Page 1
Seizures and Epilepsy
Medical Director
Acute Neurological Services
Swedish Medical Center
Englewood, Colorado
Assistant Clinical Professor
University of Colorado
School of Medicine
Denver, Colorado
Ira Chang, MD
Board Review Course: NCS, Montreal 2011
Page 2
Seizures in Critical Care
Page 3
Principles
• Seizures are common in critically ill
patients
– variety of etiologies, including metabolic
• Definitions of status epilepticus has
shortened to 5min
• NCSE is common after treating CSE
• Immediate goal is to stop seizure activity
(after ABCs) – clinical and electrographic
Page 4
Principles (cont)
• Inc morbidity and mortality the longer the
seizures (CSE/NCSE) last
• Standard treatment algorithm for early
seizure tx (0-20min)
• Various definitions and approaches for
refractory status (30-60min or lack of
response to 2 IV agents)
• Standard approach to weaning off cIV
agents
Page 5
Principles (cont)
• Increasing role of continuous EEG
• Increasing experience in newer agents
• Consider autoimmune etiologies
• Consider adjunctive use of hypothermia
• Prevention of recurrence depends on
etiology and choice of AED
• Increasing recognition of SUDEP
Page 6
Incidence of seizures • Seizures
– Medical ICU -217 pts (Bleck 1993)
• 28.8% encephalopathy
• 28.1% seizures
• 0.5% status epilepticus
• Status epilepticus
– 3-5% of all ED admissions (Hauser 1990)
– 125,000-195,000 cases/year (DeLorenzo 1995,1996)
• Refractory SE
– 43% of SE pts (no response to 2 IV AEDs) (Holtkamp
2005)
Page 7
Predisposing Factors
• Hypoxia/ischemia
• Drug/substance tox
– Antibiotics
– Antidepressants
– Antipsychotics
– Bronchodilators
– Local anesthetics
– Immunosuppressives
– Stimulant drugs
• Drug/subs withdrawal
– Barbiturates
– Benzos
– Opioids
– Alcohol
• Infection/fever
• Metabolic – Ca2+, Na+,
Glu, Phos, renal
• craniotomy
Page 8
NCSE Incidence
• After control of CSE: 164 pt in eval with cEEG x 24 hrs
(DeLorenzo 1998)
– 48% with sz on EEG
– 14% with NCSE, mostly complex partial
• ICU: 236 pts in coma with 30min EEG (Towne 2000)
– 8% with NCSE
– Of these, 42% due to anoxia, 22% with stroke
• NICU: 124 pts monitored by cEEG (Jordon 1999)
– 34% with NCS
– 27% with NCSE
Page 9
High risk neurological factors
Stroke
• Hemorrhagic
• Larger cortical
• Acute confusional state
Neoplasm
• cortical
• Primary
• metastatic
Head trauma
• Contusion
• SDH
• Depressed skull fx
• Penetrating missile
• Post surgical
Mirski, M. in Seizures in Crit Care 2005
Page 10
Etiology
Adults (Claassen 2009)
• 42% prior h/o epilepsy
– 34% had low AED level
– 12% present with SE
• 22% new stroke
• 22% discont. AEDs
• 10% anoxia/hypoxia
• 10% metabolic
• 10% etoh withdrawal
(From Chen 2006)
Pediatric (Lacroix 1994)
• PICU population
– 32% epilepsy
– 13.6% atypical febrile
convulsions
– 13% meningitis
– 13% encephalitis
– 1.5-5% intox, tumor,
anoxia, Htn crisis, metab
Page 11
NCS Etiology
ICU : NCSE
• 42% anoxia/hypoxia
• 22% stroke
• 5% infection
• 5% head trauma
• 5% metabolic
• 5% etoh/AED withdrawal
• 5% tumor
(Towne 2000)
NICU: NCS
• 60% metabolic coma
• 56% epilepsy
• 54% brain tumor
• 33% CNS infection
• 28% head trauma
• 26% CNS ischemia
• 22% ICH
(Jordan 1999)
Page 12
Definitions
• Continuous or intermittent seizure activity
> 30 min without consciousness
• Seizure
– Lasts > 5 min
– 2 seizures with persistent alt mental status
Page 13
Status Epilepticus
• Seizure subtypes
– Generalized convulsive
– Nonconvulsive status (altered to comatose)
• Absence or petit mal status
• Secondary generalized seizures
• Complex partial seizures
• Subclinical SE
– focal motor SE (face, arm twitching)
Page 14
Pathophysiology • Not just a prolonged seizure
– Reconfiguration of excitatory/inhibitory brain
pathways into positive feedback loop
• Direct mechanisms (Lothman 1998)
– Facilitation – inc excitotoxins (glu), Ca2+ influx via
NMDA or AMPA receptors
– Fading of inhibition – dec GABA release due to
repetitive activation of presynaptic storage site
• Longer term effects – gene expression, hippocamp
apoptosis
• Secondary epileptogenesis – local process disseminates
– Seizures beget seizures (Fountain 1995)
Page 15
Differential Diagnosis • Myoclonus
– Toxic/metabolic
– Infec/inflamm/autoimm
– Spinal cord disease
– Brainstem/subcortical
– Cortical
– Epileptic
• Tics
• Tremor
• Asterixis
• Clonus
• Posturing
• Opisthotonus from HCP
• Shivering/rigors
• Hiccoughs
• Post-anesthesia
psychogenic SE
• Narcolepsy/cataplexy
• Syncope
• TIA
• TGA
• Pseudoseizures
(Varelas 2005, Table 5)
Page 16
Evaluation of Etiology
Laboratory Evaluations
• Blood count
• Glucose
• Electrolytes
• Liver enzymes
• Toxicology screen
• ABG
• AED level
Diagnostic Evaluations
• Head CT
• Lumbar puncture
– Benign postictal elevation
in 20% (WBC > 70)
– Protein elevation in 15%
(>50 ) (Aminoff 1980)
• Stat EEG – if pt not
waking up
• Continuous EEG
• MRI – can mimic infarct
DO NOT DELAY SEIZURE TX FOR
WORKUP
Page 17
Brief single ICU Seizure Mgt
• Observe. Eliminate etiology
• Consider AED load and maintenance
– Phenytoin (15-20 mg/kg, then 300-400mg/day)
