ACG Postgraduate Course Copyright 2012 ACG October 2012 1 Refractory IBD Refractory IBD Gary R. Gary R. Lichtenstein, MD ichtenstein, MD Professor of Medicine Professor of Medicine University of Pennsylvania School of Medicine University of Pennsylvania School of Medicine Director, Center for IBD Director, Center for IBD Hospital of the University of PA Hospital of the University of PA Philadelphia,PA Philadelphia,PA Refractory IBD Refractory IBD • Establish the Correct Diagnosis, Severity Establish the Correct Diagnosis, Severity of Disease & Extent of Disease of Disease & Extent of Disease of Disease & Extent of Disease of Disease & Extent of Disease • Evaluate for Disease Complications Evaluate for Disease Complications • Evaluate for Enteric Infections Evaluate for Enteric Infections • Use Optimal Medication Doses Use Optimal Medication Doses • Miscellaneous Miscellaneous • NonAdherence NonAdherence • Paradoxical Responses Paradoxical Responses • NSAIDs NSAIDs • Cigarettes Cigarettes
Transcript
ACG Postgraduate Course Copyright 2012 ACG
October 2012 1
Refractory IBDRefractory IBD
Gary R. Gary R. LLichtenstein, MDichtenstein, MD
Professor of MedicineProfessor of Medicine
University of Pennsylvania School of MedicineUniversity of Pennsylvania School of Medicine
Director, Center for IBDDirector, Center for IBD
Hospital of the University of PAHospital of the University of PA
Philadelphia,PAPhiladelphia,PA
Refractory IBDRefractory IBD
•• Establish the Correct Diagnosis, Severity Establish the Correct Diagnosis, Severity of Disease & Extent of Diseaseof Disease & Extent of Diseaseof Disease & Extent of Diseaseof Disease & Extent of Disease
•• Evaluate for Disease Complications Evaluate for Disease Complications •• Evaluate for Enteric InfectionsEvaluate for Enteric Infections•• Use Optimal Medication DosesUse Optimal Medication Doses•• MiscellaneousMiscellaneous
I. Establish the Correct Diagnosis, Severity of I. Establish the Correct Diagnosis, Severity of Disease & Extent of DiseaseDisease & Extent of DiseaseDisease & Extent of DiseaseDisease & Extent of Disease
Ulcerative Colitis versus Crohn’s DiseaseUlcerative Colitis versus Crohn’s Disease
Disease DistributionDisease Distribution
Severity of DiseaseSeverity of Disease
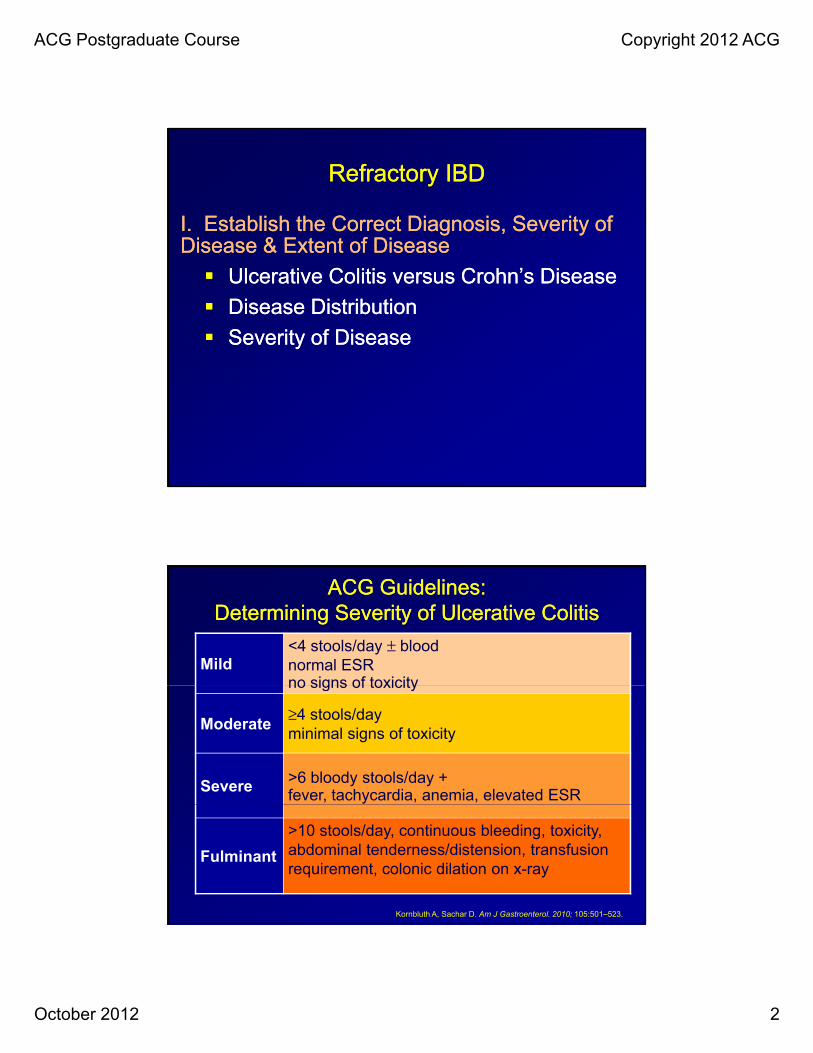
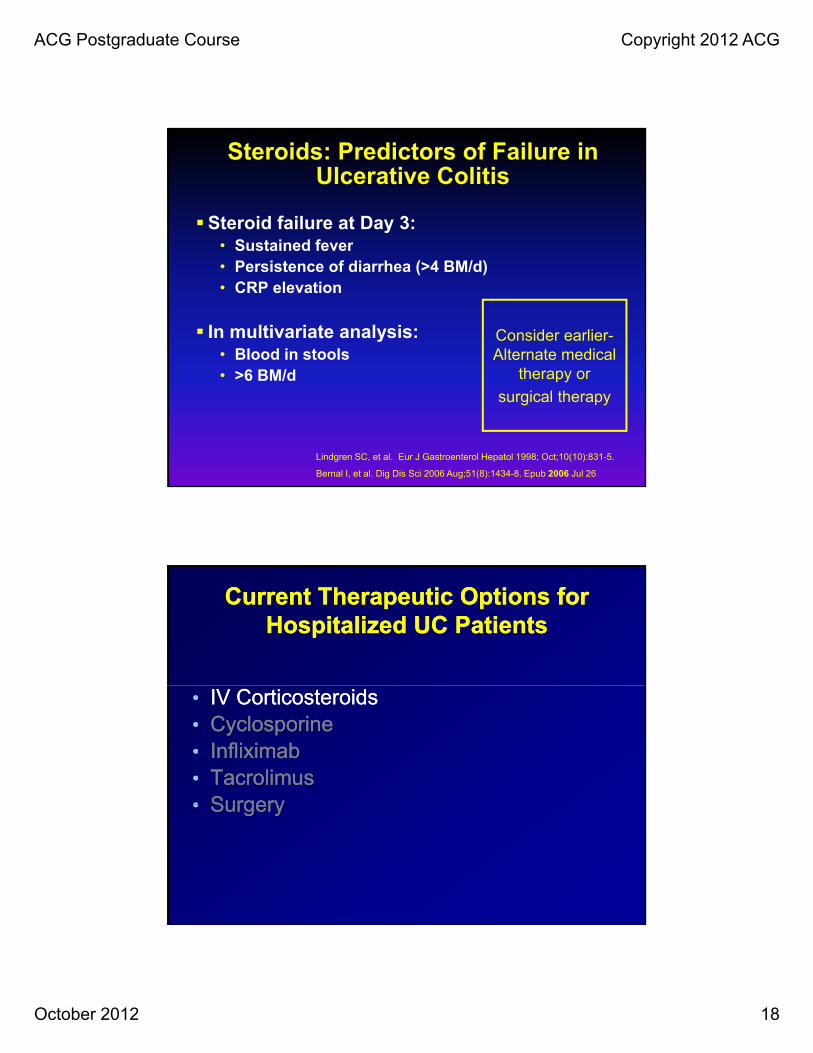
ACG Guidelines: ACG Guidelines: Determining Severity of Ulcerative ColitisDetermining Severity of Ulcerative Colitis
Mild<4 stools/day ± blood normal ESR no signs of toxicityno signs of toxicity
Moderate≥4 stools/day minimal signs of toxicity
Severe >6 bloody stools/day + fever, tachycardia, anemia, elevated ESR
Degree of obstruction (if present)Degree of obstruction (if present)
