to use!
IHC panel for MEC• CK7 (Strong +)• CK14 (Scattered +)• P63 +( striated ductal phenotype, basal cells origin, Exclude Metastatic RCC)• MUC1, MUC4, MUC5AC +
• Myoepithelial markers-> Negative
• Mucicarmine staining

Prognosis for MEC
Correlate strongly with clinical stageTumor site
Adequacy of surgical procedure
Adjuvant therapy
• Importance of early diagnosis
Tumor size Tumor invasion Vascular/ perineural invasion Surgical margins

Case 2- video 2 attached
A 44 yrs. old woman with a submandibular
masshttps://www.dropbox.com/s/nkpxhabnkjeh2p5/2.mp4?dl=0
To see video #2, please find the attached video or, click
the below link to open it in the browser:
What is your diagnosis?
• A. Salivary duct carcinoma
• B. Adenoid cystic carcinoma
• C. Basal cell adenocarcinoma
• D. Polymorphous adenocarcinoma (PAC)
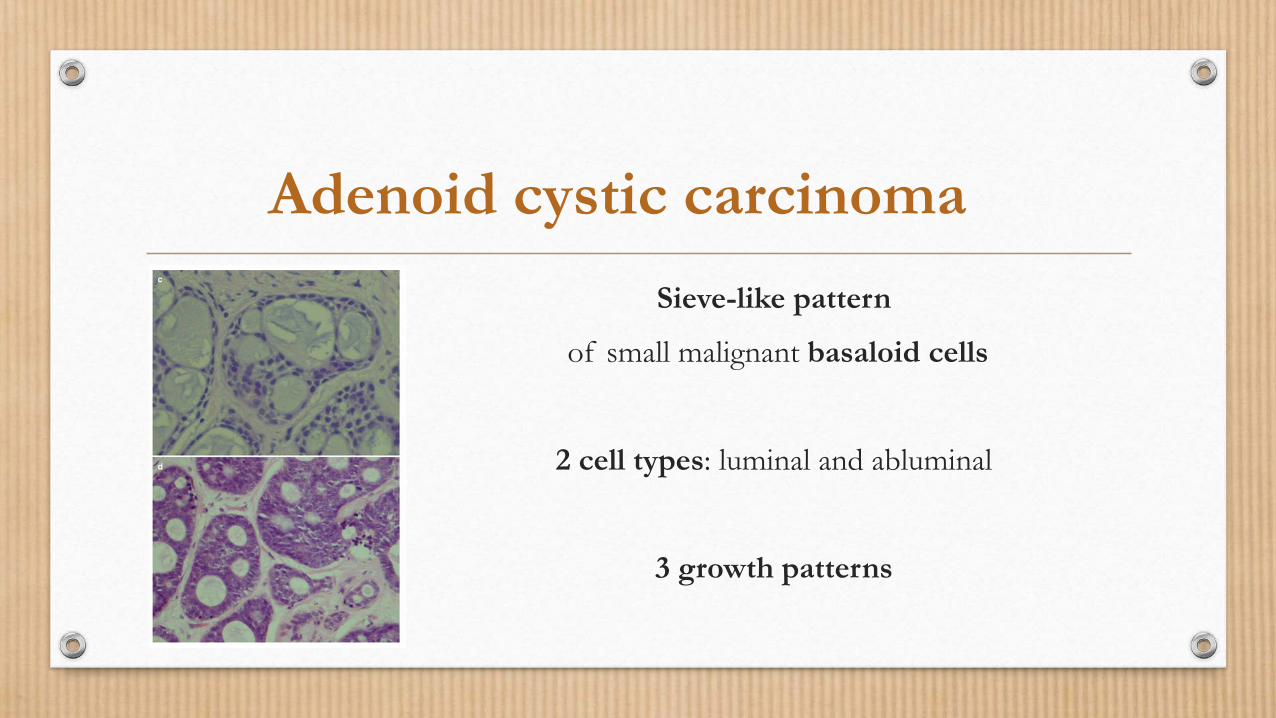
