47
SPoC as Centerpiece of Real Family-Centered Care Coordination” Jeanne McAllister, BSN, MS, MHA Research Associate Professor IUSM Pediatrics

SPoC as Centerpiece of Real Family-Centered Care Coordination”
Jeanne McAllister, BSN, MS, MHAResearch Associate Professor IUSM Pediatrics

It Takes a Team: Why, What, and How We Do This & Lessons
Care Coordination Team (L-R): Thomas Lock, Jeannie McAllister, Jordan Huskins, Rylin Rodgers, Rebecca McNally-Keehn,
Holly Paauwe, Ann Clark & Margo Ramaker

Objectives
1. Describe how and why a SPoC can improve outcomes
2. Explore strategies for engagement of children and families and professionals
3. Describe why/how a SPoC can be valuable to medical practices/ members of the health care team
4. Discuss national examples of SPoC implementation (progress/challenges)

Care Coordination
Why ?


Value of Care CoordinationVideo Part A
(video run 00:00 to 02:08)

We Know Families Experience:• Spent time coordinating
• (14% > 11 hours/week) • Financial impact (high costs, lost
income• Need additional resources
• Families Ask For:• Communication
• Listening/Respect/ Compassion• Access
• Knowledge

Family“If you can bring us real care coordination,
you will have saved our family”.

Homographs/Homonyms –same spelling, ~sounds, multiple meanings
B – O - W

Homonym –one word, multiple meanings
bow –wooden stick with horse hair, play string the violin
bow –bend forward at the waist, "bow down")
bow –front of the ship (e.g. "bow and stern")
bow –bow on a present, a bowtie)
bow –"bow-legged" cowboy)\
Bow – a district in London
bow—bow and arrow
bow - wow
Homographs/Homonyms –same spelling, ~sounds, multiple meanings
Chat Box –
Name other homonyms or homographs?

Care Coordination?
“REAL”
Fidelity to
Best Practice Model:
Activities …?
Family-Centered
Assessment driven
Continuous
Team-based
Bio psychosocial focused
Build Skills

Recommendations – Family-Centered Care Coordination/Shared Plan of Care (SPOC)
Achieving a SPOC w/CYSHCN & Families
Principles1) Patients & families are central
and engaged
2) Teams are enabled/supported to help co-create/use SPOC
3) Health care and community professionals efforts - are integrated
4) Cross system family-centered care coordination is sustained
McAllister J. Achieving a Shared Plan of Care with Children and Youth with Special Health Care Needs:A White Paper and Implementation Guide. Lucille Packard Foundation for Children's Healthcare;2014
• An opportunity to test a care coordination model,
• But…- how best to engage families in design and implementation
Family Leaders: Essential in Program Design, Implementation and Evaluation
Family-Centered Care
Family-centered care is an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families.
Kuhlthau,K., et.al

Family Leaders/Essential Partners in Program Design, Implementation and Evaluation
Quality
Family Centered Care/Families as Partners Families as active, critical
partners in decision-making across all levels of care
FCC is a Foundational Standard for Systems of Care for CYSHCN
Care Standards
Slide Credit : Rylin Rodgers

Why Care Coordination
FamilyNeeds
Physician Needs
PayerNeeds
CareNeighbor-hoodNeeds
Slide Credit : Rylin Rodgers 17
This is the Moment

• An opportunity to test a care coordination model, but
-what do things look like from the clinical & health systems angle?
Have you ever built it and they didn’t come?
Have you ever worked really hard on a diagnosis and/or recommendations, and: Nothing happened? People did some things, but missed the main point? Things just got worse?
Slide Credit: Tom Lock, MD

When that happened was it because:
You recommended the wrong thing?
You recommended the right thing …but it wasn’t available in the community?
The insurance was wrong?
There was a barrier that you didn’t anticipate?
Slide Credit: Tom Lock, MD

Indiana Baseline for Children with Autism/NDD
Screening Initiative
Regional Autism HubsEarly evaluation Diagnosis
Then what? …
Slide Credit: Tom Lock, MD

Then What . . .
ABA Insurance Private providers
Preschool Overextended system Suspicion of public
school systems
Hospital/Clinic based therapies Limited medically
designed experiences
Mental health Inexperience with non-
verbal patients Opioid crisis Non-evidence bases
therapies

Care Coordination/Care Coordinators!
Slide Credit: Tom Lock

Model Approach - Boiling down a non-specific problem into goals.
Requires input from Family-
specific family circumstances family priorities
Clinicians- knowledge of evidence based interventions prognosis
Coordinator- Experience with identifying & activating care community Ability to define goals with family Time to bring things together
Slide Credit: Tom Lock, MD