Evaluation for Dysplasia or CancerEvaluation for Dysplasia or Cancer
Evaluate for infectious ComplicationsEvaluate for infectious Complications
CMVCMV
ACG Postgraduate Course Copyright 2012 ACG
October 2012 4
CT EnterographyCT Enterography
Combines highCombines high--resolution CT scanning with some of the resolution CT scanning with some of the concepts of barium radiographyconcepts of barium radiography
Ingestion of large volume of a Ingestion of large volume of a negativenegative contrast agent contrast agent (either PO or (either PO or via via NJT) to distend loopsNJT) to distend loops water or diluted PEG or diluted methylcellulose water or diluted PEG or diluted methylcellulose
or highly diluted barium sulfate in sorbitolor highly diluted barium sulfate in sorbitol
Intravenous contrast, scan after 70 seconds Intravenous contrast, scan after 70 seconds (venous phase)(venous phase)Thi li h li l CTThi li h li l CT Thin slices on helical CTThin slices on helical CT
Radiation exposureRadiation exposure More appropriate for advanced disease and More appropriate for advanced disease and
•Detects erosions in suspected Crohn’s disease with negative SBFT / colonoscopy•Need blinded comparison studies vs other imaging to calculate true sensitivity
and specificity•Need to determine specificity (prevalence of SB erosions in general population)•Need to clarify safety in stricturing Crohn’s disease – patency capsule may help
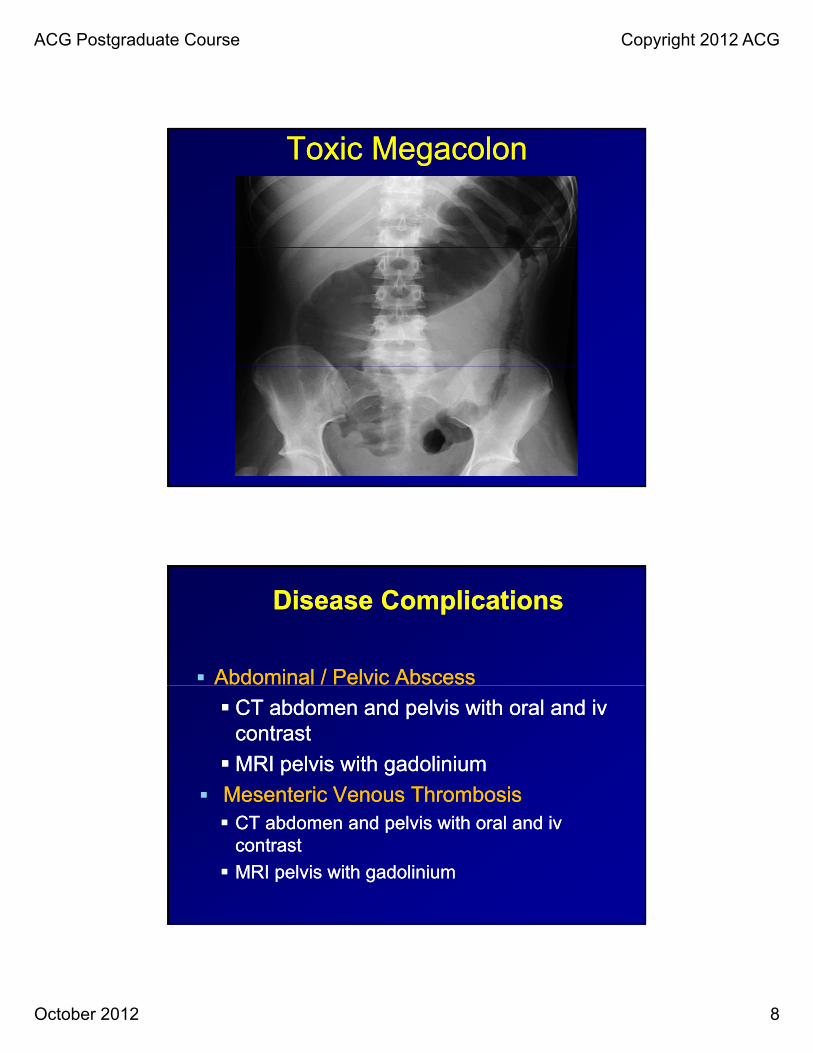
II. Identify Disease Related II. Identify Disease Related ComplicationsComplications
Identify Disease Related Identify Disease Related ComplicationsComplications
Fibrostenotic Disease Fibrostenotic Disease ––Inappropriately Treated Inappropriately Treated I fl t DiI fl t Dias Inflammatory Diseaseas Inflammatory Disease
CT enterography or MRI enterographyCT enterography or MRI enterography CT enterography or MRI enterographyCT enterography or MRI enterography•• HyperenhancementHyperenhancement
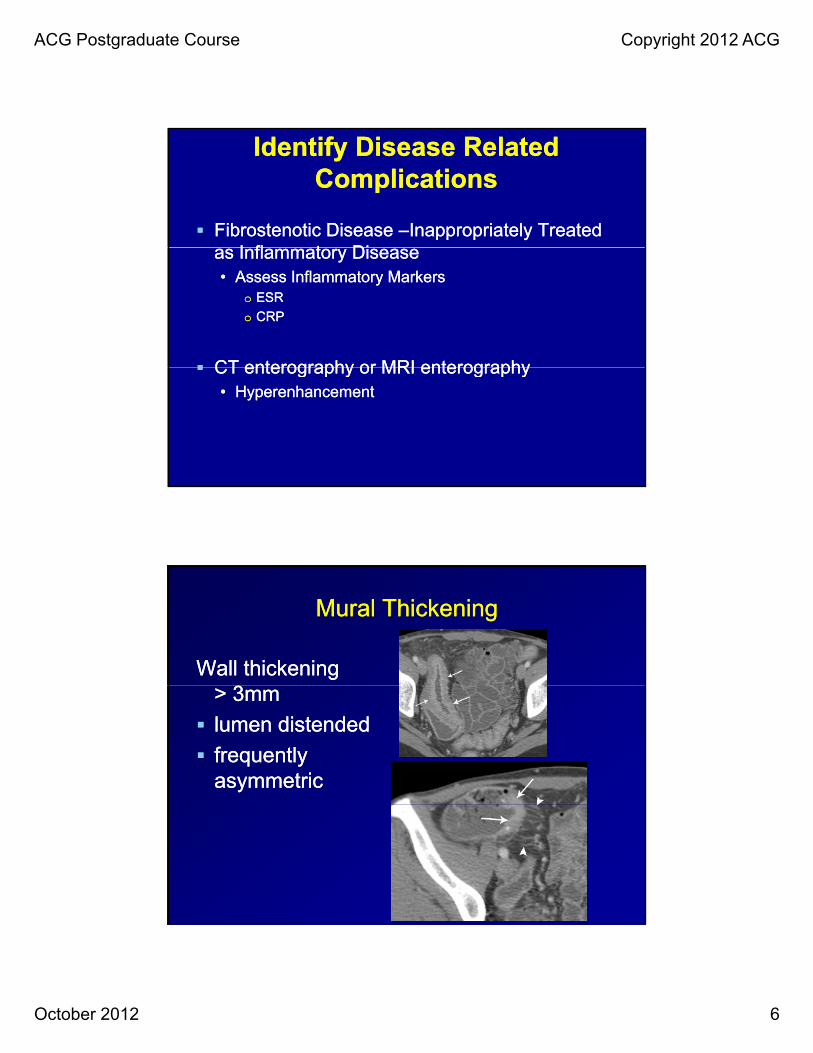
Mural ThickeningMural Thickening
Wall thickening Wall thickening > 3mm> 3mm
lumen distendedlumen distended
frequently frequently asymmetricasymmetric
ACG Postgraduate Course Copyright 2012 ACG
October 2012 7
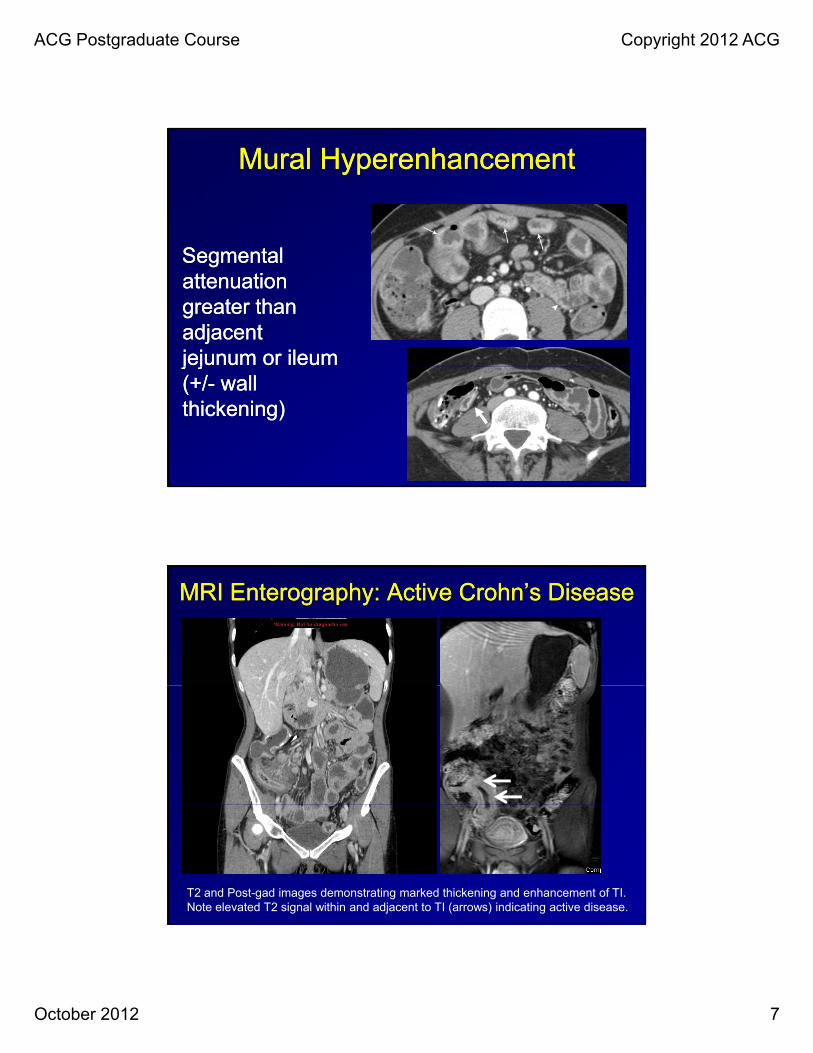
Mural HyperenhancementMural Hyperenhancement
S lS lSegmental Segmental attenuation attenuation greater than greater than adjacent adjacent jejunum or ileum jejunum or ileum j jj j(+/(+/-- wall wall thickening)thickening)
MRI Enterography: Active Crohn’s DiseaseMRI Enterography: Active Crohn’s Disease
T2 and Post-gad images demonstrating marked thickening and enhancement of TI. Note elevated T2 signal within and adjacent to TI (arrows) indicating active disease.