Sieve-like pattern
of small malignant basaloid cells
2 cell types: luminal and abluminal
3 growth patterns
Adenoid cystic carcinoma
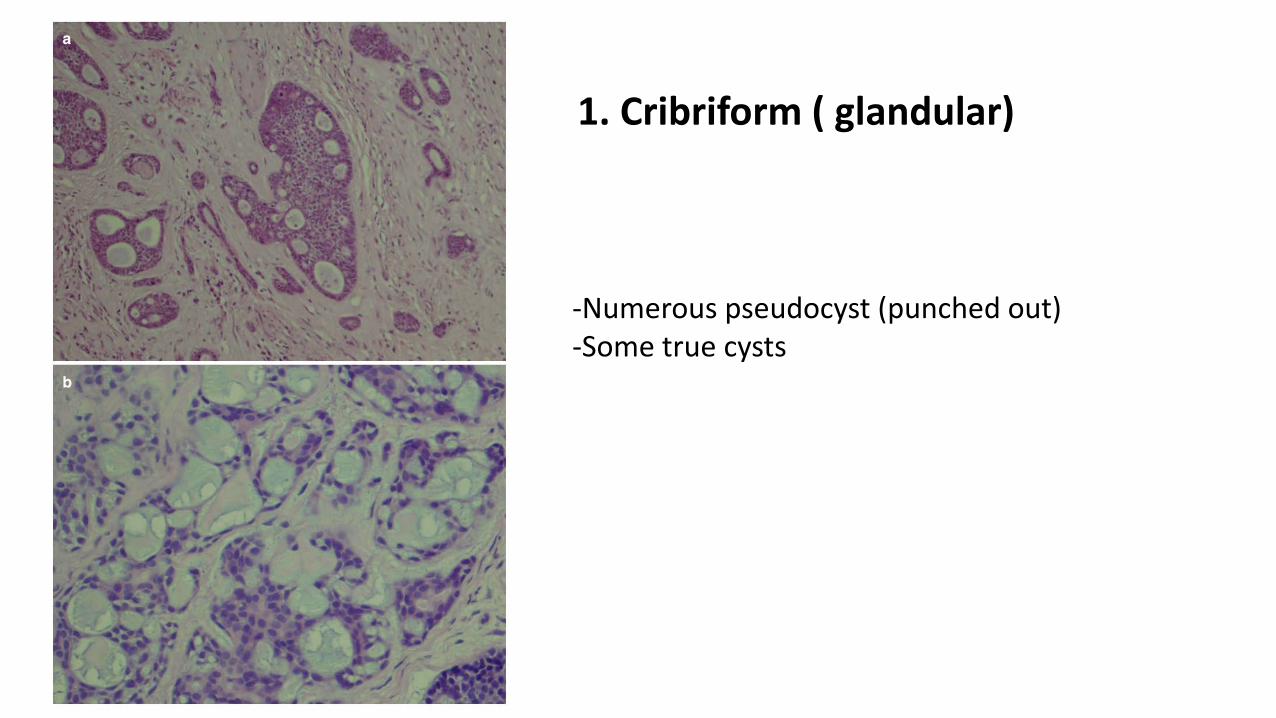
1. Cribriform ( glandular)
-Numerous pseudocyst (punched out)-Some true cysts
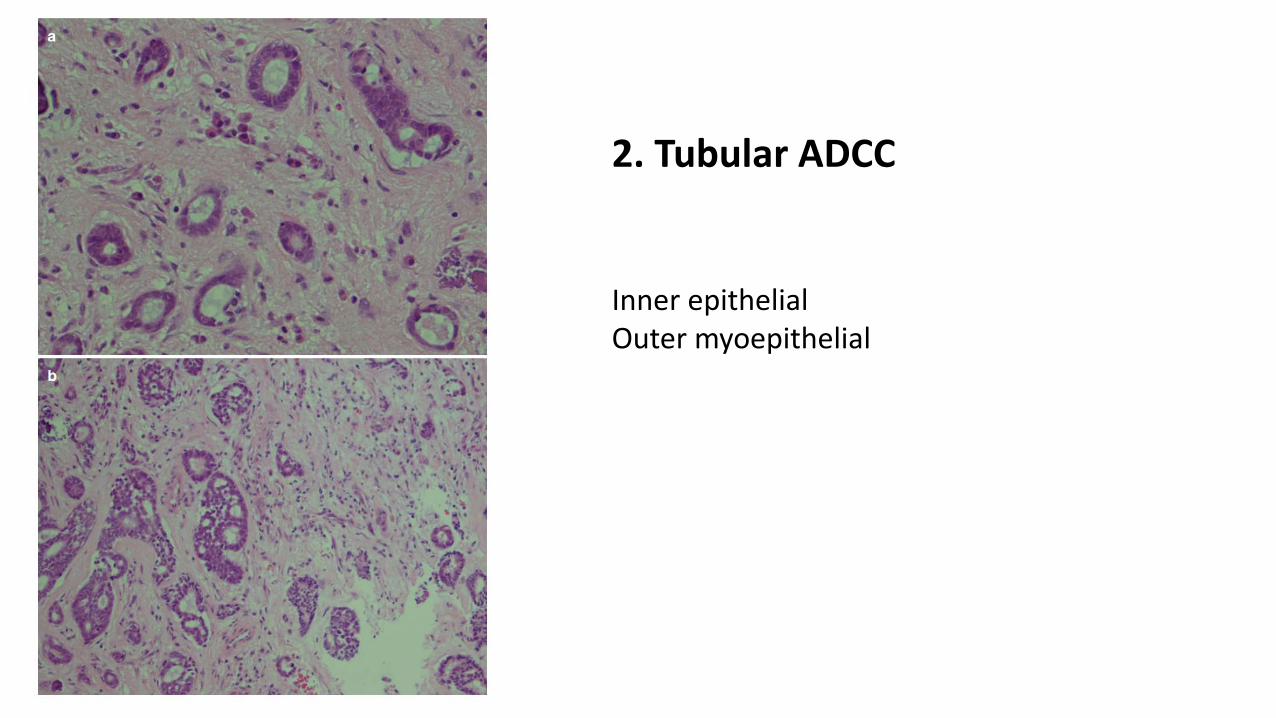
2. Tubular ADCC
Inner epithelialOuter myoepithelial
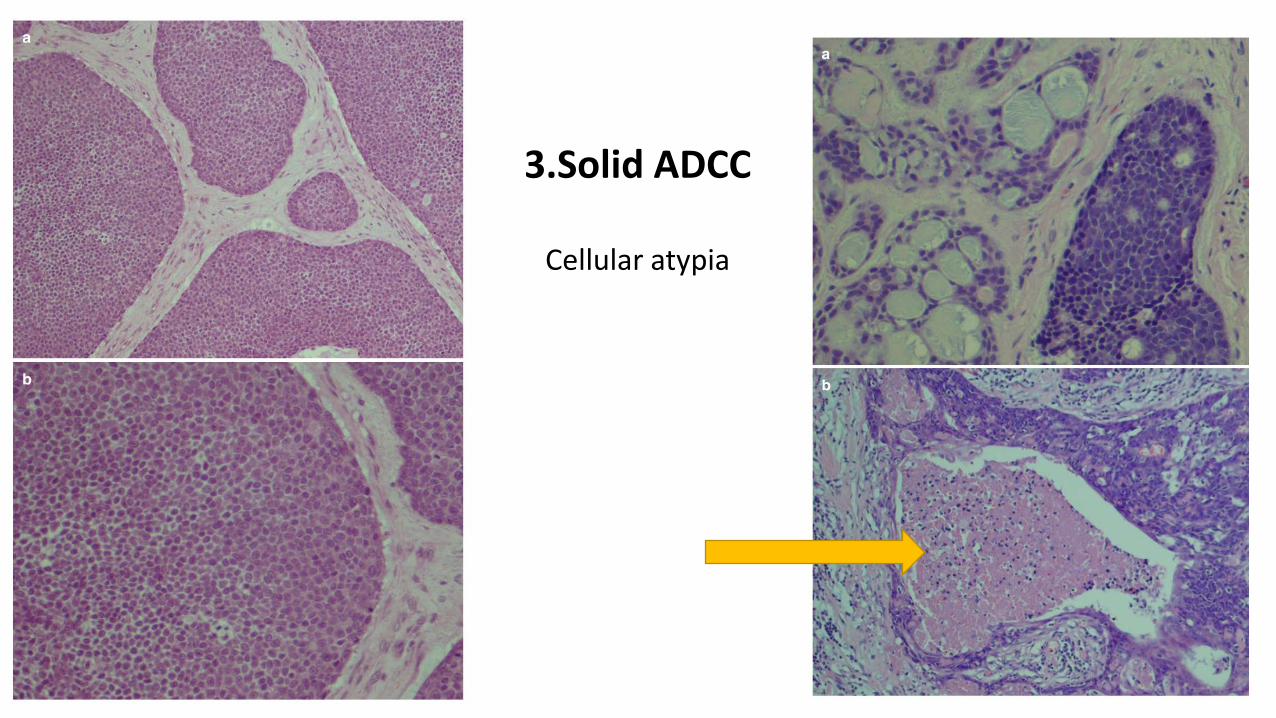
3.Solid ADCC
Cellular atypia