– Fosphenytoin (15-20 mg/kg PE, then 300-400mg/d)
– Valproate (15-20 mg/kg, then 600-3000mg/d)
– Levetiracetam (1000 mg, then 1000-3000mg/d)
• Seizure precaution: padded bed rails, increase
observation
From Varelas 2005, table 6
Adaptation from Varelas, Mirski 2001
Page 18
SE Algorithm
Emergency med mgt –
ABCs
Terminate seizures
Prevent recurrence of
seizures
Treat complications
Page 19
ABCs: Med mgt
• ABC’s
• Intubation
– Short acting – rocuronium or vecuronium
– Thiopental (3mg/kg) can also treat seizures
– Avoid overcorrecting to resp alkalosis
• No need to treat BP unless extreme (>230 mmHg
systolic)
• Thiamine 100mg IV if etoh or history unknown
• Glucose (D/W 50%) – only if BS < 40-60 or few minutes
to get result
Page 20
SE Algorithm
Emergency med mgt –
ABCs
Terminate seizures
Prevent recurrence of
seizures
Treat complications
Page 21
First known description of
status epilepticus
(Sakikku cuneiform,
ca. 700 B.C)
give lorazepam
Courtesy of Dr. Bleck
Page 22
SE Algorithm
• First line agent – lorazepam
– Midazolam ( buccal, IM, IN) or rectal diazepam
• Second line agents
– Fosphenytoin or phenytoin
– Phenobarbital
– Valproate (Shorvon 2011)
IV levetiracetam – open
label trials (CPSE)
Good efficacy
Low toxicity and
interactions
Page 23
VA Cooperative Trial
• 570 pts in RCT; 4 iv tx arms
• overt SE or subtle SE
• First line treatment options
• Second, third line tx algorithm
• End pt: seizure cessation < 20min
• No return of seizure activity for 40 min
Treiman, Meyers, Walton 1998
Page 24
VA Study Results
Success rate Lorazepam Phenobarb Diaz/Pheny Phenytoin
First drug 64.9% 58.2% 55.8% 43.5%
Second drug PHT 7.2 % PHT 3.3% LRZ 3.2% LRZ 13.9%
Third drug PB 2.1 % LRZ 2.2% PB 2.1 % PB 3.0%
Other drugs 17.5% 25.3% 23.2 % 26.7%
No response 8.3% 11.0% 15.8% 12.9%
•Lorazepam was the most effective first line agent
•Overall, if first line agent fail, second line choice had low success rates
•If LZP and PHT fail to control < 30min, consider going to refractory
agent
Page 25
Treatment Principles
• Treat quickly
– 80% response to 1st line meds if tx < 30min
– < 40% response if tx < 2 hrs
– 2x mortality if tx delayed > 24 hr (NCSE)
• Risk of respiratory depression less than
risk of prolonged seizures
(Claassen 2009)
Page 26
BZDs – First Line
Agent • Pharmacokinetics
– Less rapid redistribution
– Longer half-life (8-25 hr)
– Less CV depression
• 81 episodes of SE (Leppik 1983) DZ vs
LZP
– 89% controlled with lorazepam
– 76% controlled with diazepam
• Pediatric study (Appleton 1995)
– 76% controlled w/LZP
– 51% controlled w/DZP
– less respiratory depression (3% vs
15% w/DZP
• High tendency for tolerance
•Enhance GABA
inhibition
•Lorazepam
•0.1mg/kg (4 mg
bolus q 10 min)
•Diazepam
•Midazolam
Page 27
BZDs – First Line
Agent
• Pharmacokinetics
– Highly lipid soluble
– Redistributes out of brain rapidly
(distribution half-live 30-60 min)
– Long elimination half-life (24 – 57 h)
– Persistent and cumulative sedation
– Respiratory depression
• Rectal diazepam
– 2 RCT’s ( Cereghino 1998, Dreifuss
1998)
– 55-62% were seizure free
– Somnolence most frequent side eff
– No episode of respiratory depression
in 500 patients
•Enhance GABA
inhibition
•Lorazepam
•Diazepam
•10-20mg IV(5-10mg
boluses)
•Rectal gel
•Midazolam
Page 28
BZDs – First Line
Agent • Pharmacokinetics
– Water-soluble that converts to
lipophilic in serum
– Rapidly absorbed by IM, IN, buccal
– Short distrib half-life < 5min
– Short elimination half-life 1.5-4 hr
• best as continuous infusion
• IM when no IV access
• Buccal (McIntyre 2005)
– 219 seizure episodes in children
– 56% sz cessation < 10min for 1 hr
– 29% for rectal dzp < 15min
•Lorazepam
•Diazepam
•Midazolam
• 0.1-0.3mg/kg
bolus (< 4mg/min),
then 0.08-
0.4mg/kg/hr
•Buccal - first line
in children without
IV access, pre-
hospital
•IM – 5-10mg
Page 29
Second Line
Agents • Phenytoin – Water insoluble
– pH 12; caustic to veins
– Hypotension, QT prolongation
– Peak brain levels in 15min
– Slow redistribution out of CNS
– 96% protein bound
• Low cost, so consider for
maintenance
•Phenytoin
•20mg/kg load
•5 mg/kg addtl
•300-400mg/d
•Fosphenytoin
•Phenobarbital
•(Valproate)
Page 30
Second Line
Agents • Fosphenytoin – PHT pro-drug; water soluble
– Therapeutic levels within 10min
– Need to wait for conversion to PHT
before measuring level (1-1.5 hrs)
– Expressed in phenytoin equivalents
• Fewer local side effects
• Less hypotension (7.7%)
• Preferred for IV loading dose
•Phenytoin
•Fosphenytoin
•20mg/kg PE
•5 mg/kg PE
addtl load
•Phenobarbital
•(Valproate)
Page 31
Second Line
Agents
• Does not cause sedation or
respiratory depression
• Broad efficacy – GTC, focal,
absence, myoclonic
• European study (Giroud 1993)
– 23 pts with CSE or NCSE
– 83% had sz cessation < 20min
• Multiple studies show efficacy
comparable to PHT (Trinka 2009)
• Absence SE or myoclonic SE
• Pts who do not want mech
ventilation
• Pts intolerant to phenytoin
• Considered third line agent
•Phenytoin
•Fosphenytoin
•Phenobarbital
•(Valproate)
•15-20mg/kg
•400-600mg q
6hr maint.