E Coli 0157:H7E Coli 0157:H7 Shiga ToxinShiga Toxin
ACG Postgraduate Course Copyright 2012 ACG
October 2012 10
““Pseudointractibility” of IBDPseudointractibility” of IBD
•• Cytomegalovirus (CMV)Cytomegalovirus (CMV)•• 5050--80% of the world’s population is seropositive80% of the world’s population is seropositive5050 80% of the world s population is seropositive80% of the world s population is seropositive
•• Initial infection in the immune competent host is Initial infection in the immune competent host is typically mild typically mild –– goes undetected clinicallygoes undetected clinically
•• Chronic latent state followsChronic latent state follows-- virus remains virus remains present within host cells. Virus proliferation is present within host cells. Virus proliferation is prevented by host cellprevented by host cell--mediated immunitymediated immunityprevented by host cellprevented by host cell mediated immunity. mediated immunity.
•• When immune containment failsWhen immune containment fails--reactivation reactivation with viral proliferation and severe systemic with viral proliferation and severe systemic illness may ensue.illness may ensue.
““Pseudointractibility” of IBDPseudointractibility” of IBD
•• Fever, pancytopenia, inflammatory changes of Fever, pancytopenia, inflammatory changes of multiple organsmultiple organs-- including liver, lungs, retina, colon.including liver, lungs, retina, colon.
•• Patients are rendered susceptible to systemic Patients are rendered susceptible to systemic CMV by CMV by
•• TTreatment with immunosuppressive medications orreatment with immunosuppressive medications or
•• Illnesses that reduce cell mediated immunity (e.g. Illnesses that reduce cell mediated immunity (e.g. HIV)HIV)
•• Patients with IBD get CMV in the presence of Patients with IBD get CMV in the presence of colonic inflammation and ongoing colonic inflammation and ongoing immunosuppressive therapy.immunosuppressive therapy.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 11
““Pseudointractibility” of IBDPseudointractibility” of IBD
•• A person was infected with CMV at some time A person was infected with CMV at some time during their life (uncertain exactly when).during their life (uncertain exactly when).
•• If antibody tests are paired acuteIf antibody tests are paired acute-- and convalescent and convalescent –– phase serum samples show a fourfold rise in IgG phase serum samples show a fourfold rise in IgG CMVCMV AbAb and CMV IgM antibody is present or CMVand CMV IgM antibody is present or CMVCMV CMV AbAb and CMV IgM antibody is present or CMV and CMV IgM antibody is present or CMV virus is cultured from a urine or throat specimenvirus is cultured from a urine or throat specimen--active CMV is present. active CMV is present.