Boiling down - “I don’t know how to find the best program for my child”
Triggers questions- What should you be looking for? How do you access information? On line? Need translator? Print?
What are your resources? Insurance? Transportation? Time?
What’s in your community? Intervention Centers? ABA by another name?
School uses ABA elements?
What if there is no ABA? Speech? OT? School
Slide Credit: Tom Lock, MD
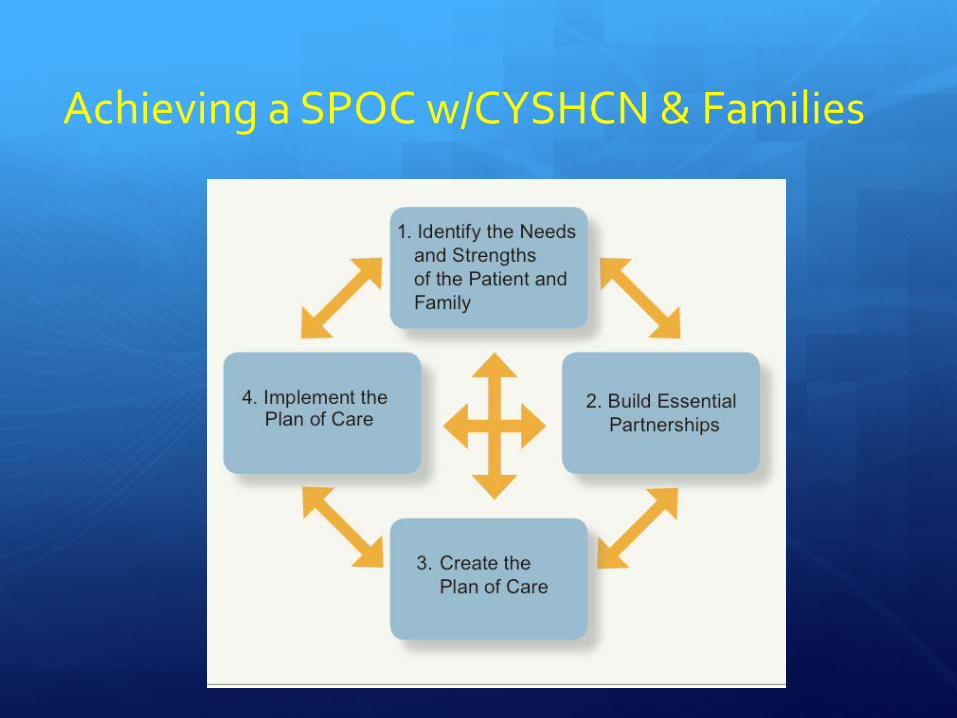
Achieving a SPOC w/CYSHCN & Families

Ten Steps to Achieving a Shared Plan of Care (SPOC)
1. Identify who will benefit from a SPOC2. Discuss with families/colleagues the value of using a SPoC3. Assess -Select, use , review a multi-faceted assessment with each
child, youth and family4. Goals - Set shared personal family, as well as clinical goals5. Partner - Identify other needed partners /link w/the planning process6. SPoC - Develop plan of care’s “Medical Summary (data, partners)7. SPoC Establish plan of care’s “Negotiated Actions” (goals/strategies) 8. Share - Ensure that the SPOC is available, accessible/retrievable9. Use - Provide tracking, monitoring and care plan oversight10. Population Approach - Systematically use the SPOC/ model process
with an aligned group of patients / families
Achieving a Shared Plan of Care with Children with Special Health Care Needs and their Families Lucile Packard Foundation for Children’s Health; www.http://www.lpfch.org/sites/default/files/field/publications/achievinga_shared_plan_of_care_full.pdf
What We Set Out to Do/Approach

Family Outreach & Engagemen
t ➤
Partnership & Pre-Visit
Preparation ➤
Teamwork & Population
Care ➤
“Planned Care Visit” &
SPOC Co-Production
➤
Ongoing CC &
Community Transfer ➤
Rapport TeamPrepare
Assess Listen/HearCo-Produce
UseImprove
Using a SPoC as Approach to Family-Centered Care Coordination