Page 32
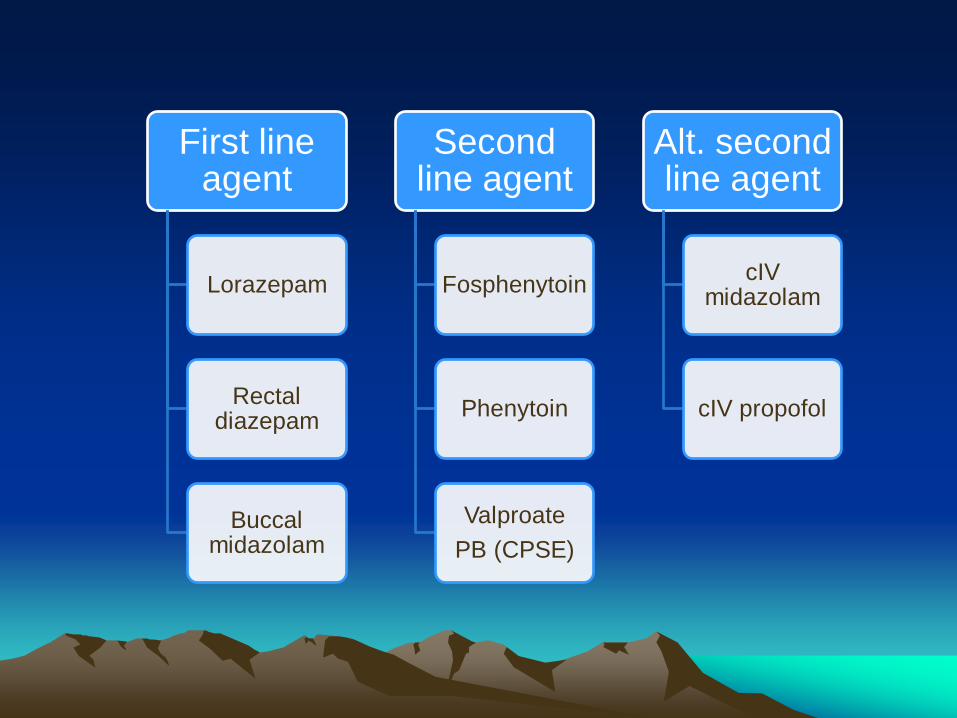
First line agent
Lorazepam
Rectal diazepam
Buccal midazolam
Second line agent
Fosphenytoin
Phenytoin
Valproate
PB (CPSE)
Alt. second line agent
cIV midazolam
cIV propofol
Page 33
Alternate 2nd / 3rd
line agent - cIV • cIV drips can be second line
agent after lorazepam
• Systematic review of RSE
(Claasen 2002)
– No difference in mortality (48%)
between cIV mdz, prop, pentobarb
– Acute tx failure, breakthrough sz
• cIV mdz = cIV prop
• Less with cIV pentobarb - ?due to highest
rate of burst suppression goal
– Hypotension highest with cIV pentob
•cIV midazolam
•cIV propofol
Page 34
Alternate 2nd / 3rd
line agent - cIV • Effective in minutes
• Easy to titrate
• Minimal cardiovascular effects
• Tachyphylaxis in 24-48 hrs
• cEEG may be diffuse slow, burst-
suppression or flat
• Wean after 12-24 hrs of sz
suppresion
•cIV midazolam
•0.2-0.4mg/kg
boluses q 5min
•Max of 2.0
mg/kg/hr
•cIV propofol
Page 35
Alternate 2nd / 3rd
line agent - cIV
• Non-barbiturate anesthetic
• GAB A-R effects similar to BZD
and barbiturates
• Rapid onset < 3min
• Rapid recovery 5-10min
• Liver metabolism
• Seizure like phenomenon (SLP)
– Rigidity, myoclonus, opisthoclonus
– Subcortical disinhibition
• Hypotension, bradycardia
• Propofol infusion syndrome
– Cardiac failure, metab acidosis,
rhabdomyolysis, renal failure
•cIV midazolam
•cIV propofol
•3-5mg/kg bolus
•1-15 mg/kg/hr
Page 36
Propofol Infusion Syndrome (PIS)
• Tx > 48 hr, dose > 5mg/kg/hr (350mg)
• 41 pts with RSE (retrospective) (Lyer 2009)
– 31 pt - propofol
– 10 pt – other anesthetics
• 3 pts in prop grp had sudden unexplained cardioresp.