Clostridium Difficile in IBDClostridium Difficile in IBD
Increasing prevalence in outIncreasing prevalence in out--patient and patient and
hospitalized patientshospitalized patients
Present in 16% of all hospitalized IBD pts.Present in 16% of all hospitalized IBD pts.
76% of infected hospitalized pts. acquired76% of infected hospitalized pts. acquired
Clostridium difficile as outpatients.Clostridium difficile as outpatients.
40% had 40% had NONO antibiotic exposureantibiotic exposure
Issa ,et al. CGH 2007
ACG Postgraduate Course Copyright 2012 ACG
October 2012 12
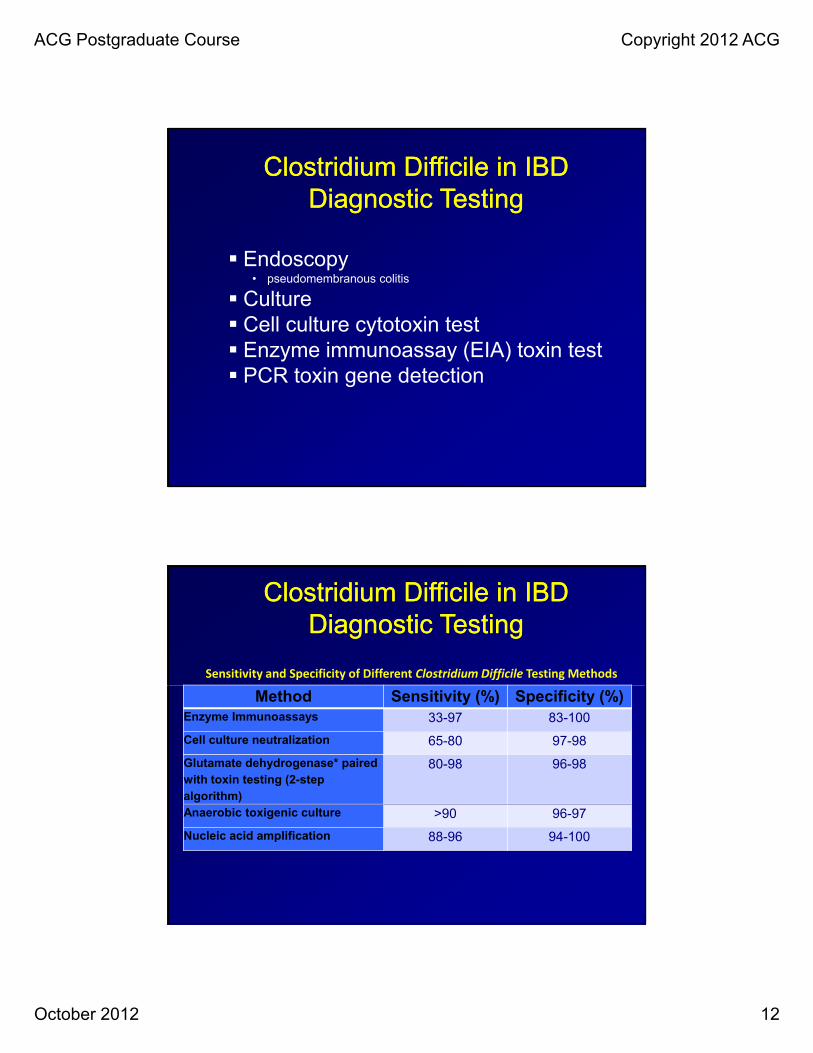
Clostridium Difficile in IBD Clostridium Difficile in IBD Diagnostic TestingDiagnostic Testing
Endoscopy• pseudomembranous colitis
Culture Cell culture cytotoxin test Enzyme immunoassay (EIA) toxin test
PCR i d i PCR toxin gene detection
Clostridium Difficile in IBD Clostridium Difficile in IBD Diagnostic TestingDiagnostic Testing
Sensitivity and Specificity of Different Clostridium Difficile Testing Methods
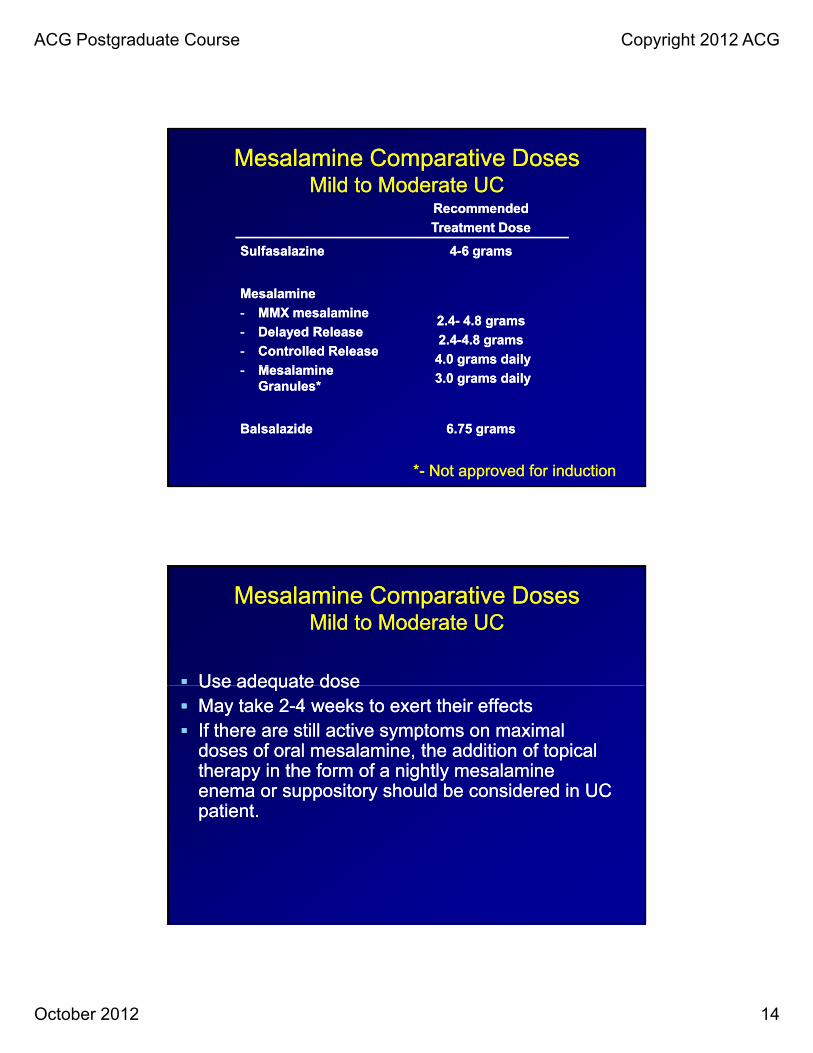
**-- Not approved for inductionNot approved for induction
Use adequate doseUse adequate dose
Mesalamine Comparative DosesMesalamine Comparative DosesMild to Moderate UCMild to Moderate UC
Use adequate doseUse adequate dose May take 2May take 2--4 weeks to exert their effects4 weeks to exert their effects If there are still active symptoms on maximal If there are still active symptoms on maximal
doses of oral mesalamine, the addition of topical doses of oral mesalamine, the addition of topical therapy in the form of a nightly mesalamine therapy in the form of a nightly mesalamine enema or suppository should be considered in UC enema or suppository should be considered in UC
ti tti tpatient.patient.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 15
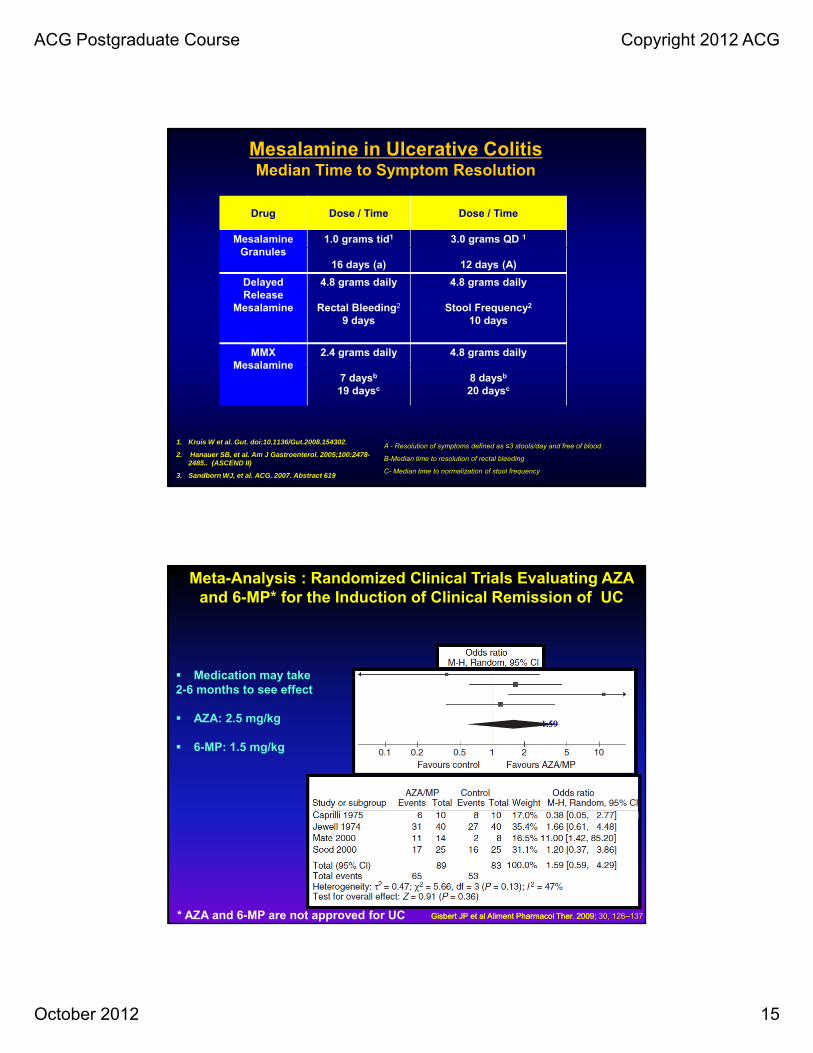
Mesalamine in Ulcerative Colitis Median Time to Symptom Resolution
Drug Dose / Time Dose / Time
Mesalamine 1.0 grams tid1 3.0 grams QD 1
Granules16 days (a) 12 days (A)
Delayed Release
Mesalamine
4.8 grams daily
Rectal Bleeding2
9 days
4.8 grams daily
Stool Frequency2
10 days
MMX Mesalamine
2.4 grams daily 4.8 grams dailyMesalamine
7 daysb
19 daysc8 daysb
20 daysc
1. Kruis W et al. Gut. doi:10.1136/Gut.2008.154302.
2. Hanauer SB, et al. Am J Gastroenterol. 2005;100:2478-2485.. (ASCEND II)
3. Sandborn WJ, et al. ACG. 2007. Abstract 619
A - Resolution of symptoms defined as ≤3 stools/day and free of blood.