Perineural and intraneuralinvasion
Centered around a vessel

Infiltrative borders
Pseudopapillarygrowth pattern
PAC?
-Ki67>10%
-GFAP+

Differential diagnosisfor ADCC

ADCC
A high grade malignancy and
histological grading is of less importance!
Clinical staging

Case 3- video 3 attached
A 55 yrs. old woman with a parotid mass
https://www.dropbox.com/s/73puz6564xbcrqw/3.mp4?dl=0
To see video #3, please find the attached video or, click
the below link to open it in the browser:

What is your diagnosis?
• A. Mucoepidermoid carcinoma
• B. Acinic cell carcinoma
• C. Secretory carcinoma
• D. Metastatic thyroid carcinoma
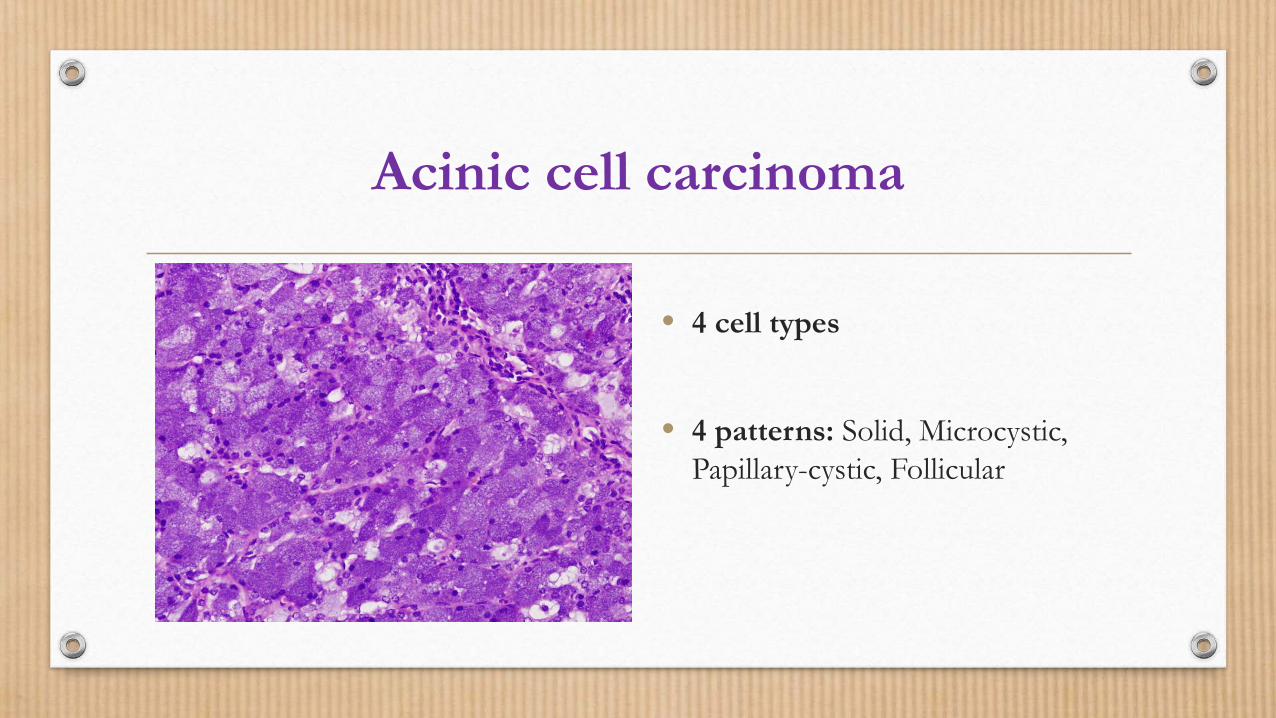
Acinic cell carcinoma
• 4 cell types
• 4 patterns: Solid, Microcystic, Papillary-cystic, Follicular
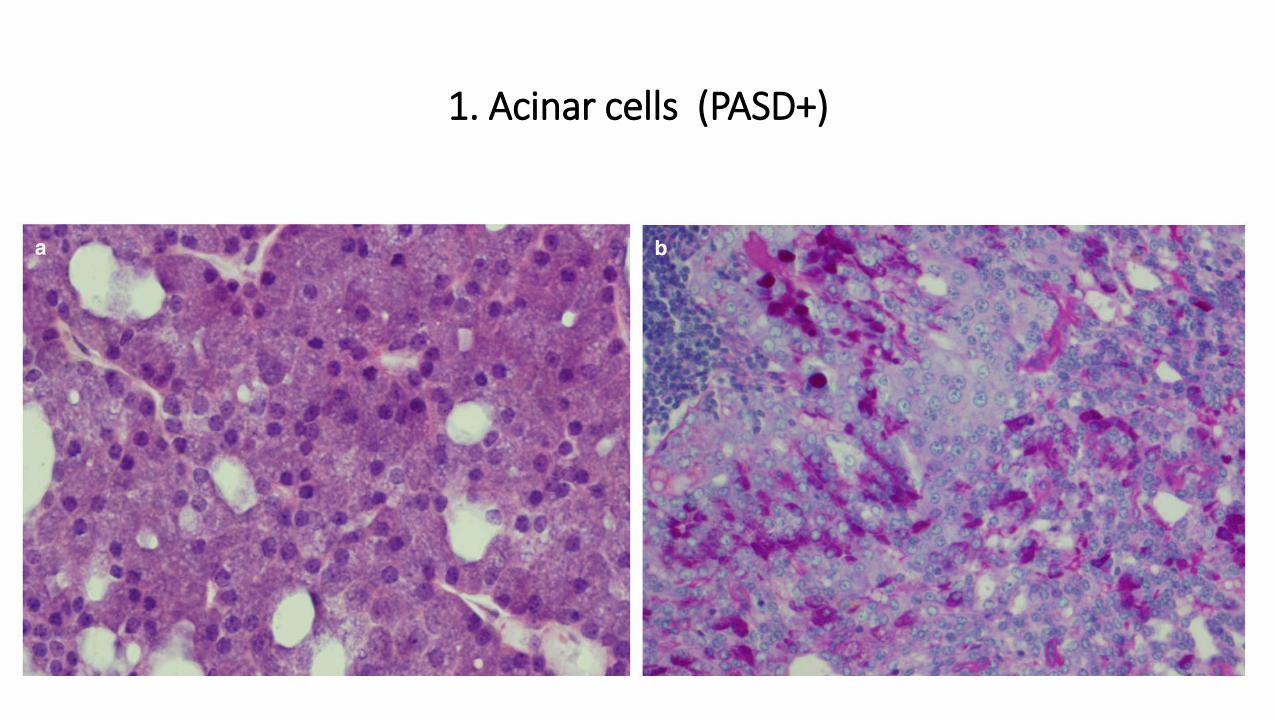
1. Acinar cells (PASD+)