Shared Plan of Care
About Me
Medical Summary
Negotiated
Actions40%
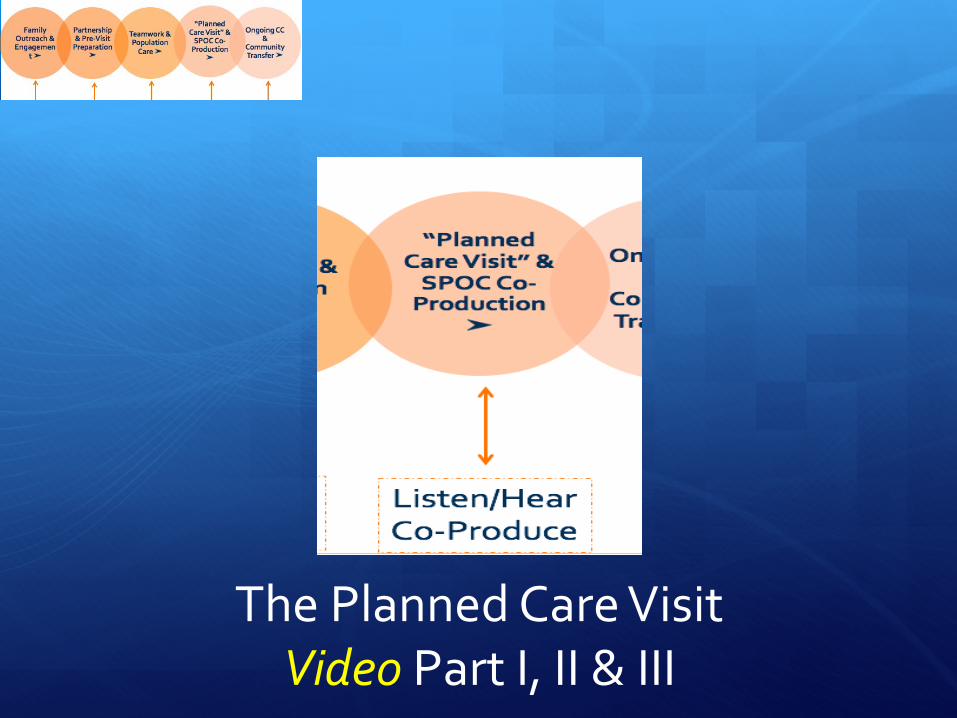
The Planned Care Visit Video Part I, II & III

Questions & Comments

What Did We Learn?
1. Family Goals 2. Family pre post surveys with Care Coordination Questions:
1. Mangione-Smith, AHRQ CC Measurement Set2. National Survey CYSHCN3. Family Empowerment Scales (2/3)4. CMHI/McAllister questions

1) Access to care coordination/coordinator ✔
2) Co-production /use of a Shared Plan of Care (SPoC) ✔
3) Identification/achievement of family & clinician goals✔
4) Family-professional partnerships ✔
5) Unmet needs (care and treatment of neurodevelopmental
disabilities/other conditions) ✔
6) Family empowerment (navigation skills, confidence) ✔
7) Family worry- about their child’s health ✔
Hypothesis -care coordination intervention; does it improve (✔) ?

SPOCS; Jan 2015-Aug 2016; n=232
SPOC / Care Coordination In Place (232)Standard of Care (AMCHP) 18 Months
• Target Population CSHCN 2-10 years old w/neurodevelopmental diagnosis followed in sub specialty programs
• SPOC as standard of care and educational instrument for “neighborhood”
• SPOC captures child/family; medical summary and goals with progress against goals
Jan 2015-Present
0
50
100
150
200
250
Jan-15 April July October Jan-16 April July


Unmet Child/Family NeedsPre/ Post Care Coordination
1. Family identified needs
2. Family identified needs met
3. Services reported received
1. No change in # (quantity) of identified needs
2. Significant + change in % of identified needs met
3. Higher # of services received for family identified needs
1. E.g.., more children received physical/occupational/speech therapy and ABA or play therapy
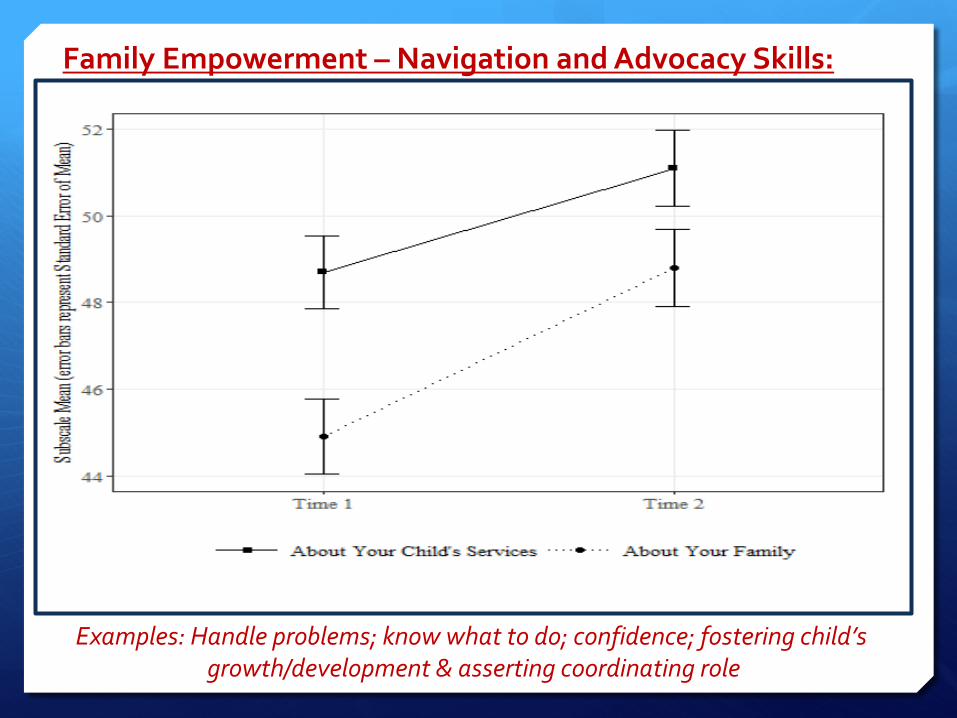
Family Empowerment – Navigation and Advocacy Skills:
Examples: Handle problems; know what to do; confidence; fostering child’s growth/development & asserting coordinating role