B-Median time to resolution of rectal bleeding
C- Median time to normalization of stool frequency
Meta-Analysis : Randomized Clinical Trials Evaluating AZA and 6-MP* for the Induction of Clinical Remission of UC
Medication may take 2 6 h ff
1.591.59
2-6 months to see effect
AZA: 2.5 mg/kg
6-MP: 1.5 mg/kg
Gisbert JP et al Aliment Pharmacol Ther. 2009; Gisbert JP et al Aliment Pharmacol Ther. 2009; 30, 126–137* AZA and 6-MP are not approved for UC
ACG Postgraduate Course Copyright 2012 ACG
October 2012 16
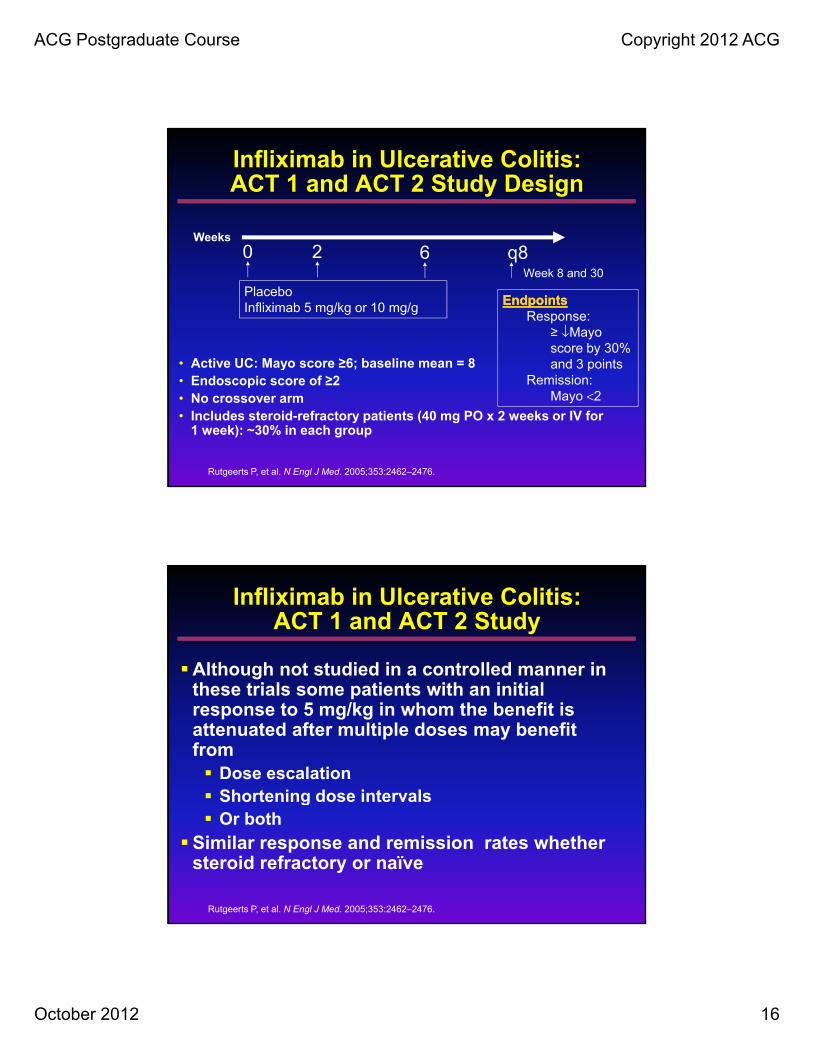
Infliximab in Ulcerative Colitis:ACT 1 and ACT 2 Study Design
Weeks
0 2 6 8
• Active UC: Mayo score ≥6; baseline mean = 8
0 2
PlaceboInfliximab 5 mg/kg or 10 mg/g
6 q8
EndpointsEndpointsResponse:
≥ ↓Mayo score by 30% and 3 points
Week 8 and 30
Active UC: Mayo score ≥6; baseline mean 8• Endoscopic score of ≥2• No crossover arm• Includes steroid-refractory patients (40 mg PO x 2 weeks or IV for
1 week): ~30% in each group
and 3 pointsRemission:
Mayo <2
Rutgeerts P, et al. N Engl J Med. 2005;353:2462–2476.
Although not studied in a controlled manner in th t i l ti t ith i iti l
Infliximab in Ulcerative Colitis:ACT 1 and ACT 2 Study
these trials some patients with an initial response to 5 mg/kg in whom the benefit is attenuated after multiple doses may benefit from Dose escalation Shortening dose intervals g Or both
Similar response and remission rates whether steroid refractory or naïve
Rutgeerts P, et al. N Engl J Med. 2005;353:2462–2476.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 17
The success of a steroid free remission at
Infliximab in Ulcerative Colitis:ACT 1 and ACT 2 Study
week 54 occurs in 21% of patients.
These studies did not prospectively address whether concomitant thiopurine therapy would influence clinical success rate.
Rutgeerts P, et al. N Engl J Med. 2005;353:2462–2476.
Severe Disease D it ti l d f
Management of Severe Ulcerative Colitis
Despite optimal dose of - Steroids orally (40-60 mg of prednisone)
* P < 0.001 vs. placebo; **P < 0.005 vs. placebo; † P = 0.009 vs. placebo. 1. Rutgeerts P, et al. Presented at DDW 2005. Chicago, IL: May 14-19, 2005. 2. Sandborn WJ, et al. Presented at DDW 2005. Chicago, IL: May 14-19, 2005.
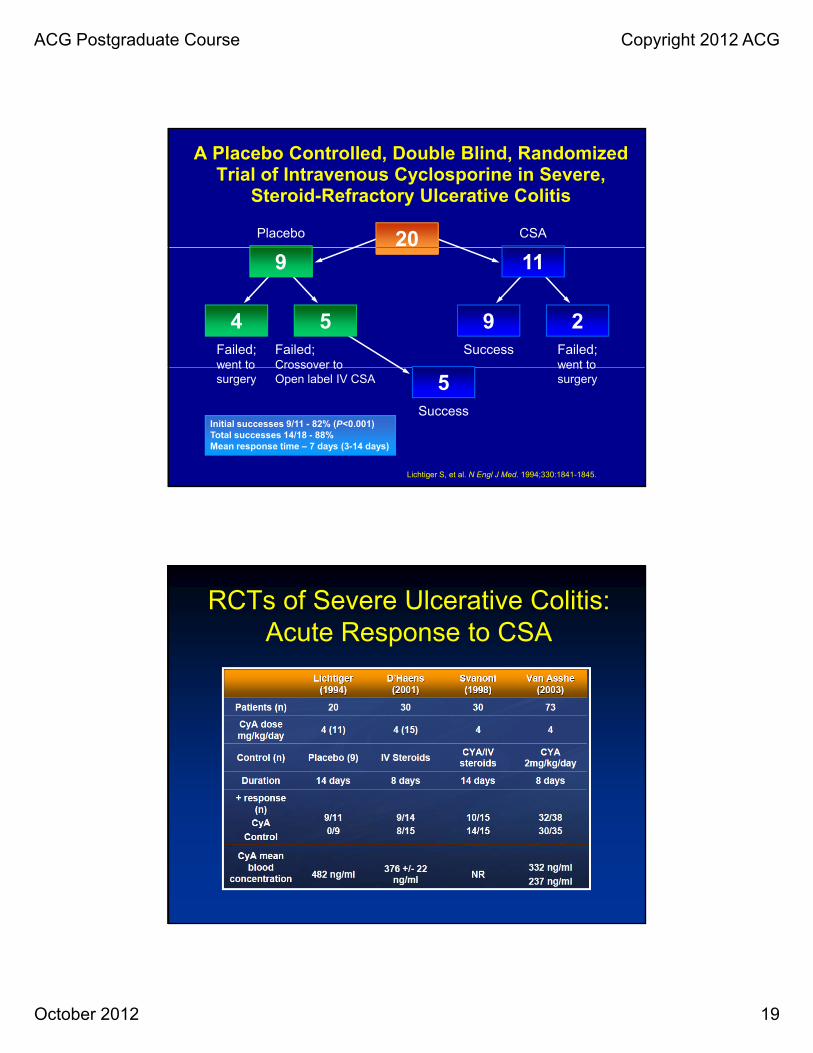
Infliximab for Severe Infliximab for Severe Ulcerative ColitisUlcerative Colitis: : Avoidance of Colectomy: Controlled Avoidance of Colectomy: Controlled trialtrial Randomized, double blind, placebo controlled trialRandomized, double blind, placebo controlled trial
P ti tP ti t f ili IV t idf ili IV t id ithith:: Patients Patients failing IV steroids failing IV steroids withwith::•• Fulminant Fulminant disease at day 4, or disease at day 4, or
•• Severe disease at Severe disease at day day 66--88
Treated withTreated with
•• single infusion 5mgsingle infusion 5mg/kg infliximab /kg infliximab (N= 24) or (N= 24) or g gg g gg ( )( )