2. Vacuolated cells (PAS -)( papillary cystic- microcystic variant)
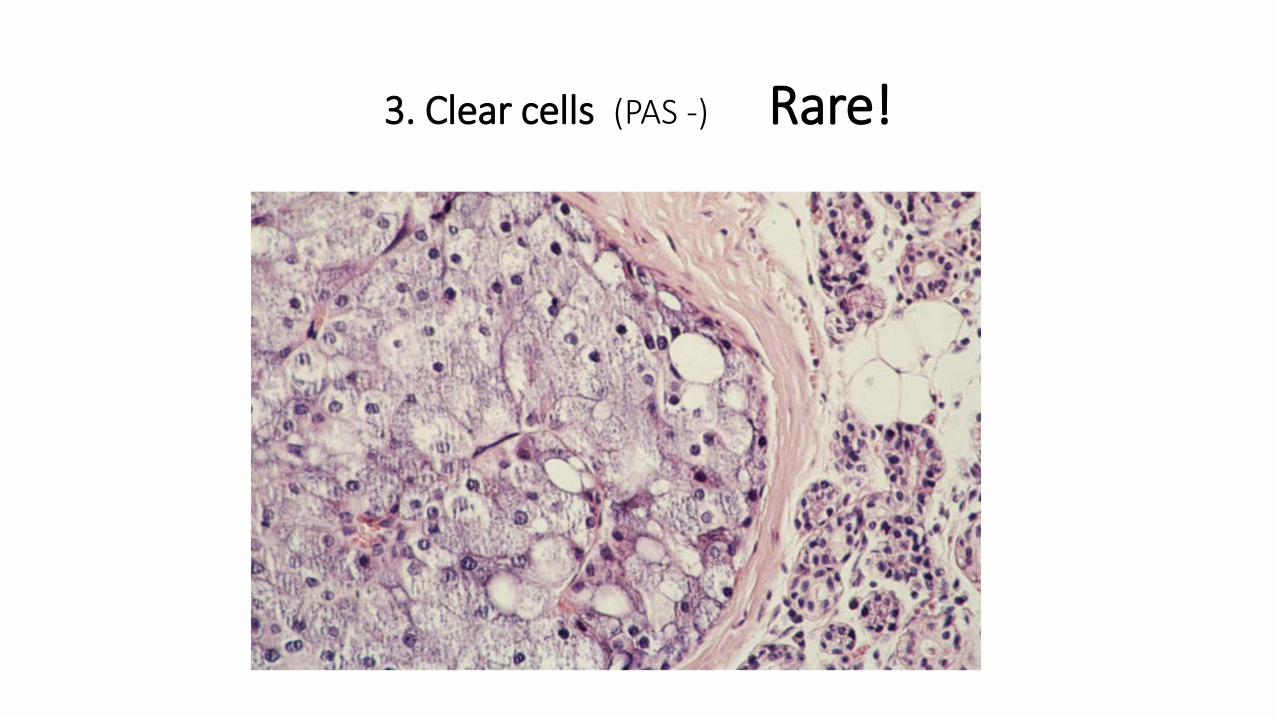
3. Clear cells (PAS -) Rare!
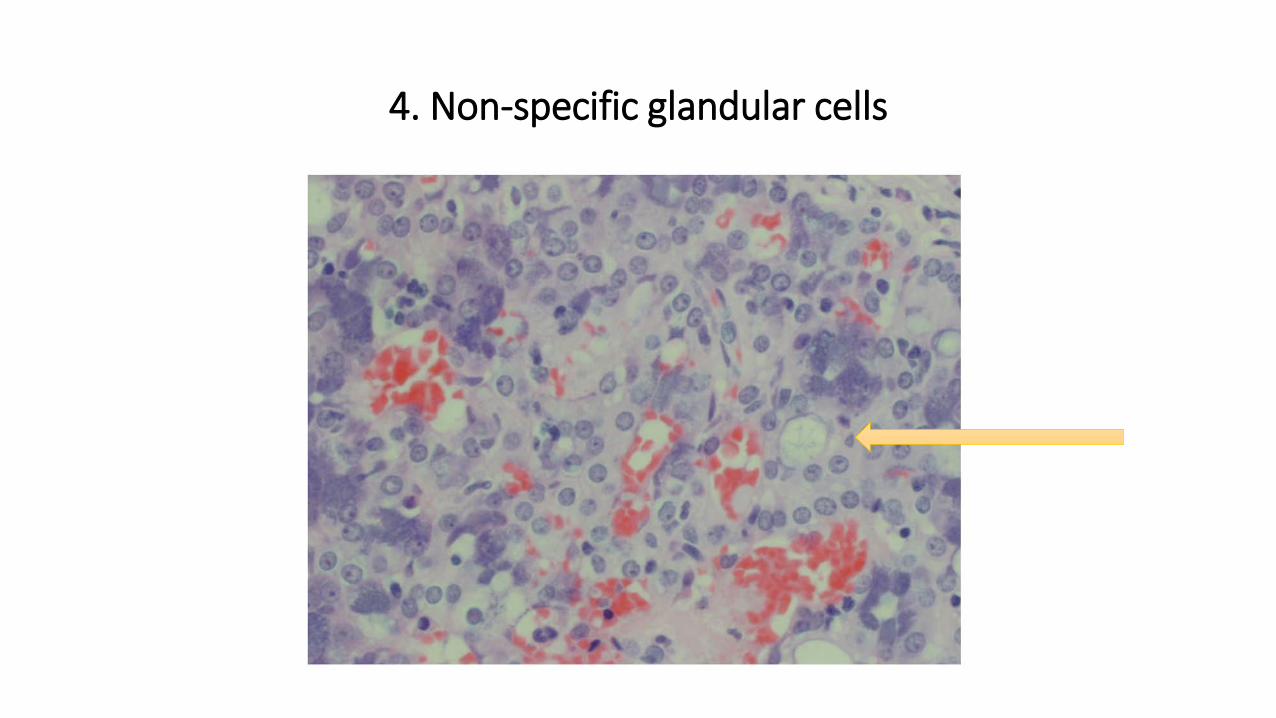
4. Non-specific glandular cells