❦ CC is feasible and effective;
>80% of all family goals across the 7 categories “met” or “in progress”.
❦ Improved partnerships & communication pave the way for addressing unmet needs and worry
(e.g. preventive care, ABA/ therapies, nutrition, finding good school, insurance, etc.)
❦ Empowerment positively impacted,
*family/professional partnerships are integral, quality CC does not foster dependency
Reflection/ Lessons:

❦ CC requires teamwork with clear role descriptions and protected time (+ attitude, aptitude and passion help)
❦ CC supports family, subspecialty, primary care, and other efforts; a worthy investment
❦ Coaching and support needed to enable CC professionals to drive more integrated care
❦ Language matters (in so many ways)
❦ CC is rewarding, and fun….
Reflection/ Lessons:
Family Feedback
“No one asked these questions prior; I have never had a visit like this before” (Family)
“I have felt so alone in this, care coordination has opened my mind; I now know how to use the many special services available to our son” (Family).

Team Feedback
“I have spent a lifetime learning evidence-based strategies for children and families; but… the constraints of our payment system prevent me
from ensuring that families access best practices and optimal services. (Clinician)
“Learning family goals & using them to drive CC is better, I cannot go back to working the way I did before” (Coordinator)

Care Coordination ObservationsVideo: 2 parents, 1 coordinator
and 1 clinician Value:
1. Teamwork2. Personal Benefits
I. For familiesII. For health professionals
3. Efficient, effective, rewarding
Video 06 Value 2B.mov
SPoC – Examples/Spread
State Efforts (VT, MN, WI, VT, others & D70 Grants
Pediatric Learning Collaborative Efforts CARE –national States - Vermont, Maine, NIPN efforts
Health Care Transition (GotTransition)
Future - EDHI/Hearing Loss , other condition specific efforts
Linked to value based purchasing (adult) Holistic, unified approach

Homonyms -Same spelling, sound; multiple meanings
F – L – U – K -E

Homonymone word, multiple meanings
Fluke - A fish, and a flatworm.
Fluke - The end parts of an anchor.
Fluke - The fins on a whale's tail.
Fluke - A stroke of luck. (is quality care coordination a fluke?)

REAL Care Coordination - using a SPoC is an authentic pathway to family-centered care.
References ① Association of Maternal and Child Health Programs, Standards for Systems of
Care for Children and Youth with Special Health Care Needs, Antonelli, R.J., McAllister, J., & Popp, P. (2009). Making care coordination a critical component of the pediatric health care system: A multidisciplinary framework. New York, New York: The Commonwealth Fund. Standards
② American Academy of Pediatrics Council on Children with Disabilities and Medical Home Advisory Committee. (2014). Patient and family centered care coordination: A framework for integrating care for children and youth across multiple systems. Pediatrics, 133(5), e1451-e1460. Definition
③ Antonelli, R.J., McAllister, J., & Popp, P. (2009). Making care coordination a critical component of the pediatric health care system: A multidisciplinary framework. New York, New York: The Commonwealth Fund. Framework
④ McAllister, J.W. (2014). Achieving a shared plan of care with children and youth with special healthcare needs: White paper and implementation guide. Lucile Packard Foundation for Children’s Health. Retrieved from http://lpfch-cshcn.org/publications/research-reports/achieving-a-shared-plan-of-care-with-children-and-youth-with-special-health-care-needs/ Model

