placebo (n=21)placebo (n=21)
Clinical Endpoint at Day 90Clinical Endpoint at Day 90
•• The avoidance of death or colectomyThe avoidance of death or colectomy
• Jarnerot G, et. Al Gastroenterology 2005; 128: 1805
ACG Postgraduate Course Copyright 2012 ACG
October 2012 21
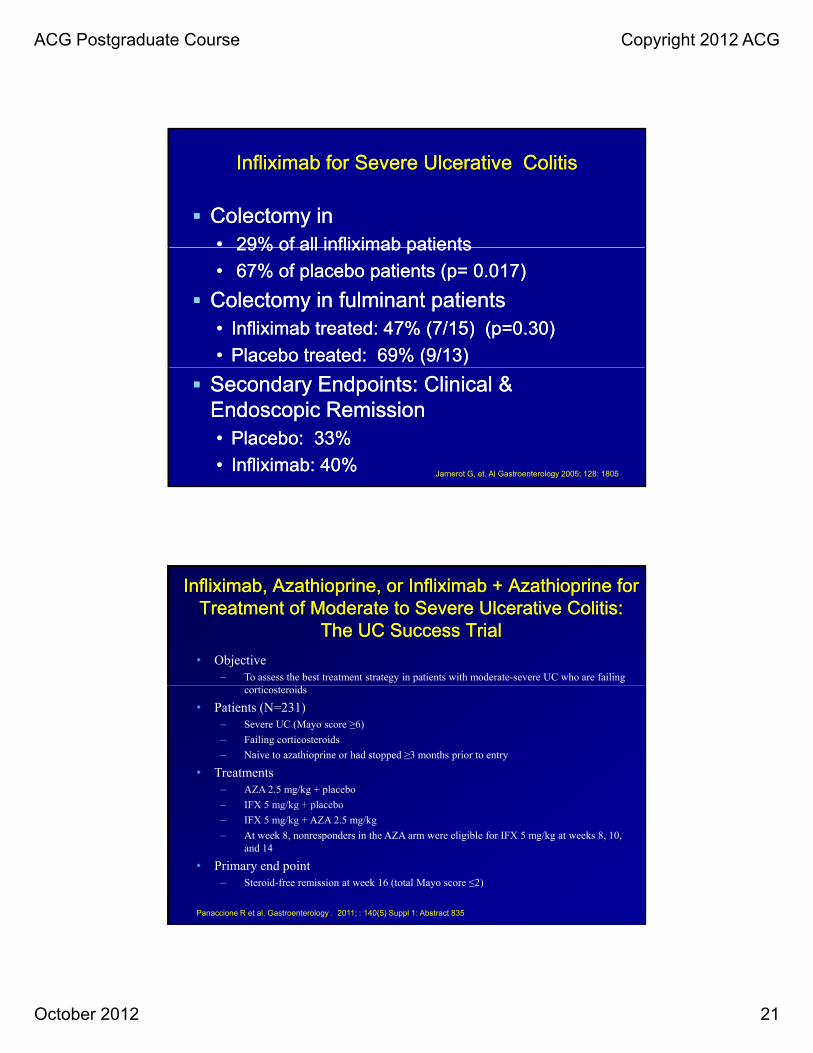
Infliximab for Severe Infliximab for Severe Ulcerative Ulcerative ColitisColitis
Colectomy in Colectomy in •• 2929% of all infliximab patients% of all infliximab patients2929% of all infliximab patients% of all infliximab patients
•• 6767% of placebo % of placebo patients (ppatients (p= = 0.017)0.017)
Colectomy in fulminant Colectomy in fulminant patients patients •• IInfliximab treated: 47% (7/15) (p=0.30) nfliximab treated: 47% (7/15) (p=0.30)
Infliximab, Azathioprine, or Infliximab + Azathioprine for Infliximab, Azathioprine, or Infliximab + Azathioprine for Treatment of Moderate to Severe Ulcerative Colitis: Treatment of Moderate to Severe Ulcerative Colitis:
The UC Success TrialThe UC Success Trial
• Objective– To assess the best treatment strategy in patients with moderate-severe UC who are failing
corticosteroids
• Patients (N=231)– Severe UC (Mayo score ≥6)
– Failing corticosteroids
– Naive to azathioprine or had stopped ≥3 months prior to entry
• Treatments– AZA 2.5 mg/kg + placebo
IFX 5 mg/kg + placebo– IFX 5 mg/kg + placebo
– IFX 5 mg/kg + AZA 2.5 mg/kg
– At week 8, nonresponders in the AZA arm were eligible for IFX 5 mg/kg at weeks 8, 10, and 14
• Primary end point– Steroid-free remission at week 16 (total Mayo score ≤2)
Panaccione R et al. Gastroenterology . 2011; : 140(5) Suppl 1: Abstract 835
ACG Postgraduate Course Copyright 2012 ACG
October 2012 22
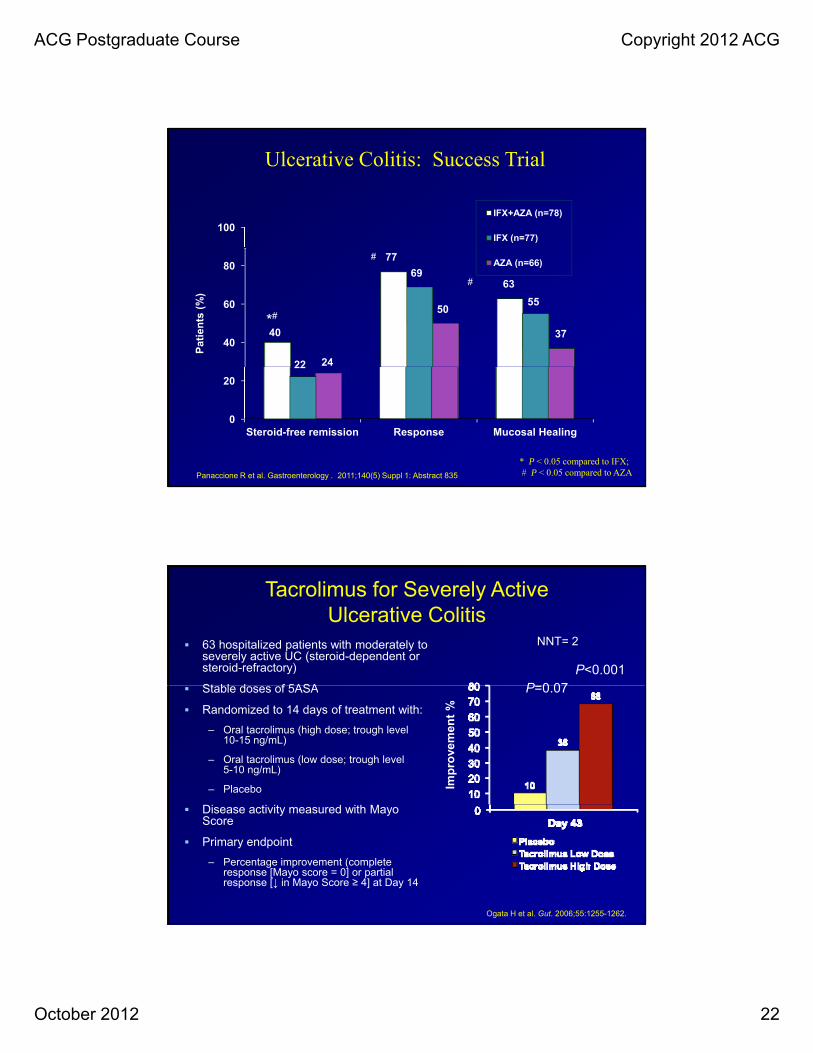
Ulcerative Colitis: Success Trial
100
IFX+AZA (n=78)
IFX (n=77)
40
60
80
40
77
63
22
69
55
24
50
37
AZA (n=66)
Pat
ien
ts (
%)
*#
#
#
0
20
Steroid-free remission Response Mucosal Healing
22
* P < 0.05 compared to IFX;# P < 0.05 compared to AZAPanaccione R et al. Gastroenterology . 2011;140(5) Suppl 1: Abstract 835
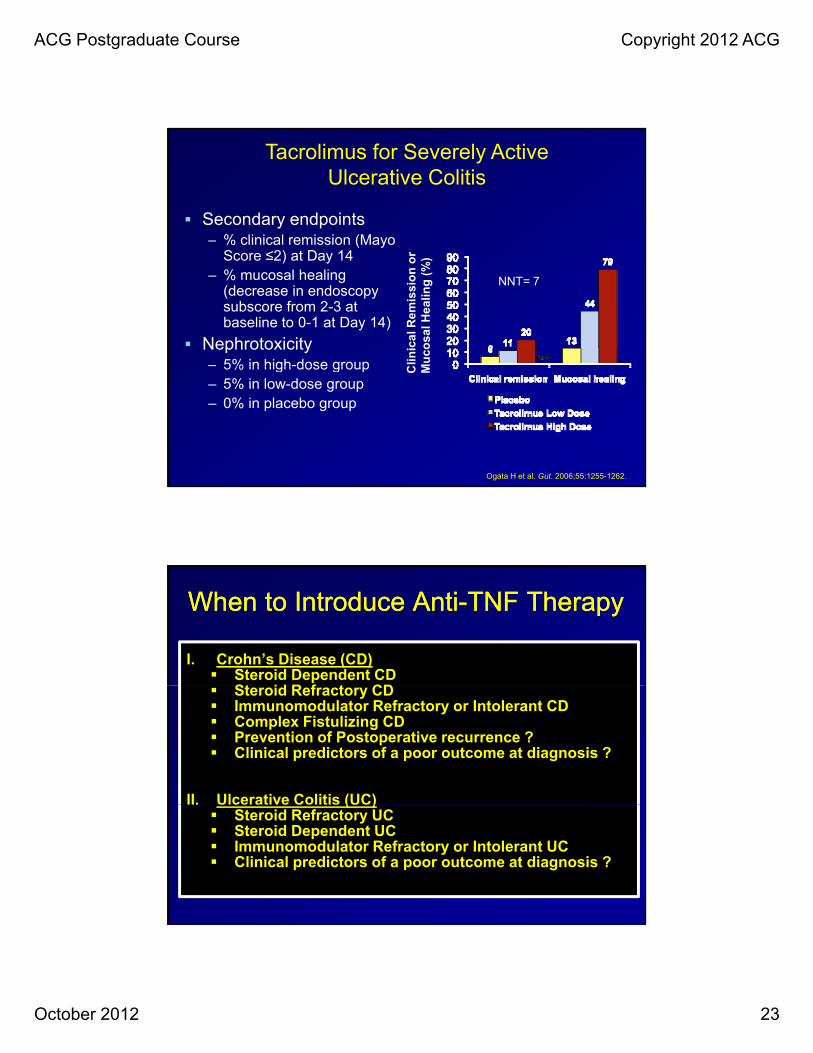
63 hospitalized patients with moderately to severely active UC (steroid-dependent or steroid-refractory)
– Percentage improvement (complete response [Mayo score = 0] or partial response [↓ in Mayo Score ≥ 4] at Day 14
Ogata H et al. Gut. 2006;55:1255-1262.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 23
Secondary endpoints– % clinical remission (Mayo
Tacrolimus for Severely Active Ulcerative Colitis
( yScore ≤2) at Day 14
– % mucosal healing (decrease in endoscopy subscore from 2-3 at baseline to 0-1 at Day 14)
Nephrotoxicity – 5% in high-dose group C
linic
al R
emis
sio
n o
rM
uco
sal H
eali
ng
(%
)
NNT= 7
5% in high dose group– 5% in low-dose group – 0% in placebo group
C M
Ogata H et al. Gut. 2006;55:1255-1262.