arrest with no prior disease
• 11 pts with non-life threatening PIS
– Median admin = 63 hr, dose of 12,750mg cumulative
Page 37
Stat EEG
• not recommended in first 15min (Epilep Found 1993)
• if pt not waking up after tx (15-30min) (Bleck 1993)
• EEG (30min) – diagnose 1/3 of NCS (24hr cEEG)
• Limited montages (6 channels, hairline) not sensitive
• cEEG –
– 24hr detect 95% in altered MS and 80% of comatose pts
• VideoEEG – need to distinguish artifacts, pseudosz
Page 38
Newer
Second/Third line
agents
• Pharmacokinetics
– Unique mechanism of action
– Metabolism by hydrolysis in serum
– Renal excretion
– No significant drug interactions
• Multiple open label studies in
various types of epilepsy
(Shorvon 2011)
– Excellent efficacy
– Low toxicity
• Increasing use off label as
second line drug of choice
• Important in CPSE
•Levetiracetam
•1000-4000mg IV
•Lacosamide
•400mg bolus
Page 39
Third Line
Agents • Rarely used anymore as second
line agent for GSE
– Slower entry into brain
– Long half-live of 4 days
• Respiratory depression
• Hypotension common
• May be useful in partial SE
• Can use when weaning from high
dose midazolam or barbiturates
•cIV midazolam
•cIV propofol
•cIV phenobarbital
•20mg/kg at 50-
100mg/min
•IV valproate
Page 40
Refractory Status Epilepticus
• Definitions
– Sz > 60 min (Shorvon 2011)
– Sz not responding to 2 IV drugs (Delorenzo 1995, Holtkamp
2005)
• 1/3 of SE pts – refractory to 1st/2nd line agents (Mayer 2002)
– 83 episodes of status, retrospective
– Seizure after BZD – 69%
– Seizure after second agent – 31%
– Risk factors:
• NCSE
• Focal motor seizure at onset
Page 41
RCT in RSE
• First RCT (Rosetti 2010) – single-blind, multicenter
• After failure of BZD and second line agent
• enrolled 24/150 target in 3 yrs
– Propofol – 43% termination of RSE (not statis sig)
– Barbiturates – 22% term of RSE
• Mortality and recovery to baseline similar
• Mechanical ventilation time – much longer for barbs
Page 42
RSE (fourth line)
Agents • Barbiturates
– Long half-life
– Cardiovascular depression
• Hypotension, myocardial
depression, dec renal perfusion
– Suppress cough, ciliary immob
– Immunosuppression
– Poikilothermia
– GI hypomotility
– Immobilization (DVT, decub)
• Goal of EEG to burst suppression
to flat
•Pentobarbital
•Thiopental
Page 43
RSE (fourth line)
Agents • Pentobarbital
– Shorter elimination half-life than
phenobarb (24 hr)
– Sz can occur in w/d period
• Duration- 24 - > 96 hrs
– 44 RSE episodes (Krishnamurthy
1996) - >96hr tx and phenobarb use
during taper less relapse
– Reports of very long duration with
good functional recovery (Mirski 1995)
•Pentobarbital
•6-15mg/kg (1hr)
•1mg/kg/hr (0.25-
10mg/kg/hr
•Thiopental