Prominent lymphocytic infiltrationGerminal center formation
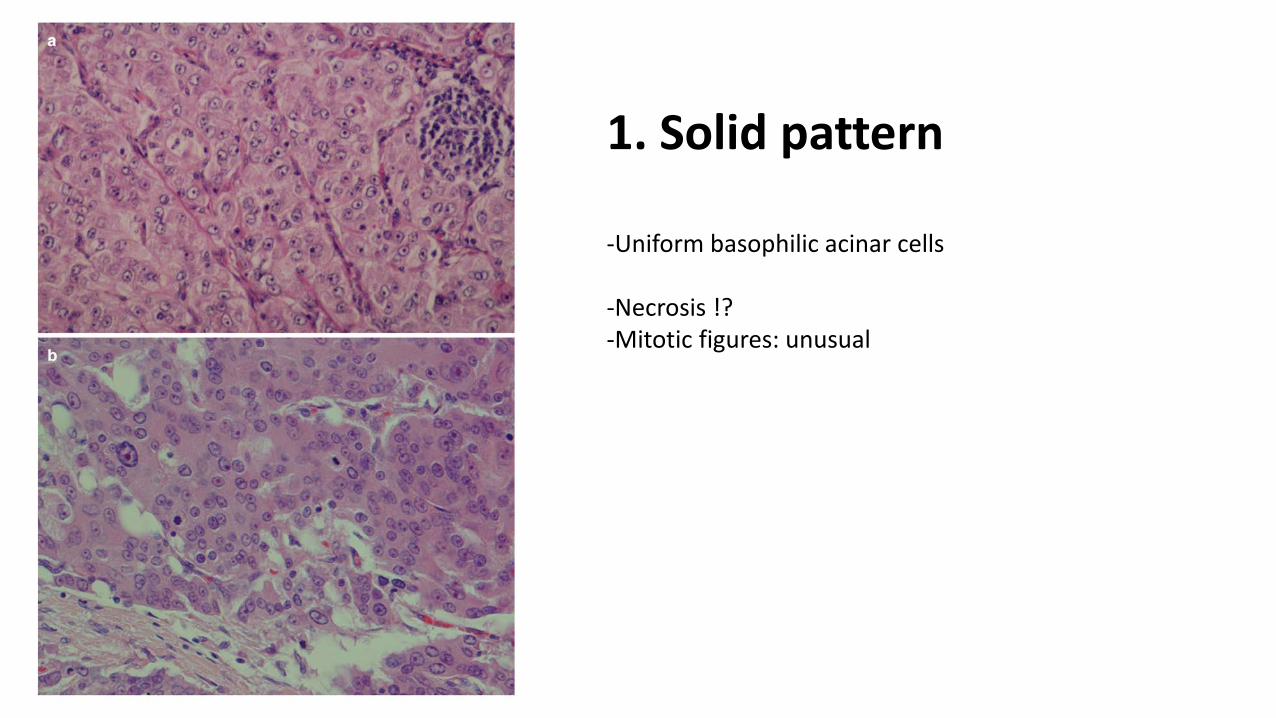
1. Solid pattern
-Uniform basophilic acinar cells
-Necrosis !?-Mitotic figures: unusual