When to Introduce AntiWhen to Introduce Anti--TNF TherapyTNF Therapy
I. Crohn’s Disease (CD) Steroid Dependent CD
St id R f t CD Steroid Refractory CD Immunomodulator Refractory or Intolerant CD Complex Fistulizing CD Prevention of Postoperative recurrence ? Clinical predictors of a poor outcome at diagnosis ?
II. Ulcerative Colitis (UC)U ce at e Co t s (UC) Steroid Refractory UC Steroid Dependent UC Immunomodulator Refractory or Intolerant UC Clinical predictors of a poor outcome at diagnosis ?
ACG Postgraduate Course Copyright 2012 ACG
October 2012 24
Dosing of AntiDosing of Anti--TNF TherapyTNF Therapy
I. Infliximab 5 mg/kg at 0, 2, 6 weeks then every 8 weeks Dose escalation to 10 mg/kg up to every 4 weeks
maximum
II. Adalimumab 160 mg at 0 then 80 mg at 2 wks then 40 mg sq every
2 weeks Dose escalation to 40 mg sq weeklyDose escalation to 40 mg sq weekly
III. Certolizumab Pegol 400 mg sq at 0 then 400 mg at 2 wks then 400 mg sq
every 2 weeks Extra single 400 mg sq dose at week 3
Secondary NonresponderSwitch from Infliximab to Adalimumab
• GAIN trial, 325 adults 18-75 years of age with moderate to severe Crohn disease (CDAI score, 220-moderate to severe Crohn disease (CDAI score, 220450 points) and who had lost response to infliximab or had adverse events were randomly assigned to receive induction doses of adalimumab, 160 mg/80 mg, or placebo at weeks 0 and 2; 301 completers
• Twenty-one percent (34 of 159) of patients in the adalimumab group vs 7% (12 of 166) in placebo g p ( ) pgroup achieved remission at week 4
• 70-point response at week 4 in 52% (82 of 159) of patients in adalimumab group vs 34% (56 of 166) of patients in placebo group
Sandborn WJ, et al. Ann Intern Med. 2007;146(12):829-38.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 25
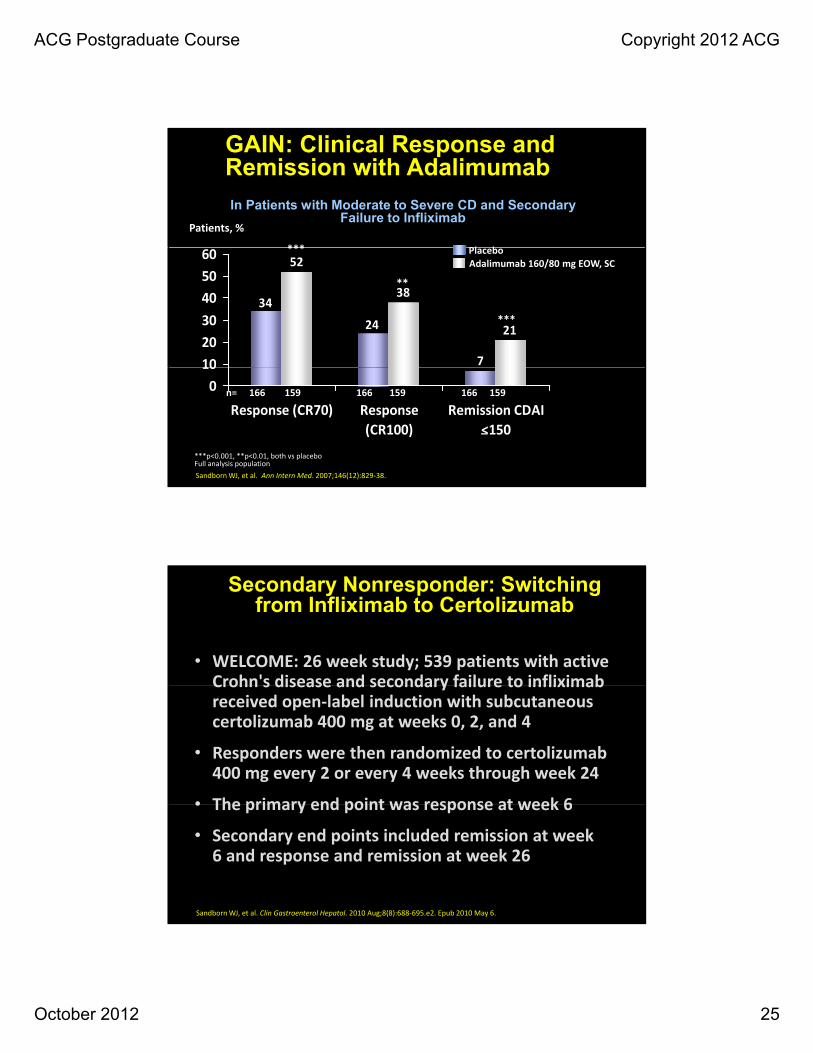
GAIN: Clinical Response and Remission with Adalimumab
In Patients with Moderate to Severe CD and Secondary Failure to Infliximab
Patients, %
*** Pl b
7
24
34
21
38
52
102030405060 ***
**
***
PlaceboAdalimumab 160/80 mg EOW, SC
Sandborn WJ, et al. Ann Intern Med. 2007;146(12):829-38.
010
Response (CR70) Response(CR100)
Remission CDAI<150
n= 166 159 166 159 166 159
_
***p<0.001, **p<0.01, both vs placeboFull analysis population
Secondary Nonresponder: Switching from Infliximab to Certolizumab
• WELCOME: 26 week study; 539 patients with active Crohn's disease and secondary failure to infliximabCrohn s disease and secondary failure to infliximab received open-label induction with subcutaneous certolizumab 400 mg at weeks 0, 2, and 4
• Responders were then randomized to certolizumab 400 mg every 2 or every 4 weeks through week 24
• The primary end point was response at week 6• The primary end point was response at week 6
• Secondary end points included remission at week 6 and response and remission at week 26
Sandborn WJ, et al. Clin Gastroenterol Hepatol. 2010 Aug;8(8):688-695.e2. Epub 2010 May 6.