•Isoflurane
•Ketamine
•Lidocaine
Page 44
RSE (fourth line)
Agents • Thiopental
– Rapid onset, AED efficacy
– Potential neuroprotective
– Dec ICP, CBF, cerebral metab
• Preferred in europe for barb anesth
in RSE
• Bispectral Index Monitor (BIS)
– 10 RSE pt tx with propofol
(Musialowicz 2010)
– Score of 30 correlates with burst supp
on EEG; sens 99%, spec 98%
•Pentobarbital
•Thiopental
•2-4mg/kg bolus
(100-250mg bolus
over 20s, then
50mg q 3min)
•3-5mg/kg/hr cIV
Page 45
RSE Treatments
Pharmacologic
• Isoflurane • End-tidal concen of 1.2-5%
• Ketamine – NMDA antagonist
• Lidocaine
– Stabilizes cell membranes
– Risk for toxicity and inc sz
with repeated dose
• Topiramate
• IVIG, methylprednisolone,
rituximab, cytoxan
Non-pharmacologic
• Hypothermia (31-24° C)
– 4 adults RSE (Corry 2008)
– 2 sz control, 1 dec sz
• Vagal nerve stimulation
• Surgical resection
• Ketogenic diet
• Electroconvulsive tx
• Plasma exchange
Page 46
Autoimmune epilepsy
• Cryptogenic epilepsies - assoc with cognitive
decline or personality changes (Tan 2010, Dalmau
2009)
• 25-50% of adult onset temporal lobe epilepsy +
hippocampal sclerosis = limbic encephalitis (Bien
2007)
• NMDA-R Ab (Tan 2010, Dalmau 2008,2009, Lancaster 2010)
• Voltage-gated potassium channel Abs – VGKC-complex
(CASPR2, LGI1, Contactin-2) (Irani 2010)
• GABAB1, AMPA-R Abs (Lancaster 2010, Lai 2009)
Page 47
SE Algorithm
Emergency med mgt –
ABCs
Terminate seizures
Prevent recurrence of
seizures
Treat complications
Page 48
Weaning Protocols
Continue cIV for 12-24 hrs
after stopping seizure activity (clinical/cEEG)
taper over 24
hrs
Seizures recur
Longer taper +
inc AEDs
Long term AEDs + cEEG
Page 49
SE Algorithm
Emergency med mgt –
ABCs
Terminate seizures
Prevent recurrence of
seizures
Treat complications
Page 50
Complications in SE Caused by SE
• Rhabdomyolysis
– Saline diuresis
– Neuromuscular blockade
• Hyperthermia
– Resolve with term of SE
– External cooling devices
• Vasogenic edema
• Drug interactions
• ICU complications
– Sedation, mech ventilation,
immobility
Considerations in SE
• Hepatic failure
– PHT- free levels
– PB - 25% metab in urine
• Half-life – to 130 hrs
– BDZ - reduce dose
– Pentob,thiop – do not use
– VPA – inc ammonia levels
• Renal failure
– No effect on BDZ, VPA
• Hematopoetic dysfx – PHT, PB – megaloblastic anemia
– VPA – thrombocytopenia
– CBZ – neurotropenia, aplastic
anemia
Page 51
Outcome in SE
• Dependent on cause, clinical type, age (Tsai 2009)
• Adherence to 1st line tx protocol – 7x increase in
seizure termination (Aranda 2010)
• RSE prospective study (Novy 2010)
– 23% were refractory to 1st / 2nd line agents
– 39% mortality
– 1 in 5 returned to clinical baseline