2. Microcystic patternMucinous, proteinaceous material

3. Papillary-cystic patternACC or metastatic PTC ?

4. Follicular patternMetastatic follicular thyroid carcinoma ?

• Well-differentiated ACC associated with lymphoid stromaMicrocystic growth pattern + dense lymphoid stroma
Low Ki-67 labelling index
Thin pseudocapsule
• High grade transformation (dedifferentiation) Conventional low-grade ACC + high grade ACC
High Ki-67 labelling

ACC diagnosis and treatmentDOG1 staining for ACC diagnosis (acinar differentiation) MUC3 positive in ACC ( not in MEC, ADCC)Always negative for P63 ( MEC is always +)
• Histological grade is stronger predictor of survival than TNM stage.• Surgical resection -> excellent results• Best survival rate of all salivary gland carcinomas
MASC 2010
SC 2017
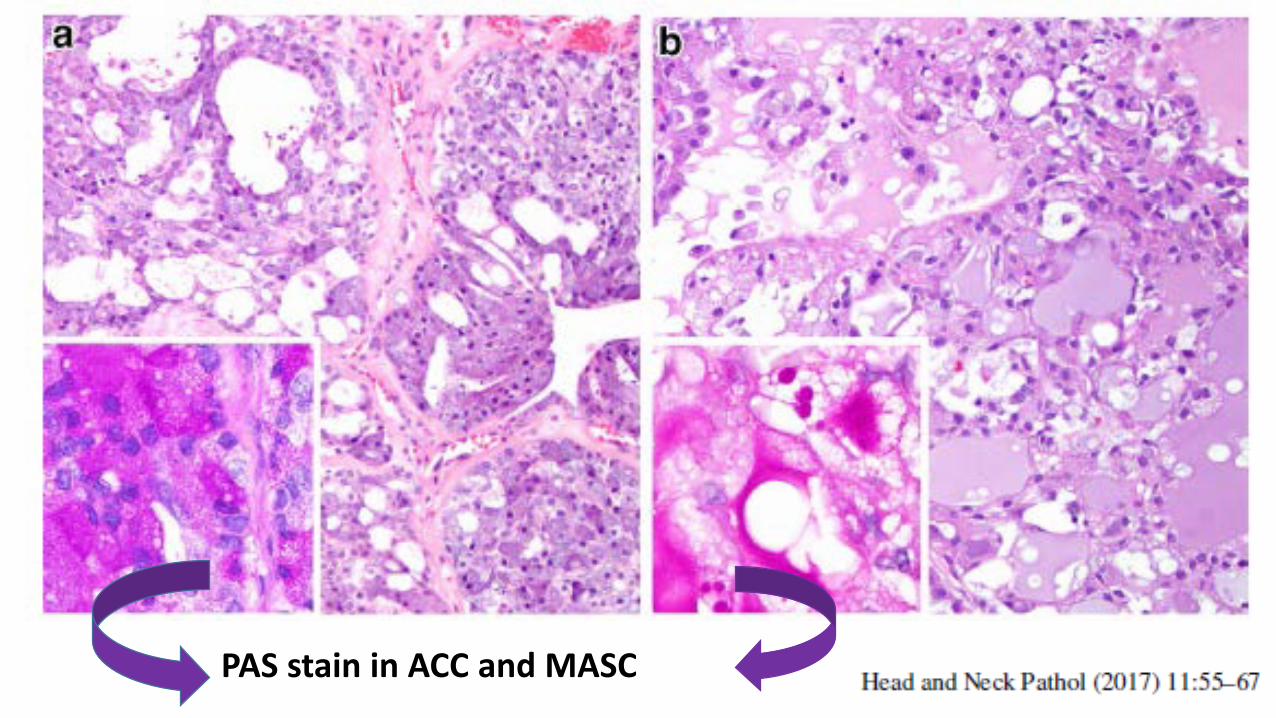
PAS stain in ACC and MASC
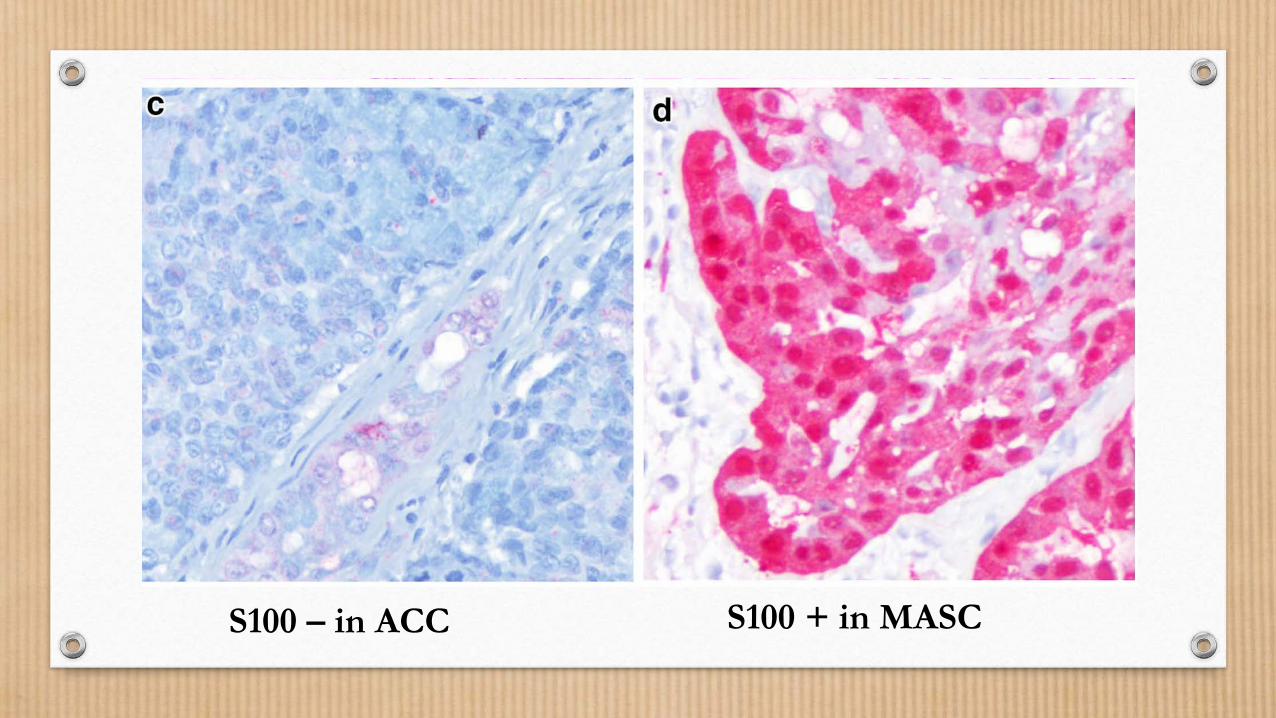
S100 – in ACC S100 + in MASC

DOG1 + in ACC(apical and membranous)
Mammaglobin + in MASC

In SC ( no other salivary gland tumor!)
ETV6-RET ETV6-MET
Positive ETV6-NTRK3 gene fusion

100 % specific90.7% sensitive

Immunohistochemistry
Plays a limited, even though important rolein diagnosing salivary gland tumors
Assist the final diagnosis! CK7+/CK20-

Strongly recommended!

Thank you and have a lovely day

