ACG Postgraduate Course Copyright 2012 ACG
October 2012 26
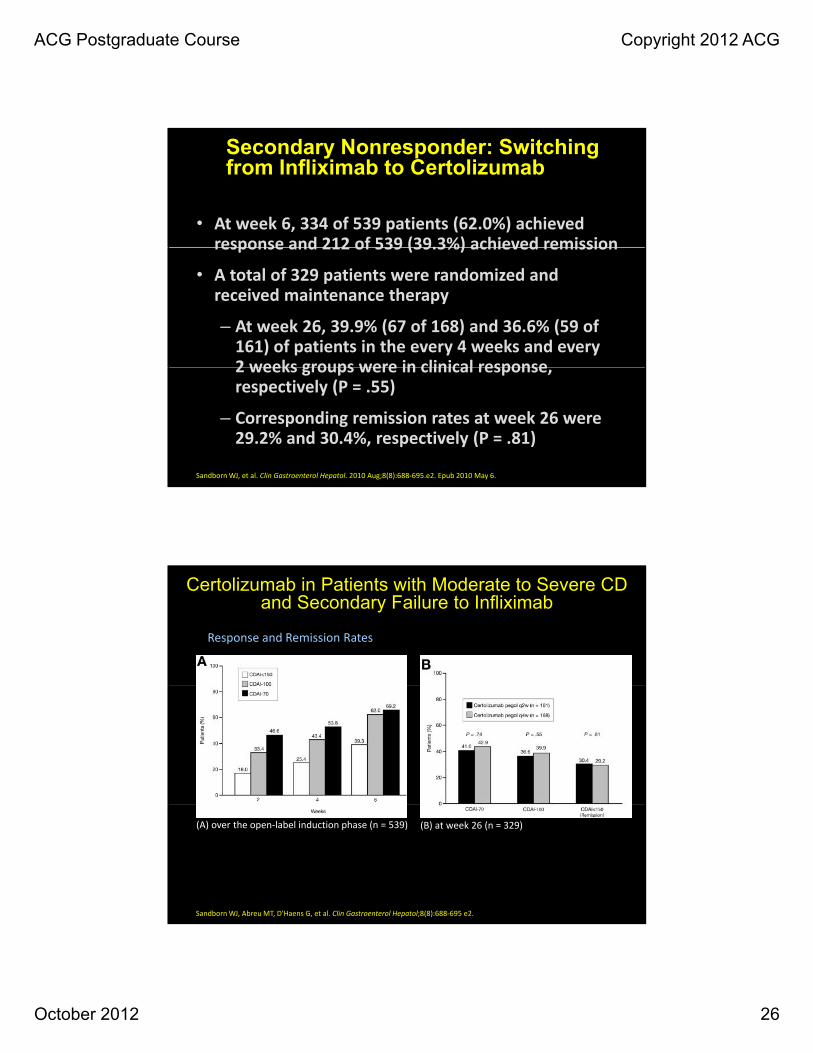
• At week 6, 334 of 539 patients (62.0%) achieved response and 212 of 539 (39.3%) achieved remission
Secondary Nonresponder: Switching from Infliximab to Certolizumab
response and 212 of 539 (39.3%) achieved remission
• A total of 329 patients were randomized and received maintenance therapy
– At week 26, 39.9% (67 of 168) and 36.6% (59 of 161) of patients in the every 4 weeks and every 2 weeks groups were in clinical response2 weeks groups were in clinical response, respectively (P = .55)
– Corresponding remission rates at week 26 were 29.2% and 30.4%, respectively (P = .81)
Sandborn WJ, et al. Clin Gastroenterol Hepatol. 2010 Aug;8(8):688-695.e2. Epub 2010 May 6.
Certolizumab in Patients with Moderate to Severe CD and Secondary Failure to Infliximab
(B) at week 26 (n = 329)Response and remission rates
ACG Postgraduate Course Copyright 2012 ACG
October 2012 27
Secondary NonresponderSwitching to a Third Anti-TNF
• Open label study of the use of certolizumab or adalimumab after failure and/or intolerance to two /different anti-TNF agents
• Sixty-seven patients treated with certolizumab (n = 40) or adalimumab (n = 27) were included – Clinical response observed in 41 patients (61%) at week 6
and 34 patients (51%) at week 20Probability of remaining on treatment at 3 6 and 9– Probability of remaining on treatment at 3, 6 and 9 months was 68%, 60% and 45%, respectively
– At end of follow-up, third anti-TNF stopped in 36 patients for intolerance (n = 13), or failure (n = 23)
– Two deaths observed (sudden death and line sepsis)
Allez M, et al. Aliment Pharmacol Ther;31(1):92-101.
V. Immunogenicity
• Three potential strategies alone or in combination to lessen immunogenicity to anti-TNF agents and g y gthus lessen the potential for drug resistance.
Concomitant immunosuppressant – AZA, 6-MP, MTX
Induction and maintenance dosing of anti-TNFInduction and maintenance dosing of anti TNF therapy- NOT on demand
Premedication with hydrocortisone 200 mg iv
ACG Postgraduate Course Copyright 2012 ACG
October 2012 28
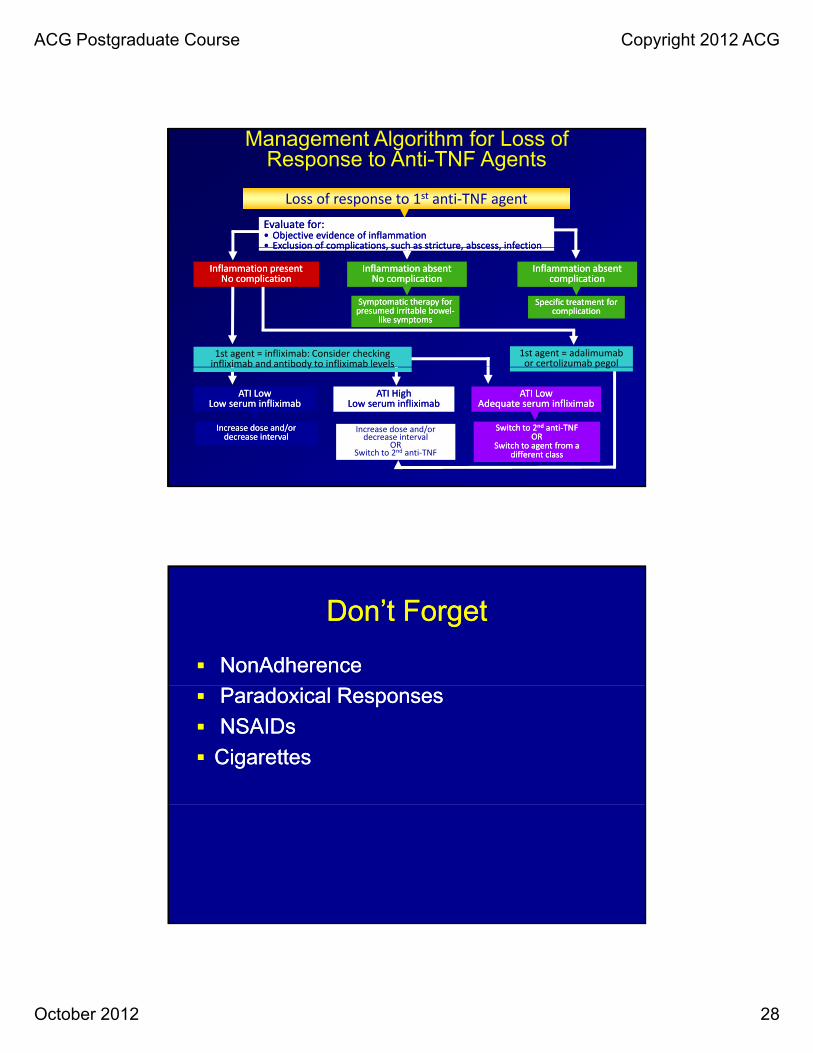
Loss of response to 1st anti-TNF agent Evaluate for:Evaluate for:•• Objective evidence of inflammationObjective evidence of inflammation•• Exclusion of complications, such as stricture, abscess, infectionExclusion of complications, such as stricture, abscess, infection
Management Algorithm for Loss of Response to Anti-TNF Agents
1st agent = adalimumab or certolizumab pegol
1st agent = infliximab: Consider checking infliximab and antibody to infliximab levels






















![Lichtenstein v. Lichtenstein · [Cite as Lichtenstein v.Lichtenstein, 2020-Ohio-5080.] COURT OF APPEALS OF OHIO EIGHTH APPELLATE DISTRICT COUNTY OF CUYAHOGA RYAN LICHTENSTEIN, : Plaintiff-Appellee,](https://static.documents.pub/doc/80x56/60903f096995511fe42a0d9e/lichtenstein-v-cite-as-lichtenstein-vlichtenstein-2020-ohio-5080-court-of.jpg)