• Conclusion: pt with prolonged SE can survive with good
outcome ;depends on underlying cause and
complications rather than duration (Holtkamp 2011)
Page 52
Focal SE
Clinical types (> 30min)
• Epilepsy partialis
continua – distal limb
• Opercular myoclonic –
glossopharyngeal
• Sensory
• Aphasic
• Occipital lobe- visual loss
(Varelas 2005)
Etiologies
• Focal cerebral pathology
• Diffuse process (Schomer
1993)
– Nonketotic hyperglycemia
– Hyponatremia
– Mitochondrial
encephalopathy
– Rasmussen’s encephalitis
– Antibiotics – PCN,
azlocillin/cefotaxime
Page 53
Focal SE Treatment
• No convincing data re: significant long term
effects independent of etiology (Holtkamp 2011)
• Less aggressive treatment – 1st / 2nd line agents
trying to avoid general anesthesia
• Systemic complications – HR, temp, rhabdo
• May require polypharmacy
• Choose potent AED with low sedation/resp dep
• Response to AED may be delayed up to 48hrs (Drislane 1999)
Page 54
Focal SE Agents
• Levetiracetam
– Second line after BZD
– Third line after valproate or
phenytoin
• Lacosamide
– Retrospective case series
(Kellinghaus 2011)
• 39 pts (6 GSE,17 CPSE, 16
SPSE)
• Median dose 400mg (40-
80mg/min)
• 44% success rate (17 pts)
•Levetiracetam
•valproate
•Phenobarbital
•lacosamide
•Oral AEDs
•Carbamazepine
•Oxcarbazepine
•Topiramate
•zonisamide
•Gabapentin
•Lamotrigine
•Pregabalin
Page 55
Focal SE Agents
• Topiramate
– Multiple mech of action, via NG tube
– Effective in 6 pts in GSE, NCSE
(Towne 2003)
• Zonisamide – Sodium and calcium channel blocker
– Approved in Japan for adjunctive tx for
refractory partial epilepsy
• Lamotrigine
– NCSE (Trinka 2002)
– myoclonic SE (Guerrini 1999)
• Pregabalin
– Retrosp study in RSE (Novy 2010)
– 8/11 pts response (5/11 definite)
– No side effects
•Levetiracetam
•valproate
•Phenobarbital
•lacosamide
•Oral AEDs
•Carbamazepine
•Oxcarbazepine
•Topiramate
•zonisamide
•Lamotrigine
•Pregabalin
Page 56
Pediatric SE
• Cardioresp support while treating motor/EEG sz
• focus on prehospital treatments (Alldredge 1995, 2001)
– Shorter duration SE: 32 min vs 60min
– Less recurrent sz in ED: 58% vs 85%
• Lorazepam – fewer repeat doses and less respiratory
depression than diazepam (Appleton 1995)
• cIV midazolam in refractory SE – assoc with lower
mortality in children (Gilbert 1999)
• Pentobarbital therapy – burst supp for 12 hrs (Kinoshita
1995)
Page 57
ICU EEG monitoring
• Seizure detection – Acute, unexplained change in mental status
– MS exam out of proportion to underlying injury
– Persistent unresponsiveness after tx CSE
– Comatose with subtle motor/eye movements
• Titration of medications
• Ischemia detection
• Prognostication
• Characterization of clinical spells
Page 58
Duration of cEEG
Claassen Neurol 2004
N=105 Clin events EEG szs
Routine EEG (>= 30 mins) 21% 11%
cDVEEG (mean 2.9 d) 40% 27%
P 0.01 0.01
Pandian Arch Neurol 2004
Monitor
Altered MS-
24 hr
Comatose-
48 hr
Page 59
NCSE Treatment • Controversial patterns: ictal-interictal
continuum
– PLEDs, GPEDs, BiPLEDs
– Triphasics, SIRPIDs
• BZD trial with clinical improvement or
resolution of EEG pattern or appearance
of background pattern. If EEG improves
but pt does not, result is equivocal.
Page 61
PLEDs
• Sharp/spike waves/slow waves that occur in regular
periodic intervals (Young 1988)
• Usually occurs with cortical injury
• Also in metabolic or post SE (Raroque 1993)
• Considered cerebral response to acute focal process
– Ischemic stroke
– Linked to parox depolarizing shift at cellular level/
membrane/chemical disruption
– Linked to basal ganglia circuit
• Inconclusive relationship to outcomes (Garcia-Morales
2002)
Page 62
Outcomes in NCSE
• 134 pt with subtle SE (Treiman study) – worse outcomes
than with CSE
• 100 pts with NCSE (Shneker 2003)
– Overall mortality 18%
• 27% in medical group
• 17% in cryptogenic group
• 3% in epilepsy group
– No correlation between sp/w discharge on EEG and mortality
– Independent assoc. of mental status change and mortality
• Duration > 36-72 hrs leads to inc. morbidity and mortality
(Krumholz 1995)
Page 63
Outcomes in NCSE
• Clinical data:
• Nontraumatic ICH: nonconvulsive szs may be associated with mass
effect and shift Vespa ‘03, Claassen, ’07
• NCSZ post TBI may be a/w long-term hippocampal atrophy Vespa
‘10
• Neurochemistry:
• NSE: levels highest with acute brain injury + szs; szs alone can
cause elevation DiGiorgio ’95 + ‘99
• Glutamate: szs may be associated with glutamate spikes, including
to toxic levels Vespa ‘98
• Lactate pyruvate ratio increased in post traumatic seizures Vespa
‘07
Page 64
Outcomes in NCSE
• 134 pt with subtle SE (Treiman study) – worse outcomes
than with CSE
• 100 pts with NCSE (Shneker 2003)
– Overall mortality 18%
• 27% in medical group
• 17% in cryptogenic group
• 3% in epilepsy group
– No correlation between sp/w discharge on EEG and mortality
– Independent assoc. of mental status change and mortality
• Duration > 36-72 hrs leads to inc. morbidity and mortality
(Krumholz 1995)
Page 65
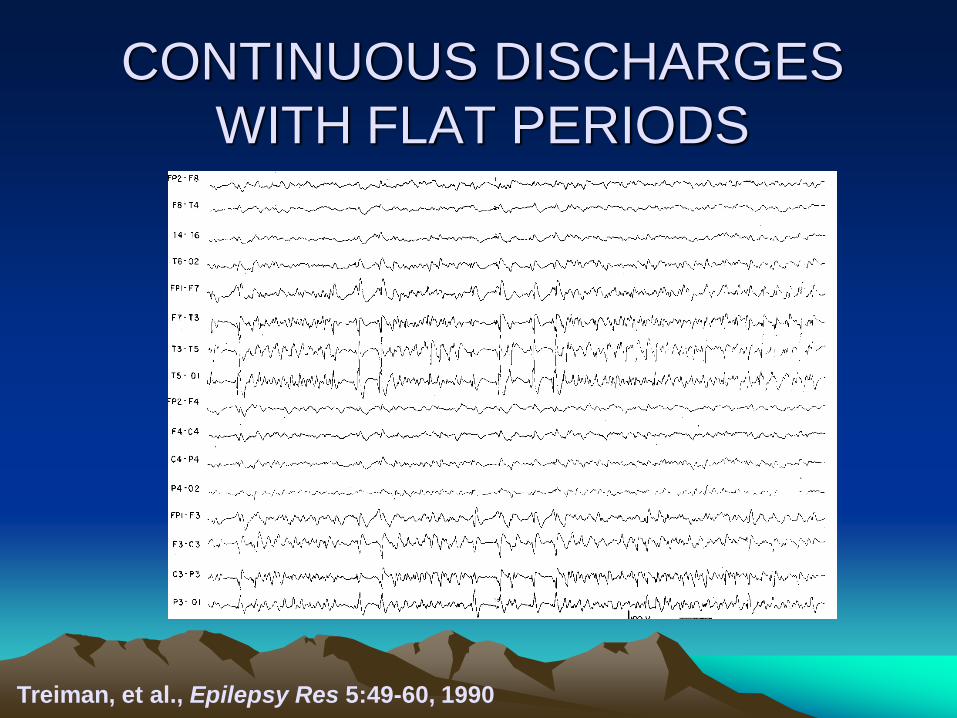
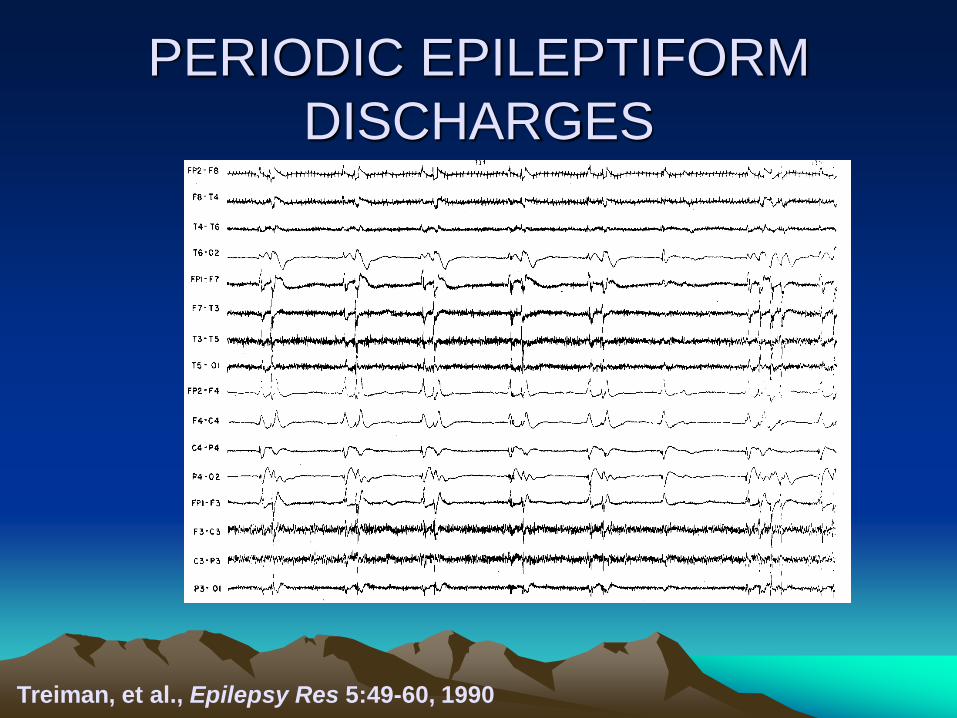
Evolution of SE
• Phases of progression of electrographic
findings in status epilepticus
(Treiman 1990)
Page 66
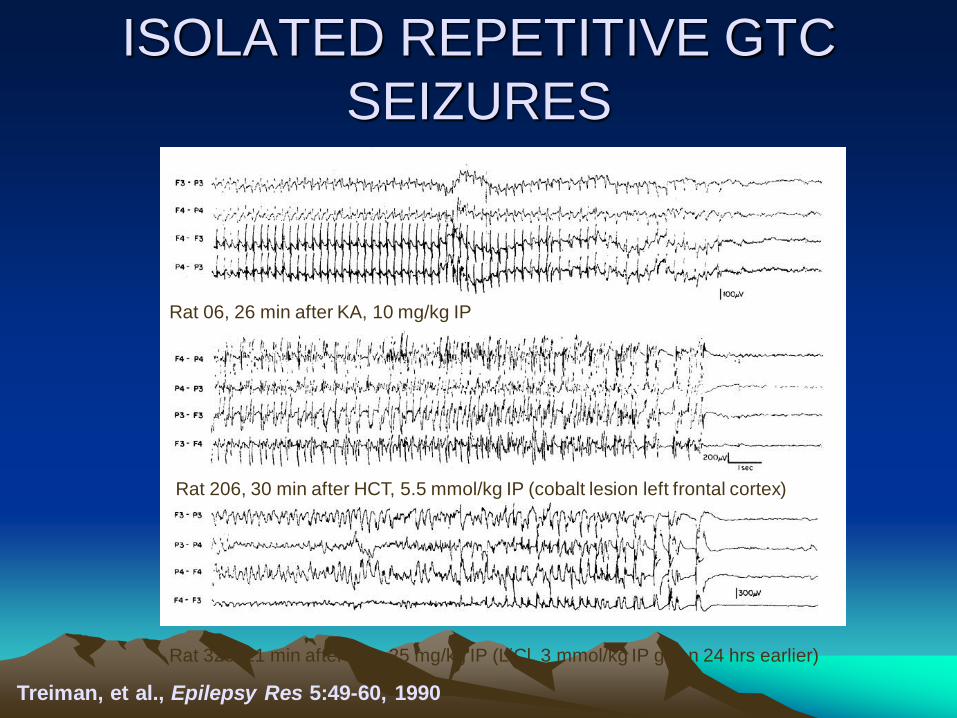
ISOLATED REPETITIVE GTC
SEIZURES
Treiman, et al., Epilepsy Res 5:49-60, 1990
Page 67
ISOLATED REPETITIVE GTC
SEIZURES
Treiman, et al., Epilepsy Res 5:49-60, 1990
26 min after 10 mg/kg KA Rat 06, 26 min after KA, 10 mg/kg IP
Rat 206, 30 min after HCT, 5.5 mmol/kg IP (cobalt lesion left frontal cortex)
Rat 325, 21 min after Pilo, 25 mg/kg IP (LiCl, 3 mmol/kg IP given 24 hrs earlier)
Page 68
MERGING OF I.R. SEIZURES Waxing and Waning Ictal Discharges
Treiman, et al., Epilepsy Res 5:49-60, 1990
Page 69
MERGING OF I.R. SEIZURES Waxing and Waning Ictal Discharges
Treiman, et al., Epilepsy Res 5:49-60, 1990
Rat 06, 75 min after KA
Rat 206, 37 min after HCT
Rat 325, 24 min after Pilo
Page 70
CONTINUOUS ICTAL DISCHARGES
Treiman, et al., Epilepsy Res 5:49-60, 1990
Page 71
CONTINUOUS ICTAL DISCHARGES
Treiman, et al., Epilepsy Res 5:49-60, 1990
Rat 06, 103 min after KA
Rat 206, 48 min after HCT
Rat 325, 28 min after Pilo
Page 72
CONTINUOUS DISCHARGES
WITH FLAT PERIODS
Treiman, et al., Epilepsy Res 5:49-60, 1990
Page 73
CONTINUOUS DISCHARGES
WITH FLAT PERIODS
Treiman, et al., Epilepsy Res 5:49-60, 1990
Rat 06, 148 min after KA
Rat 206, 75 min after HCT
Rat 325, 109 min after Pilo
Page 74
PERIODIC EPILEPTIFORM
DISCHARGES
Treiman, et al., Epilepsy Res 5:49-60, 1990
Page 75
PERIODIC EPILEPTIFORM
DISCHARGES
Treiman, et al., Epilepsy Res 5:49-60, 1990
Rat 06, 5 hr 46 min after KA
Rat 206, 2 hr 12 min after HCT
Rat 325, 2 hr 19 min after Pilo
Page 76
Prognostication EEG findings associated with poor prognosis:
• Seizures
• Status epilepticus
• Generalized or lateralized periodic epileptiform discharges
• Nonreactivity
• Absent sleep architecture
• Percent alpha variability within 3 d post TBI correlates with fct outcome
at 6 m
Bricolo EGCN 1978; Jaitly J Clin Neurophysiol. 1997; DeLorenzo Epilepsia. 1998; Lawn Clin
Neurophysiol. 2000; Vespa Neurology 2003; Claassen NCC 2006 and Neurology 2007;
Vespa JNsurg 2002, Hebb J Neurotr 2007
Caveat: unclear if these EEG findings are markers of the extent of brain
injury or if they cause additional brain injury
From Claassen
Page 77
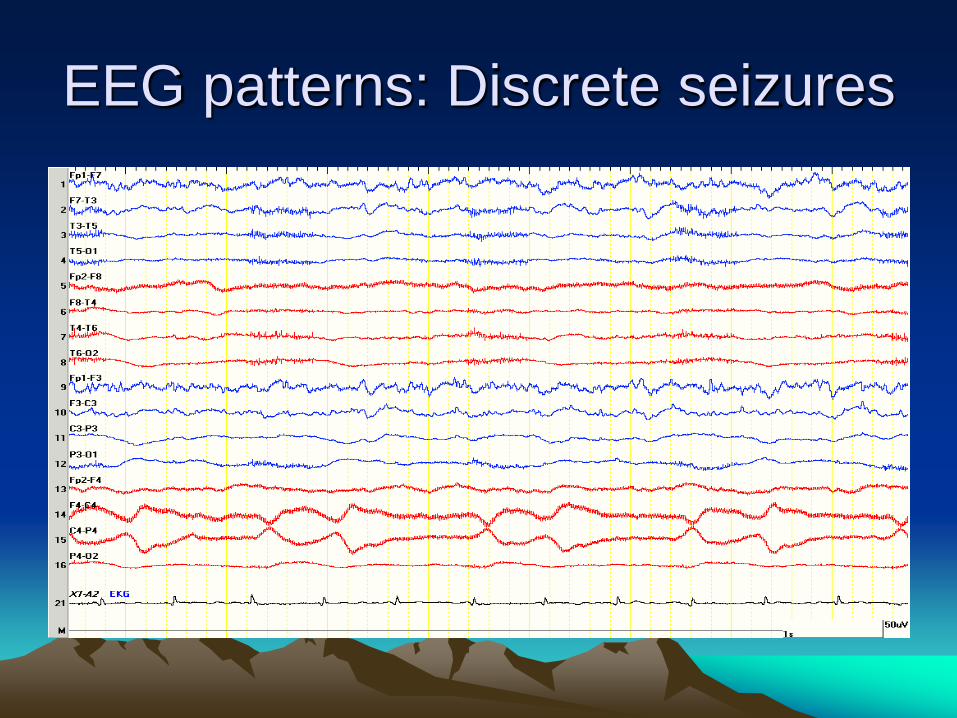
EEG pattern: discrete seizure
Page 78
EEG patterns: Discrete seizures
Page 79
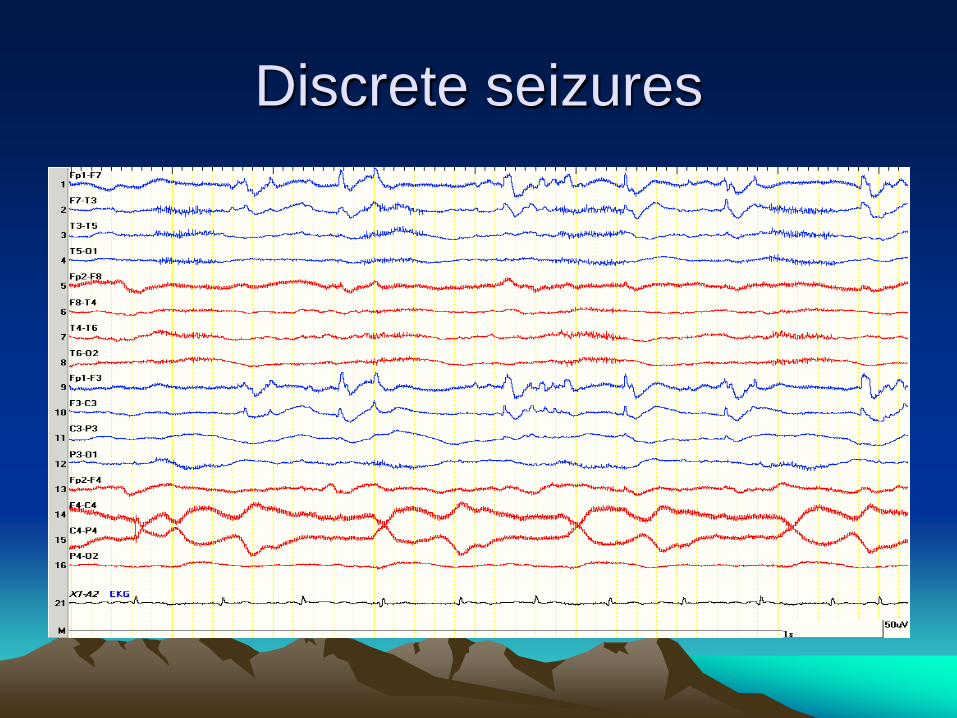
Discrete seizures
Page 80
EEG patterns: Triphasics
57 yr old with acute renal failure; COPD and acute mental status changes
Page 81
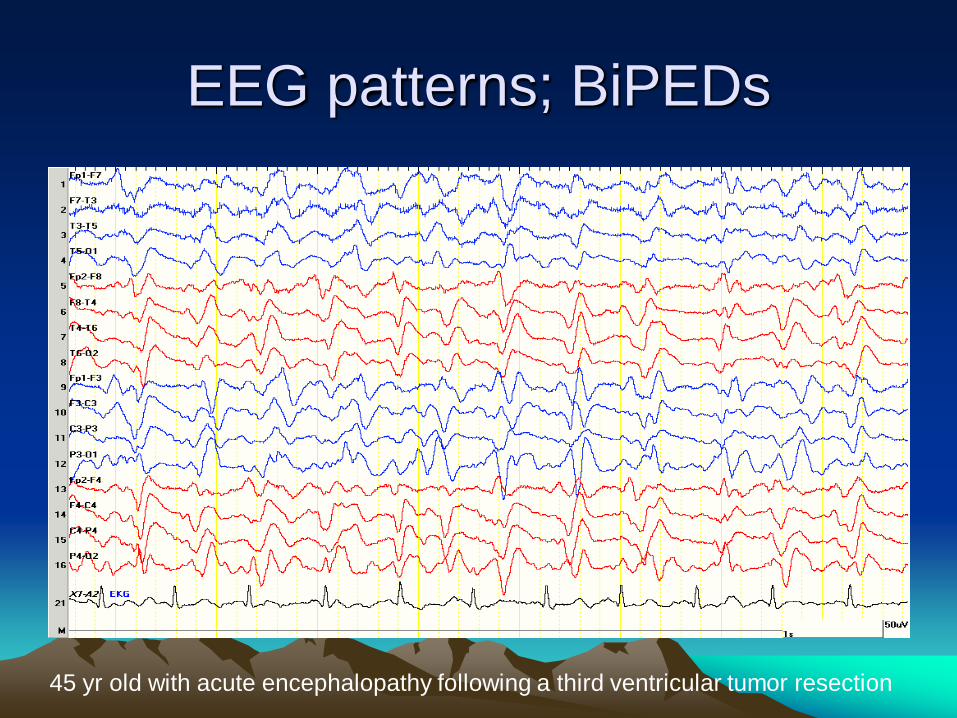
EEG patterns; BiPEDs
45 yr old with acute encephalopathy following a third ventricular tumor resection
Page 82
EEG pattern: GPEDs
55 yr old with anoxic brain injury (post cardiac arrest)
Page 83
EEG pattern: PLEDs
50 yr old S/p Right sided AVM resection. Witnessed seizure followed by
obtundation
Page 84
EEG pattern: Suppression-Burst
Page 85
EEG pattern: SIRPIDS
SIRPIDS can be focal or generalized